DATE OF MEETING PAPER REF MAB/16/93 AUTHOR PRESENTER · 21 July 2016 . PAPER REF: MAB/16/93 ....
24
MANSFIELD AND ASHFIELD CCG GOVERNING BODY TITLE: Better Together Programme update DATE OF MEETING: 21 July 2016 PAPER REF: MAB/16/93 AUTHOR: Dawn Atkinson PRESENTER: Dawn Atkinson SUMMARY: • The Better Together monthly summary as prepared for the June Alliance Leadership Board is attached for information. The report provides a brief progress report on each of the projects under the clinical and enabling programme areas. • The programme stocktake report provides an overview of the programme key performance indicators used to track delivery of the six key strategic objectives. The information is presented as Mid Nottinghamshire total and at CCG level activity at Sherwood Forest Hospitals NHS Foundation Trust Programme. The information is also available for all provider organisations. ACTION: To note to approve To agree the recommendation (see details below) HOW DOES THIS CONTRIBUTE TO THE OUTCOMES AND OBJECTIVES OF THE CCG: Quality Health Financial Clinical Performance Other (specify) (tick as appropriate) RISK ASSURANCE: CONFLICTS OF INTEREST: This is a recommended action to be agreed by the Chair at the beginning of the item. No conflict identified Conflict noted, conflicted party can participate in discussion but not decision (see below) Conflict noted, conflicted party can remain but not participate (see below) Conflicted party is excluded from discussion (see below)
Transcript of DATE OF MEETING PAPER REF MAB/16/93 AUTHOR PRESENTER · 21 July 2016 . PAPER REF: MAB/16/93 ....

MANSFIELD AND ASHFIELD CCG GOVERNING BODY TITLE: Better Together Programme update DATE OF MEETING: 21 July 2016 PAPER REF: MAB/16/93 AUTHOR: Dawn Atkinson PRESENTER: Dawn Atkinson
SUMMARY:
• The Better Together monthly summary as prepared for the June Alliance Leadership Board
is attached for information. The report provides a brief progress report on each of the projects under the clinical and enabling programme areas.
• The programme stocktake report provides an overview of the programme key performance indicators used to track delivery of the six key strategic objectives. The information is presented as Mid Nottinghamshire total and at CCG level activity at Sherwood Forest Hospitals NHS Foundation Trust Programme. The information is also available for all provider organisations.
ACTION:
To note to approve To agree the recommendation (see details below)
HOW DOES THIS CONTRIBUTE TO THE OUTCOMES AND OBJECTIVES OF THE CCG:
Quality Health Financial Clinical Performance Other (specify) (tick as appropriate)
RISK ASSURANCE:
CONFLICTS OF INTEREST:
This is a recommended action to be agreed by the Chair at the beginning of the item. No conflict identified Conflict noted, conflicted party can participate in discussion but not decision (see below) Conflict noted, conflicted party can remain but not participate (see below) Conflicted party is excluded from discussion (see below)

CONFIDENTIALITY:
Is the information in this paper confidential? No Yes
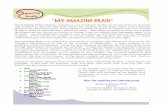
Better Together Programme June Summary Report – Alliance Leadership Board
15.1% reduction in A&E attendances
19.% reduction in non-elective admissions
30.5% reduction in non-elective bed days
25% reduction in admissions to nursing and residential homes
9.8% reduction in secondary care elective referrals
20% reduction in paediatric non-elective admissions
Better Together
Programme Area
Workstream
Sponsor/PM/ Clinical Lead
June summary progress
Remedial action
RAG
status
Urgent and Proactive Care Local Integrated Care Teams – an integrated health and social care model for the Mid-Notts footprint Specialist Intermediate Care Team & crisis Response – will support patients requiring intensive intermediate care and rehabilitation on
Dr Andy Haynes/ Dr James Mills
Dr Andy Haynes/ Dr James Mills
The pilot between LICT and START has now started in Hardwick. The pilot will run for 6 months with evaluation to take place in Sept 16. Recruitment remains challenging although there has been some progress with some community nursing posts recruited to and awaiting start dates. N&S will not achieve full year trajectory for proxy avoided admissions - action plan in place. M&A has over-achieved (although worth noting their target was smaller than N&S) A review of the LICT specification has started with the goal of refreshing the specification to take into account changes within the service and the operating landscape. Single Assessment template is complete expected to go live in June. The SICT operating model is being finalised now an agreed level of medical input has been determined. The medical input will be reviewed after 3 months to confirm level is appropriate and sustainable. Recruitment of the required additional nursing staff is on-going.
No additional action required at this stage.
