CPC19 Diabetes - naceonline.comnaceonline.com/CME-Courses/cpc-slides/CPC19_Diabetes_Print.pdf · He...
21
2/4/19 1 Conversations in Primary Care February 9, 2019 Agenda 9:00-9:05 AM Welcome Remarks Gregg Sherman, MD and Matt Rosenberg, MD 9:05-10:05 Optimizing Diabetes Care: Evolving Strategies for Safer Integration of Insulin Therapy Robert Busch, MD, FACE Moderator Gregg Sherman, MD 10:05-10:10 Break 10:10-11:15 Pulmonary Arterial Hypertension: Importance of Early Diagnosis and Updates in Management Charles D. Burger, MD Moderator Matt Rosenberg, MD 11:15-11:20 Break 11:20-12:20 PM Case Studies in MDD: Individualizing Care Greg Mattingly, MD Moderator Gregg Sherman, MD 12:20-12:50 Lunch Break 12:50-1:50 Improving Outcomes in ADHD: It Can be Done in Primary Care! Greg Mattingly, MD Moderator Matt Rosenberg, MD 1:50-1:55 Break 1:55-2:55 Secondary Cardiovascular Risk Reduction: Incorporating Evolving Data to Individualize Care Karol E. Watson, MD, PhD Moderator Gregg Sherman, MD 2:55-3:00 Closing Remarks Gregg Sherman, MD 2 How to Receive Your CME Credits 3 vHow many credits will I receive? This program is approved for 5 AMA PRA Category 1 Credits™, and 5 AANP contact hours of continuing education which includes 2.5 pharmacology hours. vHow do I get my CME Evaluation? You will receive an email with a link to complete your CME Evaluation form after the program today, and again in the coming week. vHow do I get my CME Certificate? Upon completing the program, and NACE processing your CME Evaluation form, you will be sent an email with instructions on how to download your CME certificate. Please look for this email 1-2 weeks following completion of the CME Evaluation form. vWho do I contact if I have a question about CME credits? You can email us at [email protected] or call us at 1-800-266-6223
Transcript of CPC19 Diabetes - naceonline.comnaceonline.com/CME-Courses/cpc-slides/CPC19_Diabetes_Print.pdf · He...

2/4/19
1
Conversations in Primary CareFebruary 9, 2019
Agenda9:00-9:05 AM Welcome Remarks
Gregg Sherman, MD and Matt Rosenberg, MD
9:05-10:05 Optimizing Diabetes Care: Evolving Strategies for Safer Integration of Insulin TherapyRobert Busch, MD, FACEModerator Gregg Sherman, MD
10:05-10:10 Break
10:10-11:15 Pulmonary Arterial Hypertension: Importance of Early Diagnosis and Updates in ManagementCharles D. Burger, MDModerator Matt Rosenberg, MD
11:15-11:20 Break11:20-12:20 PM Case Studies in MDD: Individualizing Care
Greg Mattingly, MDModerator Gregg Sherman, MD
12:20-12:50 Lunch Break12:50-1:50 Improving Outcomes in ADHD: It Can be Done in Primary Care!
Greg Mattingly, MDModerator Matt Rosenberg, MD
1:50-1:55 Break1:55-2:55 Secondary Cardiovascular Risk Reduction: Incorporating Evolving Data to Individualize Care
Karol E. Watson, MD, PhDModerator Gregg Sherman, MD
2:55-3:00 Closing RemarksGregg Sherman, MD
2
How to Receive Your CME Credits
3
vHow many credits will I receive?This program is approved for 5 AMA PRA Category 1 Credits™, and 5 AANP contact hours of continuing education which includes 2.5 pharmacology hours.
vHow do I get my CME Evaluation?You will receive an email with a link to complete your CME Evaluation form after the program today, and again in the coming week.
vHow do I get my CME Certificate?Upon completing the program, and NACE processing your CME Evaluation form, you will be sent an email with instructions on how to download your CME certificate. Please look for this email 1-2 weeks following completion of the CME Evaluation form.
vWho do I contact if I have a question about CME credits?You can email us at [email protected] or call us at 1-800-266-6223

2/4/19
2
Optimizing Diabetes Care: Evolving Strategies for Safer Integration of Insulin Therapy
FacultyvMark Stolar, MD
Associate Professor of Clinical Medicine
Feinberg School of Medicine
Northwestern University
Chicago, IL
vJavier Morales, MD, FACP, FACEClinical Associate Professor of Medicine
Donald and Barbara Zucker School of
Medicine At Hofstra/Northwell University
Vice President
Advanced Internal Medicine Group, P.C.
East Hills, NY
vRobert S. Busch, MD, FACEDirector of Clinical ResearchAlbany Medical Faculty: Community
Endocrine GroupAlbany, NY
5
DisclosuresvMark Stolar, MD has no relationships to disclose.vRobert S. Busch, MD, FACE has served as a researcher for Novo Nordisk, Sanofi and
Amarin. He has also served as a Speaker for Novo Nordisk and Sanofi.vJavier Morales, MD, FACP, FACE serves as a speaker for Novo Nordisk, Janssen and
Abbott Laboratories. He is also an Advisory Board member for Eli Lilly and has served as a consultant for Novo Nordisk and Eli Lilly.
6

