Designing and commissioning services for adults with ... · Designing and commissioning services...
39
Designing and commissioning services for adults with asthma: A good practice guide
-
Upload
nguyenduong -
Category
Documents
-
view
217 -
download
0
Transcript of Designing and commissioning services for adults with ... · Designing and commissioning services...
Designing and commissioning services for adults with asthma: A good practice guide

© PCC 2012 32 © PCC 2012
PCC | Foreword
Foreword by Professor Martyn Partridge
There are no grounds for complacency with regards to asthma. The United Kingdom has the highest prevalence of asthma in the world. Despite recent declines in death rates and hospitalisation rates, many patients do not lead lives free of symptoms and this is despite the availability of well-constructed guidelines and good medicines. Some parameters have shown a plateauing, suggesting that improvements are not being maintained and information regarding equalities in healthcare suggests that significant differences in outcomes exist between geographical areas. If we are to control asthma’s continuing burden we need to look in detail at the services available for those with the condition to ensure optimal configuration of care and services suitable for all. This document provides information for everyone involved in commissioning and delivering care to those with asthma, so that they can work alongside clinicians and patients to improve outcomes.
Professor Martyn PartridgeProfessor of Respiratory Medicine, Imperial College Londonand Senior Vice Dean, Lee Kong Chian School of Medicine,Singapore
Foreword
Part one - introduction
1. Executive summary 42. Who is this document for? 63. Why do we need to improve outcomes for people with asthma? 84. The policy context 105. Role of commissioners in improving outcomes for people with asthma 126. Guidance on good practice: How to use this guide 14
Part two - guidance on good practice
7. A patient-centred service and shared decision making 168. Preventing asthma 189. Accurate and timely diagnosis 2010. Information for patients 2211. Supporting self management 2412. Structured review by asthma-trained clinicians 2613. Optimising medication 2814. Smoking and asthma 3215. Risk assessment and at risk registers 3416. Severe/brittle/difficult-to-control asthma 3617. Asthma in the workplace 3818. Asthma and mental health 4019. Managing acute and life threatening episodes 4220. Avoiding hospital admissions and emergency department attendances 4621. Following up acute episodes 50Annex A A patient-centred asthma service checklist 54Annex B Good asthma services checklist from Asthma UK 56Annex C CQUINS: Commissioning for quality and innovation 58Annex D The Quality and Outcomes Framework 60Annex E Examples of self-management plans 62Annex F Pathway diagrams 64Annex G Levers for change 66Annex H Partner organisations 68Annex I Asthma steering group 70References 72
Contents
Acknowledgments and thanksMany people have contributed to this document by writing pieces and reviewing content. We would particularly like to express our appreciation to the following: Professor Martyn Partridge and the members of the Asthma Steering Group, Asthma UK, British Thoracic Society, Primary Care Respiratory Society UK, Hannah Wall, David Fishwick, Paul Cullinan, John White, Liam Heaney, Dermot Ryan, Bernard Higgins, Emily Humphreys, Simon Dunn, Steve Callaghan, Robert Winter, Sue Hill, Anne Moger, Matt Kearney, Joanna Clarke, Kevin Holton.
September 2012.

© PCC 2012 54 © PCC 2012
PCC | Executive summary
This good practice guide outlines the case for improving outcomes for people with asthma and what the elements of a good service look like.
Commissioners, clinicians, patients and their carers need to work together on the following areas if we are to see the step-change in asthma care that is required for the goals of asthma management to be achieved in most patients.
1. A patient-centred service and shared decision makingCommissioners should not only involve patients in the design of local services, but should also seek evidence from clinicians that they are taking a patient-centred approach to care.
2. Preventing asthmaThe causes of asthma are not well understood, so preventing asthma from developing is not possible (except in some instances where factors in the workplace can cause asthma). All efforts should focus on helping patients to lead lives as free of symptoms as possible
3. Accurate and timely diagnosis Commissioners should ensure that clinicians are adequately skilled to make an accurate diagnosis of asthma and have access to the required diagnostic facilities and expertise.
4. Information for patientsIt is important to tailor information to different patients according to their needs.
Executive summary
Asthma is a long-term condition that cannot be cured, but for most people it can be effectively managed. People with asthma live with their condition and should be the primary decision makers in the management of their own health and healthcare. Clinicians should be supporting people to make the right choices to manage their asthma, by giving them information about their condition and providing clinical expertise. Asthma varies from day to day and from person to person, so managing it daily is not a straightforward process. People need help to recognise when their asthma is worsening and when they need access to the expertise of the NHS. When they do have contact with a healthcare professional, the aim must be to make the interaction as productive as possible and this means within a partnership of care based upon a process of shared decision making. Inputs of care must also be integrated across the traditional boundaries of hospital and community-based services. All involved in designing, commissioning or providing services for people with asthma should ensure that services are designed with these principles in mind.
15. Supporting self management Commissioners should ensure that written individualised self-management plans are a key element of asthma care for all patients.
6. Structured review by asthma-trained cliniciansCommissioners should ensure that structured reviews are based on evidence based guidance and there is a regular programme of education for all involved in the care of people with the condition.
7. Optimising medicationCommissioners, clinicians and pharmacists need to consider how to achieve improved outcomes for people with asthma, while minimising wasteful use of medicines.
8. Smoking and asthmaSmoking cessation must be included in any asthma care pathway.
9. Risk assessment and at-risk registersAn asthma population could usefully be stratified according to control so that appropriate interventions can be put in place to ensure their condition remains well controlled.
10. Severe/brittle/difficult-to-control asthmaIt is important that expert or specialist services are available for this group, which may comprise only 5-10% of the asthma population, but use up to 80% of the costs of asthma care.
11. Asthma in the workplaceAccess to specialists in occupational asthma through a specially commissioned service is essential, so the cause of such asthma is effectively identified and appropriate advice given to patients.
12. Asthma and mental health There needs to be greater awareness of the need for psychological support to improve outcomes.
13. Managing acute and life-threatening episodesThis requires well-trained staff in emergency departments or other healthcare settings who have access to specialist advice and expertise in managing acute asthma, and good communication between emergency and respiratory departments. 14. Avoiding hospital admissions and emergency department attendancesAll healthcare professionals should be working with patients to ensure that loss of asthma control is identified early and appropriate steps are taken to regain control to avoid a full attack developing. Commissioners should ensure that communication between emergency services and primary care are built into asthma care pathways.
15. Following up acute episodes A full review of the patient to avert future loss of control should be specifically commissioned following an acute attack.

© PCC 2012 76 © PCC 2012
PCC | Who is this document for?
l Strategic leaders and commissioners: Locally, those leading on healthcare services, engaging with clinicians and professionals (including GPs, specialists, nurses, public health, Health and Wellbeing Boards and others) and people with asthma l Primary care: All healthcare professionals working in GP practices and non-clinical staff (eg receptionists) who are often the first person someone with asthma will see during an emergency. Primary care is the cornerstone of patient-centred asthma care
l Urgent care and hospital care: Everyone in emergency and urgent care settings (Emergency Departments, ambulances, out of hours, walk-in centres) who are involved in designing and delivering services – whether for emergency, in-patient or out-patient care, including reception staff who are receiving emergencies l Community health providers: Community health colleagues should be involved in the design and delivery of services eg community matrons, respiratory nurse specialists and consultants in integrated respiratory care
l Other health-care providers: Staff in walk-in centres, GP-led health centres, out-of-hours services providing support to people with asthma and their families
l Employers: Employers need to be aware of the needs of people with asthma. They need to understand the necessity for time off work for some people, to offer support to those whose condition deteriorates during work hours, and understand when it may be necessary to seek urgent medical help. If the asthma is caused by something in the work environment, the employer should work with the individual and specialists in occupational asthma to find ways to eliminate the cause or to distance the person from the causative factor.
Delivering excellent services requires co-operation and partnership between all those involved in the care of people with asthma.
Who is this document for?2

© PCC 2012 98 © PCC 2012
PCC | Why do we need to improve outcomes for people with asthma?Why do we need to improve outcomes for people with asthma? 3
l Asthma costs the NHS an estimated £1 billion a year. n Poorly controlled asthma is more expensive for the NHS than well controlled asthma. 1A patient whose asthma exacerbates and requires hospital treatment is likely to cost 3.5 times that of a patient who does not 2
n The cost of GP prescriptions alone for respiratory disease exceeded £1 billion in 2009/10. Respiratory products have the second highest net ingredient cost per item 3 n Research shows that 50% of asthma expenditure is spent on 5% of people with the most severe asthma 4
n The cost of hospital admissions is estimated at £61 million and aiming to reduce admissions is good for both patient care and delivers a health economic benefit. Asthma UK has estimated that at least £4.5 million could be saved if PCTs with higher than average admissions for asthma reduced their rates to the national average 5.
l The UK has the highest prevalence of asthma in the world 6. n GP records from QOF data, which are almost certainly an underestimate, suggest that 5.9% of the English population, around 3 million people, has asthma (2010-11). However prevalence rates vary from 3.5% to 7.1% across PCTs 7
n The Health Survey for England results suggest a higher prevalence of 9-10% for adults (4.68-5.2 million adults) 8.
l Mortality rates for asthma are much higher in the UK than in many other European countries 9 n Asthma deaths have preventable factors in up to 90% of cases10 n The number of deaths from asthma has only been falling gradually and appears to have plateaued over the last 5-10 years n Around 1,000 people still die from asthma each year in England and Wales, with more than 35% of deaths occurring in people under 75 11.
l Asthma cannot be prevented or cured, so attention must be focused on helping people with asthma to be free from symptoms and avoid asthma attacks
l Diagnosis may be difficult – it’s often delayed and may be wrongn In a direct access diagnostic clinic at Charing Cross Hospital, 40% of people referred with definite asthma received a confirmed diagnosis and of those referred with suspected asthma this could be confirmed in only 10% 12
l Whenever possible the diagnosis should be confirmed before starting treatment, but one-point-in-time investigations are often inconclusive and a definitive diagnosis may necessitate more than one consultation
l People with asthma do not always take their recommended treatment 13. This may be due to poor communication between healthcare professionals and those with asthma, lack of opportunity to discuss fear of side effects, omission of shared decision making or the patient not feeling in control.
l When patients do take their medication, many do it incorrectly, which will have an impact on the cost of treatment, and lead to suboptimal outcomes
l Large numbers of clinicians are not following best practice clinical guidelines 14. This will have a significant impact on patient experience and lead to poor outcomes
l In one survey, 65% of people described having had an asthma attack so severe that they were unable to talk. The Health Survey for England found that 30-40% 15 of people with asthma had had an attack in the previous 12 months 16
l Hospital admission rates in England are among the highest in the world. There is considerable variation in rate of admissions across the country 17. The NHS Atlas of Variation 2011 showed you may be six times more likely to be admitted with asthma in some parts of the country than others 18
l Quality of life is often impaired19 and people may have to take time off workn One survey found that over a quarter of people with asthma reported having missed time at work because of their asthma in the previous 12 months 20
l Asthma is responsible for at least 12.7 million lost working days each year 21
1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
1800
1600
1400
1200
1000
800
600
400
200
0
Series 1
YEAR
PERS
ONS
England deaths from asthma – all agesEngland deaths from asthma – all agesSource: ONS data 2010
l An international survey of asthma patients found that patients reported that the three most important attributes in a doctor were 22.n Listens carefully when I talk about my symptoms and problemsn Understands clearly what I am trying to expressn Explains well what asthma is and what problems it can cause.
© PCC 2012 1110 © PCC 2012
PCC | The policy contextThe policy context 4
Quality standard for asthma
The Department of Health has requested that NICE develops a quality standard for asthma and work started on this in March 2012, with a completion date of February 2013. NICE quality standards provide a clear description of what a high-quality service looks like, so organisations can improve quality and achieve excellence. They should support benchmarking of current performance against evidence-based measures of best practice to identify priorities for improvement. The NHS Atlas of Variation in Healthcare – 2nd edition (November 2011) 26
This highlighted that there may be as much as a sixfold difference in the likelihood of an asthma admission, depending on which part of the country people with asthma live in.
National review of asthma deaths 27
In the first project of its kind, work is under way to learn more about why so many people still die from asthma in the UK. Data collection for this piece of work began in February 2012, and for 12 months every death from asthma across England and the other three nations will be systematically investigated. The number of deaths from asthma in England each year has been at a plateau of around 1,000 for several years. The intention is that the learning will help to reduce the number of deaths in the future. The Royal College of Physicians runs the project and is leading a consortium of 13 organisations to try to understand the circumstances surrounding each death, so that learning from the review can be fed back into clinical practice. They expect to be reporting the results of this work in 2014.
There are several indicators in the COF for 2013/14 relevant to the treatment and care of people with asthma, including: n Under 75 mortality rate from respiratory disease n Unplanned hospitalisation for chronic ambulatory care sensitive conditions (adults) n Unplanned hospitalisation for asthma, diabetes and epilepsy in under 19s
An outcomes strategy for chronic obstructive pulmonary disease (COPD) and asthma in England (July 2011) 25
Linking respiratory disease to the current reforms, this document features a chapter on asthma and outlines how outcomes for people with asthma can be improved. The asthma objective in this strategy is: To ensure that people with asthma, across all social groups, are free of symptoms because of prompt and accurate diagnosis, shared decision making regarding treatment and on-going support as they self-manage their own condition to reduce the need for unscheduled healthcare and risk of death.
The NHS companion document to the outcomes strategy for COPD and asthma (published May 2012) outlined a set of key actions to help implement the strategy, aligned with the domains in the NHS Outcomes Framework.
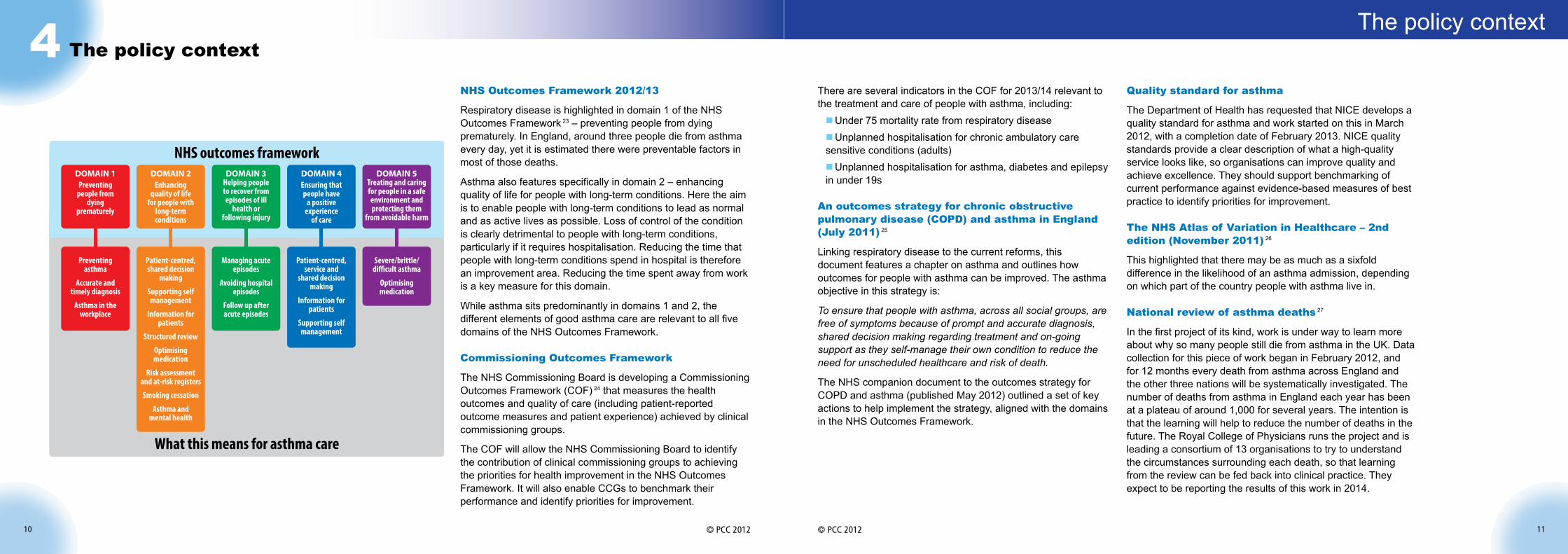
NHS Outcomes Framework 2012/13
Respiratory disease is highlighted in domain 1 of the NHS Outcomes Framework 23 – preventing people from dying prematurely. In England, around three people die from asthma every day, yet it is estimated there were preventable factors in most of those deaths.
Asthma also features specifically in domain 2 – enhancing quality of life for people with long-term conditions. Here the aim is to enable people with long-term conditions to lead as normal and as active lives as possible. Loss of control of the condition is clearly detrimental to people with long-term conditions, particularly if it requires hospitalisation. Reducing the time that people with long-term conditions spend in hospital is therefore an improvement area. Reducing the time spent away from work is a key measure for this domain. While asthma sits predominantly in domains 1 and 2, the different elements of good asthma care are relevant to all five domains of the NHS Outcomes Framework.
Commissioning Outcomes Framework
The NHS Commissioning Board is developing a Commissioning Outcomes Framework (COF) 24 that measures the health outcomes and quality of care (including patient-reported outcome measures and patient experience) achieved by clinical commissioning groups.
The COF will allow the NHS Commissioning Board to identify the contribution of clinical commissioning groups to achieving the priorities for health improvement in the NHS Outcomes Framework. It will also enable CCGs to benchmark their performance and identify priorities for improvement.
DOMAIN 2Enhancing
quality of lifefor people with
long-termconditions
Patient-centred,shared decision
making
Supporting selfmanagement
Information forpatients
Structured review
Optimisingmedication
Risk assessmentand at-risk registers
Smoking cessation
Asthma andmental health
DOMAIN 1Preventing
people fromdying
prematurely
Preventingasthma
Accurate andtimely diagnosis
Asthma in theworkplace
DOMAIN 4Ensuring thatpeople have
a positiveexperience
of care
Patient-centred,service and
shared decisionmaking
Information forpatients
Supporting selfmanagement
DOMAIN 5Treating and caringfor people in a safeenvironment andprotecting them
from avoidable harm
Severe/brittle/di�cult asthma
Optimisingmedication
DOMAIN 3Helping peopleto recover fromepisodes of ill
health orfollowing injury
Managing acuteepisodes
Avoiding hospitalepisodes
Follow up afteracute episodes
NHS outcomes framework
What this means for asthma care

