Copy Of Cva(3)
88
Cerebro Cerebro vascular vascular accidents accidents PRESENTED BY PRESENTED BY JOMI JOSEPH E JOMI JOSEPH E GIKKU ALIAS BENNY GIKKU ALIAS BENNY
-
Upload
jomijosephe -
Category
Health & Medicine
-
view
7.715 -
download
1
description
see this....
Transcript of Copy Of Cva(3)

Cerebro Cerebro vascular vascular accidentsaccidents
PRESENTED BYPRESENTED BY
JOMI JOSEPH EJOMI JOSEPH E
GIKKU ALIAS BENNYGIKKU ALIAS BENNY

prayerprayer
““Ragadi rogan sathathanu shakthanRagadi rogan sathathanu shakthan
AsheshakayaprasruthanasheshanAsheshakayaprasruthanasheshan
Outhusukya mohaarathithan Outhusukya mohaarathithan jakkanajakkana
Yo apoorva vaidya namosthu Yo apoorva vaidya namosthu thasmaii”thasmaii”

contentscontents Definition of CVADefinition of CVA Blood supply of cerebral hemispheresBlood supply of cerebral hemispheres ClassificationClassification StrokeStroke Ischemia & infarctionIschemia & infarction HaemorrhagesHaemorrhages Stroke in old ageStroke in old age Stroke in childrenStroke in children ExaminationExamination InvestigationInvestigation Differential diagnosisDifferential diagnosis ManagementManagement Conclusion.Conclusion.

definitiondefinition
A cerebrovascular accident (CVA) is an A cerebrovascular accident (CVA) is an ischemic attack of brain tissue or ischemic attack of brain tissue or ultimately an infarction of brain tissue ultimately an infarction of brain tissue caused by an interruption in cerebral blood caused by an interruption in cerebral blood flow. This results from damage to an flow. This results from damage to an artery supplying blood to the brain. artery supplying blood to the brain. Ischimia of brain tissue lasting five Ischimia of brain tissue lasting five minutes or less will cause permanent minutes or less will cause permanent damage because neural tissue is incapable damage because neural tissue is incapable of regenerationof regeneration

Causes of CVAsCauses of CVAs
cardiac diseasecardiac diseasetraumatraumainfectioninfectionneoplasm (tumor)neoplasm (tumor)exogenous toxinsexogenous toxinsarterio-venous malformations (AVMs) arterio-venous malformations (AVMs)

Blood Supply of BrainBlood Supply of Brain
Internal Carotid ArteriesInternal Carotid Arteries :transfer :transfer oxygen-oxygen- ated blood from the ated blood from the common carotid common carotid arteries of the arteries of the neck to the circle of neck to the circle of Willis.Willis.
Circle of WillisCircle of Willis : transfers : transfers oxygenated blood from incoming oxygenated blood from incoming arteries to deep internal arteries of arteries to deep internal arteries of the brain.the brain.

Vertebral ArteriesVertebral Arteries : transfer oxygen- : transfer oxygen-ated blood from the subclavian ated blood from the subclavian arteries, arteries, up through the up through the transverse foraminae of the cervical transverse foraminae of the cervical vertebrae and to the basilar vertebrae and to the basilar artery of the brain.artery of the brain.
Basilar ArteryBasilar Artery : transfers oxygenated : transfers oxygenated blood from the vertebral arteries to blood from the vertebral arteries to the circle of Willis of thebrain. the circle of Willis of thebrain.

Principle Brain ArteriesPrinciple Brain Arteries

•aortic archaortic arch
•external carotidexternal carotid
•Posterior cerebralPosterior cerebral
•basilarbasilar
•vertebralvertebral
•internal carotidinternal carotid
•middle cerebralmiddle cerebral
•anterior cerebralanterior cerebral

The major types of The major types of cerebrovascular accidentcerebrovascular accident
Stroke Stroke Cerebral ischaemia and Cerebral ischaemia and
infarctioninfarction Transient Ischemic AttacksTransient Ischemic Attacks Atherosclerotic thrombosisAtherosclerotic thrombosis LacunesLacunes EmbolismEmbolism HemorrhageHemorrhage

Definition Of StrokeDefinition Of Stroke
““Rapidly developed clinical sign of Rapidly developed clinical sign of focal disturbance of cerebral focal disturbance of cerebral function of presumed vascular origin function of presumed vascular origin and of more than 24 hours” (and of more than 24 hours” (WHO)WHO)
TIA (Transient Ischaemic Attack) TIA (Transient Ischaemic Attack) recovery is complete within 24 recovery is complete within 24 hours. 10% of patients will go on to hours. 10% of patients will go on to have a stroke.have a stroke.