2/4/19
3
Learning Objectives1. Recognize the risk for, and impact of hypoglycemia in patients with diabetes2. Describe strategies for reducing the occurrence of glycemic variability3. Understand effective SMBG vs. newer CGM in managing diabetes and reducing risk
of dysglycemia/hypoglycemia4. Differentiate between available insulin preparations and their effects on glycemic
variability and hypoglycemic risk
7
Pre-test Questions
8
Pre-test Question 1Pre-D1: In studies of patients with T2D, approximately what proportion have asymptomatic hypoglycemic episodes?1. <10%2. ~25%3. ~40% 4. >50%
9
2/4/19
4
Pre-test Question 2Pre-D2: In clinical trials, which of the following insulin formulations has demonstrated the lowest glycemic variability? 1. NPH insulin 2. Insulin detemir3. Insulin degludec 4. Insulin glargine U100
10
Pre-test Question 3
11
Pre-D3: Which of the following is associated with higher rates of hypoglycemia? 1. A1C levels near target2. BeAM factor < 50 mg/dL3. Higher glucose variability 4. Postprandial glucose levels above target
Pre-test Question 4Pre-D4: 54 y/o man with 9-year history of T2D presents for checkup. His A1C is 7.6%
SMBG: AM 150-200 mg/dL; HS 120-150 mg/DL.
Medications: metformin 1000 mg bid, canagliflozin 300 mg qd, and insulin glargine
U100 48 units HS.
Attempts to increase basal insulin dose in the past have led to daytime
hypoglycemia. What might you do now?
1. Add GLP-1 receptor agonist
2. Switch from basal insulin to premixed insulin
3. Switch from glargine u100 to glargine u300 and potentially increase dose
4. Ask patient to use continuous glucose monitor or SMBG 4 times a day, for 4 days and adjust meds based on findings
12
2/4/19
5
Pre-test Question 5
13
Pre-D5: 44 y/o woman with a 10-year history of T2D presents with A1C 7.6%.
Meds: metformin 1000 mg bid and insulin glargine U100 56 units qhs.
Because of inconsistent fasting self-monitored blood glucose readings, her clinician recommended she use a continuous glucose monitor for several days which show a high degree of glycemic variability throughout the day, and occasional episodes of nocturnal hypoglycemia.
What might you do now?
1. Add SGLT-2 inhibitor or GLP-1 receptor agonist
2. Administer insulin glargine U100 in divided doses3. Add prandial insulin and reduce dose of insulin glargine U100
4. Switch from insulin glargine U100 to ultralong-acting basal insulin
Hypoglycemia and Glucose Variability
14
Hypoglycemia Unawareness:A Dangerous Complication of Insulin Therapy
15
vEach episode of hypoglycemia reduces counterregulatory response to low glucose, even after one episode
vReduction in catecholamine response decreases awareness/symptoms even after a single episodevMajor hypoglycemic events lead to hypoglycemia unawareness
vNocturnal hypoglycemia is most pathogenic and unrecognizedvHypoglycemic awareness decreases significantly in the elderlyvCan be significant in patients with liver or renal impairment or with high glycemic
variability
Ahren Vasc Health Risk Manag. 2013;9:155-163.

