December 2013 Division of Orthopaedic Surgery Moll’s voice › ... ›...
9
M o l l ’ s v o i c e As I pen this slightly late departmental newsleer, I wonder how 6 months could have already whis- tled past since the last edion. The only answer of course is the excite- ment of daily Orthopaedic pracce in our depart- ment with the abundance of work and play. I will expand on some of this in the next few pages. New Dean Firstly however there has been what I consider a significant change in our arena. This is the ap- pointment of the new Dean, Prof Wim de Vil- liers. I believe this to be extremely posive for us as Orthopaedic Surgeons. Not only is Wim a clinician but has worked in the USA in a private pracce environment. It is a relief to have someone up the chain acknowledging that medicine and money co- exist! As a high tech, high cost discipline we have had lile opportunity to flour- ish in the recent past where emphasis has been on the primary care end of medicine. Although most of us accept that primary care is important, there is no point having “reps on the road” if you cannot provide the defini- ve service, i.e. curave surgical care. Up to 29% of what a GP sees is musculoskeletal pathology, and thus Or- thopaedic surgery plays a significant role in treang these paents. Raising Orthopaedic Sur- gery’s profile is an inter- naonal challenge. In SA it is also necessary to edu- cate planners that Ortho- paedic Surgery is far more extensive than trauma surgery. The new Dean seems to understand this. Orthopaedics gets a menon At one of his early presen- taons he menoned Or- thopaedic Surgery as one of the key disciplines. This is a huge change to the usual public health brigade. It is the first me I have seen “Orthopaedics” on a slide at Faculty Board meeng! This has been re-enforced when I subsequently met with him. UCT PAH One of the Dean’s priori- es is to develop the UCT Private Academic Hospi- tal. Here we share similar philosophies which has resulted in an excing OrthoUCT iniave. Prof de Villiers’ vision is to develop UCTPAH into the first choice terary / qua- ternary care environment. This is a massive swing from the previous strate- gy of servicing the boom end of the financial pile. Our department has an “RWOP” reputaon, sadly negave to many UCT staff being of the socialist persuasion. Despite high outputs, we have frequently been cricised for our of-site private pracces. Our arguments have been ignored but this is chang- ing. OrthoUCT In response, I have decid- ed to assist the Deans vi- sion by developing a Or- thoUCT pracce at UCTPAH. This is designed to be a win—win for our staff, department, pa- Division of Orthopaedic Surgery December 2013 Issue 4 HOD’s update 1 Outreach 3 Fellowships 4 Teaching 5 Scoreboard 7 Consultants WIN cricket 8 Inside this issue: Prof Wim de Villiers Our new Dean
Transcript of December 2013 Division of Orthopaedic Surgery Moll’s voice › ... ›...

Moll’s voice As I pen this slightly late departmental newsletter, I wonder how 6 months could have already whis-tled past since the last edition. The only answer of course is the excite-ment of daily Orthopaedic practice in our depart-ment with the abundance of work and play. I will expand on some of this in the next few pages.
New Dean
Firstly however there has been what I consider a significant change in our arena. This is the ap-pointment of the new Dean, Prof Wim de Vil-liers. I believe this to be extremely positive for us as Orthopaedic Surgeons. Not only is Wim a clinician but has worked in the USA in a private practice environment. It is a relief to have someone up the chain acknowledging that medicine and money co-exist!
As a high tech, high cost discipline we have had little opportunity to flour-ish in the recent past where emphasis has been on the primary care end of medicine. Although
most of us accept that primary care is important, there is no point having “reps on the road” if you cannot provide the defini-tive service, i.e. curative surgical care.
Up to 29% of what a GP sees is musculoskeletal pathology, and thus Or-thopaedic surgery plays a significant role in treating these patients.
Raising Orthopaedic Sur-gery’s profile is an inter-national challenge. In SA it is also necessary to edu-cate planners that Ortho-paedic Surgery is far more extensive than trauma surgery. The new Dean seems to understand this.
Orthopaedics gets a mention
At one of his early presen-tations he mentioned Or-thopaedic Surgery as one of the key disciplines. This is a huge change to the usual public health brigade. It is the first time I have seen “Orthopaedics” on a slide at Faculty Board meeting! This has been re-enforced when I subsequently met with him.
UCT PAH
One of the Dean’s priori-ties is to develop the UCT Private Academic Hospi-tal. Here we share similar philosophies which has resulted in an exciting OrthoUCT initiative.