Sub-types Of StrokeSub-types Of Stroke
Ischaemic – obstruction to one of Ischaemic – obstruction to one of major cerebral arteries, brainstem major cerebral arteries, brainstem strokes are less common.strokes are less common.
Haemorrhage – 9% are caused by Haemorrhage – 9% are caused by haemorrhage to the deep parts of haemorrhage to the deep parts of the brain. Patients are usually the brain. Patients are usually hypertensive.hypertensive.

classificationclassification
Based on durationBased on duration
-Stroke-Stroke
-Transiant ischaemic attack-Transiant ischaemic attack
-Minor stroke-Minor stroke Based on pathology of underlying Based on pathology of underlying
focal -brain injuryfocal -brain injury
-Infarction-Infarction
-Haemorrhage.-Haemorrhage.

Clinical classificationClinical classification
Transient ischemic attack (TIA) :lasting Transient ischemic attack (TIA) :lasting less than 24hrs.less than 24hrs.
Evolving stroke:gradual step wise Evolving stroke:gradual step wise developmentof stroke.developmentof stroke.
Reversible ischemic neurological deficit Reversible ischemic neurological deficit (RIND):resolve within 1-3 weeks.(RIND):resolve within 1-3 weeks.
Completed stroke:rapid in onset,doesn’t Completed stroke:rapid in onset,doesn’t progress beyond 96hrsprogress beyond 96hrs


EtiologyEtiology
Complication of several disordersComplication of several disorders Atherosclerosis – most common.Atherosclerosis – most common. Hypertension, smoking, diabetes.Hypertension, smoking, diabetes. Heart disease – Atrial fibrillation.Heart disease – Atrial fibrillation. Other: Other:
– Trauma – fat embolismTrauma – fat embolism– Tumor, InfectionTumor, Infection– Caissons diseaseCaissons disease

Risk factorsRisk factors
Non modifiableNon modifiable AgeAge Male sexMale sex RaceRace HeredityHeredity
ModifiableModifiable HypertensionHypertension DiabetesDiabetes SmokingSmoking HyperlipidemiaHyperlipidemia Excess Alcohol*Excess Alcohol* Heart disease (AF) Heart disease (AF)
Oral contraceptivesOral contraceptives HypercoagulabilityHypercoagulability

Complications of acute Complications of acute strokestroke
Chest infectionChest infection Epileptic seizuresEpileptic seizures Deep venous thrombosisDeep venous thrombosis Pulmonary embolisamPulmonary embolisam Painful sholderPainful sholder Pressur soresPressur sores Urinary infectionUrinary infection ConstipationConstipation Depression & anxietyDepression & anxiety

Stroke: IschemiaStroke: Ischemia
Insufficiency of blood supplyInsufficiency of blood supplyGlucose & O2 deprivation, build-up of Glucose & O2 deprivation, build-up of
wasteswastesNOT synonymous Anoxia: NOT synonymous Anoxia:
O2 deprivation onlyO2 deprivation only
Few seconds: little or no damageFew seconds: little or no damage 6-8 minutes ---> Infarction6-8 minutes ---> Infarction
neurons & other cells dieneurons & other cells die

A consequence of ischemia. Acute A consequence of ischemia. Acute right hemispheric infarction withright hemispheric infarction withswelling leading to uncal herniation. swelling leading to uncal herniation. This picture of the base of the This picture of the base of the
A consequence of ischemia. Acute right hemispheric infarction withA consequence of ischemia. Acute right hemispheric infarction with
swelling leading to uncal herniation. This picture of the base of theswelling leading to uncal herniation. This picture of the base of the
brain shows the necrotic, herniated mesial temporal lobe (arrowhead).brain shows the necrotic, herniated mesial temporal lobe (arrowhead).

Cerebral ischaemia and Cerebral ischaemia and infarctioninfarction
The principal pathological process The principal pathological process under consideration here is the under consideration here is the occlusion of arteries supplying the occlusion of arteries supplying the brain. The two internal carotid arteries brain. The two internal carotid arteries and the basilar artery form the Circle and the basilar artery form the Circle of Willis at the base of the brain, of Willis at the base of the brain, which acts as an efficient anatomotic which acts as an efficient anatomotic device in the event of occlusion of device in the event of occlusion of arteries proximal to it.arteries proximal to it.

Occlusion leads to sudden severe Occlusion leads to sudden severe ischaemia in the area of brain tissue ischaemia in the area of brain tissue supplied by the occluded artery, and supplied by the occluded artery, and recovery depends upon rapid lysis or recovery depends upon rapid lysis or fragmentation of the occluding material:fragmentation of the occluding material:Reversal of neurological function within Reversal of neurological function within minutes or hours gives rise to the clinical minutes or hours gives rise to the clinical picture of a transient ischaemic attackpicture of a transient ischaemic attack..When the neurological deficit lasts longer When the neurological deficit lasts longer than 24 hours, it may be called a than 24 hours, it may be called a reversible ischaemic neurological deficit reversible ischaemic neurological deficit ( RIND ) if it recovers completely in a few ( RIND ) if it recovers completely in a few days,days,or a completed stroke if there is a or a completed stroke if there is a persistent deficit.persistent deficit.Sometimes recovery is very slow and Sometimes recovery is very slow and incompleteincomplete..