Amber Amber
1 | P a g e

discharge Single Front Door – improved patient triage/streaming protocols to ensure patients received the most appropriate care in the right setting Call for Care (Care Navigation Service) – single point of access for health professionals to have access to quick and effective care co-ordination
Dr Andy Haynes/ Dr Benjamin Owens Dr Andy Haynes/CHP/ Dr James Mills Dr Andy Haynes/ Dr James Mills
King’s Mill Hospital SFD Attendances at ED and PC24 for the month of April have declined however; work is on-going to determine the reasons for the recent significant rise in activity. The March spike in activity has been experienced across a number of urgent care systems nationally. Recent change to the provider of the PC24 service will require a period of support to ensure the service operating model is understood and benefits realised. However, discussions with the new provider NEMs are presenting opportunities for the introduction of new patient pathways that would support reduction in admissions. Newark Hospital SFD A clinical pathway to support a primary care led front door model has been developed and being discussed as part of the overall Newark Strategy and the Urgent Primary Care Hub development. Roz Howie, Acting Deputy COO, SFHFT is the identified led for SFHFT, David Ainsworth and Andrea Brown are leading for the CCGs. The pathway provides much greater emphasis on the role general practice will play in service provision. Expressions to federate in a way that provides a service offer will be sought from local practices. Calls received in May were 112, this is a worsening position against the monthly target Health Partnerships, the service provider, has undertaken a number of actions to raise awareness of the service to increase service take up. GP’s and EMAS have been specifically targeted. A ‘deep dive’ audit of all CfC referrals identified the 30% of referrals had social care needs. Social cares has reviewed the referrals and have suggested an appropriate level of social care input that would support an early/urgent response. Discussions are on-going. The numbers through the self-care hub are slowly increasing and traffic through
Analysis of ED and PC24 activity on-going Formal review of the specification to take place. On-going
Red
Green
Red Amber
2 | P a g e

Self-Care Hub – targeted approach and support for patients and families to self-care
the self-care website is encouraging. Discussion about how the website activity, not simple ‘hits’ but where an extensive search has taken place, is recorded and reflected in reporting is on-going. More work is needed to reach target. The Hub is not current achieving the targets around Cancer and Diabetes; however the necessary links are being established and progressed. As a large part of this work is based on interdependencies with other stakeholders, this has proved challenging and is taking time. The Cancer element is developing faster, in part due to the organisation’s links with the CCGs Cancer programme which would seem more robust than with the Diabetes Workstream. The LICTS are also not achieving their Cancer quality targets in terms of onward referrals/self-care interventions because the patients who fall into this category aren’t an appropriate cohort for this delivery. E.g. they are just too ill for uptake/the MDT which is involved has addressed these needs. This is being picked up as part of the contract review meetings to understand what can realistically be achieved.
monitoring of activity and actions.
Elective Care Review Ophthalmology – redesign of the Ophthalmology pathway to support demand and capacity constraints
Dr Gavin Lunn/Jane Thornley/Dr Hilary Lovelock
Project plans, pathway and business case being developed for creation of Community Minor Eye conditions service, using HEEM (Health Education East Midlands) funding. This funding is being used to facilitate development of pathways, including training for independent prescribers. Key focus will be on the development of minor eye condition service and development of a community glaucoma pathway and wider transformation for community provision. Advert for Optom training has been shared with community optometrists. Transfer suitable activity from secondary care to a community setting – this will include stable Wet AMD and Stable Glaucoma and suitable post op Cataract follow ups. Wet AMD training programme approved by CCG Quality & Risk Cte with recommendations on monitoring and training provider. Alternative training provision is being sourced. Pathways and processes being refined. Further analysis of activity data provided for Wet AMD and Glaucoma has been requested by CCG.
None required.
Green
3 | P a g e

Integrated Musculoskeletal (Trauma and Orthopaedics workstream) – improve referral management and increase the management of patients in a community setting
Urology – shift of activity to community setting and improved service delivery models Referral Facilitation
Dr Gavin Lunn /Jane Thornley/Dr Andy Sommers
Dr Gavin Lunn/Jane Thornley/Dr Nigel Marshall
Dr Gavin Lunn/Jane Thornley/Dr Nigel Marshall
Work continues on the development of an Integrated Musculoskeletal (MSK) service, which will include T&O, Pain Management, Rheumatology, Therapies and Diagnostics. MSK network launched on 16 June, including representation from all stakeholders. Draft business case has been to CCG FDPG for preliminary discussion and final version to be completed by the end of June. Scoping of current physiotherapy/therapies provision on-going and re-design session with relevant stakeholders held in March and project plan is being worked through. Workforce evaluation being developed. Current Provider now not in agreement with revised Specification awaiting feedback from Provider around issues with Specification. Urology Referral form being trialled until 19/05/16. Assumptions range from movement of 20% to 75% of routine male urology activity into community clinic; these cannot be triangulated against 15/16 routine male activity for conditions defined to be treated in Community Urology Clinic as current provider does not code activity to enable this. Clinical judgement made that between 65%-70% of routine activity based on the new defined community conditions identified could be delivered in Community Clinic. Utilisation rates and financial viability of Community Clinic is being discussed with the SFHFT.
Clinical Pathways Web Page – Phase 2 is now live. Targeted upload of educational videos to be phased over the next 12 months.
Referral Templates – Orthopaedic and generic templates have been amended
Activity reduction trajectory to be included in the final business case. Escalated to STEG for discussion.
Amber
Amber
Amber
4 | P a g e

and are now in circulation for general use. Urology template is being piloted.
Gateway Re-Procurement - Work is underway to review and re-procure the current N&S Gateway model, to allow required work up and procurement processes to take place in line with 1.4.16 target. M&A CCG will continue with partial use of the gateway for triaged services. Contracts in process of being signed off.
Referral Facilitation Model (M&A): Referral Facilitation Model (M&A): Further development of the proposed M&A referral facilitation model is in progress. Partial engagement with CCG membership has been positive and feedback received is being written into the business case. This model will cover the main elements of the original referral facilitation model; peer review, and clinical partnership. This is a locality based model which would be clinically led by a team of Clinical Referral Advisors. It is anticipated that these posts will be recruited as 3 x 0.20 WTE pa, with a lead role at 1 x 0.3 WTE. The Clinical Referral Advisors would have responsibility for lead areas, and would work closely with the practices within their designated Locality Group. They would support practices with all aspects of the referral process, providing support with peer review, advice and guidance on primary care management and pre-referral work up, helping to change referral behaviour and improve the referral process. This model will be supported by a team of Referral Support Facilitators, working closely with the GP practices and the Clinical Referral Advisors. Finance have approved go live in one locality area and it has been agreed that Ashfield South will proceed initially. Both vacancies have now been advertised. Working with locality group to prepare for implementation – Mid August subject to recruitment process.
