Vitamin K2 in Bone Metabolism and Osteoporosis K2 in Bone Metabolism and Osteoporosis_0.pdf ·...
13
Vitamin K / Osteoporosis Review Vitamin K2 in Bone Metabolism and Osteoporosis Steven M. Plaza, ND, LAc, and Davi.s W. Lamson, MS, ND Abstract This article covers in vitro, in vivo, and human data on the positive effect of vitamin K2 on osteoporosis. Data is available on vitamin K2 for osteoporosis caused by a number of conditions, including postmenopausal osteoporosis, Parkinson's disease, biliary cirrhosis, stroke, and drug-induced osteoporosis. The activity of vitamin K2 involves both an increase in the bone-building process and a separate decrease in the bone- loss process. Vitamin K2 exerts a more powerful influence on bone than vitamin K1, and should be considered for prevention or treatment in those conditions known to contribute to osteoporosis. {Aitern Metf/?ei^2005;10(1):24-35) Introduction Vitamin K2 exerts a powerful influence on bone building, especially in o.steoporosis. and has been cited as one of the most frequently prescribed treatments for osteoporosis in Japan.' The ability to better facilitate bone growth, especially in osteoporosis and fracture, has long been of interest. Repair of non-pathogenic fracture Is a nor- mal process, generally engaged in without difficulty. Osteoporosis, a pathogenic process, is increasingly occurring in developed countries, and pathologic fracture due to osteoporosis in the elderly can be a life-shortening event. A five-year prospective study on fracture and mortality rale in men and women age 60 and older found all major fractures were associ- ated with increased mortality, especially in men.- Osteoporosis, a multifactorial palhology, has been reviewed extensively in recent years.^"^ A review by Gaby of nutritional and hormonal management of osteoporosis is an excellent and well-referenced source for further edification.^ Evaluation of the etiology of osteoporosis in a particular individual can involve examination of hormonal aspects, exercise patterns, nutrient in- take, digestion, and nutrient absorption. This article addresses the aspects of vitamin K2 in bone forma- tion. The subject of nutrient absorption is pertinent because the vitamin Ks are lipid soluble; therefore, fat malabsorption may create a deficiency. Recent reviews revealing celiae disease is eommon (1 in 266)^" underscore its involvement in the etiology of osteoporosis due to malabsorptiun of necessary bone factors, including vitamin K.'- Documentation is plentiful illustrating the importance of vitamin K in bone maintenance. Its importance is easily evidenced by the osteoporosis and fractures resulting from long- term use of the anticoagulant drug warfarin, which inhibits the bone-building effect of vitamin K."'" The Vitamin Ks Vitamin K is a family of structurally similar, fat-soluble. 2-methyl-1.4-naphthoquinones. includ- ing phylloquinone (Kl). menaquinones (K2), and menadione (K3). The structural difference is in the substituent R group (Figure t). The best-known member of the vitamin K family is phylk>quinone (Kl). also known as phyto- nadione because of its relationship with photosyn- thesis. Phylloquinone is found in higher plants and algae, with the highest concentrations found in green leafy vegetables.''' Steven Plaza. NO, LAc - Faculty member ot Oncology department. Bastyr University, Kenmore. WA; Private practice. Norttiwest Center for Natural Medicine, Oiympia, WA Correspondence address: 1324 Harrison Ave. NW. Olympia, WA 98502 Davis W. Lamson. MS. ND - Coordinator of Oncology, Bastyr University. Kenmore. WA; Private practice, Tahoma Clinic. Renton, WA. Product consultant, Thome Research. Page 24 Alternative Medicine Review • Volume 10, Number 1 • 2005
Transcript of Vitamin K2 in Bone Metabolism and Osteoporosis K2 in Bone Metabolism and Osteoporosis_0.pdf ·...
Vitamin K / Osteoporosis Review
Vitamin K2 in Bone Metabolismand Osteoporosis
Steven M. Plaza, ND, LAc, and Davi.s W. Lamson, MS, ND
AbstractThis article covers in vitro, in vivo, and humandata on the positive effect of vitamin K2 onosteoporosis. Data is available on vitamin K2 forosteoporosis caused by a number of conditions,including postmenopausal osteoporosis,Parkinson's disease, biliary cirrhosis, stroke, anddrug-induced osteoporosis. The activity of vitaminK2 involves both an increase in the bone-buildingprocess and a separate decrease in the bone-loss process. Vitamin K2 exerts a more powerfulinfluence on bone than vitamin K1, and should beconsidered for prevention or treatment in thoseconditions known to contribute to osteoporosis.{Aitern Metf/?ei^2005;10(1):24-35)
IntroductionVitamin K2 exerts a powerful influence on
bone building, especially in o.steoporosis. and hasbeen cited as one of the most frequently prescribedtreatments for osteoporosis in Japan.'
The ability to better facilitate bone growth,especially in osteoporosis and fracture, has long beenof interest. Repair of non-pathogenic fracture Is a nor-mal process, generally engaged in without difficulty.Osteoporosis, a pathogenic process, is increasinglyoccurring in developed countries, and pathologicfracture due to osteoporosis in the elderly can be alife-shortening event. A five-year prospective studyon fracture and mortality rale in men and women age60 and older found all major fractures were associ-ated with increased mortality, especially in men.-
Osteoporosis, a multifactorial palhology, hasbeen reviewed extensively in recent years.̂ "^ A reviewby Gaby of nutritional and hormonal managementof osteoporosis is an excellent and well-referencedsource for further edification.^
Evaluation of the etiology of osteoporosisin a particular individual can involve examinationof hormonal aspects, exercise patterns, nutrient in-take, digestion, and nutrient absorption. This articleaddresses the aspects of vitamin K2 in bone forma-tion. The subject of nutrient absorption is pertinentbecause the vitamin Ks are lipid soluble; therefore,fat malabsorption may create a deficiency. Recentreviews revealing celiae disease is eommon (1 in266)^" underscore its involvement in the etiologyof osteoporosis due to malabsorptiun of necessarybone factors, including vitamin K.'- Documentationis plentiful illustrating the importance of vitamin K inbone maintenance. Its importance is easily evidencedby the osteoporosis and fractures resulting from long-term use of the anticoagulant drug warfarin, whichinhibits the bone-building effect of vitamin K."'"