Neurological symptoms Neurological symptoms and signs and signs
The loss of function that the The loss of function that the patient notices, and which may patient notices, and which may be apparent on examination, be apparent on examination, entirely depends on the area entirely depends on the area of brain tissue involved in the of brain tissue involved in the ischaemic processischaemic process

Clinical CategoriesClinical Categories
Global Ischemia.Global Ischemia.Hypoxemic encephalopathyHypoxemic encephalopathyHypotension, hypoxemia, anemia.Hypotension, hypoxemia, anemia.
Focal Ischemia.Focal Ischemia.Obstruction to blood supply to focal Obstruction to blood supply to focal
area.area.Thrombosis, embolism or hemorrhageThrombosis, embolism or hemorrhage

Global IschemiaGlobal Ischemia Etiology:Etiology:
– Impaired blood supply -Lung & Heart disorders.Impaired blood supply -Lung & Heart disorders.– Impaired O2 carrying – Anemia/Blood dis.Impaired O2 carrying – Anemia/Blood dis.
MorphologyMorphology::– Laminar necrosis, Hippocampus, Purkinje cells.Laminar necrosis, Hippocampus, Purkinje cells.– Border zone infarcts – “Watershed”Border zone infarcts – “Watershed”– Sickle shaped band of necrosis on cortex.Sickle shaped band of necrosis on cortex.
ClinicalClinical FeaturesFeatures::– Mild transient confusion state toMild transient confusion state to– Severe irreversible brain death. Flat EEG, Severe irreversible brain death. Flat EEG,
Vegetative state. Coma.Vegetative state. Coma.

Focal IschemiaFocal Ischemia
Thrombosis:Thrombosis:– Progressive, recurrent, Progressive, recurrent, – Pale or ischemic infarct.Pale or ischemic infarct.– Eg. Lacunar infarctEg. Lacunar infarct
Embolism / Hemorrhage:Embolism / Hemorrhage:– Sudden.Sudden.– Red or hemorrhagic infarct.Red or hemorrhagic infarct.– Atherosclerosis – rupture/embolismAtherosclerosis – rupture/embolism

Transient Ischemic Transient Ischemic Attacks(TIA)Attacks(TIA)
– Definition of termDefinition of term
Current opinion holds that TIAs are Current opinion holds that TIAs are brief, reversible episodes of focal, brief, reversible episodes of focal, nonconvulsive ischaemic neurologic nonconvulsive ischaemic neurologic disturbance, Consensus has been that disturbance, Consensus has been that their duration should be less than 24 h.their duration should be less than 24 h.

PathogenesisPathogenesis
Pathogenesis of Ischemic neuronal Pathogenesis of Ischemic neuronal deathdeath
IschemiaIschemia
↓ ↓ Excitatory amino acid receptorsExcitatory amino acid receptors
↓ ↓ Borderzone or penumbraBorderzone or penumbra
↓ ↓ Programmed cell deathProgrammed cell death

Different types of TIADifferent types of TIA
LOW FLOW TIA- Brief, recurrent,sterrotyped LOW FLOW TIA- Brief, recurrent,sterrotyped associated with atheroscleroticlesion at associated with atheroscleroticlesion at ICA,MCA STEM junction of veretabral ICA,MCA STEM junction of veretabral &basilar arteries.&basilar arteries.
embolicTIA-discrete,single,prolonged,it lasts embolicTIA-discrete,single,prolonged,it lasts for less than 24 hrs,it idicates infarct has for less than 24 hrs,it idicates infarct has occuered.occuered.
Lacunar/penetrating vessel TIA-occlusion of Lacunar/penetrating vessel TIA-occlusion of small vessels as a result of lipohyalinosis in small vessels as a result of lipohyalinosis in response to HTNresponse to HTN

Clinical pictureClinical picture
Transient Ischaemic Attacks can reflect the Transient Ischaemic Attacks can reflect the involvement of any cerebral artery. The loss of involvement of any cerebral artery. The loss of function entirely depends on the influenced function entirely depends on the influenced artery.artery.It may last a few seconds or up to 12 to 24 h, It may last a few seconds or up to 12 to 24 h, Most of them last 2 to 15 min.Most of them last 2 to 15 min.There are only a few attacks or several hundred.There are only a few attacks or several hundred.Between attacks, the neurologic examination may Between attacks, the neurologic examination may disclose no abnormalities.disclose no abnormalities.A stroke may occur after numerous attacks have A stroke may occur after numerous attacks have occurred over a period of weeks or months.occurred over a period of weeks or months.