© PCC 2012 1312 © PCC 2012
PCC | Role of commissioners in improving outcomes for people with asthma Role of commissioners in improving outcomes for people with asthma
What do commissioners need to know to design a good asthma service?
l Their local figures and geographical context for prevalence, consultations, attendances in emergency departments, admissions and readmissions, deaths, cost of care, cost of prescribing, smoking prevalence rates and how these vary from national and/or similar areas. This data should be available from:n The local public health observatory. n The Atlas of Variation and the respiratory atlas 28. n The IMPRESS (improving and integrating respiratory services) guide to information on respiratory disease, which provides useful pointers to data sources 29. n INHALE (Interactive health atlas for lung conditions in England), which contains valuable information on respiratory disease that can be interrogated at PCT level 30.
l What the main challenges/weaknesses/issues are in managing asthma locally
l What the clinical guidelines say about best practice
l How these translate into service needs for people with asthma
5Commissioners need to be working towards the goal of asthma management just as clinicians and patients are. By working towards freedom from symptoms for patients, they should be able to reduce emergency department attendances and asthma admissions, manage the cost of medication, and achieve improved patient experience and quality of life for the patient.
l The experience and expectations of people with asthma and their carers – people with asthma should be invited to become involved in the design and evaluation of asthma services
l What they can build into local service specifications and contracts to improve the quality of care and the patient experience
l Levers for change – the national and local levers that are available to them to drive improvements in quality and outcomes of services (see annex G).
Commissioners are in a strong position to ensure there are good communication systems across different parts of the local NHS so that the asthma patient experiences a joined- up service and potential fragmentation and duplication from multiple providers is avoided

© PCC 2012 15
Guidance on good practice: How to use this guide
14 © PCC 2012
This guide is not about managing individual patients. Instead it aims to identify the elements of good service that people with asthma need, so that:
l Commissioners know what a good service looks like and commission it
l Providers can see what a good service should comprise and deliver it.
This good practice guide is not prescriptive about where care happens (unless there is clear evidence in the guidelines), so the content will be of value both to people commissioning services from secondary care and to those considering the services that primary care and pharmacy provide.
This publication has been organised around key headings, which set out: l What the clinical guidelines say about best practice, which is relevant to service design and delivery. The SIGN/BTS asthma guideline 2011 is the source of this material unless otherwise specified 31.l What the evidence tells us – either from literature or from other studies, audits and surveys on current patterns of care in the NHS and other healthcare systemsl What this means for those who are designing, commissioning and providing servicesl Relevant examples of good practice.
At the end there is a checklist of good practice points that commissioners and providers can use to benchmark their own locality or service against.
This document has been organised around areas of weakness in asthma care, which, if addressed, could make a significant impact in improving outcomes for people who live with this condition. These are the areas that commissioners, and anyone involved in service design, should focus on. There is excellent evidence for these areas and clear guidance in the SIGN/BTS guidelines, yet they are not being translated into practice. It is these areas that this good practice guide will focus on.
Clinicalguidelines
Evidence – clinicalresearch, patientexperience andreal world data
Implications forservice design
and commissioning
Guidance on good practice: How to use this guide
Person has treatment initiated
Personpresents...
Person has regular reviews
Exacerbation
What patientscan expect
Rapid access to treatment as close to home as possible for when symptoms do
not respond to usual treatment.
This should be available 24/7,
whether in primary care, out of hours, walk-in centre or
emergency department.
Self-managementand support
Discussion of self-management
approaches as part of wider view.
Speci�c support in areas identi�ed
by person.
What patientscan expect
Regular review including:
• Assessment of controlusing e.g. RCP
3 questions.
• Assessment of inhaler usage and compliance.
• Optimisation oftreatment via shared
decision making.
• Review and revision of PAAP if necessary.
Self-managementand supportResponse to an
exacerbation as recommended in the
person’s PAAP.
Feedback o�ered in cases of optimal
self-management.
What patientscan expect
Any unscheduled intervention must be
followed up with a review to check that
control has been regained.
If not – adjust treatment and review PAAP.
What patientscan expect
Medication according to the British Asthma
Guidelines.
Start at the step appropriate to the symptoms.
Options for inhalers are discussed with
person – and choice made together.
Inhaler technique demonstrated and
taught.
Personal Asthma Action Plan (PAAP) agreed and given.
Self-managementand supportPerson o�ered
appropriate information about
treatments & necessary lifestyle
changes.
Person given contact information for all
local services including out-of-hours services
and NHS Direct.
Person given contact for independent sources
of information such as Asthma UK.
What patientscan expect
Access to healthcare sta� with appropriate
training.
Comprehensive and appropriate
investigation & diagnosis.
Diagnosis may require repeated visits
over time.
Expert opinion is available if necessary.
Self-managementand supportIndividual has opportunity to
express concerns or ask quaetions.
The individual’s understanding of
their diagnosis should be checked.
Urgent need for healthcareDiagnosis Ongoing support
with symptons suggestive of
asthma(cough, chest tightness,
wheezing or breathness
characteristically worse at night or in early morning.
The care pathway The sections follow broadly in the order of the asthma pathway shown here.
6

© PCC 2012 17
A patient-centred service and shared decision making
16 © PCC 2012
A patient-centred service and shared decision making
What is recommended in clinical guidelines
l Supporting the patient in understanding and managing their condition is underpinned by Grade A evidence in the clinical guideline resulting in the recommendation that: ‘All patients should be offered self-management education that focuses on individual needs, and is reinforced by a written personalised action plan’.
l Every consultation should therefore be seen as an opportunity to review, reinforce and extend the knowledge and skills of the patient.
l In the context of improving concordance, clinicians should ask open-ended questions to be more patient-centred – such as ‘If we could make one thing better for your asthma, what would it be?’
l Monitoring asthma control is best done by monitoring symptoms, since people with good symptom control have a low risk of exacerbations. So using one of the assessment tools for asthma is good practice – such as the RCP three questions 32 (below), the asthma control questionnaire 33 or the asthma control test 34. These ask about the impact that asthma is having on the patient’s life and their ability to undertake everyday activities.
7What does this mean for commissioners and service developers?
l People with asthma should not just be considered as service users but also as co-creators throughout the commissioning cycle, particularly in planning and reviewing services. In practice, this means:n Asking patients about the quality of local asthma servicesn Inviting patients to plan, develop and monitor asthma services in their arean Consulting with and inviting patients to become members of respiratory working groups to improve local asthma servicesn Involving patients in creating care pathways, so that the perspectives of people with asthma are central to the processn All involved in designing services for people with asthma ensuring that patients are treated as equal and expert partners with their healthcare professional at each stage of their treatment and care.l Commissioners should require providers to produce evidence of shared decision making and should expect to find this in patients’ notes. In this context shared decision-making involves:n Eliciting the patient’s goals for treatmentn Determining the patient’s relative priorities regarding symptom control and regimen conveniencen Discussing side effectsn Considering the cost of medications where relevantn Sharing with the patient a list of available treatments (both devices and dosing)n Patient and physician then coming to a mutual decision regarding the optimal treatment regimen.
Significantly enhanced concordance is seen with such interventions and a reduced need for unscheduled health care.
What the evidence tells us
l An international study including 190 UK patients with asthma reported that patients’ greatest needs were to be listened to by their clinicians when talking about symptoms and problems, a need for clear explanations about their condition, and sufficiently long consultations. n The areas of greatest disparity between their expressed need and healthcare professionals meeting their need was in receiving clear explanation of possible side effects and risks of prescribed medicine, being consulted in the choice of inhaler and receiving support to self-manage their condition 35.
l Evidence shows that adherence to medication and asthma control are improved if patients are involved in decision making about their treatment 36.
l People with asthma attending DH listening events wanted better trained staff, a more holistic approach where their lifestyle and other conditions are taken into account, to be listened to and given more information, emergency department staff who understand asthma and more joined up services across the healthcare system 37.
Examples of good practice
The Royal College of General Practitioners (RCGP) promotes a care planning approach for people with long-term conditions. It moves the focus from the clinician ‘doing’, to the clinician ‘enabling’ the patient to manage the challenges of their condition, fully supported by their GP surgery. The RCGP claims that incorporating the model of care planning into daily general practice will not only improve the health outcomes and well-being of patients, but will also save the NHS time and money by reducing hospital admissions, A&E attendance and medication expenditure 38.
Asthma UK, in partnership with other leading health and social care charities has defined good patient-centred care as including:Co-ordinated carePatients being engaged in decisions about the careSupported self-managementPrevention, early diagnosis and interventionEmotional, psychological and practical support 39.
The Royal College of Physicians (RCP) three questions
Note: one ‘yes’ indicates medium morbidity and two or three ‘yes’ answers indicate high morbidity.
1. In the last month/week have you had difficulty sleeping due to your asthma (including cough symptoms)?
2. Have you had your usual asthma symptoms (eg cough, wheeze, chest tightness, shortness of breath) during the day?
3. Has your asthma interfered with your usual daily activities (eg school, work, housework)?

© PCC 2012 19
Preventing asthma (primary prevention)
18 © PCC 2012
Preventing asthma (primary prevention)
What does this mean for commissioners and service developers?
l There is no value in developing or commissioning services designed to prevent asthma occurring (primary prevention).
8
ENVIRONMENTChanges in home
environment(moulds, cooking
methods, chemicals,pets, allergens)
Changes in outdoorenvironment
ASTHMA
SUSCEPTIBILITYGenetic factors
Early life factors
Changes in diet/ breast feeding
Maternal smoking/ETS
Use of medication
Obesity/physical activity
Vaccination
Migration
+ =
What is recommended in clinical guidelines
l The guideline states that there is little evidence for any strategies for preventing asthma from developing in children, though breast feeding may have a potential protective effect in relation to early asthma.
l The guideline suggests that 9-15% of adult onset asthma may be caused by factors in the workplace. This is the only form of asthma that can be eliminated completely if the person can be separated from the sensitiser (for more on asthma in the workplace – see section 15).
What the evidence tells us
l Unfortunately, apart from the avoidance of occupational sensitizers, asthma cannot yet be prevented from developing and cannot be cured 40. Asthma arises as result of an interaction between a susceptible host and a factor or factors in the environment.

