
COPD Session 2
89
-
Upload
gamal-agmy -
Category
Health & Medicine
-
view
739 -
download
4
Transcript of COPD Session 2

COPD Session 2
Gamal Rabie Agmy, MD, FCCP Professor of chest Diseases, Assiut university

Diagnosis & Differential Diagnosis 2
Goal of this learning modules
• To Provide a framework to make informed decisions regarding the diagnosis and differential diagnosis of Chronic obstructive pulmonary disease

Learning objectives
After completing this module you should know:
• Know the clinical features of COPD
• Know the basic investigations needed
• Know when should you prompt further investigations
• Differentiate COPD from other similar conditions

Key Indicators for Considering a Diagnosis of COPD
Dyspnea: •Progressive (worsens over time) •Characteristically worse with exercise •Persistent (present every day)
Chronic Cough: •May be intermittent and may be unproductive
Chronic sputum production: • Any pattern of chronic sputum production may indicate COPD
History of exposure to risk factors: •Tobacco smoke. •Occupational dusts and chemicals •Smoke from home cooking and heating fuels
Family history of COPD
Consider COPD: indicators are present in an individual over age 40. Spirometry is required to establish a diagnosis of COPD
The COPD patient Generally over 40 years
A smoker or ex-smoker
Presentation with:
– cough
– excessive sputum production
– shortness of breath
Dyspnea is the reason most patients seek medical attention.
1. BTS, 1997; 3. GOLD, 2003

Dyspnea: its importance in COPD
• One of the most common and distressing symptoms for patients with COPD, and the reason most patients seek medical attention.
• Disabling, limits activity , and reduces quality of life.
• An important outcome variable for clinical and research evaluations.
• Related to, but independent of lung function.
*Mahler D, Harver A. Am Rev Respir Dis (1992)

“ The Downward Spiral ” Airflow
limitation
Inactivity
Isolation
Dyspnea
Muscle Impairment
Hyper Inflation
Severe Dyspnea
Deconditioning
Weight Loss
Depression
Poor Quality of Life
Mortality
Hypoxia

The causes of dyspnea are complex
• Hyperinflation at rest or with exertion (Dynamic).
• Increased ventilation demand.
• Weak respiratory muscles.
All will lead to limitation of activity in COPD .

Causes of Chronic Cough with a Normal Chest X-ray
Intrathoracic • Chronic obstructive pulmonary disease • Bronchial asthma • Central bronchial carcinoma • Endobronchial tuberculosis • Bronchiectasis • Left heart failure • Interstitial lung disease • Cystic fibrosis
Extrathoracic • Postnasal drip • Gastroesophageal reflux • Drug therapy (e.g., ACE inhibitors)
Medical History • Patient’s exposure to risk factors
• Past medical history (asthma, allergy, sinusitis or nasal polyps; respiratory infections in childhood; other respiratory diseases)
• Family history of COPD or other chronic respiratory disease
• Pattern of symptom development: COPD typically develops in adult life and most patients are conscious of increased breathlessness, more frequent “winter colds,” and some social restriction for a number of years before seeking medical help.
• History of exacerbations or previous hospitalizations
• Presence of comorbidities
• Impact of disease on patient’s life
• Social and family support
• Possibilities for reducing risk factors

Clinical features Chronic bronchitis
• Mild dyspnea
• Cough before dyspnea starts
• Copious, purulent sputum
• More frequent infections
• Repeated resp. insufficiency
• PaCO2 50-60 mmHg
• PaO2 45-60 mmHg
• Hematocrit 50-60% • DLCO is not that much ↓ • Corpulmonale common
Emphysema • Severe dyspnea
• Cough after dyspnea
• Scant sputum
• Less frequent infections
• Terminal RF
• PaCO2 35-40 mmHg
• PaO2 65-75 mmHg
• Hematocrit 35-45%
• DLCO is decreased
• Corpulmonale rare.
BLUE BLOTTER PINK PUFFER
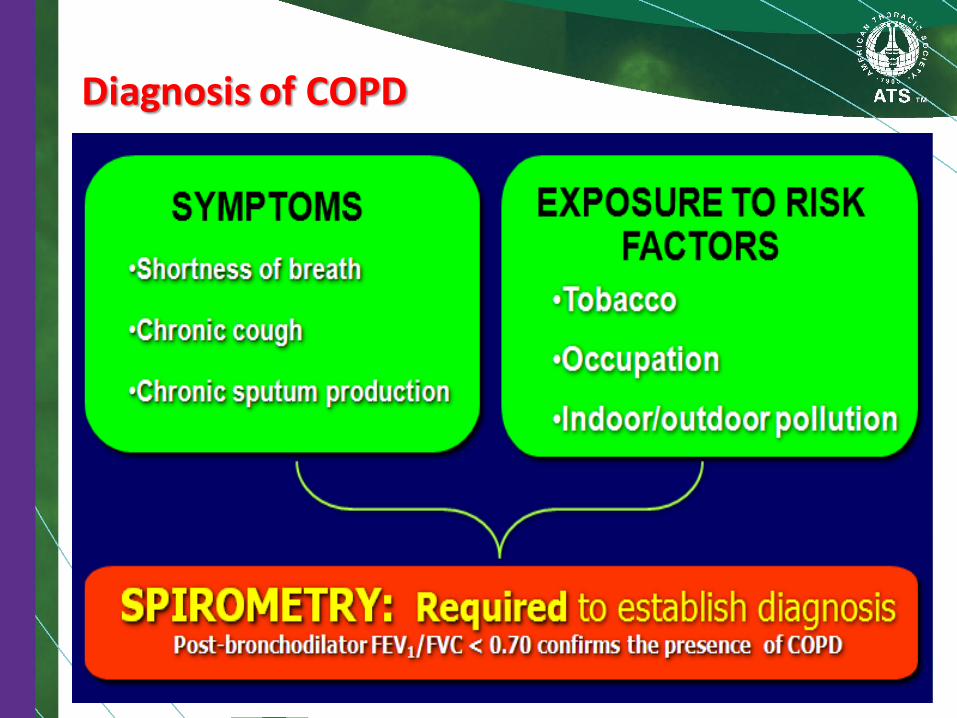
Diagnosis of COPD

Why Do We Need Spirometry?
• Spirometry is useful for:
– Screen individuals at risk for pulmonary disease
– Confirmation of COPD diagnosis
– Assessing severity of pulmonary dysfunction
– Guiding selection of treatment
– Assessing the effects of therapeutic interventions
Spirometry
A post-bronchodilator FEV1/FVC < 0.70 confirms the presence of airflow limitation.
Where possible, values should be compared to age-related normal values to avoid overdiagnosis of COPD in the elderly.
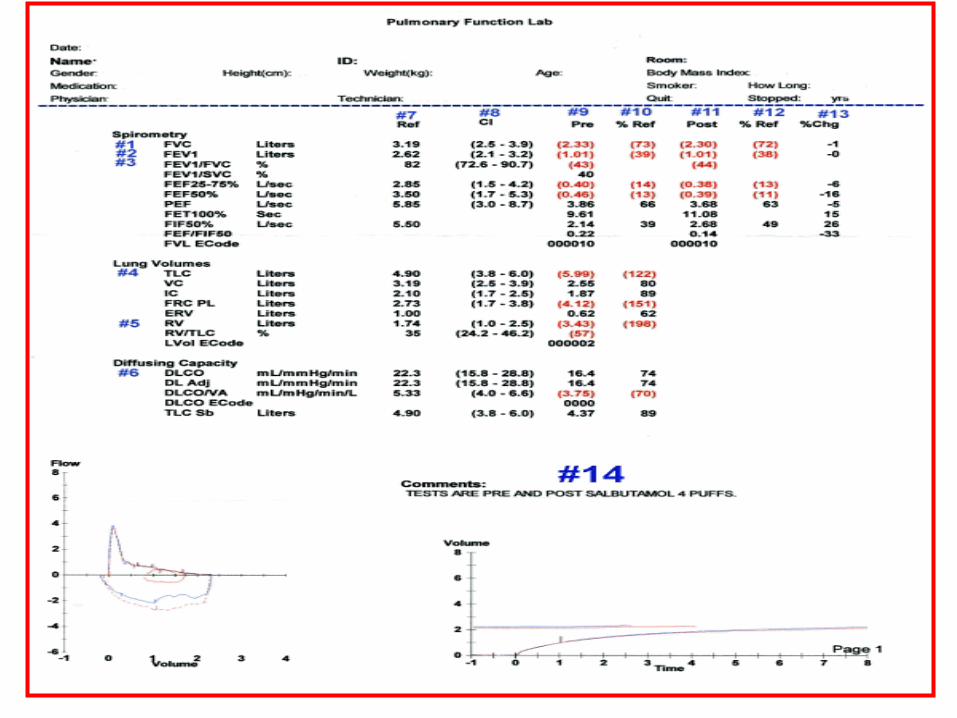
Spirometry should be performed after the administration of an adequate dose of a short-acting inhaled bronchodilator (e.g. 400 µg Salbutamol) to minimize variability.

Acceptability & Repeatability

Acceptability
At least three (3) acceptable maneuvers:
• Good start to the test.
• No hesitation or coughing for the 1st second.
• FVC lasts at least 6 seconds with a plateau
of at least 1 second.
• No valsalva maneuver or obstruction of the
mouthpiece.
• FIVC shows apparent maximal effort.