Brain infarctionBrain infarction
Blood supply to brain is interuptedBlood supply to brain is interupted For 30 sec. Brain metabolism For 30 sec. Brain metabolism
alteredaltered For 1 mte neuronal function may For 1 mte neuronal function may
ceasecease For 5 mte anoxia initiates.For 5 mte anoxia initiates.

local vaso dilation local vaso dilation
stasis of blood stasis of blood
colum colum
segmentation of blood cellssegmentation of blood cells
oedemaoedema
necrosis of brain necrosis of brain tissuetissue

Infarct PathogenesisInfarct Pathogenesis
Reduced blood supply – hypoxia/anoxia.Reduced blood supply – hypoxia/anoxia. Altered metabolism Altered metabolism Na/K pump block. Na/K pump block. Glutamate receptor act. Glutamate receptor act. calcium calcium
influx.influx. 1-6 min – ischemic injury – vacuolation.1-6 min – ischemic injury – vacuolation. >6 min – cell death.>6 min – cell death.

Causes of infarctsCauses of infarcts Thrombosis/occlusionThrombosis/occlusion Decreased blood flow:Decreased blood flow:
- hypotension- hypotension
- vascular stenosis- vascular stenosis
- increase in vascular permeability- increase in vascular permeability EmboliEmboli
- artery to artery ( arterial territory )- artery to artery ( arterial territory )
- cardioembolic - cardioembolic

Infarct StagesInfarct Stages
Immediate – 6 hoursImmediate – 6 hours– No Change both gross & microNo Change both gross & micro
Acute stage – 2 daysAcute stage – 2 days– Oedema, loss of grey/white matter border.Oedema, loss of grey/white matter border.– Inflammation, Red neurons, neutrophilsInflammation, Red neurons, neutrophils
Intermediate stage – 2 weeks.Intermediate stage – 2 weeks.– Demarcation, soft friable tissue, cystsDemarcation, soft friable tissue, cysts– Macrophages, liquifactive necrosisMacrophages, liquifactive necrosis
Late stage – After 4 weeks.Late stage – After 4 weeks.– Fluid filled cysts with dark grey margin (gliosis)Fluid filled cysts with dark grey margin (gliosis)– Removal of tissue by macrophagesRemoval of tissue by macrophages– Gliosis – proliferation of glia, loss of architectureGliosis – proliferation of glia, loss of architecture

typestypes
Atherosclerottic infarctionAtherosclerottic infarction Cardiac embolisamCardiac embolisam Small vessel lacunar infarction Small vessel lacunar infarction Cryptogenic infarction.Cryptogenic infarction.

Atherosclerotic Atherosclerotic infarctioninfarction
Atherosclerotic plaque at the Atherosclerotic plaque at the bifurcation or curve in one of the bifurcation or curve in one of the large vesselslarge vessels
Leads to progressive stenosis with Leads to progressive stenosis with final large artery occlusionfinal large artery occlusion
Caused by trombosis of narrowed Caused by trombosis of narrowed lumen.lumen.


Embolic infarctionEmbolic infarction
This is one of the most common cause of This is one of the most common cause of stroke. In most cases of cerebral embolism, stroke. In most cases of cerebral embolism, the embolic material consists of a fragment the embolic material consists of a fragment that has broken away from a thrombus that has broken away from a thrombus within the heart. Embolism due to fat, within the heart. Embolism due to fat, tumor cells, fibrocartilage, amniotic fluid, or tumor cells, fibrocartilage, amniotic fluid, or air is a rare occurrence and seldom enters air is a rare occurrence and seldom enters into the differential diagnosis of stroke.into the differential diagnosis of stroke.

Clinical PictureClinical Picture
Of all strokes, those due to cerebral Of all strokes, those due to cerebral embolism develop most rapidly.embolism develop most rapidly.The embolus strikes at any time of The embolus strikes at any time of the day or night. Getting up to go to the day or night. Getting up to go to the bathroom is a time of danger.the bathroom is a time of danger.The neurologic picture will depend The neurologic picture will depend on the artery involved and the site on the artery involved and the site of obstruction.of obstruction.

It is important to repeat that an It is important to repeat that an embolus may produce a severe embolus may produce a severe neurologic deficit that is only neurologic deficit that is only temporary; symptoms disappear as temporary; symptoms disappear as the embolus fragments. In other the embolus fragments. In other words , embolism is a common words , embolism is a common cause of a single evanescent cause of a single evanescent stroke that may reasonably be stroke that may reasonably be called a prolonged TIA. Also as called a prolonged TIA. Also as already pointed out, several already pointed out, several emboli can give rise to two or emboli can give rise to two or three transient attacks of three transient attacks of differing pattern or , rarely , of differing pattern or , rarely , of almost identical pattern.almost identical pattern.