2/4/19
6
CV Consequences of HypoglycemiavProlonged QT intervals1
vCan be of long duration2
vGreater with higher catecholamine levels3
vAssociated with angina/ischemic EKG changes4,5
vAssociated with arrhythmias
vAssociated with sudden death6
vIncreased glycemic variability can lead to adverse ICU outcomes/Increased vascular inflammation7
1. Diabetologia. 2009;52:42; 2. IJCP Sup 129, 7/02; 3. Europace 10,860; 4. Diabetes Care. 2003;26:1485; 5. Porcellati, ADA 2010; 6. Endocrine Practice. 2010;16; 7. Hirsch, ADA 201016
Asymptomatic Episodes of Hypoglycemia may go Unreported
vIn a cohort of patients with diabetes, more than 50% had asymptomatic (unrecognized) hypoglycemia, as identified by continuous glucose monitoring1
vOther researches have reported similar findings2,3
55.7%62.5%
46.6%
0.0 %
25 .0%
50 .0%
75 .0%
10 0.0%
A ll pat ient swit h dia bet es
Typ e 1diab et es
Typ e 2diab et es
Patie
nts,
%
Patients With ≥ 1 UnrecognizedHypoglycemia Event, %
1. Copyright © 2003 American Diabetes Association. Chico A et al. Diabetes Care. 2003:26(4):1153-1157. Reprinted with permission from The American Diabetes Association.
2. Webber KK et al. Exp. Clin Endocrinol Diabetes. 2007:115(8):491-494.3. Zick R et al. Diabetes Technol Ther. 2007:9(6):483-492
n=70 n=40 n=30
17
Why Discuss Glucose Variability?
vShould minimal blood glucose variability become the gold standard of glycemic control?
vPost-prandial hyperglycemia is a better predictor of CV mortality/complications than fasting glycemia…1-3,5
vDCCT Type I DM
vPatients with lower A1C (eg, <6%)
vPredicted ~10% of future hypoglycemic events
vHigher glucose variability
vPredicted ~60% of future hypoglycemic events
vVariability recognized as a risk for future hypoglycemia
DCCT. Diabetes. 1995;44:968-983; McCall, et al. J Diabetes Sci Technol. 2009 January;3(1):3-11.1. Hanefeld, et al. Diabetalogia. 1996;39(12):1577; 2. Ceriello. Am Heart J. 2004; 147(5):803; 3. Cavalot, et al. J Clin Endocrinol Metab, 2006;91(3):813; 4. Hirsch IB. Am J Med, 2004;116 Suppl 3A:17S; 5. Sorkin et al. Diabetes Care. Nov 2005;28(11):2626-2632.18

2/4/19
7
“Dysglycemia” = Glycemic VariabilityvThe presence of hypo and hyperglycemia in a given patient
vInsulins with high coefficient of variability can increase risk of hypoglycemia
vHypoglycemia is likely to reduce adherence to prescribed insulin regimens
vGlycemic variability increases risk of “oxidative stress” which promotes long-term diabetes related complications
vGlycemic variability is frustrating for patients and clinicians
Unger J. Concentrated and Fixed-Dose Insulin Formulations can Improve Outcomes in Patients with Type 2 Diabetes. Endocrinology, Diabetes, Metabolism Journal. 2018. 2 (1). 1-519
Glycemic Variability is Often Patient-driven
vPatients using basal-bolus insulin therapy usually adjust basal insulin rather than
short acting for hypoglycemia (it’s the bigger dose)
vBasal adjustments are reactive not proactive
vEg: PM dose needs to be lowered for AM hypo
vShort-acting insulin gets omitted, not reduced
vPatients don’t understand the insulin/glucose/meal relationship
Personal communication, Stolar M. 201820
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 23 24
120
40
80
0
160
200
240
280
320
360
400
22
Time (hours)
Glu
cose
mg
/dL
Image adapted from Penckofer et al. Diab Tech Ther 2012;14:303–10
Glucose Variability can Manifest as Both Fluctuating and Unpredictable Glucose Levels
21

2/4/19
8
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 23 24
120
40
80
0
160
200
240
280
320
360
400
22
Time (hours)
Unpredictability
Glu
cose
mg
/dL
Glucose Variability can Manifest as Both Fluctuating and Unpredictable Glucose Levels
22 Image adapted from Penckofer et al. Diab Tech Ther 2012;14:303–10
Glucose Variability can be Measured Between Individuals or Within the Same Person
v Inter-individual variabilityv GIR curves from 2 subjects with T1D
each administered insulin detemir 0.4U/kg on 4 occasions
v Responses are predictable, but vary between subjects
v Insulin doses must be individualized
v Intra-individual variabilityv GIR curves from 1 subject with T1D
administered NPH insulin 0.4U/kg on 4 occasions
v Responses are unpredictablev This patient will have difficulty titrating
to glucose targetsG IR cu rve s ad ap te d fro m H e ise et a l. D ia b etes 2 0 0 4 ;5 3 :1 6 1 4 – 2 0 0 0 ; G IR , g lu co se in fu sio n rate
0 4 8 12 16 20 24
0
1
2
3
4
5
6
7
0 4 8 12 16 20 24
0
1
2
3
4
5
6
7
GIR
(mg/
kg/m
in)
0 4 8 12 16 20 24
0
1
2
3
4
5
6
7
GIR
(mg/
kg/m
in)
23
Glucose Variability is not Apparent from A1C
24
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 23 24
120
40
80
0
160
200
240
280
320
360
400
22
Time (hrs)
Image adapted from Penckofer et al. Diab Tech Ther 2012;14:303–10
Mean BG (≈ A1C) Patient A (A1C = 7.8%) Patient B (A1C = 7.8%)
Glu
cose
mg/
dL
Hypoglycemia
Hyperglycemia