Repeatability
Repeatability criteria act as guideline to
determine need for additional efforts.
– Largest and 2nd largest FVC must be within 150
mL.
– Largest and 2nd largest FEV 1 must be 150 mL.
– PEF values may be variable (within 15%).
If three acceptable reproducible maneuvers
are not recorded, up to 8 attempts may be
recorded.
Spirometry Value
• Spirometry is typically reported in both
absolute values and as a predicted
percentage of normal.
• Normal values vary and are dependent on:
– Gender,
– Race,
– Age,
– Weight and
– Height.
Reporting Standards
• Largest FVC obtained from all acceptable
efforts should be reported.
• Largest FEV1 obtained from all acceptable
trials should be reported.
• May or may not come from largest FVC
effort.
• All other flows, should come from the effort
with the largest sum of FEV 1 & FVC.
• PEF should be the largest value obtained
from at least 3 acceptable maneuvers.
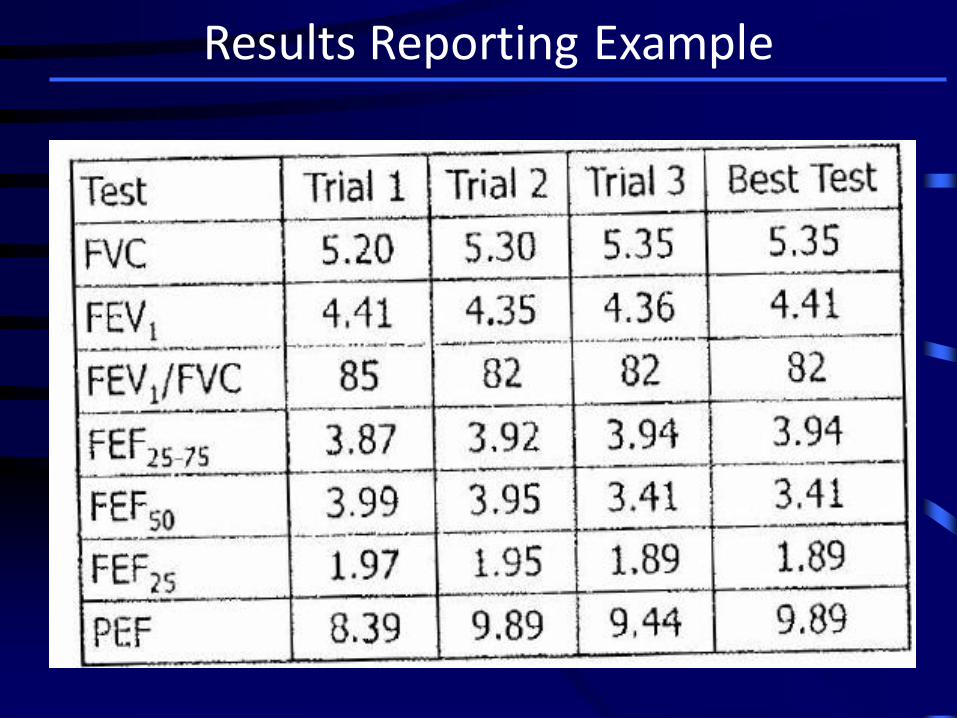
Results Reporting Example
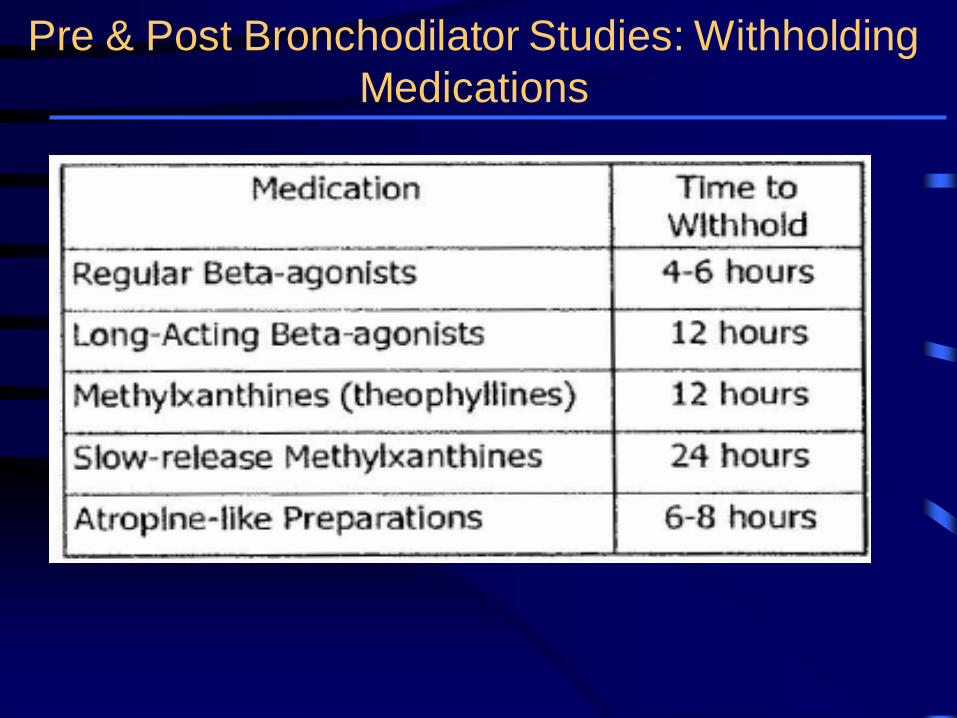
Pre & Post Bronchodilator Studies: Withholding
Medications

Reversibility
Reversibility of airways obstruction can be
assessed with the use of bronchodilators.
• > 12% increase in the FEV1 and 200
ml improvement in FEV1
OR
• > 12% increase in the FVC and 200
ml improvement in FVC.


1-First Step, Check quality of the test
1- Start:
*Good start: Extrapolated volume (EV) < 5% of FVC or 0.15 L
*Poor start: Extrapolated volume (EV) ≥5% of FVC or ≥ 0.15 L
2- Termination:
*No early termination :Tex ≥ 6 s
*Early termination : Tex < 6 s
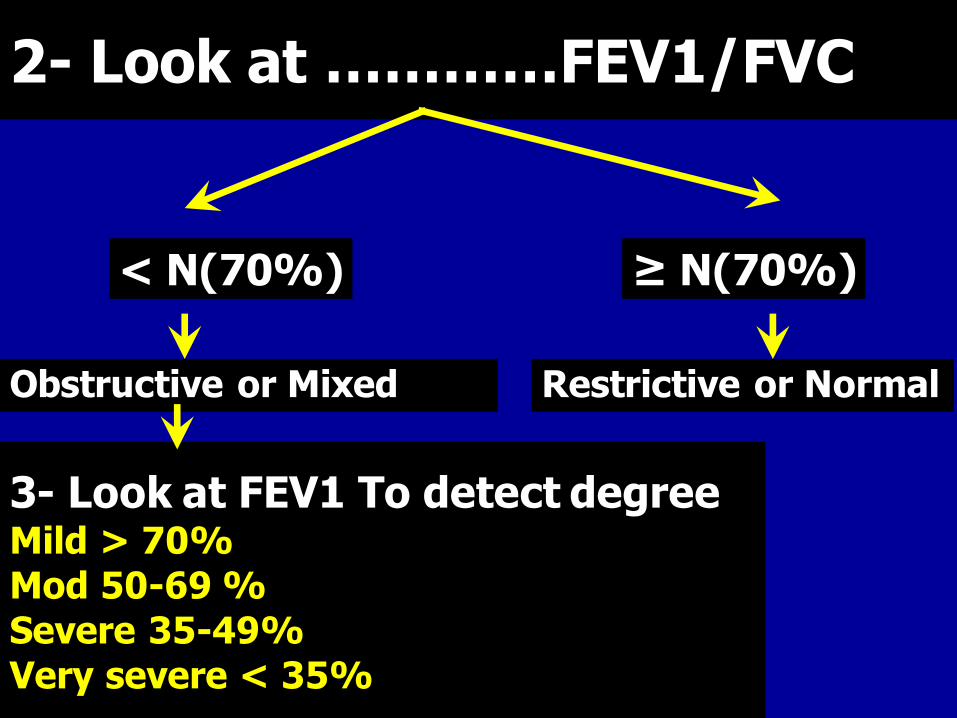
2- Look at …………FEV1/FVC
< N(70%)
Obstructive or Mixed
≥ N(70%)
Restrictive or Normal
3- Look at FEV1 To detect degree Mild > 70% Mod 50-69 %
Severe 35-49%
Very severe < 35%

