
COPD Bone Metabolism and Osteoporosis
10
648 CHEST Recent Advances in Chest Medicine Recent Advances in Chest Medicine C OPD is a major cause of chronic morbidity and mortality worldwide. The Global Initiative for Chronic Obstructive Lung Disease (GOLD) has defined COPD as a preventable and treatable disease that is primarily characterized by progressive airflow limitation. This airflow limitation is not fully revers- ible and is associated with an abnormal inflammatory response of the lung to noxious particles or gases, most often cigarette smoke. 1 COPD is often associ- ated with different comorbidities and systemic conse- quences, which further impair functional status, reduce quality of life, and increase mortality. 2 Of these, osteo- porosis is increasingly being appreciated as an impor- tant target for therapeutic intervention. Osteoporosis is a systemic skeletal disorder that is characterized by compromised bone strength due to an impaired bone quality, leading to increased frac- ture risk. Bone strength depends on the structural and material properties of bone, both of which are influ- enced by the rate of bone turnover. Not all determi- nants of bone strength are well represented by a bone mineral density (BMD) measurement, but BMD pro- vides a very useful estimate of fracture risk. 3 BMD is measured accurately by dual-energy x-ray absorp- tiometry (DXA) and is used to define osteoporosis. DXA measures BMD by dividing bone mineral con- tent by bone area. The T score is calculated by sub- tracting the mean BMD of a young-adult reference population from the patient’s BMD and dividing by the SD of the reference population. Z scores are used to compare the patient’s BMD to a popula- tion of peers. According to the World Health Orga- nization, a T score . 2 1 is accepted as normal, and T scores between 2 1 and 2 2.5 are considered to be osteopenia, whereas T scores of , 2 2.5 are defined as osteoporosis, at least in postmenopausal wome n. 4 Ost eoporosi s-related fractures are divided COPD and osteoporosis are strongly associated because of common risk factors such as age, smoking, and inactivity. In addition, COPD-related syst emic inflammation, vitamin D deficiency , and the use of systemic corticosteroids enhance ongoing bone destruction. Osteoporosis, in turn, may cause fragility fractures, which further impair mobility and increase morbidity and mortality. Vertebral compression fractures and rib cage f ractures in patients with COPD may also reduce pulmonary function or enhance exacerbations. Early prevention and treatment of osteoporosis in COPD is, therefore, important and should be based on integrated risk assessment tools such as FRAX, which take bone mineral density, history of fragility fractures, and population-specific clinical factors into account. As long as intervention studies focusing on the bone in CO PD are lacking, a more rigorous application of existing treatment guidelines of osteoporosis in general is mandatory. CHEST 2011; 139(3):648–657 Abbre viations: 1,25(OH) 2 D 5 1,25 dihydroxyvitamin D; 25-OHD 5 25 hydroxyvitamin D; BMD 5bone mineral density; DXA 5 dual-energy x-ray absorptiometry; GCS 5 glucocorticosteroid; GOLD 5 Global Initiative for Chronic Obstruc- tive Lung Disease; ICS 5 inhaled corticosteroid; OPG 5 osteoprotegerin; PTH 5 parathyroid hormone; RANK 5 receptor activator of nuclear factor- kB; RANKL 5 receptor activator of nuclear factor- kB ligand COPD, Bone Metabolism, and Osteoporosis An Lehouck , MSc ; Steven Boonen , MD , PhD ; Marc Decramer , MD , PhD ; and Wim Janssens , MD, PhD Manuscript received June 18, 2010; revision accepted September 3, 2010. Affil iatio ns: From the Respiratory Division (Ms Lehouck and Drs Decramer and Janssens) and the Center of Metabolic Bone Diseases (Dr Boonen), University Hospital Gasthuisberg, Katholieke Universiteit Leuven, Leuven, Belgium. Funding/Support: This study was supported by the Funds for Scientific Research-Flanders [Grant 059809N] and the Institute for Promotion of Innovation Through Science and Technology- Flanders [Grant 335102]. Correspondence to: Wim Janssens, MD, PhD, Respiratory Divi- sion, University Hospital Gasthuisberg, KUL, Herestraat 49, 3000 Leuven, Belgium; e-mail: [email protected] .be © 2011 American College of Chest Physicians. Reproduction of this article is prohibited without written permission from the American College of Chest Physicians (http://www.chestpubs.org/ site/misc/reprints.xhtml ). DOI: 10.1378/chest.10-1427 Downloaded From: http://journal.pu blications.ches tnet.org/ on 06/25/201 5
-
Upload
ari-kuncoro -
Category
Documents
-
view
219 -
download
0
Transcript of COPD Bone Metabolism and Osteoporosis

8/21/2019 COPD Bone Metabolism and Osteoporosis
http://slidepdf.com/reader/full/copd-bone-metabolism-and-osteoporosis 1/10
648
CHEST Recent Advances in Chest Medicine
Recent Advances in Chest Medicine
COPD is a major cause of chronic morbidity andmortality worldwide. The Global Initiative for
Chronic Obstructive Lung Disease (GOLD) hasdefined COPD as a preventable and treatable diseasethat is primarily characterized by progressive airflowlimitation. This airflow limitation is not fully revers-ible and is associated with an abnormal inflammatoryresponse of the lung to noxious particles or gases,most often cigarette smoke.1 COPD is often associ-ated with different comorbidities and systemic conse-quences, which further impair functional status, reduce
quality of life, and increase mortality.2 Of these, osteo-porosis is increasingly being appreciated as an impor-
tant target for therapeutic intervention.Osteoporosis is a systemic skeletal disorder that is
characterized by compromised bone strength due toan impaired bone quality, leading to increased frac-ture risk. Bone strength depends on the structural andmaterial properties of bone, both of which are influ-enced by the rate of bone turnover. Not all determi-nants of bone strength are well represented by a bonemineral density (BMD) measurement, but BMD pro-
vides a very useful estimate of fracture risk.3 BMD ismeasured accurately by dual-energy x-ray absorp-tiometry (DXA) and is used to define osteoporosis.
DXA measures BMD by dividing bone mineral con-tent by bone area. The T score is calculated by sub-tracting the mean BMD of a young-adult referencepopulation from the patient’s BMD and dividingby the SD of the reference population. Z scores areused to compare the patient’s BMD to a popula-tion of peers. According to the World Health Orga-nization, a T score . 2 1 is accepted as normal, andT scores between 2 1 and 2 2.5 are considered tobe osteopenia, whereas T scores of , 2 2.5 aredefined as osteoporosis, at least in postmenopausal
women.4 Osteoporosis-related fractures are divided
COPD and osteoporosis are strongly associated because of common risk factors such as age,smoking, and inactivity. In addition, COPD-related systemic inflammation, vitamin D deficiency,and the use of systemic corticosteroids enhance ongoing bone destruction. Osteoporosis, in turn,may cause fragility fractures, which further impair mobility and increase morbidity and mortality.
