Dalle linee guida dell'epatocarcinoma alla pratica clinica - Gastrolearning®
87
Corso “Gastrolearning” Bologna, 20 Maggio 2013 Linee guida AISF Franco Trevisani Semeiotica Medica Dipartimento di Scienze Mediche e Chirurgiche Alma Mater Studiorum - Università di Bologna
-
Upload
gastrolearning -
Category
Education
-
view
1.298 -
download
5
description
Gastrolearning XVI lezione Dalle linee guida dell'epatocarcinoma alla pratica clinica - Prof. F. Trevisani (Università di Bologna).
Transcript of Dalle linee guida dell'epatocarcinoma alla pratica clinica - Gastrolearning®

Corso
“Gastrolearning”Bologna, 20 Maggio 2013
Linee guida AISFFranco Trevisani
Semeiotica Medica
Dipartimento di Scienze Mediche e Chirurgiche
Alma Mater Studiorum - Università di Bologna

2012
2010

Adjuvant therapy after resectionOLT-extended
Neoadjuvant therapy in waiting list
LDLT
Downstaging
Internal radiation Y90
Resection
Levels of evidence
(NCI)
Grade of recommendation(GRADE)
1
2
3
2 (weak) 1 (strong)
RF (<5 cm), RF/PEI (<2 cm)
Chemoembolization
External/palliative radiotherapy
Sorafenib
AC BAC B
OLT-Milan
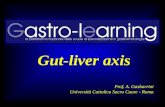
EASL–EORTC Clinical Practice Guidelines: Management of hepatocellular carcinoma. Journal of Hepatology 2012 vol. 56 j 908–943
Levels of evidence and grade of raccomandation

Sorveglianza del paziente a rischio di HCC

Surveillance for HCC: the RCT
Zhang BH, et al. J Cancer Res Clin Oncol. 2004;130:417-22
18,816 patients with HBsAg+ chronic hepatitis
9,373AFP + US (semi-annual)
9,443No surveillance
86 67HCC
83/100,000 131/100,000 HCC mortality
HCC mortality rate ratio:0.63 (95% CI 0.41–0.98)
- Compliance 58%- LT not available
AFP = alpha-fetoprotein;RCT = randomized controlled trial; US = ultrasonography.

205 cirrhotic patients (Child–Pugh A/B)
Decision aid paper
Surveillance for HCC in cirrhosis: unfeasibility of RCT when informed consent is given
Poustchi H, et al. Hepatology ,2010; 54: 1998–2004 [Epub ahead of print 2011 July 28]
181chose
surveillance
21continued their
usual care
2were
undecided
6 mo. US + 3 mo. AFPvs
no surveillance
204 pts. (99.5%)declined randomization
This topic can be only addressed with carefully conducted cohort studies

Surveillance for HCC in cirrhosis: survival in cohort studies
De Masi S, et al. Dig Liver Dis. 2005;37:260-8.
Cirrhosis 3-year survival rate
Kemp, 2005Australia
HCV, HBV, alcohol
Retrospective US 6–12 m 41 55 38% 19% 329 days(median)
Toyoda, 2006Japan
HCV, HBV Retrospective US + AFP + DCP
1,050 591 36% 19%
Stravitz, 2008USA
HCV, acohol Retrospective US (others) 12 m
172 107 40% 13% 916 days(median)
Kuo, 2010Taiwan
HBV, HCV Retrospective US ≤12 m 318 1118 59% 29%
Kemp W, et al., J Gastroenterol Hepatol. 2005;20:873-8. Toyoda H, et al., Clin Gastroenterol Hepatol. 2006;4:1170–6. Stravitz RT, et al., Am J Med. 2008 Feb;121:119-26. Kuo Y-H, et al., Eur J Cancer 2010; 46:744-51

Surveillance for HCC in cirrhosis: survival in cohort studies
De Masi S, et al. Dig Liver Dis. 2005;37:260-8.
Lead time

Surveillance for HCC

Pazienti candidati alla sorveglianza
AISF position paper, Digest Liver Dis, 2013

Subject to PATH Program Disclaimer
Effect of surveillance on survival (adjusted for the “lead time”) in cirrhosis
Child–Pugh CChild–Pugh B
Trevisani F et al., for ITA.LI.CA. Am J Gastroenterol 2002;97:734-44Trevisani F et al., for ITA.LI.CA. Am J Gastroenterol 2007;102:2448-57
Surveillance
No surveillance
Lead time
Child–Pugh A