Prof de Villiers’ vision is to develop UCTPAH into the first choice tertiary / qua-ternary care environment. This is a massive swing from the previous strate-gy of servicing the bottom end of the financial pile.
Our department has an “RWOP” reputation, sadly negative to many UCT staff being of the socialist persuasion.
Despite high outputs, we have frequently been criticised for our of-site private practices. Our arguments have been ignored but this is chang-ing.
OrthoUCT
In response, I have decid-ed to assist the Deans vi-sion by developing a Or-thoUCT practice at UCTPAH. This is designed to be a win—win for our staff, department, pa-
Division of Orthopaedic Surgery December 2013 Issue 4
HOD’s update 1
Outreach 3
Fellowships 4
Teaching 5
Scoreboard 7
Consultants WIN cricket
8
Inside this issue:
Prof Wim de Villiers
Our new Dean

tients and UCT.
With a more aligned vi-sion with the faculty, we are able to function with-in the system to all’s ad-vantage.
The aim is to allow im-proved access of the pub-lic to our specialists. Cur-rently, paying patients are disadvantaged by inacces-sibility to the academic practitioners, many of which are leaders in their fields. This paradox is caused by the clinical overload at the Groote Schuur clinics, often by secondary level pathology that should be dealt with by generalists.
OrthoUCT will allow sur-geons affiliated to the department to practice privately under our ban-ner and continue to build the brand across all sec-tors of the community. The synergies of the group practice will opti-mise the financial aspects to allow a viable RWOP practice without the con-stant pull of increased private commitment as experienced when work-ing off site with full time costs.
In addition, OrthoUCT will increase the teaching and training platform at post-graduate and fellowship
level as well as generate revenue to promote these activities.
We have met with the relevant parties and a dedicated area is being refurbished to accommo-date dedicated admin-istration staff. Other chal-lenges of radiology and theatre equipment is cur-rently being addressed.
Research
Another of the Dean’s priorities is research hubs or nodes. Here he has encouraged Orthopaedic Surgery to develop a re-search unit. We are al-ready extremely produc-tive in research and sub-specialist training, but this may be more sustainable with some re-organisation , especially with longer term funding and dedicated support staff. This may well inter-leave with the OrthoUCT project.
All in all, an exciting 2014 coming. RD
Grand ward rounds back online thanks to Ortho Ingenuity!
With the radiology migra-tion to the digital platform, clinicians were left with the frustration of walking between patient’s beds and wall mounted PACS stations. You can imagine the result—patient or x-ray, never both.
PGWC’s COW’s as they were called were never ordered by GSH as they failed at Tygerberg due to poor battery life, connec-
Page 2 Mol l ’s vo ice I ssue 4
tion issues and the like.
Following a successful prototype, Dave Chivers welded up the mobile stand with Tom Hilton lending a hand to the fin-ishing touches. RD com-pleted the IT side, squeez-ing a screen and 3G mo-dem out of PGWC.
The BEAST has now suc-cessfully been employed and Grand Rounds have returned.
We are taking orders from other departments but are not cheap!
Proof that the pot of gold is in D10

Nick Kruger was first to brave the Namib and had this to say: It was a whistle stop tour. Left Cape town 0630, arrived 0830 Windhoek, met by Alex and whisked off the Central State Hospital where we did a ward round. Was introduced to the staff as well as the new Spinalis spinal rehab unit sponsored by Sweden, where paraplegics train and rehabili-tate new patients. Alex was most proud of the attractive foreign OT’s. Grabbed breakfast on the go then went to theatre where Alex had lined up two cases needing our skills. Very little in the way of spinal specific instruments available, the surgery was done with mostly ancient 5mm blunt upcuts and tiny nibblers. No spinal frames, the patients were proned onto 2 pillows and some blankets. Before you could even look for a 3rd pillow the scoline was in and patient turned. After theatre, lunch eaten whilst being whisked off to the new Namibian Medical school where we spent the remainder of the day teaching and lecturing the 4th year med-ical students.