© PCC 2012 21
Accurate and timely diagnosis
20 © PCC 2012
Examples of good practice
In a south east coast clinical commissioning group with 18 practices, interrogation of GP registers found more than 2,500 patients taking asthma medication without a recorded diagnosis of asthma. The list of patients was validated and relevant patients were called for diagnosis. Some were found to have COPD and other respiratory conditions, while others received a recorded asthma diagnosis and had medications optimised accordingly.
Accurate and timely diagnosis
What is recommended in clinical guidelines
l There is no single test to diagnose asthma. More tests need to be done and in difficult cases extra, more sophisticated testing is definitely worthwhile
l There is a well documented method for diagnosis of asthma – based on the probability of the presenting symptoms being asthma
l Initial diagnosis should be based on assessment of symptoms and a measure of airflow obstruction l Clinicians must aim for objective support for the diagnosis
l Repeated assessment and measurement may be necessary before confirmatory evidence is achieved.
What does this mean for commissioners and service developers?
l There should be access to quality assured spirometry in any setting where diagnosis of asthma takes place and it should be carried out by staff trained to perform and interpret the results of spirometry
l Healthcare professionals diagnosing asthma need to be aware and have an understanding of differential diagnosis and co-morbidity with other respiratory conditions. This is particularly important in the differential diagnosis of asthma and COPD
l Access to a comprehensive diagnostic service is required, with all appropriate tests available – eg bronchial hyperreactivity, sputum eosinophil count, exhaled nitric oxide concentration (FENO), mannitol challenge, response to trial of steroid, exercise challenge test, treatment trials and specific occupational challenge
l Community-based or community-accessed diagnostic services may enable more efficient diagnosis 43
l People with asthma have a higher risk of associated allergic conditions such as eczema and allergic rhinitis. Recognition of the coexistence of these conditions is important clinically and those configuring services for adults with asthma should ensure high awareness of the coexistence of allergy and asthma and the need for access to investigations and prompt treatment, and configuration of services which facilitates liaison between GP practices and specialist allergy services
9l Auditing GP practice records may help to identify whether a practice is taking a long time to diagnose asthma or that there are patients receiving asthma medication who do not have an asthma diagnosis or have been misdiagnosed
l Patients should be given information at point of diagnosis which is relevant, easy to understand and in an accessible format. They should be referred to reputable online information sources such as NHS Choices and Asthma UK
l The new medicines services introduced in October 2011 as a new element of the pharmacy contract, is an ideal opportunity for GPs and pharmacists to work together to improve the service given to adults who have just been diagnosed with asthma and are starting new medication
l Considering an occupational cause for asthma in adults is important. It provides the only realistic chance of cure and if it is missed then any treatment is likely to be ineffective – and other investigations pointless. See separate section on work-related asthma (section 16).
Definiteasthma
44
Normal27%
Confirmed39%
Restrictive23% (10/44)
Suspectedasthma
99
Normal76%
Confirmed11%
Restrictive7% (4/99)
55 on already inhaled therapy, 26 ICS, 5ICS/LABA
GP diagnosis or suspected diagnosis and outcome in patients referred to the Charing Cross Open Access Diagnostic Unit
What the evidence tells us
l Diagnosis can be difficult – there is no single diagnostic test so it may be confused with other lung conditions l Delayed or mis-diagnosis of respiratory conditions may be common in primary care due to underuse of spirometry or poor spirometric technique 41
l Diagnosis needs to happen efficiently – if patients are started on treatment before full diagnostic investigation, then they may not appear to have asthma 42 because their treatment is already controlling it, or they may be being treated for a condition they do not have
l Rapid and systematic diagnosis by trained staff may help to reduce consultation rates, since delays in diagnosis are associated with more consultations
l Examination of existing asthma registers in primary care suggests there are patients taking asthma medication who do not have a formal diagnosis of asthma in their notes. And when diagnosis is checked, some prove to have asthma while others are found to have COPD.

© PCC 2012 23
Information for patients
22 © PCC 2012
What is recommended in clinical guidelines
l Every consultation is an opportunity to review, reinforce and extend knowledge and skills
l Information about recognising loss of control should be part of a self-management programme
l Simple verbal and written instructions and information on drug treatment should be provided to patients and carers.
What the evidence tells us
l Giving information is an important component of any partnership approach to a long-term condition, as set out in Equity and Excellence: Liberating the NHS, and patients should be given information according to their needs and preferences l A good understanding of their condition and the situations and triggers which may bring on symptoms is key to a patient managing their asthma effectively. This is important at diagnosis when a patient may find the diagnosis hard to accept, but should also be a feature of ongoing care as the patient’s needs change
l Patients want to receive information about their medicines and potential side effects. One study found that only 58% of asthma patients in primary care felt they were given enough information about potential side effects of medication, whereas 41% said they were not given enough or would have liked more. In contrast only 37% of patients receiving new medicines in a hospital setting felt they were given enough information about side effects 44
l The same survey suggested that patients are particularly concerned that they do not get sufficient information about side effects
l GPs are giving out less information than specialists. In one study, 47% of patients with asthma reported that they were given written information by specialists, but only 28% said they received information from GPs 45
l Information given in a way that is appropriate to the level of the patient’s health literacy enabled patients who had impaired health literacy to achieve the same degree of improvement in outcomes as those with higher health literacy 46
l Giving information in isolation is not sufficient in asthma. It needs to be accompanied by structured self management support and shared decision making about treatment 47,48.
Information for patients 10
Yes, enough information
Some, but I wouldhave liked more
No
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
61% 61% 58%
21% 21% 22% 18% 18% 20%
58% given enoughinformation
41% not given enough
information orwould haveliked more
Only 37% of hospital patients being given new medications felt that they had been given complete information about side e�ectsInformation on asthma received by patients
47%
28%
Given written information by specialists Received information from GPs
Information on asthma received by patients
What does this mean for commissioners and service developers?
l Provision of information could be incorporated into an asthma care pathway so there is discussion and agreement about appropriate and consistent information for patients, which will avoid patients receiving conflicting information
l Commissioners should expect providers to demonstrate that they are providing patients with information tailored to their asthma as an individual, which encourages them to be active partners in their care
l Clinicians should be providing information to patients in a format appropriate and understandable to them, taking account of issues such as language and levels of health literacy 49. Commissioners can expect to see evidence of this in clinical practice. This sharing of information could include signposting patients to a range of sources including: n Reputable organisations such as Asthma UK and the British Lung Foundationn NHS sources such as NHS Choices n Relevant helplines n Self-management courses n Local self-support groups n Other community support resources, including local physical activity groups n Voluntary sector organisations n Other sources of information about asthma.

© PCC 2012 25
Supporting self management
24 © PCC 2012
l People with self-management plans have better control of their asthma, compliance with medication and outcomes and fewer serious events. 52 They show fewer hospitalisations, emergency dept visits, unscheduled visits to the doctor, days off work and fewer nighttime symptoms 53
l Research in 2007 found that only 23% of people with asthma had a self-management plan. 54 This was consistent with a UK study of over 500 patients, which found that 80% of people with asthma did not have a self-management plan, yet 68% of these indicated they would be comfortable following one. 55 The reasons why health professionals do not implement guideline advice regarding self management has been studied and may include:n Doubt about the evidence base and relevance to primary caren A lack of knowledge, skills and misconceptionsn Practical issues (time and resources)n Poor teamwork 56.
l Trained and paid lay educators may be able to support patient education, develop self-management plans with patients and have the same impact on outcomes, for a third of the price of a nurse 57
l Successive Cochrane reviews have demonstrated clearly the value that self management support brings to patients and the NHS and that regular clinician review is no more effective at maintaining control of symptoms than the patient taking a self-management approach 58.
What is recommended in clinical guidelines
l Self-management plans have been recommended in asthma guidelines since 1990 and are supported by Grade A evidence
l Patients with asthma should be offered self-management education that focuses on individual needs and be reinforced by a written personalised action plan
l Personalised action plans should be introduced as part of a structured educational discussion
l A hospital admission represents a window of opportunity to review self-management skills. Before hospital discharge, patients should receive written personalised action plans, given by clinicians with expertise in asthma management.
What the evidence tells us
l A survey undertaken by DH into attitudes to self management in the population, found that 90% of people with long-term conditions are interested in being more actively involved in their care and more than 75% would feel more confident about self management if they had help from a healthcare professional or peer 50
l Self management is about making therapeutic, behavioural, and environmental adjustments in accordance with advice from healthcare professionals 51. Motivational interviewing may be necessary within consultations to encourage those with asthma to take control of their own condition
Supporting self management
What does this mean for commissioners and service developers?
l Commissioners should stipulate in contracts that every patient should receive tailored information about their asthma, and have an asthma action plan, so they can respond appropriately to symptoms and particularly to any worsening of controln Evidence of written asthma action plans should be available in patients’ notes and commissioners should actively check for this.
l Commissioners should know the percentage of patients in their locality that have written asthma action plans l Commissioners should ensure that no patient with asthma leaves hospital without a written self-management plan, developed jointly by the clinician and patient, and a discussion about how to avoid future exacerbations. This should be communicated to the patient’s practice and pharmacist, so they can reinforce the content of the plan, and give consistent advice. This includes patients who have been in-patients and those who have attended an emergency department. This could be incorporated into a CQUIN or discharge bundle.
11Examples of good practice
See examples of self-management plans in Annex E.
Asthma UK has a range of resources to support patients in understanding their condition and in managing their own asthma. This includes a checklist of the information they need, and the actions they need to be able to take in the event that their asthma worsens. The Be in Control pack is available from its website, and includes a personal asthma action plan, a medicine card, a peak flow diary and a copy of Making the Most of Your Asthma Review.
http://www.asthma.org.uk/all_about_asthma/controlling_your_asthma/resources_to_help_you/index.html
© PCC 2012 27
Structured review by asthma trained clinicians
26 © PCC 2012
What is recommended in clinical guidelines
l Proactive regular reviews have been shown to improve clinical outcomes such as reducing exacerbation rates, improving symptom control and reducing attendance at emergency departments and time off work. People most at risk of fatal or near-fatal asthma are those who do not participate in regular review l Regular reviews are most effective when they include discussion and use of a written action plan
l Outcomes are probably similar regardless of whether it is a practice nurse or GP that undertakes the review, but clinicians trained in asthma management achieve better outcomes for their patients
l Exact frequency of the review will vary according to the severity of the condition, but should be at least annually
l Reviews by telephone may be as effective as face-to-face consultations, unless asthma control is poor or there are problems with inhaler technique
l It is recommended that an audit is undertaken of the percentage of clinicians who have undertaken a suitable educational update on asthma in the previous two years.
What the evidence tells us
l As early as 1991, research showed that regular structured review can improve symptom control, reduce exacerbations and reduce time lost from work 59
l Regular review is most effective when combined with self management support 60
l Regular review should include specific morbidity questions, possibly using one of the recognised assessment tools to establish symptom levels, examination of frequency of use of short-acting bronchodilators (quantity may indicate poor control) and recent history of acute attacks. Adherence to treatment, inhaler technique, smoking status, trigger factors and concomitant rhinitis should all be checked 61
l There is increasing evidence that regular review carried out by a telephone consultation may be as effective as a face-to-face consultation. It may enable more people to receive a review, and may take a shorter time, with no loss of clinical efficacy or patient satisfaction 62
l The Quality and Outcomes Framework in the GMS contract recommends that all patients with asthma are reviewed every 15 months. Since April 2012, it is expected that clinicians will ask patients specific questions about waking at night, symptoms during the day and whether asthma interferes with daily activities (known as the Royal College of Physicians (RCP) three questions - see page 18)
l Healthcare professionals who have received asthma training are better equipped to manage asthma. A survey in 2009 found that less than half of primary care healthcare professionals who responded to an online survey answered questions on British asthma guidelines correctly, with scores lower among GPs than practice nurses 63.
Structured review by asthma trained clinicians12What does this mean for commissioners and service developers?
l Commissioners should ensure that regular reviews are being undertaken by a nurse or GP who has received training in asthma management and commission education and training accordingly
l Commissioners should check the quality of the regular reviews being conducted and whether the detail of what a review should comprise, as outlined in the QOF guidance notes, is being followed by practices
l Where there are high QOF exception rates for asthma reviews, pharmacists can play an important role in encouraging people to attend their GP practice for regular review. The new targeted medicines use review (MUR) service introduced in October 2011, which aims to encourage MURs in respiratory conditions, presents an ideal opportunity for pharmacists to discuss medication issues and improve concordance, and should be actively encouraged by commissioners. Commissioners should ensure that pharmacists have adequate asthma training
l Practices with high numbers of asthma patients excepted from the QOF indicator for regular review should be investigated and encouraged to find ways of reviewing them. This may require the commissioning of good communication between practices and pharmacists
l Audit the number of primary care clinicians who have received specific education in asthma in the previous two years.
Examples of good practice
A clinical commissioning group of 19 practices in the south east coast convened a multi-disciplinary clinical group to create an asthma review template for completion by nurses with asthma patients in all practices with read codes for separate parts of the review eg inhaler check and self-management plan issued. This ensures standard training and work for staff undertaking the reviews and equality of treatment for an asthma patient having a review in any practice, which can be easily monitored.

