Delayed Surgical Retrieval of Retained Guidewire Following Percutaneous Coronary Intervention
32
c 2010 Wiley Periodicals, Inc. 37 CASE REPORTS Successful Management of a Posterior Saccular Coronary Artery Aneurysm at the Left Main Coronary Artery Bifurcation Rajesh Ramankutty, M.D., Turki B. Albacker, M.D., Karl G. Reyes, M.D., and Jose L. Navia, M.D. Department of Thoracic and Cardiovascular Surgery, Cleveland Clinic Foundation, Cleveland, Ohio ABSTRACT Left main coronary artery aneurysm is a rare condition that presents as a potential surgical challenge due to its location. We present a case of successful repair of a posterior saccular aneurysm of the left main coronary artery by aneurysm ex- clusion, afferent and efferent ligation with coro- nary artery bypass grafting. doi: 10.1111/j.1540- 8191.2010.01030.x (J Card Surg 2011;26:37-39) Aneurysm of the left main coronary artery (LMCA) is an extremely rare condition. Compared to aneurysms of the right main coronary artery, surgical management of LMCA aneurysms is more challenging because of its location behind the main pulmonary artery. We present a case of successful management of a large posterior saccular aneurysm involving the LMCA bifurcation. CASE REPORT A 46-year-old woman presented with an incidental finding of 9 × 7 × 7.5 mm aneurysm at the level of the LMCA bifurcation. The patient was initially asymp- tomatic and the aneurysm was detected incidentally by chest computed tomography scan when she volun- teered as the first patient for the new scanner installed at the facility where she worked as a radiology tech- nician. Since she was asymptomatic, she was initially managed conservatively with antiplatelets and serial follow-ups. Two years later, she developed new atypi- cal chest pain and exertional dyspnea, New York Heart Association class II-III, with no medical comorbidities. Physical exam, chest x-ray (CXR), and electrocardio- gram were unremarkable. Transthoracic echocardiog- Address for correspondence: Turki B. Albacker, M.D., Department of Thoracic and Cardiovascular Surgery, 9500 Euclid Avenue/J4- 133E, Cleveland, OH 44195. Fax: 1(216) 636-1286; e-mail: dr_turki@ yahoo.com raphy demonstrated good biventricular function, nor- mal valves, and was negative for stress-induced is- chemia. Computed tomography of the chest showed a marginally increased aneurysm size to 11 × 9 × 10 mm. Coronary angiography confirmed this to be at the poste- rior aspect of bifurcation of the left main and excluded any coronary stenosis (Fig. 1). Operative treatment was considered as she was symptomatic. The operative approach was through a median ster- notomy. Bilateral internal mammary arteries (IMAs) were harvested. Cardiopulmonary bypass was estab- lished through aorta and right atrial cannulation. After aortic cross-clamp, cold-blood cardioplegic arrest (ante- grade and retrograde) was used and repeated every 15 minutes. The main pulmonary artery was divided be- low the bifurcation and was retracted anteriorly along with the right ventricular outflow to expose the left main bifurcation. The aneurysm was not visible exter- nally (Fig. 2A). Arteriotomy of the left main revealed the neck of the saccular aneurysm on the posterior wall (Fig. 2B). The aneurysm sac was free of thrombus. The left main (afferent), left anterior descending (LAD), and circumflex (efferents) were individually identified, probed, transfixed and suture ligated, and the sac was excluded. Coronary bypasses were performed with left IMA to LAD and right IMA to high-lateral circumflex artery. The right IMA was taken off the left IMA as a Y graft because it was not long enough to reach the high- lateral circumflex through the retro-aortic route. The postero-lateral circumflex artery was bypassed with re- versed saphenous vein graft because the aneurysm was involving the left main (LM) bifurcation and ori- gin of the high-lateral circumflex artery was coming off the aneurysm. By ligating the aneurysm, there would be no communication between the high-lateral circum- flex and the postero-lateral circumflex artery. Radial artery was not used due to poor arterial perfusion index of the nondominant hand. The pulmonary artery was closed directly with a continuous suture technique with 5-0 prolene suture. The aortic cross-clamp time was 65 minutes and the pump time was 105 minutes. The patient had an uneventful recovery and was discharged after four days on Clopidogrel for six weeks and on Aspirin and Lipitor. DISCUSSION Coronary artery aneurysms are diagnosed with in- creasing frequency since the advent of coronary angiography with an incidence of up to 5.3%. 1 Typ- ical causes include Kawasaki disease, atheroscle- rosis, trauma, polyarteritis nodosa, systemic lupus erythrematosus, syphilis, and idiopathic. 2 Small asymp- tomatic aneurysms are treated with simple observation whereas giant or symptomatic aneurysms are consid- ered for operative treatment. The cut-off size for LMCA aneurysm repair is not well described. We believe that
Transcript of Delayed Surgical Retrieval of Retained Guidewire Following Percutaneous Coronary Intervention

c© 2010 Wiley Periodicals, Inc. 37
CASE REPORTS
Successful Management of aPosterior Saccular CoronaryArtery Aneurysm at the LeftMain Coronary ArteryBifurcation
Rajesh Ramankutty, M.D.,Turki B. Albacker, M.D.,Karl G. Reyes, M.D.,and Jose L. Navia, M.D.
Department of Thoracic and CardiovascularSurgery, Cleveland Clinic Foundation,Cleveland, Ohio
ABSTRACT Left main coronary artery aneurysm is arare condition that presents as a potential surgicalchallenge due to its location. We present a case ofsuccessful repair of a posterior saccular aneurysmof the left main coronary artery by aneurysm ex-clusion, afferent and efferent ligation with coro-nary artery bypass grafting. doi: 10.1111/j.1540-8191.2010.01030.x (J Card Surg 2011;26:37-39)
Aneurysm of the left main coronary artery (LMCA) isan extremely rare condition. Compared to aneurysmsof the right main coronary artery, surgical managementof LMCA aneurysms is more challenging because of itslocation behind the main pulmonary artery. We presenta case of successful management of a large posteriorsaccular aneurysm involving the LMCA bifurcation.
CASE REPORT
A 46-year-old woman presented with an incidentalfinding of 9 × 7 × 7.5 mm aneurysm at the level ofthe LMCA bifurcation. The patient was initially asymp-tomatic and the aneurysm was detected incidentallyby chest computed tomography scan when she volun-teered as the first patient for the new scanner installedat the facility where she worked as a radiology tech-nician. Since she was asymptomatic, she was initiallymanaged conservatively with antiplatelets and serialfollow-ups. Two years later, she developed new atypi-cal chest pain and exertional dyspnea, New York HeartAssociation class II-III, with no medical comorbidities.Physical exam, chest x-ray (CXR), and electrocardio-gram were unremarkable. Transthoracic echocardiog-
Address for correspondence: Turki B. Albacker, M.D., Departmentof Thoracic and Cardiovascular Surgery, 9500 Euclid Avenue/J4-133E, Cleveland, OH 44195. Fax: 1(216) 636-1286; e-mail: [email protected]
raphy demonstrated good biventricular function, nor-mal valves, and was negative for stress-induced is-chemia. Computed tomography of the chest showed amarginally increased aneurysm size to 11 × 9 × 10 mm.Coronary angiography confirmed this to be at the poste-rior aspect of bifurcation of the left main and excludedany coronary stenosis (Fig. 1). Operative treatment wasconsidered as she was symptomatic.
The operative approach was through a median ster-notomy. Bilateral internal mammary arteries (IMAs)were harvested. Cardiopulmonary bypass was estab-lished through aorta and right atrial cannulation. Afteraortic cross-clamp, cold-blood cardioplegic arrest (ante-grade and retrograde) was used and repeated every 15minutes. The main pulmonary artery was divided be-low the bifurcation and was retracted anteriorly alongwith the right ventricular outflow to expose the leftmain bifurcation. The aneurysm was not visible exter-nally (Fig. 2A). Arteriotomy of the left main revealedthe neck of the saccular aneurysm on the posteriorwall (Fig. 2B). The aneurysm sac was free of thrombus.The left main (afferent), left anterior descending (LAD),and circumflex (efferents) were individually identified,probed, transfixed and suture ligated, and the sac wasexcluded. Coronary bypasses were performed with leftIMA to LAD and right IMA to high-lateral circumflexartery. The right IMA was taken off the left IMA as a Ygraft because it was not long enough to reach the high-lateral circumflex through the retro-aortic route. Thepostero-lateral circumflex artery was bypassed with re-versed saphenous vein graft because the aneurysmwas involving the left main (LM) bifurcation and ori-gin of the high-lateral circumflex artery was coming offthe aneurysm. By ligating the aneurysm, there wouldbe no communication between the high-lateral circum-flex and the postero-lateral circumflex artery. Radialartery was not used due to poor arterial perfusion indexof the nondominant hand. The pulmonary artery wasclosed directly with a continuous suture technique with5-0 prolene suture. The aortic cross-clamp time was65 minutes and the pump time was 105 minutes. Thepatient had an uneventful recovery and was dischargedafter four days on Clopidogrel for six weeks and onAspirin and Lipitor.
DISCUSSION
Coronary artery aneurysms are diagnosed with in-creasing frequency since the advent of coronaryangiography with an incidence of up to 5.3%.1 Typ-ical causes include Kawasaki disease, atheroscle-rosis, trauma, polyarteritis nodosa, systemic lupuserythrematosus, syphilis, and idiopathic.2 Small asymp-tomatic aneurysms are treated with simple observationwhereas giant or symptomatic aneurysms are consid-ered for operative treatment. The cut-off size for LMCAaneurysm repair is not well described. We believe that

38 RAMANKUTTY, ET AL.MANAGEMENT OF A POSTERIOR SACCULAR CORONARY ARTERY ANEURYSM
J CARD SURG2011;26:37-68
Figure 1. Coronary angiography demonstrating posteriorly lo-cated saccular coronary artery aneurysm.
size alone should not be a factor in determining timingof operation as besides rupture (determined by size)there are other dreaded complications (inherent to thelocation) such as thrombosis, embolization, dissection,mechanical obstruction, and erosion into surroundingstructures with fistula formation. Aneurysm resectionwith interposition graft with or without coronary bypasshas been the most commonly used method for repairof fusiform coronary aneurysms.3-6 Aneurysm resec-tion and patch repair with vein or autologous pulmonaryartery has been described for anteriorly located saccu-lar aneurysms.7,8 Posteriorly located aneurysms, how-ever, are more technically challenging due to limita-tions with adequately visualizing the origin and courseof the aneurysm. Strategies for repairing these types ofaneurysms have not been described. Patch closure ofthe aneurysm neck at the posterior wall of the coro-nary artery combined with patch closure of the anteriorwall may be a theoretical option but carries the risk ofcompression of LMCA behind the pulmonary artery atthe area of the two patches. We advocate in this papertreating posterior saccular aneurysms in the same way
Figure 2. Intraoperative photo showing the left main coronary artery with no visible aneurysm (A, left), and the left main coronaryartery after arteriotomy revealing the neck of the saccular aneurysm (B, right).
like fusiform aneurysms with afferent and efferent liga-tion and exclusion of the aneurysmal sac with coronaryartery bypass grafting (CABG). This technique is safe,simple, and reproducible in most experienced centers.In addition, it avoids potential compression risk withpatch repair.
The use of Clopidogrel in our patient was based onsurgeon’s preference. The use of Clopidogrel post-CABG in patients at high risk for cardiac events wasshown to reduce their risk by 20% to 30% in CAPRIEtrial. Other studies showed that Clopidogrel can re-duce the risk of recurrent cardiac events post off-pumpCABG when used for one month postoperation with noadded benefits beyond this period. The benefit of us-ing Clopidogrel postoperatively in all CABG patients isa controversial topic and needs further studies. Giventhe fact that the majority of coronary artery aneurysmsare atherosclerotic in origin, we believe that this patientwill need long-term statin therapy, despite her normalpreoperative low-density lipoprotein level, since it wasshown to delay the atherosclerotic changes in the veingraft as well as arterial grafts, and it will also be use-ful as a primary preventive therapy for native vesselatherosclerosis.
CONCLUSION
The management of coronary aneurysms of theLMCA requires an individualized approach that isdependent upon size, shape, and location. While patchrepair has been emerging more frequently as the pre-ferred option, this is not usually feasible for posteriorlylocated aneurysms. Simple ligation with coronary graft-ing for aneurysms not accessible to patch repair can beperformed with acceptable outcomes that are only lim-ited by the duration of patency of the coronary bypassgrafts.
REFERENCES
1. Demopoulos V, Olympios C, Fakiolas C, et al: The natu-ral history of aneurysmal coronary artery disease. Heart1997;78:136-141.

J CARD SURG2011;26:37-68
NWILOH, ET AL.PAPILLARY FIBROELASTOMA
39
2. Hartnell GG, Parnell BM, Pridie RB: Coronary artery ectasia:Prevalence and clinical significance in 4993 patients. BrHeart J 1985;54:392-395.
3. Li D, Wu Q, Sun L, et al: Surgical treatment of gi-ant coronary artery aneurysm. J Thorac Cardiovasc Surg2005;130:817-821.
4. Unic D, Mihaljevic T, Leacche M, et al: Surgical treatmentof a large left main coronary artery aneurysm. Thorac Car-diovasc Surg 2004;52:230-231.
5. Anderson CA, Filsoufi F, Kadner A, et al: Repair of aleft main coronary artery aneurysm using the circumflexfemoral artery as a Y-interposition graft. Ann Thorac Surg2004;78:314-316.
6. Turkay C, Golbasi I, Sahin N, et al: Surgical managementof an atherosclerotic aneurysm of the left main coronaryartery. J Thorac Cardiovasc Surg 2001;122:626-627.
7. Patila T, Virolainen J, Sipponen J, et al: Resection and patchrepair of a large saccular coronary artery aneurysm at theleft main bifurcation. Ann Thorac Surg 2009;87:297-299.
8. Pruetz JD, Takahashi M, Reemtsen BL, et al: A novel ap-proach to left main coronary artery giant aneurysm throm-bosis in a child with a history of Kawasaki disease. J ThoracCardiovasc Surg 2009;137:1030-1032.
Right Atrial PapillaryFibroelastoma
Jonathan Nwiloh, M.D.,∗Earnesto Hernandez, M.D.,†and Ada Mercado, M.D.†Section of ∗Cardiothoracic Surgery, and†Cardiology, St. Joseph’s Hospital, Atlanta,Georgia
ABSTRACT Papillary fibroelastoma (PFE) is a benigncardiac tumor rarely seen in the right atrium and of-ten misdiagnosed as atrial myxoma or thrombus.We report one such case found in the right atriumduring workup in a patient presenting with tran-sient ischemic attack (TIA). PFEs are found mostfrequently in the valvular endocardium of the leftheart. When encountered in the right heart andsymptomatic, they tend to be larger in size pre-sumably due to a longer latent period of growth. Al-though histologically the tumors are benign, theyhave the potential for fatal complications due totheir propensity to embolize. doi: 10.1111/j.1540-8191.2010.01042.x (J Card Surg 2011;26:39-41)
Address for correspondence: Jonathan Nwiloh, M.D., Section ofCardiothoracic Surgery, St. Joseph’s Hospital, 5665 PeachtreeDunwoody Rd, Atlanta, GA 30342. Fax: 678-904-5186; e-mail:[email protected]
CASE REPORT
A 73-year-old male with no prior neurologic or car-diac history developed sudden onset of numbness withtingling of the left side of his face and the left fin-gers lasting less than an hour. He was diagnosed withtransient ischemic attack (TIA) by the neurologist andneurologic workup with a magnetic resonance imagingand carotid duplex scan were negative. Cardiac workupwith electrocardiogram showed regular sinus rhythm,while transthoracic and transesophageal echocardio-gram revealed a 3.3 × 3-cm irregular mobile mass in theright atrium and normal left ventricular function (Fig. 1).The differential diagnosis was thrombus or myxoma.Lower extremities venous duplex scan was normal.Cardiac catheterization revealed severe triple-vesselcoronary artery disease. Patient subsequently under-went surgery via a median sternotomy, with cardiopul-monary bypass via ascending aortic and bicaval cannu-lation. The tumor was exposed through a right obliqueatriotomy and a gelatinous 3 × 3-cm tumor attached viaa small stalk to the interatrial septum above the fossaovalis was excised. There was no atrial septal defect orpatent fossa ovalis seen. Triple coronary artery bypasswith left internal mammary artery to the left anteriordescending and reversed saphenous vein grafts to theposterior descending and obtuse marginal coronary ar-teries were next performed. Postoperatively, patienthad paroxysmal atrial fibrillation and was dischargedon day 8 in sinus rhythm. Pathology showed a 3.1 ×2.6 × 1.1-cm friable glistening tan-red tissue, withmicroscopy showing papillary proliferation composedof a single layer of flattened cuboidal cells surround-ing an avascular core of dense hypocellular collage-nized fibrous tissue surrounded by myxoid ground sub-stance consistent with of papillary fibroelastoma (PFE)(Fig. 2).
COMMENT
Primary cardiac tumors are relatively rare, with PFEbeing the third most common after atrial myxomas andlipomas. PFEs are relatively rare in the right atrium asdocumented in a review of 725 cases of PFE publishedin all languages reported by Gowda et al.1 and 162cases by Sun et al.2 showing only 2.3% and 1.8%, re-spectively, were located in the right atrium. The meanage was 60 years with no sex preference in both series.While the etiology is unknown, tumors are mainly ac-quired and some have suggested they represent a neo-plasm, hamartomas, or inflammatory nodules possi-bly from mechanical trauma. These tumors are grosslygelatinous with a sea anemone appearance. They arefriable and prone to emboli and thus their characteris-tic presentation with ischemic neurological or cardiacsymptoms for left heart tumors. Paradoxical embolifrom right-sided tumors can occur in the presence ofright-to-left shunting septal defects. They can also man-ifest with obstructive symptoms if the tumor interfereswith flow across the atrioventricular valves.
Only seven surgical cases of right atrial PFE tothe best of our knowledge have been reported

