
CT Imaging of the Breast with a Novel New System · Biopsy. Limitations of Mammography High spatial...
27
CT Imaging of the Breast CT Imaging of the Breast with a Novel New System with a Novel New System John Neugebauer John Neugebauer [email protected] [email protected] Cell 412 Cell 412 - - 779 779 - - 0392 0392 Cone Beam CT
-
Upload
dinhkhuong -
Category
Documents
-
view
217 -
download
3
Transcript of CT Imaging of the Breast with a Novel New System · Biopsy. Limitations of Mammography High spatial...

CT Imaging of the BreastCT Imaging of the Breast
with a Novel New Systemwith a Novel New System
John NeugebauerJohn Neugebauer
[email protected]@koningcorporation.com
Cell 412Cell 412--779779--03920392
Cone Beam CT

Breast CancerBreast Cancer
No cureNo cureEtiology of the disease is unknownEtiology of the disease is unknownMammography is limited in dense breastsMammography is limited in dense breastsTo affect mortality rates and reduce the cancerTo affect mortality rates and reduce the cancer
burden, we need to find cancer in the earliestburden, we need to find cancer in the earlieststages.stages.
7 Years-
Palpable
5 Years-Mammography
98% <70%
IVIII
<56% <16%

Standard of Care for DetectionStandard of Care for Detectionand Diagnosisand Diagnosis
MammographyMammography�� Additional viewsAdditional views-- spot, angled,spot, angled,
magnificationmagnification
UltrasoundUltrasoundDuctographyDuctographyMRIMRIBiopsyBiopsy
Limitations of MammographyLimitations of Mammography
High spatial resolutionHigh spatial resolutionbut limited contrastbut limited contrastresolutionresolutionespecially in denseespecially in densebreastsbreasts
Mammography is a 2DMammography is a 2Dprojectionprojectionacquisition of a 3Dacquisition of a 3Dstructure leading tostructure leading tostructure and tissuestructure and tissueoverlapoverlap
Extent of diseaseExtent of disease�� Actual tumor size,Actual tumor size,
multifocality, andmultifocality, andmulticentricitymulticentricity

Limitations of UltrasoundLimitations of Ultrasound
Operator dependent and timeOperator dependent and timeconsumingconsuming
ACRIN 6666 (2004ACRIN 6666 (2004--2008)2008)�� Many more false positive biopsies to getMany more false positive biopsies to get
to a true cancerto a true cancer
Low spatial resolution and has severeLow spatial resolution and has severelimitations in visualizing andlimitations in visualizing andcharacterizing calcificationscharacterizing calcifications

Limitations of Breast MRILimitations of Breast MRIThe dependence of MRI onThe dependence of MRI on
contrast constrains thecontrast constrains themodality to balance spatialmodality to balance spatialresolution against temporalresolution against temporalresolutionresolution
Breast MRI cannot distinguishBreast MRI cannot distinguishcalcificationscalcifications�� High sensitivity for invasiveHigh sensitivity for invasive
breast cancer but limited inbreast cancer but limited indetecting DCISdetecting DCIS
Breast MRI 3D renderingBreast MRI 3D rendering�� Maximum contrast uptakeMaximum contrast uptake
intensity projection (MIP) usedintensity projection (MIP) usedfor geographic location onlyfor geographic location only

Why not CT?Why not CT?
•• Patient Positioning andPatient Positioning andAccessAccess
•• Tissue CoverageTissue Coverage
•• Resolution/ Image QualityResolution/ Image Quality
•• DoseDose
•• IV ContrastIV Contrast
Not with current design andNot with current design andconfiguration:configuration:

Current Use of CT in Breast ImagingCurrent Use of CT in Breast Imaging

GENERAL ELECTRICGENERAL ELECTRIC-- CT/MCT/M
First CT from GE
Unit #1- 1975- Mayo Clinic
Unit #2- 1976- U of Kansas

Specifications: GE CT/MSpecifications: GE CT/M
Slice ThicknessSlice Thickness 55 --10mm10mmSpatial ResolutionSpatial Resolution .32 lp/mm.32 lp/mmScan TimeScan Time 10 seconds per slice10 seconds per sliceDoseDose 3939--73 mGy73 mGyTechniqueTechnique 75 kVp75 kVp -- 200 mA200 mAReconstruction TimeReconstruction Time 90 seconds per slice90 seconds per slice

Results: University of Kansas Medical CenterResults: University of Kansas Medical Center
1976-1979
1625 Patients- All withContrast
78 Cancers
Increase in CT Number
CT- 94% Sensitivity
Mammo - 77% Sensitivity