4- Postbronchodilator FEV1/FVC
> 70%
asthma
< 70%
COPD

5- Reversibility test of FEV1
> 12%, 200 ml
Reversible (asthma)
< 12% ,200 ml
Ireversible (COPD)
6- Look at TLC
≥ 80-120% Pure
obstruction
< 80% Mixed
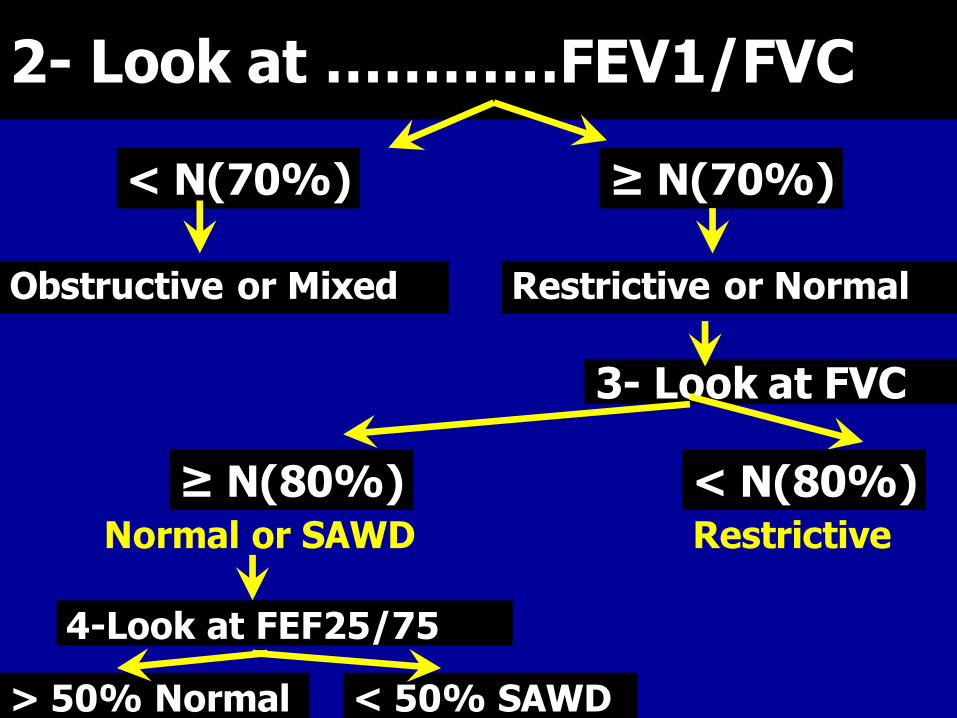
2- Look at …………FEV1/FVC
< N(70%)
Obstructive or Mixed
≥ N(70%)
Restrictive or Normal
3- Look at FVC
≥ N(80%) < N(80%) Normal or SAWD
4-Look at FEF25/75
> 50% Normal < 50% SAWD
Restrictive
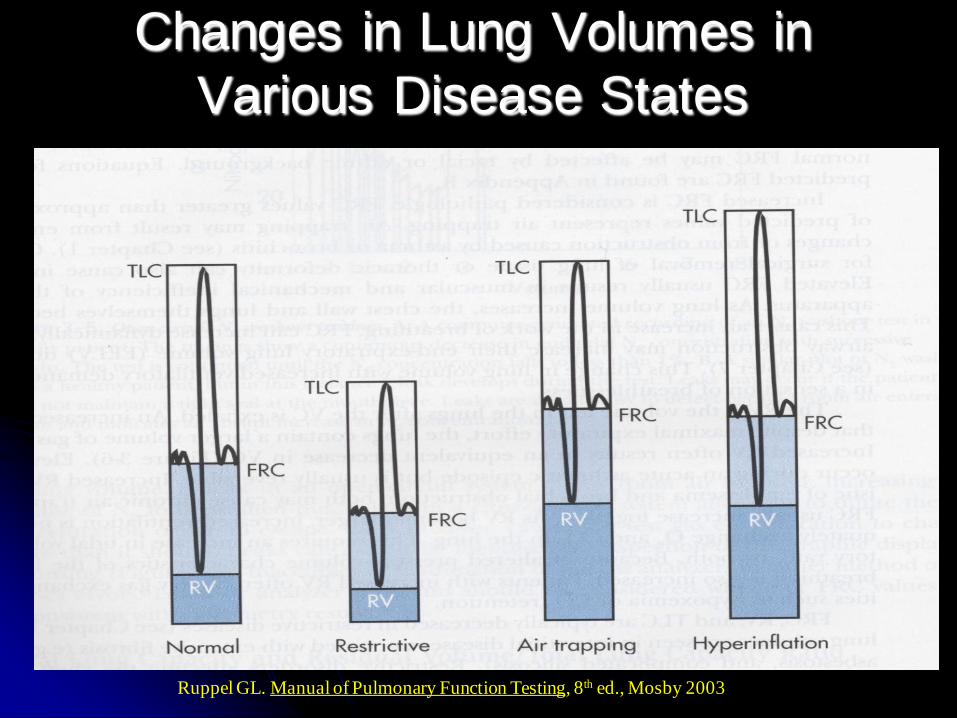
Changes in Lung Volumes in
Various Disease States
Ruppel GL. Manual of Pulmonary Function Testing, 8th ed., Mosby 2003

Patterns of Abnormality
Restriction low FEV1 & FVC, high FEV1%FVC
Recorded Predicted SR %Pred
FEV 1 1.49 2.52 -2.0 59
FVC 1.97 3.32 -2.2 59
FEV 1 %FVC 76 74 0.3 103
PEF 8.42 7.19 1.0 117
Obstructive low FEV1 relative to FVC, low PEF, low FEV1%FVC
Recorded Predicted SR %Pred
FEV 1 0.56 3.25 -5.3 17
FVC 1.65 4.04 -3.9 41
FEV 1 %FVC 34 78 -6.1 44
PEF 2.5 8.28 -4.8 30
high PEF early ILD
low PEF late ILD

Patterns of Abnormality
Upper Airway Obstruction low PEF relative to FEV1
Recorded Predicted SR %Pred
FEV 1 2.17 2.27 -0.3 96
FVC 2.68 2.70 0.0 99
FEV 1 %FVC 81 76 0.7 106
PEF 2.95 5.99 -3.4 49
FEV 1 /PEF 12.3
Discordant PEF and FEV1
High PEF versus FEV1 = early interstitial lung disease (ILD)
Low PEF versus FEV1 = upper airway obstruction
Concordant PEF and FEV1
Both low in airflow obstruction, myopathy, late ILD

Common FVL Shapes
Volume
Flo
w
Normal Young or quitter Poor effort
Hesitation Knee Coughing
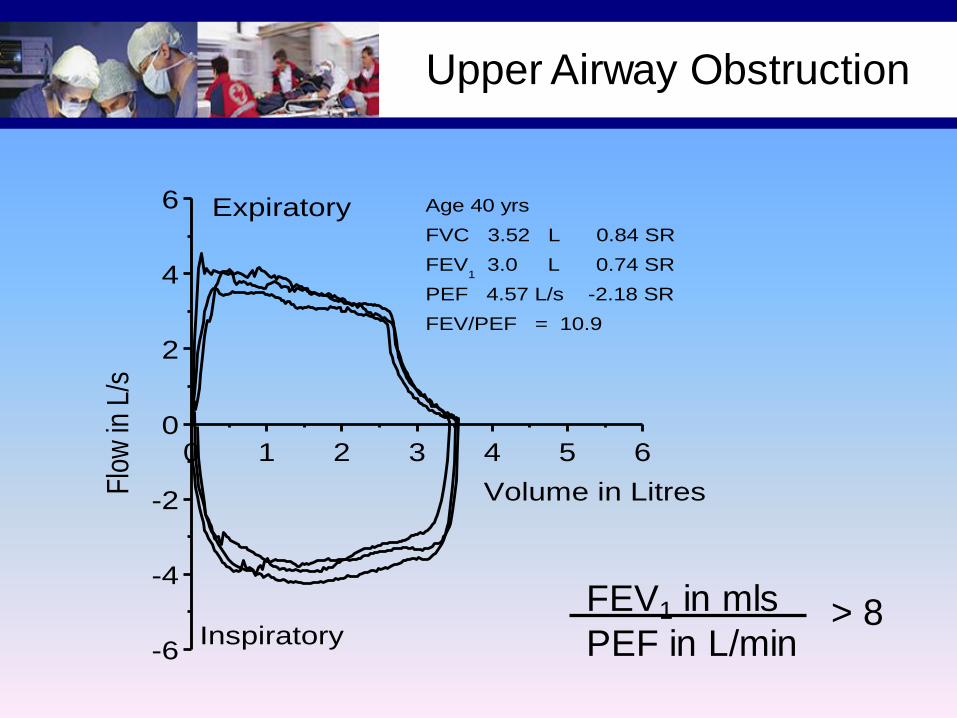
Upper Airway Obstruction
0 1 2 3 4 5 6
-6
-4
-2
0
2
4
6 Age 40 yrs
FVC 3.52 L 0.84 SR
FEV1 3.0 L 0.74 SR
PEF 4.57 L/s -2.18 SR
FEV/PEF = 10.9
Inspiratory
Expiratory
Flo
w in
L/s
Volume in Litres
FEV1 in mls
PEF in L/min > 8