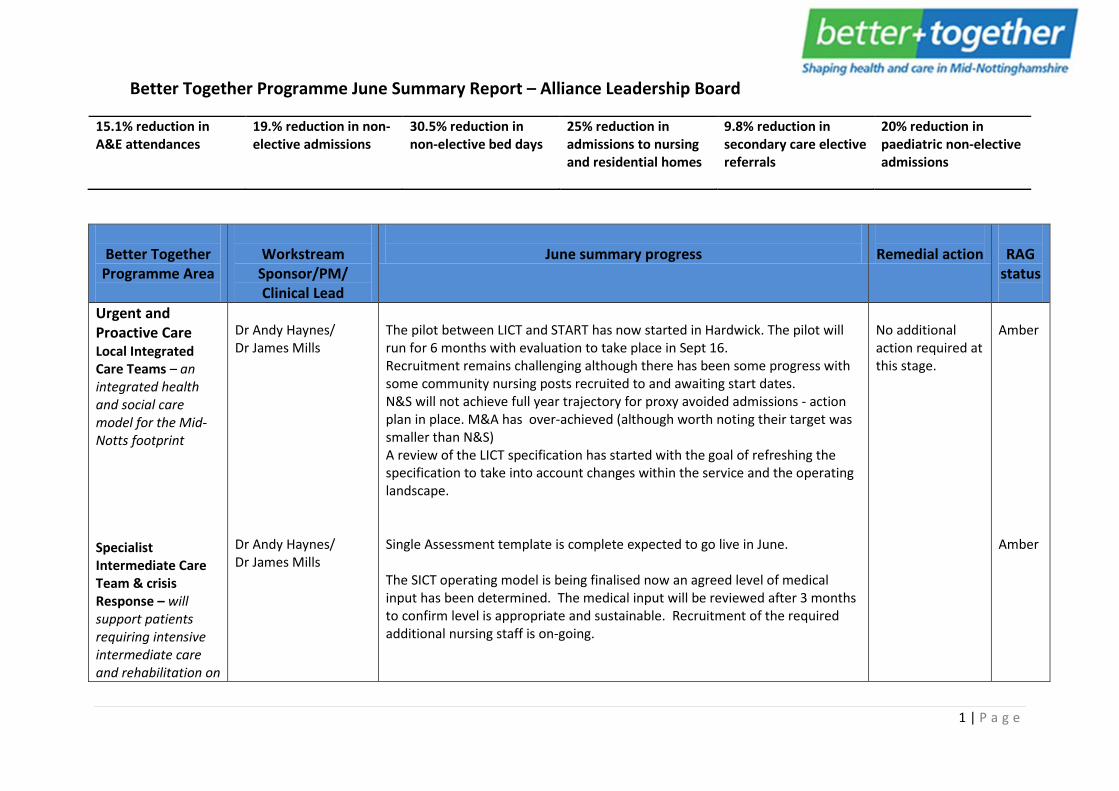
IM&T Medical Interoperability Gateway (MIG2) - a county wide
Dr Mark Jefford/ Andy Peers
The Privacy Impact Assessment (PIA), Quality Impact Assessment (QIA) and Equality Impact Assessment (EIA) approval confirmed at the last MIG Project Board held on the 25th May. The combined Information Sharing Agreement (ISA) and Information Access
None required.
Green
5 | P a g e
initiative to help support improvements in unplanned and urgent care Enhanced Data Sharing Model - Nottinghamshire wide consent sharing model SystmOne in Care Homes - supporting the single front door shared patient records
Dr Mark Jefford/Andy Peers Dr Mark Jefford/Andy Peers
Agreement (IAA) approval was also confirmed at the last MIG Project Board Testing has commenced on the new supportive EOL dataset using EMISWeb first with SystmOne to follow, overall progress to be reviewed at the next Project Board meeting scheduled for 29th June As reported last month there is no spare availability in the PLT events to deliver a roadshow style presentation to promote the new MIG service and wider sharing principles. Instead alternative options are being considered, which include a virtual roadshow on a dial-in interactive basis, or for those unable to attend, a non-interactive version to access when convenient. In addition, the support materials along with key messages are currently under review and will be revamped accordingly. Proposed dates publishing the event are still be confirmed The latest percentage of patient records shared out across the Mid-Notts practices remains constant for M&A at 88% and N&S at 97% Last month reported 3 M&A practices had lower sharing rates than the 65% minimum threshold. Unfortunately this was an oversight there are actually 4 practices involved. The practices and individual sharing percentages are Kirby Community Primary Care Centre (56.2%), Harwood Close Surgery (26.4%), Meden Vale Medical Services (53.4%) and Willowbrook Medical Practice (31.9%). Review meetings are being organised with the practices. Draft PID distributed for review and feedback by 22nd June Creation of Information Governance pack still in progress with checkpoint review scheduled for the 23rd June The SystmOne Care Home units will be deployed across 4 phases (10 homes in each phase). Phase 1 Care Homes in scope are: Wren Hall (M&A), Sutton Manor (M&A), Sutton Lodge (M&A), Sutton Court (M&A), Lowmoor (M&A), Pathfinders (N&S), Red Rose (N&S), Southwell Court (N&S), Highfields (N&S) and Barby Gate (N&S) Engagement activities are in progress, both with the Care Homes and GP Practices that support them, and so far 60% have either been meet or meetings are scheduled, with the remaining 40% homes and supporting practices to be contacted throughout June
None required. None required.