40 NWILOH, ET AL.PAPILLARY FIBROELASTOMA
J CARD SURG2011;26:37-68
Figure 1. Two-dimensional transesophageal echocardiogram showing right atrial PFE.
previously.3-8 Review of these seven cases and ourown patient shows there were four males and foursfemales with mean age of 70 years. The mean diame-ter at diagnosis of the right atrial PFE was 27 mm com-pared to 10 mm and 9 mm in the mainly left-sided PFEreports by Gowda et al. and Sun et al.,1,2 respectively.Three patients had only neurologic symptoms (syncopeand TIA), three only respiratory symptoms (dyspnea),one had both neurologic and respiratory symptoms,and one was asymptomatic, picked up on routine pre-
Figure 2. Papillary proliferation with core of dense fibrous tissue surrounded by myxoid ground substance covered by cuboidalcells.
operative echocardiogram for an orthopedic procedure.The clinical presentation of TIA in our patient, however,was serendipitous and unlikely related to the PFE, aswe were unable to document a patent foramen ovaleor other right-to-left shunt at surgery. All reported eightpatients underwent surgical resection on cardiopul-monary bypass and made uneventful recovery.
Unlike left-sided PFE, which manifests early clinicalsymptoms despite their smaller sizes (9 to 10 mm) atpresentation, the right atrial PFE tend to be 2 to 3 times

J CARD SURG2011;26:37-68
REZAIAN, ET AL.AMPLATZER DEVICE-ASSOCIATED THROMBOSUS
41
larger (27 mm) at the time of diagnosis in the reportedeight surgical series. This observation of larger sizetumors on the right compared to the left heart suggeststhat the natural history for these tumors is to grow overtime if left untreated.
With the ubiquitous use of echocardiography andother imaging techniques, these tumors are likely tobe discovered earlier when smaller and asymptomaticespecially in the right atrium. Because of their propen-sity for growth with time, we recommend surgical re-section for right atrial tumors larger than 1 cm, even inasymptomatic patients as the operative mortality andmorbidity are extremely low, unless the patient is a highsurgical risk. However, anticoagulation may be indi-cated if there is a high index of suspicion for a thrombusin the presence of the mass attached to an indwellingcatheter, transvenous pacemaker lead, or evidence ofdeep venous thrombosis. To aid in the differential di-agnosis with a thrombus, Sun et al.2 have describedthe characteristic echocardiographic appearance ofPFE as round, oval, or irregular, well demarcated andhomogenous.
Finally with the advanced age of the typical patientswith right atrial PFE, concomitant coronary artery dis-ease is not uncommon as with our patient who requiredtriple coronary artery bypass and in two other reportedsurgical cases.6,7
REFERENCES
1. Gowda RM, Khan IA, Nair CK, et al: Cardiac papillary fi-broelastoma: A comprehensive analysis of 725 cases. AmHeart J 2003;146:404-410.
2. Sun JP, Ascher CR, Yang XS, et al: Clinical and echocardio-graphic characteristics of papillary fibroelastoma: A retro-spective and prospective study in 162 patients. Circulation2001;103:2687-2693.
3. Gallas MT, Reardon MJ, Reardon PR, et al: Papillary fi-broelastoma. A right atrial presentation. Tex Heart Inst J1993;20:293-295.
4. Crestanello JA, Orszulak TA: Giant papillary fibroelastomaof the right atrium: An unsual presentation. Ann ThoracSurg 2002; 74: 1252-1254.
5. Hindupur S, Schwabe JL: Papillary fibroelastoma of theright atrium: An atypical presentation. J Cardiovasc Surg2005;45:589-591.
6. Lotto AA, Earl UM, Owens WA: Right atrial mass: Throm-bus, myxoma or cardiac papillary fibroelastoma. J ThoracCardiovasc Surg 2006;132:159-160.
7. Abad C, De la Rosa P: Right atrial papillary fibroelastoma as-sociated with atrial septal defect, persistent superior venacava and coronary artery disease. J Thorac Cardiovasc Surg2008;136:538.
8. Gabbieri D, Rossi G, Bavutti L, et al: Papillary fibroelas-toma of the right atrium as an unusual source of recurrentpulmonary embolism. J Cardiovasc Med 2006;7:373-378.
Nitinol Wire Mesh Fracture andTraumatic Left Atrial Thrombusin a Patient with Atrial SeptalDefect Amplatzer Occluder
Gholam Reza Rezaian, M.D.,∗Ahmad Ali Amirghofran, M.D.,†Sasan Afifi, M.D.,∗ Ali Reza Moaref, M.D.,∗and Sheema Rezaian, M.D.‡∗Department of Medicine (Cardiology),†Department of Surgery (Cardiac Surgery),and ‡Alzahra Cardiovascular ResearchCenter, Shiraz University of MedicalSciences, Shiraz, Iran
ABSTRACT Although wire device frame fractureassociated with thrombus formation has been re-ported in some types of atrial septal defect occlud-ers, it has not been detected in patients with Am-platzer devices. Here, we describe an unusual caseof Nitinol wire mesh fracture associated with leftatrial endocardial damage and thrombus formationin an adult with Amplatzer septal occluder. doi:10.1111/j.1540-8191.2010.01104.x (J Card Surg2011;26:41-43)
Device-associated atrial thrombi are rare but well-known complications after atrial septal defect (ASD) orpatent foramen ovale (PFO) closure. The majority ofthese clots occur within the first six months after de-vice implantation despite adequate antiplatelet or anti-coagulant therapy. A persistant atrial septal aneurysm,new onset or persistent atrial fibrillation (AF),1 and cer-tain closure device types2 may act as predisposingfactors.
The Amplatzer septal occluders are generally asso-ciated with infrequent complications such as deviceembolization or thrombus formation.3
We present an unusual case of Nitinol wire meshfracture associated with left atrial (LA) endothelial dam-age and thrombus formation in an adult with an Am-platzer septal occluder while receiving prophylactic as-pirin (ASA).
CASE REPORT
A 38-year-old single, unmarried woman was admit-ted to our university hospital for a follow-up trans-esophageal echocardiography (TEE). Two years earliershe had undergone a TEE-guided transcatheter clo-sure of her ASD under local anesthesia using a 28-mm
Conflict of interest: None.
Address for Correspondence: Gholam Reza Rezaian, M.D., Depart-ment of Medicine (Cardiology), Namazee Hospital, 71937-11351 Shi-raz University of Medical Sciences, Shiraz, Iran. Fax: 98-711-648-6509;e-mail: [email protected]

42 REZAIAN, ET AL.AMPLATZER DEVICE-ASSOCIATED THROMBOSUS
J CARD SURG2011;26:37-68
Figure 1. (A) Apical four-chamber view of two-dimensionaltransthoracic echocardiogram revealing the interatrial septaldefect occluder as well as the clot (arrow head) in the leftatrial cavity. (B) Bicaval transesophageal view showing theleft atrium (LA) and right atrium (RA), the occluder device (O),the clot (C) in the left atrial cavity, and the inferior vena cava(IVC) and superior vena cava (SVC).
Amplatzer septal occluder (AGA Medical, Minneapolis,MN, USA) with no residual shunt and was dischargedon aspirin 100 mg/day. Her exertional dyspnea im-proved and she was doing well. Although she refusedfollow-up transesophageal echocardiogram (TEE), allher TTEs were normal.
Recently she came back for a scheduled follow-up echocardiogram after two years of Amplatzer im-plantation. She did not have any symptoms and hercardiac examination was unremarkable. Her transtho-racic echocardiogram, however, showed a floating
Figure 2. Multiple interoperative views (A) showing the opened left atrial (LA) chamber, the ASD occluder (O), and the clot in theposterior aspect of LA, unattached to the device. (B) The arrow points toward the attachment site and stalk of the clot. (C) Thewhite arrow head demonstrates the small-sized fractured (F) portion of the Nitinol mesh and the arrow points toward the tinyinjured site of LA endocardium that was the attachment site of the clot stalk. (D) Magnified view of the occluder and its fractured(F) part, protruding into LA cavity and pointing to its posterior wall.
echogenic structure in the LA cavity (Fig. 1A). She wasadvised to be hospitalized and to have TEE as well.On admission to the Coronary Care Unit (CCU), herblood pressure was 130/90 mmHg, the pulse rate was80 beats/min and regular, and she was afebrile. Therest of her physical examination including neurologicalfindings was normal.
The electrocardiogram showed normal sinus rhythmand her TEE revealed a well-seated Amplatzer devicewith no residual shunt. A large highly mobile thrombusmeasuring about 1.6 × 1.3 cm was noted attached tothe postero-inferior wall of the left atrium adjacent tothe device with a very thin stalk (Fig. 1B).
No spontaneous echo contrast or additional clotswere detected in the cardiac chambers. Coagulationprofile, platelet count, erythrocyte-sedimentation rate,anti-phospholipid antibodies, ANA, dsDNA, and factorV leiden were normal.
She was started on heparin drip and because of dan-ger of possible catastrophic embolization she agreedto undergo surgery.
It was decided to operate using a video-assisted,minimally invasive approach. The patient was fully hep-arinized and cardiopulmonary bypass was institutedthrough the femoral artery and femoral vein cannula(19 mm Fr and 24 mm Fr, respectively). Through aright (4 cm) mini-thoracotomy under the right breast,the chest was entered. Aorta was directly clamped byChit wood clamp and cold blood cardioplegia was givenwhile the patient was cooled to 32 ◦C. The left atriumwas opened. There was a 15 × 15 mm white–red massattached loosely by a 10-mm stalk to the posterior wallof the left atrium just opposite the ASD closure de-vice but not attached to it (Fig. 2A). The mass, which

J CARD SURG2011;26:37-68
REZAIAN, ET AL.AMPLATZER DEVICE-ASSOCIATED THROMBOSUS
43
looked like an organized clot, was removed and thedevice was carefully examined by the thoracoscope.The device had successfully closed the ASD without aresidual defect but there was a 6-mm-long wire fromthe metallic network of the device that had perpendicu-larly protruded from the surface of the device and waspointing toward the posterior LA wall just opposite theattachment site of the clot (Fig. 2B–D). The confrontinglocation of the wire and the clot highly raised the pos-sibility of irritation of the posterior LA free wall by thetip of the protruded wire causing endocardial damageand clot formation (Fig. 2C). The wire was cut from itsbase and the left atrium was closed after plication ofLA appendage.
The patient had a completely uneventful recovery pe-riod and was discharged from the hospital on postop-erative day 7 with an oral anticoagulant (warfarin). Thefinal pathology showed an organized thrombus. RepeatTEEs four and 16 weeks later showed no residual clotin the LA cavity. The device was functioning well andno shunt could be detected.
DISCUSSION
This is the first documented case of an Amplatzerdevice fracture associated with LA endocardial traumaand thrombus formation.
Although the majority of device-associated thrombirespond successfully to anticoagulant therapy and sub-sequently resolve without symptoms,4 they are still amajor concern because of the chance of embolizationto the central nervous system5 especially within thefirst year after device implantation.6
Our patient had a highly mobile clot carrying a higherrisk of catastrophic embolization. Thus, surgical inter-vention was indicated.
The Amplatzer septal occluder device is made up ofa Nitinol wire mesh in the form of a self-expandabledouble disc and a connecting waist. As shown in Fig-ure 2, a small piece of the Nitinol wire was detachedfrom the original wire mesh and was protruding intothe LA cavity causing the endocardial damage and clotformation.
Generally this occluder is associated with very sat-isfactory long-term results and has been associatedwith infrequent, albeit nonsurgically manageable com-plications.3,7 In their series of 1000 consecutive pa-tients undergoing PFO or ASD closure by nine dif-ferent occluder devices, Krumsdorf et al.1 reportedthe four-week prevalence of thrombotic events to be7.1% in patients with the CardioSeal occluder com-pared to the 0% prevalence in those with Amplatzerdevice. In addition to the type of device, the presenceof a septal aneurysm as well as new onset AF arealso important factors that contribute to clot forma-tion with ASD occluders. Wire device frame fractureshave also been associated with thrombus formation;however, these have all been reported to occur in theright atrium and none were found with an Amplatzerdevice.2
A wire device frame fracture associated with throm-bus formation was found in three of the 20 (15%) pa-
tients of Krumsdorf’s series.1 However, all wire frac-tures were on the right atrial side of the occluders,none of which were an Amplatzer device.
This case highlights the importance of long-termTEE follow-up for all patients receiving an AmplatzerASD occlusion device because of the possibility of latethromboembolic events.
Acknowledgement: We thank Mrs. K. Shashok (AuthorAIDin the Eastern Mediterranean Journal) for improving the useof English in the manuscript.
REFERENCES
1. Krumsdorf U, Ostermayer S, Billinger K, et al: Incidenceand clinical course of thrombus formation on atrial septaldefect and patent foramen ovale closure devices in 1000consecutive patients. J Am Coll Cardiol 2004;43:302-309.
2. Anzai H, Child J, Natterson B, et al: Incidence of thrombusformation on the CardioSeal and the Amplatzer interatrialclosure devices. Am J Cardiol 2004;93:426-431.
3. Losay J, Petit J, Lambert V, et al: Percutaneous closurewith Amplatzer devices is a safe and efficient alternativeto surgery in adults with large atrial septal defects. AmHeart J 2001;142:544-548.
4. La Rosee K, Deutsch HJ, Schnabel P, et al: Thrombus for-mation after transcatheter closure of atrial septal defect.Am J Cardiol 1999;84:356-359.
5. Nkomo VT, Theuma P, Maniu CV, et al: Patent foramenovale transcatheter closure device thrombosis. Mayo ClinProc 2001;76:1057-1061.
6. Braun MU, Fassbender D, Schoen SP, et al: Trans-catheter closure of patent foramen ovale in patients withcerebral ischemia. J Am Coll Cardiol 2002;39:2019-2025.
7. Cowley CC, Lloyd TR, Bove EL, et al: Comparison of resultsof closure of secondum atrial septal defects by surgery ver-sus Amplatzer septal occluder. Am J Cardiol 2001;88:589-591.

