Daily Saftey Tool Box Meeting
2
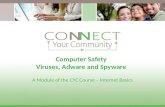
daiLY TOOL BOX MEETING Project Name: -…………………….Project Reference ……….. Date ……../..…../………….. Name Of Employee Leading Tool Box Meeting…………………………………………………….. Meeting Location:…………………………………………………….. 1. Were there any Incidents, Injuries or First-Aid Reports for the day? O Yes O No Describe: …………………………………………………………………………………………………………….... …………………………………………………………………………………………………………………………………………………….. …………………………………………………. 2. Were there any STOP WORK interventions due to safety negligence? O Yes O No Describe: …………………………………………………………………………………………………………….... …………………………………………………………………………………………………………………………………………………….. ……………………………………………… 3. Were any areas for improvement identified? O Yes O No Describe: …………………………………………………………………………………………………………….... …………………………………………………………………………………………………………………………………………………….. ……………………………………………… 4. At the conclusion of the day, I certify that the job site is being left in a safe condition and there were no unreported incidents or first aid: O Yes O No Describe:…………………………………………………………………………………………………………….... …………………………………………………………………………………………………………………………………………………….. ………………………………………………………………………………………………………………………………………………….……. 5. Job Related Problem Areas/Concerns: 1. ………………………………………………. 6. ……..……………………………………….. 2. ……………………………………………..... 7. ..…………………………………………….. 3. ………………………………………………. 8. ………………………………………………. 4. ………………………………………………. 9. ………………………………………………. 5. ………………………………………………. 10. .…………………………………………….. MEETING ATTENDEE DETAILS Si No. Name Company Name / Designation Signature 1. 2. 3. 4. 5 6 7
-
Upload
nadim-jilani -
Category
Documents
-
view
22 -
download
0
description
meeting doc
Transcript of Daily Saftey Tool Box Meeting

daiLY TOOL BOX MEETING
Project Name: -……………………. Project Reference ……….. Date ……../..…../…………..
Name Of Employee Leading Tool Box Meeting……………………………………………………..Meeting Location:……………………………………………………..
1. Were there any Incidents, Injuries or First-Aid Reports for the day? O Yes O No Describe:……………………………………………………………………………………………………………....……………………………………………………………………………………………………………………………………………………..………………………………………………….
2. Were there any STOP WORK interventions due to safety negligence?O Yes O No Describe:……………………………………………………………………………………………………………....……………………………………………………………………………………………………………………………………………………..………………………………………………
3. Were any areas for improvement identified?O Yes O No Describe:……………………………………………………………………………………………………………....……………………………………………………………………………………………………………………………………………………..………………………………………………
4. At the conclusion of the day, I certify that the job site is being left in a safe condition and there were no unreported incidents or first aid:O Yes O No Describe:……………………………………………………………………………………………………………....……………………………………………………………………………………………………………………………………………………..………………………………………………………………………………………………………………………………………………….…….
5. Job Related Problem Areas/Concerns:1. ………………………………………………. 6. ……..………………………………………..2. ……………………………………………..... 7. ..……………………………………………..3. ………………………………………………. 8. ……………………………………………….4. ………………………………………………. 9. ……………………………………………….5. ………………………………………………. 10. .……………………………………………..
MEETING ATTENDEE DETAILS
Si No. Name Company Name / Designation Signature
1.2.3.4.5678910

daiLY TOOL BOX MEETING
Project Name: -……………………. Project Reference ……….. Date ……../..…../…………..
Name Of Employee Leading Tool Box Meeting……………………………………………………..Meeting Location:……………………………………………………..
Signature of Site Engineer
--------------------------------------------------.