Vertebral compression fractures and rib cage fractures in patients with COPD may also reducepulmonary function or enhance exacerbations. Early prevention and treatment of osteoporosis inCOPD is, therefore, important and should be based on integrated risk assessment tools such as FRAX,
which take bone mineral density, history of fragility fractures, and population-specific clinical
factors into account. As long as intervention studies focusing on the bone in COPD are lacking, amore rigorous application of existing treatment guidelines of osteoporosis in general is mandatory.CHEST 2011; 139(3):648–657
Abbreviations: 1,25(OH)2 D51,25 dihydroxyvitamin D; 25-OHD525 hydroxyvitamin D; BMD5bone mineral density;DXA5dual-energy x-ray absorptiometry; GCS5glucocorticosteroid; GOLD5Global Initiative for Chronic Obstruc-tive Lung Disease; ICS5 inhaled corticosteroid; OPG5osteoprotegerin; PTH5parathyroid hormone; RANK5receptoractivator of nuclear factor-kB; RANKL5 receptor activator of nuclear factor-kB ligand
COPD, Bone Metabolism, and Osteoporosis
An Lehouck , MSc ; Steven Boonen , MD , PhD ; Marc Decramer , MD , PhD ;and Wim Janssens , MD, PhD
Manuscript received June 18, 2010; revision accepted September3, 2010.
Affil iations: From the Respiratory Division (Ms Lehouck andDrs Decramer and Janssens) and the Center of Metabolic BoneDiseases (Dr Boonen), University Hospital Gasthuisberg, KatholiekeUniversiteit Leuven, Leuven, Belgium.Funding/Support: This study was supported by the Funds forScientific Research-Flanders [Grant 059809N] and the Institutefor Promotion of Innovation Through Science and Technology-Flanders [Grant 335102].Correspondence to: Wim Janssens, MD, PhD, Respiratory Divi-sion, University Hospital Gasthuisberg, KUL, Herestraat 49,3000 Leuven, Belgium; e-mail: [email protected]© 2011 American College of Chest Physicians. Reproductionof this article is prohibited without written permission from theAmerican College of Chest Physicians (http://www.chestpubs.org/ site/misc/reprints.xhtml).DOI: 10.1378/chest.10-1427
wnloaded From: http://journal.publications.chestnet.org/ on 06/25/2015

8/21/2019 COPD Bone Metabolism and Osteoporosis
http://slidepdf.com/reader/full/copd-bone-metabolism-and-osteoporosis 2/10
www.chestpubs.org CHEST / 139 / 3 / MARCH, 2011 649
sion fractures in COPD, which may vary from 24%to 63%, depending on the population studied.17-20
Vertebral compression fractures should be of majorconcern in COPD, even when remaining asymptom-atic. Different studies have shown that, besides backpain, they can result in significant performanceimpairments and decline of pulmonary function.21,22 Moreover, a previous fracture is a well-known risk fac-
tor for new vertebral and nonvertebral fractures, indi-cating that their diagnosis is important. In fact, within1 year after sustaining a vertebral compression fracture,the rate of new vertebral fractures is close to 20%.23
Prevalence of Hip Fractures in COPD
Although hip fractures are generally considered to bethe most dramatic complication of osteoporosis in termsof morbidity, mortality, and economic cost,24 theirexact prevalence in patients with COPD has not beenstudied in detail. Walsh et al25 reported an increased
prevalence of hip fractures in a population of patients with miscellaneous lung diseases, 52% of whom werepatients with COPD, when compared with age-matchedcontrol subjects. More recently, the OsteoporosisFractures in Men (MrOS) research group demon-strated that a reported history of COPD or asthma
was associated with a lower BMD at the spine and hip,even when adjusting for confounders such as corticos-teroid use, age, hospital site, BMI, and smoking.26
Pathogenesis of Osteoporosis in COPD
Bone is generally classified into two types. Corticalbone is a dense and strong bone found primarily inthe shaft of long bones. Trabecular bone is moreporous or weak and typically occurs at the ends of longbones and within the interior of vertebrae and flatbones. Bone tissue is continuously renewed through-out life and it is estimated that in adults, approxi-mately 25% of trabecular bone and 3% of cortical boneis replaced every year. After reaching peak bone mass atthe age of 25 to 30 years, remodeling is associated
with an imbalance between formation and resorption,resulting in a mean annual bone loss of 0.5% to 1%,
which differs by sex, skeletal site, and age. Key deter-minants of the rate of bone remodeling and bone lossare parathyroid hormone (PTH), vitamin D, and sexhormones.27-29 At the cellular level, bone remodelingis a complex interplay in which osteoblasts, osteo-clasts, and osteocytes work together ( Fig 1). Basically,osteoclasts resorb bone and osteoblasts replace boneby forming an osteoid protein matrix that subsequentlymineralizes, whereas osteocytes and their canicularnetwork serve as sensors to adjust bone responseto mechanical stimuli. On their surface, osteoblastsconstitutively express the receptor activator of nuclear
into vertebral fractures (predominantly at the tho-racolumbar spine) and nonvertebral or peripheralfractures, including hip fractures. Hip bone density isslightly more predictive of hip fracture risk than BMDmeasured at the spine; for other fracture types, DXAmeasurements at the spine and hip have similar pre-dictive value. In this regard, hip bone density is pre-ferred for estimating fracture risk, whereas for treat-
ment monitoring, spine bone density is often selectedbecause the trabecular bone of the spine is more rap-idly affected by treatment. Measures of bone turn-over, on the other hand, like C-terminal cross-linkedtelopeptide of type 1 collagen, or bone alkaline phos-phatase, are less predictive of fracture risk, at leastin the individual. As a result, such markers are notused routinely in clinical practice to identify patientsat risk. However, in osteoporotic patients receivingtreatment, biochemical markers are more sensitivethan BMD to therapeutic interventions, allowing earlyfeedback and, potentially, enhanced compliance.5
Because of pain and decreased mobility, osteoporo-tic fractures frequently cause significant morbidity inolder individuals. At this stage in life, hip fracturesand other types of nonvertebral fractures are associ-ated with increased mortality, functional decline, lossof quality of life, and need for institutionalization.6 Indisabled patients with COPD who are more at risk ofosteoporosis, the impact of such events may be even
worse. Furthermore, vertebral compression fracturesmay also lead to increased kyphosis and reduced ribcage mobility, leading to a further deterioration of pul-monary function.7 Finally, fragility fractures of the rib
may cause hypoventilation and reduce sputum evacu-ation, which may lead to, or aggravate, exacerbations.8 Hence, more attention should be attributed to the inti-mate relationship between COPD and osteoporosis.