After long day ( up since 0430 to get flight) was re-warded by Alex taking me to the Skylounge- top of the Hilton where sundown was monitored over a glass of Windhoek’s finest brew. Next stop was the appropri-ately named Joes Beerhouse where we quaffed down some steak and ribs and more beer surrounded by a huge amount of atmosphere and stuffed animals. Next day, started 0700 with student presentation of ankle fractures then trauma post intake meeting at the Centrale Government Hospital. They get through a huge amount of trauma with very little re-sources. Ward round followed then off to the local Mediclinic to do two cases. The government hospitals outsource some of their cases to be done at the Mediclinic when they don’t have proper theatre equip-ment or post op ICU facili-ties. Morning list done, off to the medical school for an after-noon of practical teaching and examination techniques.
Page 3 Newsletter T i t le I ssue 4
430 taken back to airport for flight home. I recommend we should have a regular outreach to Wind-hoek, it flies the UCT flag high and helps out with their complex cases where there is a deficit in training. Nick Kruger
Outreach Outreach continues to be an important part of departmental service. GSH / RXH cannot service everyone and there is a paucity of skill outside with many state hospitals struggling to retain staff. It also allows us to spend other budgets, e.g. the Eastern Cape, rather than try and continually stretch ours. Thus outreach allows skills transfer, increased patient access to care and if well planned, good fun. No point doing it, if you’re not enjoying it.
Windhoek outreach
With Alex vd Horst taking up a Namibian university and State post in Windhoek, we have been begged for help. It appears every Namibian has a spine issue.
Alex and Nick reckon they had a hard day!
I followed Nick some weeks later. Alex and I per-formed 11 cases in 3 days. This included a national hero, a wheelchair athlete who had cycled 700km from Oshakati to Windhoek. He had subsequently spent a year in hospital with TB spine and no one to manage it. Despite the limited resource, we and the patient survived the surgery.
We were ‘privileged’ to have the head anaesthetist who spent as much time in theatre as the average porter! He put up a ‘pinkie’ drip and despite my hint of ‘are you happy with your ve-nous access?’ said ‘carry on’.
So carry on we did with diligent hae-mostasis rescuing every RBC possi-ble. Anyway, all’s well that ends well.

In an effort to stem the tide of spinal patients from the Eastern Cape, I re-turned to Livingstone Hos-pital in October. There is no shortage of work there, but the ability to do it is another matter.
Valentine Mandizvidza, Spine fellow from Zimba-bwe, and myself encoun-tered Eastern Cape chaos at its best.
The lifts were not working and our patient was 2 floors above the theatre. We initially did the Eastern Cape thing - sit and wait. There was no apparent action but we learnt that OTIS refused to assist as
Although our priority remains registrar training, we have increased our fellowship of-ferings based both on our state training platform as well as our affiliated private prac-tices.
Currently we offer two spine fellowships, one upper limb, one lower limb arthroplasty and one knee fellowship and 2014 adds a Trauma fellow. Funding models differ but in essence they cost the state nothing but provide addition-al service to our community, a win-win situation.
These fellowships increase our visibility nationally and promote research.
In addition there is a constant
Page 4 Mol l ’s vo ice I ssue 4
they had not been paid for 6 months.
It was a choice between a wasted trip and entertain-ing the locals. We chose the latter , grabbing a trol-ley we carried our quad-raparetic patient down the stairs to much amusement.
In the end we managed to perform two major spine surgeries with a positive impact for the patients.
We need to thank DuPuy for their ongoing support in funding the Eastern Cape spine outreach.
Outreach Doctors carrying our quadraparetic patient to theatre - two floors down while Eastern Cape admin decide whether to pay Otis lifts .
Can this be the same place? - the view from Cubana, Port Elizabeth, while revitalising.
Fellowships
The spine unit is leading the way with transfor-mation from the stereotypical “Orthopod”. Not only have we re-educated two neurosurgeons, we currently have Dr Lusanda Bomela as our first female spine fellow.
From the photo, it appears our patients don’t always keep up with our progressive steps. He is clearly confused by this set up.
stream of observers.
In 2014 we expect a Not-tingham Spine registrar for three months as well as a consultant from Denmark. A Swiss registrar will be joining our training program as well.
TB and trauma, and no doubt the best city in the world, seem to the major draw cards.

Teaching We continue to build on our previous efforts to enhance undergraduate education. Following curricular changes and development of OSCE testing, we have initiated prac-tical skill training outside the conventional block but as workshop open to all interest-ed students on a registration basis. Nick Kruger led this with a few gently coerced registrars to great effect. A POP application course was held in conjunction with Ra-chel Weiss and the teaching unit to great effect. It was attended by 40 6th year MBChB students with very good feedback from the stu-
dent body. Not only does this improve primary care doctor skills but creates enthusiasm about Orthopaedic Surgery and hopefully an increased interest in our specialty by UCT students who seem to be largely absent from our post graduate circuit.