2/4/19
9
Glucose Variability is not Apparent from A1C
25
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 23 24
120
40
80
0
160
200
240
280
320
360
400
22
Time (hrs)
Mean BG (≈ A1C) Patient A (A1C = 7.8%) Patient B (A1C = 7.8%)
Glu
cose
mg/
dL
Hypoglycemia
Hyperglycemia
Image adapted from Penckofer et al. Diab Tech Ther 2012;14:303–10
SMBG vs. CGM
26
Self-Monitoring Blood Glucose (SMBG) vs. Continuous Glucose Monitoring (CGM)
27
2/4/19
10
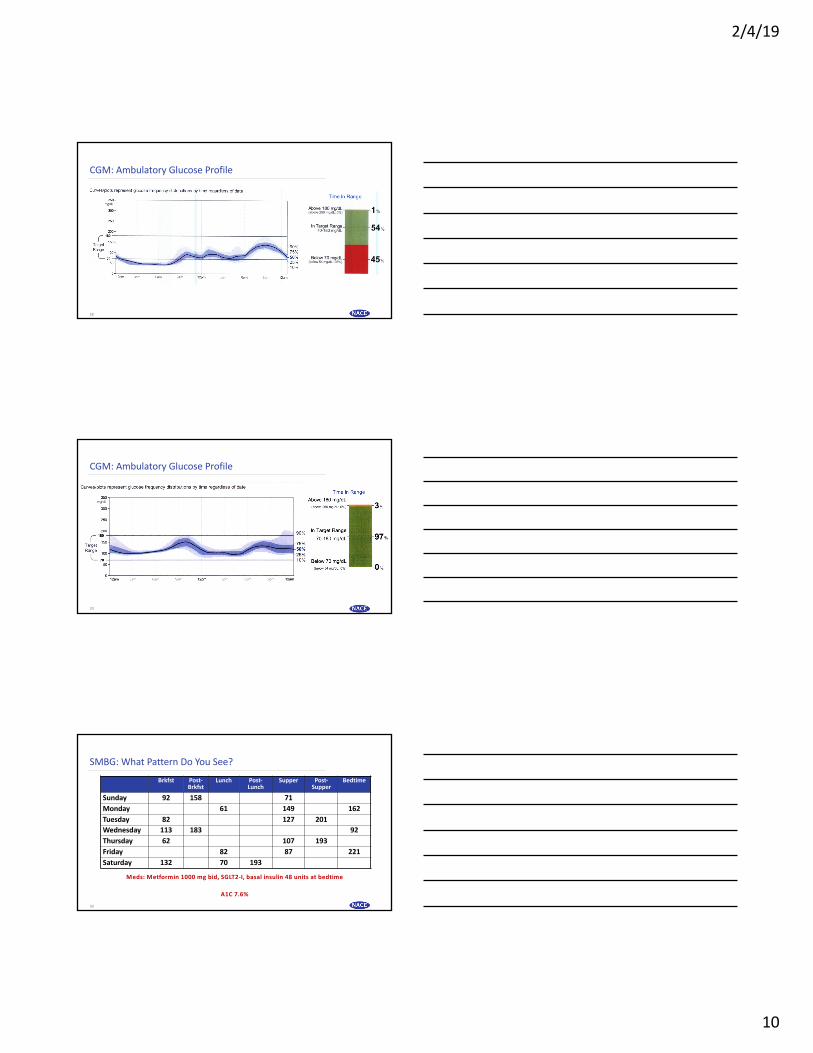
CGM: Ambulatory Glucose Profile
28
CGM: Ambulatory Glucose Profile
29
SMBG: What Pattern Do You See?Brkfst Post-
BrkfstLunch Post-
LunchSupper Post-
SupperBedtime
Sunday 92 158 71
Monday 61 149 162
Tuesday 82 127 201
Wednesday 113 183 92
Thursday 62 107 193
Friday 82 87 221
Saturday 132 70 193
Meds: Metformin 1000 mg bid, SGLT2-I, basal insulin 48 units at bedtime
A1C 7.6%
30

2/4/19
11
CGM: What Pattern Do You See?
Meds: Metformin 1000 mg bid, SGLT2-I, basal insulin 48 units at bedtime
A1C 7.6%
31
Available Glucose Sensors
Type of CGM Abbott Freestyle Libre Medtronic EnliteGuardian Sensor 3
iPro2
Dexcom 4, 5, 6, 7
Calibration necessary? No Yes Yes
Sensor duration 14 days 6 days 7 days (G4,5,6)14 days (G7)
Audible alerts for high and low glucose
No Yes Yes
Trend arrow displayed? Yes Yes Yes
Connectivity to insulin pump No Yes Anticipated 2019
Smartphone app Yes No Yes
32
Individualizing Insulin Therapy
33