Conclusion:Conclusion:
““The CT/M appears to be especially superior to theThe CT/M appears to be especially superior to themammography formammography for detectingdetecting cancers in dense,cancers in dense,premenopausal dysplastic breasts. The CT/M can detectpremenopausal dysplastic breasts. The CT/M can detecttotally unsuspected very small breast cancers that weretotally unsuspected very small breast cancers that wereunable to be identified by conventional mammographyunable to be identified by conventional mammographyor physical exam. The CT/M scan also seems to be aor physical exam. The CT/M scan also seems to be abetter test for recognizing precancerous high risk lesions.better test for recognizing precancerous high risk lesions.CT/M evaluation affords definitiveCT/M evaluation affords definitive diagnosticdiagnostic help inhelp ininstances where the mammographic and/or physicalinstances where the mammographic and/or physicalexaminations are inconclusive. Although CT/M will notexaminations are inconclusive. Although CT/M will notreplace conventional mammography in routine breastreplace conventional mammography in routine breastexaminations, it overcomes the limitations ofexaminations, it overcomes the limitations ofmammography.mammography.””
Cancer 46: 939Cancer 46: 939--946, 1980946, 1980

Lesion Differentiation Based on CT Number
Japan
154 Cancers
Cutoff Attenuation 60HU
90% sensitivity
77% specificity

Multi Detector CTMulti Detector CT
•• ItalyItaly•• 61 Birads 4/5 Patients61 Birads 4/5 Patients•• Unable to undergo MRIUnable to undergo MRI•• 47 to Surgery47 to Surgery•• Cutoff Attenuation 90Cutoff Attenuation 90
HUHU•• 25 of 27 Malignant25 of 27 Malignant
(92% Sensitivity)(92% Sensitivity)•• 20 of 20 Benign20 of 20 Benign
(100% Specificity)(100% Specificity)

20042004 -- UC Davis Clinical PrototypeUC Davis Clinical PrototypeCone Beam Scanner
30 x40 cm Flat Panel Detector
Neoprene Hammock for Breast Support
16.6 second scan time
10 to 110kVp Fluoroscopic Operation (6mA)
0.4mm x 0.4mm focal spot

Results: Radiology Jan 08Results: Radiology Jan 08•• Overall equal in visualizationOverall equal in visualization•• Better on MassesBetter on Masses•• Inferior on calcificationsInferior on calcifications•• More comfortableMore comfortable……but notbut not
for everyonefor everyone•• No visualization differenceNo visualization difference
malignant or benignmalignant or benign•• Less coverage of pectoralisLess coverage of pectoralis
and axillary tailand axillary tail•• Dose equal to a two viewDose equal to a two view
mammogrammammogram
Conclusion: Some technicalConclusion: Some technicalchallenges remain butchallenges remain butpromisingpromising

20062006-- URMC Clinical PrototypeURMC Clinical Prototype
•• Cone Beam/Flat Panel ScannerCone Beam/Flat Panel Scanner
•• Mammography Tube/Mammography Tube/Tungsten Anode (0.3) (49kVp)Tungsten Anode (0.3) (49kVp)
•• Radiographic TechniqueRadiographic Technique
•• 10 second exposure10 second exposure
•• 140 and 270 micron (isotropic)140 and 270 micron (isotropic)
•• 0.25mm slice thickness0.25mm slice thickness
•• Slip Ring TechnologySlip Ring Technology
•• Patient access either sidePatient access either side
•• Table/ Gantry Elevation to 5Table/ Gantry Elevation to 5feetfeet

Initial Pilot StudyInitial Pilot Study
Comparison with Mammography
-Image Quality
-Coverage
-Dose
23 Patients/44 Breasts
All Birads 1&2
Ages40-65
7 patients-40 to 45
7 patients-45 to 50
Clinical Study Conducted By:
Highland Breast Center-URMC
Elizabeth Wende Breast Care LLC
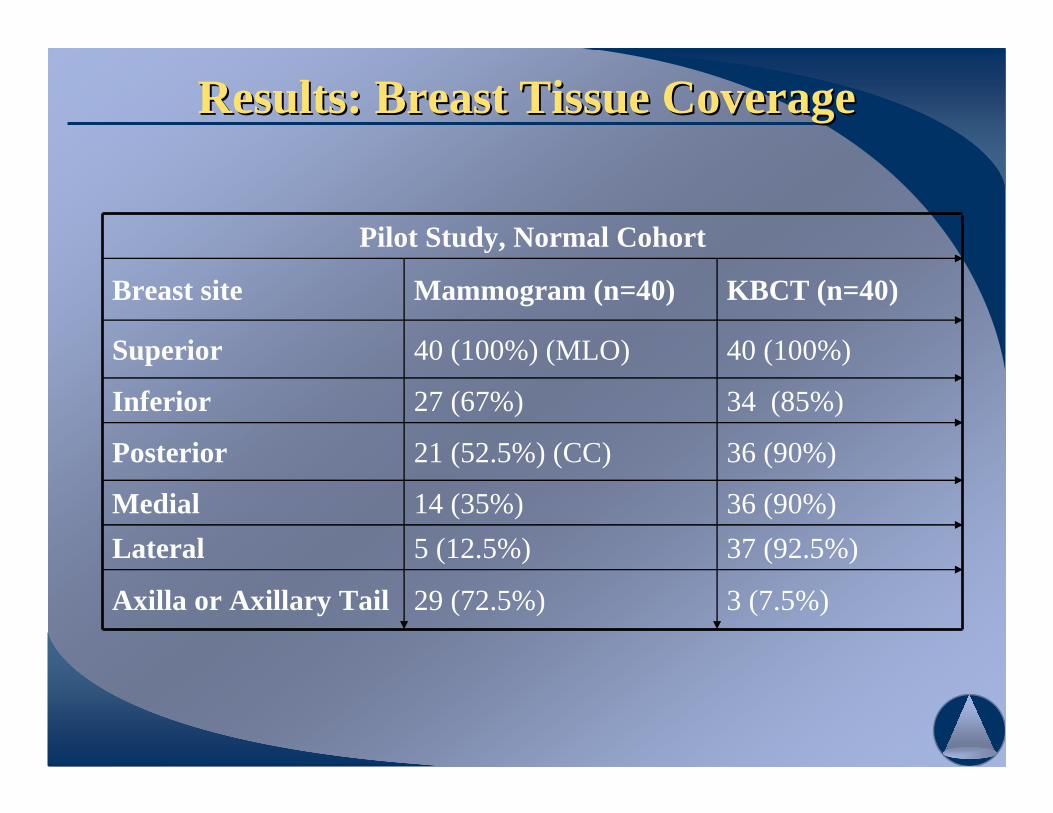
Results: Breast Tissue CoverageResults: Breast Tissue Coverage
Pilot Study, Normal Cohort
Breast site Mammogram (n=40) KBCT (n=40)
Superior 40 (100%) (MLO) 40 (100%)
Inferior 27 (67%) 34 (85%)
Posterior 21 (52.5%) (CC) 36 (90%)
Medial 14 (35%) 36 (90%)
Lateral 5 (12.5%) 37 (92.5%)
Axilla or Axillary Tail 29 (72.5%) 3 (7.5%)