Pazienti candidati alla sorveglianza
AISF position paper, Digest Liver Dis, 2013

Baseline HBV-DNA level and risk of HCC in chronic hepatitis B
Chen et al., JAMA 2006
<10˙000 c/mL
1˙000˙000 c/mL
>1˙000˙000 c/mL
100˙000 c/mL
At entry:- HBeAg neg.- Normal ALT- No cirrhosis
HBV-DNA (c/mL) Annual incidence of HCC (%)
<10,000 0.11
10,000-99,9999 0.29
100,0000-999,9999 0.96
≥1 Million 1.15

Yang HI, et al. Lancet Oncol. 2011;12:568-74.
Risk estimation for hepatocellular carcinoma in chronic hepatitis B (REACH-B):
development and validation of a predictive score
12 months
6 months

Pazienti candidati alla sorveglianza
AISF position paper, Digest Liver Dis, 2013

HCC risk in non-cirrhotic HCV+ patients
Lok AS, et al. Gastroenterology. 2009;136:138-48.
0.8% / year
1.4% / year

HCC risk in non-cirrhotic populations
Masuzaki R, et al. Hepatology, 2009:49:1793-4
Liver stiffness (kPa) Hazard ratioAnnual incidence
of HCC (%)
≤ 10 1 0.1
10.1–15 16.7 2.9
15.1–20 20.9 5.0
20.1–25 25.6 8.3
> 25 45.5 14.4
Prospective study with elastography (FibroScan®) 866 patients anti-HCV+
Cirrhosis: 13–17 kPa
Starting pointfor
surveillance?

Pazienti candidati alla sorveglianza

Rischio HCC in pazienti divenuti non viremici
HBV
HCV
Aghemo et al., J Hepatol 2012;57:1326-35

Surveillance for HCC: how?
The popularity of US relies on the absence of risk, non-invasiveness,easy accessibility, and relatively moderate cost
Bruix J, Sherman M. Hepatology. 2011;53:1020-2Raccomadazioni AISF 2012; www.webaisf.org
EASL-EORTTC guidelines. J Hepatol 2012; 56; 908–943
Surveillance with US should be performed by an experienced operator (evidence 5, strengh D).

Pooled sensitivity of ultrasoundultrasound for early stageearly stage HCC HCC
Surveillance for HCC: how?
Singal A, et al. Aliment Pharmacol Ther 2009;30:37-47

Pooled sensitivity of ultrasound ultrasound for early stage HCCearly stage HCC
Pooled sensitivity of ultrasound + AFP ultrasound + AFP forearly stage HCCearly stage HCC
Sensitivity: + 6%
Surveillance for HCC: is US plus AFP better?
Singal A, et al. Aliment Pharmacol Ther 2009;30:37-47

Sensitiv. False + PPV
• US 84% 2.9% 6.6%
• US + AFP 92% 7.5% 3.0%
• AFP 69% 5.0% 3.3%
Semi-annual surveillance of 9,373 patients with HBsAg+ or with chronic hepatitis
+ 8%
Zhang B, Yang B. J Med Screen 1999;6:108-10
PPV = positive predictive value.
Alpha-fetoprotein as surveillance test

Cost for each small HCC detected
(USA $)
• US 1,980
• US + AFP 3,640 (+84%)
• AFP 3,030 (+53%)
Alpha-fetoprotein as surveillance test
Semi-annual surveillance of 9,373 patients with HBsAg+ or with chronic hepatitis
Zhang B, Yang B. J Med Screen 1999;6:108-10

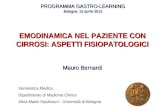
Sensitivity of US-based surveillancefor early HCC early HCC by interval (6 vs 12 months)
Meta-regression
Singal A, et al. Aliment Pharmacol Ther 2009;30:37-47

Distribution of HCC staging according to the surveillance interval (6 vs 12 months)
Retrospective study on 634 patients with Child–Pugh class A/B cirrhosis
HCC (number and )6 months
(497 patients)
12 months
(137 patients)
Single ≤ 2 cm (very early) 120 (24%) 7 (5%)
Single 2.1–3 cm (early) 94 (19%) 22 (16%)
Single 3.1–5 cm (early) 61 (13%) 30 (22%)
2–3 x ≤ 3 cm (early) 73 (15%) 20 (15%)
Milan out 149 (30.0%) 58 (42%)
p < 0.001
STAGE
M IGRAT ION
Santi V et al., for ITA.LI.CA, J Hepatol 2010;53:291-7