© PCC 2012 29
Optimising medication
28 © PCC 2012
What is recommended in clinical guidelines
l A step-wise approach to asthma medication is now well established, according to the degree of control of asthma
l Patients are more likely to under-use than over-use medication. Patient self-reporting and clinician assessment both overestimate regular use of prophylactic medication
l Good asthma control is associated with little or no need for short-acting bronchodilators
l Frequency of use of short-acting bronchodilators and oral steroids are indicators of poor control. Heavy or increasing use of short-acting bronchodilators is associated with asthma death
l Before initiating a new therapy, clinicians should recheck adherence, inhaler technique and eliminate trigger factors
l Inhaled steroids are the most effective preventer drugs for adults for achieving overall treatment goals. They should be prescribed to any patient using their short-acting bronchodilator treatment three times a week or more
l Inhaled steroids should be considered in any patients who have had a course of oral steroids in the previous two years
l No patient should leave hospital without being on an inhaled steroid
l Combination products of inhaled steroids and long-acting bronchodilators are considered to aid compliance in asthma care and ensure that long-acting bronchodilators are not taken without inhaled steroids, in line with Medicines and Healthcare products Regulatory Agency (MHRA) guidance on safety.
l Regular review should be conducted in order for appropriate stepping down of treatment to be initiated if control is good
l Simple verbal and written instructions and information on drug treatment may help to improve concordance and may be incorporated into a self-management plan.
What the evidence tells us
l Pharmacological treatment is the mainstay of asthma management
l Regular use of low dose inhaled steroids is associated with a reduced risk of death from asthma 64
l Poor concordance with treatment is a significant issue in asthma management. People with asthma don’t always take their medicines as prescribed or fully appreciate the level of control they can have over their asthma. They need help understanding that the benefits of medicines far outweigh the risk of side effects. Concerns about the safety of treatment are often at the root of poor adherence
Optimising medication 13Study of patients with
severe asthma
82%
21%
Not complying with treatmentafter initial denial
Actually collected alltheir prescriptions
Study of patients withsevere asthma
l Poor concordance may be linked to suboptimal doctor patient communication, lack of opportunity to discuss side effects, omission of shared decision making and not feeling in control
l In a study of patients with severe asthma, 82% admitted to not adhering to treatment after initial denial, and only 21% actually collected all their prescriptions. 65And in a study across five countries, over half the asthma patients reported adjusting their regular treatment according to how they feel 66.
l Poor inhaler technique is common and can lead to patients not getting the benefit they should from their medication. Inhalers should only be prescribed after a patient has received training in the use of that specific device and inhaler technique should be checked and demonstrated as part of regular review
l Though it is critical that concordance with current treatment, inhaler technique and elimination of trigger factors are checked before any changes are made to treatment, this is generally not done systematically in practice
l The step-wise asthma guidelines are not being followed by many clinicians. Combination treatments should only be used after inhaled corticosteroids are found to provide inadequate levels of control. In a study looking into the patterns of prescribing leading up to initiation of a combination (steroid/long acting bronchodilator) treatment, only 52% of patients had been prescribed an inhaled corticosteroid on its own in the 12 months before receiving a combination treatment for the first time 67. Considerable savings could be made if inhaled corticosteroids are used first and are sufficient to achieve control of patients’ asthma.

© PCC 2012 31
Optimising medication
30 © PCC 2012
What does this mean for commissioners and service developers?
l Practices can be asked to audit their asthma register to determine the number of prescriptions for short-acting bronchodilators, since this is an indicator of poor control. Use of a short-acting bronchodilator three times a week or more is an indication that treatment should be stepped up. All patients using more than two canisters a month (or 10-12 puffs a day) should be called for review, because such high usage is a marker of poorly controlled asthma
l Prescribing records can be examined to ensure that no long- acting bronchodilators are being prescribed without inhaled corticosteroids, following a review in 2007 by and safety advice from the MHRA
l Prescribing records can be audited to check whether inhaled steroids have been tried on their own and whether control can be achieved, before stepping up to combination treatment. Considerable savings may be possible
l Patients on doses of inhaled corticosteroids greater than 1,000mcg beclometasone (or equivalent) whether as monotherapy or as part of combination therapy should be reviewed and stepped down or referred for specialist assessment. There is a real opportunity to reduce the cost of prescribing. Auditing use of high dose inhaled steroids may enable the dose to be reduced, which may reduce side effects and produce savings. Asthma is different from many other long-term conditions where there is deterioration over time and escalation of treatment.
l Patient notes could be audited to see whether there has been any documented discussion of stepping down treatment
l The new medicines service (NMS) and medicines use reviews (MURs) are both tools in the pharmacy contract (October 2011) that can help people get the best from their medicines and improve adherence to medication. They are targeted to respiratory patients, and both pharmacists and GP practices should see that these services are offered to their patients with asthma
l Primary care arrangements for the supply of repeat asthma medications should be optimised and every person encouraged to get repeat supplies when they start using their last full inhaler(s), so that exacerbations do not develop simply because supplies of medication run out.
Examples of good practice
Asthma patients under the Durham and Easington Clinical Commissioning Group are now signposted to local pharmacists offering the medicines use review service if they are on high- dose steroids, have not attended an annual review or have used more than six blue inhalers within the past 12 months. A pharmaceutical company that works with the CCG has trained pharmacists to conduct thorough face-to-face reviews. They have also received a template to undertake the review (including the asthma control test), which can be returned to the patient’s local GP for their healthcare records to be updated.

© PCC 2012 33
Smoking and asthma
32 © PCC 2012
What is recommended in clinical guidelines
l Direct or passive exposure to cigarette smoke adversely affects quality of life and lung function and affects the need for rescue medications for acute episodes of asthma
l Current and previous smoking reduces the effectiveness of inhaled steroids, which may result in higher doses being required to achieve control. Inhaled steroids are the mainstay of preventer therapy for asthma
l Stopping smoking needs to be vigorously encouraged for all patients with asthma who smoke (guidelines from Global Initiative for Asthma – GINA) 68.
What the evidence tells us
l Of people with asthma attending hospital for urgent asthma care 33% were current smokers and 18.8% said they had previously been smokers. 69 In contrast, current estimates of smoking prevalence in the general population are around 21% 70
l International studies have found that large numbers of people with asthma are current or past smokers. 71 One study found that 39% of people with asthma in Europe are current smokers and concluded that the high prevalence of smoking remains a major barrier to combating the global burden of asthma 72
l An analysis of admissions from over 8,000 practices found that for every 1% increase in smoking prevalence in a local area, asthma admissions rise by 1% 73.
What does this mean for commissioners and service developers?
l Commissioners should know how many patients on asthma registers are current smokers
l Commissioners should expect every patient with asthma to be encouraged to stop smoking and offered the appropriate support to do so
l Commissioners should ask hospitals to gather data on the number of patients with asthma who attend emergency departments or are admitted, and are current or past smokers
l A hospital attendance provides an opportunity to refer a patient with asthma who smokes to a stop smoking service. Commissioners should build this into contracts with secondary care
l Stop smoking services should have specific and compelling messages for people with asthma who smoke, to spell out the benefits of stopping to themselves and their children l Maternity hospitals should have specialist support services to help women to stop smoking during pregnancy.
Smoking and asthma 14Examples of good practice
The National Centre for Smoking Cessation and Training has an excellent training module on how to deliver very brief advice on quitting smoking.
Smoking related to patients attending hospital for urgent asthma care
33%
Current smokers
18.8%
Had previously been smokers
21%
Smoking prevalence in thegeneral population

© PCC 2012 35
Risk assessment and at-risk registers
34 © PCC 2012
What is recommended in clinical guidelines
l Patients with poor lung function and with a history of exacerbations in the previous year may be at greater risk of future exacerbations, so may need more frequent monitoring than an annual review l Specifically identifying patients with high risk asthma (eg those with frequent admissions) in an effort to target more detailed input is logical but supported by limited evidence.
What the evidence tells us
l The risk of an asthma attack increases with each increasing treatment step of the BTS/SIGN asthma guideline. Therefore early identification of factors associated with the risk of an attack could contribute to better management 74
l The NHS has developed a range of tools to help to profile people with long-term conditions according to their risk status. These enable a greater focus on those most at risk, so that resources and interventions can be targeted to them accordingly 75
l The long-term conditions pyramid highlights that stratifying patients into three categories according to the degree of resource and attention that they need is a useful approach for all long-term conditions. So around 70-80% of people with a condition may be managed appropriately by supporting them to self manage and providing them with sufficient information about their condition. At the top, a smaller number will be living with more complex conditions, which require more intensive interventions using a case management approach.
What does this mean for commissioners and service developers?
l Patients at risk of future exacerbations should be put onto a high risk register and offered more frequent reviews and encouraged to attend. This includes those with poor lung function, a history of exacerbations or course of oral steroids in the previous six months, using a bronchodilator more than five times a day, concomitant allergic rhinitis, food allergy or psychosocial problems
l Commissioners can expect practices to have identified their high risk asthma patients. Those who have had an attack in the previous 12 months are likely to cost 3.5 times as much as someone who has not had an asthma attack 76.
Risk assessment and at-risk registers15
LEVEL 170-80% of a Chronic CareManagement population
LEVEL 2High risk patientsCare management
LEVEL 3Highly complex
patientsCase management
HEALTH PROMOTION
Examples of good practice
Triple A test: avoid asthma attacks: Asthma UK has developed the triple A asthma test – an online test that people with asthma can take to check whether they are at risk of an asthma attack. By answering eight questions about their medication, other conditions and recent asthma control, their risk of an asthma attack is assessed and they are advised about any action they should take. Asthma UK is collecting the data from this test and will be publishing the results and undertaking further work to develop a validated risk-assessment tool tailored for commissioners, clinicians and people with asthma. http://www.asthma.org.uk/all_about_asthma/triple_a_test_avoid.html
ESyDoc Clinical Commissioning Group stratified adult asthma patients with a confirmed diagnosis (read-code recorded) into three key cohorts. The most at risk cohort was defined as 18 years or over, with asthma diagnosis in QOF, one read code of exacerbation and one read code of hospitalisation within the past 12 months. All patients within the three cohorts were called for nurse-led clinic review over a six month period and over the course of the year-long project admissions reduced by 21% from the previous year.
Stratifying patients according to need continues to be a vital component of the Long Term Conditions (LTC) generic model and key to the delivery of good LTC management. By using a risk prediction approach it is possible to identify those people who are the most regular users of hospital services (and are at risk of re-admissions), then stratify them according to complexity of need and commission cost effective interventions to meet those needs. Stephen Johnson, Deputy Director - Head of Long Term conditions, DH August 2011

© PCC 2012 37
Severe/brittle/difficult-to-control asthma
36 © PCC 2012
Severe/brittle/difficult-to-control asthma
What is recommended in clinical guidelines
l The guideline defines difficult asthma as persistent symptoms and/or frequent exacerbations despite treatment at step four or five of the treatment pathway
l Poor adherence, psychosocial factors and concomitant conditions are associated with difficult asthma, so a comprehensive approach to assessment, diagnosis and management is key
l Patients with difficult asthma should be systematically evaluated – to confirm diagnosis, to identify the mechanism of persisting symptoms and assessment of adherence
l Patients need a dedicated multidisciplinary difficult asthma service by a team experienced in the assessment and management of difficult asthma
l Patients with brittle asthma or who have had near-fatal asthma should be under specialist supervision indefinitely.
What the evidence tells us
l Estimates of the burden of patients with difficult asthma range from 5% of patients being responsible for 50% of asthma costs 77 to 20% of patients accounting for 80% of expenditure 78
l Non-adherence is an important issue to address in patients with severe asthma and may deliver as significant a benefit as an expensive novel treatment. 79 In a study exploring medicine-taking in these patients, 88% admitted to poor adherence after initial denial and 45% were non-adherent with oral steroids, which are taken when asthma is severe 80
l There are seven centres in the UK which provide support for severe asthma. This network submits data to a national registry to gather information about this group of patients.
16
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
Measurements and main results (182 patients assessed)
63%
�lled 50% or fewer inhaled
medication prescriptions
21%
�lled more than 100% of presciptions
45%
�lled between 51 and 100%
of presciptions
88%
poor adherencewith inhaled therapy after initial denial
45%
nonadherentto prescribedoral steroid
Measurements and main results (182 patients assessed)Source: Gamble Non-adherence in difficult asthma
What does this mean for commissioners and service developers?
l Commissioners should ensure that services are available in their area for those with difficult asthma, as this has traditionally been a very poorly served subgroup of the asthma population. Special clinics for this group are currently not available in all parts of the country
l Commissioners may wish to encourage all large departments of respiratory medicine to consider appointing one respiratory physician to have special responsibility for asthma in the same way that there are usually leads for lung cancer, TB and COPD
l Such services need to have specialist diagnostic and monitoring methods available so that treatment is finely tailored to the needs of patients. They should also offer treatment and support from psychologists, dieticians and physiotherapists as well as specialist doctors and nurses in respiratory disease and allergy
l People with difficult asthma may need help continuing to work or may be eligible for disability benefit. Many patients do not get this level of recognition and support which a multidisciplinary holistic service can provide
l Commissioners should ensure that newer treatments are available for people with severe asthma. NICE has issued guidance on omalizumab and bronchial thermoplasty, which would both be indicated for initiation by specialist severe asthma clinics for appropriate patients. New biologics are also becoming available and would be trialled by these centres.
Examples of good practice
Asthma UK has published a useful document on the challenges and issues faced by patients with severe asthma – Fighting for breath: the hidden lives of people with severe asthma 81.

© PCC 2012 39
Asthma in the workplace
38 © PCC 2012
What is recommended in clinical guidelines
l It recommends a high degree of suspicion in adults presenting for the first time with symptoms of asthma and appropriate investigation by someone with experience and detailed knowledge in this field. 82 The ‘Standard of Care’ recommends asking adults what they do for a living as a minimum, to determine whether occupational asthma is unlikely or possible
l Someone with possible work-related asthma should be referred quickly to a chest physician or occupational physician with a particular interest in occupational asthma. These specialists are all members of the group of occupational respiratory disease specialists (GORDS) and are listed on the GORDS website 83. They are also the people best placed to offer appropriate employment (and compensation) advice l The diagnosis of occupational asthma should be confirmed by a specialist in this field and should not be based solely on the medical history. Objective information from tests is needed, given the overall importance of diagnosis 84,85 l If work-related asthma is diagnosed, they recommend removing the worker from exposure or reducing exposure where removal is not practical or acceptable, as soon as possible.
What the evidence tells us l Work-related asthma is the commonest occupational lung disease in the developed world. Several hundred agents have been reported to cause occupational asthma 86
l Generally occupational asthma has a poor prognosis and is likely to persist and deteriorate unless identified early and effectively 87
l Unemployment may be result of diagnosis in around a third of cases and this proportion of cases may still be out of work up to six years after diagnosis 88.
Asthma in the workplace17
What does this mean for commissioners and service developers? l Commissioners should ensure that services are available to investigate patients and workers. These should identify workplace allergens that may be causing asthma which develops in adults, where there is a high suspicion that the cause may be allergens in the workplace. Investigation should first confirm a diagnosis of asthma, then confirm the relationship between asthma and work exposure, and finally identify the specific cause. Once a diagnosis is made, appropriate advice should be given to workers. It is also important to exclude a diagnosis where possible as this will allow workers to continue to work safely l A clear pathway should be in place to ensure that patients can be referred quickly to specialist services.
Source Agent or job
Most commonly reported agents causing (OA)
Isocyanates, flour and grain dust, colophony and fluxes, latex, animals, aldehydes, adhesives, metals, resins and wood dust
Workers most commonly reported to surveillance schemes of (OA)
Animal handlers, bakers and pastry makers, chemical workers, food processing workers, hairdressers, paint sprayers, nurses and other health professionals, timber workers and welders
Workers reported from population studies to be at increased risk of developing asthma
Bakers, chemical workers, cleaners, cooks, electrical and electronic production workers, farm workers, food processors, forestry workers, healthcare workers, laboratory technicians, mechanics, metal workers, painters, plastics and rubber workers, storage workers, textile workers, waiters, welders and wood workers.
Common agents and jobs related to occupational asthma (OA)