Diffusing Capacity
Diffusing capacity of lungs for CO
Measures ability of lungs to transport inhaled gas
from alveoli to pulmonary capillaries
Depends on:
- alveolar—capillary membrane
- hemoglobin concentration
- cardiac output
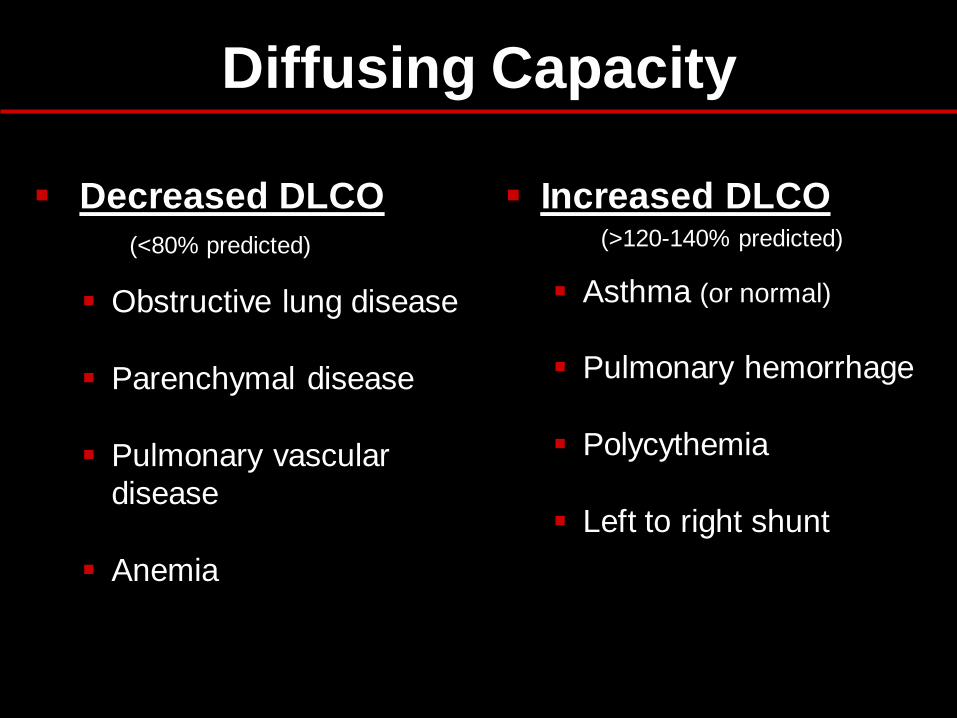
Diffusing Capacity
Decreased DLCO
(<80% predicted)
Obstructive lung disease
Parenchymal disease
Pulmonary vascular
disease
Anemia
Increased DLCO (>120-140% predicted)
Asthma (or normal)
Pulmonary hemorrhage
Polycythemia
Left to right shunt

DLCO — Indications
Differentiate asthma from emphysema
Evaluation and severity of restrictive lung disease
Early stages of pulmonary hypertension
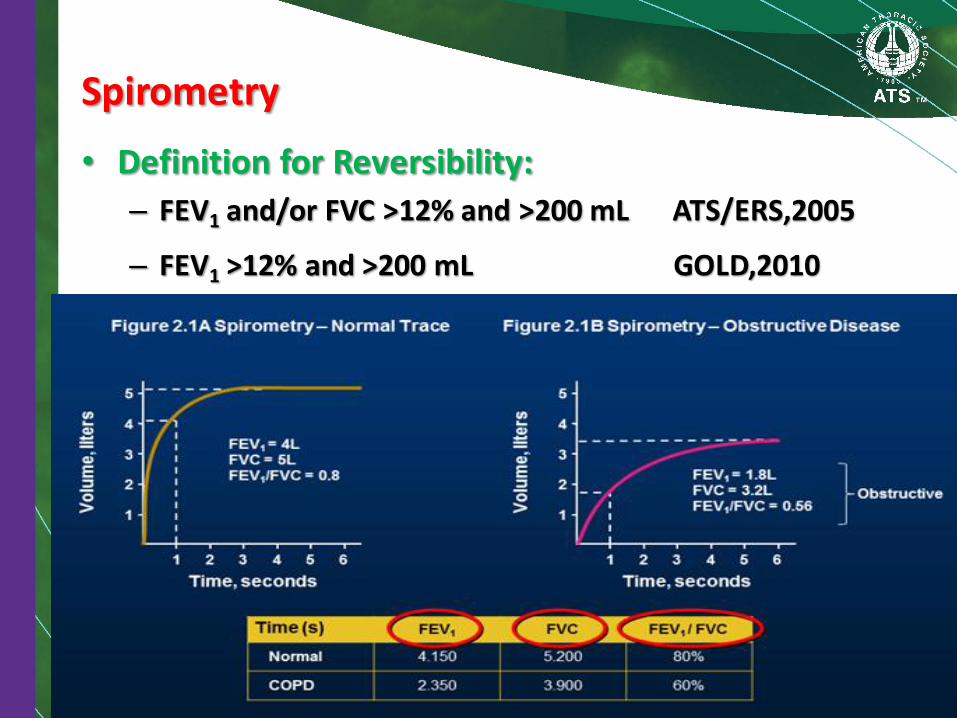
Spirometry
• Definition for Reversibility:
– FEV1 and/or FVC >12% and >200 mL ATS/ERS,2005
– FEV1 >12% and >200 mL GOLD,2010


Additional Optional Investigations
• Imaging
• Arterial blood gas measurement
• Alpha-1 antitrypsin deficiency screening
• Lung volumes & diffusing capacity
• Sleep study
• Exercise testing
• Composite scores

Chest X-ray

Chest X-ray

CT findings in emphysema
• Relatively well-defined, low attenuation areas with very thin (invisible) walls, surrounded by normal lung parenchyma.
• As disease progresses:
– Amount of intervening normal lung decreases.
– Number and size of the pulmonary vessels decrease.
– +/- Abnormal vessel branching angles (>90o), with vessel bowing around the bullae.
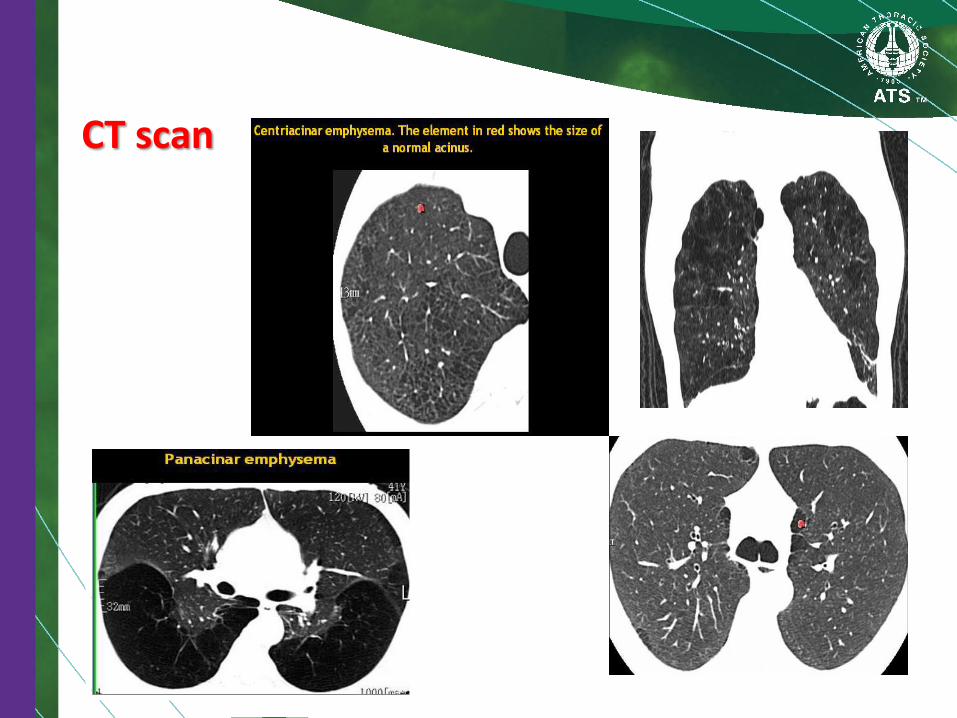
CT scan
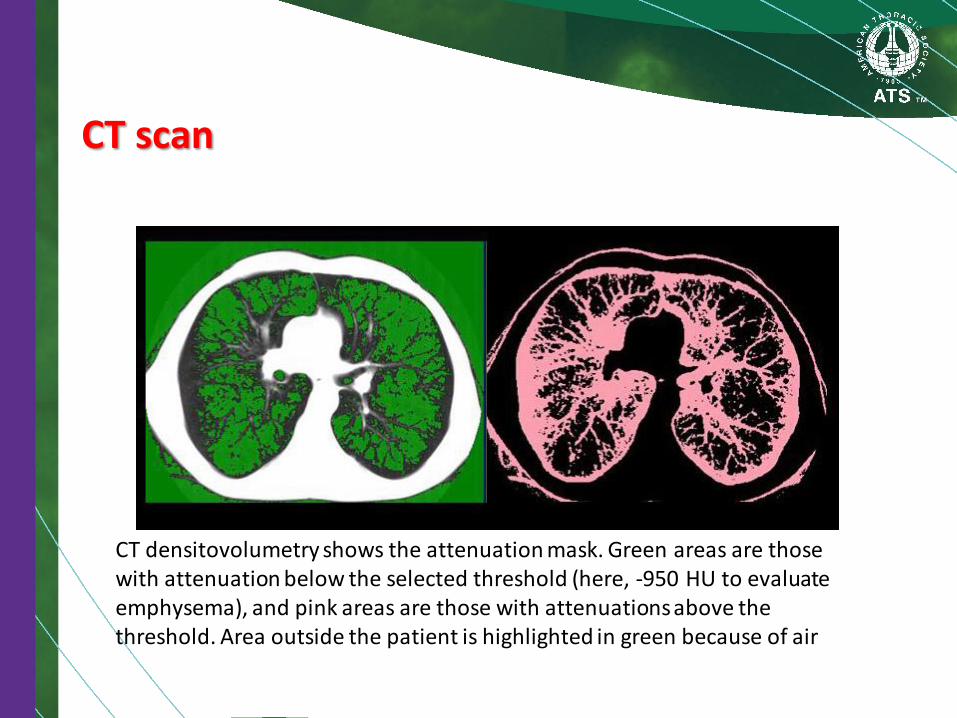
CT scan
CT densitovolumetry shows the attenuation mask. Green areas are those with attenuation below the selected threshold (here, -950 HU to evaluate emphysema), and pink areas are those with attenuations above the threshold. Area outside the patient is highlighted in green because of air