Green Green
6 | P a g e

Middleton Lodge practice raised concerns about care home staff at Pathfinders having access to patient data. A follow-up meeting has been arranged on the 16th June to review with GP colleagues to provide reassurance and seek agreement to engage and deploy the solution at Pathfinders A request will be issued to HSCIC later this month to register the ODS codes for all the Phase 1 Care Homes to the NHS Spine A similar request will also go to TPP to order the SystmOne units for each Phase 1 Care Home ready for deployment NHIS Business Relationship team are currently drafting a quotation for the ongoing support service that will form an integral part of the business case for subsequent CCG approval Benefits workshop to define KPI measures will take place on the 24th June Phase 1 deployments are planned to commence in July and finish by the end of August Phase 2 scope for the next batch of 10 Care Homes will be reviewed at team meeting scheduled for 23rd June
Cancer Earlier Diagnosis of Cancer – analysis of the impact of the national recommendations for early diagnosis
Dr Thilan Bartholomeuz/Julia King
'The Earlier Diagnosis workstream plans have been revised and prioritised in light of the RightCare CFV Cancer report released in May 2016. Priorities are confirmed as Lung and Lower GI. Vague Symptoms pilot and MDC/ MDT development Action plans remain in draft and subject to change and additions. The Early Diagnosis Clinical Reference Group has agreed the draft Vague Symptoms Pathway to be tested across Mid Notts and approved the N+S CCG Clinical Executive on 2nd June and noted at M+A on 9th June. Concerns noted that implementation may increase avoidable workload for GPs and diagnostics. A range of KPIs to support the pilot were agreed in principle locally and with EMSCN on 7th June. SFHFT have commenced base lining against some of the idenitified KPIs. Further work is needed and therefore it has been agreed to undertake a 'pathway and information' stocktake across Mid Notts at the end July /early Aug to refine the KPI requirements, inform the EMSCN data collection systems needed to monitor the impact and evaluation of the pilot and support decisions regarding use of the grant from EMSCN to support the programme. For review of progress on 15 June. Workstream action plans have been refreshed follwing update from the
None required.
Green
7 | P a g e

Cancer Pathways - phased programme of redesign and risk stratification of key tumour site
Dr Thilan Bartholomeuz/Julia King
RightCare to be signed off at the July Steering Group. Activity and finance modelling underway - further development and refinement needed, due to complexity of the impact of the pathway on diagnostics, FOPA, OPAFU and Primary Care costs. EMSCN leading this work - coordination needed with local CCGs. Diagnostic acvitity modelling for Direct Access CT, USS and XR to be tested as part of the pilot. Cancer Research UK and CCG to meet on 20th June to plan a shared resource agreement to deliver Primary Care support to deliver improved pick up of cancer screening, data collection and education and learning in Primary Care. Right Care packs published in May confirmed the priorities previously agreed within the Cancer programme. The order of pathway review has been revised in light of the data and information available. a joint approach to review of UGI and LGI diagnostic pathways will be considered together where possible, due to the complexity of the pathways for patients with difficult to diagnose primary. The diagnostic pathway developments will work closely with the emerging vague symptoms pathways, to develop optimum diagnostic pathways where possible. Lung will also remain a priority for the programme, with a specific focus on enhanced supportive care recommendations, to ensure coordinated care for patients diagnosed with lung cancer, reduction in emergency admissions, LoS, preferred place of care and potential to deliver Nurse led FU. Breast Cancer remains a priority, however, the MDTs at SFHFT and NUH will be combined as part of the Partnership and therefore, review of Breast pathways will be held until the merger is completed. The partnership board will support the development of coordinated pathway developments between NUH and SFHFT. Revised workstream briefs will be shared with the Partnership Board at their July meeting, to gain final agreement from both Trusts. Base lining of the pathways is underway at SFHFT. Agreement in principle reached to align Pathways Programme at NUH with priorities for Mid Notts. The Pathways Workstream Group at the May meeting agreed therefore to develop a phased approach to Pathways development, commencing with LGI /UGI and Lung, with Urology and Breast for ongoing review of opportunity to commence work. Redesign will consider 3 areas: Delivery of 62 day treatment pathways
None required.
Green
8 | P a g e
Living with Cancer - deliver coordinated care through systematic assessment, care planning and proactive care for patients from the point of diagnosis, through their cancer pathway
Dr Thilan Bartholomeuz/Julia King
(approved by the EMSCN - base lining complete and planning underway), Risk stratification of follow up pathways and integration with community / primary care service developments, underpinned by Self Care) and review of place of care and other recommendations highlighted within Lung supportive care report published in April. Last Living with Cancer meeting held 11th May 2016. Next meeting scheduled 22nd June 2016 Action plan progress reviewed, including milestones and risks Exploring feasibility of access to HNA systems, to support pilot of eHNA in primary care. Meeting with SFHFT to consider opportunities for roll out of HNA/ eHNA Further revision of survivorship patient questionnaire underway, for review at next meeting Health & Wellbeing workshop in planning, to engage stakeholders across the system in developing health & wellbeing survivorship agenda, and integrating supported self-care as part of cancer pathways. Planning continues for Health & Wellbeing workshop on 5.7.16. Current sign up lower than anticipated. Planning team has revised format to facilitate better attendance amongst staff with clinic commitments. Participation in patient forums and engagement sessions to promote cancer programme, e.g. carer roadshow Review of evaluation tools ongoing, with intention to hold wider appraisal meeting with partners Draft KPIs proposed, to be reviewed by the group and feedback shared at next meeting
None required.