Survival according to the surveillance interval (6 vs 12 months)
Corrected (for the lead time) survival
Sensitivity analysis: semi-annual is superior to annual program in patients witha tumor volume doubling time 147 days
Observed survival
Santi V et al., for ITA.LI.CA, J Hepatol 2010;53:291-7
Retrospective study on 634 patients with Child–Pugh class A/B cirrhosis

Politica di richiamo(diagnosi)

* OneOne imaging technique only in centers of excellence with high-end radiological equipmentin centers of excellence with high-end radiological equipment.
** HCC radiological hallmark: arterial hypervascularity and venous/late phase washout
Mass/nodule on US
< 1 cm 1-2 cm > 2 cm
4-phase CT or DynamicContrast enhanced MRI
4-phase CT/DynamicContrast enhanced MRI
Repeat US at 4 mo
Growing/ChangingCharacter
Stable
1 or 2 positive techniques*:HCC radiological Hallmarks**
1 positive technique:HCC radiological Hallmarks**
Yes No
HCC Biopsy
Investigate according to size
Inconclusive
Yes No
HCC Biopsy
EASL–EORTC Clinical Practice Guidelines: Management of hepatocellular carcinoma. J Hepatol 2012; 56; 908–943
Diagnostic recall policy
?

Algoritmo diagnostico raccomandazioni AISF
Nuovo nodulo in cirrosi
Aumento (Ø > 1 cm)
NO Sì
Ecografia/3 mesi
Ø < 1 cm
Aumento (Ø > 1 cm)
Ecografia/3 mesi (per 12 mesi)
NO
Ecografia/6 mesi
Sì
HCC
Non diagnostica
Ø > 1 cm
Aspetto atipico
Altra metodica contrastografica
Aspetto tipico (wash-in e wash-out)
NO Sì
Aspetto tipico
Biopsia
TC, RM, CEUS
Altra diagnosi
AISF position paper, Digest Liver Dis, 2013

Efficacy vs effectiveness of surveillance
Efficacy (mortality reduction) H R 3-year - ITA.LI.CA (Am J Gastroenterol, 2002) 41% -
- Kemp et al. (J Gastroent Hepatol,2005) 76% 100%- Bolondi et al. (Gut, 2001) - 42%- Toyoda et al. (Clin Gastroenterol Heptol, 2008) - 89%- Kuo et al. (Eur J Cancer, 2010) -103%
Determinants of Effectiveness - Doctor recommendation 80%- Patient acceptance 90%- Patient adherence 80%- Proper recall policy 80%- Timely available diagnostic and therapeutic options 80%
Effectiveness: 40% x 0.8 x 0.9 x 0.8 x 0.8 x 0.8 = 15%80% x 0.8 x 0.9 x 0.8 x 0.8 x 0.8 = 29%

Stadiazione e prognosi

Portal pressure/bilirubin
HCC
PEI/RFA Sorafenib
Stage 0PST 0, Child–Pugh A
Very early stage (0) 1 HCC < 2 cm
Carcinoma in situ
Early stage (A)1 HCC or 3 nodules
< 3 cm, PST 0
End stage (D)
Liver transplantation TACEResection
Curative treatments (30%)5-year survival (40–70%)
Target: 20%OS: 20 mo (45-14)
Associated diseases
YesNo
3 nodules ≤ 3 cm
Increased
Normal
1 HCC
Stage DPST > 2, Child–Pugh C
Intermediate stage (B)Multinodular,
PST 0
Advanced stage (C) Portal invasion, N1, M1, PST 1–2
Stage A–CPST 0–2, Child–Pugh A–B
EASL–EORTC Clinical Practice Guidelines: Management of hepatocellular carcinoma. Journal of Hepatology 2012 vol. 56 j 908–943
Target: 40%OS: 11 mo (6-14)
Best supportivecare
Target: 10%OS: <3 mo
Updated BCLC staging system and treatment strategy
PST 0-1

PERFORMANCE STATUS(Eastern Cooperative Oncology Group)
Grade ECOG
0 Fully active, able to carry on all pre-disease performance without restriction
1 Restricted in physically strenuous activity but ambulatory and able to carry out work of a light or sedentary nature, e.g., light house work, office work
2 Ambulatory and capable of all selfcare but unable to carry out any work activities. Up and about more than 50% of waking hours
3 Capable of only limited selfcare, confined to bed or chair more than 50% of waking hours
4 Completely disabled. Cannot carry on any selfcare. Totally confined to bed or chair
5 Dead
Oken, et al., Am J Clin Oncol 5:649-655, 1982

