Dental emergencies
54
Emergency Management in Dental Office By Dr. Ishfaq Ahmad
-
Upload
ishfaq-ahmad -
Category
Health & Medicine
-
view
115 -
download
0
Transcript of Dental emergencies

Emergency Management in
Dental OfficeBy Dr. Ishfaq Ahmad
Introduction Any dental emergency like an injury to the teeth or gums can be potentially
serious and should not be ignored. Ignoring a dental problem can increase the risk of permanent damage as well as the need for more extensive and expensive treatment later on.
What is Dental Emergency
An acute disorder of oral health that requires dental and/or medical attention, including broken, loose, or avulsed teeth caused by traumas,infections and inflammations of thesoft tissues of the mouth; and complications of oral surgery, such as dry tooth socket.

Anxiety recognition & stress reduction protocol
Recognize patient’s anxiety level.
Consider using pre-medication or sedation
Schedule morning appointments.
Minimize waiting time and watch appointment length.
Make sure to use adequate pain control. This will vary from patient to patient.
Monitor vital signs.
Medical consult if required.

When & Where To Refer
According to the General Dental Council’s ‘Standards for Dental Professionals’,2009, registered dentists are expected to:Work within your knowledge, professional competence and physical abilities. Refer patients for a second opinion and for further advice when it isnecessary, or if the patient asks. Refer patients for further treatment whenit is necessary to do so.As such, the need for referral may be that the situation lies outside: the knowledge the skill the experience the facilities available to the referring dentist.
Careful consideration should be made with regard to where, and whom torefer a patient.


How Can An Emergency Arise
Dental Emergencies
Medical Emergencies

Protocol for Management of Dental Emergencies
Prompt Diagnosis
Reassurance
Pain relief
Medication
Referral for definitive treatment

Dental Emergencies
Acute Oral Medical and Surgical Conditions
Restorative Dental Emergencies
Acute Presentations of Chronic Oro-Facial Pain Conditions
Traumatic Injuries to the Teeth and Oral Soft Tissues
Pain Relief in the Dental Emergency Clinic
Management of the Special Needs Patient