Course and prognosisCourse and prognosis Most patients survive the initial Most patients survive the initial
insult, and in many the neurologic insult, and in many the neurologic deficit may recede relatively deficit may recede relatively rapidly, as indicated above. rapidly, as indicated above. The eventual prognosis is The eventual prognosis is determined by the occurrence of determined by the occurrence of further emboli and the gravity of further emboli and the gravity of the underlying illness- cardiac the underlying illness- cardiac failure myocardial infarction, failure myocardial infarction, bacterial endocarditis and so on.bacterial endocarditis and so on.

Embolism formationEmbolism formation

Cerebral thrombosisCerebral thrombosis
Most cerebrovascular disease can Most cerebrovascular disease can be attributed to atheroscleroses be attributed to atheroscleroses and chronic hypertension; until and chronic hypertension; until ways are found to prevent or ways are found to prevent or control them, vascular disease of control them, vascular disease of the brain will continue to be a the brain will continue to be a major cause of morbiditymajor cause of morbidity

EmbolismEmbolism

Clinical pictureClinical picture In more than half of patients, the main In more than half of patients, the main
part of the stroke is preceded by minor part of the stroke is preceded by minor signs or one or more transient attacks signs or one or more transient attacks of focal neurologic dysfunction. The of focal neurologic dysfunction. The final stroke may be preceded by one or final stroke may be preceded by one or two attacks or a hundred or more brief two attacks or a hundred or more brief TIAs, and stroke may follow the onset of TIAs, and stroke may follow the onset of the attacks by hours, weeks, or, rarely, the attacks by hours, weeks, or, rarely, months.months.
The most occurrence of the thrombotic The most occurrence of the thrombotic stroke is during sleep.The patient stroke is during sleep.The patient awakens paralyzed. Either during the awakens paralyzed. Either during the night or in the morning.night or in the morning.
Unaware of any difficulty, he may arise Unaware of any difficulty, he may arise and fall helplessly to the floor with the and fall helplessly to the floor with the first stepfirst step

Clinical pictureClinical picture
Associated symptomsAssociated symptoms
– SeizuresSeizures accompany the onset of stroke accompany the onset of stroke in a small number of cases (10-50%); in in a small number of cases (10-50%); in other instances, they follow the stroke other instances, they follow the stroke by weeks to years. The presence of by weeks to years. The presence of seizures does not definitively distinguish seizures does not definitively distinguish embolic from thrombotic strokes, but embolic from thrombotic strokes, but seizure at the onset of stroke may be seizure at the onset of stroke may be more common with embolus.more common with embolus.

Clinical pictureClinical picture
Associated symptomsAssociated symptoms– Headache Headache occurs in about 25% of occurs in about 25% of
patients with ischaemic stroke, patients with ischaemic stroke, possibly because of the acute dilation possibly because of the acute dilation of collateral vessels.of collateral vessels.

Course and PrognosisCourse and Prognosis When the patient is seen early in the When the patient is seen early in the
cerebral thrombosis, it is difficult to cerebral thrombosis, it is difficult to give an accurate prognosis.give an accurate prognosis.
As for the eventual or long-term As for the eventual or long-term prognosis of the neurologic deficit , prognosis of the neurologic deficit , there are many possibilities.there are many possibilities.
It must be mentioned that having had It must be mentioned that having had one thrombotic stroke, the patient is one thrombotic stroke, the patient is at risk in the ensuing months and at risk in the ensuing months and years of having a stroke at the same years of having a stroke at the same or another site, especially if there is or another site, especially if there is hypertension or diabetes mellitushypertension or diabetes mellitus

•Normal blood Normal blood flowflow
•ThrombosisThrombosis
•ArteryArtery
•Blood supplyBlood supply•Blood clotBlood clotOxygenOxygen
starvedstarved
brainbrain
tissuetissue

Lacunar infarctLacunar infarct
small penetrating branches of small penetrating branches of the cerebral arteries may become the cerebral arteries may become occluded, and the resulting occluded, and the resulting infarcts may be so small or so infarcts may be so small or so situated as to cause no symptoms situated as to cause no symptoms whatever. As the softened tissue whatever. As the softened tissue is removed, it leaves a small is removed, it leaves a small cavity, or lacune.cavity, or lacune.

Lacunar infarctLacunar infarct In our clinical and pathologic In our clinical and pathologic
material, there has always been a material, there has always been a strong correlation of the lacunar state strong correlation of the lacunar state with a combination of hypertension with a combination of hypertension and atherosclerosis and, to a lesser and atherosclerosis and, to a lesser degree, with diabetes.degree, with diabetes.In all the cases of lacunar infarction, In all the cases of lacunar infarction, the diagnosis depends essentially on the diagnosis depends essentially on the occurrence of the certain unique the occurrence of the certain unique stroke syndromes of limited stroke syndromes of limited proportions. proportions.