2/4/19
12
Insulins to Match the Physiologic Insulin Profile
vBasal (background) insulinvLong-acting (~24 hours), peakless (doses < 0.5 units/kg)
vReduces hepatic glucose production (gluconeogenesis, glycogenolysis) and lipogenesis
vApproximately 60% of patients with T2D can achieve targeted A1C with basal insulin alone if taken CONSISTENTLY
vNormal basal insulin concentration = 1 unit/hr (24 units/d)
Unger, J. Diabetes Therapy. 2011;2 (1):1-11.34
Desired Characteristics of Replacement Basal Insulin
35
v Mimics “physiologic” pancreatic basal insulin secretory pattern
v Peakless and predictable PK profile
v Protracted duration of action to provide dosing flexibility
v Minimizes risk of nocturnal hypoglycemia and weight gain
v Can be used in combination with other antidiabetic drugs
Basal Insulin Coefficient of Variability*
36
Insulin Coefficient of Variability (%)NPH 68Glargine U100 48Detemir 27Glargine U300 34.8Degludec 20
*% within-subject variability based on glucose infusion rates and AUC
Patients receive 4 single subcutaneous doses of 0.4 U/kg under euglycemic glucose clamp conditions on 4 study days
Unger J. Concentrated and Fixed-Dose Insulin Formulations can Improve Outcomes in Patients with Type 2 Diabetes. Endocrinology, Diabetes, Metabolism Journal. 2018. 2 (1). 1-5.Heise et Al (2012).diabetes obesity metabolism. 2012; 14(9): 859-864
2/4/19
13
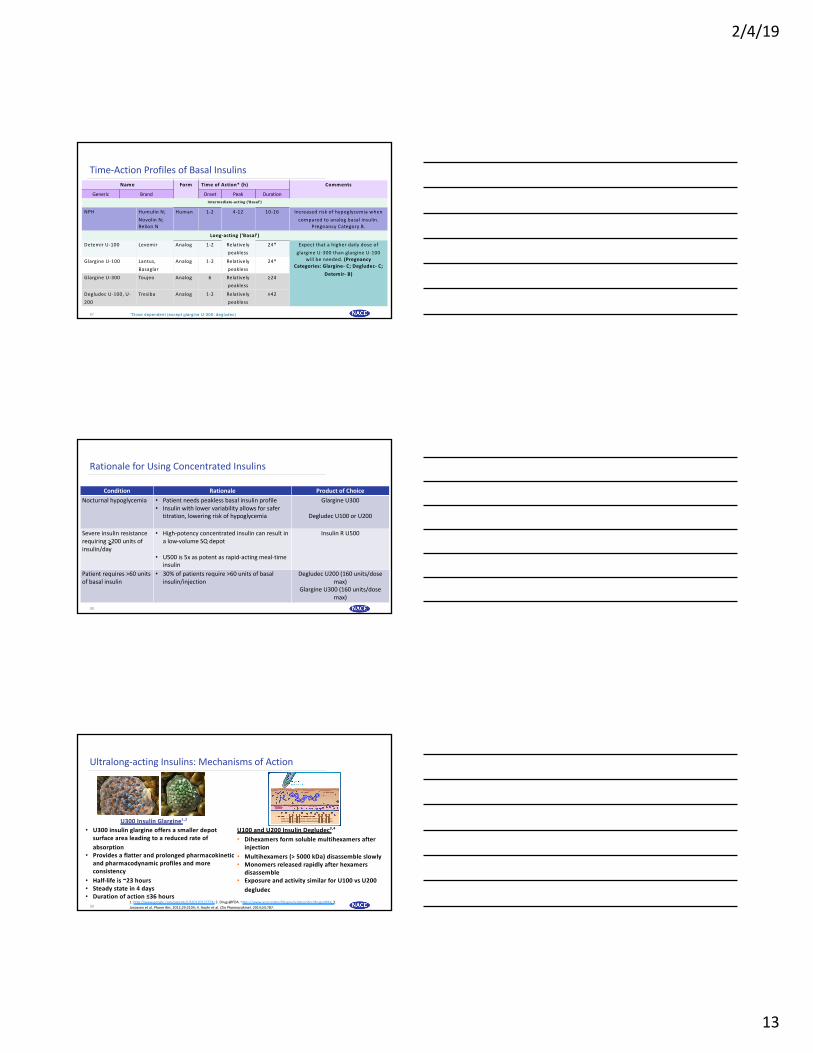
Name Form Time of Action* (h) Comments
Generic Brand Onset Peak Duration
Interm ediate-acting (‘Basal’)
NPH Humulin N;
Novolin N;
Relion N
Human 1-2 4-12 10-16 Increased risk of hypoglycemia when
compared to analog basal insulin.
Pregnancy Category B.
Long-acting (‘Basal’)
Detemir U-100 Levemir Analog 1-2 Relatively
peakless
24* Expect that a higher daily dose of
glargine U-300 than glargine U-100
will be needed. (Pregnancy Categories: Glargine- C; Degludec- C;
Detemir- B)
Glargine U-100 Lantus,
Basaglar
Analog 1-2 Relatively
peakless
24*
Glargine U-300 Toujeo Analog 6 Relatively
peakless
≥24
Degludec U-100, U-
200
Tresiba Analog 1-2 Relatively
peakless
≥42
*Dose dependent (except glargine U-300, degludec)
Time-Action Profiles of Basal Insulins
37
Rationale for Using Concentrated Insulins
Condition Rationale Product of ChoiceNocturnal hypoglycemia • Patient needs peakless basal insulin profile
• Insulin with lower variability allows for safer titration, lowering risk of hypoglycemia
Glargine U300
Degludec U100 or U200
Severe insulin resistance requiring >200 units of insulin/day
• High-potency concentrated insulin can result in a low-volume SQ depot
• U500 is 5x as potent as rapid-acting meal-time insulin
Insulin R U500
Patient requires >60 units of basal insulin
• 30% of patients require >60 units of basal insulin/injection
Degludec U200 (160 units/dose max)
Glargine U300 (160 units/dose max)
38
Ultralong-acting Insulins: Mechanisms of Action
1. http://www.google.com/patents/US20120122774; 2. Drugs@FDA. https://www.accessdata.fda.gov/scripts/cder/drugsatfda; 3. Jonassen et al. Pharm Res. 2012;29:2104; 4. Haahr et al. Clin Pharmacokinet. 2014;53:787.
U300 Insulin Glargine1,2
U100 and U200 Insulin Degludec3,4
• Dihexamers form soluble multihexamers after injection
• Multihexamers (> 5000 kDa) disassemble slowly• Monomers released rapidly after hexamers
disassemble • Exposure and activity similar for U100 vs U200
degludec
• U300 insulin glargine offers a smaller depot surface area leading to a reduced rate of absorption
• Provides a flatter and prolonged pharmacokinetic and pharmacodynamic profiles and more consistency
• Half-life is ~23 hours • Steady state in 4 days• Duration of action ≤36 hours
39