Acute Oral Medical and Surgical Conditions
Blistering disorders of the oral mucosa
Oral ulceration
Disturbed oro-facial sensory or motor function
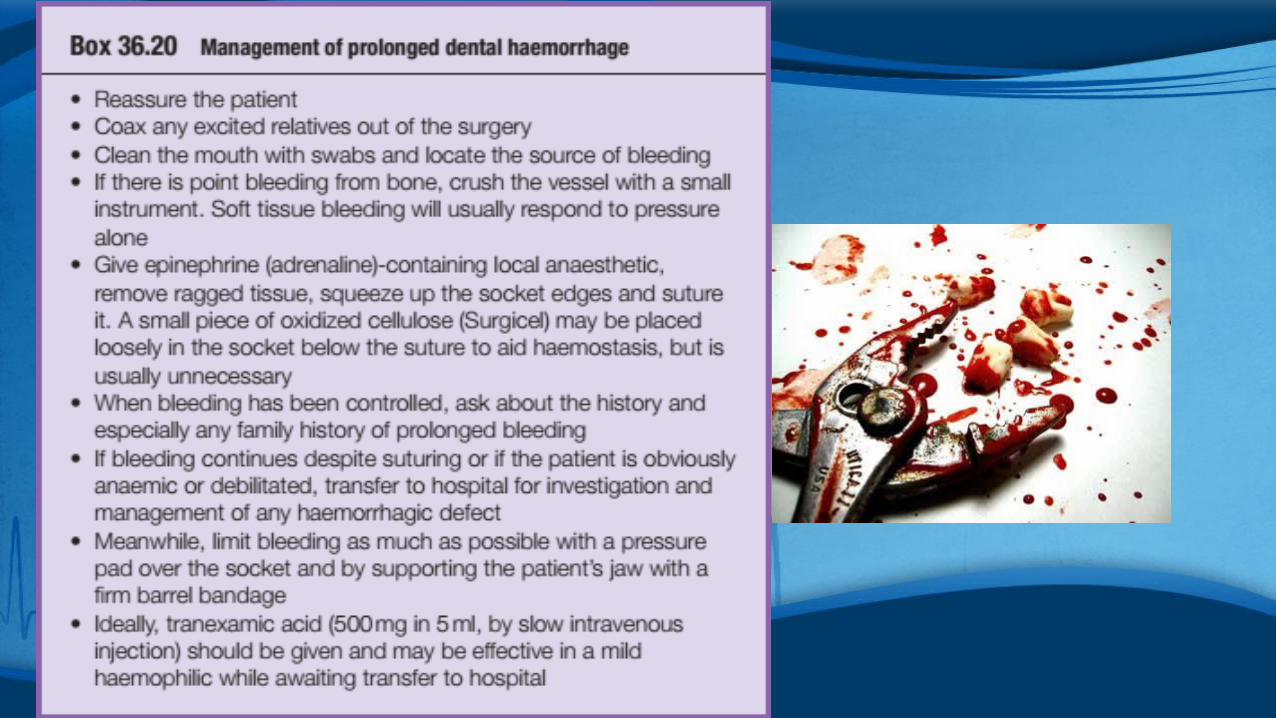
Hemorrhage
Other acute conditions
Bony pathology
Fracture
Restorative Dental Emergencies
Pain management
Infections and soft tissue problems
Crack, fracture and mobility of teeth and dental restorations
Fractured and loose implants
Fractures and swallowing of removable prostheses
Traumatic Injuries to the Teeth and Oral Soft Tissues
Assessment of the traumatized patient
Management of traumatic dental injuries
Injuries to the hard dental tissues, the pulp and the alveolar process
Injuries to the periodontal tissues
Dento-alveolar fractures
Acute Presentations of Chronic Oro-Facial Pain Conditions
Oro-facial pain history
Examination of patients with oro-facial pain
Special investigations for oro-facial pain
Presentation, investigations and initial management of acute non-odontogenic oro-facial pain
Management of the Special Needs Patient
Assessment
Diagnosis
Symptomatic relief
Counselling
Referral
Medical Emergencies in the Dental Clinic
The commonest medical emergencies seen in the dental emergency clinic arefaints. Hypoglycemia, asthma, anaphylaxis, angina and seizures may also beseen but are less common. All members of the dental team need to be awareof what their role would be in the event of a medical emergency and shouldbe trained appropriately with regular practice sessions.