The Vitamin KsVitamin K is a family of structurally similar,
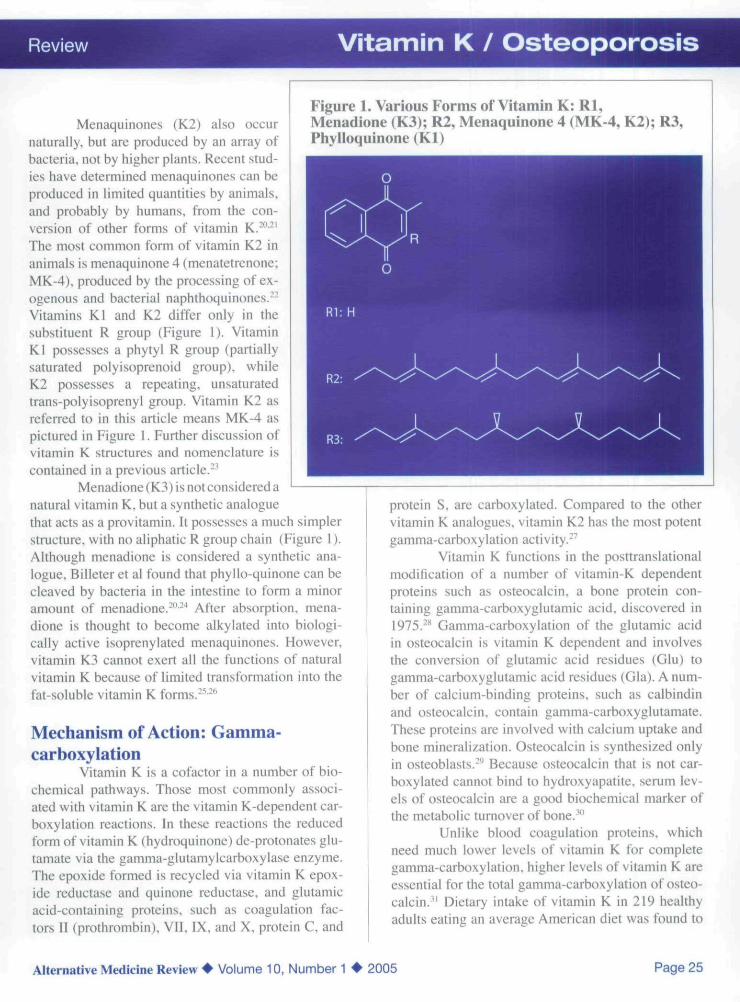
fat-soluble. 2-methyl-1.4-naphthoquinones. includ-ing phylloquinone (Kl). menaquinones (K2), andmenadione (K3). The structural difference is in thesubstituent R group (Figure t).
The best-known member of the vitamin Kfamily is phylk>quinone (Kl). also known as phyto-nadione because of its relationship with photosyn-thesis. Phylloquinone is found in higher plants andalgae, with the highest concentrations found in greenleafy vegetables.'''
Steven Plaza. NO, LAc - Faculty member ot Oncology department. BastyrUniversity, Kenmore. WA; Private practice. Norttiwest Center forNatural Medicine, Oiympia, WACorrespondence address: 1324 Harrison Ave. NW. Olympia, WA 98502
Davis W. Lamson. MS. ND - Coordinator of Oncology, Bastyr University.Kenmore. WA; Private practice, Tahoma Clinic. Renton, WA. Product consultant,Thome Research.
Page 24 Alternative Medicine Review • Volume 10, Number 1 • 2005
Vitamin K / Osteoporosis
Menaquinone.s (K2) also occurnaturally, but are produced by an array ofbacteria, not by higher plants. Recent stud-ies have determined menaquinones can beproduced in limited quantities by animals,and probably by humans, from the con-version of other forms of vitamin K.-"-'The most common form of vitamin K2 inanimals is menaquinone 4 (menatetrenone:MK-4), produced by the processing of ex-ogenous and bacterial naphthoquinones."Vitamins Kl and K2 differ only in thesubstituenl R group (Figure I). VitaminKl possesses a phytyl R group (partiallysaturated polyisoprenoid group), whileK2 possesses a repeating, unsaturatedtrans-polyisoprenyl group. Vitamin K2 asreferred to in this article means MK-4 aspictured in Figure 1. Further discussion ofvitamin K structures and nomenclature iscontained in a previous article.''
Menadione (K3) is not considered anatural vitamin K. but a synthetic analoguethat acts as a provitamin. It possesses a much simplerstructure, with no aliphatic R group chain (Figure I).Although menadione is considered a synthetic ana-logue. Billeter et al found that phyllo-quinone can becleaved by bacteria in the intestine to form a minoramount of menadione.^-"* After absorption, mena-dione is thought to become alkylated into biologi-cally active isoprenylated menaquinones. However,vitamin K3 cannot exert all the functions of naturalvitamin K because of limited transformation into thefat-soluble vitamin K forms.-''• '̂'
Mechanism of Action: Gamma-carboxylation
Vitamin K is a cofactor in a number of bio-chemical pathways. Those most commonly associ-ated with vitamin K are the vitamin K-dependent car-boxylation reactions. In these reactions the reducedform of vitamin K (hydroquinone) de-protonates glu-tamate via the gamma-giutamylcarboxylase enzyme.The epoxide formed is recycled via vitamin K epox-ide reductase and qiiinone reductase. and glutamicacid-containing proteins, such as coagulation fac-tors II (prothrombinj, VII, IX, and X, protein C, and
Figure 1. Various Forms of Vitamin K: Rl,Menadione (K3); R2, Menaquinone 4 (MK-4, K2); R3,Phylloquinone (Kl)
protein S. are carboxylated. Compared to the othervitamin K analogues, vitamin K2 has the most potentgamma-carboxylation activity.-"^
Vitamin K functions in the posttranslationalmodification of a number of vitamin-K dependentproteins such as osteocalcin. a bone protein con-taining gamma-carboxyglutamic acid, discovered in\915r'^ Gamma-carboxylation of the glutamic acidin osteocalcin is vitamin K dependent and involvesthe conversion of glutamic acid residues (Glu) togamma-carboxyglutamic acid residues (Gla). A num-ber of calcium-binding proteins, such as calbindinand osteocalcin, contain gamma-carboxyglutamate.These proteins are involved with calcium uptake andbone mineralization. Osteocalcin is synthesized onlyin osteoblasts.''' Because osteocalcin that is not car-boxylated cannot bind to hydroxyapatite. senim lev-els of osteocalcin are a good biochemical marker ofthe metabolic turnover of bone.^"
Unlike blood coagulation proteins, whichneed much lower levels of vitamin K for completegamma-carboxylation. higher levels of vitamin K areessential for the total gamma-carboxylation of osteo-calcin.'' Dietary intake of vitamin K in 219 healthyadults eating an average American diet was found to
Alternative Medicine Review • Volume 10, Number 1 • 2005 Page 25

Vitamin K / Osteoporosis
be insufficient for gamma-carboxylation of osteocal-cin. while maintaining normal prothrombin time.^-An elevated level of serum glutamic acid-under-carboxylated osteocalcin is indicative of vitamin Kdeficiency and is associated with reduced hip bonemineral density (BMD) and increased fracture risk inhealthy elderly women." Rats with hypoprothrom-binemia were given menadione (K3) or K2 orally(0.1 mg/kg) and the absorption and concentration inthe liver were compared. The most potent form wasfound to be vitamin K2.̂ "̂'
Safety of Vitamin K2 with Respect toHypercoagulation in Humans
From a large number of clinical trials usingdosages in excess of 40 mg/day. there were no re-ports of side effects associated with any type of hy-percoagulable state.'-^''"^ Both animal and clinicalstudies support the eonclusion that vitamin K2 has noabnormal hemostatic activity. In one study, vitaminK2 given to rats at a dose of 250 mg/kg body weightper day for 10 days resulted in no appreciable changein blood coagulation characteristies or platelet aggre-gation."
In a elinieal study, 29 elderly, osteoporoticpatients were given vitamin K2 (15 mg three timesdaily, 30 minutes post meals) for 12 weeks and moni-tored for any change in hemostatic balance. After12 weeks of administration, al! hemo.static markersremained within normal range.' In another study ex-amining the effect of vitamins K2 (45 mg/day) andD3 (1 meg/day) on BMD in postmenopausal women,hemostatic measures were also examined. Increasesin both coagulation and fibrinolysis were noted, butremained within nonnal range and in balance, withno adverse reactions observed.'^
It should be noted that the anticoagulant ef-fect of warfarin, functioning by its interference withthe clotting effect of vitamin K, can be oifset with aslittle as 1 mg of vitamin K.'*̂ Therefore, use of vita-min K is contraindicated in people on anticoagulanttherapy.