Green
Workforce -
Peter Wozencroft/Charlotte Lawson/David Ainsworth
A Nottinghamshire wide workforce group has been established and brings together the Greater Nottinghamshire and Mid Nottinghamshire transformation Programmes. The scope of the programme is to develop, plan and deliver an integrated workforce development and organisational development strategy that supports both transformational programmes. The programmes will also co-ordinate activities with the Vanguards to ensure there is coherent and integrated approach across the transformation agenda. The first meeting of the Nottinghamshire Workforce Transformation Delivery Group was held 13th May 2016. Membership and Terms of reference for the
None required. Amber
9 | P a g e

group were agreed. A review of the Mid Notts GP workforce data submitted as part of the national collection has been undertaken. The information highlighted a number of issues:
- GP age profile – circa 30% - Nurse age profile - Gender split of GPs - In complete data returns
A local task and finish group has been established to consider what additional information is required to help and inform workforce actions that will support primary and community care across Mid Nottinghamshire.
10 | P a g e
1
June 2016
1
PROGRAMME STOCK TAKE

2
2 Programme Stocktake – update
Board Members are asked to note the following: • Programme Stocktake graphs have been updated to include the April
2016 activity data
• Next month a revised set of graphs will be presented aligning the Better Together system objectives with the 16/17 QIPP / transformation plans using month 2 actuals

KPI & Benefit Tracking OBJECTIVE 1- 15.1% REDUCTION IN A&E ATTENDANCES
3
Observations The chart above shows the detail of ED attendances data for the Mid Notts CCGs with FY 14 actuals (baseline) and target trend lines, showing the current year compared with the targets for the FY15 and the CCG 5 year target. • The dotted redline shows the CCG 5yr Strategic Objective as per the original model. • The dotted black line shows our FY14 actuals which is our baseline for the model
Go Live Dates Social Marketing & Communications: Urgent Primary Care: Care Navigator : Readmission reduction:
Readmission reduction Social MarketingCare Navigator
Urgent Primary Care
7,000
8,000
9,000
10,000
11,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Go-Live 2015
FY14(Baseline)
FY15
FY15 Target
5yrs Target

KPI & Benefit Tracking OBJECTIVE 2 - 19.5% REDUCTION IN EMERGENCY ADMISSIONS
4
Observations The chart above shows the detail of Emergency Admissions data for the Mid Notts CCGs with FY 14 actuals (baseline) and target trend lines, showing the current year compared with the targets for FY15 and the CCG 5 year target. • The dotted red line shows the CCG 5yr Strategic Objective as per the original model
Go Live Dates Social Marketing & Communications: Urgent Primary Care: Care Navigator : Single Front Door:
Readmission reduction SFD Social MarketingCare NavigatorUrgent Primary Care
1,500 1,700 1,900 2,100 2,300 2,500 2,700 2,900 3,100 3,300 3,500
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Go-Live2015FY14(Baseline)FY15
FY15 Target
5yrs Target
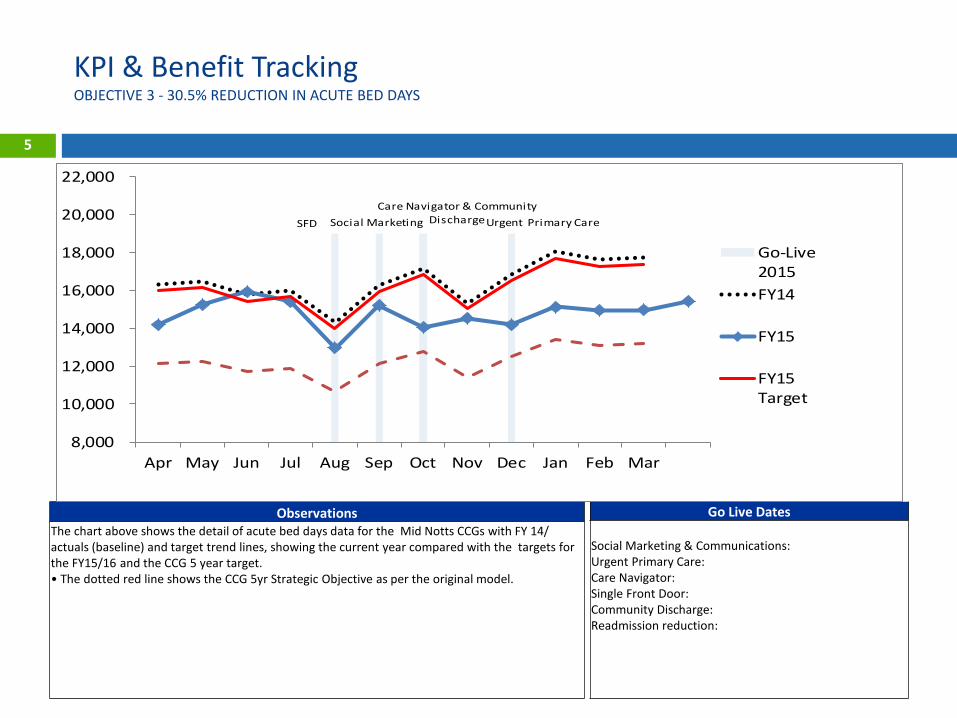
KPI & Benefit Tracking OBJECTIVE 3 - 30.5% REDUCTION IN ACUTE BED DAYS
5
Observations The chart above shows the detail of acute bed days data for the Mid Notts CCGs with FY 14/ actuals (baseline) and target trend lines, showing the current year compared with the targets for the FY15/16 and the CCG 5 year target. • The dotted red line shows the CCG 5yr Strategic Objective as per the original model.