Quantitative CT:
• Spirometically triggered images at 10% and
90% vital capacity (VC) have been reported
to be able to distinguish patients with chronic
bronchitis from those with emphysema.
– Patients with emphysema had significantly lower
mean lung attenuation at 90% VC than normal
subjects or patients with chronic bronchitis.
– Attenuation was the same for normal subjects and
those with chronic bronchitis.


Where is the pathology ???????
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping

Pathology in black areas
Airtrapping: Airway Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic, connective tissue diseases, drug reaction,
after transplantation, after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
COPD/Asthma / Bronchiectasis / Airway diseases
Airway Disease
what you see……
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration ‘black’ areas remain in volume and density ‘white’ areas decrease in volume and increase in density INCREASE IN CONTRAST DIFFERENCES AIRTRAPPING
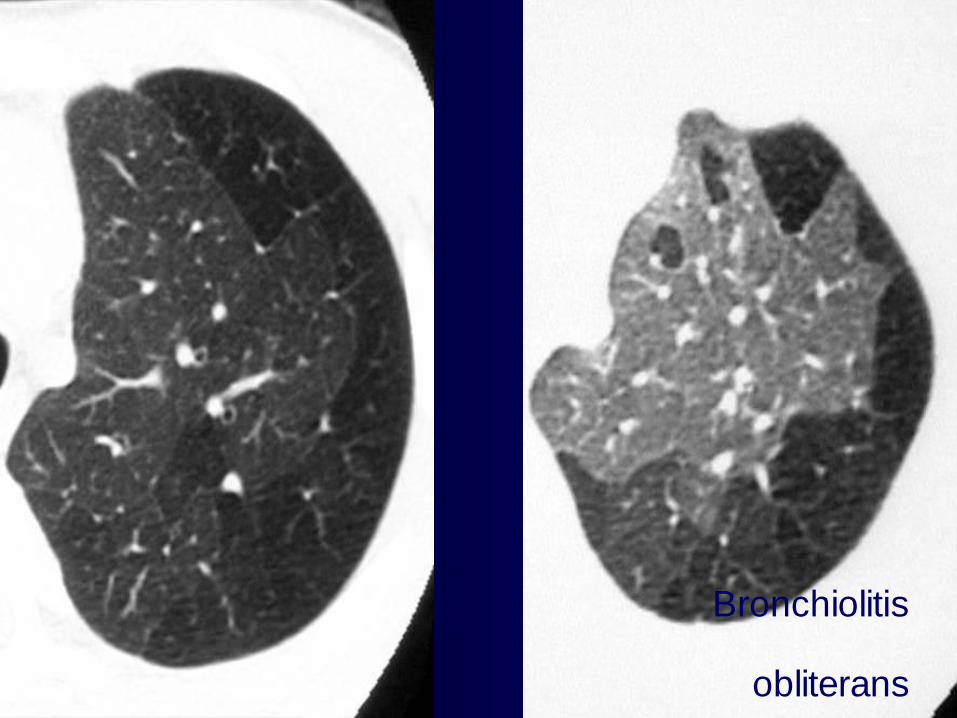
Bronchiolitis
obliterans

Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall, producing a punched-out appearance.
Often the centrilobular artery is visible within the
centre of these lucencies.
55
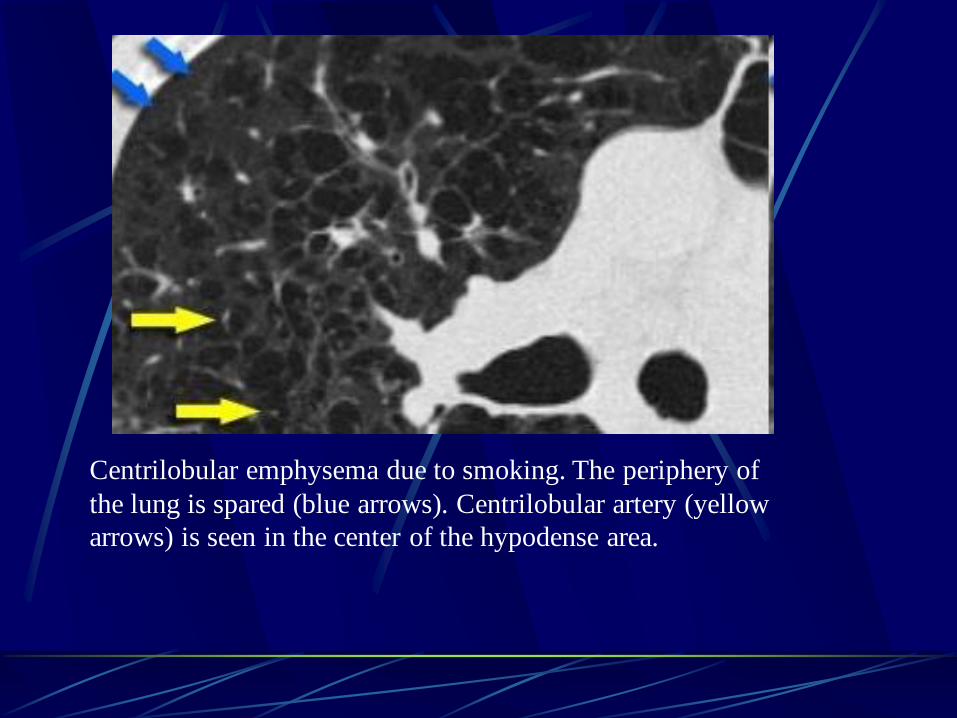
Centrilobular emphysema due to smoking. The periphery of
the lung is spared (blue arrows). Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area.
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency, but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule.
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
58
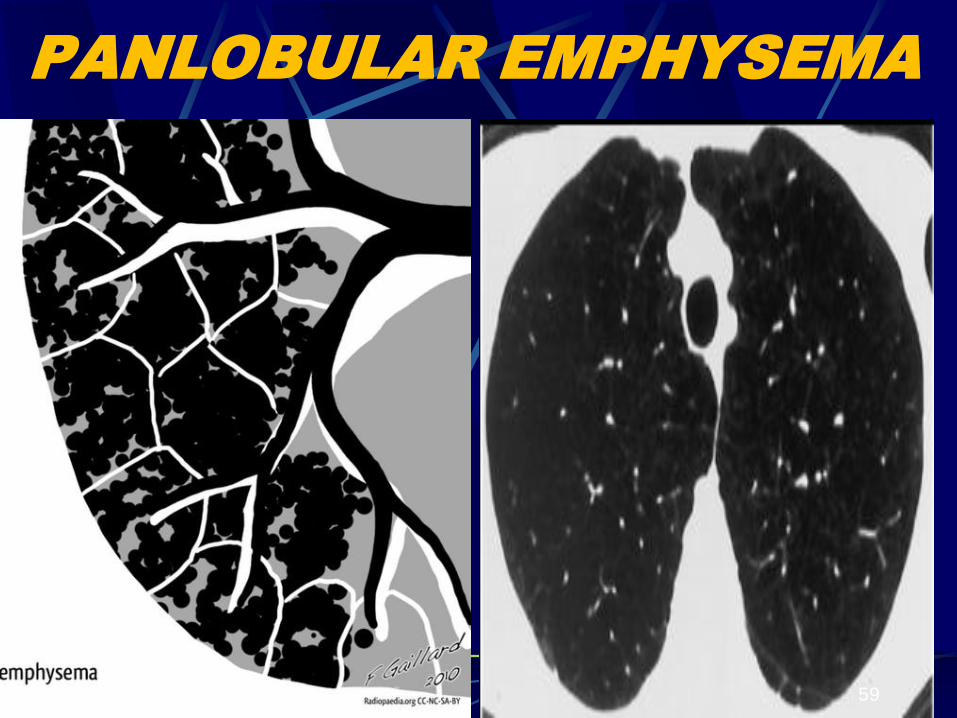
PANLOBULAR EMPHYSEMA
59
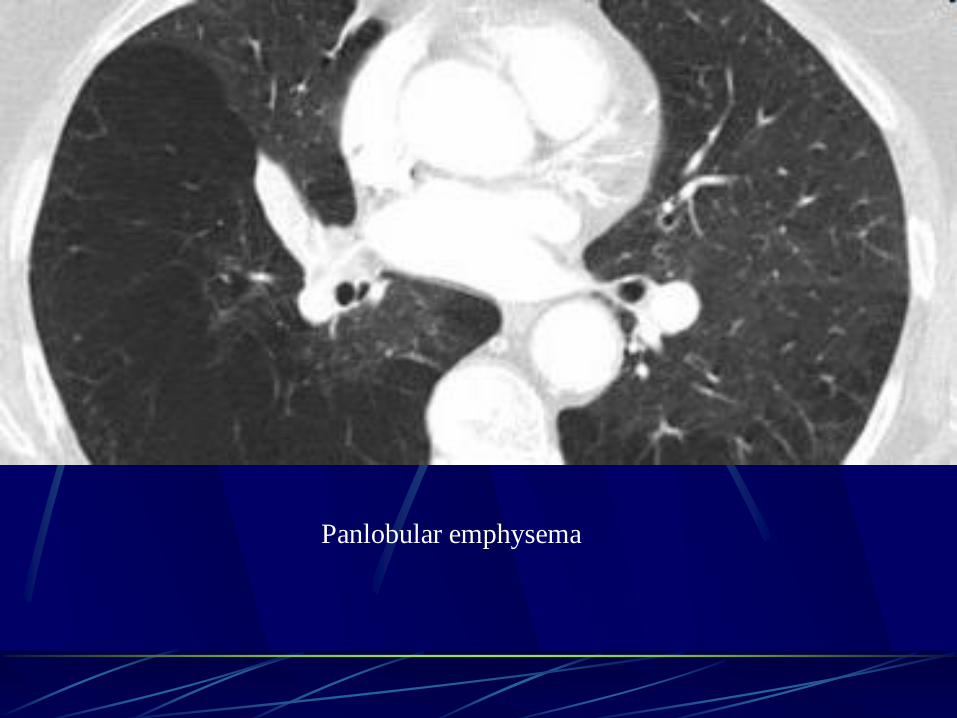
Panlobular emphysema
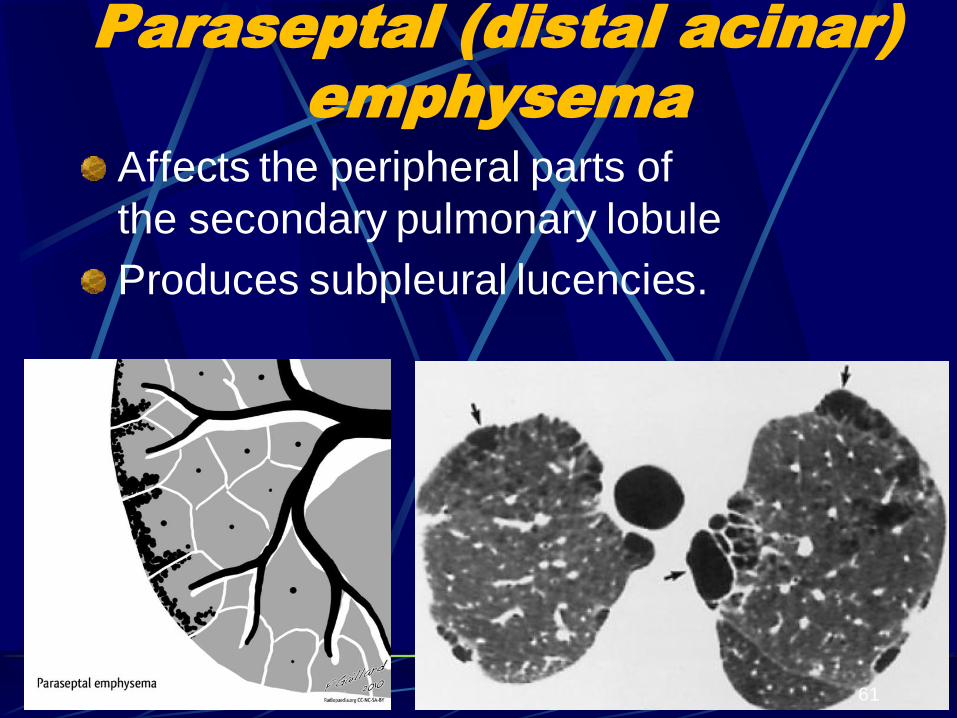
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies.
61