Medical Emergencies in the Dental Clinic
Vasovagal syncope (faint)
Hyperventilation/‘panic attack’
Acute asthma attack
Angina/myocardial infarction
Epileptic seizures
Diabetic emergencies
Allergies/hypersensitivity reactions
Choking and aspiration
Adrenal insufficiency
Stroke
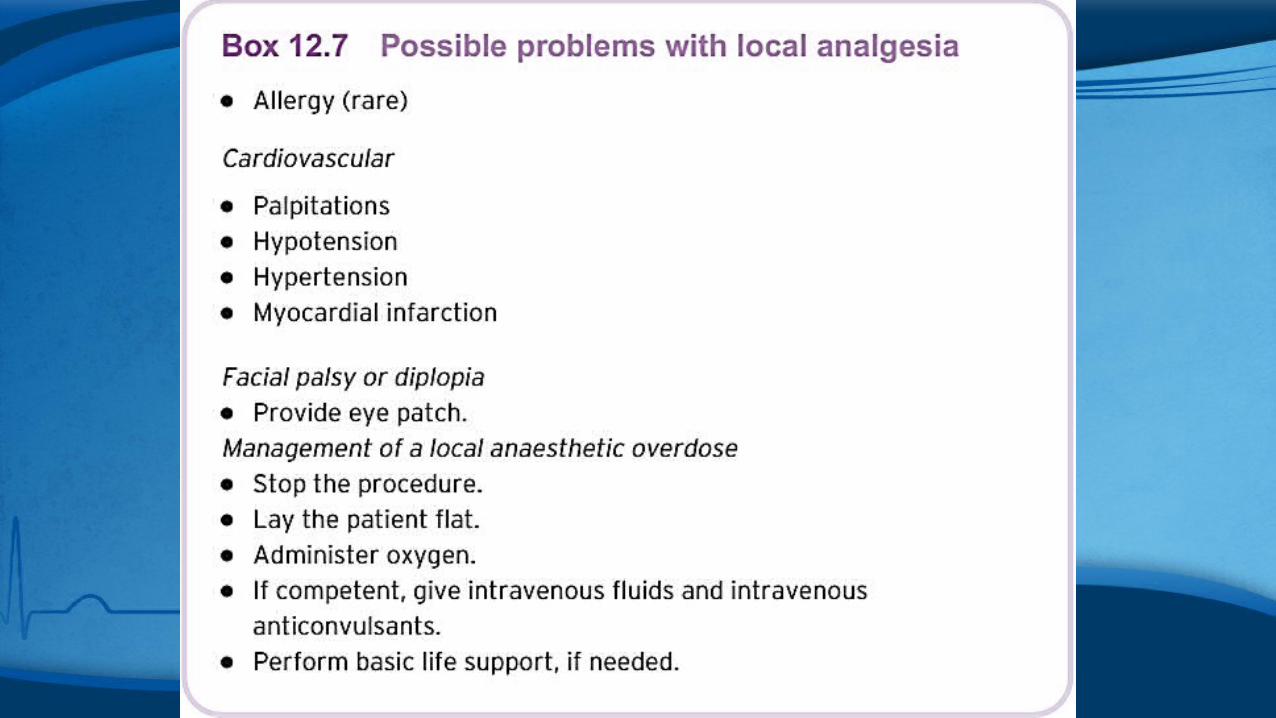
Local anesthetic emergencies
Problems with hemostasis

