CYSTIC FIBROSIS. Who are we talking about? L.L is a 4 year old Preschooler Has a 6 year old brother,...
35
CYSTIC FIBROSIS
-
Upload
thomas-hart -
Category
Documents
-
view
215 -
download
0
Transcript of CYSTIC FIBROSIS. Who are we talking about? L.L is a 4 year old Preschooler Has a 6 year old brother,...

CYSTIC FIBROSIS

Who are we talking about?L.L is a 4 year old
Preschooler
Has a 6 year old brother, who does not have the disease
Lives with both parents, brother and 2 dogs
Enjoys swimming twice a week
Past HistoryBirth history:
-Born at 41 weeks,
-Had meconium ileus at 9 days of life
-Had genetic screen: CF diagnosis

Family and psychosocial History
L.L. lives with his parents, a 6 year old brother and 2 dogs.
Both parents work.
The family lives at Virginia Beach.
Mother is from South Africa and has not family in the country.
L.L. was diagnosed with CF at 2 months of age.
Grandmother helps parents during hospitalization.

Cultural considerationsL.L father is a paramedic who works
in Virginia Beach: he is constantly aware of L.L health changes.
L.L is a preschooler, who miss his friends at preschool.
L.L borne with this disease so he has been receiving treatment since he was 2 months old.

Reason for admission1 week of coughing, rhinorrhea and fever.
His PCP ordered Amoxicillin for otitis media on left ear.
2 days before hospitalization: tachypneic
1 day before hospitalization: retractions, belly breathing, cough, sputum, post-tussive emesis.
Day of admission: O2 sat 89%, he usually has 97-98% at home, increased WOB, fever 103 F.

Primary medical diagnosis
Cystic fibrosis exacerbation
CF is an autosomal recessive trait where both parents gave the child the CFTR gene in order to have CF.


Treatment PlanCPT: medicated aerosol
treatment. 2.5 mg, 3ml inhalant nebulizer, qid
Oxygen therapy: nasal cannula 2.5 liter/min.
CPT: vest pressure hz=14, qid (20min)
Antibiotic therapy: Trobamycin, Ticarcillin-Clavulanate
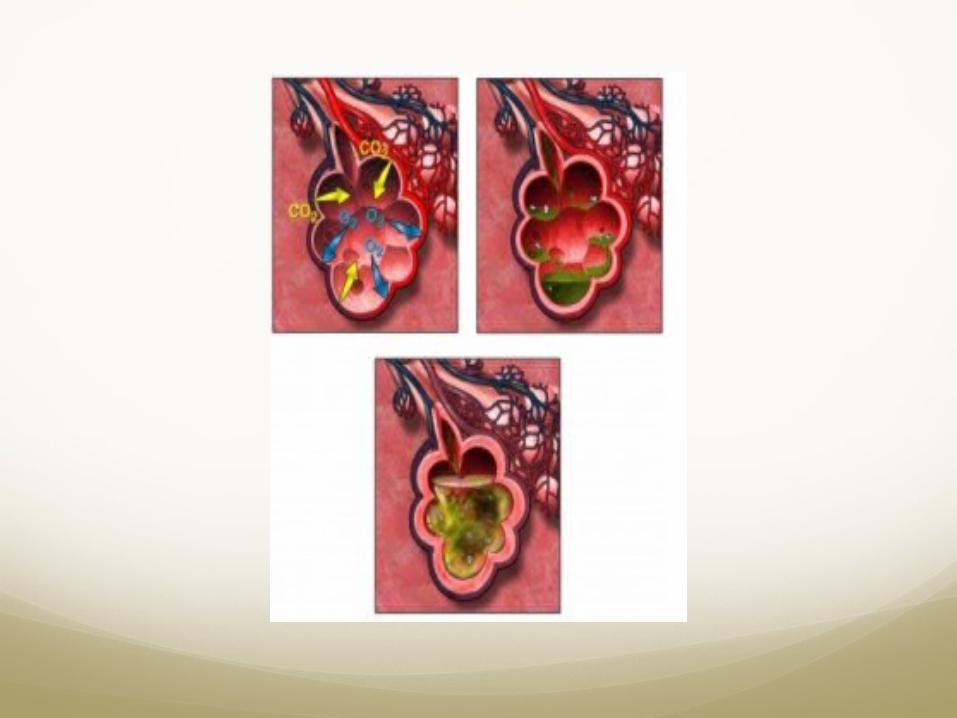
Relationship with any medical diagnosis?
He is suspected to have pneumonia
This is common in patient with cystic fibrosis
Hard to get rid off thick mucus
Perfect environment for bacteria
In what developmental age is L.L?
L.L is in the Preschooler developmental ageAdvance perception of shape and
development of fine muscle coordination (scribble and draw).
They use their fingers rather than the fits to hold writing instruments.
Between 4 and 5 child can trace and copy a square.

Psychosocial developmentMain task is acquiring sense of
initiative.Energetic to learnPlay, work, live to the fullestFeel accomplish and satisfied in in
their activitiesStart feeling guilty if they
misbehaved Superego or conscious start
developingLearning right form wrong or good
from bad> beginning of morality.
Preoperational phaseShift from total egocentric to social
awarenessCan consider other point of viewCan think in one idea at the timeAssumed that everyone thinks as
they doMagical thinkingBelieve in the power of words
(literally)

Did he meet the norms?Yes! He met the norms of this developmental
stage.
Because:He drew circles and painted them. He
knew the colors of his pens.He felt accomplished after pushing the
green button to make the medication pump work.
He loved to make bracelets from paper and tape.
Sometimes he considered other points of view.
Developmental theory to care and communication
Psychosocial theory: L.L. is likes to play , has initiative and start differentiating between right or wrong: L.L. was allowed to play and to “ help the nurse on his own care”.
Cognitive theory, he considers others point of view and can think one thing at the time: L.L was explained one thing at the time and language was simple.