44 YANAGAWA, ET AL.CORONARY BYPASS FOR ANOMALOUS CORONARY ARTERY
J CARD SURG2011;26:37-68
Coronary Artery Bypass Graftfor Anomalous Right CoronaryArtery
Bobby Yanagawa, M.D., Ph.D.,∗Abdullah A. Alghamdi, M.D., M.Sc.,∗Robert B. Chen, M.D.,†Anthony Amankwaa, B.Sc.,∗ andSubodh Verma, M.D., Ph.D.∗
∗Division of Cardiac Surgery, and†Department of Anesthesia, St. Michael’sHospital, University of Toronto, Toronto,Ontario, Canada
ABSTRACT A 27-year-old man with anomalous rightcoronary artery (RCA) presented with ventricularfibrillatory arrest. Computed tomography angiog-raphy revealed an anomalous RCA arising fromthe left sinus of Valsalva with an acute angula-tion at the coronary takeoff and compressed inter-arterial segment. This patient underwent a shortsaphenous vein coronary artery bypass graft tothe proximal RCA and recovered uneventfully. Areview of the literature and discussion of the surgi-cal management is presented. doi: 10.1111/j.1540-8191.2010.01116.x (J Card Surg 2011;26:44-46)
Although difficult to estimate the exact prevalence,anomalous coronary arteries are rare with an incidenceof 0.3% to 1.3% in an autopsy series.1 The majorityof cases are clinically silent but may occasionally resultin arrhythmias, myocardial ischemia and infarction, orsudden cardiac death. Here, we present a patient with
Conflict of interest: None.
Address for correspondence: Subodh Verma, M.D., Ph.D., F.R.C.S.C.,F.A.H.A., Division of Cardiac Surgery, Suite 8-003F, Bond Wing, St.Michael’s Hospital, 30 Bond Street, Toronto, Ontario, Canada, M5B1W8. Fax: 1-416-864-5881; e-mail: [email protected]
Figure 1. (A) Coronary angiogram aortic root injection demonstrating right (white arrows) and left (black arrows) coronary arteries,and (B) CT angiogram demonstrating narrowed anomalous right coronary artery (arrows).
a right coronary artery (RCA) anomaly who presentedwith ventricular fibrillatory arrest and was referred forsurgical revascularization.
A 27-year-old Asian male presented with cardiacarrest while playing basketball. He returned to si-nus rhythm following four defibrillatory shocks andwas taken to the hospital for treatment for presumedacute coronary syndrome. Peak troponin was 29 μg/L(Normal value <0.07 μg/L). Echocardiography demon-strated severely depressed left ventricular functionwith global hypokinesis. Past medical history was non-contributory and this patient had no coronary riskfactors.
By coronary angiography, aortic root contrast injec-tion demonstrated right and left coronary arteries withadjacent orifices from the left sinus of Valsalva (Fig. 1A).Computed tomography (CT) angiography confirmed adominant and narrowed RCA arising from the left sinusof valsalva with an acute angulation at the coronarytakeoff and a 6- to 8-mm interarterial segment thatwas compressed with 70% stenosis (Fig. 1B). Aorto-coronary coronary artery bypass graft (CABG) was per-formed on pump using a short saphenous vein graft tothe proximal RCA just distal to the anomalous seg-ment. The postoperative course was unremarkable,and the patient was discharged from the hospital onthe sixth postoperative day. At the time of discharge,echocardiography demonstrated normal left ventricu-lar function and the patient completed 65% of age-predicted maximum of the modified Bruce protocol.He was placed on oral aspirin therapy, and an im-plantable cardioverter-defibrillator was implanted forprophylaxis of future ventricular fibrillatory events. Thepatient was free of symptoms at three months follow-ing discharge.
COMMENT
In this case, the RCA originated from the oppositesinus of Valsalva with further compression in the rightatrioventricular sulcus between the pulmonary arteryand aortic roots, likely responsible for cardiac arrest.The majority of cases of anomalous coronary arteriesare clinically silent and diagnosis is incidental. How-ever, Angelini et al.2 identify anomalous coronary artery

J CARD SURG2011;26:37-68
YANAGAWA, ET AL.CORONARY BYPASS FOR ANOMALOUS CORONARY ARTERY
45
TABLE 1Surgical Revascularization Strategies for Anomalous Right Coronary Artery
Level of DifficultySurgical Technique (+ − ++++/++++) Potential Complications Reference
Coronary unroofing +++ CA injury 7, 12Aortic insufficiency
Neoostial formation ++ CA injury 12Aortic insufficiency
Ostial translocation +++ CA kinking 13Pulmonary artery translocation +++ Obstruction: acute angle at CA orifice 14Pulmonary artery translocation +++ CA injury 15
with patch arterioplasty Aortic insufficiencyCABG: vein graft + Early graft failure 16CABG: mammary artery + Vasospasm by coronary steal 16(+/− native artery ligation)
Note: Subjective level of difficulty scale ranges from least difficult (+) to most difficult (++++).CA = coronary artery; CABG = coronary artery bypass graft.
from the opposite sinus (ACAOS) as a particularly perni-cious variant associated with higher incidence of sud-den death. Indeed, ventricular fibrillation and suddendeath following exertion have been reported in severalcase series of RCA anomalies.3-5 As in our case, pooroutcome is associated with high-risk features such as aslit-like coronary ostium, acute proximal angle, and flat-tening of the interarterial segment from compressionbetween the aortic and pulmonary artery roots.6
Cardiac arrest in the setting of ACAOS is a clear in-dication for intervention. Surgical revascularization op-tions for RCA anomalies are given (Table 1). Includedis an overall subjective grade of the level of techni-cal difficulty for successful completion in the absenceof complications. A recent case series from the MayoClinic reported 36 patients with anomalous coronaryarteries and of these, 14 underwent CABG and 22 un-derwent coronary unroofing.7 Coronary artery unroof-ing and neoostial formation have excellent long-termoutcomes and avoid the use of a graft.
The surgical strategy for our patient with vein by-pass grafting was based on the following: first, therewas baseline significant stenosis (>70%) in the longintraarterial segment with normal runoff. In keepingwith the law of Laplace, the shared aortic and coro-nary artery wall likely compressed the coronary arterydue to larger radius and thus elevated aortic wall ten-sion. Second, additional complicating anatomical fac-tors included angulation of the takeoff and locationbetween the great arteries where unroofing the intraar-terial segment alone may be insufficient. Third, despitegood long-term patency with complex coronary repairs,there exists a significant risk of coronary artery injuryor alteration of the sinus geometry resulting in aorticinsufficiency, particularly in centers not experienced insuch repairs. Fourth, a venous conduit was utilized asthe use of a mammary artery, either in situ or as afree graft, is at increased risk of vasospasm and occlu-sion with competitive flow. Furthermore, contempo-rary vein graft patency to high-quality coronary targetshas been reported as 90% at 5 years and 80% at 10years.8,9 In our patient, the target vessel has optimaldistal flow, thus we expect comparable or better pa-
tency in our patient. An additional advantage of leavingthe left internal mammary artery (LIMA) in place is thatit may be utilized in the event that the patient mayrequire coronary revascularization later in life.
Alternatively, short-term results from stent place-ment in this population have been shown to be ef-fective but complicated by restenosis and further donot resolve the acute angulation at the coronary ori-fice.10,11 We felt that the young age of our patient andthe large territory of dependent myocardium posed aprohibitively high risk for this approach.12
As our patient had clear evidence of myocardial is-chemia in the context of ACAOS, prompt interventionwas indicated. However, for cases of asymptomaticanomalous RCA, the decision to operate is less clearand serial stress testing, CT angiography, and closepatient follow-up may be appropriate. Regarding therisk of subsequent ventricular fibrillatory events, if thecause was myocardial ischemia, then no further riskshould be present with restoration of coronary bloodsupply. On the other hand, myocardial infarction couldtrigger another ventricular fibrillatory event and evi-dence of such warrants an electrophysiological studyand possible cardioverter-defibrillator implantation. Ourpatient presented with elevated troponin that is likelysecondary to repeated defibrillation, but myocardial in-farction could not be ruled out. Therefore, given theyoung age of the patient, a cardioverter-defibrillatorwas implanted.
REFERENCES
1. Alexander RW, Griffith GC: Anomalies of the coro-nary arteries and their clinical significance. Circulation1956;14:800-805.
2. Angelini P, Velasco JA, Ott D, et al: Anomalous coro-nary artery arising from the opposite sinus: Descriptivefeatures and pathophysiologic mechanisms, as docu-mented by intravascular ultrasonography. J Invasive Car-diol 2003;15:507-514.
3. Taylor AJ, Byers JP, Cheitlin MD, et al: Anomalous rightor left coronary artery from the contralateral coronary si-nus: “high-risk” abnormalities in the initial coronary artery

46 MODI, ET AL.SURGICAL RETRIEVAL OF RETAINED GUIDEWIRE
J CARD SURG2011;26:37-68
course and heterogeneous clinical outcomes. Am HeartJ 1997;133:428-435.
4. Cox ID, Bunce N, Fluck DS: Failed sudden cardiac deathin a patient with an anomalous origin of the right coronaryartery. Circulation 2000;102:1461-1462.
5. Roberts WC, Siegel RJ, Zipes DP: Origin of the right coro-nary artery from the left sinus of Valsalva and its func-tional consequences: Analysis of 10 necropsy patients.Am J Cardiol 1982;49:863-868.
6. Angelini P: Coronary artery anomalies—current clinicalissues: Definitions, classification, incidence, clinical rel-evance, and treatment guidelines, Tex Heart Inst J2002;29:271-278.
7. Davies JE, Burkhart HM, Dearani JA, et al: Surgical man-agement of anomalous aortic origin of a coronary artery.Ann Thorac Surg 2009;88:844-847.
8. PAR Hayward, BF Buxton. Angiographic patency of coro-nary artery grafts: 5-year observational data from therandomized controlled Radial Artery Patency and Clini-cal Outcomes (RAPCO) Study. Ann Thorac Surg 2007;84:795-799.
9. Hayward PA, Gordon IR, Hare DL, et al: Comparablepatencies of the radial artery and right internal thoracicartery or saphenous vein beyond 5 years: Results fromthe Radial Artery Patency and Clinical Outcomes trial.J Thorac Cardiovasc Surg 2010;139:60-65.
10. Hariharan R, Kacere RD, Angelini P: Can stent-angioplastybe a valid alternative to surgery when revascularization isindicated for anomalous origination of a coronary arteryfrom the opposite sinus? Tex Heart Inst J 2002;29:308-313.
11. Yip H, Chen MC, Wu CJ, et al: Primary angioplasty inacute inferior myocardial infarction with anomalous-originright coronary arteries as infarct-related arteries: Focuson anatomic and clinical features, outcomes, selectionof guiding catheters and management. J Invasive Cardiol2001;13:290-297.
12. Rinaldi RG, Carballido J, Giles R, et al: Right coronaryartery with anomalous origin and slit ostium. Ann ThoracSurg 1994;58:829-832.
13. Di Lello F, Mnuk JF, Flemma RJ, et al: Successful coro-nary reimplantation for anomalous origin of the right coro-nary artery from the left sinus of Valsalva. J Thorac Car-diovasc Surg 1991;102:455-456.
14. Rodefeld MD, Culbertson CB, Rosenfeld HM, et al: Pul-monary artery translocation: A surgical option for complexanomalous coronary artery anatomy. Ann Thorac Surg2001;72:2150-2152.
15. Reul RM, Cooley DA, Hallman GL, et al: Surgical treat-ment of coronary artery anomalies: Report of a 37 1/2-year experience at the Texas Heart Institute. Tex HeartInst J 2002;29:299-307.
16. Alphonso N, Anagnostopoulos PV, Nolke L, et al: Anoma-lous coronary artery from the wrong sinus of Valsalva:A physiologic repair strategy. Ann Thorac Surg 2007;83:1472-1476.
Delayed Surgical Retrieval ofRetained Guidewire FollowingPercutaneous CoronaryIntervention
Amit Modi, M.R.C.S.,Aleksejus Zorinas, M.D,Hunaid A. Vohra, F.R.C.S. (C.Th.),and Markku Kaarne, F.R.C.S. (C.Th)
Wessex Cardiothoracic Centre,Southampton University Hospitals, NHSTrust, Southampton, United Kingdom
ABSTRACT An uncommon complication of percu-taneous coronary intervention (PCI) is entrapmentand/or fracture of the catheter guidewire. This re-port describes “delayed” surgical removal of re-tained guidewire from the ascending aorta follow-ing a PCI. The potential complications and themanagement options are further discussed. doi:10.1111/j.1540-8191.2010.01133.x (J Card Surg2011;26:46-48)
An estimated two million percutaneous coronaryinterventions (PCI) are performed worldwide annu-ally.1 Entrapment and/or fracture with retention of theguidewire is an extremely uncommon complication.2 Ifretained within a coronary artery, this can lead to my-ocardial ischemia, infarction, and lethal arrhythmias.3,4
The presence of a guidewire in the ascending aorta canlead to thrombus formation with subsequent systemicembolization. When confronted with this situation, sur-gical retrieval ± coronary artery bypass grafting may berequired.
CASE REPORT
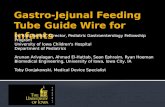
A 77-year-old male presented with unstable anginaand an urgent coronary angiogram revealed significantcalcific stenosis in a tortuous left anterior descend-ing (LAD) artery (Fig. 1) with moderate stenosis atthe origin of obtuse marginal (OM) and posterior de-scending artery (PDA). During PCI, after the first drug-eluting stent (DES) was deployed across the stenoticlesion, the guidewire got entrapped within the DESand fractured. After repeated attempts to remove theguidewire failed, it was decided to attempt to plasterthe floating guidewire to the coronary vessel wall by de-ploying further DES. In total, five DES were deployedinto the LAD (Fig. 2). An intravascular-ultrasound studyat the end of the procedure confirmed well-apposed
Conflict of interest: None.
Address for correspondence: Markku Kaarne, Wessex Cardio-thoracic Centre, Southampton General Hospital, Tremona Road,Southampton, SO16 6YD, UK. Fax: +442380 794526; e-mail:[email protected]

J CARD SURG2011;26:37-68
MODI, ET AL.SURGICAL RETRIEVAL OF RETAINED GUIDEWIRE
47
Figure 1. Left coronary angiogram demonstrating significantstenosis in the left anterior descending artery (arrow).
stents with TIMI 3 flow. The patient remained asymp-tomatic during the procedure with no electrocardio-graphic (ECG) changes. He made an uneventful recov-ery and was discharged home 10 days later with Aspirinand Clopidogrel, 75-mg each daily.
Two weeks later, he presented again with anginaand dyspnea on exertion. An exercise tolerance testresulted in lateral wall ST segment changes. This wasthought to be a consequence of compromised flow inthe first diagonal vessel. Antianginal therapy was op-timized with no improvement in symptoms. He wasreferred to the regional cardiothoracic unit four weeksafter the initial PCI, where a computed tomography(CT) scan performed revealed that the guidewire wascoiled in the ascending aorta with one end located inthe proximal LAD between the first DES and the vesselwall and the other end in the proximal brachiocephalicartery (Fig. 3). A cardiac magnetic resonance imag-ing (MRI) confirmed these findings and demonstratedgood left ventricular ejection fraction and ischemia inthe LAD territory. Hence, surgery was contemplatedfor removal of the guidewire and to surgically revascu-larise the affected myocardium. This was approachedvia a median sternotomy. The left internal mammary
Figure 2. Poststenting noncontrast view revealing the en-trapped guidewire (single long arrow) and multiple stents (mul-tiple short arrows).
Figure 3. CT scan with oblique sagittal slab (left anterior)demonstrating the extent of wire from the aortic root to theinnominate artery.
artery (LIMA) and the long saphenous vein (LSV) wereharvested. Cardiopulmonary bypass (CPB) was estab-lished with aorto-right atrial cannulation (systemic cool-ing 32 ◦C), and the heart was arrested with antegradecold blood cardioplegia with the cross-clamp applied tothe distal ascending aorta. At aortotomy, two separatelengths of the guidewire were discovered. First lengthwas seen to exit the left coronary ostium with the dis-tal end floating in the ascending aorta. Attempts toremove this wire from the coronary by gentle tuckingfailed (Fig. 4). It was firmly plastered to the wall of thecoronary, and we believe any extra force could havedamaged the left coronary system. Thus, it was cutflush with the left coronary ostium. The proximal endof the second length was freely floating in the ascend-ing aorta, and this length was removed while the aorticcross-clamp was released and the CPB flow stoppedmomentarily. A skeletonized LIMA was anastomosedto the mid-LAD, and reversed LSV anastomosed se-quentially to the OM and the PDA. The patient madean uncomplicated recovery and was discharged homeon postoperative day 8 with lifelong Aspirin and Clopi-dogrel for one year. At 12-week follow-up, the patienthad resumed routine activity and was symptom-free.
Figure 4. Intraoperative picture demonstrating tension on theguidewire (short arrows) through the aortotomy.