Terapia

Portal pressure/bilirubin
HCC
PEI/RFA Sorafenib
Stage 0PST 0, Child–Pugh A
Very early stage (0) 1 HCC < 2 cm
Carcinoma in situ
Early stage (A)1 HCC or 3 nodules
< 3 cm, PST 0
End stage (D)
Liver transplantation TACEResectionResection
Curative treatments (30%)5-year survival (40–70%)
Target: 20%OS: 20 mo (45-14)
Associated diseases
YesNo
3 nodules ≤ 3 cm
Increased
Normal
1 HCC
Stage DPST > 2, Child–Pugh C
Intermediate stage (B)Multinodular,
PST 0
Advanced stage (C) Portal invasion, N1, M1, PST 1–2
Stage A–CPST 0–2, Child–Pugh A–B
EASL–EORTC Clinical Practice Guidelines: Management of hepatocellular carcinoma. Journal of Hepatology 2012 vol. 56 j 908–943
Target: 40%OS: 11 mo (6-14)
Best supportivecare
Target: 10%OS: <3 mo
Updated BCLC staging system and treatment strategy
PST 0-1

Resection for HCCOnly single? Only without PHT
Ishizawa et al., Gastro 2008
CPA = Child Pugh Class ACPB = Child Pugh Class BPHT = Portal Hypertension

Resection for HCC The Bologna experience
P=0.008
241 pts.
156 pts.

BCLC-AASLD-EASL Staging System and Treatment Schedule
Assume i fattori prognostici negativi come “controindicazioni” a un trattamento

MELD score
9 - 10
Serum sodium level
Cirrhotic patient eligible for liver resection
≥ 140 mEq/L < 140 mEq/L
Segmentectomy or bisegmentectomy
Segmentectomy or limited resection
Major hepatectomy (up
to 4 segments)
Risk of IPLF>15% in all types of
hepatectomy
>10<9
Algoritmo per candidare alla resezione epatica il paziente con HCC
0 - 3.3% 0 – 2.5%0Mortalità
AISF position paper, Digest Liver Dis, 2013

Algoritmo per candidare alla resezione epatica il paziente con HCC
Ascites, Bilirubin, Indocianine green retention rate at 15 min
Imamura H et al, J Hepatobiliary Pancreat Surg. 2005:16-22
A
B
I

ResectionAblation
Is there a winner?

RF results in Child-Pugh A patients with a single HCC 2 cm
Livraghi et al., Hepatology 2008
Mortality 0
Major complications 1.8% (1 seeding case)
Complete radiological necrosis - 1st course 86% - 2nd course 12% - Total 98%
Sustained complete response 97%(median follow-up 31 mo)
Treatment failure 3%
232 pts
218 pts
6 pts(2.6%)
unfeasibility

Survival of patients with single HCC <2 cm treated by ablation
Analysis by surgical candidacy (100 vs 118)
Livraghi et al., Hepatology 2008

Results of RF and resection in patients with very early HCC (single <2 cm)
Propensity analysis (resection 52 vs RF 9152)
Wang JH et al., J Hepatol 2011 [Epub haed of print]
One-to-one near-neighbor matching for: sex, age, HBsAg, anti-HCV, platelet, Child-Pugh, AFP, ALT, BMI, hypertension, diabetes.
• Negligible mortality• Lower liver mutilation • Lower costs• Shorter hospital stay• Easy repeatibility

Cho YK et al., Hepatology 2010; 51: 1284-90
In compensated cirrhosis, first-line RF (followed by resection if failure) is better than resection (followed by RF for recurrence)
if:
>>
>>
<

Cho YK et al., Hepatology 2010; 51:1284-90
Two-way sensitivity analysis:
HR mortality vs. local recurrence for overall mortality
HResectionRF (± HR)
2.5% increase in local recurrence = 1% increase in periop. Mortality

Tumor size and first-line treatment
≤ 2 cm
2.1- 3 cm
> 3 cm
RFA
Resection
AISF position paper, Digest Liver Dis, 2013

Portal pressure/bilirubin
HCC
PEI/RFA Sorafenib
Stage 0PST 0, Child–Pugh A
Very early stage (0) 1 HCC < 2 cm
Carcinoma in situ
Early stage (A)1 HCC or 3 nodules
< 3 cm, PST 0
End stage (D)
Liver transplantation TACEResection
Curative treatments (30%)5-year survival (40–70%)
Target: 20%OS: 20 mo (45-14)
Associated diseases
YesNo
3 nodules ≤ 3 cm
Increased
Normal
1 HCC
Stage DPST > 2, Child–Pugh C
Intermediate stage (B)Multinodular,
PST 0
Advanced stage (C) Portal invasion, N1, M1, PST 1–2
Stage A–CPST 0–2, Child–Pugh A–B
EASL–EORTC Clinical Practice Guidelines: Management of hepatocellular carcinoma. Journal of Hepatology 2012 vol. 56 j 908–943
Target: 40%OS: 11 mo (6-14)
Best supportivecare
Target: 10%OS: <3 mo
Updated BCLC staging system and treatment strategy
PST 0-1

