CT scan in head and spine injuries BY : DR AHMED MOHAMMED DEBES سایت جامع رادیولوژی...
22
CT scan in head and spine injuries BY : DR AHMED MOHAMMED DEBES ی وژ ل و ی ع ژاد م ا ج ت ی ساWWW.RADIOLOGYHA.COM
-
Upload
maude-bradford -
Category
Documents
-
view
214 -
download
0
Transcript of CT scan in head and spine injuries BY : DR AHMED MOHAMMED DEBES سایت جامع رادیولوژی...

CT scan in head and spine injuries
BY : DR AHMED MOHAMMED DEBES
رادیولوژی جامع سایت
WWW.RADIOLOGYHA.COM

Brief history
Basic physics
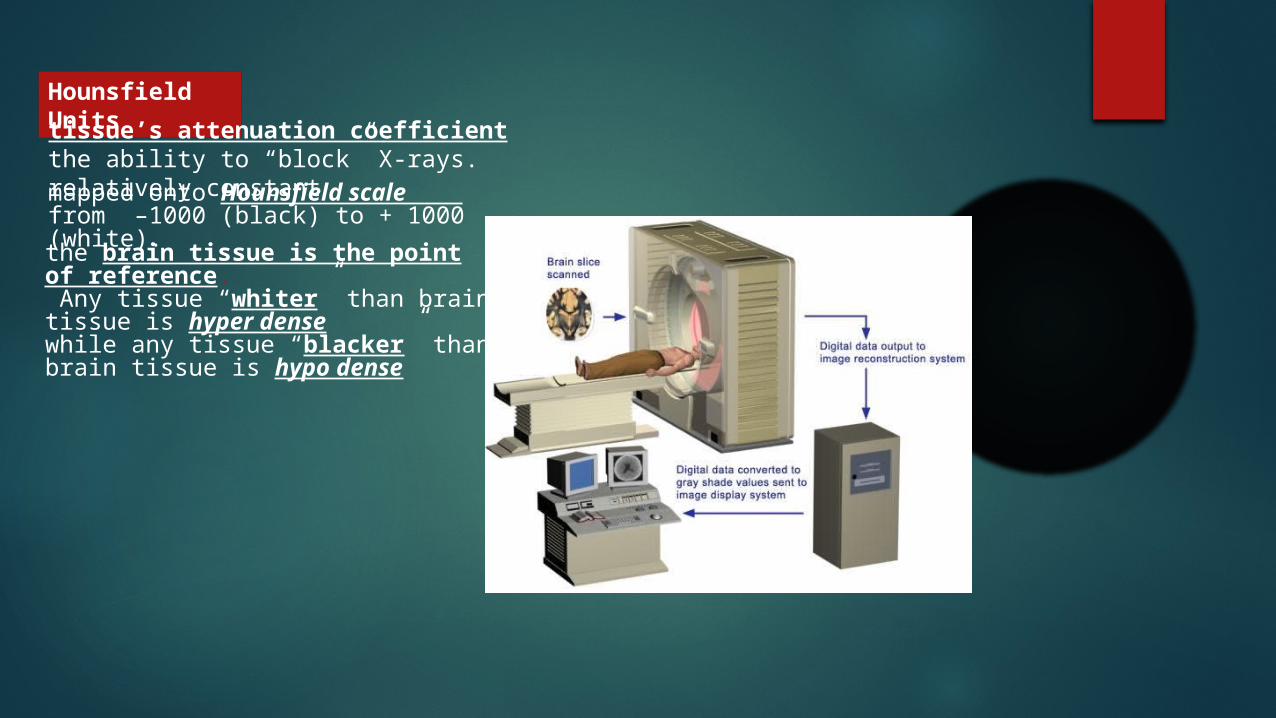
mapped onto Hounsfield scale from –1000 (black) to + 1000 (white).
the brain tissue is the point of reference. Any tissue “whiter” than brain tissue is hyper densewhile any tissue “blacker” than brain tissue is hypo dense
Hounsfield Unitstissue’s attenuation coefficient the ability to “block” X-rays. relatively constant
Image acquisition

LOOK for
I - Skull Fractur
e
II – Pneumo-cephalus
III - Hematom
a
IV - Cerebral Edema
V - Herniatio
n
What to look for in CT scan brain of a head trauma patient ?