Paraseptal emphysema

Alpha-1 antitrypsin deficiency screening
• Caucasian descent who develop COPD at a young age (< 45 years) lower lobe emphysema or who have a strong family history of the disease
• A serum concentration of alpha-1 antitrypsin below 15-20% of the normal value is highly suggestive of homozygous alpha-1 antitrypsin deficiency.
• 11 mmol/L (80 mg/mL) represents the threshold level below which emphysema is common
• Only 2% of COPD is alpha 1- AT deficiency

ALPHA1 ANTITRYPSIN ↓ EMPHYSEMA
Specific circumstances of Alpha 1- AT↓include.
• Emphysema in a young individual (< 35)
• Without obvious risk factors (smoking etc)
• Necrotizing panniculitis, Systemic vasculitis
• Anti-neutrophil cytoplasmic antibody (ANCA)
• Cirrhosis of liver, Hepatocellular carcinoma
• Bronchiectasis of undetermined etiology
• Otherwise unexplained liver disease, or a
• Family history of any one of these conditions
• Especially siblings of PI*ZZ individuals.
• Only 2% of COPD is alpha 1- AT ↓
Arterial blood gas (ABG) measurement Indicated: • Stable patients with FEV1 < 35%
predicted • Clinical signs suggestive of respiratory
failure or right heart failure.
Considerations:. • The inspired oxygen concentration (FiO2) –
should be noted
• Especially when using an O2-driven nebulizer. ??
• Changes in ABG take time to occur→ 30 minutes should pass before rechecking the gas tensions
• Adequate pressure must be applied at the arterial puncture site for at least one minute
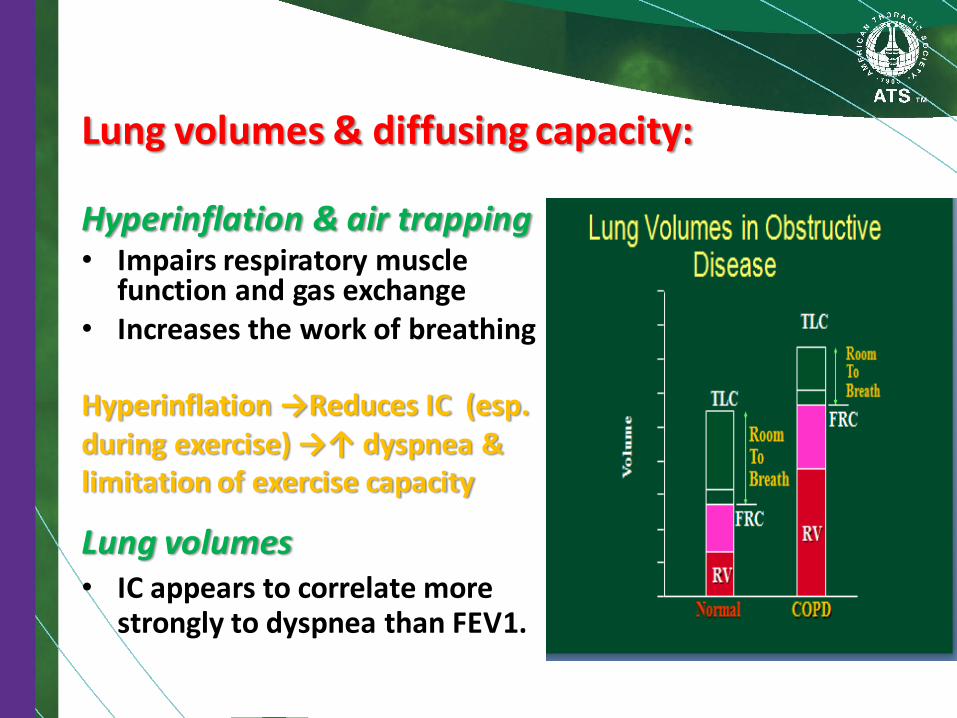
Lung volumes & diffusing capacity: Hyperinflation & air trapping • Impairs respiratory muscle
function and gas exchange • Increases the work of breathing Hyperinflation →Reduces IC (esp. during exercise) →↑ dyspnea & limitation of exercise capacity
Lung volumes • IC appears to correlate more
strongly to dyspnea than FEV1.

Lung volumes & diffusing capacity:
Effect of exercise on Hyperinflation

Hyperinflation & air trapping
• Explains why airway medications are effective in
COPD
Proc Am Thorac Soc Vol 2. pp 267–271, 2005
Lung volumes & diffusing capacity:
Lung volumes & diffusing capacity:
• Measurement of diffusing capacity (DLco) → provides information on functional impact of emphysema in COPD & it is helpful in breathlessness out of proportion with the degree of airflow limitation.

Sleep study
• Symptoms related to sleep disturbances are common in moderate to severe COPD, particularly in elderly patients.
• COPD+ obstructive sleep apnea (OSA) (overlap syndrome) occurs in 1% of adults and overlap patients have worse nocturnal hypoxemia and hypercapnia than COPD and OSA patients alone.
May be indicated when:
• Hypoxemia or right heart failure develops in the presence of relatively mild airflow limitation or when the patient has symptoms suggesting the presence of sleep apnea.