Lacunar infarctLacunar infarct
Recognition of lacunar stroke Recognition of lacunar stroke is importantis important
Future lacunar stroke can be Future lacunar stroke can be reduced byreduced by
treatingtreating HTN HTN
Anticoagulation is not Anticoagulation is not indicated ( No evidence)indicated ( No evidence)
Aspirin is also of uncertantyAspirin is also of uncertanty

Lacunar Infarct in pons Lacunar Infarct in pons

Cryptogenic infarctionCryptogenic infarction
Infarct of undetermind cause.Infarct of undetermind cause.

Cerebral hemorrhageCerebral hemorrhage
““Neurologic symptoms from mass Neurologic symptoms from mass effect on neural structures or from effect on neural structures or from toxic effects of blood itself.”toxic effects of blood itself.”

typestypes
IntracranialIntracranial IntracerebralIntracerebral Sub arachnoidSub arachnoid

Intracranial Intracranial HemorrhageHemorrhage
This is the common, well-known This is the common, well-known “spontaneous” brain hemorrhage. It “spontaneous” brain hemorrhage. It is due predominantly to chronic is due predominantly to chronic hypertension and degenerative hypertension and degenerative changes in cerebral changes in cerebral arteries.Hemorrhage may interfere arteries.Hemorrhage may interfere with cerebral function through a with cerebral function through a variety of mechanisms, including variety of mechanisms, including destruction or compression of brain destruction or compression of brain tissue and compression of vascular tissue and compression of vascular structures, leading to secondary structures, leading to secondary ischaemia and edema. ischaemia and edema.

Intracranial hemorrhage is Intracranial hemorrhage is classified by its location as classified by its location as intracerebral, subarachnoid, intracerebral, subarachnoid, subdural, or epidural, all of which- subdural, or epidural, all of which- except subdural hemorrhage- are except subdural hemorrhage- are usually caused by arterial usually caused by arterial bleeding.bleeding.

The bleeding occurs within The bleeding occurs within brain tissue, and rupture of brain tissue, and rupture of arteries lying in the arteries lying in the subarachnoid space is subarachnoid space is practically unknown apart from practically unknown apart from aneurysms. The extravasation aneurysms. The extravasation forms a roughly circular or oval forms a roughly circular or oval mass that disrupts the tissue mass that disrupts the tissue and grows in volume as the and grows in volume as the bleeding continues . Adjacent bleeding continues . Adjacent brain tissue is distorted and brain tissue is distorted and compressed. If the hemorrhage compressed. If the hemorrhage is large, midline structures are is large, midline structures are displaced to the opposite side displaced to the opposite side and reticular activating and and reticular activating and respiratory centers are respiratory centers are compromised, leading to coma compromised, leading to coma and death.and death.


Intraventricular Intraventricular HemorrhageHemorrhage

Intracerebral Intracerebral HemorrhageHemorrhage
Of all the cerebrovascular Of all the cerebrovascular diseases, brain hemorrhage is diseases, brain hemorrhage is the most dramatic.It has been the most dramatic.It has been given its own name, given its own name, “apoplexy”.“apoplexy”.

Clinical PictureClinical Picture
With smaller hemorrhages, the With smaller hemorrhages, the clinical picture conforms more clinical picture conforms more closely to the usual temporal closely to the usual temporal profile of a stroke, i.e, an abrupt profile of a stroke, i.e, an abrupt onset of symptoms that evolve onset of symptoms that evolve gradually and steadily over gradually and steadily over minutes, hours, or a day or two, minutes, hours, or a day or two, depending on the size of the depending on the size of the ruptured artery and the speed of ruptured artery and the speed of bleeding. bleeding.
Headache and vomiting are cardinal Headache and vomiting are cardinal features.Very small hemorrhages in features.Very small hemorrhages in “silent” regions of the brain may “silent” regions of the brain may escape clinical detection.escape clinical detection.

Clinical PictureClinical Picture
Clinical features vary with the site of Clinical features vary with the site of hemorrhage.hemorrhage.
Deep cerebral hemorrhage Deep cerebral hemorrhage The two The two most common sites of hypertensive most common sites of hypertensive hemorrhage are thehemorrhage are the putamen putamen and the and the thalamusthalamus, which are separated by the , which are separated by the posterior limb of the internal posterior limb of the internal capsule. This segment of the capsule. This segment of the internal capsule is traversed by internal capsule is traversed by descending motor fibers and descending motor fibers and ascending sensory fibers, including ascending sensory fibers, including the optic radiations.the optic radiations.

Clinical PictureClinical Picture
Lobar hemorrhage Lobar hemorrhage Hypertensive Hypertensive hemorrhages also occur in hemorrhages also occur in subcortical white matter subcortical white matter underlying the frontal, underlying the frontal, parietal, temporal, and parietal, temporal, and occipital lobes. Symptoms and occipital lobes. Symptoms and signs vary according to the signs vary according to the location.location.