I - Skull Fracture
Look in head CT bone window
I - Linear, non-depressed fracture

II - Depressed fractureConsider open when
- Skin laceration over the fracture- Through par nasal sinuses, middle ear structures
Surgical elevation in
- Depressed > 5 mm and overlies motor or speech areas- Depressed > skull thickness
Causes laceration of Dura, arachnoid and possible brain parenchyma

III - Diastatic fracture
Spreading of suture, 1-2 mm more than normal contralateral sideMay tear Dural venous sinus

IV - Basilar fracturePresentations
- CSF otorrhea, bruising over mastoid (Battle sign)- CSF rhinorrhea, bruising around the eyes (raccoon eyes)

II - Pneumocephalus
Presence of air in the cranial cavity
Indicates communication between intracranial and extra cranial spacescomplications: meningitis, CSF otorrhea or rhinorrhea

III - Hematoma
I - Epidural HematomaSource of bleeding
most commonly middle meningeal artery
Don't cross sutures
Hyper dense biconvex extra-axial mass
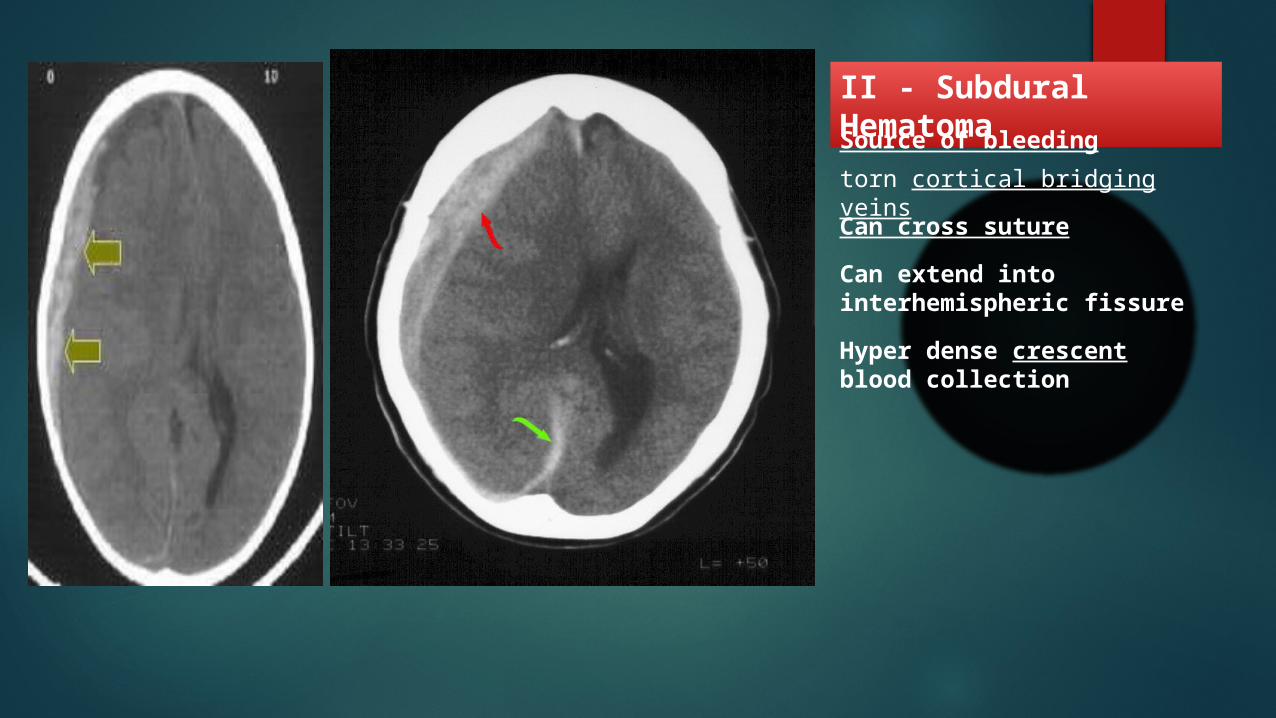
II - Subdural HematomaSource of bleeding
torn cortical bridging veins
Hyper dense crescent blood collection
Can cross suture
Can extend into interhemispheric fissure

III - Traumatic SubarachnoidHemorrhageSource of bleeding
Tear of veins in subarachnoid space
High density blood in sulci/cisterns