Mazzaferro et al., Lancet Oncol 2009
1556 pts. from 36 centres (1122 Milano-out at pathology examination)5-year overall-survival
Linee guida: rapidi cambiamenti delle evidenze.Chi trapiantare?
1 5 1510 8520 25 30 35 504540 55 60 65 7570 80
Size of the largest tumor (mm)

Linee guida: rapidi cambiamenti delle evidenze. Criteri down-staging di Bologna
Down-staging:- 5.1-6 cm - 3.1-5 cm “Milano-in” dopo down-staging- ≤4 cm ciascuno, somma Ø 12 cm
0
20
40
60
80
100
0 12 24 36
Act
uari
al s
urvi
val (
%)
Milano-in Down-staging
Post-Tx (88 vs. 32 pts)
0
20
40
60
80
100
0 12 24 36
Act
uari
al s
urvi
val (
%)
Milano-in Down-staging
Intention-to-treat (129 vs. 48 pts)
Ravaioli et al., Am J Transplant 2008

Linee guida: rapidi cambiamenti delle evidenze. Criteri down-staging UCSF
Down-staging:- 8 cm - 5 cm ciascuno, somma Ø 8 cm - ≤ 3 cm ciascuno, somma Ø 12 cm
Yao et al., Hepatology 2008
Inizio down-staging

Multimodal treatment of HCC
OLT and neoadjuvant theraphy: the down-staging
Clavien et al., Lancet Oncol 2012; 13: 11-22

Multimodal treatment of HCC
OLT and neoadjuvant theraphy
AISF position paper, Digest Liver Dis, 2013

Portal pressure/bilirubin
HCC
PEI/RFA Sorafenib
Stage 0PST 0, Child–Pugh A
Very early stage (0) 1 HCC < 2 cm
Carcinoma in situ
Early stage (A)1 HCC or 3 nodules
< 3 cm, PST 0
End stage (D)
Liver transplantation TACEResection
Curative treatments (30%)5-year survival (40–70%)
Target: 20%OS: 20 mo (45-14)
Associated diseases
YesNo
3 nodules ≤ 3 cm
Increased
Normal
1 HCC
Stage DPST > 2, Child–Pugh C
Intermediate stage (B)Multinodular,
PST 0
Advanced stage (C) Portal invasion, N1, M1, PST 1–2
Stage A–CPST 0–2, Child–Pugh A–B
EASL–EORTC Clinical Practice Guidelines: Management of hepatocellular carcinoma. Journal of Hepatology 2012 vol. 56 j 908–943
Target: 40%OS: 11 mo (6-14)
Best supportivecare
Target: 10%OS: <3 mo
Updated BCLC staging system and treatment strategy
PST 0-1

HCC in stadio intermedioPaz. 58 aa, Child-Pugh A, MELD 9, PS 0, non invasione portale, N 0, M 0,
non comorbilità, varici F1.
6 cm
TACE (sempre?)
3.5 cm

Trattamento HCC in stadio BCLC intermedio
Lin et al., W J Surg 2010
Overall survivals adjusted for serum albumin (independent factor)in Hepatic Resection (n. 93) and TACE (n. 73) pts.
Child-Pugh A

Trattamento HCC in stadio BCLC intermedio
Vitale et al., Transplant Proc 2009
Surgical options: LT, resection, laparoscopic ablation
(124 pts.)
(91 pts.)