Pontine hemorrhage Pontine hemorrhage With bleeding With bleeding into the pons, coma occurs within into the pons, coma occurs within seconds to minutes and usually seconds to minutes and usually leads to death within 48 hours. leads to death within 48 hours. Ocular findings typically include Ocular findings typically include pinpoint pupils. Horizontal eye pinpoint pupils. Horizontal eye movements are absent or movements are absent or impaired, but vertical eye impaired, but vertical eye movements may be preserved.movements may be preserved.Cerebellar hemorrhage Cerebellar hemorrhage The The distinctive symptoms of cerebellar distinctive symptoms of cerebellar hemorrhage (headache, dizziness, hemorrhage (headache, dizziness, vomiting, and the inability to vomiting, and the inability to stand or walk) begin suddenly, stand or walk) begin suddenly, within minutes after onset of within minutes after onset of bleedingbleeding..

Clinical PictureClinical Picture
Of all strokes, those due to cerebral Of all strokes, those due to cerebral embolism develop most rapidly.embolism develop most rapidly.The embolus strikes at any time of The embolus strikes at any time of the day or night. Getting up to go to the day or night. Getting up to go to the bathroom is a time of danger.the bathroom is a time of danger.The neurologic picture will depend The neurologic picture will depend on the artery involved and the site on the artery involved and the site of obstruction.of obstruction.

Subarachnoid Subarachnoid HemorrhageHemorrhage
This is the fourth most frequent This is the fourth most frequent cerebrovascular disorder following cerebrovascular disorder following atherothrombosis, embolism, and atherothrombosis, embolism, and primary intracerebral hemorrhage. primary intracerebral hemorrhage. Saccular aneurysms are also called Saccular aneurysms are also called berry” aneurysms; actually they berry” aneurysms; actually they take the form of small, thin-walled take the form of small, thin-walled blisters protruding from arteries of blisters protruding from arteries of the circle of Willis or its major the circle of Willis or its major branches. Their rupture causes a branches. Their rupture causes a flooding of the subarachnoid space flooding of the subarachnoid space with blood under high pressure. with blood under high pressure.
Aneurysms are multiple in 20 Aneurysms are multiple in 20 percent of patientspercent of patients

In childhood , rupture of saccular In childhood , rupture of saccular aneurysms is rare, and they are aneurysms is rare, and they are seldom found at routine seldom found at routine postmortem examination; beyond postmortem examination; beyond childhood, they gradually increase childhood, they gradually increase in frequency to reach their peak in frequency to reach their peak incidence between 35 and 65 incidence between 35 and 65 years of age.years of age.proximately 90 to 95 percent of proximately 90 to 95 percent of saccular aneurysms lie on the saccular aneurysms lie on the anterior part of the circle of Willisanterior part of the circle of Willis


WHAT IS A STROKE?WHAT IS A STROKE?

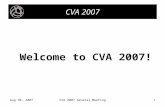
Qureshi, A. I. et al. N Engl J Med 2001;344:1450-1460
Most Common Sites and Sources of Intracerebral Hemorrhage

Subarachnoid Subarachnoid HemorrhageHemorrhage


Stroke in old ageStroke in old age Incidence:2/3 rd of stroke patients are Incidence:2/3 rd of stroke patients are
aged over 60 yrsaged over 60 yrs Diagnosis:a clear history to be neededDiagnosis:a clear history to be needed Thrombolysis:few data avilable.Thrombolysis:few data avilable. Carotid endarterectomy:benefits Carotid endarterectomy:benefits
occur quickly after transiant stroke,it occur quickly after transiant stroke,it indicates age alone is nota contra indicates age alone is nota contra indication.indication.
Cormobiditis:IHD,cardiac Cormobiditis:IHD,cardiac failure,COPD,OA,& visual failure,COPD,OA,& visual impairements.impairements.

Contd.Contd.
Cognitive impairment : adversely Cognitive impairment : adversely affects outcome.affects outcome.
Diffuse small vessel CVD: very Diffuse small vessel CVD: very common & may present insidiously common & may present insidiously with gait abnormalities or with gait abnormalities or significant memory impairment.significant memory impairment.

STROKE IN CHILDREN STROKE IN CHILDREN Stroke in children differs from that of Stroke in children differs from that of
adult by 3 waysadult by 3 ways Predisposing factors:cyanotic heart Predisposing factors:cyanotic heart
disease.disease. Clinical evaluvation:stroke is often Clinical evaluvation:stroke is often
improved due to collateral cir improved due to collateral cir culation.culation.
Anatomical site:perferal bifurcation of Anatomical site:perferal bifurcation of cerebral arteries.adult-circle of williscerebral arteries.adult-circle of willis
Incidence:252/100000 children.Incidence:252/100000 children. Cva complications-6-25%with sickle Cva complications-6-25%with sickle
cell diseasecell disease 67%untreated sickle cell disease.67%untreated sickle cell disease.