2/4/19
14
Ultralong-acting Basal InsulinsHave Minimal Glycemic Variability
40
1. Becker RH, et al. Diabetes Obes Metab. 2015;17:261-267. 2. Haahr H, Heise T. Clin Pharmacokinet. 2014;53:787-800.3. Porcellati F, et al. Diabetes Care. 2011;34:2521-2523.
a 2-period crossover study in T1DM ; n = 50.b 3-period crossover study in T2DM .
0
1
3
Time, h
2Period 1 Period 2
Average glucose infusion rate (GIR)G
IR, m
g/kg
/min
0 6 12 18 24
U-300 glargine1,a
Time Since Injection, h
11.0
8.3
5.5
2.8
0 6 36 420.0
Bloo
dG
luco
seLe
vel,
mm
ol/L
Individual patient profilesMean profile
12 18 24 30
U-100 degludec2
U
Pharmacodynamics: U300 Glargine v U100 Glargine
41
• U300 glargine has a flatter more prolonged effect
• Time required for 50% of the effect of a single injection:
– U100 = 12.1 hours
– U300 = 16.7 hours
GIR: glucose infusion rate
GIR
(m
g/
kg
-1m
in-1
)*
1.5
3.0
0
0 36
Time (hours)3024126 18
0.5
2.5U100 0.4 U/kg-1
U300 0.4 U/kg-12.0
1.0
U300 0.6 U/kg-1
U300 0.9 U/kg-1
SC Injection
Tillner J, et al. Poster 920P 73rd ADA Scientific Sessions June 21-25, 2013, Chicago, IL.
Pharmacodynamics of Degludec
42Josse RG and Woo V. Diabetes Obes Metab. 2013;15(12):1077-1084; Garber AJ. Diabetes Obesity Metab 2014; 16:483-491; Heise et al. Diabetes Obes Metab 2012;14:944–50
Gluc
ose
Low
erin
g Ef
fect
on D
ay 6
(mg/
kg/m
in)
2
6
0
0 24
Time since Injection (hours)201684 12
4
1
3
5
Ideg 0.4 U/kg
Ideg 0.8 U/kgIdeg 0.6 U/kg
6 ►desB30 insulin acylated (16-c fatty acid
chain) at LysB29
►Half-life is ~25.4 h, duration > 42 h