Prevalence of Osteoporosis
and Fractures in COPD
Prevalence of Osteoporosis in COPD
The prevalence of osteoporosis in COPD variesbetween 4% and 59%, depending on the diagnosticmethods used, the population studied, and the sever-ity of the underlying respiratory disease.9 Table 1 sum-marizes the most important studies. Overall, a higherprevalence of osteoporosis is generally found in patients
with COPD when compared with healthy controlsubjects. In addition, the majority of studies reportan increased risk of osteoporosis with lower FEV1 .10-16
Prevalence of Vertebral CompressionFractures in COPD
Several studies, summarized in Table 1, have exploredby radiograph the prevalence of vertebral compres-
wnloaded From: http://journal.publications.chestnet.org/ on 06/25/2015

8/21/2019 COPD Bone Metabolism and Osteoporosis
http://slidepdf.com/reader/full/copd-bone-metabolism-and-osteoporosis 3/10
650 Recent Advances in Chest Medicine
Table 1 — Prevalence of Osteoporosis and Vertebral Compression Fractures in COPD
Study Patient Group Subjects BMD Measurements
Prevalence ofOsteoporosis,
% RX diagnosis of VCFPrevalence of
VCF, %
OsteoporosisGraat-Verboom et al10 COPD patients
(GOLD I-IV) referredfor PR
554 Whole-body BMD(DXA)
21 … …
Ferguson et al11
COPD patients(GOLD II-IV) 658 BMD LS and hip(DXA) 24 … …
Sin et al12 COPD patients(GOLD I-IV)
5215 BMD total femur(DXA)
4-33 … …
Forli et al13 COPD patients awaitingLTX
40 BMD LS and FN(DXA)
59 … …
Iqbal et al14 Patients with chroniclung disease
130 BMD LS and hip(DXA)
36 … …
Sabit et al15 COPD patients(GOLD I-IV)
75 BMD LS and hip(DXA)
24 … …
Bolton et al16 Respiratory outpatientsreferred for PR
81 BMD total body, LS,and hip (DXA)
32 … …
Compression fractures Jorgensen et al17 Ambulatory COPD
outpatients(GOLD III-IV)
62 … … Thoracic and lumbar spineradiographs
24
Nuti et al18 Ambulatory COPDoutpatients(GOLD I-IV)
2981 … … Lateral chest radiograph 41
Papaioannou et al19 COPD patients(GOLD not reported)
127 … … Lateral chest radiograph 27
McEvoy et al20 Male COPD patients(GOLD not reported)
312 … … Lateral lumbar and thoracicradiograph
49-63
BMD5bone mineral density; DXA5dual-energy x-ray absorptiometry; FN5 femoral neck; GOLD5Global Initiative for Chronic ObstructiveLung Disease; LS5 lumbar spine; LTX5 lung transplant; PR5pulmonary rehabilitation; RX5radiograph; VCF5 vertebral compression fractures.
factor- k B ligand (RANKL). When binding to its recep-tor (receptor activator of nuclear factor- k B [RANK])on the surface of preosteoclast cells, the latter differ-entiate into mature and activated osteoclasts. Addi-tionally, osteoblasts but also stromal cells secrete asoluble decoy receptor, osteoprotegerin (OPG), whichblocks the RANK/RANKL interaction, thereby actingas a physiologic regulator of bone turnover.30 Imbal-ance between RANKL and OPG results in excessiveactivity of osteoclasts and is considered a major causeof osteoporosis.31 Another pathway that is less wellunderstood is the Wnt/b -catenin signaling cascadedownstream of a number of osteoblast-activating pro-teins and receptors. Wnt signaling activates osteo-blasts and bone formation, whereas reduced Wntsignaling may lead to osteoporosis.32 Several factorsthat have often been described in COPD patients(ie, systemic inflammation, use of corticosteroids,and vitamin D deficiency) clearly interact with thesepathways and are discussed in the following sections.
Systemic Inflammation
Systemic inflammation is thought to play an impor-tant role in the development of osteoporosis inCOPD.33 Key inflammatory cytokines such as tumor
necrosis factor a and IL-6 are known to induceexpression of RANKL and RANKL-mediated boneresorption.34 In addition, many other cytokines havebeen found to interact with the OPG/RANKL sys-tem, supporting the concept that inflammatory medi-ators contribute to the regulation of bone remodeling.35 In line with this concept, recent data from the arthri-tis field demonstrate that inflammation can also trig-ger the Wnt/b -catenin pathway.36
Use of Corticosteroids
Several in vitro and in vivo studies have demon-strated profound effects of glucocorticosteroids (GCSs)
on bone turnover by different mechanisms. GCSspreferentially affect trabecular bone because ofits higher metabolic activity, but with prolongeduse, cortical bone is also affected.37 Briefly, GCSsrapidly increase the expression of RANKL and mac-rophage colony-stimulating factor, while decreasingthe expression of OPG. Along with reduced apop-tosis of mature osteoclasts, enhanced and prolongedresorption occurs, which gradually slows down duringcontinued use of GCSs because of the inhibition ofosteoclast precursors.38 In a second phase, inhibitionof proliferation, differentiation, and maturation of
wnloaded From: http://journal.publications.chestnet.org/ on 06/25/2015

8/21/2019 COPD Bone Metabolism and Osteoporosis
http://slidepdf.com/reader/full/copd-bone-metabolism-and-osteoporosis 4/10
www.chestpubs.org CHEST / 139 / 3 / MARCH, 2011 651
tion. A recent systematic review examined risk factorsfor low BMD and bone loss in healthy men aged50 years or older.43 In addition to a history of fragilityfractures and advancing age, consistent evidence wasfound for smoking, low body weight or weight loss,and physical or functional limitations. Inconsistentto poor evidence was available for physical activity,alcohol use, and muscle strength. Overall, these clini-cal determinants of fracture risk in men were in line
with those previously reported in women.44 Becausemany of these risk factors coincide with COPD, espe-cially at the more severe stages, it should be no sur-prise that osteoporosis and COPD are strongly linked(Fig 2). A recent literature survey by Graat-Verboomand colleagues9 confirmed that a number of risk fac-tors for osteoporosis in general can be identifiedin COPD patients, including low body mass, diseaseseverity, use of corticosteroids, age, and femalegender. Of particular interest might be the presenceof emphysema, which is associated with lower BMIand reduced BMD, and which may represent a clinicalphenotype at high risk of osteoporosis.45,46 However,the exact role of most factors and the extent to whichthey independently contribute to the risk of osteopo-rosis in COPD remain to be determined, preferablyin large-scale longitudinal studies. Three differentfactors deserve further attention because they maybe amendable for intervention: the optimization of
vitamin D status, the limitation of corticosteroid use,and the substitution of sex steroids.
Vitamin D Deficiency
Vitamin D plays a crucial role in bone homeo-stasis. A significant positive association between
osteoblasts leads to long-lasting impairment ofbone formation.39 In this process, inhibition of the
Wnt/b -catenin pathway is likely to be involved.40 GCSsalso exert negative effects on osteocytes, resulting ina modification of their microenvironment that mayalter their mechanosensor function and render thebone more susceptible to fragility fractures.
Vitamin D Deficiency
Vitamin D plays a key role in the regulation of cal-
cium and bone homeostasis.41 Low levels of vitamin Dstimulate the parathyroid glands to increase secretionof PTH to compensate for the low bioavailability ofcalcium. More importantly, PTH induces renal 1alpha-hydroxylase expression, with consequent productionof active1,25 dihydroxyvitamin D (1,25[OH]2 D).1,25(OH)2 D enhances intestinal calcium absorption.It also acts on the immature osteoblastic cells to stim-ulate osteoclastogenesis through the RANKL/RANKregulatory system, finally resulting in enhanced boneresorption and mobilization of calcium from the bonecompartment. Resulting higher levels of calcium and
1,25(OH)2 D then downregulate PTH secretion andprevent unlimited resorption of bone. In addition,several reports indicate that 1,25(OH)2 D enhancesOPG expression in mature osteoblasts, thus furtherreducing osteoclastogenesis in vivo.42
Risk Factors for Osteoporosis in COPD
Apart from important inherent risk factors such asage, female gender, and genetic background, severalother factors that may contribute to the developmentof osteoporosis are potentially amendable for interven-
Figure 1. Key mechanisms in the pathogenesis of osteoporosis in COPD. Osteoblasts direct osteoclastprecursors into mature activated osteoclasts through RANK/RANKL, an interaction that is blocked byOPG. OPG5osteoprotegerin; PTH5parathyroid hormone; RANK5 receptor activator of nuclearfactor-kB; RANKL5 receptor activator of nuclear factor-kB ligand; WNT5 Wnt signaling pathway.