General examination of stroke patientsEyes
Diabetic changes Hypertensive changes Retinal emboli Arcus senilis
Cardiovascular system
Blood pressure Heart rhythm Murmurs Jugular venous pressure Peripheral pulses and bruits
Respiratory system
Pulmonary oedema Respiratory infection
Abdomen
Urinary retention

InvestigationsInvestigations Computed Tomographic ScansComputed Tomographic Scans
– Usually demonstrates the lesion, more ever it is very Usually demonstrates the lesion, more ever it is very useful to exclude hemorrhagic lesion.useful to exclude hemorrhagic lesion.
– In ischemic stroke, occasionally CT may be normal in In ischemic stroke, occasionally CT may be normal in first 24 hours.first 24 hours.
– Small posterior fossa or lacunar infarction may be Small posterior fossa or lacunar infarction may be easily missed by CT.easily missed by CT.
Other imaging techniques (MRI, angiography, transcranial Other imaging techniques (MRI, angiography, transcranial doppler) can be applied in selected cases.doppler) can be applied in selected cases.
Carotid doppler Carotid doppler ECG, echocardiogram in suspected Cardiac emboliECG, echocardiogram in suspected Cardiac emboli Assessment of the risk factors for stroke: blood sugar, Assessment of the risk factors for stroke: blood sugar,
serum lipids, polycythemiaserum lipids, polycythemia

Investigation of a patient with an acute stroke
Diagnostic question investigation
Is it a vascular lesion? CT/MRI
Is it ischaemic or haemorrhage? CT Lumbaer puncture
What is the un derlying vascular ECG cardiac ultra sound MRA Doppler ulrasound contrast angiography
What are the risk facctors? Blood count cholesterol clotting/thrombopenia screen blood glucose
Investigation of a patient with an acute strokeDiagnostic question investigationIs it a vascular lesion? CT/MRIIs it ischaemic or haemorrhage? CT Lumbaer punctureWhat is the underlying vascular disease? ECG cardiac ultra sound MRA doppler ultra sound contrast angiography What are the risk facctors? Blood count cholesterol clotting/thrombopenia screen blood glucose

Differential Diagnosis Differential Diagnosis Of CVAOf CVA
Primary cerebral tumoursPrimary cerebral tumours Metastatic cerebral tumoursMetastatic cerebral tumours Subdural heamatomaSubdural heamatoma Cerebral abscessCerebral abscess DemylinationDemylination HypoglycemiaHypoglycemia EncephalitisEncephalitis Hysterical conversionHysterical conversion

ManagementManagement
(1)(1) Supportive measures Supportive measures
(2)(2) Antiplatelet agents Antiplatelet agents
(3)(3) ThrombolysisThrombolysis
(4)(4) Anticoagulation Anticoagulation
(5)(5) Secondary preventionSecondary prevention

Anti-platelet agentsAnti-platelet agentsAspirin 325 mg per dayAspirin 325 mg per dayContraindicated in associated hemorrhageContraindicated in associated hemorrhageActive bleeding lesion (e.g. bleeding peptic Active bleeding lesion (e.g. bleeding peptic ulcer)ulcer)
AnticoagulationAnticoagulationIndicated in cardiac emboli in presence of Indicated in cardiac emboli in presence of atrial fibrillation or thrombus in left ventricleatrial fibrillation or thrombus in left ventricleStart with heparin infusion continue with Start with heparin infusion continue with warfarin .warfarin .Complication : hemorrhagic transformation Complication : hemorrhagic transformation

ThrombolysisThrombolysis– Frequently associated with hemorrhagic Frequently associated with hemorrhagic
transformation of ischemic stroketransformation of ischemic stroke– Still can be tried if patients presents within Still can be tried if patients presents within
6 hours of onset, absence of hypertension, 6 hours of onset, absence of hypertension, when CT does not show excessive low when CT does not show excessive low density, or there are no other obvious density, or there are no other obvious contraindication.contraindication.
– Drugs that can be used are streptokinase Drugs that can be used are streptokinase and Rt-PA.and Rt-PA.
Secondary preventionSecondary prevention– Control of risk factorsControl of risk factors– Antiplatelet agent ( aspirin, ticlopidine, Antiplatelet agent ( aspirin, ticlopidine,
Dipyridamole, clopidogrelDipyridamole, clopidogrel))

conclusionconclusion Thus we have gone through the Thus we have gone through the
basic pathology, clinical features, basic pathology, clinical features, investigations and complications of investigations and complications of cerebro -vascular accidents. cerebro -cerebro -vascular accidents. cerebro -vascular accidents are those occuring vascular accidents are those occuring due to impaired structure and function due to impaired structure and function of various blood vessels suppling the of various blood vessels suppling the brain.even a mild infarct or brain.even a mild infarct or haemorrhage can create wide spread haemorrhage can create wide spread consequnce in the body.they are consequnce in the body.they are medical emergencies.medical emergencies.

Thank YouThank You