In Vitro Studies of Vitamin K2:Osteoblastic and OsteoclasticModulation
Variuus forms of vitamin K have been trans-formed into K2 in the femur. Rats fed MK-7 (contain-ing three more isoprene units in the MK-4 side-chain)were found to transform this longer chain analogueinto MK-4 in the femur. Vitamin K2 has been shownto be the most important inducer of bone mineraliza-tion in human osteoblasts.̂ "* Vitamin K2. in combina-tion with l-alpha-25-dihydroxyvitamin D3 has alsobeen shown to increase osteocalcin production.""' Invitro studies have shown that application of K2 re-sults in gamma-carboxylation of l-aIpha-25-dihy-droxyvitamin D3-induced osteocalcin, which in turnis able to deposit gamma-earboxyglutamic acid-con-taining osteocalcin to the extracellular matrix on hu-man osteoblasts.^'
//; vitro studies using assays from variousspecies demonstrate vitamin K2 inhibits osteoclasto-genesis of bone.̂ ^ Akiyama et al found that a dose-dependent inhibition of mouse 1.25-dihydroxyvita-min D3 stimulated multinucleate osteoclast-like cellformation. The mechanism of osteoclastic inhibitionby vitamin K2 is not due to cell toxicity and did notaffect cell proliferation.-"^-" The osteoclastic inhibi-tory action by K2 is unique to its structure. VitaminK1 does not affect bone resorption and multinucleateosteoclast-like cell formation.-'̂ //; vitro studies withmouse cell cultures found a dose-dependent inhibi-tion by K2 of prostaglandin E2 {PGE2) synthesis,which in turn was shown to inhibit bone resorption.''^The inhibition of 1,25-dihydroxyvitamin D3-inducedPGE2 production by K2 was found dependent on theinhibition of cyclooxygenase-2 expression."̂ "* Furtherresearch with human bone marrow cell culture foundevidence that the inhibition of osteoclast formationwas not due to an increase in cell death, but rather to adecrease in the production of the receptor activator ofnuclear factor kappaB ligand (RANKL) and associat-ed osteoclast differentiation factor, whieh are criticalto osteoclastogenesis.^' The prevention of bone lossdue to the inhibition of bone resorption found for ///vitro studies has been verified by in vivo studies withovariectomized rats fed vitamin K2 (50 mg/kg) fortwo weeks.""'
Page 26 Alternative Medicine Review • Volume 10, Number 1 • 2005
Review Vitamin K / Osteoporosis
Animal Studies with Vitamin K2Rat Model of Disuse Osteopenia
Studies of rats fed a vitamin K-deficient dietdetermined that larger amounts of vitamin K are need-ed for femur bone metabolism compared to the liver^^A number of studies have examined orchidectomizedor sciatic-neurectomized rats. The sciatic-neurecto-mized rat is used as a model of immobilization os-teopenia in humans and is used to study prevention ofdisuse osteopenia. The procedure reduces the normalmaturation-related increase in cortical and cancellousbone, inducing cortical and cancelious osteopenia.Orchidectomy results in a testosterone deficiency,which in turn reduces periosteal bone formation,while also increasing cancellous bone turnover. Theultimate result is an inhibition of cortical and cancel-lous bone gain without net bone loss.""* Cancellousbone loss is attributable to decreased bone formationand increased bone resorption; whereas, cortical boneloss results from decreased periosteal bone formationand increased endocortical bone resorption.
In neurectomized rats, oral administration ofvitamin K2 (10 or 30 mg/kg) for seven to 42 daysincreased bone mass and maintained secondary spon-gia microstructure in the immobilized tibiae. In theK2 30-mg/kg group, trabecular number and thicknessincreased and osteoblast-induced mineralization wasenhanced. By day 42. the osteoclast surface per boneperimeter, the number of osteoclasts per bone peri-meter, and the mineral apposition rate (MAR) werereduced in the controls, suggesting bone turnover wassuppressed. Low-dose vitamin K2 increased MARand bone formation rate, without increasing bone re-sorption. In this study, oral administration of vitaminK2 was found to reduce loss of trabecular bone, pre-vent osteoblast dysfunction, increase bone formationrate, and preserve trabecular microstructure in an im-mobilization model.̂ *̂
Vitamin K2 (30 mg/kg) administered twieeweekly for 10 weeks to orchidectomized rats re-sulted in suppressed endoeortical bone resorptionand trabecular bone turnover. Vitamin K2 in sciatic-neurectomized and orchidectomized rats suppressedbone resorption and stimulated bone formation. Theevidence indicates K2 has potential to enhance boneformation and inhibit bone resorption in orchidecto-mized or neurectomized rats."***
Rat Model of PostmenopausalOsteoporosis
Estrogen deficiency results in increased boneturnover leading to an increase in osteoclasts andtrabecular bone loss. Postmenopausal osteoporosis,characterized by increased fracture risk, can be ac-curately modeled using ovariectomized animals.Because ovariectomy in rats results in significant de-crease of BMD and eancellous bone remodeling, ithas been used as a model for estrogen-deficient, post-menopausal bone loss.
The administration of vitamin K2 has beenshown to prevent bone loss induced by ovariectomyin rats.-"'-'̂ ""-'- Vitamin K2 at 50 mg/kg inhibited theexpected decreases in trabecular number and BMDof the femur, and improved other bone parameterscaused by ovariectomy in only a two-week period."**In contrast, Binkley et al found no benefit on boneturnover or distal femur BMD density in ovariecto-mized rats."*' This study used an approximately equiv-alent dose of K2 (50 mg/kg) for three months. Theauthors suggest these disparate results might be ex-plained by three factors. First, the slight differencesin vitamin D3- (2.4 lU/g in previous studies versus2.2 IU/g by Binkley et al) and calcium- (0.02-0.5%in previous studies versus 1% by Binkley et al) defi-cient diets are proposed as a causative factor, with theresearchers speculating vitamin K may work best incalcium- and/or vitamin D-deprived rats. Second, theuse of a different strain of rat might cause the discrep-ancy, although earlier positive studies used the samestrain of rat as the negative study.'"' Third, the lengthof the study, Binkley "s being one month compared toAkiyama's two-week study, might contribute to thedisparity. However, earlier studies found effect aftersix months, which has been supported by later studiesthat have shown a minimum of six months for effec-tiveness at a dosage of 30 mg/kg.̂ •̂ •'̂ •' Despite the neg-ative results of Binkley et al, recent studies supportearlier work that clearly demonstrates vitamin K2 (30mg/kg) for six months prevented bone loss and fragil-ity of spine and femur in ovarieetomized rats.^-
Ovariectomy is also a good model to demon-strate degeneration of the microarchitecture of boneassociated with osteoporosis. Studies of the three-di-mensional trabecular microarchitecture in ovariecto-mized and calcium-deficient rats fed vitamin K2 (30
Alternative Medicine Review • Volume 10, Number 1 • 2005 Page 27
Vitamin K / Osteoporosis Review
mg/kg) for eight weeks demonstrated a significantpreservation (approximately 55% that of sham) oftrabecular bone volume, connectivity, and trabecu-lar complexity.^' The protective effect of vitamin K2on femoral strength and prevention of mechanical-strength decrease has also been supported by recentstudies of ovariectomized rats.^- Ovariectomized ratsgiven K2 (30 mg/kg) in combination with l-25-di-hydroxyvitamin D3 (0.3 mcg/kg three times weekly)orally for eight weeks demonstrated a significantlyhigher BMD, cortical thickness, and bone strengththan rats given either vitamin alone.̂ -̂
Other Animal Studies of Vitamin K2and Bone Preservation
Orchidectomized rats given vitamin K2 (30mg/kg twice weekly, subcutaneously) for eight weeksexhibited a significant increase in cancellous bonevolume but not cortical area compared to orchidec-tomized rats not given vitamin K. The researchersconcluded vitamin K2 was more effective at preserv-ing cancellous than cortical bone."'' In aged male rats,a caleium-deficient diet resulted in a 12-pereent de-crease in BMD. which was reversed by the adminis-tration of vitamin K2 (30 mg/kg daily) within eightweeks."