Trattamento HCC in stadio BCLC intermedio
Wang et al., Eur J Cancer 2008
Resection
TAE

Resection for HCC: an international study from referral centers Resection for HCC: an international study from referral centers (Asia, Europe, America)(Asia, Europe, America)
Trattamento HCC in stadio BCLC intermedio
Torzilli G et al., Ann Surg 2013 257; 929-37

RecommendationContraindications and specifications
BCLC stage B pts not eligible for surgery or ablation (1a-A).
Best candidates are asymptomatic (PS 0) Child-Pugh class A pts (1b-A);
Child-Pugh score of B7 or PS 1 can be considered (5-D)
Jaundice, untreatable ascites, portal or main branch thrombosis, hepatofugal portal flow, and HCC >10 cm
TACE can be utilized in pts with early stage HCC if surgical or ablative techniques are not applicable (technical reasons and/or comorbidities)
TACE should be performed with a selective or super-selective (segmental or sub-segmental) technique to optimize risk/benefit ratio and increase likelihood of complete response (2b-B)
For bi-lobar HCCs not treatable with a super-selective approach, treating a single lobe per session should be considered (5-D)
Peripheral, segmental or intra-tumoral thrombosis is not an absolute contraindication to TACE, and should be used in association with a systemic treatment (5-D)
Should be considered in the frame of controlled clinical studies
In absence of radiologic evidence of disease persistence (complete response), TACE should not be repeated, due to its risks, costs and impact on the pt’s quality of life. TACE should be repeated “on demand” (5-D)
2012 AISF recommendations forTACE in HCC
AISF position paper, Digest Liver Dis, 2013

HCC in stadio intermedio
Paz. 58 aa, Child-Pugh A, MELD 9, PS 0, non invasione portale, N 0, M 0, non comorbilità, varici F1.
TACE (sempre?)

Intermediate-stage HCC
ITA.LI.CA database 2008
The “real word” treatment in… ITA.LI.CA
324 intermediate (BCLC C) HCC pts.
124 TACE(38%)
18 TACE + PEI(5.5%)
85 curative treatments
(26.5%)
68 BSC(30%)
3-year survival: 32%
Mean survival:- Ablation 62 months (I.C. 43-82) - Surgery 42 months (I.C. 29-55) - TACE 37 months (I.C. 30-43)- BSC 27 months (I.C. 17-36)
(p<0,001)
Child A
Child BElderly

Quale trattamento per HCC intermedio?
SorafenibChemoembolizatio
nPEI/RFA
Liver transplantation
(CLT/LDLT)
Resection
Curative treatments
HCC
Stage A–COkuda 1–2, PS 0–2, Child-Pugh A–B
Stage 0PS 0, Child-Pugh A
Stage DPS >2, Child-Pugh C
Very early stage (0)
Single <2 cmcarcinoma in situ
Early stage (A)
1–3 nodules <3 cm, PS 0
Intermediate stage (B)
Multinodular,PS 0
Advanced stage (C)
Portal invasion, N1, M1, PS 1–2
End stage (D)
Single 3 nodules ≤3 cm
Portal pressure/bilirubin
Increased Associated diseases
Normal No Yes
Randomized controlled trialsSymptomatic
treatment

Criteri radiologici di valutazione della risposta al trattamento

1979 1992 2000 2001 2009 20102008
WHOHandbook for
reporting results of cancer treatment1
mWHOModified WHO
criteria2,3
RECISTResponse
Evaluation Criteria In Solid Tumors4
EASL criteriaConclusions from the Barcelona 2000 EASL
conference5
RECIST 1.1Revised RECIST
guidelines8
mRECIST for HCCProposed modifications to RECIST 1.1 for assessing
response in HCC6,7
EASL, European Association for the Study of the Liver; HCC, hepatocellular carcinoma; RECIST, Response Evaluation Criteria In Solid Tumors; WHO, World Health Organisation. 1. WHO 1979. Available at: http://whqlibdoc.who.int/offset/WHO_OFFSET_48.pdf; 2. Green S, et al. Invest New Drugs 1992;10:239-53; 3. P. TherasseAnn Oncol (2002) 13(suppl 4): 127-129 ; 4. Therasse P, et al. J Natl Cancer Inst 2000;92:205-16; 5. Bruix J, et al. J Hepatol 2001;35:421-30; 6. Llovet JM, et al. J Natl Cancer Inst 2008;100:698-791; 7. Lencioni R, et al. Semin Liver Dis 2010;30:52-60; 8. Eisenhauer EA, et al. Eur J Cancer 2009;45:228-47; 9. EASL-EORTC Guidelines. J Hepatology 2012;56:908-43
Guidelines for evaluating response to treatment in solid tumours have evolved
mRECISTEASL-EORTC HCC guideline9
2012

Conventional RECIST: longest overall tumor diameter
mRECIST:
longest viable tumor diameterLencioni R, Llovet JM. Semin Liver Dis. 2010;30:52–60.