Exercise testing
• To measure exercise capacity, e.g., treadmill and cycle ergometry in the laboratory – or six-minute and shuttle walking tests.
• Powerful indicator of health status impairment and predictor of prognosis.
• Assess disability & effectiveness of pulmonary rehabilitation
• Primarily used in conjunction with pulmonary rehabilitation programs.

Composite scores
The cutoff values for the assignment of points are shown for each variable. The total possible values range from 0 to 10, with higher scores indicating a greater risk of death.
Approximate 4 Year Survival Interpretation
0-2 Points: 80%
3-4 Points: 67 %
5-6 Points: 57%
7-10 Points: 18%
Differential Diagnosis of COPD
Asthma
Congestive heart failure
Bronchiectasis
Tuberculosis
Obliterative bonchiolitis
Diffuse Panbronchiolitis
Differential Diagnosis of COPD
Asthma – Similarities with COPD
• Major epidemiologic causes of chronic obstructive airway disease
• Involve underlying airway inflammation
• Can cause similar chronic respiratory symptoms and fixed airflow limitation
• Can co-exist with the other making diagnosis more difficult
Differential Diagnosis of COPD
Asthma – Differences from COPD • Underlying immune mechanism of chronic
inflammation different – Eosinophilic and CD4-driven in asthma & neutrophilic
and CD8-driven in COPD • Age of onset
– Earlier in life with asthma – Usually > age 40 in COPD
• Symptoms in asthma vary; COPD slowly progressive • Smoking associated with COPD • Asthma with reversible airflow limitation; irreversible
airflow limitation in COPD
Differential Diagnosis of COPD
• Asthma-COPD Overlap Syndrome (ACOS) is characterized by persistent airflow limitation with several features usually associated with asthma and several features usually associated with COPD. ACOS is therefore identified in the features that it shares with both asthma and COPD.
Asthma COPD
ACOS

Differential Diagnosis of COPD
Clinical Feature COPD Asthma
Age Older than 35 years Any age
Cough Persistent, productive Intermittent, usually
nonproductive
Smoking Typical Variable
Dyspnea Progressive, persistent Variable
Nocturnal symptoms Breathlessness, late in
disease Coughing, wheezing
Family history Less common More common
Atopy Less common More common
Significant diurnal or day to day variability
Less common More common
Spirometry Irreversible airway
limitation Reversible airway
limitation
Differential Diagnosis of COPD
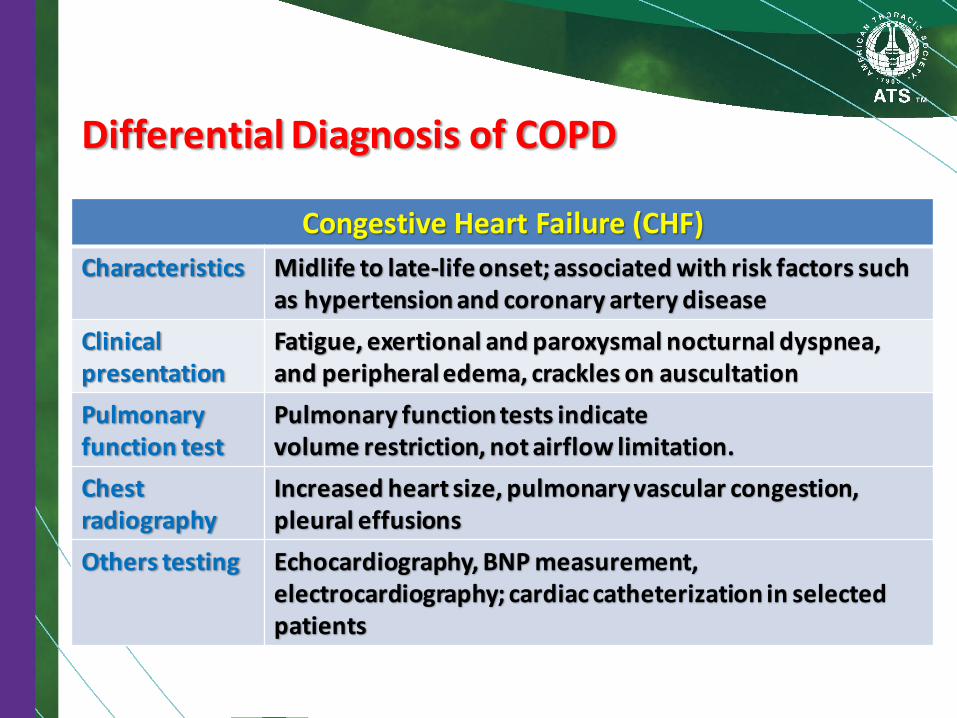
Congestive Heart Failure (CHF)
Characteristics Midlife to late-life onset; associated with risk factors such as hypertension and coronary artery disease
Clinical presentation
Fatigue, exertional and paroxysmal nocturnal dyspnea, and peripheral edema, crackles on auscultation
Pulmonary function test
Pulmonary function tests indicate volume restriction, not airflow limitation.
Chest radiography
Increased heart size, pulmonary vascular congestion, pleural effusions
Others testing Echocardiography, BNP measurement, electrocardiography; cardiac catheterization in selected patients

Differential Diagnosis of COPD
Bronchiectasis
Characteristics Usually midlife onset; progressive with exacerbations
Clinical presentation
Productive cough with large volumes of thick, purulent sputum; ±related to posture , ±bad odor dyspnea; and wheezing associated with bacterial infections, crackles, and clubbing on exam
Pulmonary function test
Obstructive airflow limitation, both fixed and reversible
Chest radiography Focal pneumonia, atelectasis; dilated bronchial tree, thickened airways (ring shadow)
Other testing Bacterial, & microbacterial sputum culture, high resolution chest CT.

Differential Diagnosis of COPD
Tuberculosis
Characteristics Onset at any age; associated with history of exposure, High local prevalence of tuberculosis may suggest diagnosis
Clinical presentation Productive cough, hemoptysis, fever, and weight loss
Pulmonary function test
Not used for diagnosis
Chest radiography Infiltrate, nodular lesions, hilar adenopathy, cavitary lesions or granulomas
Other testing Sputum AFB culture, sputum cultures