Vitamin K2 in Bone Loss fromPrednisolone
Bone loss is one of the side effects of corti-eosteroid use in clinical practice. The damage stemsfrom a reduction in osteoblastic activity and bone for-mation.''** '̂' Application of prednisolone (3 or 30 mg/kg ) and vitamin K2 (15 mg/kg) for eight weeks com-pletely inhibited loss of BMD in trabecular bone, butthe data appears to indicate no effect of vitamin K2on loss of subcortical bone.* '̂ These results comparefavorably with earlier work on rats given predniso-lone (7 mg/kg/day) for nine weeks along with vitaminK2 (17 mg/kg/day). This combination significantlyinhibited the decrease in length, dry weight, and bonedensity of femurs and tibiae, and completely inhibit-ed decrease in urinary gamma-carboxyglutamic acid(Gla). Vitamin K2 (0.4, 10, and 50 mg/kg/day) sig-nificantly inhibited the reduction of calcium contentin the femur.""
Osteopenia Due to Over-expression ofGCSF
Transgenic mice (over-expressing granulo-cyte colony-stimulating factor [GCSF], which causesosteopenia and increased osteoclast number with ac-celeration of bone resorption) were given vitaminK2 at a dose of 0.05 mg/100 g feed (control group)or 20.0 mg/lOO g feed (experimental group) for 12weeks. The decreased bone mineralization was par-tially offset in the high vitamin-K group. Microcom-puted tomography den"ionstrated both cortical andtrabecular bone increase." '̂
Bone Loss due to PhenytoinThe anti-epileptic drug phenytoin has been
shown to induce bone loss,''- previously ascribed tophenytoin's interference with vitamin D metabolism.In rats, decreased BMD in both diaphysis and me-taphysis of femoral bones was thought to be due todecreased levels of vitamin K2 from administrationof phenytoin. Administration of vitamin K2 (30 mg/kg daily) prevented BMD reduction from phenytoin(20 mg/kg subcutaneously) over five weeks.*''
Human Studies with Vitamin K2A number of human trials have found vitamin
K2 effective in the treatment of osteoporosis (TableIj i.r.35,.16.64.65 jp ̂ fandomized, open-label study, 241osteoporotic women were given either 45 mg/day vi-tamin K2 and 150 mg elemental calcium (treatmentgroup; n=120) or 150 mg elemental calcium (con-trol group; n=121). After two years, vitamin K2 wasshown to maintain lumbar BMD. Patients receivingK2 also experienced significantly lower fracture inci-dence (10% versus 30%, in the treatment and controlgroups, respectively).^^ In a double-blind, placebo-controlled, 24-week study, 80 patients with osteopo-rosis received either 90 mg/day vitamin K2 or place-bo. Second metacarpal BMD was increased by 2.20± 2.48 percent compared to placebo, which decreasedby 7.31 ±3.65 percent.'"
Page 28 Alternative Medicine Review • Volume 10, Number 1 • 2005

Review Vitamin K / Osteoporosis
Vitamin K2 in Osteoporosis ofPostmenopausal Women
The incidence of osteoporosis is high in post-menopausal women. Anumber of trials have demon-strated vitamin K2 can induce significant reductionsin bone loss in postmenopausal osteoporotic women.In a controlled clinical trial. 172 osteoporotic/os-teopenic women (BMD < 0.98 g/cm-) were randomlyassigned to receive vitamin K2 (45 mg/day). 1-al-pha-hydroxycholecalciferol vitamin D3 (1 meg/day),both, or placebo for 24 months. Combination therapyresulted in a significant 4.92 ± 7.89 percent increasein BMD. while vitamin K2 alone resulted in only a0.135 ± 5.44 percent increase in BMD - higher, butnot statistically significantly higher, than baselinevalues. However, at 18- and 24-month evaluations.BMD was significantly higher in the K2 group com-pared to the control group. In this study, a combina-tion of vitamins K2 and D3 proved more protectivethan either supplement alone.-'
A longitudinal study of 17 postmenopausalwomen given vitamin K2 (45 mg/day) for one yearfound that K2 was able to suppress the decrease inspinal BMD, with a slight increase (0.23 ± 0.47%)compared to the control group of 19 postmenopausalwomen who experienced a decrease (-2.87 ± 0.51%)in BMD.'"'
Ninety-two postmenopausal women, ages55-81 years, were randomly assigned to one of fourgroups: vitamin K2 (45 mg/day).. 1-alpha-hydroxyvi-tamin 03 (0.75 meg/day), a combination of vita-mins K and D (same dosage as above), or calciumlactate (2 g/day). The vitamin-K and -D groups bothexperienced significant increases in BMD comparedto the calcium group over a two-year period, whilecombined treatment was synergistic. significantly in-creasing lumbar BMD by 1.35
Vitamin K2 and BisphosphonatesA number of bisphosphonates (e.g.. etidro-
nate, alendronate, and risedronate) are used in thetreatment of osteoporosis. These drugs, although gen-erally considered more effective than vitamin K inincreasing BMD. seem to work synergistically withit. A recent randomized, open-label study of 98 post-menopausal, osteoporotic women found significantlydecreased fracture rates in 23 subjects (2/23) taking
vitamin K2 (45 mg/day) and 25 subjects (2/25) takingetidronate (200 mg/day for two weeks every threemonths), compared to 24 subjects (6/24) taking calci-um lactate (2 g/day). The fracture rate was decreasedfurther in 26 subjects (1/26) taking a combination ofvitamin K2 and etidronate.''"