48 SHIMAMURA, ET AL.EXCISION OF RIGHT CORONARY ARTERY ANEURYSM
J CARD SURG2011;26:37-68
DISCUSSION
Severe calcified stenosis and tortuosity is considereda risk factor for the entrapment of a PCI guidewire ina coronary artery.5 A retained guidewire within a coro-nary vessel may serve as a nidus for endothelial injuryand platelet deposition. If asymptomatic, cardiologistsmay choose to pursue a conservative approach, leav-ing the guidewire in place with regular follow-up, whileothers prefer removing it by percutaneous or surgicalmeans.6
Percutaneous removal of a fractured guidewire maynot be straightforward. Use of Tornus catheter, Mi-crosnare, balloon wedge, and multiple guidewire tech-niques have all been used.7 Implantation of a syntheticcoronary stent graft to isolate a small fragment fromthe blood stream has also been reported.8 We believethat such isolation strategies usually leave parts of wireexposed serving as a nidus for thrombus formation.Retained guidewire fragments in patent coronary ar-teries may cause arterial narrowing despite systemicanticoagulation.9
If percutaneous techniques are unsuccessful andthere is ongoing ischemia, surgery should be con-sidered. In two reported case series, all the symp-tomatic patients following coronary guidewire entrap-ment were sucessfully managed surgically.6-10 Theprinciples of surgery in this scenario are complete re-moval of the guidewire and revascularization of theaffected vessel. In the presented case, the guidewirewas firmly plastered to the wall of the coronary withthe stents and forceful pulling could have damaged theleft coronary system. Thus, it was cut flush with theleft coronary ostium, and the coronary blood flow wasprotected with bypass grafts as proposed in the cur-rent literature.10 Imaging in our patient demonstrateda long piece of wire between the proximal LAD andthe brachiocephalic artery, but at surgery two lengthsof the guidewire with snapped ends in the ascendingaorta proximal to the aortic cross-clamp were discov-ered. We are unable to explain this, but surely eventualembolization of the wire could lead to devastatingconsequences.
Although uncommon, it can be imagined that withthe increasing application of PCI, a retained fracturedguidewire will be seen in an interventional cardiol-ogist’s practice. It is thus imperative that a multi-disciplinary strategy that includes radiologists shouldbe followed, and that cardiac surgeons are familiar withthe different management options for retrieval of re-tained guidewire.
REFERENCES
1. Smith SC Jr, Feldman TE, Hirshfeld JW Jr, et al:ACC/AHA/SCAI 2005 guideline update for percutaneouscoronary intervention: A report of the American Collegeof Cardiology/American Heart Association Task Force onpractice guidelines (Acc/Aha/Scai Writing Committee toupdate the 2001 guidelines for percutaneous coronaryintervention). J Am Coll Cardiol 2006;47:216-235.
2. Steffenino G, Meier NB, Finci L, et al: Acute complica-tions of elective coronary angioplasty: A review of 500consecutive procedures.Br Heart J 1988;59(2):151-158.
3. Giammarco GDi, Turillazzi E, Bolino G, et al: Pushing acatheter remnant into the coronary tree: Complicationof the procedure? Maybe, but sometimes the fragmentneeds to be removed. Int J Cardiol 2009 (Epub; PMID:19339065).
4. Kuruma A, Saitoh H, Ino T, et al: Case of cardiac foreignbodies associated with four types of tachycardias. PacingClin Electrophysiol 1992;15:1215-1224.
5. Breisblatt WM: Inflated balloon entrapped in a calcifiedcoronary stenosis. Cathet Cardiovasc Diagn 1993;29:224-228
6. Alexiou K, Kappert U, Knaut M, et al: Entrapped coronarycatheter remnants and stents: Must they be surgicallyremoved? Tex Heart Inst J 2006;33:139 -142.
7. Cho YH, Park S, Kim JS, et al: Rescuing an entrappedguidewire using a Tornus catheter. Circ J 2007;71:1326-1327.
8. Marti V. Markarian L: Angioplasty guidewire entrapmentaffer stent implantation: Report of two cases and reviewof the literature. Archiv Cardio Mexico 2007;77:54-57.
9. Doorey AJ, Stillabower M: Fractured and retained guide-wire fragment during coronary angioplasty—unforeseenlate sequelae. Cathet Cardiovasc Diagn 1990;20:238-240.
10. Chang TM, Pellegrini D, Ostrovsky A, et al: Surgical man-agement of entrapped percutaneous transluminal coro-nary angioplasty hardware. Tex Heart Inst J 2002;29:329-332.
Excision of Right CoronaryArtery Aneurysm
Junichi Shimamura, M.D.,Hiroshi Kubota, M.D., Ph.D.,Hidehito Endo, M.D.,and Kenichi Sudo, M.D., Ph.D.
Department of Cardiovascular Surgery,School of Medicine, Kyorin University,Tokyo, Japan
ABSTRACT A coronary artery aneurysm (CAA), theetiology and treatment of which are still not fullyunderstood, is uncommonly encountered. A giantCAA is extremely rare and only a limited num-ber of cases have been reported. We report thecase of a 37-year-old female with a giant rightcoronary artery aneurysm that was successfullytreated by surgical excision. doi: 10.1111/j.1540-8191.2010.01130.x (J Card Surg 2011;26:48-51)
Giant coronary artery aneurysm (CAA) is an ex-tremely rare entity with an incidence of only 0.02%.We report a case of CAA that was successfully treated
Conflict of interest: None.
Address for correspondence: Junichi Shimamura, M.D., Departmentof Cardiovascular Surgery, School of Medicine, Kyorin University, 6-20-2 Shinkawa, Mitaka-shi, Tokyo 181-8611 Japan. Fax: 81-422-42-7587;e-mail: [email protected]

J CARD SURG2011;26:37-68
SHIMAMURA, ET AL.EXCISION OF RIGHT CORONARY ARTERY ANEURYSM
49
Figure 1. A multi-detector-row computed tomography(MDCT) showing a giant right coronary artery aneurysm.
by surgical excision. The presentation, diagnosis, andsurgical management of CAA are the subjects of thiscase report.
CASE REPORT
A 37-year-old female patient presented with thechief complaint of palpitation. An echocardiogram re-vealed moderate tricuspid regurgitation (TR) with nor-mal ventricular wall motion. Multi-detector-row com-puted tomography (MDCT, Fig. 1) and magnetic res-onance imaging (MRI) (Fig. 2) revealed an organizedthrombus of the right coronary artery (RCA). Findings
Figure 2. Magnetic resonance image (MRI) showing a gi-ant aneurysm compressing the right atrium with partialenhancement.
Figure 3. Coronary angiography showed a giant coronaryartery aneurysm and the right coronary artery flowing intothe aneurysm. The enhanced lesion was only a part of theaneurysm. There was no arterial flow from the aneurysm.
of the dobutamine stress echocardiography and thal-lium scintigraphy were suggestive of ischemia in theRCA region. The coronary angiography (CAG) revealeda large aneurysm in the mid RCA (Fig. 3). The ostium ofthe distal RCA was totally occluded, with no blood flowfrom the aneurysm. The atrioventricular node arteryand posterior descending artery were well enhancedthrough the collaterals from the left circumflex artery(LCx).
Working through a median sternotomy, cardiopul-monary bypass was established via cannulation ofthe ascending aorta, superior vena cava, and inferiorvena cava, with the insertion of a left ventricular ventfrom the right superior pulmonary vein. The aneurysm,which measured 5 × 7 cm, was excised with the heartbeating under mild hypothermia (32 ◦C). Blood flowfrom mid RCA into the aneurysm was noted; how-ever, no coronary arterial flow was observed from theaneurysm, and the edge of the distal RCA was formedby a blind sac (Fig. 4). The proximal ostium of theaneurysm was ligated. The thrombus was removedand the aneurysmal sac was partially resected, with theremnant being obliterated with running sutures. Evenafter the excision, the tricuspid valve was severely de-formed, with persistent TR; therefore, tricuspid ringannuloplasty was performed (Edwards MC3 annulo-plasty system; Edwards Lifesciences, Irvine, CA, USA).Histopathologic examination of the excised aneurysmrevealed an arterial wall with an organized throm-bus and nonspecific inflammation. The postoperativecourse was uneventful and at present, 16 months af-ter the surgery, the patient remains asymptomatic withaspirin therapy. The postoperative echocardiogram re-vealed good ventricular function without TR, and theMDCT showed the patency of the RCA region with thecollaterals from the LCx (Fig. 5).

50 SHIMAMURA, ET AL.EXCISION OF RIGHT CORONARY ARTERY ANEURYSM
J CARD SURG2011;26:37-68
Figure 4. Intraoperative photograph showing the openedaneurysm of the right coronary artery (RCA) filled with a mas-sive organized thrombus. The RCA is seen flowing into theaneurysm.
COMMENT
CAA is commonly defined as a localized dilatationexceeding the diameter of the adjacent normal arterialsegments by at least 50%.1 CAA has been reportedto occur at an incidence of 0.15% to 4.9% in patientsundergoing CAG and at an incidence of 1.4% in post-mortem examinations.2,3 Markis et al. classified coro-nary artery aneurysms based on the appearance andnumber of coronary arteries involved.3 Our presentcase was categorized as type 3, which is defined asdiffuse ectasia in one vessel only.4 Although a precisedefinition is still lacking, Li et al. termed CAA larger than2 cm as “giant CAA,” and reported that these occur ata frequency of only 0.02%.5 Aneurysms are observedmost commonly in the RCA, and least frequently in theleft main coronary artery.4
CAA can be detected by noninvasive studies, suchas echocardiography, computed tomography (CT), and
Figure 5. Postoperative MDCT showed the patency of theRCA region with the collaterals from the left circumflex artery(LCx).
MRI; however, CAG remains the gold standard, provid-ing precise information about the size and location ofthe aneurysm and also about any coexisting anomalies,such as coronary artery disease.
Giant CAAs are mainly atherosclerotic in origin,and are often associated with poststenotic dilatation.More than 50% of the cases are due to atherosclero-sis. Other causes include Kawasaki disease, trauma,infection, connective tissue diseases, dissection, con-genital malformations, and angioplasty.1 In our presentcase, the patient did not have any history of traumaor angioplasty. There was no evidence of infectiousdisease or connective tissue disease. There was nohistory suggestive of Kawasaki disease during the pa-tient’s childhood, besides the aneurysm was too distalto be considered as being associated with Kawasakidisease. Judging from the clinical course and charac-teristics of the thrombus, the aneurysm was most likelya congenital aneurysm in our patient, although the pre-cise etiology could not be determined.
CAAs are asymptomatic in most cases; however,these patients may present with angina pectoris, my-ocardial infarction (MI), sudden death, thrombus for-mation, rupture, cardiac tamponade, compression ofsurrounding structures, and congestive heart failure.Giant CAAs may also present as mediastinal or intra-cardiac masses or with superior vena cava syndrome,in addition to the symptoms outlined above.2
Due to the rare occurrence of the condition, thereare still no uniform guidelines for the managementof giant CAAs.1,2 Because of its effectiveness in pre-venting thrombus formation, antiplatelet or anticoagu-lant therapy is administered as an effective therapeu-tic measure. Some reports suggest that angiotensintype 1-receptor antagonists and statins are effective forinhibiting the destruction of the tunica media that ischaracteristic in CAA.6 Because pharmacotherapy mayprevent only potential complications of the aneurysm,the importance of the aneurysm removal itself can-not be overemphasized. The procedures employedvary from angioplasty with implantation of a stent toaneurysm resection with or without coronary arterybypass grafting (CABG).1 Cases with MI or rupture areabsolute indications for emergency surgery, and sur-gical repair must be considered for aneurysms havinga diameter larger than three times the normal vesseldiameter, as these are associated with a high risk ofrupture.7 Surgical repair should be planned accordingto the location, severity of the coronary artery stenosis,and other relevant clinical factors. The overall five-yearsurvival of CAA is reported to be 71%.1
In our present case, the patient was a youngwoman without coronary risk factors. There were well-developed collaterals and the degree of ischemia wasmild. If we performed CABG, the collaterals wouldregress; and judging from the organized appearanceof the thrombus, it was thought that it had formedover a long time course. The patient may even havedelivered her child with this aneurysm. Therefore, wedetermined that we may expect a better prognosiswithout reconstruction of the RCA. Giant CAA is ararely encountered condition with varied clinical pre-sentation. Since therapeutic management is yet to bestandardized, the treatment of giant CAAs, including