wnloaded From: http://journal.publications.chestnet.org/ on 06/25/2015

8/21/2019 COPD Bone Metabolism and Osteoporosis
http://slidepdf.com/reader/full/copd-bone-metabolism-and-osteoporosis 5/10
652 Recent Advances in Chest Medicine
Use of Corticosteroids
Systemic GCSs are used as evidence-based treat-ment of COPD exacerbations despite their deleteri-ous effect on BMD and fracture incidence. A surveyof seven studies in 42,500 subjects concluded thatprior and current exposure to GCSs is correlated
with an increased risk of fractures.55 A meta-analysisby van Staa et al56 showed a strong inverse correla-tion between bone density and total cumulativedose of GCSs. A significant correlation was alsofound between the daily dose of GCSs and the riskof fractures. Even oral doses as low as 2.5 to 5 mgprednisone equivalent daily were associated with anincrease in fracture risk. The risk of fracture increasedrapidly after the start of oral corticosteroid therapy(within 3 to 6 months) but most of the excess riskof fracture disappeared within 1 year after stoppingtherapy. For COPD patients in particular, differentstudies demonstrate that patients receiving oral GCSare more likely to have one or more vertebral frac-tures.20,25 The effect of inhaled corticosteroids (ICSs)on bone loss and fracture risk, on the other hand, is lessclear, with several cross-sectional studies reportingmild effects of high doses of ICSs on bone turnover.57 In a meta-analysis, Drummond et al58 included threelarge randomized controlled trials on ICSs in COPD
with fractures as secondary outcome and could notfind any statistically significant difference betweengroups. Similarly, a recent substudy of Towards aRevolution in COPD Health (TORCH) in 658 patientsrevealed no significant effect of ICS on BMD over
the course of 3 years.11
Because the follow-up in mostof these studies was relatively short compared withthe need for long-term treatment of COPD patientsin real life and because high doses have been associ-ated with increased rates of bone turnover,59 furtherstudies are needed and further care should be givento prescribe the lowest dose of ICSs possible.
Gonadal Sex Steroids
Sex steroids and their receptors play a crucial rolein skeletal growth and maturation but are also impor-tant for the maintenance of skeletal integrity at later
stages in life. It is well established that a decreasein bioavailable sex steroid hormones is related tobone loss not only in postmenopausal women, butalso in elderly men.60,61 Although estrogen concen-trations (17b -estradiol) are linked with bone turn-over, bone loss, and even fracture risk in both post-menopausal women and elderly men, the evidencefor androgens is less convincing.62,63 Testosteronemay have direct effects on the bone via androgenreceptors, but it may also act on estrogen receptorsafter aromatization to estradiol in vivo.64 Hypogonad-ism in men is an accepted risk factor for osteoporosis,
25 hydroxyvitamin D (25-OHD) levels and BMD hasbeen described in different populations, includingCOPD patients.47,48 Lower 25-OHD levels are alsoassociated with muscle weakness and an increasedrisk of falls.49 The prevalence of vitamin D defi-
ciency is rising. According to data from the NationalHealth and Nutrition Examination Survey in theUnited States, population mean 25-OHD levelsdecreased from 30 ng/mL to 24 ng/mL over thelast 15 years.50 In elderly patients, it is estimatedthat vitamin D deficiency may even occur in up to40% to 70% of the population.51,52 Some contro-
versy stil l exists about which cutoffs are appropri-ate for defining optimal vitamin D levels, butnowadays most experts agree on a 25-OHD levelbelow 20 ng/mL (50 nmol/L) to define low circulat-ing vitamin D levels. With respect to this 20-ng/mL
threshold, a cross-sectional analysis of 25-OHDlevels in 414 smokers revealed that compared with31% of the healthy smokers, 39%, 47%, and as manyas 60% and 77% of the patients with GOLD I to IVexhibited vitamin D deficiency. 25-OHD levels wereindependently determined by season and diseaseseverity, but also by genetic variation in the vitaminD binding gene,53 supporting a role for standardsupplementation in the majority of patients. Thecurrently recommended supplementation dose of800 International Units/d is an estimated averagerequirement for older adults to reach 25-OHD lev-
els of 30 ng/mL, a serum concentration well abovethe cutoff for deficiency and certainly sufficientfor adequate bone protection. However, the effec-tive repletion dose for an individual patient variesaccording to the initial level of deficiency, BMI, effec-tive sun exposure, and genetic and other unidenti-fied factors. Each 100 International Units/d isestimated to increase the serum 25-OHD level by1.0 ng/mL (range 0.7-1.1 ng/mL) and when usingsuch calculated repletion doses in high risk patients,25-OHD should be retested after 3 months oftherapy.54
Figure 2. COPD-related risk factors for osteoporosis and itsfunctional consequences.
wnloaded From: http://journal.publications.chestnet.org/ on 06/25/2015
8/21/2019 COPD Bone Metabolism and Osteoporosis
http://slidepdf.com/reader/full/copd-bone-metabolism-and-osteoporosis 6/10
www.chestpubs.org CHEST / 139 / 3 / MARCH, 2011 653
vention in COPD patients, and the benefits of multi-disciplinary rehabilitation in symptomatic patientshave been clearly established.72 However, althoughseveral training methods have demonstrated positive
effects on bone density in a healthy general popula-tion, studies in COPD patients are lacking. Ran-domized controlled trials are definitely required todetermine which training modalities, from a skeletalperspective, are most efficient in the context of COPD.Indirectly, training benefits on skeletal muscle force,balance impairment, and self-confidence may alsoreduce the risk of falling and prevent osteoporosisfrom causing symptoms. Furthermore, the beneficialeffects of other lifestyle modifications, such as smok-ing cessation and healthy diet, on osteoporosis andosteoporotic fracture occurrence in established COPD
should still be confirmed with intervention studies.
Calcium and Vitamin D Supplementation
Supplementation of calcium and vitamin D enhancesbone density, suppresses bone remodeling, andreduces fracture risk in older individuals.73 However,compliance with supplements is essential, with nolong-lasting benefits once calcium and vitamin D havebeen discontinued.74 In a recent meta-analysis, Bischoff-Ferrari et al75 studied the efficacy of oral vitamin Dsupplements on nonvertebral fractures in an elderly
but testosterone-replacement studies have yieldedconflicting results with only beneficial bone effectsbelow a testosterone serum threshold of 200 ng/dL.65,66 In COPD, low 17b -estradiol levels have been asso-
ciated with an increased risk of osteoporosis.14 Men with COPD exhibit reduced testosterone levels whencompared with healthy control subjects,67,68 but dif-ferent intervention trials with androgens demon-strated only modest effects on muscle mass andstrength, especially in combination with rehabilita-tion. They did not report beneficial effects on thebone.69,70 A crossover study in asthmatic men on long-term GCS, however, indicated that testosterone couldalso increase BMD.71 Not in the least because of sideeffects and increased cancer risk, more research isneeded to define the role of sex steroids and analogs
in the treatment of COPD and osteoporosis.