Go Live Dates Social Marketing & Communications: Urgent Primary Care: Care Navigator: Single Front Door: Community Discharge: Readmission reduction:
SFD Social MarketingCare Navigator & Community
DischargeUrgent Primary Care
8,000
10,000
12,000
14,000
16,000
18,000
20,000
22,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Go-Live2015FY14
FY15
FY15Target
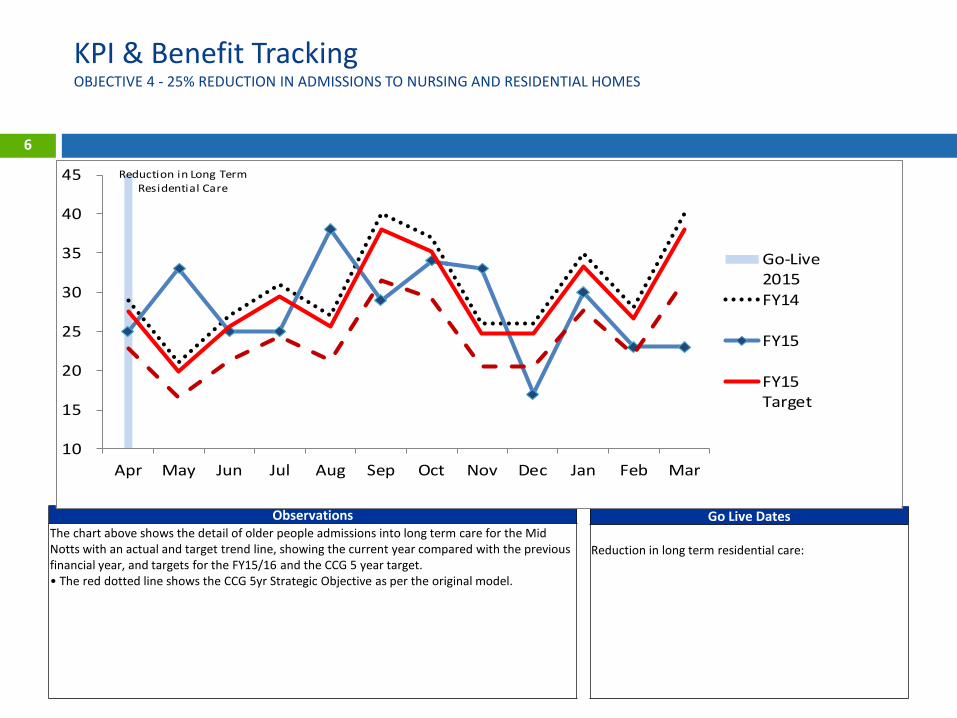
KPI & Benefit Tracking OBJECTIVE 4 - 25% REDUCTION IN ADMISSIONS TO NURSING AND RESIDENTIAL HOMES
6
Observations The chart above shows the detail of older people admissions into long term care for the Mid Notts with an actual and target trend line, showing the current year compared with the previous financial year, and targets for the FY15/16 and the CCG 5 year target. • The red dotted line shows the CCG 5yr Strategic Objective as per the original model.
Go Live Dates Reduction in long term residential care:
Reduction in Long Term Residential Care
10
15
20
25
30
35
40
45
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Go-Live2015FY14
FY15
FY15Target
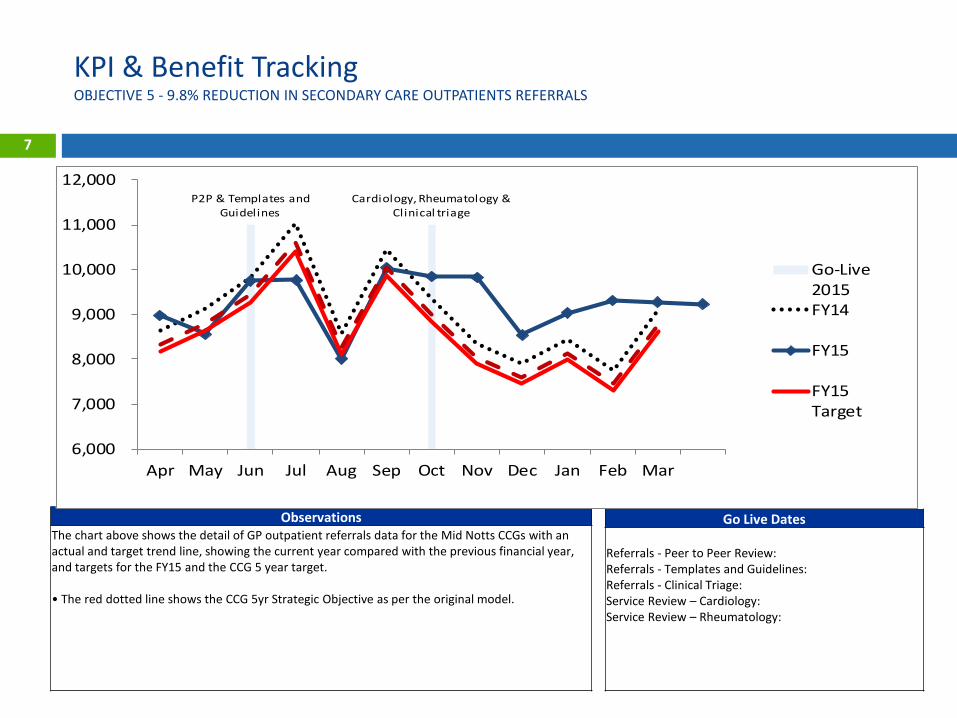
KPI & Benefit Tracking OBJECTIVE 5 - 9.8% REDUCTION IN SECONDARY CARE OUTPATIENTS REFERRALS
7
Observations The chart above shows the detail of GP outpatient referrals data for the Mid Notts CCGs with an actual and target trend line, showing the current year compared with the previous financial year, and targets for the FY15 and the CCG 5 year target. • The red dotted line shows the CCG 5yr Strategic Objective as per the original model.