Differential Diagnosis of COPD
Obliterative bonchiolitis
Characteristics
Onset at any age but often younger; may be associated with history of flu-like illness, collagen vascular disease, or toxic fume exposure, non-smokers
Clinical presentation
Often subacute presentation with dyspnea, cough, and fever
Pulmonary function test
Decreased vital capacity, decreased DLCO, usually no obstructive component
Chest radiography Multifocal, bilateral alveolar infiltrates
Other testing High-resolution CT shows hypodense areas on expiration, lung biopsy
Differential Diagnosis of COPD
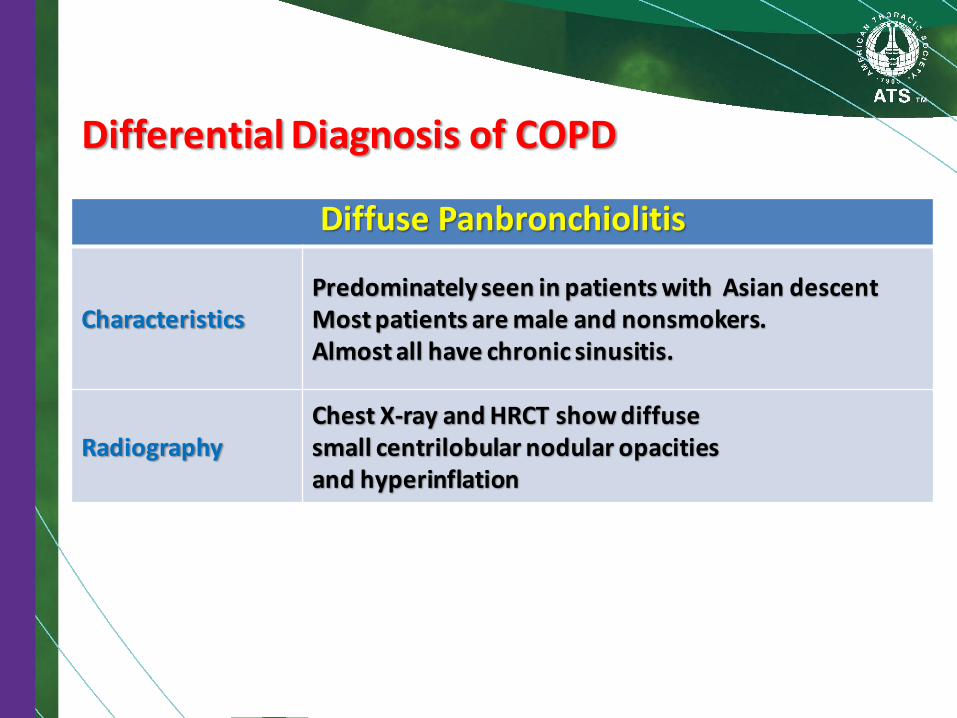
Diffuse Panbronchiolitis
Characteristics Predominately seen in patients with Asian descent Most patients are male and nonsmokers. Almost all have chronic sinusitis.
Radiography Chest X-ray and HRCT show diffuse small centrilobular nodular opacities and hyperinflation
83
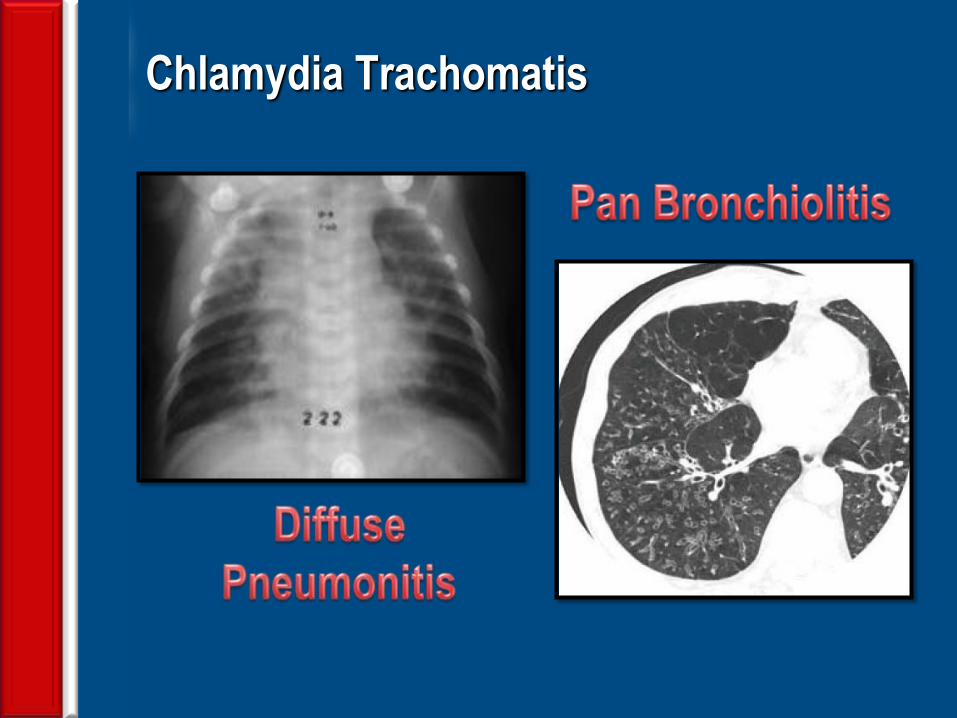
Chlamydia Trachomatis
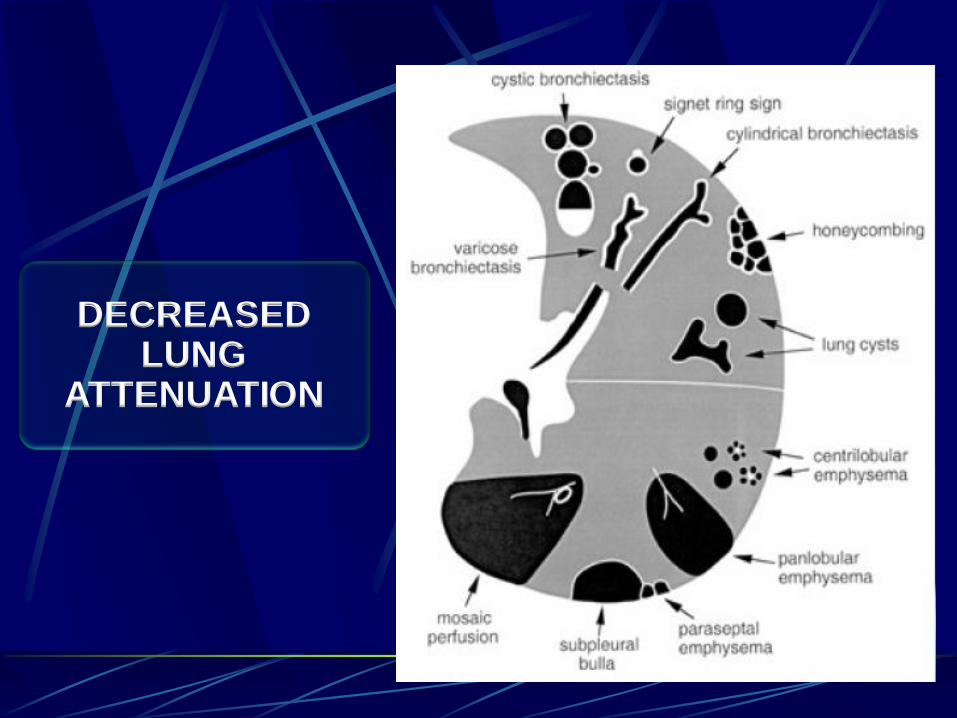
DECREASED LUNG
ATTENUATION

ABPA: glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma.

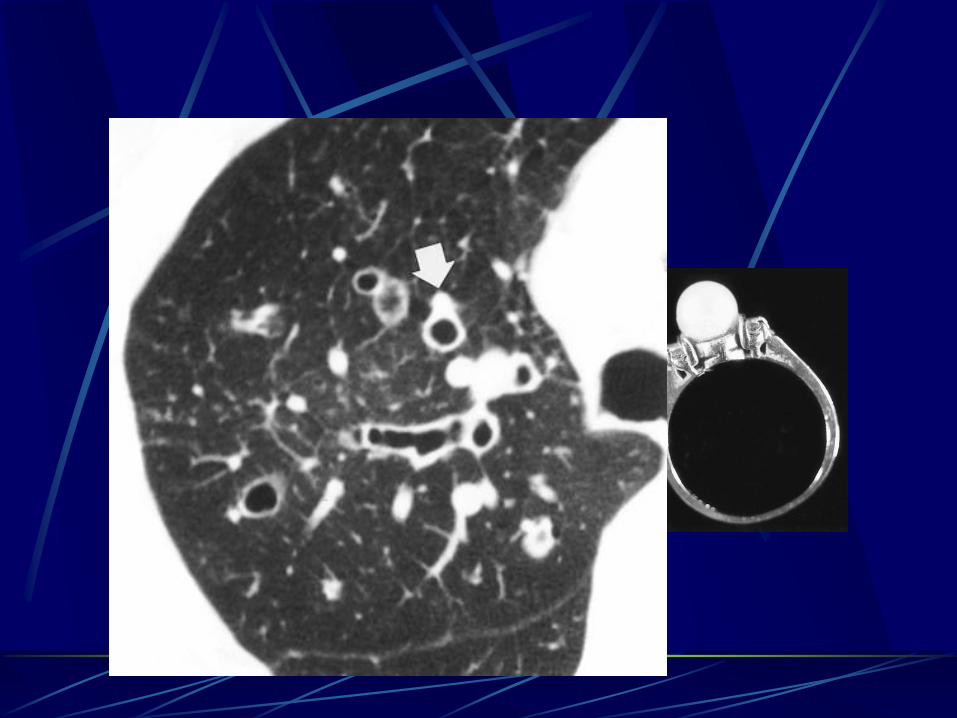
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet).
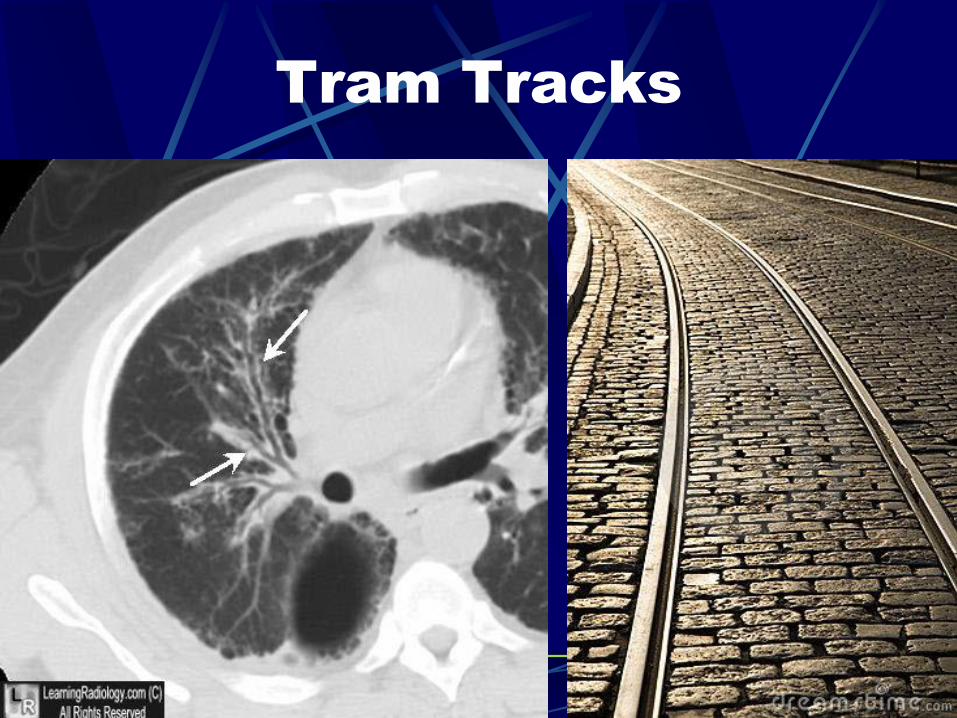
Tram Tracks

Thank you


