Alendronate (Fosamax®) encourages corti-cal bone growth by inducing apoptosis of osteoclasts.The infiuence of vitamin K2 on trabecular and corticalbone formation has been shown not to interfere withbisphosphonates and the apoptosis of osteoclasls. Infact, the authors conclude the combination of vitaminK2 and bisphosphonates could produce an additiveeffect in osteoporosis prevention.̂ ""
Vitamin K2 in Osteoporosis ofParkinson's Disease
Although as a general population the elderlyare at high risk for osteoporosis, Parkinson's diseasecompounds the risk. Research of elderly populationshas found a high incidence of hip fractures and os-teoporosis in Parkinson's patients,**"™ in part relatedto vitamin D deficiency" and immobilization^^ in thispopulation. The deficiency does not seem to be re-lated to lack of 25-hydroxyvitamin D3. but rather tosuppression of 1.25-dihydroxyvitamin D3 (the activeform of vitamin D) by high serum calcium. The appli-cation of vitamin K2 significantly increased 1,25-di-hydroxyvitamin D3 and decreased serum calcium.^-Vitamin K2 (45 mg/day for 12 months) to 54 femaleosteoporotic Parkinson's patients 65 years or olderresulted in one hip fracture, compared to 10 fractures(eight hip, one radius, one ankle) in 54 matched, un-treated, osteoporotic Parkinson's patients. All hipfractures were caused by falls and no significantdifferences were noted in number of falls betweengroups. The average bone loss in the untreated groupwas 4.3 ± 2.5 percent compared to 1.3 + 0.4 percentin age-matched controls. Vitamin K2-treated patientsexperienced a 0.9 ± 1.2 percent gain in BMD.'-
Vitamin K2 in Bone Loss fromLeuprolide
A moderate reduction in BMD is one of thefrequent side effects of the gonadotropin-reieasinghormone antagonist leuprolide for endometriosis,leiomyomas. and prostate cancer."''' Administration
Alternative Medicine Review • Volume 10, Number 1 • 2005 Page 29

Vitamin K / Osteoporosis Review
of vitamin K2 (45 mg/day; n=28) or the combinationof K2 and 1,25-dihydroxyvitamin D3 (45 mg/dayand 0.5 meg/day, respectively; n=28) resulted in par-tial prevention of bone loss compared to the leupro-lide-only group (n=28) or the vitamin D-only group(n=26). Bone loss after six months as measured bylumbar spine BMD was 5.25 percent in the leupro-lide-only group, 4.13 percent in the vitamin D group,3.72 percent in the vitamin K group, and 3.59 in thegroup taking vitamins K and D.'"
Vitamin K2 in Bone Loss fromPrednisolone
Use of glucocorticoids is the most commoncause of drug-induced secondary osteoporosis.^" Ad-ministration of glucocorticoids for long periods oftime can lead to a decrease in bone mineral density ofalmost four percent." Several studies found vitaminK2 has a marked effect on the loss of BMD in pred-nisolone-treated patients. Sixty patients with chronicglomerulonephritis were randomized to four groups:control. 1-alpha-hydroxyvitamin D3 (0.5 meg/day),vitamin K2 (45 mg/day), or vitamins K2 with D3. Pa-tients concomitantly received prednisolone at a dailydose of 0.7 mg/kg up to a maximum of 40 mg for fourweeks, then tapered to 25 mg daily for another fourweeks prior to assessment. The control group expe-rienced a significant decrease from baseline in BMDover the eight-week study: -3.19 ± 1.11 percent, com-pared to the vitamins D, K. and D+K groups thatmaintained baseline levels (0.28 ± 1.30. 0.50 ± 1.17,and 0.44 + 1.36 percent, respectively).'**
In a prospective pilot study 20 children be-ing treated with prednisolone and vitamin D3 (0.03mcg/kg/day) were continued on D3 plus prednisoloneor given that combination plus vitamin K2 (approxi-mately 2 mg/kg/day) for 12 weeks. Vitamins K2 andD3 combined had an additive effect, with a signifi-cant increase in lumbar BMD and osteocalcin com-pared to vitamin D3 alone.'''
Similar results were obtained in a random-ized, prospective, controlled study of 20 patients withglomeruionephritis given 0.8 nig/kg/day prednisoloneup to a maximum of 40 mg/day for four weeks, thentapered to 20 mg/day over a six-week period. Onegroup received only prednisolone. while a secondgroup also received vitamin K2 (15 mg three times
daily). After 10 weeks, a reduction in lumbar spineBMD (from 1.14 ± 0.12 to 1.10 ± 0.11 g/cw) wasnoted in the prednisolone-only group. The vitaminK2 group demonstrated a somewhat slower, rate ofbone loss (from 1.09 ± 0.09 to 1.07 ± 0.07 g/cm-)."
Vitamin K2 in the Treatment of BoneLoss in Biliary Cirrhosis
Patients with primary biliary cirrhosis expe-rience osteodystrophy and increased fracture rate andfat malabsorption that results in deficiencies of vita-mins D and K. Serum levels of vitamin K have beenfound to be low in this population. In a randomized,controlled trial of 27 patients with primary biliarycirrhosis, the treatment group (n=l4) received vita-min K2 (45 mg/day) for two years. After one year thecontrol group (n=I3) experienced a 3.5 ± 1.2 percentdecrease in BMD, while the vitamin K2 group dem-onstrated a 0.3 ± 2.3 percent increase in BMD. Aftertwo years, the control group demonstrated a 6.9 ± 2.1percent decrease in BMD, compared to only a 0.8 ±3.4 percent decrease in the K2 group. BMD was sig-nificantly higher in the vitamin K2 group during thetwo-year period compared to controls.**^
Vitamin K2 in the Treatment ofOsteopenia of Stroke Patients andSkeletal Unloading
Victims of stroke are often immobilized, lead-ing to significant loss of BMD. The most pronouncedloss of bone occurs on the hemiplegic side comparedto the unaffected side. This loss has been attributed toincreased bone resorption. immobilization-inducedhypercatcemia, and hypovitaminosis D. '̂ A recentrandomized, controlled trial of 108 hemiplegic strokevictims, 54 subjects treated with 45 mg vitamin K2daily for 12 months and 54 subjects serving as con-trols, found K2 effective for preventing disuse boneloss. Second metacarpal BMD on the hemiplegic sideincreased an average of 4.3 percent with vitamin K2and decreased an average of 4.7 percent with no treat-ment. The unaffected side had a 0.9-pcrcent decreasewith K2 treatment compared to 2.7-percent decreasewith no treatment.**"
Page 30 Alternative Medicine Review • Volume 10, Number 1 • 2005

Review Vitamin K / Osteoporosis
Table 1. Clinical Studies of Vitamin K for Osteoporosis
Condition
PostmenopausalOsteoporosis
Postmenopausal Osteoporosiswith Bisphosphonates
Parkinson'sDisease
Bone Loss from Leuprolide
Bone loss from Prednisolone
Bone Loss in Biliary Cirrhosis
Osteopenia from Stroke
Skeletal Unloading inA Bedridden Child
Osteoporosis of Anorexia
Intervention
45 mg/day K2
45 mg/day K2; 1 meg/day D3
45 mg/day K2; 0.75 meg/day D3
45 mg/day K2
45 mg/day K2
45 mg/day K2
15 mg K2 three times/day
45 mg/day K2;0.5 meg/day D3
2 mg/kg/day K2; 0.03mcg/kg/day D3 (Child Dose)
45 mg/day K2
45 mg/day K2
2 mg/kg/day K2;0.05 mcg/kg D3
45 mg/day K2
Outcome Reference
Inhibited decrease in 66BMD
Increased BMD 27
Increased BMD 65
Increased 68effectiveness of
bisphosphonates
Decreased fracture 72rate: increased BMD
Slowed decrease in 75BMD
Slowed rate of 77bone loss
Inhibited decrease 78in BMD
Increased lumbar 79BMD
Maintained BMD 80
Increased BMD 82
Increased BMD and 83Osteocalcin
Slowed rate 88of bone loss
Skeletal unloading is a serious consequenceof prolonged bedridden states leading to pathologicfractures. In a case of a bed-ridden, eight-year-oldgirl with low BMD. vitamin K2 at a dose of 2 mg/kg/day and vitamin D3 at a dose of 0.05 mcg/kg/dayfor 12 months resulted in an increase in osteocalcinlevels (from 8.2 to 27.9 ng/mL) and cortical BMD ofthe radius from 0.370 g/cnr to 0.420 g/cm-/'
Symptoms of skeletal unloading are also ob-served in astronauts, due to a microgravity environ-ment.^''Vitamin K2 (22 mg/kg) for four weeks to ratssubjected to tale suspension mimicking a micrograv-ity environment effectively prevented significant lossof BMD. Analysis revealed that volume and structureof trabecular bone were maintained.**^ An astronaut onthe EUROMIR-95 mission was tested durins the first
Alternative Medicine Review • Volume 10, Number 1 • 2005 Page 31
Vitamin K / Osteoporosis Review
part of a six-month space flight and found to haveincreased markers of bone loss. The astronaut wasgiven vitamin K(in this case, vitamin Kl)at adoseof10 mg/day for six weeks, resulting in increased mark-ers of bone formation - osteocalcin (14%) and bonealkaline phosphatase
Vitamin K2 in the Treatment ofOsteoporosis of Anorexia
Anorexia is an eating disorder associatedwith pronounced weight loss, osteopenia, and os-teoporosis that affects approximately one percent ofU.S. females.'̂ ' Twenty-one patients diagnosed withanorexia completed an 11-month study, during which10 patients were given vitamin K2 (45 mg/day) and11 chose not to and served as controls. The treatmentgroup experienced significantly slower decrease inBMD compared to controls (-2.8% versus -6.9%, re-spectively). Levels of gamma-carboxyglutamic acidosteocalcin also significantly increased in the treat-ment group compared to controls (128.6% versus28.3%, respectively).^^
ConclusionBone formation and bone loss involves a
complex array of nutrients and molecular signals.This article covers the influence of vitamin K (mostspecifically K2) on these processes as a separate anddistinct requirement from other nutrients. In vitrostudies show vitamin K2 is far more active than Kiin both bone formation and reduction of bone loss.-**Human studies demonstrate the potential of vitaminK2 as a strategic intervention for osteoporosis. Thistreatment is already in general use outside tbe UnitedStates.' at a typical dose of 45 mg daily.