© PCC 2012 41
Asthma and mental health
40 © PCC 2012
What is recommended in clinical guidelines
l People with severe and difficult-to-control asthma tend to have a high level of psychological morbidity
l Assessment of co-existent psychological morbidity should be performed as part of a difficult asthma assessment.
What the evidence tells us
l Psychological conditions such as anxiety and depression may be up to six times more common in people with asthma 89 and may be associated with poor control
l People with asthma who also have depression or anxiety experience more asthma symptoms and have worse outcomes in terms of higher use of healthcare resources, increased healthcare costs, less successful emergency treatment and increased hospitalisation 90
l Poorly controlled asthma can also be a cause of poor mental health in itself and patients with severe asthma have more psychological distress and difficulty coping with their disease, both emotionally and behaviourally, compared to patients with moderate asthma
l Psychological issues may be responsible for some of the risk-taking behaviours of people with asthma, such as not taking their medication and smoking 91.
Asthma and mental health 18What does this mean for commissioners and service developers?
l Commissioners should ensure that psychological support is available and easily accessible for people with asthma
l Services for severe asthma should have psychological assessment and support as a core part of their service and included as part of a commissioned pathway.
© PCC 2012 43
Managing acute and life-threatening episodes
42 © PCC 2012
Managing acute and life-threatening episodes
What is recommended in clinical guidelines
l Mild to moderate exacerbations should be treated by a short acting bronchodilator in a standard inhaler (pressurised metered dose inhaler) with spacer
l All possible initial contact personnel such as practice receptionists, ambulance call takers and NHS Direct should be aware that asthma patients complaining of respiratory symptoms may be at risk and should have immediate access to a doctor or trained asthma nurse
l The guideline articulates clear criteria for when patients with acute asthma should be admitted and discharged
l Nebulised beta agonist bronchodilators, where indicated, should preferably be driven by oxygen, not air-driven compressors
l The guidelines provide clear guidance for the assessment and treatment of acute asthma in general practice, the accident and emergency department and in hospital (see annexes 2- 8 of the British asthma guideline). Guidelines also mention that if clinical staff fail to assess severity of an acute exacerbation by objective measurement and under-use of corticosteroids it can lead to poor outcomes including avoidable deaths.
What the evidence tells us
l It was reported in 2008 that 57% of people with asthma were poorly controlled. Over 50% were having daytime symptoms more than once a week and almost 40% were having their sleep interrupted 92,93
l There is a six-fold variation between PCTs in the number of acute admissions for asthma in adults around the country. The range is from 30.1 to 193.0 admissions per 100,000 adult population. Some variation may be due to local population characteristics, but much is unwarranted and due to differences in the quality of asthma care and the support people receive to manage their condition 94
l Emergency hospital admissions are extremely costly and account for £61 million of the estimated £1 billion cost of asthma to the NHS each year. However, it has been estimated by Asthma UK that at least £4.5 million could be saved if PCTs with higher than average admissions for asthma committed to reducing their rates to the national average 95
l Around 75% of asthma admissions are considered to have preventable factors
19l Many emergency departments are still using nebulisers to deliver short-acting bronchodilators for emergency care, but a standard inhaler with a spacer device has been shown to be as effective, for all except those with severe asthma or life threatening asthma.
l As much as a third of the cost of managing asthma may be related to emergency attendances, hospitalisation and death, with hospitalisation accounting for between 20 and 25% of the overall cost. There is significant scope for reducing costs by improving disease control 96
l When direct and indirect costs are taken into account, as much as 75% of the cost of asthma may be attributable to suboptimal control.
50%
Having daytime symptomsmore than once a week
40%
Having their sleepinterrupted
Reported 2008

© PCC 2012 45
Managing acute and life-threatening episodes
44 © PCC 2012
What does this mean for commissioners and service developers?
l Since poorly controlled asthma is costly, the efforts of commissioners should be firmly focused on achieving and maintaining good control in as many patients as possible
l Acute attendances and admissions may have their roots in prior care in the community and in patient self management, so a system-wide approach will be needed to address poor control
l Ambulance staff may be the first healthcare professionals people will encounter in an emergency. They need to have the right skills and training to provide support before they can reach more specialist treatment. They also need to be able to distinguish between people who need hospitalisation and those who could safely be redirected to community services
l Commissioners should ensure that all NHS staff involved with patients experiencing an exacerbation have appropriate training in arranging rapid assessment, including receptionists, in all healthcare settings which patients may attend in an emergency
l Out-of-hours and walk-in centres are increasingly the first port of call for people experiencing an exacerbation. Staff in these settings need to be as well trained as in all other settings and in particular need to have close communication with primary care to ensure prompt and appropriate follow-up after the episode. It is particularly important that out-of-hours services are aware of people at greatest risk of having an attack, are knowledgable and competent in dealing with asthma attacks
l There is overuse of nebulisers in acute situations. Delivery of short acting bronchodilators by nebuliser instead of by standard inhaler with spacer can encourage a reliance on hospital care. It can lead to repeat hospital attendances by patients, when delivery using an inhaler and spacer may be adequate. Commissioners are advised to ensure that emergency departments are not using nebulisers routinely for treatment of acute attacks, except where appropriate
l Commissioners should ensure that oxygen driven rather than air-driven nebulisers are used when nebulisers are considered necessary. This will prevent oxygen desaturation that can occur with air-driven compressors
l Commissioners should ensure that each person admitted with asthma receives a detailed assessment by a respiratory specialist before discharge
l Patients who are admitted should be nursed in a ward where nurses have adequate experience in monitoring the acutely ill patients and are proficient at administering medications
l Every acute unit should have an individual who is responsible for ensuring that their asthma care across all departments conforms to British asthma guidelines and keeps records and audits processes and outcomes l Commissioners should consider setting up a CQUIN for acute asthma care to encourage adherence to best practice guidelines.
Examples of good practice
NHS Yorkshire and the Humber has developed a CQUIN for the management of asthma in emergency departments. This clearly sets out the components of good asthma care that commissioners expect to see implemented in emergency care. They expect that ‘by providing the correct assessment, education and support, re-attendance rates will be reduced, admissions prevented and patient outcomes improved.’ See annex B for the full CQUIN.
St Guy’s and St Thomas’ Teaching Hospitals NHS Foundation Trust introduced an asthma proforma for use with all asthma related A&E attendances, supported by continual training and awareness sessions from the asthma specialist nurse. The form ensures a standard approach for staff to all asthma patients and is fully compliant with the BTS-SIGN guidelines, which will also help compliance with future BTS audits. It also contains a section on good practice discharge actions eg a follow-up letter for patient to take to their local GP.
Asthma UK has produced an emergency asthma care pack to assist all healthcare professionals (including pharmacists) who come into contact with people with asthma at the time of an attack. This is to develop good quality care from when the person first presents through to their discharge and follow-up arrangements.
Deaths from asthma
l Although it is a highly prevalent condition, asthma has a low mortality rate. However, deaths do occur and are often sudden and unexpected
l Bereavement services are required for the families of people who die from asthma. Families are often not involved in significant event analysis and do not have the opportunity to ask questions about why their family member died. Proper services should be provided to support them following the death of a family member.

© PCC 2012 47
Avoiding hospital admissions and emergency department attendances
46 © PCC 2012
What is recommended in clinical guidelines
l Most attacks of asthma severe enough to require hospital admission develop relatively slowly over a period of six hours or more. So there’s enough time for effective action to reduce the number of attacks requiring hospitalisation
l Steroids reduce mortality, relapses, subsequent hospital admissions and requirement for Beta-2 agonist therapy. The earlier they are given in an acute attack the better the outcome
l Before discharge, trained staff should give asthma education. This should include inhaler technique, a symptom and peak- flow based action plan, which allows the patient to adjust their medication within recommendations. These measures have been shown to reduce morbidity after exacerbation and reduce relapse rates
l A respiratory specialist should follow up patients admitted with severe asthma for at least a year after the admission
l A register of patients at risk may help primary care health professionals to identify patients who are more likely to die from their asthma, and therefore such a register may also help to identify those most likely to seek emergency hospital care.
What the evidence tells us
l An analysis of ED attendances for acute asthma identified that 30-40% had been admitted in the previous 12 months, and a quarter had attended an emergency department in the previous three months 97,98
l The British Thoracic Society acute asthma audit in 2011 showed that 9.5% of people admitted for asthma had also been
admitted in the previous month. This figure has been relatively static in recent years, though was lower in 2010 (7.4%). There was a rise in the numbers of patients re-admitted between three and 12 months following discharge – 15.1% in 2011 compared with 12.3% in 2010 99
l Most patients with asthma have symptoms for several days/nights before attending an emergency department, so there is time for interventions to prevent the asthma attendance happening 100
l Many aspects of managing acute attacks is not being carried out in accordance with the guideline.Initial assessment is suboptimal. Peak flow readings are not being taken on presentation or after bronchodilator treatment, although this is a key step in determining severity and informs the decision as to whether to admit 101
l Early use of steroids is key for managing acute asthma, yet only 46% of patients have steroids started within an hour of arriving in hospital or before arriving in hospital 102 l Patients with self-management plans have fewer asthma events, 103 and the Cochrane review noted that they show fewer hospitalisations, emergency department visits and unscheduled visits to the doctor 104. l The estimated probability of having an exacerbation in any week is higher the more uncontrolled the asthma is the previous week 105
l Follow-up after an acute admission, which is important to prevent future re-admissions is a significant area of weakness in asthma management (see next section).
Avoiding hospital admissions and emergency department attendances 20
10%
9%
8%
7%
6%
5%
4%
3%
2%
1%
0%
7.4%
The British Thoracic Society acute asthma audit 2011
Admissions for asthma who had also been admitted in the previous month
2010
9.5%
2011
20%
18%
16%
14%
12%
10%
8%
6%
4%
2%
0%
12.3%
Number of patients readmitted between 3 and 12 months following discharge
2010
15.1%
2011
The British Thoracic Society acute asthma audit 2011 What does this mean for commissioners and service
developers?
l Since it is usually possible to identify deterioration in symptoms before this happens and prevent emergency department attendances and admissions, commissioners are advised to focus on initiatives that will help to achieve this, for example identifying the people who have attended once or more in previous 12 months are at-risk patients (see sections 13 and 14). This creates the opportunity to: n Review these patients’ management in detail
n Support patients in their understanding of how deterioration happened
n Put written asthma management plans in place
n Give patients a number to call for urgent advice should symptoms deteriorate n Ensure practices give priority appointments to these patients when they seek a consultation
n Alert ambulances to these patients to explore whether a member of the community team can attend
n Recall such patients for review in primary care more frequently than annually and see them in their home if necessary
l Commissioners should require emergency departments to audit the extent to which they are delivering care in line with the guidelines, and to compare their own performance in the British Thoracic Society acute asthma audit with the national findings
l Commissioners should consider setting up a CQUIN for acute asthma care to encourage adherence to best practice guidelines.
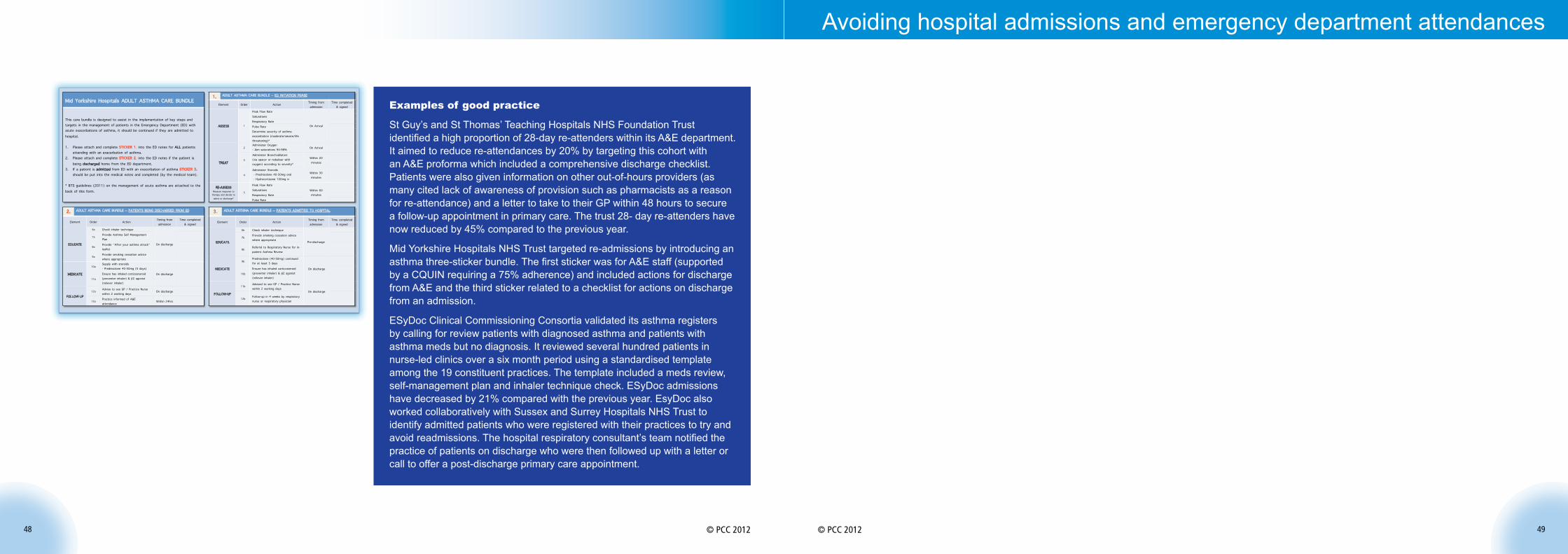
© PCC 2012 49
Avoiding hospital admissions and emergency department attendances
48 © PCC 2012
Examples of good practice
St Guy’s and St Thomas’ Teaching Hospitals NHS Foundation Trust identified a high proportion of 28-day re-attenders within its A&E department. It aimed to reduce re-attendances by 20% by targeting this cohort with an A&E proforma which included a comprehensive discharge checklist. Patients were also given information on other out-of-hours providers (as many cited lack of awareness of provision such as pharmacists as a reason for re-attendance) and a letter to take to their GP within 48 hours to secure a follow-up appointment in primary care. The trust 28- day re-attenders have now reduced by 45% compared to the previous year.
Mid Yorkshire Hospitals NHS Trust targeted re-admissions by introducing an asthma three-sticker bundle. The first sticker was for A&E staff (supported by a CQUIN requiring a 75% adherence) and included actions for discharge from A&E and the third sticker related to a checklist for actions on discharge from an admission. ESyDoc Clinical Commissioning Consortia validated its asthma registers by calling for review patients with diagnosed asthma and patients with asthma meds but no diagnosis. It reviewed several hundred patients in nurse-led clinics over a six month period using a standardised template among the 19 constituent practices. The template included a meds review, self-management plan and inhaler technique check. ESyDoc admissions have decreased by 21% compared with the previous year. EsyDoc also worked collaboratively with Sussex and Surrey Hospitals NHS Trust to identify admitted patients who were registered with their practices to try and avoid readmissions. The hospital respiratory consultant’s team notified the practice of patients on discharge who were then followed up with a letter or call to offer a post-discharge primary care appointment.
1.! ADULT ASTHMA CARE BUNDLE – ED INITIATION PHASE !
Element! Order! Action!Timing from
admission!
Time completed
& signed!
ASSESS ! 1!
Peak Flow Rate!
On Arrival!
Saturations!
Respiratory Rate!
Pulse Rate!
Determine severity of asthma
exacerbation (moderate/severe/life
threatening)*!
TREAT!
2!Administer Oxygen!
- Aim saturations 94-98%!On Arrival!
3!
Administer Bronchodilators !
(via spacer or nebuliser with
oxygen) according to severity* !
Within 20
minutes!
4!
Administer Steroids!
- Prednisolone 40-50mg oral!
- Hydrocortisone 100mg iv !
Within 30
minutes!
RE-ASSESS!Measure response to
therapy and decide to
admit or discharge* !
5!
Peak Flow Rate!
Within 60
minutes!
Saturations!
Respiratory Rate!
Pulse Rate!
2.! ADULT ASTHMA CARE BUNDLE – PATIENTS BEING DISCHARGED FROM ED!
Element ! Order! Action!Timing from
admission!
Time completed
& signed!
EDUCATE!
6a! Check inhaler technique!
On discharge!
7a!Provide Asthma Self Management
Plan!
8a!Provide “After your asthma attack”
leaflet!
9a!Provide smoking cessation advice
where appropriate!
MEDICATE!
10a!Supply with steroids!
- Prednisolone 40-50mg (5 days)!
On discharge!
11a!
Ensure has inhaled corticosteroid
(preventer inhaler) & β2 agonist
(reliever inhaler)!
FOLLOW-UP!
12a!Advise to see GP / Practice Nurse
within 2 working days !On discharge!
13a!Practice informed of A&E
attendance!Within 24hrs!
3.! ADULT ASTHMA CARE BUNDLE – PATIENTS ADMITTED TO HOSPITAL!
Element ! Order! Action!Timing from
admission!
Time completed
& signed!
EDUCATE!
6b! Check inhaler technique!
Pre-discharge!
7b!Provide smoking cessation advice
where appropriate!
8b!Referral to Respiratory Nurse for in-
patient Asthma Review!
MEDICATE!
9b!Prednisolone (40-50mg) continued
for at least 5 days!
On discharge!
10b!
Ensure has inhaled corticosteroid
(preventer inhaler) & β2 agonist
(reliever inhaler)!
FOLLOW-UP!
11b!Advised to see GP / Practice Nurse
within 2 working days ! On discharge!
12b!Follow-up in 4 weeks by respiratory
nurse or respiratory physician!
Mid Yorkshire Hospitals ADULT ASTHMA CARE BUNDLE!
This care bundle is designed to assist in the implementation of key steps and
targets in the management of patients in the Emergency Department (ED) with
acute exacerbations of asthma, it should be continued if they are admitted to
hospital. !
1. Please attach and complete STICKER 1. into the ED notes for ALL patients
attending with an exacerbation of asthma.!
2. Please attach and complete STICKER 2. into the ED notes if the patient is
being discharged home from the ED department.!
3. If a patient is admitted from ED with an exacerbation of asthma STICKER 3.
should be put into the medical notes and completed (by the medical team).!
* BTS guidelines (2011) on the management of acute asthma are attached to the
back of this form.!