2/4/19
15
Glycemic Variability: Glargine U100 v. Degludec ― SWITCH 2
43
v721 pts with T2D randomized to glargine U100 or degludec
vTwo 32-week trial periods; crossover design
vCompared with glargine, degludec resulted in:
v30% ¯ confirmed hypoglycemia
v42% ¯ nocturnal hypoglycemia
v51% ¯ in severe hypoglycemia
vGlargine and degludec patients achieved similar A1C reductions and had similar insulin dose requirements
Wysham C, et al. Paper presented at: 76th Scientific Sessions of the American Diabetes Association; June 10-14, 2016; New Orleans, LA.
Glycemic Variability: Glargine U100 v. Glargine U300 ― EDITION 1
Ritzel et al. Diabetes Obes Metab. Sep 2015;17(9):859-867.44
Beyond Basal
45
2/4/19
16
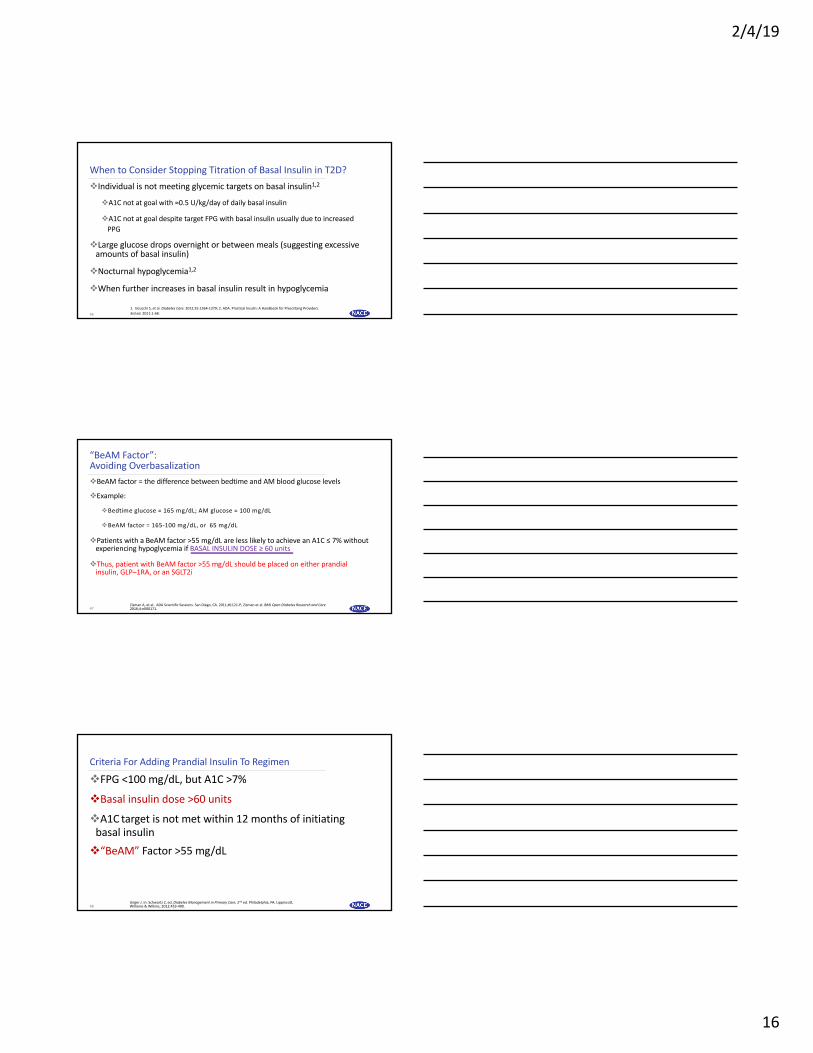
When to Consider Stopping Titration of Basal Insulin in T2D?
46
vIndividual is not meeting glycemic targets on basal insulin1,2
vA1C not at goal with ≈0.5 U/kg/day of daily basal insulin
vA1C not at goal despite target FPG with basal insulin usually due to increased PPG
vLarge glucose drops overnight or between meals (suggesting excessive amounts of basal insulin)
vNocturnal hypoglycemia1,2
vWhen further increases in basal insulin result in hypoglycemia
1. Inzucchi S, et al. Diabetes Care. 2012;35:1364-1379; 2. ADA. Practical Insulin: A Handbook for Prescribing Providers. 3rd ed. 2011:1-68.
“BeAM Factor”: Avoiding Overbasalization
47
vBeAM factor = the difference between bedtime and AM blood glucose levels
vExample:
vBedtime glucose = 165 mg/dL; AM glucose = 100 mg/dL
vBeAM factor = 165-100 mg/dL, or 65 mg/dL
vPatients with a BeAM factor >55 mg/dL are less likely to achieve an A1C ≤ 7% without experiencing hypoglycemia if BASAL INSULIN DOSE ≥ 60 units
vThus, patient with BeAM factor >55 mg/dL should be placed on either prandial insulin, GLP–1RA, or an SGLT2i
Zisman A, et al.. ADA Scientific Sessions. San Diego, CA. 2011;#1121-P; Zisman et al. BMJ Open Diabetes Research and Care 2016;4:e000171.
Criteria For Adding Prandial Insulin To Regimen
vFPG <100 mg/dL, but A1C >7%
vBasal insulin dose >60 units
vA1C target is not met within 12 months of initiating basal insulin
v“BeAM” Factor >55 mg/dL
Unger J. In: Schwartz Z, ed. Diabetes Management in Primary Care, 2nd ed. Philadelphia, PA: Lippincott, Williams & Wilkins; 2012:453-490.48