RECIST vs mRECIST criteria
Dr. Golfieri (Bologna, Italy) has proposed a graphical representation of the change in tumour dynamic for RECIST vs mRECIST

TACE: concordance between EASL and mRECIST responses
Gillmore R, et al. J Hepatol 2011;55:1309–16;
Overall response (CR +PR), assessed at a median of 64 days after TACE, was:
- almost identical using EASL and mRECIST
- much better than that calculated with RECIST
•EASL: 58%
•mRECIST: 57%
•RECIST 1.1: 7%

TACE: prognostic power of the response according to the criteria utilized
EASL1 RECIST1mRECIST1
Survival similar with EASL and mRECIST, and better in pts. with an overall response, assessed at an early time point (median 64 days)1:
Responder Non-responders P•EASL: 22.0 months 12.7 months 0.019
•mRECIST: 20.7 months 13.3 months 0.009
•RECIST 1.1: 12.4 months 16.8 months n.s
1. Shim et al. Radiology 2012;262(2):708-18; 2. Llovet JM, Ducreux M, et al. J Hepatol. 2012;56:908-943

TACE: concordance between EASL and mRECIST responses
Retrospective analysis: 332 patients in Korea treated with TACE1
– CP-A liver function and BCLC-B disease prior to treatment•Excellent agreement between EASL and mRECIST
– κ value of 0.94 (95% CI: 0.91-0.97)•Poor correlation between WHO and RECIST vs enhancement criteria
– κ value of <0.20 for both comparisons
EASLRECIST mRECIST
1. Shim et al. Radiology 2012;262(2):708-18; 2. Llovet JM, Ducreux M, et al. J Hepatol. 2012;56:908-943
WHO
OS according to:
EASL-EORTC and AISF guidelines recommend mRECIST criteria for assessment of response in HCC2

http://www.webaisf.org/

RECIST vs. mRECIST with Sorafenib
Edeline J et al., Cancer 2011;118:147–56
Before After rafenib
RECIST
mRECIST

Quando continuare e quando fermarsi con la TACE?
Proposta di un algoritmo AISF «razionale»

* percorso valido per ogni seduta di TACE; ** :i caso di cTACE è preferibile RM, in quanto alla TC l’accumulo di lipidol può “mascherare un’attività residua di malattia
*** risposta al trattamento definita secondo i criteri RECIST modificati [CR: risposta completa; PR: risposta parziale; SD: malattia stabile (si intende nessuna modificazione favorevole della lesione trattata); DP: progressione di malattia.
HCC CANDIDATO A TACEHCC CANDIDATO A TACE- No trombosi portale (ammessa trombosi di ramo segmentario)
- No malattia extraepatica- Classe di Child Pugh A o B7
Deterioramento epatico,complicazioni maggiori *
CR ***
RM o TCtrimestrale
Recidiva di malattia ***PR ***
RisoluzioneNo
PalliazioneSì
Progressione di malattia(DP) o non risposta altrattamento (SD) ***
Nuova lesione
Crescita lesionitrattate o SD***
ConsideraSORAFENIB
Considera nuovo trattamento(cTACE o DEB-TACE)
Trattamento cTACE o DEB-TACE
RM o TC **(dopo 1 mese)
Trattamento cTACE o DEB-TACE
RM o TC **(dopo 1 mese)
AISF position paper, Digest Liver Dis, 2013

Trattamenti combinati/sequenziali

Per-nodule response rate to the 1st TACE: the role of tumour size
• Retrospective cohort study: 271 patients eligible to TACE with 635 treated nodules• cTACE* performed ‘on demand’ upon demonstration of viable tumour (non-CR)• Tumour assessment according to mRECIST (after 1 month and then every 3–4 months)• Mean follow-up: 12 months (range 1-51)
CR, complete response; PR, partial response;; TACE, transarterial chemoembolization *cTACE was 50 mg doxorubicin + Spongel; superselective technique where possible Golfieri R et al., JVIR 2013
Tumor diameter ≤2 cm (N=386) 2.1-5 cm (N=211) >5 cm (N=36)
N. nodes % N. nodes % N. nodes %
Tumour response
CR 263 68 134 64 9 25
PR 123 32 77 36 27 75
Local Recurrence Rate 52 20 36 27 6 57
Only 25% of large (>5 cm) nodules achieve CR and, in these nodules, local relapse is very frequent.