© PCC 2012 51
Following up acute episodes
50 © PCC 2012
What is recommended in clinical guidelines
l The GP practice should be informed within 24 hours of a patient’s discharge from the emergency department or hospital following asthma exacerbation. Ideally this should be directly with a named individual responsible for asthma care within the practice by fax or email l There should be a GP follow-up within two working days – and ideally arranged before discharge, and a follow-up appointment in the respiratory clinic within four weeks
l A respiratory specialist should follow up patients admitted with severe asthma for at least one year after the admission
l A careful history should elicit the reasons for the exacerbation and explore possible actions the patient could take to prevent future emergency attendances. Inhaler technique should be checked and corrected and the importance of adherence to prescribed medication discussed. Medication should be optimised and the patient provided with an asthma action plan aimed at recognising their asthma is worsening, preventing relapse, optimising treatment and preventing delay in seeking assistance in the future.
What the evidence tells us
l Follow-up after an acute admission, which is important to prevent future re-admissions is a significant area of weakness in asthma management
l The BTS adult asthma audit 2011 showed that while 68.6% people had a further hospital review within the recommended four weeks following discharge, only 37.2 % were advised to attend their GP surgery within the following week and only 41% of people had their action plan reviewed or were provided with an asthma action plan 106 l Less than 50% of patients had documented evidence of inhaler technique review
l Only 41% had an asthma action plan on discharge – which would help them to recognise any deterioration in control in future and take appropriate action
l Some repeat attenders need emergency care, but many delay seeking help and are under-treated and/or under-monitored 107.
Following up acute episodes21What does this mean for commissioners and service developers?
l Commissioners should require secondary care providers to demonstrate that they are following the guidelines for education before discharge and for following up these patients after an exacerbation, as they represent a high risk group of patients. Follow up should be specifically commissioned
l Commissioners should ensure there are systems in place between secondary care providers, GPs, practice nurses and pharmacists to communicate effectively and promptly about a patient’s attendance or admission, so that appropriate follow- up can take place in the practice. Secondary care needs to be aware of and have confidence in the services available in the community
l Practice systems should enable patients who have had an exacerbation to access a nurse or GP for a follow-up after a discharge as recommended
l Commissioners should consider setting up a CQUIN for acute asthma care to encourage adherence to best practice guidelines.
BTS adult asthma audit 2011
68.6%
Further hospital review within the recommended 4 weeks following discharge
37.2%
41%
Advised to attend their GP surgery within the following week
Action plan reviewed or were provided with an asthma action plan

© PCC 2012 53
Following up acute episodes
52 © PCC 2012
Examples of good practice
St Guy’s and St Thomas’ Teaching Hospitals NHS Foundation Trust implemented a proforma for managing adult asthma patients who attend at A&E to ensure equal and standard care. A comprehensive discharge checklist within the proforma must be completed by staff which involves demonstration of inhaler technique, giving an After Your Asthma Attack leaflet and a printed letter for the patient to take to their GP within 48 hours to book a follow-up appointment. The patient is also telephoned by the hospital asthma nurse specialist within 48 hours of discharge for a follow-up check
A checklist approach could be used after each episode of uncontrolled asthma. One example is shown on the right.

© PCC 2012 55
Annex A – A patient-centred asthma service checklist
54 © PCC 2012
A Annex A – A patient-centred asthma service checklist
An integrated care pathway for asthma that encompasses all healthcare settings, so the patient journey is supported by good communication between professionals who are aware of the role of other parties and all are working to best practice in the British asthma guidelines
o
Good understanding of the burden of asthma locally to provide a sound basis for a local asthma strategy to improve outcomes – prevalence rates, outcomes in primary and secondary care, deaths and so on oAll patients with suspected asthma have access to a professional appropriately trained in performing diagnostic level spirometry and the basis upon which the diagnosis of asthma was made is recorded in the clinical records oA lead health professional for asthma in each practice who co-ordinates services in accordance with the British asthma guideline and local care pathways oAt least one practice nurse in every practice is trained in managing asthma (ie holds a recognised certificate of competence eg an asthma diploma) oRoutine use of personalised asthma action plans for all people with asthma – developed by professionals in collaboration with patients, who are competent in the skills required to support patients in self management oRegular reviews of all with asthma, at least annually and definitely after any need for urgent healthcare in any part of the healthcare system o
Primary care practices are performing well against the asthma indicators in the Quality and Outcomes Framework oAudits of medication in primary care undertaken to ensure that medication is being optimised and in line with the British asthma guideline oA system for stratifying patients with asthma according to risk, so that appropriate interventions are available to those at higher risk of acute attacks and high cost care oHigh quality information sources (eg Asthma UK and BLF materials/websites) are made available to all people with asthma and their families at diagnosis and regular review to encourage understanding of asthma and support self care oSystematic approach to help patients with asthma to quit smoking in routine consultations and as part of treatment of an acute episode oA named lead for respiratory emergencies in emergency departments is responsible for ensuring that appropriate emergency care is given oAccess to a respiratory specialist and respiratory nurse specialists in place in each setting or hospital facility that cares for those with exacerbations of asthma o
Robust systems of communication and follow-up are in place for those with asthma who have received care in out-of-hours services, ambulances, hospitals, walk-in centres or other urgent health care settings oAdults with late onset of asthma have access to specialist services to investigate potential causes in the workplace and receive advice and support oSpecialist services for people with severe/brittle/difficult asthma are available and accessible to patients who need a comprehensive multidisciplinary approach to asthma care oMonitoring and audit arrangements to ensure all levels of care are available and delivered according to the British asthma guideline o
The following checklist can be used to help commissioners identify whether the patients in their area have the services they need, whether best practice guidelines are being followed, and whether different sectors of the NHS are working effectively together to deliver seamless care.

© PCC 2012 57
Annex B – Good asthma services checklist from Asthma UK
56 © PCC 2012
Annex B – Good asthma services checklist from Asthma UK B
Asthma UK, Summit House, 70 Wilson Street, London EC2A 2DB T 020 7786 4900 F 020 7256 6075
©2008 Asthma UK Registered charity number England 802364 and Scotland SCO39322 PP04
0050
8
Good Asthma Services Checklist
receives a quick and accurate diagnosis of asthma, through the most appropriate methods, with referral to a respiratory specialist if required.
has a Personal Asthma Action Plan, in an appropriate format, that they have discussed and agreed through a face-to-face consultation with their healthcare professional.
has access to appropriately trained healthcare professionals who follow the BritishGuideline on Management of Asthma and who work across organisational boundaries.
has access to effective emergency and out-of-hours services when experiencing an asthma attack or worsening of their condition with follow up appointments arranged prior to discharge.
has access to specialist healthcare professionals and services that meet individual needs, including specialist wards and centres.
has their condition managed in an appropriate manner, with particular recognition given if they are a young person moving into adulthood.
and their parent/carer has access to a range of local services including education, social care and housing that also meet their social, emotional and psychological needs.
and their parent/carer is empowered to be actively involved in the local planning, delivery, development and evaluation of services to meet the diverse needs of all people with asthma.
has access to easy-to-understand high quality asthma information in a format and language they can understand as part of an effective health inequalities strategy.
benefits from an integrated approach between local government and health services to tackle the wider social and economic factors of health inequalities with an emphasis on targeting ‘seldom heard’ groups.
✓
✓
✓
✓
✓
✓
✓
✓
✓
✓
To pledge your support for the Good Asthma Services Checklist contact Asthma UK’s Supporter & Information Team (08456 03 81 43; [email protected]).
Asthma UK calls on healthcare decision-makers to ensure that every child and adult with asthma:
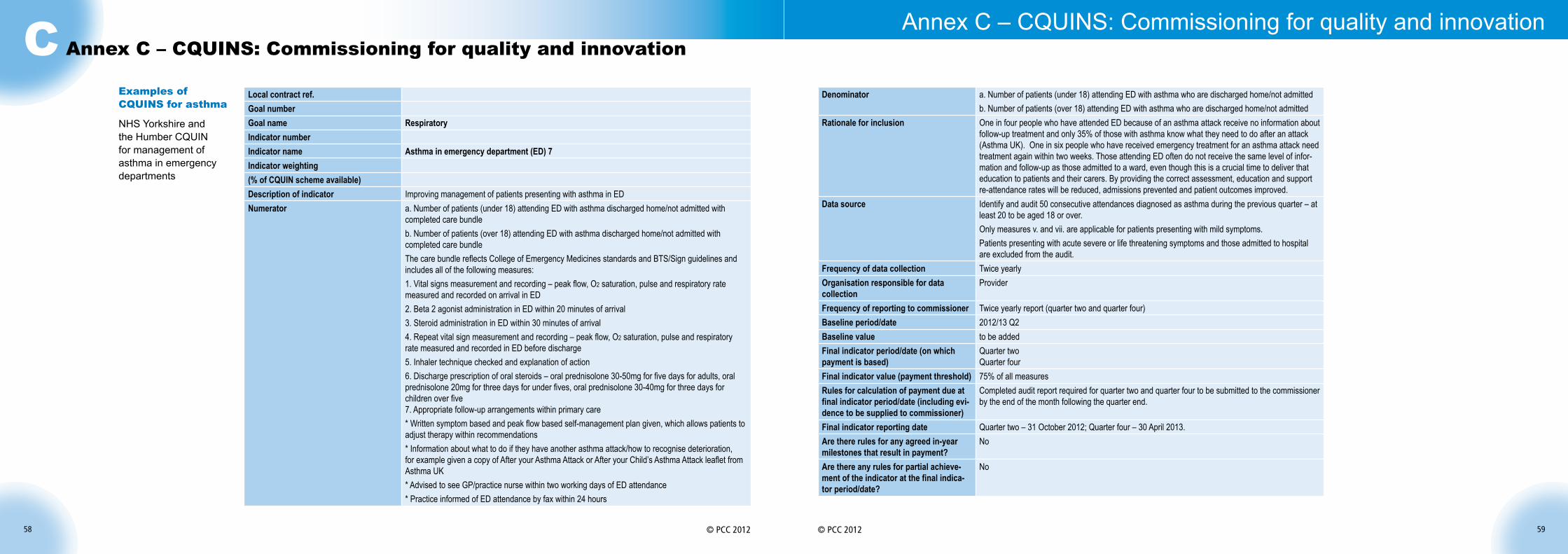
© PCC 2012 59
Annex C – CQUINS: Commissioning for quality and innovation
58 © PCC 2012
Annex C – CQUINS: Commissioning for quality and innovation
Examples of CQUINS for asthma
NHS Yorkshire and the Humber CQUIN for management of asthma in emergency departments
Local contract ref. Goal number Goal name RespiratoryIndicator number Indicator name Asthma in emergency department (ED) 7Indicator weighting (% of CQUIN scheme available) Description of indicator Improving management of patients presenting with asthma in EDNumerator a. Number of patients (under 18) attending ED with asthma discharged home/not admitted with
completed care bundleb. Number of patients (over 18) attending ED with asthma discharged home/not admitted with completed care bundleThe care bundle reflects College of Emergency Medicines standards and BTS/Sign guidelines and includes all of the following measures:1. Vital signs measurement and recording – peak flow, O2 saturation, pulse and respiratory rate measured and recorded on arrival in ED2. Beta 2 agonist administration in ED within 20 minutes of arrival3. Steroid administration in ED within 30 minutes of arrival4. Repeat vital sign measurement and recording – peak flow, O2 saturation, pulse and respiratory rate measured and recorded in ED before discharge5. Inhaler technique checked and explanation of action6. Discharge prescription of oral steroids – oral prednisolone 30-50mg for five days for adults, oral prednisolone 20mg for three days for under fives, oral prednisolone 30-40mg for three days for children over five7. Appropriate follow-up arrangements within primary care* Written symptom based and peak flow based self-management plan given, which allows patients to adjust therapy within recommendations * Information about what to do if they have another asthma attack/how to recognise deterioration, for example given a copy of After your Asthma Attack or After your Child’s Asthma Attack leaflet from Asthma UK* Advised to see GP/practice nurse within two working days of ED attendance* Practice informed of ED attendance by fax within 24 hours
Denominator a. Number of patients (under 18) attending ED with asthma who are discharged home/not admittedb. Number of patients (over 18) attending ED with asthma who are discharged home/not admitted
Rationale for inclusion One in four people who have attended ED because of an asthma attack receive no information about follow-up treatment and only 35% of those with asthma know what they need to do after an attack (Asthma UK). One in six people who have received emergency treatment for an asthma attack need treatment again within two weeks. Those attending ED often do not receive the same level of infor-mation and follow-up as those admitted to a ward, even though this is a crucial time to deliver that education to patients and their carers. By providing the correct assessment, education and support re-attendance rates will be reduced, admissions prevented and patient outcomes improved.
Data source Identify and audit 50 consecutive attendances diagnosed as asthma during the previous quarter – at least 20 to be aged 18 or over. Only measures v. and vii. are applicable for patients presenting with mild symptoms. Patients presenting with acute severe or life threatening symptoms and those admitted to hospital are excluded from the audit.
Frequency of data collection Twice yearlyOrganisation responsible for data collection
Provider
Frequency of reporting to commissioner Twice yearly report (quarter two and quarter four)Baseline period/date 2012/13 Q2Baseline value to be addedFinal indicator period/date (on which payment is based)
Quarter twoQuarter four
Final indicator value (payment threshold) 75% of all measuresRules for calculation of payment due at final indicator period/date (including evi-dence to be supplied to commissioner)
Completed audit report required for quarter two and quarter four to be submitted to the commissioner by the end of the month following the quarter end.
Final indicator reporting date Quarter two – 31 October 2012; Quarter four – 30 April 2013.Are there rules for any agreed in-year milestones that result in payment?
No
Are there any rules for partial achieve-ment of the indicator at the final indica-tor period/date?
No
C