2/4/19
17
Clinical Features of Rapid-Acting Analogues: Aspart, Glulisine, and Lispro
49
vAdministration immediately prior to meals
vFaster onset of action matches timing of carbohydrate absorption
vLimits postprandial hyperglycemic peaks
vShorter duration of activity
vReduced risk of late postprandial hypoglycemia
vFrequently can have late postprandial hyperglycemia
vGlulisine can be given after meals if needed1
1. Garg S et al. American Diabetes Association 64th Scientific Sessions; June 4-8, 2004; Orlando, FL; Abstract 530-P.
Fewer Nocturnal Hypoglycemic Events in Patients Treated with Aspart v. Regular Human Insulin
50
Aspart0
Regular Human Insulin
0.5
1.0
1.5
2.0
2.5
3.0
72%
P=0.001
Maj
or N
octu
rnal
Hyp
oglyc
emic
Even
ts p
er P
atie
nt-Y
ear
Adapted from Heller SR et al. Diabet Med. 2004;21:769-775.
Post-meal Delta Interpretation
>50 mg/dL
►Not enough insulin used to cover carbs
►�Insulin lag time� not utilized
► Illness (flu)
►Snacking between the meal and 2-hour check time
>100 mg/dL
►Forgot to give insulin (especially if delta >200 mg/dL)
► Insulin has expired or is denatured
► Insulin antibodies forming
► Insulin-to-carb mismatch
<50 mg/dL
►Too much insulin (watch for hypoglycemia)
►Alcohol use (decreases gluconeogenesis)
► Insulin stacking: consider this option when the delta is NEGATIVE at
2 hours!
Paired Glucose Testing Can Provide Valuable Information to Patients
51 Unger J. Educating patients about hypoglycemia prevention and self-management. Clinical Diabetes. 2013. 31 (4). 179-188

2/4/19
18
Summary
52
SummaryvPatients are often unaware of hypoglycemic episodes
vMajor hypoglycemic events increase risk for hypoglycemia unawareness
vNocturnal hypoglycemia is largely unrecognized
vThe risks of hypoglycemia include increased risk for adverse cardiac outcomes
vGlycemic variability increases risk for hypoglycemia
vTraditional basal insulins have relatively high coefficients of variability
vNewer, concentrated insulins have longer duration of action, reduced variability, and lower risks for nocturnal hypoglycemia and weight gain
vStructured BG monitoring can help to detect variability, nocturnal hypoglycemia, and other key patterns
vCGM provides the best representation of daily glycemic patterns 53
Post-test Questions
54

2/4/19
19
Post-test Question 1Post-D1: In studies of patients with T2D, approximately what proportion have asymptomatic hypoglycemic episodes?1. <10%2. ~25%3. ~40% 4. >50%
55
Post-test Question 2Post-D2: In clinical trials, which of the following insulin formulations has demonstrated the lowest glycemic variability? 1. NPH insulin 2. Insulin detemir3. Insulin degludec 4. Insulin glargine U100
56
Post-test Question 3
Post-D3: Which of the following is associated with higher rates of hypoglycemia? 1. A1C levels near target2. BeAM factor < 50 mg/dL3. Higher glucose variability 4. Postprandial glucose levels above target
57

2/4/19
20
Post-test Question 4Post-D4: 54 y/o man with 9-year history of T2D presents for checkup. His A1C
is 7.6%
SMBG: AM 150-200 mg/dL; HS 120-150 mg/DL.
Medications: metformin 1000 mg bid, canagliflozin 300 mg qd, and insulin
glargine U100 48 units HS.
Attempts to increase basal insulin dose in the past have led to daytime hypoglycemia. What might you do now?
1. Add GLP-1 receptor agonist 2. Switch from basal insulin to premixed insulin
3. Switch from glargine u100 to glargine u300 and potentially increase dose4. Ask patient to use continuous glucose monitor, or SMBG 4 times a day, for 4
days and adjust meds based on findings
58
Post-test Question 5
59
Post-D5: 44 y/o woman with a 10-year history of T2D presents with A1C 7.6%.
Meds: metformin 1000 mg bid and insulin glargine U100 56 units qhs.
Because of inconsistent fasting self-monitored blood glucose readings, her clinician recommended she use a continuous glucose monitor for several days which show a high degree of glycemic variability throughout the day, and occasional episodes of nocturnal hypoglycemia.
What might you do now?
1. Add SGLT-2 inhibitor or GLP-1 receptor agonist2. Administer insulin glargine U100 in divided doses3. Add prandial insulin and reduce dose of insulin glargine U100 4. Switch from insulin glargine U100 to ultralong-acting basal insulin
Post-test Question 6
60
Post-D6: Approximately how many patients with Type 2 Diabetes do you see on a weekly basis, in any clinical setting? 1. None2. 1-53. 6-104. 11-15 5. 16-206. 21-257. > 25

2/4/19
21
Q&A
61