Go Live Dates Referrals - Peer to Peer Review: Referrals - Templates and Guidelines: Referrals - Clinical Triage: Service Review – Cardiology: Service Review – Rheumatology:
P2P & Templates and Guidelines
Cardiology, Rheumatology & Clinical triage
6,000
7,000
8,000
9,000
10,000
11,000
12,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Go-Live2015FY14
FY15
FY15Target
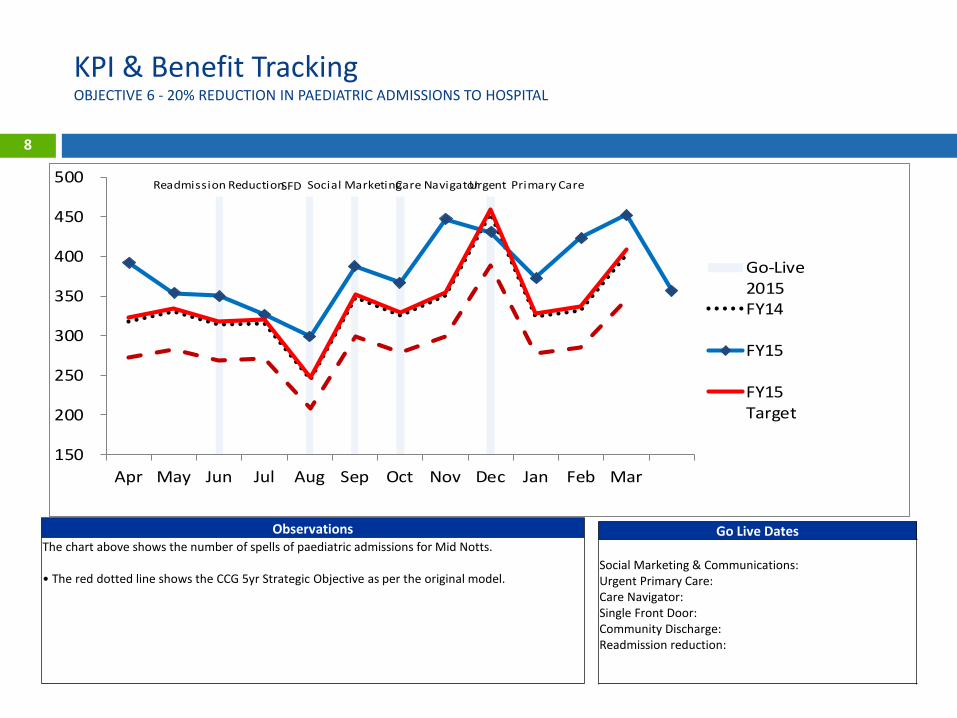
KPI & Benefit Tracking OBJECTIVE 6 - 20% REDUCTION IN PAEDIATRIC ADMISSIONS TO HOSPITAL
8
Observations The chart above shows the number of spells of paediatric admissions for Mid Notts. • The red dotted line shows the CCG 5yr Strategic Objective as per the original model.