Prevention and Treatment of
Osteoporosis in COPD Patients
Nonpharmacologic Interventions
Cross-sectional and epidemiologic evidence sug-gests a strong association between several lifestyle fac-tors in COPD patients and the risk of osteoporoticfragility fractures. Physical inactivity, smoking, andpoor diet are accepted as important domains for inter-
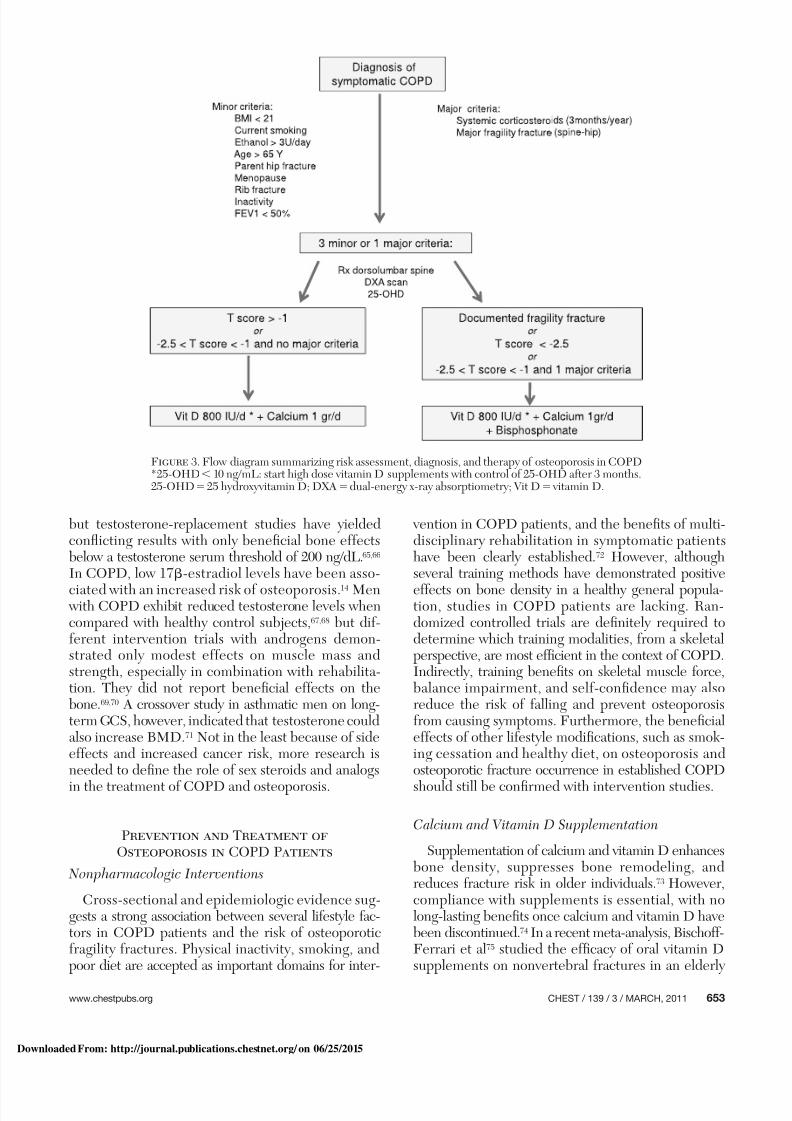
Figure 3. Flow diagram summarizing risk assessment, diagnosis, and therapy of osteoporosis in COPD*25-OHD, 10 ng/mL: start high dose vitamin D supplements with control of 25-OHD after 3 months.25-OHD525 hydroxyvitamin D; DXA5dual-energy x-ray absorptiometry; Vit D5 vitamin D.
wnloaded From: http://journal.publications.chestnet.org/ on 06/25/2015

8/21/2019 COPD Bone Metabolism and Osteoporosis
http://slidepdf.com/reader/full/copd-bone-metabolism-and-osteoporosis 7/10
654 Recent Advances in Chest Medicine
multiple existing deformities), teriparatide may be apreferred alternative.
To take into account independent clinical deter-minants of fracture risk (such as corticosteroid use),FRAX was developed recently. FRAX is a computer-based algorithm (http://www.shef.ac.uk/FRAX) thatprovides models for assessment of fracture probabil-ity in men and women from the information provided
from clinical risk factors such as age, sex, BMI, priorfragility fracture, smoking status, ethanol abuse, andprior use of GCS. With FRAX, the 10-year fractureprobability can be derived from these clinical riskfactors for fractures, alone or with femoral neckBMD, to enhance fracture risk prediction and to iden-tify patients who will benefit most from treatment.85,86 FRAX will likely become an increasingly useful toolfor defining intervention thresholds in patients receiv-ing corticosteroids, including patients with COPD.However, for the time being, the identification ofpatients who need antiresorptive treatment contin-
ues to be based on bone density and prevalent frac-ture status. Trials in osteoporosis have typically usedDXA-defined T scores below 2 2.5 SD or existing(vertebral) fractures to enroll patients and defineintervention thresholds. However, it is recognizedthat these thresholds are different for high-risk patientsreceiving long-term GCS treatment (. 3 months)because corticosteroid treatment enhances fractureprobability, independently of age or bone density. Inthis regard, numerous guidelines, including those ofthe Royal College of Physicians and the AmericanCollege of Rheumatology, recommend antiresorptive
treatment in corticosteroid-treated patients withDXA-defined osteopenia (T score between 2 1 and2 2.5), even in the absence of existing fragility frac-tures.87,88 Because these guidelines predated PTHtherapy and have not yet integrated multiple risk-assessment tools, an update in the nearby future willbe required. The controversy on repetitive BMD mea-surements and/or the use of biochemical markers tomonitor treatment effects may then be tackled as well.89 At present, clinicians should consider a follow-upDXA scan 1 year after starting pharmacologic therapyand thereafter at intervals determined by the indi-
vidual situation.90
Conclusions
Osteoporosis is common in COPD and should be amajor concern in the diagnostic and therapeuticapproach to COPD patients, who should be regardedas individuals at risk benefiting from osteoporosisassessment and therapy. A clinical guidance to a moreaggressive approach is summarized in a flowchart, whichintegrates risk assessment, diagnosis, and therapeuticinterventions ( Fig 3). Briefly, early diagnosis is important,
population aged older than 65 years. They concludedthat, compared with calcium or placebo, vitamin D
was able to reduce fracture risk and that this effect was dose dependent. Higher doses of vitamin D(800 International Units/d) reduced nonvertebralfractures by approximately 20% and hip fracturesby approximately 18%, whereas 400 InternationalUnits/d was not effective. To address the potential
benefit of calcium in individuals treated with vitamin D,Boonen et al76 performed a comparative meta-analysisand found that the risk of hip fractures was reducedonly when calcium was added to vitamin D. Similarfindings were reported by a recent Cochrane review.77 Particularly appealing about calcium and vitamin Dis that supplements not only reduce bone loss butalso prevent falls. Bischoff-Ferrari and colleagues78 demonstrated that vitamin D (800 InternationalUnits/d) reduced the risk of falling in older individualsby 19%. This fall-preventive effect does not requirecalcium but is related to vitamin D-induced improve-
ments in muscle function and postural stability.Specific data for COPD patients are currently lack-
ing, but the fact that the majority of COPD patients areof older age, have many additional risk factors forosteoporosis, and are more likely to have at least somedegree of vitamin D deficiency supports the need forstandard supplementation (800 International Units/d)in most of these risk patients. We recommend an evenmore aggressive repletion regimen when 25-OHDlevels are below 10 ng/mL.54 Moreover, we and oth-ers have suggested that the effect of high doses of
vitamin D supplementation might extend beyond
the protection of bone because 1,25-(OH)2 D maydirectly affect inflammation and interfere with othercomorbidities.79
Antiresorptive Therapy
Bisphosphonates are the most widely used drugsfor osteoporosis. They have a high affinity for bonemineral and impair bone resorption by blocking keyenzymes of osteoclasts.80 Numerous studies havedemonstrated a protective effect of bisphosphonatesin postmenopausal and glucocorticoid-induced osteo-
porosis.81 but few trials have specifically addressed theeffect of antiresorptive agents in COPD. One excep-tion is a randomized controlled trial by Smith et al82 demonstrating a significant improvement in lumbarspine BMD through daily intake of alendronate. Forglucocorticoid-induced osteoporosis in particular,teriparatide, a more potent anabolic drug, was foundto be superior to alendronate in increasing bone den-sity and reducing vertebral (but not nonvertebral)fracture risk.83,84 Although more studies are neededto determine its exact place in the current treatment,in high-risk patients receiving GCS (eg, those with
wnloaded From: http://journal.publications.chestnet.org/ on 06/25/2015

8/21/2019 COPD Bone Metabolism and Osteoporosis
http://slidepdf.com/reader/full/copd-bone-metabolism-and-osteoporosis 8/10
www.chestpubs.org CHEST / 139 / 3 / MARCH, 2011 655
pulmonary disease: an underestimated systemic component.Respir Med . 2009;103(8):1143-1151.