Studies confirm the effectiveness of vitaminK2 for decreased BMD from a variety of cau.ses, in-cluding postmenopausal osteoporosis, Parkinson'sdisease, use of leuprolide or prednisolone. biliarycirrhosis, stroke inactivity, and anorexia. Few, if any.multiple vitamin and mineral supplements contain vi-tamin K2. The authors recommend it be more widelysupplemented as it has beneficial activity far beyondosteoporosis. Supplementation becomes even moreimportant for those with a tendency to lipid malab-sorption. A common cause of malabsorption is celiacdisease, which affects one in 266 persons.
A normal prothrombin time is not an indi-cation that enough vitamin K activity is present tomaintain bone osteocalcin activity. Moderately highdoses of vitamin K2 do not produce hypercoagulableor toxic states in humans, although the useof K2, likeany vitamin K. is contraindicated in people takingwarfarin (Coumadin®),
Considering the extensive application of vi-tamin K beyond blood coagulation - osteoporosis,anticancer therapy,-' pain reduction,'̂ " mitochondrialaspects," '̂ hepatitis C,'" and protection of sphingolip-ids''- - the vitamin Ks have been therapeutically un-derutilized.
References1. Asakura H. Myou S. Ontachl Y. et al. Vitamin K
administration to elderly patients with osteoporosisinduces no hemostatic activation, even in thosewith suspected vitamin K deficiency, Osteoporos/«/2001:12:996-1000.
2. Center JR. Nguyen TV. Schneider D. et al.Monatily after all major types of osteoporoticfracture in men and women: an observational study.Uxncet 1999:353:878-882.
3. Shepherd AJ. An overview of osteoporosis. AlternThcr Health Med 2004: lO:26-33:quiz 34,92.
4. Kenny AM. Joseph C. Taxel P, Prestwood KM.Osteoporosis In older men and women. Conn Med2003:67:481-486.
5. South-Paul JE. Osteoporosis: part I. Evaluationand assessment. Am Fam Phvsician 2()01;63:897-904.908.
6. South-Paul JE. Osteoporosis: part II.Nonpharmacologic and pharmacologic treatment.Am Fam Physician 2001:63:1121 -1128.
7. Rubin CD. Treatment considerations in themanagement of age-related osteoporosis. Am J MedSci 1999;318:I58-17O.
8. Gaby A. Preventiiif; and fiever.sinf> Osteoporosis.Every Woman's Essential Guide. Rockiin. CA:Prima Publications: 1994.
9. Fasano A. Catassi C. Current approaches todiagnosis and treatment of celiac disease:an evolving spectrum. Gastroenterology201)1:120:636-651.
10. Green PH. Jabri B. Coeliac disease. Lancet2003:362:383^391.
11. Maki M, Collin P. Coeliac disease. Lancei1997:349:1755-1759.
12. Moreno ML. Vazquez H. Mazure R. et al.Stratification of bone fracture risk in patientswith celiac disease. Clin Gastroenterol Hepatol2004:2:127-134.
Page 32 Alternative Medicine Review • Volume 10, Number 1 • 2005

Review Vitamin K / Osteoporosis
13. Booth SL, Mayer J. Warfarin use and fracture risk.Ntnr Rev 2{)a)\5H:2(h22.
14. Simon RR. Beaudin SM. Johnston M, el al. Long-term treatment with sodium warfarin results indecreased femoral bone strength and ^anceilousbone volume in rats. Thromh Res 2002; 105:353-358,
15. von Tirpitz C, Reinshagen M. Management ofosteoporosis in patients with gastrointestinaldiseases. EurJ Gastroenterol Hepatol2003; 15:869-876.
16. Bottaro G. Fichera A. Ricca O. et al. Effect of thetherapy with vitamin K on coagulation factorsin celiac disease in children, Pediatr Med Chir1986;8:551-554. [Article in Italian]
17. Rodesch P, Cadranel S. Winckler M. Loeb H.Hypovitaminosis K in coeliac disease. ActaPaediatr Bel^ 1976:29:123-124,
18. Shearer MJ. Mallinsnn CN, Webster GR. BarkhanP, Absorption of tritiated vitamin KI in patientswith fat matabsorption. Gttt 1970; 11:1063-1064.
19. Thomson RH. Naturally Occurring Quinones. NewYork. NY: Academic Press; 1971.
20. Davidson RT. Foley AL, Engelke JA. Suttie JW.Conversion of dietary phylloquinone to tissuemenaquinone-4 in rats is not dependent on gutbacleria. J Nutr 1998:128:220-223.
21. Thijssen HH. DrittiJ Reijnders MJ. VitaminK status in human tissues: tissue-specificaccumulation of phylkxiuinone and menaquinone-A.BrJNutr 1996:75:121-127.