Results: Average Glandular DoseResults: Average Glandular DosePilot Study, Normal Cohort
• N = 44 breasts• Average glandular radiation dose (mGy) as a function of x-ray tube current (mA)
• Voltage [kVp] and time [ms] are constant• Determined from prior dose phantom studies• The mA-to-mGy relationship was verified using an FDA-approved 16-cm
PMMA head dose phantom to measure the weighted computer tomographydose index (CTDIw)
• 2 orthogonal low dose scout images of the breast were obtained prior to the scan.• The optimal tube current (mA) to obtain sufficient contrast-to-noise ratio in the
reconstructed cross-sectional images at a minimum dose was determined fromthese scout images.
• Dose was tailored to each breast, depending on breast size and density
• Mammogram (dose per complete exam)• Range: 2.2 mGy to 15 mGy; Mean = 6.5 mGy; Standard deviation = 2.8 mGy
• CBCT (dose per scan)• Range: 4 mGy to 12.8 mGy; Mean = 8.2 mGy; Standard deviation = 1.2 mGy

Results: Image QualityResults: Image Quality

Results: Image QualityResults: Image Quality

Results: Patient ComfortResults: Patient Comfort
Comfort on CBBCT Exam Table (n=23)
4.3%
39.1%
17.4%
39.1%
No discomfort
SlightdiscomfortManageablediscomfortIntolerablediscomfort
Comfort: CBBCT vs. Mammo Exam(n=23)
43.5%
43.5%
13.0%Better
Equal
Worse
Comfort of CBCTTable
Comfort of CBCTvs.
Mammogram

Koning CorporationKoning Corporation
•• Privately held Delaware C Corp (2004)Privately held Delaware C Corp (2004)
•• West Henrietta, New YorkWest Henrietta, New York
•• Exclusive License from URMCExclusive License from URMC
•• Extensive Intellectual PropertyExtensive Intellectual Property
•• Virtual ManufacturingVirtual Manufacturing
•• Financing to date:Financing to date:$2.65 million SBIR Grant$2.65 million SBIR Grant$5.0 million Angel and VC Funding$5.0 million Angel and VC Funding

20082008-- First 2 Production SystemsFirst 2 Production Systems

Additional FeaturesAdditional Features
•• Self ShieldedSelf Shielded
•• Independent OperatorsIndependent OperatorsConsoleConsole
•• AddAdd--on Biopsy Deviceon Biopsy Device
•• 10 Second Scan Time10 Second Scan Time
•• 90 Second Reconstruction90 Second Reconstruction
•• DICOM CompliantDICOM Compliant
•• PACS, HIS, RISPACS, HIS, RISConnectivityConnectivity
•• Internet Accessible from 4Internet Accessible from 4Separate LocationsSeparate Locations

AddAdd-- On BiopsyOn Biopsy







![Aceso Dual-Modality Imaging - CapeRay · whole breast ultrasound and mammography in radiographically dense breasts”, European Radiology, 20(3): 734-742, 2010. [5] Giuliano V, Giuliano](https://static.fdocuments.in/doc/165x107/60f8bf9a12e97f57f163a45b/aceso-dual-modality-imaging-caperay-whole-breast-ultrasound-and-mammography-in.jpg)