11. Ferguson GT, Calverley PM, Anderson JA, et al. Prevalenceand Progression of Osteoporosis in Patients with COPD:results From the TOwards a Revolution in COPD healthStudy. Chest . 2009;136(6):1456-1465.
12. Sin DD, Man JP, Man SF. The risk of osteoporosis inCaucasian men and women with obstructive airways disease.
Am J Med . 2003;114(1):10-14.13. Førli L, Mellbye OJ, Halse J, Bjørtuft O, Vatn M, Boe J.
Cytokines, bone turnover markers and weight change incandidates for lung transplantation. Pulm Pharmacol Ther .2008;21(1):188-195.
14. Iqbal F, Michaelson J, Thaler L, Rubin J, Roman J, Nanes MS.Declining bone mass in men with chronic pulmonary disease:contribution of glucocorticoid treatment, body mass index,and gonadal function. Chest . 1999;116(6):1616-1624.
15. Sabit R, Bolton CE, Edwards PH, et al. Arterial stiffness andosteoporosis in chronic obstructive pulmonary disease. Am JRespir Crit Care Med . 2007;175(12):1259-1265.
16. Bolton CE, Ionescu AA, Shiels KM, et al. Associated lossof fat-free mass and bone mineral density in chronic obstruc-tive pulmonary disease. Am J Respir Crit Care Med . 2004; 170(12):1286-1293.
17. Jørgensen NR, Schwarz P, Holme I, Henriksen BM, Petersen LJ,Backer V. The prevalence of osteoporosis in patients withchronic obstructive pulmonary disease: a cross sectional study.Respir Med . 2007;101(1):177-185.
18. Nuti R, Siviero P, Maggi S, et al. Vertebral fractures in patients with chronic obstructive pulmonary disease: the EOLO Study.Osteoporos Int . 2009;20(6):989-998.
19. Papaioannou A, Parkinson W, Ferko N, et al. Prevalence of vertebral fractures among patients with chronic obstructivepulmonary disease in Canada. Osteoporos Int . 2003;14(11): 913-917.
20. McEvoy CE, Ensrud KE, Bender E, et al. Associationbetween corticosteroid use and vertebral fractures in oldermen with chronic obstructive pulmonary disease. Am J Respir
Crit Care Med . 1998;157(3 Pt 1):704-709.21. Lyles KW, Gold DT, Shipp KM, Pieper CF, Martinez S,Mulhausen PL. Association of osteoporotic vertebral com-pression fractures with impaired functional status. Am J Med .1993;94(6):595-601.
22. Nevitt MC, Ettinger B, Black DM, et al. The associationof radiographically detected vertebral fractures with backpain and function: a prospective study. Ann Intern Med .1998;128(10):793-800.
23. Lindsay R, Silverman SL, Cooper C, et al. Risk of new ver-tebral fracture in the year following a fracture. JAMA . 2001; 285(3):320-323.
24. Myers AH, Robinson EG, Van Natta ML, Michelson JD,Collins K, Baker SP. Hip fractures among the elderly: fac-tors associated with in-hospital mortality. Am J Epidemiol .
1991;134(10):1128-1137.25. Walsh LJ, Wong CA, Oborne J, et al. Adverse effects of oral
corticosteroids in relation to dose in patients with lung dis-ease. Thorax . 2001;56(4):279-284.
26. Dam TT, Harrison S, Fink HA, et al. Bone mineral densityand fractures in older men with chronic obstructive pulmo-nary disease or asthma. Osteoporos Int . 2009;21(8):1341-1349.
27. Raisz LG. Pathogenesis of osteoporosis: concepts, conflicts,and prospects. J Clin Invest . 2005;115(12):3318-3325.
28. Manolagas SC, Jilka RL. Bone marrow, cytokines, and boneremodeling. Emerging insights into the pathophysiology ofosteoporosis. N Engl J Med . 1995;332(5):305-311.
29. Sambrook P, Cooper C. Osteoporosis. Lancet . 2006;367(9527): 2010-2018.
even in COPD patients with no symptoms. In thisregard, identification of vertebral compression frac-tures on radiograph, measurement of 25-OHD lev-els, and DXA scan are recommended in all patients
with an obvious risk profile for osteoporosis. Standardsupplementation with vitamin D and calcium mustbe considered in all these patients at risk and, in line
with established guidelines, COPD patients receiving
GCS should be started with antiresorptive treatmentnot only when osteoporotic (T score , 2 2.5 or exist-ing fragility fracture) but even when having DXA-defined osteopenia (T score , 2 1).
Acknowledgments
Financial/nonfinancial disclosures: The authors have reportedto CHEST the following conflicts of interest: Dr Decramer hasreceived grant monies from AstraZeneca. He has been a consul-tant to Dompe, GlaxoSmithKline, Boehringer, and Nycomed andhas received monies from Pfizer. Drs Lehouck, Boonen, and Janssenshave reported that no potential conflicts of interest exist with anycompanies/organizations whose products or services may be dis-
cussed in this article.
References
1. Rabe KF, Hurd S, Anzueto A, et al; Global Initiative forChronic Obstructive Lung Disease. Global strategy for thediagnosis, management, and prevention of chronic obstruc-tive pulmonary disease: GOLD executive summary. Am JRespir Crit Care Med . 2007;176(6):532-555.
2. Decramer M, Rennard S, Troosters T, et al. COPD as alung disease with systemic consequences—clinical impact,mechanisms, and potential for early intervention. COPD .2008;5(4):235-256.
3. Felsenberg D, Boonen S. The bone quality framework:determinants of bone strength and their interrelationships,and implications for osteoporosis management. Clin Ther .2005;27(1):1-11.
4. Kanis JA; WHO Study Group. Assessment of fracture risk andits application to screening for postmenopausal osteoporosis:synopsis of a WHO report. Osteoporos Int . 1994;4(6):368-381.