© PCC 2012 61
Annex D – The Quality and Outcomes Framework
60 © PCC 2012
Information on exception reporting and true population coverage
Under the QOF scheme, GPs are rewarded for achieving an agreed level of population coverage for each indicator. In calculating coverage, practices are allowed to except appropriate patients from the target population such that they are not penalised for factors beyond their control, eg when patients do not attend for review despite repeated invitations, or if a medication cannot be prescribed due to a contra-indication or side-effect. It is this exception-adjusted population coverage that is reported annually.
However, patients not seen for review are at high risk of not receiving appropriate active chronic disease management and therefore of experiencing worse outcomes than patients who do receive a review.
Magnitude of variation
For PCTs in England, the percentage of patients with asthma who have had an asthma review in the preceding 15 months based on 2010/11 data:
l For exception-adjusted reporting, it ranged from 75.2% to 86.6% (1.2-fold variation); when the five PCTs with the highest percentages and the five PCTs with the lowest percentages are excluded, the range is 76.1-82.4%, and the variation is 1.1-fold;
l For actual coverage, it ranged from 75.1% to 86.5% (1.2-fold variation); when the five PCTs with the highest percentages and the five PCTs with the lowest percentages are excluded, the range is 76.0-82.2, and the variation is 1.1-fold.
Annex D – The Quality and Outcomes Framework
QOF indicators for asthma The QOF indicators for asthma in 2012/13 are:
QOF Management Guide, volume 3, © PCC April 2012
PCC |
89
AsthmaIndicator Points Payment stages
Records
ASTHMA1: The practice can produce a register of patients with asthma, excluding patients with asthma who have been prescribed no asthma-related drugs in the preceding 12 months
4
Initial management
ASTHMA8: The percentage of patients aged eight and over diagnosed as having asthma from 1 April 2006 with measures of variability or reversibility
15 45-80%
Ongoing management
ASTHMA10: The percentage of patients with asthma between the ages of 14 and 19 in whom there is a record of smoking status in the preceding 15 months
6 45-80%
ASTHMA9: The percentage of patients with asthma who have had an asthma review in the preceding 15 months that includes an assessment of asthma control using the 3 RCP questions
20 40-70%
Prevalence
Year Sum of register counts
Unadjusted prevalence
2010-2011 3,273,174 5.9%
2009-2010 3,254,562 5.9%
2008-2009 3,197,726 5.9%
2007-2008 3,105,212 5.7%
2006-2007 3,099,526 5.8%
2005-2006 3,101,275 5.8%
2004-2005 3,073,401 5.8%
Indicator detail
ASTHMA1: The practice can produce a register of patients with asthma, excluding patients with asthma who have been prescribed no asthma-related drugs in the previous twelve months
Key points to note
To be included on the asthma register patients need to fulfil both eligibility criteria ie they need to have a diagnosis of asthma and a record of a prescription for asthma-related drugs in the current QOF year.
As with all registers, assessors should discuss with practices their processes for ensuring that the register is complete and accurate. QOF Management Guide volume 2 describes the general principles of register development on p25.
Although there are legitimate reasons for exception-reporting, the degree of variation observed suggests that some practices are more effective than others at reaching the local asthma population and thereby influencing patient outcomes.Actual population coverage for systematic chronic disease management in people with asthma is considerably lower than the reported QOF achievement indicates. Patients not reached for chronic disease management are more likely to have worse outcomes than patients who receive chronic disease management. It is possible that many of the people not attending for regular review are among the more poorly controlled and high-risk patients. Novel and creative strategies may be needed to reach these patients to optimise their asthma control.
Local commissioners could assist GP practices to increase the local population coverage of their chronic disease management in asthma by considering the interventions in the box to the right.
For further information see the respiratory atlas of variation 2012. See http://www.rightcare.nhs.uk/index.php/nhs-atlas/
Increasing local population coverage of chronic disease management in asthma
l Calculate the actual chronic disease management coverage of registered asthma patients by including excepted patients in the denominator
l Benchmark and share local exception-reporting data
l Identify systems used by the best-performing practices to maximise patient reach
l Support local practices with high exception rates to implement best-practice systems and improve patient outcomes through systematic chronic disease management; this should help more practices to become effective at reaching the entire asthma population through a regular review.
D

© PCC 2012 63
Annex E – Examples of self-management plans
62 © PCC 2012
Annex E – Examples of self-management plans EAn action plan should contain three action points advising the person when to: n Increase their usual therapy - early adjustments to treatment by a confident patient can avoid or reduce the severity of an exacerbationn Start steroid tablets n Seek urgent medical attention.

© PCC 2012 65
Annex F – Pathway diagrams
64 © PCC 2012
Annex F – Pathway diagrams
The following diagrams have been included here as resources for use in documents. They can be enlarged and used as slides in presentations or in documents.
F
© PCC 2012 67
Annex G – Levers for change
66 © PCC 2012
Annex G – Levers for change GDriving changes in practice is essential if improvements in the quality of asthma care are to be achieved. There is a range of levers available in the NHS to drive improvements. Nationall The NHS Outcomes Framework and the Commissioning Outcomes Famework set a high level priority on specific outcomes at a national level. As already outlined in Chapter 4 ‘The policy context’, reducing deaths from respiratory disease is a key improvement area for the NHS and puts respiratory disease firmly on the national agenda.
l The Quality and Outcomes Framework (QOF) rewards GP practices for systematically providing high quality care for their patients. Asthma has featured in the QOF from the start of the new GMS contract in 2004, and the indicators have developed over time to become more outcomes focused and to reinforce guidelines-based good practice. This will continue to be an important tool for driving improvements in the quality of primary care.
l The quality standard for asthma will provide an important lever to drive up standards of care when it is available in February 2013. Also under discussion are the health premium and the quality premium, though details of how these will work are still in development.
Locall Quality accounts have been used since 2010 by NHS organisations to help providers identify and focus on the issues that will make the biggest difference to the quality of care they provide. They articulate to their commissioners, patients and the public which issues have been prioritised and how the organisation will address them. This is a key mechanism for reporting on how services for asthma are being improved.
l Commissioning for Quality and Innovation (CQUIN) – this payment framework enables commissioners to reward excellence by linking a proportion of acute providers’ income to the achievement of local quality improvement goals. This is therefore an excellent tool to drive specific quality improvement initiatives with providers. CQUINS are already being used to good effect in various ways for respiratory disease and examples are given within this document and in Annex C.
l Local enhanced service (LES) – This is a mechanism within the GMS contract to drive improvements in primary care services. Enhanced services plug a gap in essential services in primary care or deliver higher than specified standards. Enhanced services expand the range of services to meet local need, improve convenience and extend choice. A local enhanced service is one that is set up locally to meet specific health needs of relevance to the local population. This can be a useful lever to encourage improvements in the management of specific areas of care in primary care. Ultimately, gains made by local enhanced services or other resource allocation programmes need to be embedded into mainstream service payments to ensure that gains made are not subsequently lost following disinvestment.
Reviewing quality through audit
A regular programme of review and audit should be established to ensure that all relevant services – clinical and non-clinical – are providing the most appropriate service and support to people with asthma. The British asthma guideline contains a section on clinical audit, which may also be useful.
As a minimum, local areas should be clear about the extent to which services are delivering against requirements such as:n Number and proportion of practices with a named asthma lead GP n Number and proportion of practices with at least one nurse with additional accredited training in asthma caren Number and proportion of primary care and community nursing teams completing additional accredited training in asthma care each year n Number and proportion of adults on asthma registers with evidence of having been given a written personal asthma action plan n Number of urgent care units with a clinician trained in urgent asthma care n Number of people needing urgent care for asthma who see a respiratory specialistn Number of people leaving hospital after urgent care for whom proactive follow up in primary care has been arrangedn Number of deaths from asthma in adults.

© PCC 2012 69
Annex H – Partner organisations
68 © PCC 2012
Annex H – Partner organisationsHPartner organisations The Asthma Steering Group was formed in 2009 to support the respiratory team at the Department of Health for England in developing its asthma work. Chaired by Professor Martyn Partridge, this group comprises doctors, nurses and people with asthma who have been charged with shaping and contributing to the asthma work programme. They have contributed to a range of initiatives including the asthma chapter in the COPD and asthma outcomes strategy, developing the Quality and Outcomes Framework indicators for asthma, reviewing asthma information on NHS Choices and importantly, developing this good practice guide. Three organisations have representatives on this steering group and we would like to thank both the members of the group and these organisations for their commitment and support.
Asthma UKAsthma UK is the charity dedicated to improving the health and well-being of the 5.4 million people in the UK whose lives are affected by asthma. It aims to substantially reduce the number of asthma attacks that result every day in preventable hospital admissions and deaths. It also aims to encourage the development of new treatments that will give more people control over their asthma. Asthma UK pursues its goals by funding world-class medical research, providing practical and life-saving services and giving people with asthma a strong voice in public policy and local care delivery. Its resources for patients and health professionals have won prestigious medical awards and are independently accredited. These include a free adviceline service (0800 121 6244), a comprehensive website, self management plans, an active Facebook site and a range of targeted materials for both adults and children with asthma and their healthcare professionals.www.asthma.org.uk
British Thoracic SocietyThe BTS is a professional body and registered charity. Its members include doctors, nurses, respiratory physiotherapists, scientists and other professionals with an interest in respiratory disease. The society had 2,797 members at 1 July 2012. BTS’ main charitable objective is to improve the care of people with respiratory and associated disorders, which is achieved in various ways:l By promoting optimum standards of care and developing tools for quality improvement: treatment best practice guidelines; clinical audit tools; the development of the BTS lung disease registry and the forthcoming work on care bundlesl By promoting and advancing knowledge about the causes, prevention and treatment of respiratory diseases l By promoting and disseminating research (through the winter meeting as well as the journal Thorax).www.brit-thoracic.org.uk
The Primary Care Respiratory Society UK The Primary Care Respiratory Society UK (PCRS-UK) is a membership-led charity supporting primary care health professionals. Its mission is to give every member of the primary care practice team the confidence to deliver quality respiratory care, improve the quality of life for patients with respiratory disease, and help practices hit their Quality and Outcomes Framework (QOF). Through practice and individual membership schemes, PCRS-UK offers a wealth of practical resources for primary care health professionals, whether they are relatively new to respiratory medicine or a respiratory expert. l The PCRS-UK respiratory leaders programme also provides primary care health professionals with training workshops, policy updates and IMPRESS resources, to enable them to take the lead, motivate and inspire best practice within their locality. l The PCRS-UK quality award sets out the principles that best define high quality respiratory care in primary care and provides a developmental framework that can be used at practice, local and national level to promote, support and reward quality respiratory care in the primary care setting.www.pcrs-uk.org