Page 5 Mol l ’s vo ice I ssue 4
Postgraduate training Our partnership with Smith and Nephew and other trade in terms of cadaver based training as improved our registrar train-ing immensely.
We continue to offer Friday afternoon workshops and have expanded this to hand and foot surgery.
S&N supply arthroscopic equipment to allow our train-ees to gain skills before meet-ing the patient in theatre.
This puts us way ahead of the other national training centres.
Mike Solomons taking the registrars through a dorsal approach to the wrist during a hand workshop ar-ranged by Michelle Maree.
Rob Dachs seeing where Guyon’s canal really is ...
The 11th annual spinal approaches course was held in November drawing delegates from as far afield as Kenya. This remains a popular course nationally and is always oversubscribed.
Upper limb workshop run by Steve Roche

Teaching
Graham McCollum has made a big
impact in the Foot and ankle arena
since returning from his fellowship
abroad.
In November he ran our first fore-
foot Cadaver course. The regis-
trars and some of the consultants
went through common forefoot
procedures, such as first metatarsal
osteotomies for hallux valgus, less-
er toe surgery and soft tissue pro-
cedures.
They were then able to perform
the procedures on the cadavers
thanks to the donation of screws
and tools by BMG Orthopaedics.
Page 6 Mol l ’s vo ice I ssue 4
Foot and Ankle workshop
Sithombo Maqungo is the secretary of the local Orthopaedic Trauma society and reports the following: This past weekend we organised and hosted the inaugural symposium of the South African Orthopaedic Trauma Society at the Waterfront. This symposium also incorporated the launch of the South African Limb Reconstruction Society. Invited speakers were Piet De Boer (of Hoppenfeld and De Boer fame) from Zurich and Milan Olekasak from Bermuda (UCT ortho gradu-ate). Piet De Boer tore his quadriceps tendon a few days before the event so he underwent surgery and could not travel. He gave his presentations live from a hospital bed in Zurich. This was a major technological achievement that we doubt has ever been done before. It was certainly a South African first! UCT dominated the proceedings once again, reading 6 of the 11 free trauma papers.
First SA Orthopaedic Trauma Society meeting

The Scoreboard Our competitive edge seems to have no boundaries. Since the last scoreboard, there has been the Gun Run, the Medical 10, the newly es-tablished Registrar - consult-ant Waterpolo contest and the Cricket. Steve Carter killed us all with a 1.40 21km Gun run but I take satisfaction in beating shining light Maritz Laubscher. This was despite his early night, declining an invitation to the Friday night Pinotage evening. There was some explanation involving Barlodien setting the pace. I note that following this defeat he withdrew from the Medical 10.
Gun run 21km Steve Carter 1.40* Steve Roche 1.59 Michelle Maree 1.59 Rob Dunn 2.04 Richard v Bormann 2.10
Maritz Laubscher 2.11 Sithombo Maqungo 2.15 * claimed by Steve but no mention on official results—did anyone see him run?
Medical 10 Cobus Moolman 39.09 Steve Roche 48.57 43.27* Ian Koller 49.57 Adrian Swan 51.55 Michelle Maree 53.53 53.23* Rob Dunn 54.14 51.14* Anria Horn 65.05 Mike Mulder 70.26 * with age handicap
Page 7 Mol l ’s vo ice I ssue 4
Well done Du Preez Naude on lifting the SAOA Golf trophy at the recent SAOA meeting in Sun City.
McCollum and his Team mate Jakub gave the Nortje/Dower pairing a hiding in the recent Wines to Whales Mountain biking event, beating them by 20 minutes over three stages. Marc, bewildered at the loss blames the lack of form on the bike he was riding. Tipped to be a close tussle before the event, turned out to be rather one-sided. GM
The first Consultants versus Registrar Waterpolo contest was held at Nick’s insistence. This proved invaluable as not only did the Consultants take it with a 16 - 6 win, it may well have had a deleterious effect on the registrar bowling a the cricket match later the same day. Good plan Nick!