5. Bergmann P, Body JJ, Boonen S, et al; Members of AdvisoryBoard on Bone Markers. Evidence-based guidelines for theuse of biochemical markers of bone turnover in the selectionand monitoring of bisphosphonate treatment in osteoporosis:a consensus document of the Belgian Bone Club. Int J ClinPract . 2009;63(1):19-26.
6. Haentjens P, Magaziner J, Colón-Emeric CS, et al. Meta-analysis: excess mortality after hip fracture among older
women and men. Ann Intern Med . 2010;152(6):380-390.7. Carter JD, Patel S, Sultan FL, et al. The recognition and treat-
ment of vertebral fractures in males with chronic obstructivepulmonary disease. Respir Med . 2008;102(8):1165-1172.
8. Barrett-Connor E, Nielson CM, Orwoll E, Bauer DC, Cauley JA;Osteoporotic Fractures in Men Study Group. Epidemiologyof rib fractures in older men: Osteoporotic Fractures in Men(MrOS) prospective cohort study. BMJ . 2010;340:c1069:1-8.
9. Graat-Verboom L, Wouters EF, Smeenk FW, van den BorneBE, Lunde R, Spruit MA. Current status of research onosteoporosis in COPD: a systematic review. Eur Respir J .2009;34(1):209-218.
10. Graat-Verboom L, Spruit MA, van den Borne BE, et al; CIRONetwork. Correlates of osteoporosis in chronic obstructive
wnloaded From: http://journal.publications.chestnet.org/ on 06/25/2015

8/21/2019 COPD Bone Metabolism and Osteoporosis
http://slidepdf.com/reader/full/copd-bone-metabolism-and-osteoporosis 9/10
656 Recent Advances in Chest Medicine
52. Dawson-Hughes B, Heaney RP, Holick MF, Lips P, MeunierPJ, Vieth R. Estimates of optimal vitamin D status. OsteoporosInt . 2005;16(7):713-716.
53. Janssens W, Bouillon R, Claes B, et al. Vitamin D deficiencyis highly prevalent in COPD and correlates with variants inthe vitamin D-binding gene. Thorax . 2010;65(3):215-220.
54. Dawson-Hughes B, Mithal A, Bonjour JP, et al. IOF posi-tion statement: vitamin D recommendations for older adults.Osteoporos Int . 2010;21(7):1151-1154.
55. Kanis JA, Johansson H, Oden A, et al. A meta-analysis of
prior corticosteroid use and fracture risk. J Bone Miner Res .2004;19(6):893-899.
56. van Staa TP, Leufkens HG, Cooper C. The epidemiol-ogy of corticosteroid-induced osteoporosis: a meta-analysis.Osteoporos Int . 2002;13(10):777-787.
57. Langhammer A, Forsmo S, Syversen U. Long-term therapy inCOPD: any evidence of adverse effect on bone? Int J ChronObstruct Pulmon Dis . 2009;4(4):365-380.
58. Drummond MB, Dasenbrook EC, Pitz MW, Murphy DJ,Fan E. Inhaled corticosteroids in patients with stable chronicobstructive pulmonary disease: a systematic review and meta-analysis. JAMA . 2008;300(20):2407-2416.
59. Jones A, Fay JK, Burr M, Stone M, Hood K, Roberts G.Inhaled corticosteroid effects on bone metabolism in asthma
and mild chronic obstructive pulmonary disease. CochraneDatabase Syst Rev . 2002;(1):CD003537.
60. Riggs BL, Khosla S, Melton LJ III. Sex steroids and the con-struction and conservation of the adult skeleton. Endocr Rev .2002;23(3):279-302.
61. Callewaert F, Boonen S, Vanderschueren D. Sex steroids andthe male skeleton: a tale of two hormones. Trends EndocrinolMetab . 2010;21(2):89-95.
62. Goderie-Plomp HW, van der Klift M, de Ronde W, Hofman A,de Jong FH, Pols HA. Endogenous sex hormones, sexhormone-binding globulin, and the risk of incident vertebralfractures in elderly men and women: the Rotterdam Study.
J Clin Endocrinol Metab . 2004;89(7):3261-3269.63. Mellström D, Vandenput L, Mallmin H, et al. Older men with
low serum estradiol and high serum SHBG have an increasedrisk of fractures. J Bone Miner Res . 2008;23(10):1552-1560.64. Clarke BL, Khosla S. Androgens and bone. Steroids . 2009;
74(3):296-305.65. Snyder PJ, Peachey H, Hannoush P, et al. Effect of testoster-
one treatment on bone mineral density in men over 65 yearsof age. J Clin Endocrinol Metab . 1999;84(6):1966-1972.
66. Fink HA, Ewing SK, Ensrud KE, et al. Association of tes-tosterone and estradiol deficiency with osteoporosis andrapid bone loss in older men. J Clin Endocrinol Metab .2006;91(10):3908-3915.
67. Van Vliet M, Spruit MA, Verleden G, et al. Hypogonadism,quadriceps weakness, and exercise intolerance in chronicobstructive pulmonary disease. Am J Respir Crit Care Med .2005;172(9):1105-1111.
68. Laghi F. Low testosterone in chronic obstructive pulmonarydisease: does it really matter? Am J Respir Crit Care Med .2005;172(9):1069-1070.
69. Schols AM, Soeters PB, Mostert R, Pluymers RJ, WoutersEF. Physiologic effects of nutritional support and anabolicsteroids in patients with chronic obstructive pulmonary dis-ease. A placebo-controlled randomized trial. Am J Respir CritCare Med . 1995;152(4 Pt 1):1268-1274.
70. Casaburi R, Bhasin S, Cosentino L, et al. Effects of testosteroneand resistance training in men with chronic obstructive pulmo-nary disease. Am J Respir Crit Care Med . 2004;170(8):870-878.
71. Reid IR, Ibbertson HK, France JT, Pybus J. Plasma testoster-one concentrations in asthmatic men treated with glucocorti-coids. Br Med J (Clin Res Ed) . 1985;291(6495):574.
30. Lacey DL, Timms E, Tan HL, et al. Osteoprotegerin ligand isa cytokine that regulates osteoclast differentiation and activa-tion. Cell . 1998;93(2):165-176.
31. Leibbrandt A, Penninger JM. RANK/RANKL: regulators ofimmune responses and bone physiology. Ann N Y Acad Sci .2008;1143:123-150.
32. Patel MS, Karsenty G. Regulation of bone formation and vision by LRP5. N Engl J Med . 2002;346(20):1572-1574.
33 Biskobing DM. COPD and osteoporosis. Chest . 2002;121(2): 609-620.
34. Hardy R, Cooper MS. Bone loss in inflammatory disorders. J Endocrinol . 2009;201(3):309-320.
35. Lorenzo J, Horowitz M, Choi Y. Osteoimmunology: interactionsof the bone and immune system. Endocr Rev . 2008;29(4): 403-440.
36. Diarra D, Stolina M, Polzer K, et al. Dickkopf-1 is a mas-ter regulator of joint remodeling. Nat Med . 2007;13(2): 156-163.
37. Canalis E, Mazziotti G, Giustina A, Bilezikian JP. Glucocorticoid-induced osteoporosis: pathophysiology and therapy. OsteoporosInt . 2007;18(10):1319-1328.
38. Weinstein RS, Chen JR, Powers CC, et al. Promotion of osteo-clast survival and antagonism of bisphosphonate-inducedosteoclast apoptosis by glucocorticoids. J Clin Invest . 2002;
109(8):1041-1048.39. Eijken M, Hewison M, Cooper MS, et al. 11beta-Hydroxysteroid
dehydrogenase expression and glucocorticoid synthesis aredirected by a molecular switch during osteoblast differentia-tion. Mol Endocrinol . 2005;19(3):621-631.