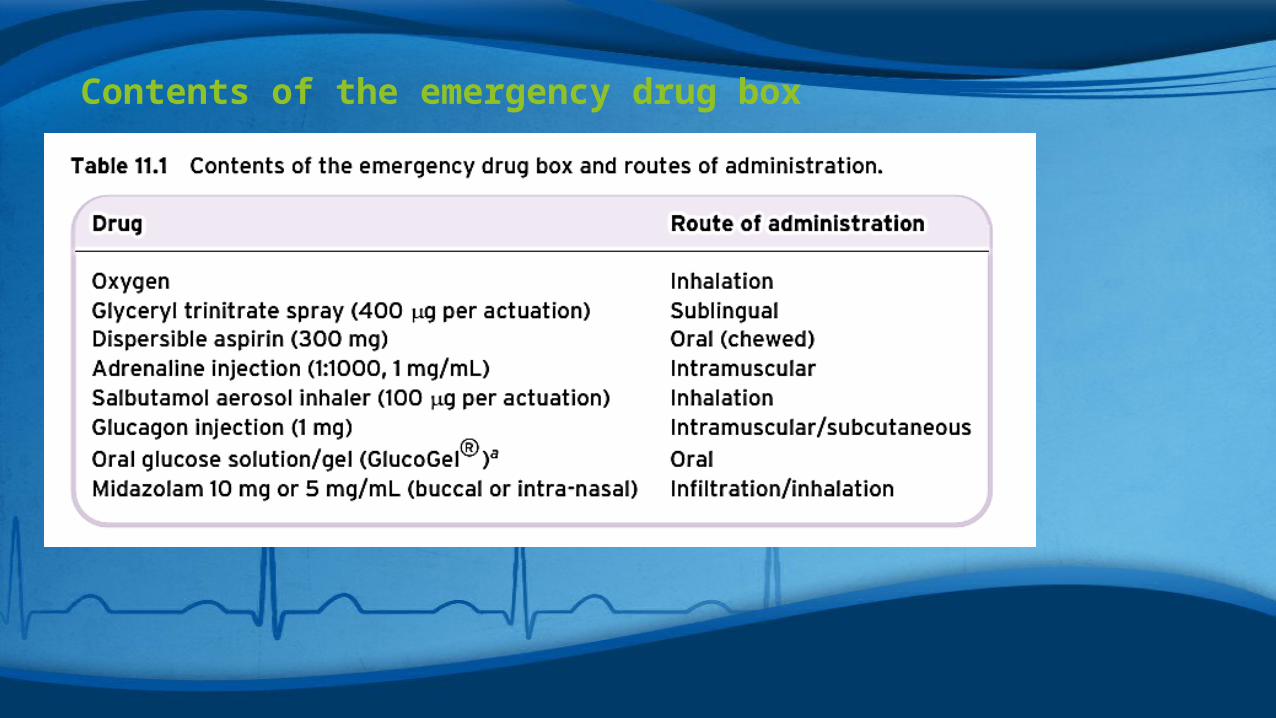
Contents of the emergency drug box


The ‘ABCDE’ approach to an emergency patient
Medical emergencies can often be prevented by early recognition. An abnormal patient color, pulse rate or breathing can signal some impendingemergencies.

Basic life support (BLS)
Advanced Cardiovascular Life Support (ACLS)
Vasovagal syncope (simple faint)
Fainting – signs and symptoms Patient feels faint/light headed/dizzy Pallor, sweating Pulse rate slows Low blood pressure Nausea and/or vomiting Loss of consciousness
Fainting – treatment Lay the patient flat and raise the legs – recovery will normally be rapid. A patent airway must be maintained. If recovery is delayed, oxygen should be administered and other causes ofloss of consciousness be considered.

Hyperventilation
Hyperventilation – signs and symptoms Anxiety Light headedness Dizziness Weakness Paresthesia Tetany Chest pain and/or palpitations Breathlessness
A demonstration of carpal spasm.

Hyperventilation
Hyperventilation – treatmentA calm and sympathetic approach from the practitioner is important. Thediagnosis, particularly in the early stages, is not always as obvious as it mayseem: Exclude other causes for the symptoms. Encourage the patient to rebreathe their own exhaled air to increase theamount of inhaled carbon dioxide – a paper bag placed over nose and mouthallows this. If no paper bag is handy, the patient’s cupped hands would be a (less satisfactory) alternative.

Asthma
Asthma is a potentially life-threatening condition and should always be takenseriously. An attack may be precipitated by exertion, anxiety, infection orexposure to an allergen.
Asthma – signs and symptoms Breathlessness (rapid respiration – more than 25 breaths per minute) Expiratory wheezing Use of accessory muscles of respiration TachycardiaSigns and symptoms of life-threatening asthma Cyanosis or slow respiratory rate (less than 8 breaths per minute) Bradycardia Decreased level of consciousness/confusion

Asthma
Asthma – treatment
Most attacks will respond to the patient’s own inhaler, usually salbutamol(may need to repeat after 2–3 minutes).
If no rapid response, or features of severe asthma, call an ambulance. A medical assessment should be arranged for patients who require additional doses of bronchodilator to end an attack.
A spacer device may need to be used if patient has difficulty using theinhaler.
If the patient is distressed or shows any of the signs of life-threateningasthma, urgent transport to hospital should be arranged.

Cardiac chest pain
Have a previous history of cardiac disease
The pain of myocardial infarction (MI) will often be similar to that of angina but more severe and, unlike angina, will not be relieved by GTN.
Dental treatment may be best left until another day if there is an attack.
Chest pain that improves on stopping exertion is more likely to be cardiac in origin than onethat is not related.