The Scoreboard
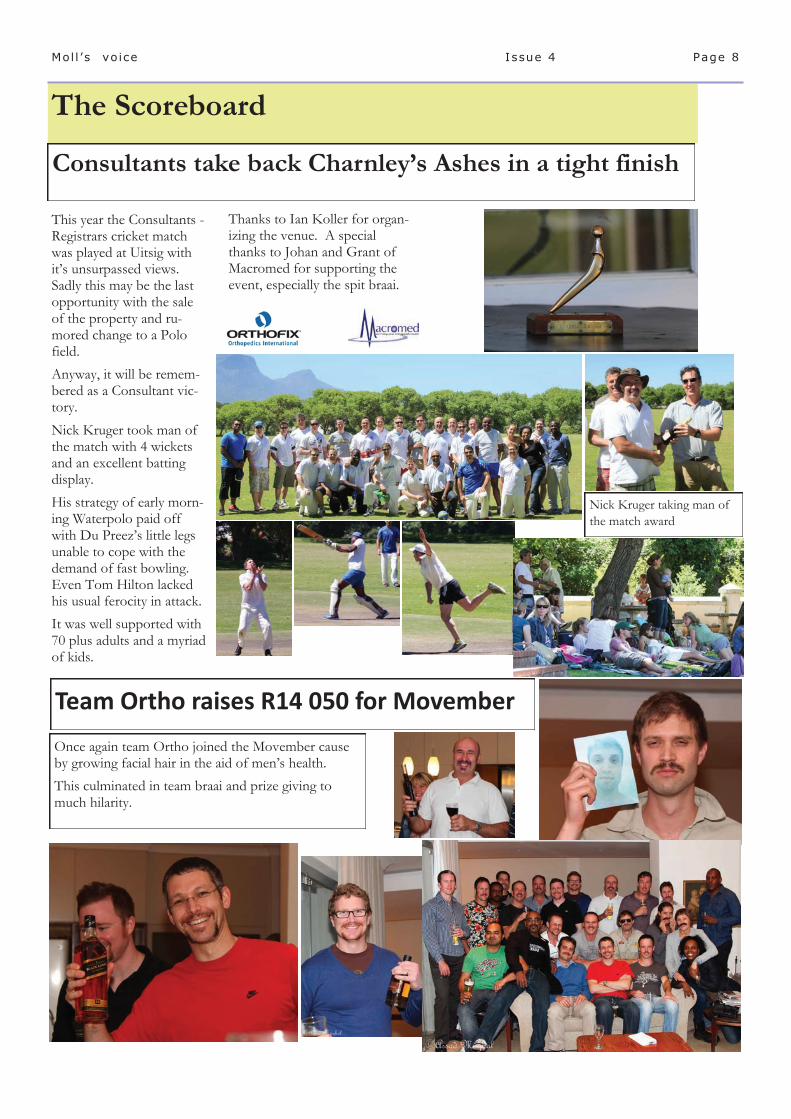
This year the Consultants - Registrars cricket match was played at Uitsig with it’s unsurpassed views. Sadly this may be the last opportunity with the sale of the property and ru-mored change to a Polo field. Anyway, it will be remem-bered as a Consultant vic-tory. Nick Kruger took man of the match with 4 wickets and an excellent batting display. His strategy of early morn-ing Waterpolo paid off with Du Preez’s little legs unable to cope with the demand of fast bowling. Even Tom Hilton lacked his usual ferocity in attack. It was well supported with 70 plus adults and a myriad of kids.
Thanks to Ian Koller for organ-izing the venue. A special thanks to Johan and Grant of Macromed for supporting the event, especially the spit braai.
Page 8 Mol l ’s vo ice I ssue 4
Consultants take back Charnley’s Ashes in a tight finish
Once again team Ortho joined the Movember cause by growing facial hair in the aid of men’s health. This culminated in team braai and prize giving to much hilarity.
Team Ortho raises R14 050 for Movember
Nick Kruger taking man of the match award
Divisional meetings CPD accredited. All our academic meetings are now CPD accredited. Private consult-ants are welcome to attend and contribute. Our Spine meeting has grown and is attracting many private surgeons, with our Trauma meet-ing following suit. I would like to see our Friday academic sessions attracting similar interest. Remember to sign the attendance register for points allocation.
Our fixed weekly academic meetings are as follows:
Monday 7 - 8 am: Trauma meeting D15
Tuesday 7.45 - 9 am: Spine meeting D15
Tuesday 1-2pm: Clinical examination meeting D6
Tuesday 8 - 10pm Registrar teaching
Friday 2 - 4.30 Dept academic meeting H49
A monthly program is available.