J CARD SURG2011;26:37-68
ELHENAWY, ET AL.ANEURYSM AFTER TRANSAPICAL VALVE
51
surgical repair, must be selected depending on individ-ual case presentations.
REFERENCES
1. Pahlavan S, Niroomand F: Coronary artery aneurysm: Areview. Clin Cardiol 2006;29:439-443.
2. Syed M, Lesch M: Coronary artery aneurysm: A review.Prog Cardiovasc Dis 1997;40:77-84.
3. Markis JE, Joffe CD, Cohn PF: Clinical significance ofcoronary artery ectasia. Am J Cardiol 1976;37:217-222.
4. Daoud A, Pankin D, Tulgan H, et al: Aneurysms of thecoronary artery. Report of ten cases and review of litera-ture. Am J Cardiol 1963;11:228-237.
5. Dianyuan L, Wu Q, Sun L, et al: Surgical treatment ofgiant coronary artery aneurysm. J Thorac Cardiovasc Surg2005;130:817-21.
6. Nichols L, Lagana S, Parwani A: Coronary arteryaneurysm: A review and hypothesis regarding etiology.Arch Pathol Lab Med 2008;132:823-8.
7. Biglioli P, Alamanni F, Antona C, et al: Aneurysms ofthe coronary arteries: one case report. Thorac CardiovascSurg 1988;36:239-40.
Persistent Left Ventricular FalseAneurysm after TransapicalInsertion of an Aortic Valve
Abdelsalam Elhenawy, M.D.,Rodolfo Rocha, M.D.,Christopher M. Feindel, M.D., andStephanie J. Brister, M.D.
Division of Cardiac Surgery, Toronto GeneralHospital, University Health Network,Toronto, Ontario, Canada
ABSTRACT Transcatheter aortic valve implantation(TAVI), via either a femoral or apical approach,has been developed as an alternative to conven-tional aortic valve replacement for patients whoseoperative risks are considered too high for con-ventional surgery. Complications with these rela-tively new procedures are being reported with in-creasing frequency. We report a case of transapi-cal TAVI, in which the patient developed a falseaneurysm at the apex of the left ventricle as a com-plication of the procedure. doi: 10.1111/j.1540-8191.2010.01149.x (J Card Surg 2011;26:51-53)
Conflict of interest: The authors have no disclosures or conflicts ofinterest. The paper has been accepted for presentation at the CanadianCardiovascular Congress, Montreal, Canada (October 23 to 27, 2010).
Source of funding: Funding support for this paper has been frominternal divisional resources.
REB Approval: As per our hospital REB, verbal consent for publicationwas obtained from the chart and recorded in the office chart.
Address for correspondence: Stephanie J. Brister, Division of Car-diac Surgery, Toronto General Hospital, Toronto 4N-472, 200 Eliz-abeth St., Ontario, Canada M5G 2C4. Fax: 416 340 4946; e-mail:[email protected]
Untreated symptomatic aortic stenosis (AS) carriesa poor prognosis with a one- and five-year survivalof 60% and 32%, respectively.1 Aortic valve replace-ment (AVR) is the only effective treatment that alle-viates symptoms and improves survival for patients.Estimated operative mortality for patients with no co-morbidities is low (4%),2 but it does increase substan-tially with increasing age, poor left ventricular dysfunc-tion, or if other comorbidities exist. One-third of thesepatients are not referred for surgery because they areconsidered to be at too high risk.3 For those patients,transcatheter aortic valve implantation (TAVI), via eithera femoral or an apical approach, is an alternative.4
CASE REPORT
A 66-year-old male presented with increasing short-ness of breath as a result of AS (New York Heart Asso-ciation [NYHA] Class III symptoms). Transesophagealechocardiogram (TEE) showed a calcified trileaflet aor-tic valve (AV) peak gradient of 119 mmHg, mean gra-dient of 69 mmHg, an AV area of 0.6 cm2, and an AVvelocity of 5.45 m/s. There was evidence of extensiveaortic wall atheroma and calcification on both echocar-diogram and CT scan of the chest (Fig. 1). Cardiaccatheterization confirmed the presence of severe ASand also demonstrated a 70% stenosis of the circum-flex artery. Other comorbidities included symptomaticcerebral vascular disease (two transient ischemic at-tacks [TIA] within the last six months), peripheral vas-cular disease with claudication, emphysema, diabetes,and hypertension. Because of his calcific aorta andother comorbidities, the patient was deemed to berisky for conventional AVR and was scheduled for atransapical TAVI via a left mini-thoracotomy. A 26-mmEdwards Sapien transcatheter heart valve (EdwardsLifesciences Inc., Irvine, CA, USA) was introducedthrough a 24-French catheter that was inserted throughthe apex of the left ventricle (LV) and passed across theAV. At completion of the deployment, the ventriculo-tomy was closed with teflon-pledgeted 2–0 prolene su-tures. Note was made that the tissues were fatty andfriable, and that part of the muscle had torn. The cir-cumflex stenosis was not treated before or during theprocedure. Because of his history of TIAs, the patientwas started on aspirin and plavix, postoperatively.
Twelve days following his operation, the patientdeveloped hemodynamic instability. Echocardiogramshowed a large pericardial effusion with evidence ofright ventricular compromise. A large bloody effusionwas drained through a subxiphoid approach. A post-operative echocardiogram two days later revealed a22 × 25 mm left ventricular echo-lucent area at the LVapex that was communicating with the cavity (Fig. 2).This was thought to be a pseudoaneurysm related tothe ventriculotomy, through which the valve was intro-duced at the initial operation. Subsequent echocardio-grams showed the aneurysm to be increasing in sizenecessitating reparative surgery.
On post-operative day 21, a repair of the apical falseaneurysm of the LV was performed. An epiaortic-echoprobe was utilized to identify an atheroma-free areaon the ascending aorta suitable for cannulation. The

52 ELHENAWY, ET AL.ANEURYSM AFTER TRANSAPICAL VALVE
J CARD SURG2011;26:37-68
Figure 1. CT of chest showing calcification in the lateral and posterior wall of aorta, which would prevent safe cross-clamping ofthe aorta.
cava were cannulated directly and cardiopulmonary by-pass (CPB) was initiated. Decompression of the thick-walled LV appeared to be adequate. No left ventricularvent was utilized. After lysis of the adhesions encasingthe heart, the apex was exposed. A tear was seen atthe lateral edge of the ventriculotomy, through whichthe percutaneous valve had been placed. Two 2–0 pro-lene pledgeted sutures were then placed through thetear and ventricle. Several additional 3–0 prolene su-tures with autologous pericardial pledgets were alsoused. Intraoperative echocardiogram did not visualizeflow from the left ventricular cavity into the pseudoa-
Figure 2. Two-dimensional echocardiogram showing thefalse aneurysm at the apex of the LV.
neurysm. On the seventh day after the last surgery(the 28th POD) an echocardiogram again visualized thepseudoaneurysmal space that now measured 21 mm x11 mm with bidirectional flow into an echo-lucent areaat the left ventriclular apex. The patient was broughtback to the operating room (OR) to repair the recur-rent false aneurysm, placed on CPB in a similar fash-ion, cooled to 20 ◦C, and the circulation was stopped.With complete decompression of the heart, the prob-lem could be identified. In the distal lateral anterior wall,
Figure 3. Intraoperative photo demonstrating the 4-mm neckof the false aneurysm at the apex of the LV .

J CARD SURG2011;26:37-68
ELHENAWY, ET AL.ANEURYSM AFTER TRANSAPICAL VALVE
53
Figure 4. Pericardial patch repair of the false aneurysm at theapex of the LV.
the pledgets were taken down. There was a small, 3- to4-mm hole penetrating into the LV (Fig. 3). There wasa pseudoaneurysm cavity that had not been previouslyappreciated, which had distended the fat in the epi-cardium of the LV. The original pledgeted sutures fromthe introduction of the valve and from the previous re-pair were in the fat and epicardium. After evaluation ofthe problem, due to the thick-walled nature of the LV,it was concluded that the sutures could not be placedadequately through the LV to close the hole. In addi-tion, any sutures that were thick enough to go throughboth walls of the LV would come precariously close tothe left anterior descending coronary artery. Resectionof the pseudoaneurysmal sac was done. A pericardialpatch was utilized to close the defect (Fig. 4). The intra-operative TEE post-CPB showed no evidence of resid-ual LV aneurysm. Echocardiogram performed on POD35 confirmed the absence of bidirectional flow in theleft ventricular apex (Fig. 5).
COMMENT
The transapical approach for TAVI is a new andpromising alternative for patients who are not candi-dates for conventional AVR. Complications that have
Figure 5. Postoperative two-dimensional echocardiogramshowing no flow outside of the left ventricular cavity.
been reported include bleeding with and without tam-ponade, stroke, mitral and aortic insufficiency, andseptal hematoma. False aneurysms of the LV havebeen reported but infrequently.5,6 Friable tissue andpoor visibility may predispose this patient populationto the development of this complication. As with ourpatient, the indications for surgery are increasing sizewith an impending rupture. Surgical repair of a falseaneurysm post-TAVI has met with mixed success.Wong et al.6 reported on four patients (6.6% of theirseries). Two patients were treated surgically with onedeath. Two were treated medically and currently arestable. Al-Attar et al.5 reported one patient with anLV false aneurysm post-TAVI who was successfullytreated with surgical repair utilizing CPB. In our case,the extensive calcification of the lateral and posterioraspect of the aorta precluded cross-clamping for con-ventional AVR but not for institution of CPB. Our casealso clearly illustrates the need for decompression ofthe LV during the repair. This was obtained with circu-latory arrest. Decompression facilitates visualization ofthe problem and allows closure without tension. Theuse of the pericardial patch also facilitated the latter.Use of a vent at the first attempt at repair may haveenhanced decompression of the heart, but would cer-tainly have increased the risk of air embolism giventhat the LV was open and the heart was beating. Allauthors agree at operation an aggressive approach isrequired. Decompression and excellent visualization isrequired to ensure that the problem is clearly identifiedand dealt with the first time.
REFERENCES
1. Varadarajan P, Kapoor N, Bansal RC, et al: Clinical pro-file and natural history of 453 nonsurgically managedpatients with severe aortic stenosis. Ann Thorac Surg2006;82:2111-2115.
2. Edwards FH, Peterson ED, Coombs LP, et al: Prediction ofoperative mortality after valve replacement surgery. J AmColl Cardiol 2001;37:885-892.
3. Iung B, Baron G Butchart EG, et al: A prospective sur-vey of patients with valvular heart disease in Europe: TheEuro Heart Survey on Valvular Heart Disease. Eur Heart J2003;24:1231-1243.
4. Ye J, Cheung A, Lichtenstein SV, et al: Six-month out-come of transapical transcatheter aortic valve implantationin the initial seven patients. Eur J Cardiothorac Surg. 2007;31(1):16-21.
5. Al-Attar N, Ghodbane W, Raffoul R, et al: Unexpected com-plications of transapical valve implantation. Ann ThoracSurg 2009;88:90-94.
6. Wong DR, Ye J, Cheung A, et al: Technical considerationsto avoid pitfalls during transapical aortic valve implantation.J Thorac Cardiovasc Surg 2010;140(1):196-202.

54 RABKIN, ET AL.IATROGENIC VERTEBRAL ARTERY DISSECTION
J CARD SURG2011;26:37-68
Vertebral Artery DissectionAfter Iatrogenic CervicalSubcutaneous Emphysema
David G. Rabkin, M.D.,Peyman Benharash, M.D., andRichard J. Shemin, M.D.
The Division of Cardiothoracic Surgery, LosAngeles Medical Center, University ofCalifornia, Los Angeles, California
ABSTRACT We report a case of spontaneous ver-tebral artery dissection (VAD) in a patient whodeveloped extensive subcutaneous emphysemafollowing the removal of a chest tube after a car-diac transplant. The pathophysiology and man-agement of this uncommon complication arereviewed. Although vertebral and carotid arterydissections are unusual events occurring in 2.5to 3 per 100,000 people, they are increasingly ac-knowledged to be important causes of stroke inthe young and middle-aged adult population ac-counting for up to 25% of such cases. VADs areassociated with a variety of minor traumatic mech-anisms including painting a ceiling, yoga, chiro-practic manipulation of the spine, and driving.These events cause injury to the vessel wall eitherby shearing forces secondary to rotational injuriesor direct trauma to the vessel wall on bony promi-nences, especially the transverse processes of thecervical vertebrae. We present a case of a patientwith documented previously normal vertebral ar-terial anatomy who developed a VAD after medi-astinal tube removal resulted in subcutaneous em-physema tracking through fascial planes into hisneck. doi: 10.1111/j.1540-8191.2010.01150.x (JCard Surg 2011;26:54-56)
CASE REPORT
A 42-year-old man was successfully bridged to hearttransplantation for idiopathic dilated cardiomyopathyfollowing two months on a biventricular device. Aspart of his pretransplant work-up he underwent a du-plex carotid ultrasound exam, which demonstratednormal vertebral arterial anatomy. His post-transplantcourse was uneventful until two mediastinal tubeswere removed on the fourth postoperative day re-sulting in bilateral pneumothoraces. Despite promptbilateral chest-tube placement he developed signifi-cant subcutaneous emphysema across his precordium
Conflict of interest: None of the authors have any potential conflictof interest connected to this article.
Address for correspondence: David G. Rabkin, M.D., University ofWashington Medical Center, 1959 NE Pacific St Room AA115, Box356310, Seattle, WA 98195. Fax: 206-543-0325; e-mail: [email protected]
tracking into his neck. Subsequent development ofbilateral upper extremity swelling prompted an ultra-sound of his venous anatomy, which was suboptimaldue to interference from the subcutaneous air. Conse-quently, a magnetic resonance angiogram (MRA) wasordered to evaluate the venous anatomy. This studydemonstrated significant compression of the internaljugular veins bilaterally by air tracking along the super-ficial and deep fascial planes. The arterial phase of theexam was notable for a dissection of the left-sided,dominant vertebral artery with a long-segment 50% to60% narrowing involving the entire foraminal coursefrom C2 to C6 (Figs. 1 and 2). The remainder of thecervical arterial anatomy was unremarkable and therewas no evidence of intracerebral hemorrhage. The pa-tient denied symptoms, specifically head or neck pain,nausea, vomiting, or unbalanced gait. His neurologicalexam was normal and no bruit was present. Trans-cranial Doppler examination ruled out microemboli andafter consultation with neurology and neurosurgery hewas placed on antiplatelet therapy. He was dischargedwithout further events on postoperative day numbertwelve with neurology follow-up and recommenda-tions to repeat an MRA in three months. Although hehas refused repeat MRA, one year later he remainssymptom free.
COMMENT
The inciting event in VAD is an expanding hematomain the wall of the vessel, typically localized to the me-dial layer. The source of the hemorrhage is either anintimal tear with blood dissecting into the media, or pri-mary hemorrhage of the vaso vasorum in the media ofthe artery. The sequelae of the dissection depend onits location and extent. The classic picture is a relativelyyoung person presenting with a severe unilateral pos-terior headache and neurologic signs consistent withischemia of the lateral medulla.3 Neck pain is also afrequent presenting symptom. Female sex may be arisk factor with up to 72% of reported cases occur-ring in women.3 In up to 80% of patients some typeof neck manipulation, rapid torsion, or minor trauma isreported.4
The key to establishing the diagnosis is suspectingthe disease. Computed tomography or MRA are themost useful studies to make the diagnosis and revealluminal stenosis that may appear irregular, elongatedor tapered; associated aneurysmal dilatation may beseen.3 With experienced operators duplex scanningmay also be useful in diagnosing VAD.
The goal of any treatment is to prevent cerebrovas-cular accidents from occurring. Stroke may result fromhypoperfusion secondary to a narrowed or completelyoccluded vessel, or from emboli that form in areas ofinjured endothelium. Therapies aimed at reducing therisk of stroke include anticoagulants and antiplateletagents, surgical resection of intramural hematoma,thrombectomy or ligation of the vessel proximal tothe site of dissection. While it might seem counter-intuitive to anticoagulate patients who just hemor-rhaged into the arterial wall there have been no reportsof patients subsequently deteriorating.5 However, be-cause of the small risk of subarachnoid hemorrhage,

J CARD SURG2011;26:37-68
RABKIN, ET AL.IATROGENIC VERTEBRAL ARTERY DISSECTION
55
Figure 1. MRA coronal image demonstrating long-segment narrowing of the dominant, left-sided, vertebral artery (arrow).
particularly in the case of intracranial VAD, this di-agnosis must be excluded prior to anticoagulation.Surgical therapy is reserved for patients who haverecurrent or progressive ischemia in spite of anticoag-ulation and who have focal, accessible lesions. Thereare no randomized trials to support the superiority ofWarfarin anticoagulation versus anti-platelet therapy.Re-imaging is recommended in three to six months.After the artery appears normal on imaging studiesthe anticoagulation or anti-platelet therapy can be dis-continued. The incidence of recurrent VAD is approxi-mately 5%.6
Because of the asymptomatic nature of the pre-sented event it is impossible to exclude the possi-bility that the VAD occurred spontaneously at somepoint before the development of subcutaneous em-physema and after this patient’s preoperative duplexcarotid Doppler study demonstrating normal verte-bral anatomy. However, truly spontaneous dissectionsof the vertebral artery are rare. Predisposing factors
Figure 2. MRA axial image demonstrating intimal flap of the left vertebral artery (arrow).
include hypertension, which has been noted in as manyas 48% of patients, hormonal changes and oral contra-ceptive use and intrinsic vascular abnormalities suchas fibromuscular dysplasia and cystic medial necrosis,none of which were present in our patient.7 In addition,when spontaneous VADs occur, they tend to do so inthe tortuous distal extracranial segment (segment IIIof the verterbral artery), and may extend into the in-tracranial portion of segment IV.8 The dissection in thiscase occurred entirely within the transverse foraminaof C5/C6 to C2 which is segment II.
While VAD has been reported after muscle relax-ation and cervical hyperextension during intubation thatpatient had predisposing anatomy in the form of ahigh-standing tip of the odontoid process,9 which lat-eral cervical roentgenogram excluded in our patient.We believe the etiology of this event to be subcuta-neous air (which exerted enough pressure between thefascial planes to result in clinically significant compres-sion of the venous anatomy) causing sufficient trauma