Physical assessmentResp: cough, wheezing bilaterally,
mucus, change to portable oxygen tank to ambulate, decrease appetite
Skin: peripheral IV access clean (dry and intact) skin warm. No bruises or rush
Psy/soc: has company 24 hrs (mother, father or grandmother)
Fall: likes to play and ambulate on room, has a portable oxygen tank

1)Impaired gas exchange
Excessive mucus in lung
Possible pneumonia
Cough, wheezing/1 wk
Hazy areas of opacification in lung
Retractions
O2 sat 80-90% on day of admission
Post tussive emesis
O2 sat: 94% 3 liter/min
X-ray: opacity in lung
Mucus culture: in progress
Htc: 34.0% low

Expected outcome: : Patient will maintain O2 sat> 90% before discharge
Assess respirations, adventitious sounds, and cough, and mucus production, use of accessory muscles q4r
Use pulse oximetry to monitor oxygen sat. q2r or prn
Position head of bead> 45 degrees, encourage or assist with ambulation
Use of oxygen 3 to maintain O2 sat>90%
Encourage fluid intake > 1365 ml/day
Monitor CPT treatments with vest and albuterol nebulizer asking the specialist if the tx was complete or not.


2)Imbalanced nutrition: less than body requirements
Decrease absorption of nutrients en duodenum
Needs 150% amount of nutrients
Had meconium ilues/at 9 day
Gerd
Loss of appetite
Htc: 34.0% ( check for anemia)
NPO before attempt to put a PICC
Expected Outcome: Pt will maintain or gain healthy weight during
hospitalization
Measure weight daily. Same time, same clothing, same scale.
Assess the environment were eating occurs (pleasant environment)
Provide companionship while eating
Provide good oral hygiene
Small frequent meals high in calories and proteins: 3 meals + 3 snacks
Provide medications: Pancrelipase, zantac (for GERD), Miralax ( laxative)

3) Risk for dehydration:
O consistently >I and < maintenance fluid
NPO
Increase metabolic rate/ possible infection
24 before clinical: I&O= 602.43-801=-198.57
Day 1: I&O=159/250= - 91
IV fluid discontinue
Expected Outcome: will have an intake at least minimum to keep basal metabolic intake: 1365 ml/day before discharge
Monitor daily weight, with similar clothes
Evaluate fluid intake in relation to dietary intake
Monitor BP and HR
Assess for skin turgor, mucous membrane, LOCX3
Monitor I&O q4r
Monitor hydration input should be more than 1365 output should be 415 ml/day: q4r
4) Infection
Prior ototis
Mucous in the lungs
Low fluid intake
Opacity in the lungs
Possible pneumonia
WBC:11.5
Fever: 103 F
CF exacerbation

Expected Outcome: pt will continue to not show signs of infection such as temp: BP: <37.4, no skin break down, no thick mucous secretions before discharge.
Meets minimum output of 415 ml/day , good skin turgor.
Promote ambulation
Teach parent and child hand washing technique: minimum of 30 seconds
Assess sputum for specific bacteria
Assess for fever, fatigue, malaise, oral lesions. Q4r
Provide antibiotic therapy: Tobramycin,Ticarcillin-Clavulanate

5)Caregiver role strain
Father and mother are working and have to constantly to ask for day off or switch shifts at work.
A family member always stays wit the patient (mother, father, or grandmother)
Parents had another child to take care (6 year old).
Caregiver express satisfaction with his/her role before discharge
Encourage caregiver to identify family members or friends available who can assist with care giving.
Encourage caregiver to set aside time for self; identifying what can bring them peace and relaxation.
Acknowledge to the caregiver his/her role value.
Provide time to discuss feelings and concerns (Support group)

Research: Paternal experiences of their children’s diagnosis of
Cystic Fibrosis following newborn screening diagnosis
Research was conducted on fathers of children diagnosed with CF because few studies were conducted in comparison with mothers.
15 fathers were interviewed in Western Australia using semi-structured interviews.
Interviews were conducted at home or by phone.
Fathers felt as protectors and tried to hide their feelings.
It was easy to recall their wives reactions, but difficult to recall their own reactions.
Fathers tried to support the mother-child relationship by caring for the mother.
Parental level of emotional adjustment was unclear, but anxiety was more evident.
Study highlighted the importance of providing therapeutic services to voice their concerns without reservations.
Relationship between actual nursing problems

Teaching and discharge planning
Discharge with a PICC: antibiotic treatment for 3 to 4 weeks.
Continue with routine treatment of Cf (medication reconciliation):Albuterol 2.5 mg, nebulizer BIDVest 14 mega hz, 20 min BIDCreon 6 with 3 snacks, 3 mealsMiralax, once per day.
Teaching: How to take care of a PICC while at home.
References:Ignatavicius, D. D., & Workman, M.L.
(2013). Medical Surgical Nursing: Patient- Centered Collaborative care. St. Louis Missouri: Elsevier Saunders.
Priddis, L., Dunwoodie, J., Balding, E., Barrett, A., & Douglas, T. (2010). Paternal experiences of their children's diagnosis of Cystic Fibrosis following newborn screening diagnosis. Neonatal, Paediatric & Child Health Nursing, 13(2), 4-10.