H49 Old Main Building Groote Schuur Hospital Anzio Road Observatory Cape Town 7925
http://orthopaedics.uct.ac.za
Secretary: Mrs Bernadette Priest Telephone: +27 021 404 5108 [email protected]
And UCT tells us there is more to our jobs than operating!
Part of a HOD’s job is to support his consultants, especially when they are being beaten to death by boredom in another endless meeting.
Here is a Whatsapp cry for help from Sithombo trying to survive a UCT spacial committee meeting.
Division of Orthopaedic Surgery
News snippets If anyone would like to contribute something of interest regarding our department for the next Newsletter, please send to me on:
Well done to Michael Held on achieving his FCS Orth in the recent exams.
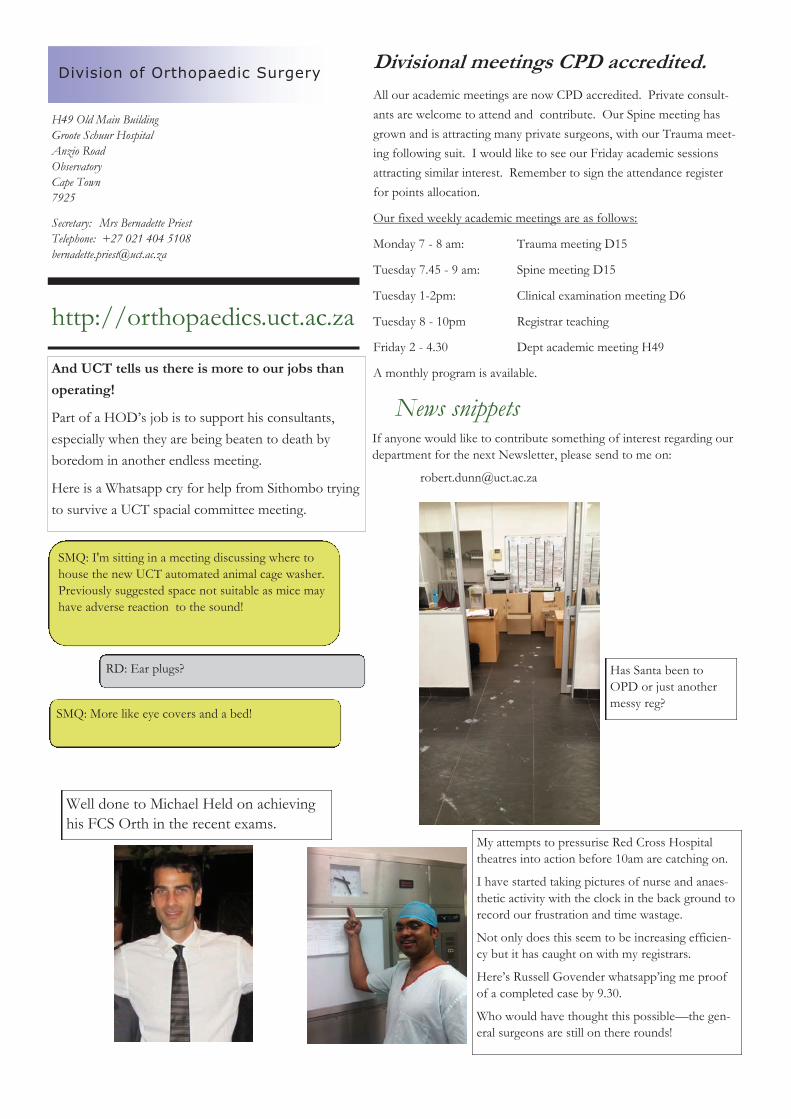
My attempts to pressurise Red Cross Hospital theatres into action before 10am are catching on.
I have started taking pictures of nurse and anaes-thetic activity with the clock in the back ground to record our frustration and time wastage.
Not only does this seem to be increasing efficien-cy but it has caught on with my registrars.
Here’s Russell Govender whatsapp’ing me proof of a completed case by 9.30.
Who would have thought this possible—the gen-eral surgeons are still on there rounds!
SMQ: I'm sitting in a meeting discussing where to house the new UCT automated animal cage washer. Previously suggested space not suitable as mice may have adverse reaction to the sound!
RD: Ear plugs?
SMQ: More like eye covers and a bed!
Has Santa been to OPD or just another messy reg?