22. Seegers WH. Bang NU. Blood Clottini-Enz\molog\\ New York. NY: Academic Press:1967.
23. Lamson DW. Piaza SM, The anticancer effects ofvitamin K. Attern Med Rev 2003:8:303-318.
24. Billeter M. Bolllger W, Martius C. Studies on thetransformation of the K vitamins given orally byexchange of side chains and the role of intestinalbacteria therein, Biochem Z 1964:340:290-303.I Article in German]
25. Budavari S, The Merck Index: .An Encyclopedia ofChemicals, Drugs, and Biotogicals. Rahway. NJ;Merck: 1989,
26. Taggart WV. Matschincr JT. Metabolism ofmenadione-6.7-3H in the rat. Biochemistry1969;8:114I-1I46.
27. UshiroyamaT. Ikeda A. Ueki M, Effect ofcontinuous combined therapy with vitamin K(2)and vitamin D(3) on bone mineral density andcoagulofibrinoiysis function in postmenopausalwomen. Mattmtas 2002:41:2! i-221.
28. Hauschka PV. Lian JB. Gallop PM, Directi dent iti cation of the calcium-binding amino acid,gamma-carboxyglutamate. in mineralized tissue,Proc Nati Acad Sci U S A l975;72:3925-3929.
29. Hara K, Akiyama Y, Nakamura T. et al. Theinhibitory effect of vitamin K2 (menatetrenone) onbone resorption may be related to its side chain.Bone 1995:16:179-184.
30. Price PA. Parthemore JG. Deftos LJ. Newbiochemical marker for bone metabolism.Measurement by radioimmunoassay of boneGLA protein in the plasma of normal subjectsand patients with bone di.sease, J Clin Invest1980:66:878-883,
31. Booth SL. Suttie JW. Dietary intake and adequacyof vitamin K, 7/V»/r 1998:128:785-788.
32. Binkley NC. Krueger DC. Engelke JA. et al.Vitamin K suppiementation reduces serumconcentrations of under-gamma-carboxyhitedosteocalcin in healthy young and elderly adults. AmJ Clin Nutr 2000:72:1523-1528.
33. Bitensky L, Hart JP Catterall A. et al. Circulatingvitamin K levels in patients with fractures. J BoneJoint Stirg Br 1988:70:663-664.
34. Akiyama Y, Hara K, Matsumoto A. et al.Comparison of intestinal absorption of vitaminK2 (menaquinone) homologues and theireffects on blood coagulation in rats withhypoprothrombinaemia. Biochem Pharmacol1995;49:I801-1807,
35. Shiraki M. Shiraki Y. Aoki C. Miura M, VitaminK2 (menatetrenone) effectively prevents fracturesand sustains lumbar bone mineral density inosteoporosis. J Bone Miner Res 2000:15:515-521,
36. Orimo H. Shiraki M. Tomita A. et al. Effects ofmenatetrenone on the bone and calcium metabolismin osteoporosis: a double-blind placebo-controlledstudy, J Bone Miner Metah 1998:16:106-112.
37. Ronden JE. Groenen-van Dooren MM. HornstraG. Vermeer C. Modulation of arterial thrombosistendency in rats by vitamin K and its side chains.Atherosclerosis 1997:132:61 -67.
38. Crowther MA. Donovan D. Harrison L. et al.Low-dose oral vitamin K reliably reverses over-anticoagulation due to warfarin. Thromh Haemost1998:79:1116-1118.
39. Yamaguchi M. Taguchi H. Gao YH. et al. Effect ofvitamin K2 (menaquinone-7) in fermented soybean(natto) on bone loss in ovariectomized rats. J BoneMiner Metah 1999:17:23-29.
40. Koshihara Y. Hoshi K. Ishibashi H. Shiraki M.Vitamin K2 promotes lalpha.25(OH)2 vitaminD3-induced mineralization in human periostealosteoblasts. Calcif Tissue Int I996;59:466-473.
41. Koshihara Y, Hoshi K. Vitamin K2 enhancesosteocalcin accumulation in the extracellular matrixof human osteoblasts //; vitro. J Bone Miner Res1997:! 2:431-438.
Alternative Medicine Review • Volume 10, Number 1 • 2005 Page 33

Vitamin K / Osteoporosis Review
42. Akiyama Y. Hara K. Tajima T. et al. Effect ofvitamin K2 (menatetrenone) on osteoclast-like cellfonnation in mouse bone marrow cultures, Ei/r JPharmacol 1994:263:18M 85.
43. Hara K. Akiyama Y, Tajima T, Shiraki M.Menatetrenone inhibits bone resorption partlythrough inhibition of PGE2 synthesis in vitro. JBone^Miner Res 1993:8:535-542.
44. Hiruma Y. Nakahama K. Fujita H. Morita I.Vitamin K2 and geranylgeraniol. its side chaincomponent, inhibited osteoclast formation In adifferent manner. Biochem Bioplns Res Commun2004:314:24-30.
45. Koshihara Y, Hoshi K. Okawara R. et at. VitaminK stimulates osteoblastogenesis and Inhibitsosteoclastogenesis in human bone marrow cellQn\me. J Endocrlnol 2003:176:339-348.
46. Akiyama Y. Hara K. Kobayashi M. ct al.Inhibitory effect of vitamin K2 (menatetrenone)on bone resorption in ovariectomized rats:a histomorphometric and dual energy X-ray absorptiometric study. Jpn J Pharmacol1999:80:67-74.
47. Sato T. Ohtani Y. Yamada Y. et al. Difference in themetabolism of vitamin K between liver and bonein vitamin K-deficient rats. B/JM///2002:87:307-314.
48. Iwamoto J. Yeh JK. Takcda T. Effect ofvitamin K2 on cortical and cancellous bones inorchidectomized and/or sciatic neurectomized rats,J Bone Miner Res 2003:18:776-783,
49. Iwasaki Y. Yamato H, Murayama H. et al.Menatetrenone prevents osteoblast dysfunctionin unilateral sciatic neurectomized rats, Jpn JPharmacol 2002:9Q:SH-93.
50. Hara K. Akiyama Y. Ohkawa I. Tajima T. Effects ofmenatetrenone on prednisolone-induced bone loss'mniis.Bone 1993:14:813-818.
51. Mawatari T. Miura H. Higaki H.et al. Effectof vitamin K2 on three-dimensional trabecularmicroarchitecture in ovariectomized rats, J BoneMiner Res 2000:15:1810-1817,
52. Shiraishi A. Higashi S. Masaki T. ct al, Acomparison of alfacalcidol and menatetrenone forthe treatment of bone loss in an ovariectomizedrat model of osteoporosis. Calcif Tissue Int2002:71:69-79.
53. Binkley N. Krueger D. Engelke J. et al. VitaminK supplementation does not affect ovariectomy-induced bone loss in rats. Bone 2002:30:897-900,
54. Akiyama Y. Hara K. Ohkawa 1. Tajima T. Effectsof menatetrenone on bone loss induced byovariectomy in rats. Jpn J Pharmacol 1993:62:145-153.
55. Hara K. Kobayashi M. Akiyama Y Effect ofcombined treatment with vitamin K2 and I alpha-(OH)-vitamin D3 on bone loss in ovariectomizedrats. Nippon Yaktirigaku Zasshi 2001:118:231-240.[Article in Japanese]
56. Iwamoto i. Takeda T. Yeh JK. et al. Effect ofvitamin K2 on cortical and cancellous bones inorchidectomized young rats. Maturitas 2003:44:19-27,
57. Kato S. Mano T. Kobayashi T. et al, A calcium-deficient diet caused decreased bone mineraldensity and secondary elevation of estrogen in agedmale rats - effect of menatetrenone and elcatonin.Metabolism 2002:51:1230-1234,
58. Meunier PJ. Dempster DW. Edouard C. ct al.Bone histomorphometry in corticosteroid-inducedosteoporosis and Cushine's syndrome. Adv ExpMed Biol 1984:171:191-2(M}.