56 YU, ET AL.INTRAVENOUS LEIOMYOMATOSIS WITH INTRACARDIAC EXTENSION
J CARD SURG2011;26:37-68
to the vertebral artery intima to provide the mechanismfor dissection.
REFERENCES
1. Schievink WI: Spontaneous dissection of the carotid andvertebral arteries. N Engl J Med 2001;344(12):898-906.
2. Gallerani M, Schena F, Fellin R, et al: Idiopathic dissectionof vertebral artery. Am J Emerg Med 2001;19(2):165-166.
3. Caplan LR, Tettenborn B: Vertebrobasilar occlusive dis-ease: Review of selected aspects. Cerebrovasc Dis 1992;2(5):256-265.
4. Hart RG: Veterbral artery dissection. Neurology 1988;38:987-989.
5. Sturzenegger M: Spontaneous internal carotid artery dis-section: Early diagnosis and management in 44 patients.J Neurol 1995;242:231-238.
6. Kim YK, Schulman S: Cervical artery dissection: Pathol-ogy, epidemiology and management. Thromb Res 2009;123(6):810-821.
7. Stahmer SA, Raps EC: Carotid and vertebral artery dissec-tions. Emerg Med Clin North Am 1997;15(3):677-698.
8. Lang E, Afilalo M: Dissection, vertebral artery. emedicine:http://emedicine.medscape.com/article/761451-overview
9. Zotter H, Zenz W, Gallisti S, et al: Stroke following appen-dectomy under general anesthesia in a patient with basilarimpression. Acta Anesth Scand 2001;44(10):1271-1272.
Intravenous Leiomyomatosiswith Intracardiac Extension: AReport of Two Cases
Lei Yu, M.D.,∗ Enyi Shi, M.D., Ph.D.,∗Tianxiang Gu, M.D., Ph.D.,Zongyi Xiu, M.D., Ph.D., Qin Fang, M.D.,and Chun Wang, M.D.
Department of Cardiac Surgery, the FirstAffiliated Hospital, China Medical University,Shenyang, P.R. China
ABSTRACT Uterine leiomyoma is a common diseasein women; however, intravenous leiomyomatosiswith intracaval and intracardiac complications isa rare condition. The initial presentation is de-pendent upon the severity of the intracardiac in-volvement. In this report, we describe two womenwith leiomyomatosis originating from the uterusand extending into the inferior vena cava to theright ventricle that was successfully resected us-ing a two-stage approach. doi: 10.1111/j.1540-8191.2010.01148.x (J Card Surg 2011;26:56-60)
Conflict of interest: None.∗Drs Lei Yu and Enyi Shi contributed equally to this work.
Address for correspondence: Tianxiang Gu, M.D., Ph.D., Departmentof Cardiac Surgery, the First Affiliated Hospital, China Medical Uni-versity, Shenyang, P.R.China 110001. Fax: 86-24-83283468; e-mail:[email protected]
Intravenous leiomyomatosis (IVL) is a rare benignsmooth muscle tumor arising from the uterine orpelvic vein and rarely to the right ventricle. Patientsmay remain asymptomatic until intracardiac growthleads to cardiac insufficiency, pulmonary embolism, oreven sudden cardiac death. In this report, we describetwo patients who underwent successful removal ofan IVL extending deep into the right ventricle usinga two-stage approach and an on-pump beating-hearttechnique.
CASE REPORT
Patient 1
A 52-year-old woman was admitted to our depart-ment with a 10-year history of shortness of breath anda three-month history of palpitation. On physical exam-ination, a grade 3/6 systolic murmur was heard at leftsternal edge. Echocardiography showed an oscillatingechogenic mass in the right atrium and right ventricleoriginating from the inferior vena cava (IVC) (Figs. 1Aand B). Ejection fraction was 60%. Computed tomog-raphy (CT) scan showed a hypodense mass emergingfrom the right iliac vein, which had invaded the IVC(Fig. 2A). MRI showed abnormal signals in the rightinternal iliac vein, common iliac vein, IVC, right atrium,and right ventricle (Fig. 2B). Abdominal ultrasound
Figure 1. (A, B) View of cardiac ultrasonogram, a large tumor(arrow) coming from the inferior vena cava (IVC) to fill theright atrium (RA) and enter right ventricle (RV) in systolicphase.

J CARD SURG2011;26:37-68
YU, ET AL.INTRAVENOUS LEIOMYOMATOSIS WITH INTRACARDIAC EXTENSION
57
Figure 2. (A) CT scanning shows a hypodense mass (arrow) emerging from the right iliac vein (RIV) to the inferior vena cava (IVC)and then to the right atrium (RA). (B) MRI demonstrates abnormal signal (arrow) from iliac vein extending to the RA.
Figure 3. Illustration of the surgical excision of the tumor inpatient 1 using CPB. The intracardiac mass was pushed intothe IVC and pulled out from the IVC.
Figure 4. (A) Gross pathologic specimen of IVL measuring30.0 cm in length of the first-stage surgery. (B) Histologicalexamination of the intracaval and intracardiac tumor showsproliferating smooth muscle cells with no abnormal mitoticactivity (hematoxylin-eosin [H&E], ×100).

58 YU, ET AL.INTRAVENOUS LEIOMYOMATOSIS WITH INTRACARDIAC EXTENSION
J CARD SURG2011;26:37-68
Figure 5. (A) A 2D echocardiogram revealing a mobile-solid mass (arrow) extending into right atrium (RA) and ventricle (RV). (B)Coronal view on abdominal and pelvic CT scans. A solid-cylindrical mass (arrow) projecting into blood vessel lumens, suggestingan intravenous-continuous lesion. (C) Histopathologic evaluation: proliferating, smooth muscle fibers, with hyperplastic vasculartissue (H&E, ×400)
revealed multiple low-echogenic mass lesions in uter-ine muscle. From these findings, the patient was diag-nosed as IVL of the uterus with intracaval and cardiacextension.
The operation was carried out using the on-pumpbeating-heart technique. The heart and IVC were ex-posed through midline incision of the chest and ab-domen. Cardiopulmonary bypass (CPB) was institutedfrom the superior vena cava and bilateral femoral veinsto the ascending aorta, as shown in Figure 3. A rightatriotomy was performed and a pump sucker was usedto rapidly empty the right atrium. A large elastic tumorwas found occupying most of the right atrium and ex-tending into the IVC. The intracardiac mass was free-floating without invasion of the myocardium. A 10-cm-longitudinal venotomy was made in the infrarenal venacava. The tumor was cut off at the level of infrarenalvein. The intracardiac mass was pushed into the IVCand pulled out from the IVC. The IVC was repaired bymeans of continuous suture with 6–0 prolene sutureline. The total time for CPB was 28 min. Two units of
packed red blood cells and four units of fresh frozenplasma were transfused during the operation.
Pathologic examination of the intracaval and intracar-diac portions of the tumor revealed a cylindrical massmeasuring approximately 30.0 cm in length and 1.0 cmto 2.0 cm in diameter (Fig. 4A). Histologic examinationshowed the tumor consisted of proliferating smoothmuscle fibers without abnormal mitotic activity, con-firming the diagnosis of intravenous leiomyomatosis(Fig. 4B).
Eight weeks after the cardiac intervention, thesecond-stage operation was performed via laparotomy.Total abdominal hysterectomy with bilateral salpingo-oophorectomy was performed. The tumor was foundoriginating from the uterine vein and continuing into theright internal iliac vein. The rest of the tumor was com-pletely excised. The length of the tumor was 15.0 cm.Pathologic diagnosis was the same as the first stageof the operation.
The postoperative course was uneventful and thepatient was discharged seven days after the second

J CARD SURG2011;26:37-68
YU, ET AL.INTRAVENOUS LEIOMYOMATOSIS WITH INTRACARDIAC EXTENSION
59
Figure 6. Illustration of the surgical excision of the tumor inpatient 2 using CPB. The intracardiac mass was pulled outfrom the right atrium.
operation. Follow-up monitoring has been undertakenwith CT and echocardiography for two years withoutevidence of recurrence.
Patient 2
A 49-year-old woman was admitted to our de-partment with a seven-month history of palpitation.Echocardiogram revealed a long linear mass arisingfrom the IVC extending into the right atrium and rightventricle (Fig. 5A). CT demonstrated an intraluminal-filling defect within the right common iliac vein ex-tending into the IVC, right atrium, and right ventricle(Fig. 5B). Abdominal ultrasound revealed multiple low-echogenic mass lesions in the uterine muscle. Fromthese findings, the patient was diagnosed as IVL ofthe uterus with intracaval and cardiac extension.
CPB was instituted as shown in Figure 6. A longitu-dinal venotomy 2 cm in length was made in the rightinternal iliac vein. The tumor was excised at the rightinternal iliac vein. The intracardiac mass was pulled outfrom the right atrium (Fig. 7A). The total time for CPBwas 14 min. Two units of packed red blood cells andtwo units of fresh frozen plasma were transfused dur-ing the operation. Pathologic examination of the tumorrevealed a cylindrical mass measuring approximately45.0 cm in length and 1.0 cm to 3.0 cm in diam-eter (Fig. 7B). Histology demonstrated a leiomyoma(Fig. 5C).
Figure 7. (A) Operative view. The tumor was pulled out fromthe right atrium. (B) A cylindrical mass, 45.0 cm in length withvarying widths in the stage 1.
Seven weeks later, the second-stage operation wasperformed via laparotomy. Total abdominal hysterec-tomy with bilateral salpingo-oophorectomy was per-formed. The length of the tumor was 7.0 cm. Thepostoperative course was uneventful, and the patientwas discharged seven days after the second operation.During the six-month follow-up, she was asymptomaticand there was no evidence of tumor recurrence withCT scan.
DISCUSSION
IVL is a rare smooth muscle cell tumor that arisesfrom the uterus and grows within veins. Intracardiacleiomyomatosis (ICL) is an insidious process and byextending into the right heart can cause heart failure,pulmonary embolization, or sudden death. CT scan andMRI provide sufficient information about the origin, lo-cation, extension, and size of the tumor. The treatmentof IVL is surgical removal of the tumor. One- or two-stage operations have been reported in the literature.In most cases, the surgical treatments were carried outunder hypothermia and circulatory-arrest techniques toavoid venous wall injury. The other surgical strategyconsists of a combined abdominal and thoracic proce-dure involving CPB, with circulatory arrest and deephypothermia. IVL extending to the caval vein and heartis free-floating without invasion into the venous andatrium wall, which indicates that the circulatory-arresttechnique may not be necessary in many cases. In ourtwo cases, we performed the first-stage surgery usingthe on-pump beating-heart technique.
ICL can cause severe heart failure, pulmonary em-bolization, or sudden death due to obstruction of thetricuspid valve. Therefore, urgent removal of the tumor

60 LONGPAPILLARY MUSCLE RUPTURE
J CARD SURG2011;26:37-68
is essential. Surgery is the treatment of choice andcomplete removal of the tumor is mandatory becauserecurrences are frequent, despite the benign nature ofthis neoplasm. Since the tumor does not grow into orattach itself to vena cava walls or cardiac chambers,total excision is possible. In an extensive search byCastelli et al., a total of 100 cases with cardiac involve-ment have been reported in the literature.1 Differentsurgical techniques have been utilized using either asingle- or double-staged operation. The two-stage op-eration involves removal of intrathoracic and abdomi-nal/pelvic components in two separate operations. Re-cently, a single-staged procedure using CPB with orwithout circulatory arrest has been employed for totalexcision of the tumor. Harris and coworkers reportedthe first single-stage procedure for total excision of thetumor without need of CPB or circulatory arrest.2 In thecurrent cases, we used CPB by on-pump beating-hearttechnique for the first stage of the operation and re-moved the remaining tumor in the second stage with-out CPB. We believe that the two-stage surgical re-moval of an IVL with intracardiac extension using theon-pump beating-heart technique is much safer andeasier than a single-stage operation. No complicationswere observed in the interval between the first andsecond procedures. The second operation enabled usto completely remove the tumor in the right internaliliac vein without difficulty.
Venous cannulation for CPB may be challenging. Webelieve that superior vena cava cannulation and cannu-lation of bilateral femoral veins should be performed,which assures adequate venous drainage for CPB. Inour cases, the venous drainage was adequate and CPBwas stable during the operation.
Recurrence has been documented in some cases.3
Therefore, all veins entering into the inferior caval veinoriginating from the uterus should be examined toavoid venous wall injury during an operation and tu-mor recurrence. This type of tumor grows very slowly,and the interval of regrowth after a subtotal or totalhysterectomy has been reported up to ten years.4 In-travenous leiomyomatosis seems to be hormone de-pendent, as in the case of uterine leiomyomas. Bilateraloophorectomy is essential because the tumor is estro-gen dependent.5 For incomplete resection or recur-rence of the tumor, antiestrogens such as tamoxifenmay be useful, but the efficacy is still controversial.6
Both patients underwent total-abdominal hysterec-tomy with bilateral salpingo-oophorectomy withoutpostoperative treatment with GnRH agonist. Our twopatients have shown no evidence of tumor recurrenceafter two years and six months, respectively.
REFERENCES
1. Castelli P, Caronno R, Piffaretti G, et al: Intravenous uter-ine leiomyomatosis with right heart extension: Successfultwo-stage surgical removal. Ann Vasc Surg 2006;20:405-407.
2. Harris LM, Karakousis CP: Intravenous leiomyomatosiswith cardiac extension: Tumor thrombectomy through anabdominal approach. J Vasc Surg 2000;31:1046-1051.
3. Shida T, Yoshimura M, Chihara H, et al: Intravenous
leiomatosis of the pelvis with reextension into the heart.Ann Thorac Surg 1986;42:104-106.
4. Cooper MM, Guillem J, Dalton J, et al: Recurrent intra-venous leiomyomatosis with cardiac extension. Ann Tho-rac Surg 1992;53:139-141.
5. Mitsuhashi A, Nagai Y, Sugita M, et al: GnRH agonist for in-travenous leiomyomatosis with cardiac extension. A casereport. J Reprod Med 1999;44:883-886.
6. Nam MS, Jeon MJ, Kim YT, et al: Pelvic leiomyomatosiswith intracaval and intracardiac extension: A case reportand review of the literature. Gynecol Oncol 2003;89:175-180.
Papillary Muscle Rupture: AnUnusual Complication ofChordal Sparing Mitral ValveReplacement
Michael A. Long, M.Med
Department of Cardiothoracic Surgery,Faculty of Health Sciences, Free StateUniversity, Bloemfontein, South Africa
ABSTRACT An adult patient with advancedrheumatic heart disease undergoing chordal spar-ing mitral valve replacement as well as aortic valvereplacement is presented. The patient developedan unusual complication of an infarction of theretained head of the anterolateral papillary mus-cle with subsequent spontaneous rupture 72-hourspostoperatively. The ruptured head of the papil-lary muscle was successfully resected via an aorto-tomy through the aortic valve prosthesis. The pa-tient made an uneventful recovery. Care to avoidexcessive tension on the preserved chordae dur-ing mitral valve replacement, especially in the set-ting of chronic rheumatic carditis, is stressed. doi:10.1111/j.1540-8191.2010.01157.x (J Card Surg2011;26:60-63)
Preservation of continuity of the mitral annulus withthat of the subvalvar apparatus during mitral valve re-placement (MVR) is of vital importance for the main-tenance of normal left ventricular (LV) geometry andpreservation of LV function postoperatively. A meta-analysis of all clinical studies comparing MVR with andwithout chordal sparing showed a significant decreasein operative mortality in the chordal sparing group.1 Sig-nificant improvement in early and late postoperative LV
Address for correspondence: Michael A. Long, M.Med, Department ofCardiothoracic Surgery, Faculty of Health Sciences, University of theFree State, PO Box 339 (Internal box G32), Bloemfontein 9300, SouthAfrica. Fax: +27-51-444-3440; e-mail: [email protected]