40. Ohnaka K, Tanabe M, Kawate H, Nawata H, Takayanagi R.Glucocorticoid suppresses the canonical Wnt signal in cul-tured human osteoblasts. Biochem Biophys Res Commun .2005;329(1):177-181.
41. Lips P. Vitamin D deficiency and secondary hyperparathy-roidism in the elderly: consequences for bone loss and frac-tures and therapeutic implications. Endocr Rev . 2001;22(4): 477-501.
42. Baldock PA, Thomas GP, Hodge JM, et al. Vitamin D
action and regulation of bone remodeling: suppression ofosteoclastogenesis by the mature osteoblast. J Bone MinerRes . 2006;21(10):1618-1626.
43. Papaioannou A, Kennedy CC, Cranney A, et al. Risk factorsfor low BMD in healthy men age 50 years or older: a system-atic review. Osteoporos Int . 2009;20(4):507-518.
44. Kanis JA. Diagnosis of osteoporosis and assessment of frac-ture risk. Lancet . 2002;359(9321):1929-1936.
45. Ohara T, Hirai T, Muro S, et al. Relationship between pulmo-nary emphysema and osteoporosis assessed by CT in patients
with COPD. Chest . 2008;134(6):1244-1249.46. Makita H, Nasuhara Y, Nagai K, et al; Hokkaido COPD
Cohort Study Group. Characterisation of phenotypes basedon severity of emphysema in chronic obstructive pulmonarydisease. Thorax . 2007;62(11):932-937.
47. Collins D, Jasani C, Fogelman I, Swaminathan R. Vitamin Dand bone mineral density. Osteoporos Int . 1998;8(2):110-114.
48. Franco CB, Paz-Filho G, Gomes PE, et al. Chronic obstruc-tive pulmonary disease is associated with osteoporosisand low levels of vitamin D. Osteoporos Int . 2009;20(11): 1881-1887.
49. Bischoff-Ferrari HA, Dawson-Hughes B, Willett WC,et al. Effect of Vitamin D on falls: a meta-analysis . JAMA .2004;291(16):1999-2006.
50. Ginde AA, Liu MC, Camargo CA Jr. Demographic differ-ences and trends of vitamin D insufficiency in the US popula-tion, 1988-2004. Arch Intern Med . 2009;169(6):626-632.
51. Holick MF. Vitamin D deficiency. N Engl J Med . 2007; 357(3):266-281.
wnloaded From: http://journal.publications.chestnet.org/ on 06/25/2015

8/21/2019 COPD Bone Metabolism and Osteoporosis
http://slidepdf.com/reader/full/copd-bone-metabolism-and-osteoporosis 10/10
www.chestpubs.org CHEST / 139 / 3 / MARCH, 2011 657
72. Troosters T, Casaburi R, Gosselink R, Decramer M. Pul-monary rehabilitation in chronic obstructive pulmonary disease.
Am J Respir Crit Care Med . 2005;172(1):19-38.73. Chapuy MC, Arlot ME, Duboeuf F, et al. Vitamin D3 and
calcium to prevent hip fractures in the elderly women. N Engl J Med . 1992;327(23):1637-1642.
74. Dawson-Hughes B, Harris SS, Krall EA, Dallal GE. Effectof withdrawal of calcium and vitamin D supplements onbone mass in elderly men and women. Am J Clin Nutr .2000;72(3):745-750.
75. Bischoff-Ferrari HA, Willett WC, Wong JB, et al. Preventionof nonvertebral fractures with oral vitamin D and dose depen-dency: a meta-analysis of randomized controlled trials. ArchIntern Med . 2009;169(6):551-561.
76. Boonen S, Lips P, Bouillon R, Bischoff-Ferrari HA, Vanderschueren D, Haentjens P. Need for additional calciumto reduce the risk of hip fracture with vitamin D supplemen-tation: evidence from a comparative metaanalysis of random-ized controlled trials. J Clin Endocrinol Metab . 2007;92(4): 1415-1423.
77. Avenell A, Gillespie WJ, Gillespie LD, O’Connell D. Vitamin Dand vitamin D analogues for preventing fractures associ-ated with involutional and post-menopausal osteoporosis.Cochrane Database Syst Rev . 2009;(2):CD000227.
78. Bischoff-Ferrari HA, Dawson-Hughes B, Staehelin HB, et al.Fall prevention with supplemental and active forms of vita-min D: a meta-analysis of randomised controlled trials. BMJ .2009;339:b3692:1-11.
79. Janssens W, Lehouck A, Carremans C, Bouillon R, Mathieu C,Decramer M. Vitamin D beyond bones in chronic obstructivepulmonary disease: time to act. Am J Respir Crit Care Med . 2009; 179(8):630-636.
80. Russell RG, Watts NB, Ebetino FH, Rogers MJ. Mechanismsof action of bisphosphonates: similarities and differences andtheir potential influence on clinical efficacy. Osteoporos Int .2008;19(6):733-759.
81. Bilezikian JP. Efficacy of bisphosphonates in reducing frac-ture risk in postmenopausal osteoporosis. Am J Med . 2009; 122(2 Suppl):S14-S21.
82. Smith BJ, Laslett LL, Pile KD, et al. Randomized controlledtrial of alendronate in airways disease and low bone mineraldensity. Chron Respir Dis . 2004;1(3):131-137.
83. Langdahl BL, Marin F, Shane E, et al. Teriparatide versusalendronate for treating glucocorticoid-induced osteoporosis:an analysis by gender and menopausal status. Osteoporos Int .2009;20(12):2095-2104.
84. Saag KG, Shane E, Boonen S, et al. Teriparatide or alen-dronate in glucocorticoid-induced osteoporosis. N Engl JMed . 2007;357(20):2028-2039.
85. Lim LS, Hoeksema LJ, Sherin K; ACPM Prevention PracticeCommittee. Screening for osteoporosis in the adult U.S.population: ACPM position statement on preventive practice.
Am J Prev Med . 2009;36(4):366-375.86. Kanis JA, McCloskey EV, Johansson H, Strom O, Borgstrom F,
Oden A; National Osteoporosis Guideline Group. Case findingfor the management of osteoporosis with FRAX—assessmentand intervention thresholds for the UK. Osteoporos Int .2008;19(10):1395-1408.
87. Compston J. US and UK guidelines for glucocorticoid-inducedosteoporosis: similarities and differences. Curr Rheumatol Rep .
2004;6(1):66-69.88. Devogelaer JP, Goemaere S, Boonen S, et al. Evidence-based
guidelines for the prevention and treatment of glucocorticoid-induced osteoporosis: a consensus document of the BelgianBone Club. Osteoporos Int . 2006;17(1):8-19.
89. Bell KJ, Hayen A, Macaskill P, et al. Value of routine moni-toring of bone mineral density after starting bisphosphonatetreatment: secondary analysis of trial data. BMJ . 2009;338: b2266:1-5.
90. Watts NB, Lewiecki EM, Bonnick SL, et al. Clinical valueof monitoring BMD in patients treated with bisphosphonatesfor osteoporosis. J Bone Miner Res . 2009;24(10):1643-1646.


