59. Jowsey J. Riggs BL. Bone formation inhypercortisonism, Acta Endocrinol (Copenh)1970:63:21-28,
60. Hara K. Kobayashi M, Akiyama Y Vitamin K2(menatetrenone) inhibits bone loss induced byprednisolone partly through enhancement of boneformation in rats. Bone 2002:31:575-581,
61. Kokai Y. Wada T. Oda T. et al. Overexpressionof granuiocyte colony-stimulating factor inducessevere osteopenia in developing mice that ispartially prevented by a diet containing vitamin K2(menatetrenone). Bone 2002:30:880-885.
62. Valimaki MJ. Tiihonen M. Laitinen K, et al.Bone mineral density measured by dual-energyx-ray absorptiometry and novel markers of boneformation and resorption in patients on antiepilepticdrugs. J Bone Miner Res 1994:9:631 -637.
63. Onodera K. Takahashi A. Wakabayashi H. et al.Effects of menatetrenone on the bone and serumlevels of vitamin K2 (menaquinone derivatives) inosteopenia induced by phenytoin in growing rats.Nutrition 2003:19:446-450.
64. Orimo H. Shiraki M. Fiujita T. et al. Clinicalevaluation of menatetrenone in the treatmentof involutional osteoporosis: a double-blindmulticenter comparative study with l-alpha-dihydroxyvitamin D3, J Bone Miner Res 1992:7:SI 22,
65. Iwamoto J. Takeda T. Ichimura S. Effect ofcombined administration of vitamin D3 and vitaminK2 on bone mineral density of the lumbar spinein postmenopausal women with osteoporosis. JO///W/7 .SW 2000:5:546-55 i.
66. Iwamoto I. Kosha S. Noguchi S. et al. Alongitudinal study of the effect of vitamin K2 onbone mineral density in postmenopausal women acomparative study with vitamin D3 and estrogen-progestin therapy. Maturitas 1999:31:161-164.
Page 34 Alternative Medicine Review • Volume 10, Number 1 • 2005

Review Vitamin K / Osteoporosis
67.
68.
69.
70.
71.
72.
73.
74.
75.
76.
77.
78.
79.
Iwamoto J. Takeda T. Ichimura S. Treatment withvitamin D3 and/or vitamin K2 tor postmenopausalosteoporosis. KeioJ Med 2{K»3:52: \41-\f^i).Iwamoto J. Takeda T. Ichimura S. Combinedtreatment wiih vitamin K2 and bisphosphonate Inpostmenopausal women with osteoporosis. Yonsei
Johnell O. Melton LJ 3rd. Atkinson EJ. et al.Fracture risk in patients with parkinsonism:a population-based study in Olmsted County,Minnesota. Ai.'t'Ai,'':'"'.',' 1992:21:32-38.Kao CH. Chen CC. Wang SJ. et al. Bone mineraldensity in patients with Parklnst)n"s diseasemeasured by dual photon absorptiometry. Nucl MedCommtm 1994; 15; 173-177.Sato Y. Kikuyama M, Oizumi K. High prevalenceof vitamin D deficiency and reduced bone massin Parkinson's disease. Neurology I997;49:1273-1278.Salo Y. Honda Y. Kaji M. et al. Amelioration ofosteoporosis by menatetrenone in elderly femaleParkinson's disease patients with vitamin Ddeficiency. Bone 2002;31:l 14-118.Smith MR. MeGovem FJ. Zietman AL. et al.Pamidronate to prevent bone loss during androgen-deprivation therapy for prostate cancer. N Engl JMed 2(M)1:345:948-935.Dawson-Hughes B. Bone loss accompanyingmedical therapies. N Engl J Med 2{K)I ;345:989-991.Somekawa Y. ChigughJ M. Harada M, IshibashiT. Useof vitamin K2 (menatetrenone) and 1,25-dihydroxyvitamin D3 in the prevention of bone lossinduced by leuproiide. J Clin Fmlocrlnol Metab1999:84:2700-2704.Rehman Q. l^ne NE. Effeel of glueoeorticoids onbone density. Med Pediatr Onrol 2003:41:212-216.Yonemura K. Kimura M. Miyaji T. Hishida A.Short-term effect cif vitamin K administration onprednisolone-induced loss of bone mineral densityin patients with chronic glomerulonephritis. CalcifT/Jfjuf-Zm 2000:66:123-128.Yonemura K. Fukasawa H. Fujigaki Y. HishidaA. Protective effect of vitamins K2 and D3 onprednisolone-indueed loss of bone mineral densityin the lumbar spine. Am J Kidnex Dis 2004:43:53-60.Inoue T. Sugiyama T. Matsubara T. et al. Inversecorrelation between the changes of lumbar lx>nemineral density and serum undercarboxylatedosteocalcin after vitamin K2 i menatetrenone)treatment in children treated with tjlucoeorticoidand alfacaleidol. Endocr J 2001 ;48:11-18.
80. Nishiguchi S. Shimoi S, Kurooka H, et al.Randomized pilot trial of vitamin K2 for bone lossin patients with primary biliary cirrhosis. J Hepatol2(M) 1:35:543-545.
81. Sato Y. Kuno H, Kaji M, et al. Increased boneresorption during the first year after stroke. Stroke1998:29:1373-1377.
82. Sato Y. Honda Y. Kuno H, Oizumi K.Menatetrenone ameliorates osteopenia in disuse-affected limbs of vitamin D- and K-deficient strokepatients. Bone 1998:23:291-296.
83. Sugiyama T. Tanaka H, Kawai S. Clinical vignette.Vitamin K plus vitamin I) treatment of lx>neproblems in a child with skeletal unloading. J BoneMiner Res 1999:14:1466-1467.
84. Vermeer C. Ulrich MM. The effeet of microgravityon plasmaHisteoealcin. Adv Space Res I986;6:I39-142.
85. Iwasaki Y, Yamato H. Murayama H, et al.Maintenance of trabecular structure and bonevolume by vitamin K(2) in mature rats withlong-term tail suspension. J Bone Miner Metab2(X)2:20:2l6-222.
86. Vermeer C, Wolf J. Craciun AM, Knajjen MH.Bone markers during a 6-month space Ilight: effectsof vitamin K supplementation. J Gravit Phx.siol1998,5:65-69.
87. Schneider M. Fisher M, Weinerman S. LesserM. Correlates of low bone density in femaleswith anorexia nervosa. //// J Adolesc Med Health2002:14:297-306.
88. Iketani T. Kiriike N. Murray, et al. Effect ofmenatetrenone (vitamin K2) treatment on bone lossin patients with anorexia nervosa. Psxchiatrv Res2(X)3:117:259-269.
89. Kubovic M. Prazic M, Atanaekovic D. Analgeticproperty of vitamin K. Proc Soc Exp Biol Med1955:90:660-662.
90. Plaza SM, Lamson DW. Mitoebondrial aspects ofvitamin K. Article in preparation.
91. Habu D. Shiomi S. Tamori A.et al. Role of vitaminK2 in the development of hepatoeellular carcinomain women with viral cirrhosis of the liver. JAMA2004:292:358-361.
92. Plaza SM. Lamson DW. Vitamin K in myelinmetabolism. Article in preparation.
Alternative Medicine Review • Volume 10, Number 1 • 2005 Page 35