J CARD SURG2011;26:37-68
LONGPAPILLARY MUSCLE RUPTURE
61
function and volumes has also been demonstrated inthose patients undergoing MVR with retention of sub-valvar apparatus.2 An advantage has also been provenin patients undergoing bileaflet sparing MVR as op-posed to patients in whom only the posterior leafletchordal attachments were retained.3
In spite of the proven benefit of bileaflet chordalpreservation in MVR, many surgeons continue to re-tain only the posterior leaflet chordae because ofthe greater technical complexity involved in bileafletchordal preservation, resulting in longer operatingtimes. Additional concerns with bileaflet chordal pre-serving MVR are the potential for interference withthe mechanical discs of the prosthesis by subvalvarstructures, the possibility of undersizing of the mitralprosthesis, and the possibility of causing LV outflowtract (LVOT) obstruction. In addition, bileaflet preser-vation can be difficult in the presence of severely fi-brosed and calcified leaflets and subvalvar apparatus,which are common in rheumatic valve disease. How-ever, bileaflet preserving MVR is possible in the vastmajority of patients with rheumatic mitral disease.2,4
We now present a case report of a patient who devel-oped spontaneous anterolateral papillary muscle rup-ture following a chordal sparing MVR. The pathophysi-ology and management of this unusual complication isdiscussed.
CASE REPORT
The patient is a 47-year-old female with advancedrheumatic heart disease. She had a tight mitral stenosisand a moderate aortic regurgitation (AR) with severelyimpaired LV function. She was in atrial fibrillation anda tachycardia-induced cardiomyopathy was thought tobe at least partially responsible for the poor LV func-tion. On echocardiography, the mitral valve (MV) areawas measured at 0.7 cm2 with a diastolic gradient of25 mmHg over the MV. The LV dimensions were 74mm (end diastolic) and 62 mm (end systolic), respec-tively. The LV ejection fraction was measured at 24%.Moderate AR was present. Right heart catheterizationrevealed severe pulmonary arterial hypertension witha systolic pressure of 80 mmHg and a mean pressureof 64 mmHg. Right ventricular end diastolic pressurewas measured at 20 mmHg. Only mild tricuspid re-gurgitation was present. Coronary angiography wasnormal. At operation, the severely stenotic and cal-cified MV precluded valve repair. The chordae werealso thickened and fibrotic. The MV was replaced with29-mm CarboMedics bileaflet mechanical valve pros-thesis (CarboMedics, Austin, TX, USA) inserted in theantianatomical orientation. Bileaflet chordal preserva-tion was accomplished utilizing Miki’s MVR chordalsparing technique.5 In this technique, the central por-tion of the anterior MV leaflet is excised, and the re-maining buttons of anterior MV leaflet containing theload-bearing chordae are shifted and reattached to theMV annulus in the regions of the left and right com-misures, respectively. The midportion of the posteriorMV leaflet is also incised from free edge to base inorder to accommodate a sufficiently sized prosthe-
Figure 1. Transthoracic echocardiogram (parasternal, long-axis view, diastole) showing the ruptured papillary musclehead floating in the left ventricular outflow tract (solid whitearrow). The hollow pointed arrow shows the aortic valve pros-thesis.
sis. The aortic valve (AV) was replaced with a 25-mm CarboMedics bileaflet mechanical valve prosthesis(CarboMedics, Austin, TX, USA). Intraoperative trans-oesophageal echocardiography (TEE) showed normalprosthetic valve function with low gradients across theAV (mean gradient of 10 mmHg and systolic gradientof 16 mmHg) and MV prostheses, respectively.
The early postoperative course was uneventful de-spite the poor LV function. On the third postopera-tive day, an extra, “knocking” systolic heart soundwas noted on auscultation of the heart. Transthoracicechocardiography (TTE) revealed a mobile, peduncu-lated structure in the LVOT (Fig. 1) knocking againstthe ventricular surface of the AV prosthesis during car-diac systole (Fig. 2). The systolic gradient in the LVOT
Figure 2. Transthoracic echocardiogram (parasternal, long-axis view, systole) showing the ruptured papillary muscle headstriking the aortic valve prosthesis (solid white arrow).

62 LONGPAPILLARY MUSCLE RUPTURE
J CARD SURG2011;26:37-68
Figure 3. The resected ruptured papillary muscle head withits attached thickened and fibrotic chordae.
had increased dramatically to a mean pressure gra-dient of 32 mmHg (systolic gradient of 53 mmHg).There was no discernable deterioration in the patient’shemodynamic status at this point in time. Becauseof concern for embolization of this structure or en-trapment of the AV discs, urgent redo surgery wasundertaken.
At operation, the floating structure in the LVOT wasapproached through the posteriorly orientated leafletof the AV prosthesis and was found to be the rup-tured head of the anterolateral papillary muscle at-tached to its corresponding chordae. The chordae sup-porting the head of the papillary muscle were thenresected, flush against the AV prosthesis at the siteof reimplantation into the MV annulus and removed(Fig. 3). The rest of the operation was without inci-dent. TEE performed just before leaving the operatingroom revealed normally functioning prosthetic valveswith a dramatically reduced gradient in the LVOT viz.a mean gradient of 8 mmHg (systolic gradient of 16mmHg) over the AV prosthesis. Histological examina-tion of the papillary muscle head revealed the presenceof infarcted muscle. The patient made an uneventful re-covery in spite of the poor cardiac function and secondopen-heart surgery and was discharged seven dayslater.
DISCUSSION
The case described presents a very unusual com-plication of chordal sparing MV replacement viz. spon-taneous rupture of one of the heads of the preservedpapillary muscles of the MV. This complication was firstdescribed in 1984.6 Subsequently, only four additionalcases7–9 have been reported in the English-speakingliterature. In three of the reported cases, the complica-tion was fatal (all of these patients had received a tilting-disc mechanical prosthesis). The cause of the rupturedpapillary muscle in our case was muscle necrosis. Inthe presence of normal coronary arteries, other fac-tors probably combined to cause the infarction in thepapillary muscle head. The normal healing process inchronic rheumatic mitral stenosis is a slow-scarring pro-
cess resulting in among other things, a fibrous thick-ening and contraction of the chordae tendineae. Thiswould have resulted in shorter than normal chordaein our patient. Hetzer et al. have described a few pa-tients in which Miki’s chordal preservation techniquewas used, in which they demonstrated excessivelyhigh tension on the reimplanted strut chordae echocar-diographically (observed as permanently “stretched”chordae on TTE).10 These factors, in combination withthe severely dilated LV, would have placed excessivetension on the papillary muscle head resulting in de-creased perfusion and subsequent infarction and rup-ture. It is thus important during chordal preservationMVR to recognize and prevent excessive tension onthe reimplanted chordae. This is particularly of impor-tance in chronic rheumatic MV disease where the chor-dae are possibly already shortened due to the fibroticprocess. Excessive tension on the reimplanted chor-dae can be recognized at the time of valve implanta-tion, if they are already stretched taut in the empty,cardioplegic heart.10 Reimplanting the chordal buttonsunderneath, that is, on the LV aspect of the MV annulusand not on the upper, left atrial aspect of the annulusmight prevents further tension on the tensor apparatus.Our approach through the AV prosthesis gave good ex-posure to the submitral area, and the resection wasperformed with ease without any damage to eitherprosthesis.
CONCLUSIONS
Chordal sparing MVR is an indispensable techniquein the armamentarium of cardiac surgeons, but caremust be taken not to reimplant these chordae underexcessive tension especially in chronic rheumatic MVdisease.
REFERENCES
1. Athanasiou T, Chow A, Rao C, et al: Preservation of themitral valve apparatus: Evidence synthesis and criticalappraisal of surgical techniques. Eur J Cardiothorac Surg2008;33:391-401.
2. Chowdhury UK, Kumar AS, Airan B, et al: Mitral valvereplacement with and without chordal preservation in arheumatic population: Serial echocardiographic assess-ment of left ventricular size and function. Ann ThoracSurg 2005;79:1926-1933.
3. Yun KL, Sintek CF, Miller DC, et al: Randomized trialcomparing partial versus complete chordal-sparing mitralvalve replacement: Effects on left ventricular function. JThorac Cardiovasc Surg 2002;123(4):707-714.
4. Garcia-Fuster R, Estevez V, Gil O, et al: Mitral valvereplacement in rheumatic patients: Effects of chordalpreservation. Ann Thorac Surg 2008;86:472-481.
5. Miki S, Kusuhara K, Ueda Y: Mitral valve replacementwith preservation of the chordae tendinea and papillarymuscles. Ann Thorac Surg 1988;45:28-34.
6. Trites PN, Kiser JC, Johnson C, et al: Occlusion ofMedtronic Hall mitral valve prosthesis by ruptured papil-lary muscle and chordae tendineae. J Thorac CardiovascSurg 1984;88:301-306.
7. Mok CK, Cheung DLC, Chiu CSW, et al: An unusualcomplication of preservation of chordae tendineae in

J CARD SURG2011;26:37-68
ANDERSON, ET AL.SCHWANNOMA ENCOUNTERED DURING AORTIC VALVE REPLACEMENT
63
mitral valve replacement. J Thorac Cardiovasc Surg1988;95:534-536.
8. Goldenberg MR, Rozanski LT, Degeratu FT, et al: Pap-illary muscle rupture after chordal sparing mitral valvereplacement. J Heart Valve Dis 1998;7:590-592.
9. Lemke P, Roth M, Kraus B, et al: Ruptured papillary mus-cle after mitral valve replacement with preservation ofchordae tendineae. Ann Thorac Surg 2001;72:1384-1386.
10. Hetzer R, Drews T, Siniawski H, et al: Preservation ofpapillary muscles and chordae during mitral valve re-placement: Possibilities and limitations. J Heart Valve Dis1995;4(Suppl.II):S115-S123.
Primary Benign InteratrialSchwannoma Encounteredduring Aortic ValveReplacement
Corey D. Anderson, M.D.,∗Samad Hashimi, M.D.,†Talitha Brown, M.D.,‡John Moyers, M.D.,∗ andRobert Saeid Farivar, M.D., Ph.D.†Department of ∗Anesthesia, †CardiothoracicSurgery, and ‡Pathology, University of IowaHospitals and Clinics, Iowa City, Iowa
ABSTRACT Primary neurogenic tumors of the heartare extremely uncommon. We report the re-section of a benign primary schwannoma ofthe right atrium found incidentally during anaortic valve replacement. doi: 10.1111/j.1540-8191.2010.01158.x (J Card Surg 2011;26:63-65)
The incidence of primary cardiac tumors is quitelow. In autopsy studies, the overall prevalence of pri-mary tumors ranges from 0.002% to 0.25%. Althoughmost of these are benign, because of the risks to im-paired function (e.g., congestive heart failure [CHF],outflow tract obstruction, conduction system involve-ment, or peripheral embolism) they mandate prompttreatment. Incidentally encountered tumors during car-diopulmonary bypass mandate additional treatment de-cisions, which impact the conduct of the operationand cardiac function. Here, we present an inciden-tally discovered schwannoma during an aortic valvereplacement.
Conflict of interest: None.
Address for correspondence: Robert Saeid Farivar, M.D., Ph.D., De-partment of Cardiothoracic Surgery, University of Iowa Hospitals andClinics, 200 Hawkins Drive, SE517 GH, Iowa City, IA 52242. Fax: 319–356-3891; e-mail: [email protected]
CASE REPORT
A 67-year-old male had a one-year history of dyspneaon exertion and syncope. Transthoracic echocardiogra-phy (TTE) examination revealed severe aortic stenosiswith a peak and mean gradient of 114 and 70 mmHg,respectively. His valve area was calculated at 0.6 cm2.Cardiac catheterization revealed nonobstructive coro-nary artery disease. He was scheduled for elective aor-tic valve replacement.
Intraoperative transesophageal echocardiogram(TEE) in the standard four-chamber view revealed acystic mass in the right atrium involving the interatrialseptum (Fig. 1A). Bicaval venous cannulation withcaval snares and standard central aortic cannulationwere placed, and the heart was arrested using ante-grade cardioplegia. The right atrium was opened and afirm, rubbery mass was appreciated subendocardiallyin the triangle of Koch. It was shelled out completelyand sent for pathological examination (Fig. 1B). Theexcised tumor was a 3.1 × 2.5 × 1.7 cm, smooth,thinly encapsulated mass (Fig. 1C).
The interatrial septum was closed in two layers, butnot tacked down to spare the conduction pathway. Aor-tic valve replacement for the stenosed bicuspid aorticvalve was routine with a 25 bovine pericardial valve(Edwards Corp, Magna Thermafix, Irvine, CA, USA).The total cross-clamp time was 119 minutes, and thetotal cardiopulmonary bypass time was 143 minutes.He had complete heart block in the operating room,but on postoperative day 2, recovered intrinsic pacerfunction completely. The patient was discharged in agood condition.
The pathology revealed a schwannoma. The cut sur-faces of the tumor were tan-white to yellow and slightlynodular, with focal hemorrhage. Microscopically, theneoplasm demonstrated a thin, fibrous capsule over-lying biphasic growth. Densely cellular areas werecomposed of interlacing streams of spindle cells withtapered nuclei (Antoni A), admixed with hypocellularareas with loosely arranged cells with areas of vac-uolization (Antoni B). There were parallel arrays of tu-mor nuclei separated by amorphous, eosinophilic com-pacted material (Verocay bodies) (Fig. 1D). There wasno evidence of malignancy. These are characteristichistomorphologic features of schwannoma, a benignperipheral nerve sheath tumor. The tumor was shelledout in toto as evidenced by a continuous sheath, andmargins were not assessed since it would involve in-cising the conduction bundle.
DISCUSSION
Neurogenic tumors comprise 10% to 30% of me-diastinal tumors. Nerve sheath tumors are more com-mon in adults than in children, and are equally malig-nant in both. Primary benign cardiac neurilemomas areextremely rare tumors. They have Schwann cell ori-gins and were first reported in the 1972.1 They havebeen reported, to our knowledge, less than ten timesin the literature.2 They have been found incidentally atautopsy3 or during surgery. The location is varied andhas included the right atrium,4–5 left atrium,6,7 and left

64 ANDERSON, ET AL.SCHWANNOMA ENCOUNTERED DURING AORTIC VALVE REPLACEMENT
J CARD SURG2011;26:37-68
Figure 1. (A) Standard four-chamber transesophageal echocardiogram (TEE) view demonstrating a cystic mass (yellow arrow)involving the interatrial septum, projecting into the right atrial cavity. (B) Intraoperative photo of the right atrial mass beingshelled out. (Forceps are pointing to the tumor.) (C) Excised tumor was a 3.1 × 2.5 × 1.7 cm, smooth, thinly encapsulatedmass. (D) Organoid configuration of palisading tumor nuclei into Verocay bodies, red arrow (Hematoxylin and eosin stain; originalmagnification, 200×). RA = right atrium; RV = right ventricle; LA = left atrium; LV = left ventricle; IVS = interventricularseptum.
ventricle.8 They appear to have a right-sided predispo-sition in the heart and have a coincidental associationwith other types of cancer.5 Limited case reports haveshown complete resection to be curative.4 Metastatic,or secondary, neurilemomas are much more com-monly reported7 and have been found in the heart withextension from the spinal plexus as well as from thepulmonary veins.
Our patient had not been screened preoperativelywith a TEE, but with TTE. Upon rereview of the TTE, it
was still difficult to identify the mass. This case reportfurther emphasizes the importance of TEE in cardiacsurgery, whether done pre- or intraoperatively. Our de-cision not to tack down the virtual space created bythe excised tumor allowed our patient potentially toavoid a pacemaker, since his tumor traveled on theconduction bundle; however, he will need cardiac MRIto document the long-term freedom from recurrence,since this space is echogenic. There are no data onthe recurrence rate of these rare tumors. We could not