IV - Cerebral Contusiondue to cerebral gyri impact inner table of the skull
Evolve from petechial hemorrhage -> small hemorrhage ->large hematomaMultiple, bilateral
MRI is better for detection
III - Cerebral Edema
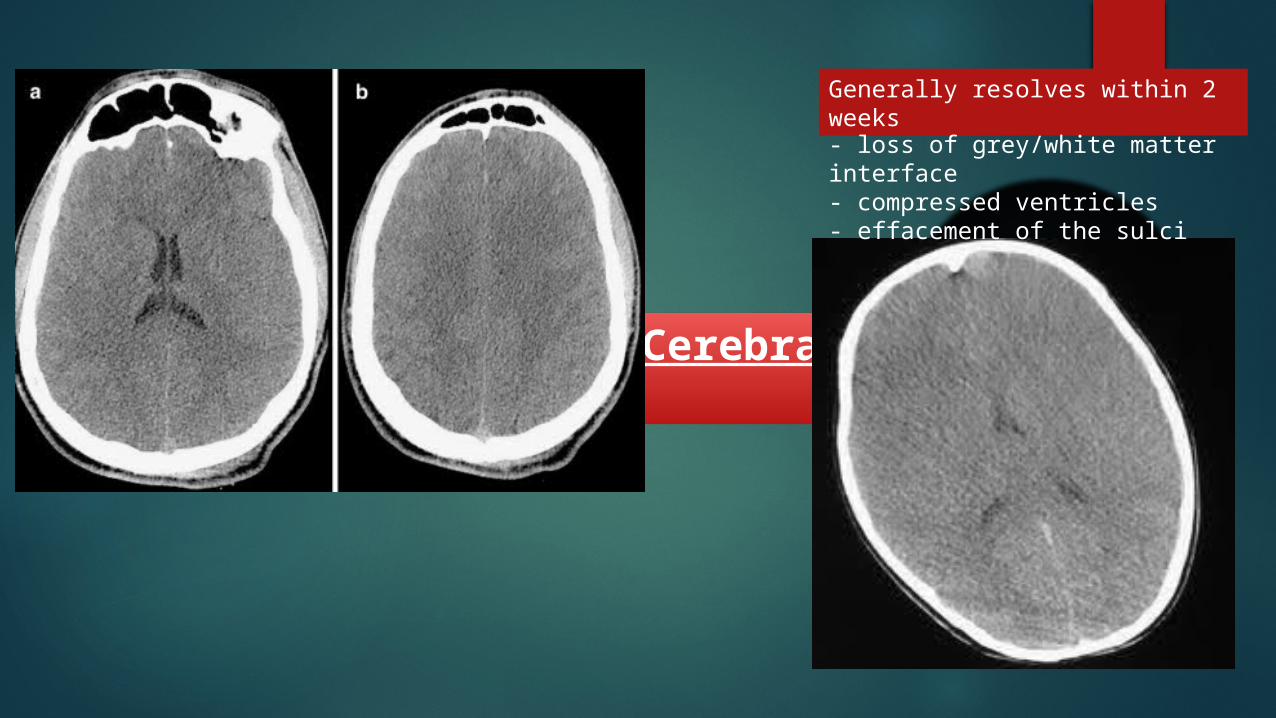
Generally resolves within 2 weeks
- loss of grey/white matter interface- compressed ventricles- effacement of the sulci
IV - Herniation
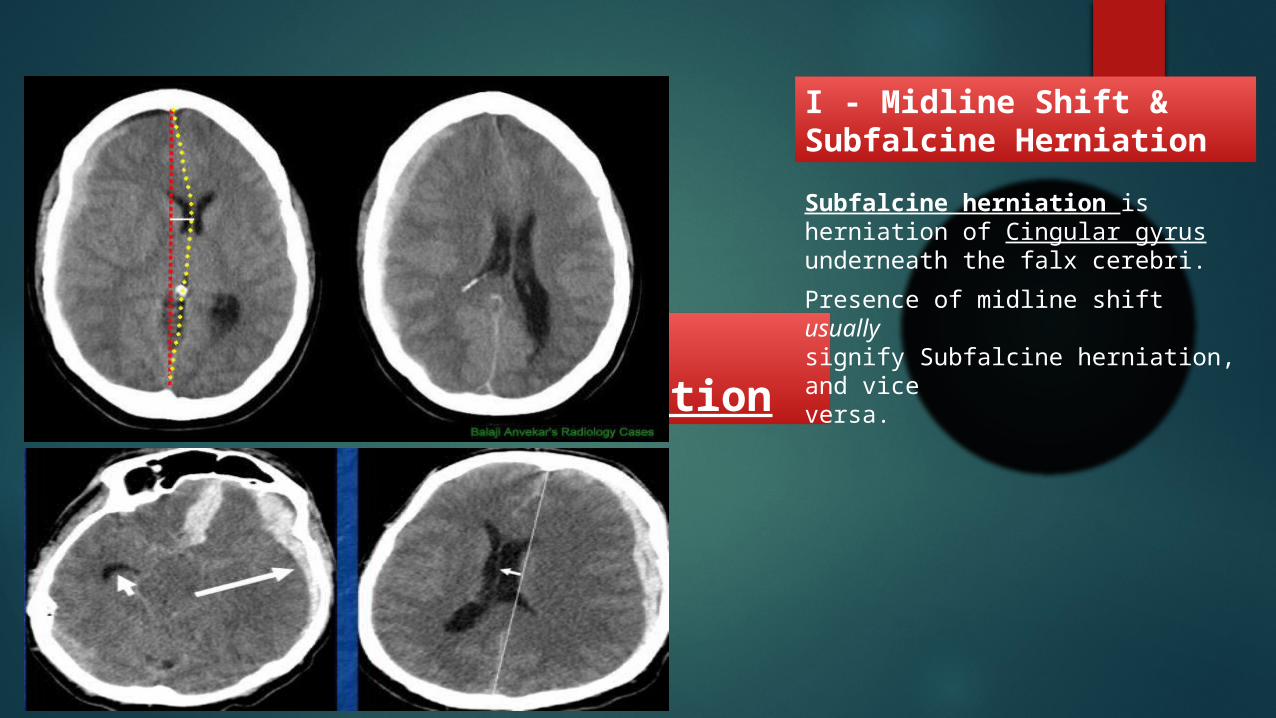