Chest pain – possible causes

Myocardial infarction
Myocardial infarction – signs and symptoms Severe, crushing chest pain, which may radiate to the shoulders and downthe arms (particularly the left arm) and into the mandible. Shortness of breath. The skin becomes pale and clammy. Pulse becomes weak and patient may become hypotensive. Often, there will be nausea and vomiting.

Myocardial infarction
Myocardial infarction – treatment The practitioner should remain calm and be a reassuring presence. Call emergency number. Most patients will be best managed in the sitting position. Patients who feel faint should be laid flat. Give high-flow oxygen (15 L/min). Give sublingual GTN spray. Give 300 mg aspirin orally to be chewed (if no allergy) – ensure that whenhanding over to the receiving ambulance crew that they are made aware ofthis as thrombolytic therapy is given by some ambulance crews. A patient who has had surgical dental treatment should be highlighted tothe ambulance crew as any significant risk of haemorrhage may affect thedecision to use thrombolytic therapy If the patient becomes unresponsive, the practitioner should check for ‘signsof life’ (breathing and circulation) and start cardiac pulmonary ressusication.

Epileptic seizures
Epilepsy – signs and symptoms The patient may have an ‘aura’ or premonition that a seizure is about tooccur. Tonic phase – loss of consciousness, patient becomes rigid and falls andbecomes cyanosed. Clonic phase – jerking movements of the limbs, tongue may be bitten. Urinary incontinence, frothing at the mouth. The seizure often gradually abates after a few minutes but the patient mayremain unconscious and may remain confused after consciousness has beenregained Hypoglycaemia may present as a fit and should be considered (including inepileptic patients). Therefore, blood glucose measurement at an early stageis wise.

Epileptic seizures
Epilepsy – treatment of a fit
As far as possible, ensure safety of the patient and practitioner (do notattempt to restrain). Midazolam given via the buccal or intra-nasal route (10 mg for adults). Thebuccal preparation is marketed as ‘Epistatus’ (10 mg/mL)
For children:❜ Child 1–5 years-5 mg❜ Child 5–10 years-7.5 mg❜ Child more than 10 years-10 mg The parents of some children with poorly controlled epilepsy will carryrectal diazepam.
In the absence of rapid response to treatment, call an ambulance.

Hypoglycaemia
Hypoglycaemia – signs and symptoms Trembling Hunger Headache Sweating Slurring of speech ‘Pins and needles’ in lips and tongue Aggression and/or confusion Seizures Unconsciousness

Hypoglycaemia – treatment Lie the patient flat (remember A, B, C). If the patient is conscious, give oral glucose (three lumps of sugar or2–4 teaspoons of sugar) or Gluco Gel R (Figure 12.3). If the patient is unconscious, give 1 mg glucagon intramuscularly (orsubcutaneously). Get medical help.

Allergies/hypersensitivity reactions
Anaphylaxis – signs and symptoms Itchy rash/erythema. Facial flushing or pallor. Upper airway (laryngeal) oedema and bronchospasm leading to stridor,wheezing and possibly hoarseness. A respiratory arrest may occur leading to cardiac arrest. Vasodilatation leading to low blood pressure and collapse, which mayprogress to cardiac arrest.Anaphylaxis – initial treatment The ABCDE approach should be employed while the diagnosis is being made. Manage airway and breathing by administering high-flow oxygen. Restore blood pressure by lying the patient flat and raising the legs.
In life-threatening anaphylaxis (hoarseness, stridor, cyanosis, dyspnoea,drowsiness, confusion or coma), adrenaline should be administered: Administer 0.5 mL of 1 in 1000 adrenaline IM and repeat and 5-minuteintervals if no improvement. The optimum site for injection is the anterolateral mid-third of the thigh.



SUMMARY & CONCLUSION
ALWAYS BE PREPARED
Prompt recognition and efficient management of medical emergencies by a well-prepared dental team can increase the likelihood of a safe & satisfactory outcome.
Basic life support training- A MUST
As always, prevention is better than cure.