J CARD SURG2011;26:37-68
KOSHY, ET AL.PAPILLARY MUSCLE LIPOMA
65
assess margins, since the tumor was excised in totoand residual cardiac tissue at the border was not sam-pled; we presume that there may have been positivemargins. Upon nine months of follow up, he continuesto do well after his surgery with no symptoms.
REFERENCES
1. Gleason TH, Dillard DH, Gould VE: Cardiac neurilemoma.N Y State J Med 1972;72:2435-2436.
2. Rausche T, El-Mokthari NE, Kruger D, et al: Benign me-diastinal schwannoma: Cardiac considerations—case re-port and a short review of the literature. Clin Res Cardiol2006;95:422-424.
3. Factor S, Turi G, Biempica L: Primary cardiac neurilemoma.Cancer 1976;37:883-890.
4. Early SA, McGuinness J, Galvin J, et al: Asymptomaticschwannoma of the heart. J Cardiothorac Surg 2007;2:1.
5. Bizzarri F, Mondillo S, Tanganelli P, et al: A primary in-tracavitary right atrial neurilemoma. J Cardiovasc Surg2001;42:777-779.
6. Forbes AD, Schmidt RA, Wood DE, et al: Schwannoma ofthe left atrium: Diagnostic evaluation and surgical resec-tion. Ann Thorac Surg 1994;57:743-746.
7. Sirlak M, Uymaz OK, Tasoz R, et al: Primary benignschwannoma of the heart. Cardiovasc Pathol 2003;12:290-292.
8. Sevimli S, Erkut B, Becit N, et al: Primary benign schwan-noma of the left ventricle coursing under the left ante-rior descending artery. Echocardiography 2007;24:1093-1095.
Intracardiac Lipoma Arisingfrom the Papillary Muscle
Anoop N. Koshy,∗George Koshy, F.R.A.C.P.,∗ andAshutosh A. Hardikar, F.R.A.C.S.†∗Department of Cardiology, LauncestonGeneral Hospital, Tasmania, Australia; and†Department of Cardiothoracic Surgery,Royal Hobart Hospital, Tasmania, Australia
ABSTRACT Cardiac lipoma is the commonest non-myxomatous benign primary cardiac tumor. Wereport a case of lipoma arising from the anterolat-eral papillary muscle and presenting with a tran-sient ischemic episode and a history of malig-nant melanoma. The lipoma was removed leavingthe mitral apparatus intact. doi: 10.1111/j.1540-8191.2010.01156.x (J Card Surg 2011;26:65-66)
Conflict of interest: None.
Address for correspondence: Ashutosh A. Hardikar, F.R.A.C.S., De-partment of Cardiothoracic Surgery, Royal Hobart Hospital, 48 Liver-pool Street, Hobart, Tasmania, Australia 7000. Fax: +61–3-62313055;e-mail: [email protected]
Figure 1. Transesophageal echocardiogram depicting LVmass (arrow) attached to papillary muscle. LV = leftventricle.
Although autopsy studies show preponderance ofsecondary cardiac tumors,1 clinical series show thatmost are primary tumors and 90% are benign.2 Of thebenign tumors reported on the heart valves or chor-dae or papillary muscles, the commonest is papillaryfibroelastoma followed by myxoma and fibroma.3 Toour knowledge, a lipoma arising from the papillary mus-cle has not been reported. We present such a case inan elderly female presenting with a transient ischemicepisode and a history of malignant melanoma.
CASE REPORT
A 67-year-old female presented with tingling andnumbness on the right side with headache and blurryvision. She had a history of a temporal malignantmelanoma (Clark’s level I) removed two years ago. Hersymptoms resolved in six to eight hours. She had ahistory of hypertension, insignificant carotid disease onultrasound, and a normal physical examination. Trans-esophageal echocardiogram (Fig. 1) and magnetic res-onance imaging (Fig. 2) images showed a left ventricu-lar mass attached to the anterolateral papillary musclewith well-defined margins and an isointense center.Coronary angiography was entirely normal. In view ofthe ischemic episode and documented left ventricularmobile mass, she was referred for surgical resection.
Figure 2. Transversal magnetic resonance imaging showingthe LV mass (arrow) attached to anterolateral papillary muscle.LV = left ventricle.

66 TSIGKAS, ET AL.MILD SYMPTOMATIC ALCAPA IN AN ELDERLY PATIENT
J CARD SURG2011;26:37-68
Figure 3. Postexcision photograph of lipoma.
Following standard bicaval cannulation on cardiopul-monary bypass, a paraseptal incision was used to ex-pose the mitral valve.
A 15 × 13 mm mass (Fig. 3) was seen attached tothe anterolateral papillary muscle between the originsof two-strut chordae of the mitral valve. It had an en-capsulated component as well as a loose filliform com-ponent and was shaved off the muscle. Histologicalexamination showed it to be composed of mature adi-pose tissue, consistent with the diagnosis of a lipoma.The patient had an uneventful postoperative coursewith normal mitral valve function predischarge and re-mains well at the one-year follow up.
DISCUSSION
Intracardiac lipomas are the second most commonbenign primary tumor of the heart and have beendescribed in the pericardium, septal tissue, heartvalves, and subendocardial. They are usually asymp-tomatic and are diagnosed incidentally at autopsy,echocardiography, or cardiac catheterization.4 Intrac-ardiac lipomas are polypoid or sessile masses macro-scopically, which originate most commonly from withinthe left ventricle or left atrium.5 Clinical presentationsdepend on the size and location of the tumor. They canbe clinically silent, or embolize and cause arrhythmias,or create a ball-valve obstruction such as myxomas.6
Cardiac lipomas can also cause impaired atrial and ven-tricular function, secondary to mass effect leading tosymptoms such as fatigue, chest pain, palpitation, dys-pnea, and syncope.7–9 This is the first case reportedfrom the papillary muscle. This patient had a historyof melanoma surgery, which along with a transient is-chemic episode made us consider the diagnosis of a
secondary neoplasm in the heart. Being aware of thepossibility of a benign neoplasm, even in someone witha past history of secondary malignancy avoids denial ofa curative procedure to such patients.
REFERENCES
1. Roberts WC: Primary and secondary neoplasms of theheart. Am J Cardiol 1997:80:671-682.
2. Yu K, Liu Y, Wang H, et al: Epidemiological and pathologicalcharacteristics of cardiac tumors: A clinical study of 242cases. Interact Cardiovasc Thorac Surg 2007;6:636-639.
3. Edwards FH, Hale D, Cohen A, et al: Primary cardiac valvetumors. Ann Thorac Surg 1991;52:1127-1131.
4. Shapiro LM: Cardiac tumors diagnosis and management.Heart 2001;85:218-222.
5. Hayashi H, Hidaka F, Tomonari K, et al: A left ventricularlipoma diagnosed on three-dimensional electrocardiogram-gated cardiac computed tomography. Heart Vessels2008;23:366-369.
6. Motallebzadeh R, Desai JB: Mitral valve regurgitation dueto a lipoma. Ann Thorac Surg 2007;83:2234.
7. Rafel J, Puiadas R, Batalla N: Cardiac lipoma presenting asangina. Rev Esp Cardiol 2004;57:884.
8. Kusano K, Ohe T: Cardiac tumours that cause arrhythmias.Card Electrophysiol Rev 2002;6:174-177.
9. Kuzuzu A, Nisanoglu V, Gunen H: A case of a large in-trapericardial lipoma occupying pericardial space. J CardSurg 2007;22:417-431.
Anomalous Origin of the LeftMain Coronary Artery from theMain Pulmonary Artery in anElderly Patient
Grigorios G. Tsigkas, M.D.,∗Georgios A. Kasimis, M.D.,∗Vasileios Karantalis, M.D.,∗Dimitris J. Nikas, M.D., F.A.C.S.,† andDimitrios K. Alexopoulos, M.D., F.E.S.C.,F.A.C.C.∗
∗Cardiology Department, University ofPatras, Greece; and †Athens MedicalCentre, Athens, Greece
ABSTRACT Anomalous origin of the left coro-nary artery from the pulmonary artery (ALCAPA)syndrome is an extremely rare diagnosis in el-derly patients. We describe a 73-year-old femalewith ALCAPA who underwent successful repairof this coronary anomaly. doi: 10.1111/j.1540-8191.2010.01155.x (J Card Surg 2011;26:66-68)
Conflict of interest: None.
Address for correspondence: Grigorios G. Tsigkas, M.D., Consultantof Cardiology, Patras University Hospital, Rion Patras 26500, Greece.Fax: +302610992941; e-mail: [email protected]

J CARD SURG2011;26:37-68
TSIGKAS, ET AL.MILD SYMPTOMATIC ALCAPA IN AN ELDERLY PATIENT
67
Anomalous origin of the left coronary artery fromthe pulmonary artery (ALCAPA) syndrome is an ex-tremely rare diagnosis in elderly patients. We describea 73-year-old female with ALCAPA who underwentsuccessful repair of this coronary anomaly. Asymp-tomatic or mildly symptomatic—of recent onset—ALCAPA syndrome is extremely rare in elderly pa-tients. Meanwhile, the usual symptoms include thoseof heart failure, mitral valve insufficiency, angina, orarrhythmias. Medical management remains controver-sial, as mortality rates are extremely high. In contrast,surgical correction by creating a two-coronary systemshould be considered as the most appropriate alterna-tive independently of age and degree of intercoronarycollateralization.
CASE REPORT
A 73-year-old female was admitted for evaluation ofexercise-induced angina and mild dyspnea. Echocardio-gram demonstrated regional motion abnormality withsevere hypokinesia of the anterolateral wall and akine-sia of the apex, mild mitral regurgitation with a globalejection fraction of 45%. Subsequently, thallium 201single photon emission computed tomography my-ocardial perfusion imaging revealed a large but mostlyreversible perfusion defect in the anteroapical area. Adual-chamber pacemaker (DDD-R) had been implantedtwo years before due to sick sinus syndrome. The re-sults from the clinical examination were unremarkable.Cardiac catheterization revealed a giant right coronaryartery (RCA) in orthotopic location feeding collaterals to
Figure 1. Right coronary angiography (LAO projection). Whitearrow indicates the giant right coronary artery. The LAD andLCX are retrogradely perfused from collaterals (thin black ar-rows). The anomalous drainage of the left coronary artery topulmonary artery is shown (thick black arrow). LAO = left an-terior oblique, LAD = left anterior descending artery, LCX =left circumflex.
Figure 2. Transverse anterior incision in the main pulmonaryartery trunk. A probe (white arrow) is inserted in the orifice ofthe left coronary artery (black arrow).
the left coronary (LC) system. The latter was drainedretrograde through a restrictive orifice into the pul-monary artery (Fig. 1).
The patient was placed on cardiopulmonary bypassvia a median sternotomy, and the heart arrested withretrograde cold blood cardioplegia for 80 minutes. Thepulmonary artery was opened and the ostium of theleft main coronary artery was closed with a 4–0 pro-lene suture (SurgiPro, Shawnee, KS, USA) from insidethe pulmonary artery, which was subsequently closedin two layers with a 4–0 prolene suture (Fig. 2). Bypassgrafts were then performed to the ramus intermediusartery using the left internal mammary artery, and asaphenous vein graft was used to bypass the left an-terior descending artery. The patient had an uncompli-cated postoperative course and has remained free ofangina and dyspnea one month following surgery.
DISCUSSION
ALCAPA is an extremely rare but potentially fatalcongenital coronary anomaly, which accounts for oneof 300,000 live births (0.25% to 0.5%),1 and results ina mortality rate of up to 90% within the first year oflife.2 It is also known as the Bland-White-Garland syn-drome. ALCAPA is usually an isolated cardiac anomalybut, rarely has been described with patent ductus ar-teriosus (PDA), ventricular septal defect, tetralogy ofFallot, and coarctation of the aorta. Because of the fa-vorable fetal physiology, including equivalent pressuresin the main pulmonary artery and aorta secondary toa nonrestrictive PDA and relatively equivalent oxygenconcentrations due to parallel circulations, ALCAPAdoes not have clinical manifestations prenatally. As thepulmonary pressure decreases during the neonatal pe-riod, the left-to-right shunt across the coronary circu-lation increases with subsequent coronary steal andmyocardial ischemia, leading to myocardial infarctionand congestive heart failure.
A large dominant RCA with extensive intercoronarycollaterals filling the LC system, known as adult-typevariety of circulation, accounts for only 10% to 15% of

68 TSIGKAS, ET AL.MILD SYMPTOMATIC ALCAPA IN AN ELDERLY PATIENT
J CARD SURG2011;26:37-68
patients3 and contributes to long-term survival. Medi-cal management is associated with high-mortality ratesthat range between 45% and 100%.3 The risk for sud-den cardiac death due to ischemic-malignant ventricu-lar arrhythmias exists even in asymptomatic adult pa-tients.4 Kristensen et al.5 reported a case of ALCAPAsyndrome patient presenting with ventricular fibrillationtreated with surgery and implantation of cardioverterdefibrillator. The differential diagnosis includes dilatedcardiomyopathy, coronary artery fistula, mitral valve in-sufficiency, and finally myocarditis. Surgical correctionwith the aim of restoring a two-coronary system circu-lation is the current standard in these patients, regard-less of age or degree of intercoronary collateralizationwith a mortality rate about 0% to 23%.6 Surgical re-pair procedures that can be implemented include aor-tocoronary saphenous vein or internal mammary arterygrafting, aortic root reimplantation with or without apulmonary flap, or Takeuchi procedure (creation of anaortopulmonary window and an intrapulmonary tunnelextending from the anomalous ostium to the window).By establishing a patent two coronary artery system,most patients experience normalization of left ven-tricular systolic function, thereby improving long-termsurvival. Presently, new technology, improvements insurgical techniques, and early diagnosis using echocar-diography with Doppler color flow mapping, computedtomography angiography, and magnetic resonance an-
giography have dramatically improved the prognosis forpatients with ALCAPA.
REFERENCES
1. Kirklin JW, Barratt-Boyes BG: Congenital anomalies of thecoronary arteries. Cardiac Surgery. John Wiley, New York,1986, pp. 945-969.
2. Wesselhoeft H, Fawcett JS, Johnson AL: Anomalous ori-gin of the left coronary artery from the pulmonary trunk. Itsclinical spectrum, pathology, and pathophysiology, basedon a review of 140 cases with seven further cases. Circu-lation 1968;38:403-425.
3. Moodie, DS, Fyfe, D, Gill, CC, et al: Anomalous originof the left coronary artery from the pulmonary artery(Bland-White-Garland syndrome) in adult patients: Long-term follow- up after surgery. Am Heart J 1983;106:381-388.
4. Frapier JM, Leclercq F, Bodino M, et al: Malignant ven-tricular arrhythmias revealing anomalous origin of the leftcoronary artery from the pulmonary artery in two adults.Eur J Cardiothorac Surg 1999;15:539-541.
5. Kristensen T, Kofoed KF, Helqvist S, et al: Anomalous ori-gin of the left coronary artery from the pulmonary artery(ALCAPA) presenting with ventricular fibrillation in an adult:A case report. J Cardiothorac Surg 2008;3:33.
6. Dodge-Khatami A, Mavroudis C, Backer CL: Anomalousorigin of the left coronary artery from the pulmonary artery:Collective review of surgical therapy. Ann Thorac Surg2002;74:946-955.