I - Midline Shift & Subfalcine Herniation
Subfalcine herniation is herniation of Cingular gyrus underneath the falx cerebri.
Presence of midline shift usuallysignify Subfalcine herniation, and viceversa.
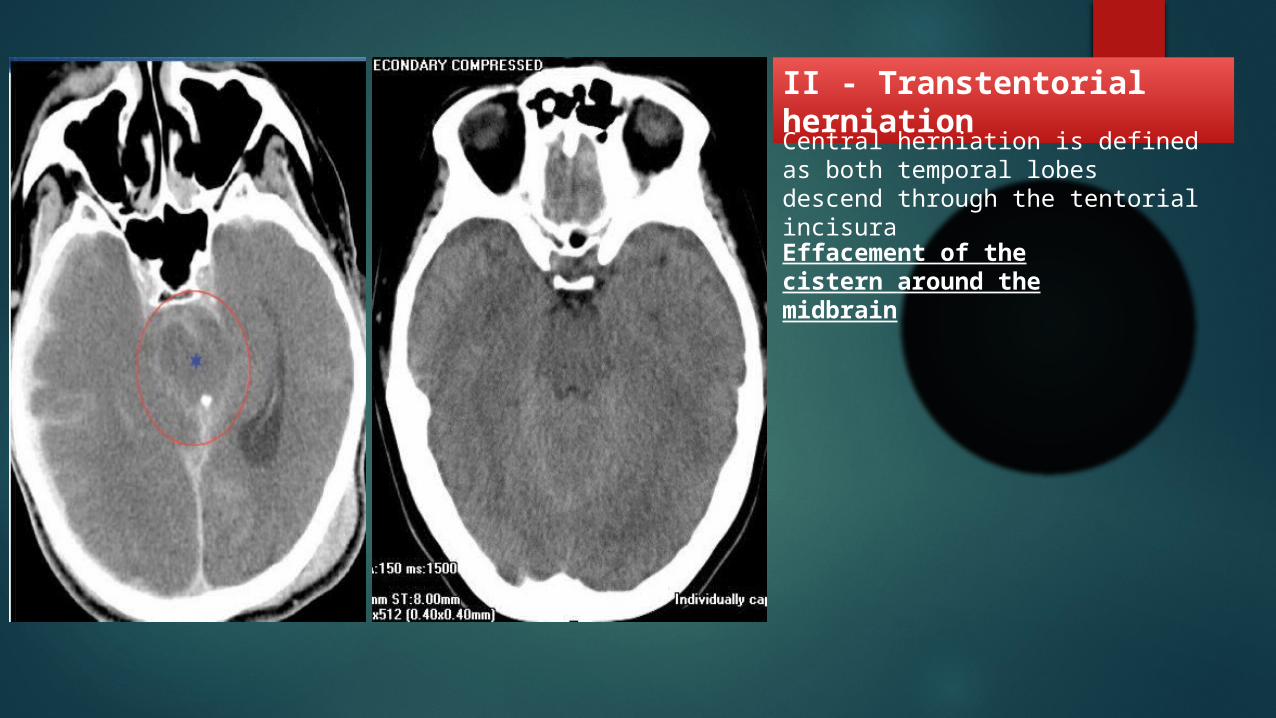
II - Transtentorial herniationCentral herniation is defined as both temporal lobes descend through the tentorial incisura
Effacement of the cistern around the midbrain