Trattamenti locoregionali combinati
Marelli L et al., Cancer Treatment Rev 2006; 32:594-606
OR = 0.53 (95% CI = 0.29-0.99)

Trattamenti locoregionali combinati
Wang W et al., Liver International 2010; 30: 741-749
Sopravvivenza a: - 1 anno: 512 paz. → OR = 3.26 (95% CI = 1.23-8.69) - 2 anni: 437 paz. → OR = 4.53 (95% CI = 2.62-7.82) - 3 anni: 425 paz. → OR = 3.50 (95% CI = 1.75-7.02)
Confronto N. trials:
•TACE + PEI vs. TACE 4•TACE + RF vs. RF 2•TACE + PEI vs. PEI 1•TACE + RF vs. TACE 1•TACE + PEI vs. TACE o PEI 1•TACE + RF vs. TACE o RF 1
Recurrence rate

Preliminary OS from start of sorafenib therapy in patients who did and did not receive concomitant TACE
CI, confidence interval; OS, overall survival ASCO GI 2012

Trattamenti locoregionali combinati
AISF position paper, Digest Liver Dis, 2013

Sorafenib
Target: 40%OS: 11 mo (6-14)
Portal pressure/bilirubin
HCC
PEI/RFA
Stage 0PST 0, Child–Pugh A
Very early stage (0) 1 HCC < 2 cm
Carcinoma in situ
Early stage (A)1 HCC or 3 nodules
< 3 cm, PST 0
End stage (D)
Liver transplantation TACEResection
Curative treatments (30%)5-year survival (40–70%)
Target: 20%OS: 20 mo (45-14)
Associated diseases
YesNo
3 nodules ≤ 3 cm
Increased
Normal
1 HCC
Stage DPST > 2, Child–Pugh C
Intermediate stage (B)Multinodular,
PST 0
Advanced stage (C) Portal invasion, N1, M1, PST 1–2
Stage A–CPST 0–2, Child–Pugh A–B
EASL–EORTC Clinical Practice Guidelines: Management of hepatocellular carcinoma. Journal of Hepatology 2012 vol. 56 j 908–943
Best supportivecare
Target: 10%OS: <3 mo
Updated BCLC staging system and treatment strategy
PST 0-1

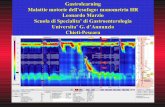
Sorafenib increased overall survival in different patient populations
1.00
0.75
0.50
0.25
0 4 6 8 10 12 14 162
0.00
18
Su
rviv
al
pro
ba
bil
ity
Months
Sorafenib (n = 150)
Median OS: 6.5 months (95% CI: 5.6–7.6)
Placebo (n = 76)
Median OS: 4.2 months(95% CI: 3.7–5.5)
1.00
0.75
0.50
0.25
0 4 8 12 220.00
2 6 10 14 16 18 20
HR = 0.68
Asia–Pacific 2
1. Llovet JM, et al. N Engl J Med. 2008;359:378-90.2. Cheng A-L, et al. Lancet Oncol. 2009;10:25-34.
Su
rviv
al
pro
ba
bil
ity
Months
Sorafenib (n = 299)
Median OS: 10.7 months(95% CI: 40.9–57.9)
HR = 0.69
SHARP 1
Placebo (n = 303)
Median OS: 7.9 months(95% CI: 29.4–39.4)
Sorafenib prolongs OS by 44%Sorafenib prolongs OS by 44% Sorafenib prolongs OS by 47%Sorafenib prolongs OS by 47%

Sorafenib dose and overall survival in clinical practice
SOFIA study
GIDEON study

• Systemic chemotherapy with conventional agents, octreotide, interferon, tamoxifen, and anti-androgenic drugs has no role in HCC treatment (1b-A).
****• Full dose sorafenib is the recommended treatment for HCC patients with
preserved liver function who are not amenable to surgery and loco-regional treatments or in whom TACE failed, according to the Italian National Health Service rules (1b-A).
In patients intolerant to full dose sorafenib, the tolerance to a reduced dose (400 mg/day) is to be pursued before definitively suspending the treatment (2b-B).
****• HCC patients who cannot receive any effective treatment for HCC must
receive symptomatic treatment for pain management, and nutritional and psychological support (5-D).
Terapia sistemica dell’HCC:raccomandazioni AISF
AISF position paper, Digest Liver Dis, 2013

Terapia antivirale:raccomandazioni AISF
• All HBV-DNA positive patients should receive antiviral therapy with nucleos(t)ide analogues at the time of and after HCC treatment (2b-B).
• HCV-RNA positive patients with preserved liver function (Child-Pugh class 8) whose HCC has been treated with curative intent should be considered potential candidates to antiviral therapy (2b-B).
• The AISF position on the usage of antiviral drugs is reported in greater detailed elsewhere
AISF position paper, Digest Liver Dis, 2013

Fine (finalmente!)