© PCC 2012 71
Annex I – Asthma steering group
70 © PCC 2012
Professor Martyn Partridge – chair
Representing Role
Jan Gould Asthma UK Lay representative
Mary Fletcher Asthma UK Lay representative
Professor Mike Thomas Asthma UK Professor of primary care respiratory research
Professor Ian Pavord Asthma UK Chest physician
Vikki Knowles Asthma UK Community respiratory nurse
Dr Bernard Higgins British Thoracic Society Chest physician
Dr Duncan Keeley Primary Care Respiratory Society UK
GP
June Roberts Primary Care Respiratory Society UK
Respiratory nurse consultant
Dr Jon Couriel Respiratory paediatrician
Fiona Fowler Lay representative
Dr Robert Winter Department of Health Joint national clinical director, respiratory disease
Bronwen Thompson Department of Health Asthma programme lead
Annex I – Asthma steering groupI

© PCC 2012 73
References
72 © PCC 2012
References
1 Chung KF et al: Severe therapy resistant asthma – Eur Res Mon 2003, 23:3132 Hoskins et al: Risk factors and costs associated with an asthma attack – Thorax 2000;55:19-24 doi:10.1136/thorax.55.1.19 3 NHS Information centre Information centre. Prescriptions dispensed in the community – 2000-2010 July 2011 Table 8: http://www.ic.nhs.uk/webfiles/publications/007_Primary_Care/Prescribing/Prescriptions%20dispensed%20in%20the%20community%202000%20-%202010/Prescriptions_Dispensed_2000_2010.pdf Accessed 26.8.114 Scottish Intercollegiate Guidelines Network and British Thoracic Society: British guideline on the management of asthma – a clinical guideline – http://www.sign.ac.uk/pdf/sign101.pdf 5 The Asthma Divide: Inequalities in emergency care for people with asthma in England – Asthma UK 20076 Global initiative for asthma – http://www.ginasthma.org/pdf/GINABurdenReport.pdf7 Quality and Outcomes Framework prevalence data – asthma 2010-11: http://www.ic.nhs.uk/statistics-and-data-collections/supporting-information/audits-and-performance/the-quality-and-outcomes-framework/qof-2010-11/qof-2010-11-data-tables/qof-prevalence-data-tables-2010-118 Health Survey for England 2010: http://www.ic.nhs.uk/webfiles/publications/003_Health_Lifestyles/HSE2010_REPORT/HSE2010_Summary_of_key_findings.pdf9 OECD data on asthma: http://www.oecd-ilibrary.org/sites/health_glance-2011-en/05/01/01/index.html?contentType=/ns/Book,/ns/StatisticalPublication&itemId=/content/book/health_glance-2011-en&containerItemId=/content/serial/19991312&accessItemIds=&mimeType=text/html10 Dept of Health – the NHS Atlas of Variation in healthcare November 2011 http://www.rightcare.nhs.uk/index.php/atlas/atlas-of-variation-2011/11 Wiener-Ogilvie et al: Do practices comply with the key recommendations of the British asthma guidelines? If not, why not? Prim Care Resp J (2007) 16(6) 369-37712 Starren ES et al: A centralised respiratory diagnostic service for primary care: a four-year audit – Prim Care Resp J Volume 21 Issue 2 June 201213 Asthma UK, national asthma panel, 200914 Health Survey for England 2010: http://www.ic.nhs.uk/webfiles/publications/003_Health_Lifestyles/HSE2010_REPORT/HSE2010_Summary_of_key_findings.pdf
15 Gamble J: The prevalence of non-adherence in difficult asthma – American Journal of Respiratory and Critical Care Medicine Vol 180. pp. 817-822, (2009)16 Partridge MR et al. Understanding patients with asthma and COPD: insights from a European study – Prim Care Respir J 2011; 20(3): 315-323 doi: 10.4104/pcrj.2011.00056 17 Asthma UK, national asthma panel, 200918 Where do we stand? – Asthma in the UK today http://www.asthma.org.uk/how-we-help/teachers-and-healthcare-professionals/health-professionals/reports/19 WHO detailed mortality database for Europe20 Partridge M 1991: Self care plans for people with asthma. The Practitioner p 715–2121 ONS data England and Wales 201022 Partridge MR et al. Understanding patients with asthma and COPD: insights from a European study Prim Care Respir J 2011; 20(x): xx-xx doi: 10.4104/pcrj.2011.00056 23 NHS outcomes framework 2012 /13: http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_13170024 NHS commissioning outcomes framework 2012/13 http://www.nice.org.uk/aboutnice/cof/cof.jsp25 An Outcomes Framework for COPD and asthma in England: http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_12797426 Atlas of Variation 2011: http://www.rightcare.nhs.uk/index.php/atlas/atlas-of-variation-2011/. Respiratory atlas of variation due for publication Autumn 201227 The national review of asthma deaths: http://www.rcplondon.ac.uk/projects/national-review-asthma-deaths28 Atlas of Variation 2011: http://www.rightcare.nhs.uk/index.php/atlas/atlas-of-variation-2011/. Respiratory atlas of variation due for publication Autumn 201229 Impress guide to information 2010: http://www.impressresp.com/index.php?option=com_docman&Itemid=8230 http://www.inhale.nhs.uk/31 Scottish Intercollegiate Guidelines Network and British Thoracic Society: British guideline on the management of asthma – a clinical guideline: http://www.sign.ac.uk/pdf/sign101.pdf
32 Pearson MB Ed: Measuring clinical outcomes in asthma: a patient centred approach: London: Royal College of Physicians 199933 Juniper EF et al: Development and validation of a questionnaire to measure asthma control. Eur Respir J 1999:14(4);902-734 Nathan RA et al: Development of the asthma control test: a survey for assessing asthma control J Allergy Clin Immunol. 2004;113(1):59-6535 Partridge MR et al. Understanding patients with asthma and COPD: insights from a European study Prim Care Respir J 2011; 20(x): xx-xx doi: 10.4104/pcrj.2011.00056:36 Wilson, S et al: Shared treatment decision making improves adherence and control in poorly controlled asthma: American Journal of Respiratory and Critical Care Medicine Vol 181. pp. 566-577, (2010)37 DH report on Events for people with COPD and Asthma – 200938 RCGP Care planning: Improving the lives of people with long term conditions 201139 King’s Fund, Asthma UK et al: How to deliver high quality, patient-centred, cost-effective care, consensus solutions from the voluntary sector, 2010 40 Global strategy for asthma management and prevention, global Initiative for asthma (GINA) 2010. Available from: http://www.ginasthma.org/.p5741 Starren ES et al: A centralised respiratory diagnostic service for primary care: a four-year audit: Prim Care Resp J Volume 21 Issue 2 June 201242 Ibid43 Ibid44 Partridge MR et al: Understanding patients with asthma and COPD: insights from a European study: Prim Care Respir J 2011; 20(3): 315-32345 Ibid46 Paasche-Orlow M et al: Tailored Education may reduce health literacy disparities in asthma self management: American Journal of Respiratory and Critical Care Medicine Vol 172. pp. 980-986, (2005)47 Lahdensuo A: Guided self-management of asthma – how to do it: BMJ 319 : 759 (Published 18 September 1999)48 Gibson PG, Limited (information only): patient education programs for adults with asthma. Cochrane Database Syst Rev. 2002;(2):CD001005.49 Paasche-Orlow M et al: Tailored Education may reduce health literacy disparities in asthma self management: American Journal of Respiratory and Critical Care Medicine Vol 172. pp. 980-986, (2005)50 DH Public attitudes to self-care - baseline survey 2005: http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/documents/digitalasset/dh_4111264.pdf
51 Partridge MR: Self-management in adults with asthma. Patient Educ Counseling 1997; 32: 1–4.52 Lahdensuo A: Randomised comparison of guided self management and traditional treatment of asthma over one year: BMJ 312 : 748 (Published 23 March 1996)53 Cochrane review 199954 Wiener-Ogilvie et al: Do practices comply with the key recommendations of the British asthma guidelines? If not, why not? Prim Care Resp J (2007) 16(6) 369-37755 Haughney J: The living & breathing study: a study of patients’ views of asthma and its treatment: Primary Care Respiratory Journal Volume 13, Issue 1, March 2004, Pages 28-3556 Wiener-Ogilvie et al: Do practices comply with the key recommendations of the British asthma guidelines? If not, why not? Prim Care Resp J (2007) 16(6) 369-37757 Partridge M et al: Can lay people deliver asthma self-management education as effectively as primary care based practice nurses? Thorax 2008;63:778-783 doi:10.1136/thx.2007.08425158 Cochrane reviews 1999 - 200359 Charlton I: Audit of the effect of a nurse-run asthma clinic on workload and patient morbidity in a general practice: Br J Gen Pract 1991 June: 41 (347):227-231 60 Ibid61 Pinnock et al: Setting the standard for routine asthma consultations: a discussion of the aims, process and outcomes of reviewing people with asthma in primary care: Primary Care Respiratory Journal (2010); 19(1): 75-8362 Pinnock H: Accessibility, acceptability, and effectiveness in primary care of routine telephone review of asthma: pragmatic, randomised controlled trial: BMJ 326 : 477 doi: 10.1136/bmj.326.7387.477 (Published 1 March 2003)63 Pinnock et al: Knowledge of asthma guidelines: results of a UK General Practice airways group (GPIAG) web-based Test your Knowledge quiz: Primary Care Respiratory Journal (2010); 19(2): 180-184. 64 Suissa S et al: Low-dose inhaled corticosteroids and the prevention of death from asthma: N Engl J Med 2000; 343:332-33665 Gamble J: The prevalence of non-adherence in difficult asthma: American Journal of Respiratory and Critical Care Medicine Vol 180. pp. 817-822, (2009)

© PCC 2012 75
References
74 © PCC 2012
66 Partridge MR et al. Understanding patients with asthma and COPD: insights from a European study: Prim Care Respir J 2011; 20(3): 315-32367 Sweeney J et al: Inappropriate prescribing of combination inhalers in asthma in Northern Ireland (NI) Abstract BTS winter meeting 201168 Global initiative for asthma – Global strategy for asthma management and prevention 2010 p5969 British Thoracic Society: Adult acute asthma audit report 2011: http://www.brit-thoracic.org.uk/Portals/0/Audit%20Tools/Adult%20Asthma%20Summary%20Report%202011.pdf70 British Heart Foundation: http://www.bhf.org.uk/research/statistics/risk-factors/smoking.aspx71 Rabe JF: Worldwide severity and control of asthma in children and adults: the global asthma insights and reality surveys. J Allergy Clin Immunol. 2004 Jul;114(1):40-7.72 Partridge MR et al. Understanding patients with asthma and COPD: insights from a European study Prim Care Respir J 2011; 20(3): 315-32373 Purdy S et al: Emergency respiratory admissions: influence of practice, population and hospital factors: J Health Ser Res Policy Vol 16 No 3 July 201174 Hoskins G et al: Risk factors and costs associated with an asthma attack: Thorax 2000; 55: 19-2475 Department of Health – Long term conditions compendium of information 2012: http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/documents/digitalasset/dh_134486.pdf76 Hoskins G et al: Risk factors and costs associated with an asthma attack: Thorax 2000; 55: 19-2477 British asthma guidelines 200878 Chung et al: Severe therapy resistant asthma: Eur Res Mon 2003 , 23:31379 Heaney, Horne: Non-adherence in difficult asthma: time to take it seriously: Thorax 2012;67:268-270 doi:10.1136/thoraxjnl-2011-20025780 Gamble et al: Non-adherence in difficult asthma: Am. J. Respir. Crit. Care Med.November 1, 2009 vol. 180 no. 9 817-82281 AsthmaUK – Fighting for breath: http://www.asthma.org.uk/how_we_help/publishing_reports/fighting_for_breath.html82 David Fishwick,et al: Guidelines update: Standards of care for occupational asthma: an update: Thorax 2012;67:3 278-28083 http://www.hsl.gov.uk/centres-of-excellence/centre-for-workplace-health/gords.aspx 84 British Occupational Health Research Foundation. March 201085 Standard of care (based on BOHRF) Thorax 2012.86 British asthma guidelines 2011
87 British Occupational Health Research Foundation. Occupational asthma. A guide for General Practitioners and practice nurses. March 2010. Available at www.bohrf.org.uk88 British asthma guidelines 201189 Thomas M et al: Asthma and psychological dysfunction: Prim Care Respir J 2011; 20(3): 250-25690 ibid91 ibid92 Demoly P et al. Update on asthma control in five European countries: results of a 2008 survey: Eur Resp Rev 2010;19:1–8.93 Rabe KF et al: Clinical management of asthma in 1999: the asthma insights and reality in Europe (AIRE) study. Eur Respir J 2000;16:802–807.94 Dept Health – the NHS Atlas of Variation in healthcare November 2011: http://www.rightcare.nhs.uk/index.php/atlas/atlas-of-variation-2011/95 The Asthma Divide: Inequalities in emergency care for people with asthma in England, Asthma: UK 200796 Barnes et al: The costs of asthma: Eur Respir J, 1996, 9, 636–64297 Partridge M: A national census of those attending UK accident and emergency departments with asthma: JAccid Emerg Med 1997;14:16-2098 Salmeron S: Asthma severity and adequacy of management in accident and emergency departments in France: a prospective study. Lancet. 2001 Aug 25;358(9282):629-35.99 British Thoracic Society: Adult acute asthma audit report 2011: http://www.brit-thoracic.org.uk/Portals/0/Audit%20Tools/Adult%20Asthma%20Summary%20Report%202011.pdf100 Turner MO: Risk factors for near-fatal asthma. A case-control study in hospitalized patients with asthma. Am J Respir Crit Care Med. 1998 Jun;157(6 Pt 1):1804-9.101 British Thoracic Society: Adult acute asthma audit report 2011: http://www.brit-thoracic.org.uk/Portals/0/Audit%20Tools/Adult%20Asthma%20Summary%20Report%202011.pdf102 ibid103 Lahdensuo A: Randomised comparison of guided self management and traditional treatment of asthma over one year: BMJ 312 : 748 (Published 23 March 1996)104 Gibson et al: Self-management education and regular practitioner review for adults with asthma: Cochrane review 2009105 Bateman E: Overall asthma control: The relationship between current control and future risk: The Journal of Allergy and Clinical Immunology Volume 125, Issue 3 , Pages 600-608.e6, March 2010
106 British Thoracic Society: Adult acute asthma audit report 2011: http://www.brit-thoracic.org.uk/Portals/0/Audit%20Tools/Adult%20Asthma%20Summary%20Report%202011.pdf107 Emerman et al: Prospective multicentre study of relapse following treatment for acute asthma among adults

© PCC 2012