III - Tonsillar Herniation
- obliteration of CSF space- displaced portions of cervicomedullary junction

CT scan in spine trauma
I - Compression fracture

II – Burst fracture
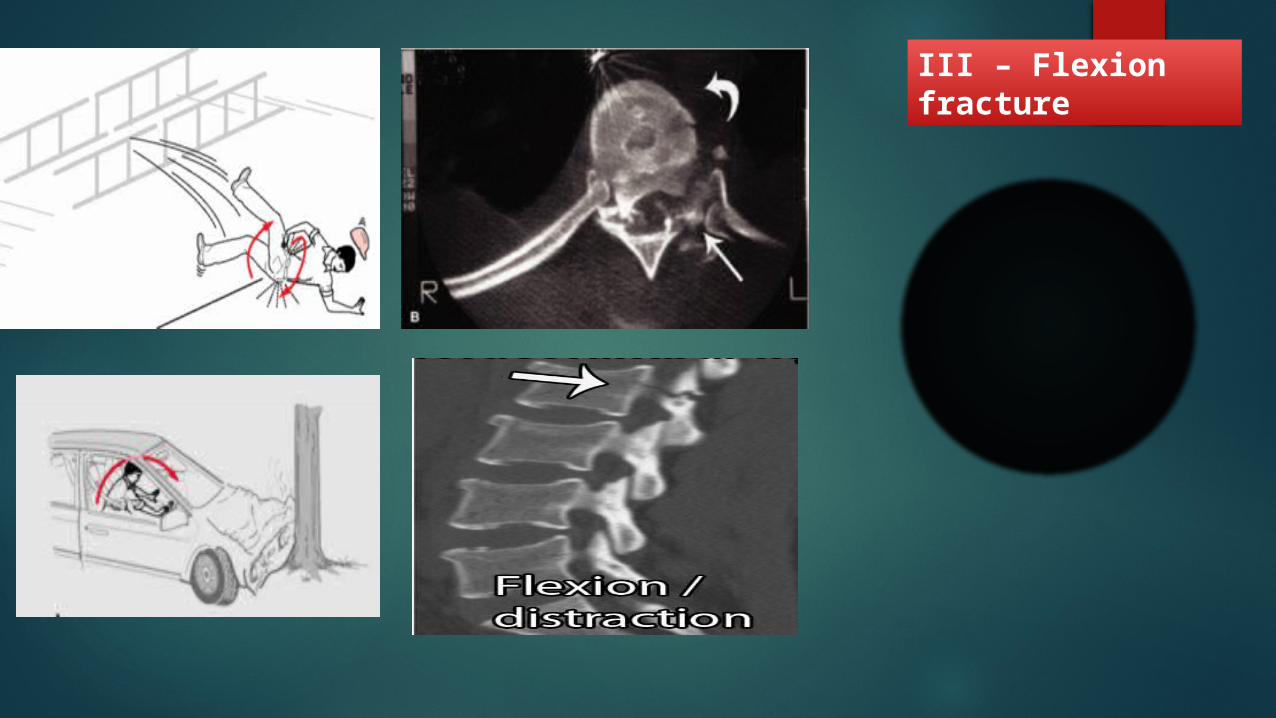
III – Flexion fracture

III – fracture dislocation

The end
Thank you














![[WEBINAR] 10 cosas que debes saber sobre Active Directory.](https://static.fdocuments.in/doc/165x107/557af909d8b42a17468b5818/webinar-10-cosas-que-debes-saber-sobre-active-directory.jpg)