Go Live Dates Social Marketing & Communications: Urgent Primary Care: Care Navigator: Single Front Door: Community Discharge: Readmission reduction:
Readmission ReductionSFD Social MarketingCare NavigatorUrgent Primary Care
150
200
250
300
350
400
450
500
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Go-Live2015FY14
FY15
FY15Target
KPIs split by CCG
9
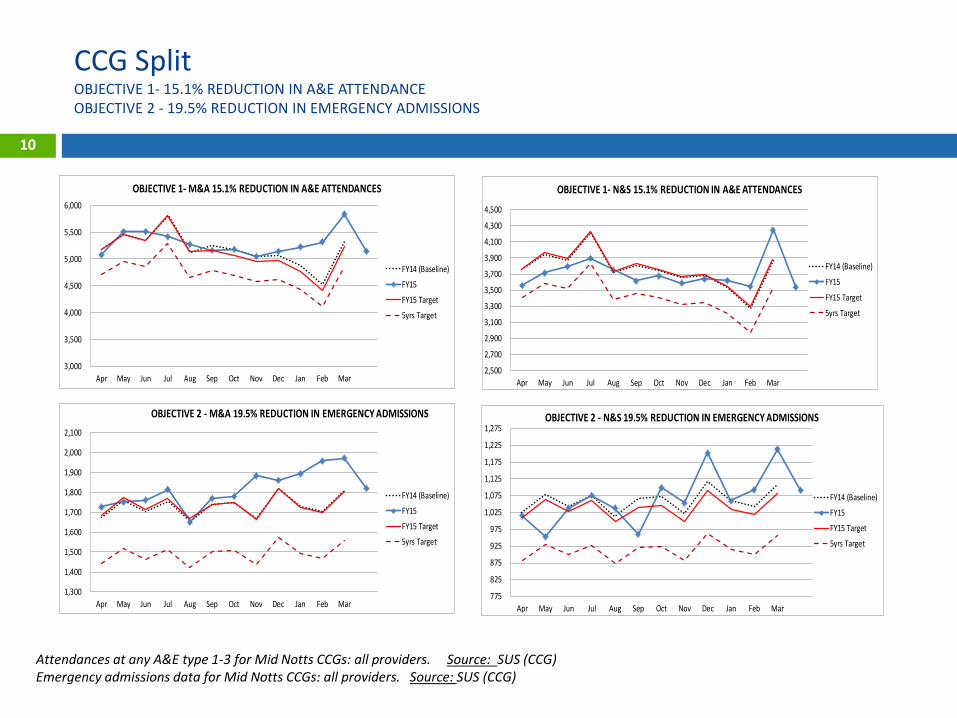
CCG Split OBJECTIVE 1- 15.1% REDUCTION IN A&E ATTENDANCE OBJECTIVE 2 - 19.5% REDUCTION IN EMERGENCY ADMISSIONS
10
Attendances at any A&E type 1-3 for Mid Notts CCGs: all providers. Source: SUS (CCG) Emergency admissions data for Mid Notts CCGs: all providers. Source: SUS (CCG)
3,000
3,500
4,000
4,500
5,000
5,500
6,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
OBJECTIVE 1- M&A 15.1% REDUCTION IN A&E ATTENDANCES
FY14 (Baseline)
FY15
FY15 Target
5yrs Target
2,500
2,700
2,900
3,100
3,300
3,500
3,700
3,900
4,100
4,300
4,500
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
OBJECTIVE 1- N&S 15.1% REDUCTION IN A&E ATTENDANCES
FY14 (Baseline)
FY15
FY15 Target
5yrs Target
1,300
1,400
1,500
1,600
1,700
1,800
1,900
2,000
2,100
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
OBJECTIVE 2 - M&A 19.5% REDUCTION IN EMERGENCY ADMISSIONS
FY14 (Baseline)
FY15
FY15 Target
5yrs Target
775
825
875
925
975
1,025
1,075
1,125
1,175
1,225
1,275
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
OBJECTIVE 2 - N&S 19.5% REDUCTION IN EMERGENCY ADMISSIONS
FY14 (Baseline)
FY15
FY15 Target
5yrs Target

11
CCG Split OBJECTIVE 3 - 30.5% REDUCTION IN ACUTE BED DAY OBJECTIVE 4 - 25% REDUCTION IN ADMISSIONS TO NURSING AND RESIDENTIAL HOMES
Number of non-elective bed days at Mid Notts. Source: Medway PAS (SFH) The number and proportion of people who were still at home 91 days after discharge from hospital into re-ablement / rehabilitation services. Source: Notts County Council
6,500
7,500
8,500
9,500
10,500
11,500
12,500
13,500
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
OBJECTIVE 3 -M&A 30.5% REDUCTION IN NON-ELECTIVE ACUTE BED DAYS
FY14
FY15
FY15 Target
5yrs Target
2,500
3,000
3,500
4,000
4,500
5,000
5,500
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
OBJECTIVE 3 -N&S 30.5% REDUCTION IN NON -ELECTIVE ACUTE BED DAYS
FY14
FY15
FY15 Target
5yrs Target
5
10
15
20
25
30
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
OBJECTIVE 4 - M&A 25% REDUCTION IN ADMISSIONS TO NURSING AND RESIDENTIAL HOMES
FY14
FY15
FY15 Target
5yrs Target
-
2
4
6
8
10
12
14
16
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
OBJECTIVE 4 - N&S 25% REDUCTION IN ADMISSIONS TO NURSING AND RESIDENTIAL HOMES
FY14
FY15
FY15 Target
5yrs Target

CCG Split OBJECTIVE 5 - 9.8% REDUCTION IN SECONDARY CARE OUTPATIENTS REFERRALS OBJECTIVE 6 - 20% REDUCTION IN PAEDIATRIC ADMISSIONS TO HOSPITAL
12
Number of referrals from Mid Notts GPs to Outpatient services: all providers. Source: SUS (CCG) Number of paediatric admission spells at SFHFT. Source: Medway PAS (SFH)
3,000
3,500
4,000
4,500
5,000
5,500
6,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
OBJECTIVE 5 - M&A 9.8% REDUCTION IN SECONDARY CARE OUTPATIENTS REFERRALS
FY14
FY15
FY15 Target
5yrs Target
Target Split: 53%
2,000
2,500
3,000
3,500
4,000
4,500
5,000
5,500
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
OBJECTIVE 5 - N&S 9.8% REDUCTION IN SECONDARY CARE OUTPATIENTS REFERRALS
FY14
FY15
FY15 Target
5yrs Target
-
50
100
150
200
250
300
350
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
OBJECTIVE 6 - M&A 20% REDUCTION IN PAEDIATRIC ADMISSION TO HOSPITAL
FY14
FY15
FY15 Target
5yrs Target
-
20
40
60
80
100
120
140
160
180
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
OBJECTIVE 6 - N&S 20% REDUCTION IN PAEDIATRIC ADMISSIONS TO HOSPITAL
FY14
FY15
FY15 Target
5yrs Target