Connecting to the Hispanic/Latino Community: Essential Elements for Quality Care Eduardo R. Ochoa,...
34
Connecting to the Hispanic/Latino Community: Essential Elements for Quality Care Eduardo R. Ochoa, Jr., M.D. Assistant Professor General Pediatrics, Maternal Child Health UAMS Colleges of Medicine and Public Health
-
Upload
todd-french -
Category
Documents
-
view
214 -
download
0
Transcript of Connecting to the Hispanic/Latino Community: Essential Elements for Quality Care Eduardo R. Ochoa,...

Connecting to the Hispanic/Latino Community:Essential Elements for Quality Care
Eduardo R. Ochoa, Jr., M.D.Assistant Professor
General Pediatrics, Maternal Child HealthUAMS Colleges of Medicine and Public Health

Overview
Introduction Culture and its Role Environmental Landscape Impact on Health and Health Care The Culturally Competent Encounter Connection to Disparities
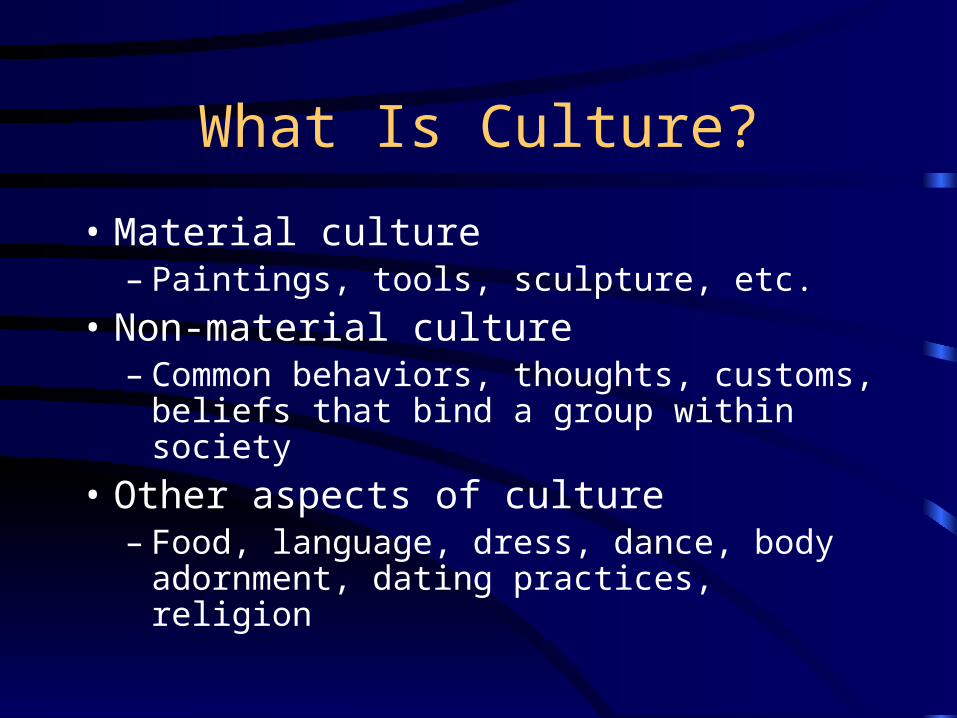
What Is Culture?
• Material culture– Paintings, tools, sculpture, etc.
• Non-material culture– Common behaviors, thoughts, customs,
beliefs that bind a group within society
• Other aspects of culture– Food, language, dress, dance, body
adornment, dating practices, religion

Culture in the Health Arena
• Every patient-provider interaction is a cross-cultural experience– The provider must have comfort with his or
her own cultural background– The patient brings a set of cultural values
that will uniquely impact his or her health– Bridging the cultural divide is the essence
of a quality encounter

Cultural Competence
• Describes the system meeting the client
• “The set of behaviors, attitudes and policies that come together in an institution, agency, or among a group of individuals, that allows them to work effectively in cross-cultural situations.”
– Cross, TL, BJ Bazron, KW Dennis, and MR Isaacs. “The Cultural Competence Continuum”

Cultural Competence
• “…the ability of systems to provide care to patients with diverse values, beliefs and behaviors, including tailoring delivery to meet patients’ social, cultural, and linguistic needs.”
– JR Betancourt, AR Green and JE Carrillo, “Cultural Competence in Health Care: Emerging Frameworks and Practical Approaches”, The Commonwealth Fund, October 2002.

Value of Cultural Competence
• Vehicle to achieve better access to care
• Strategy to attract new patients
• Vehicle to reduce racial and ethnic disparities in outcomes and quality
• Better understanding of the consumer
• Part of an organizational strategy to address barriers to quality care

Environmental LandscapeUS Population
Census 2000
75
12.3
12.5
5.53.6 0.11
White Afr-Am LatinoAI/AN Asian H/PIOther
1990
80
12
9
7.92.9 3.9

US Demographic Projection
• Children’s Defense Fund 2030 Predictions– 5.5 million more Hispanic children
– 2.6 million more African-American children
– 1.5 million more children of other races
– 6.2 million fewer white, non-Hispanic children
Hanson MJ: “Ethnic, Cultural, and Language Diversity in Intervention Settings,” in Developing Cross-Cultural Competence: A Guide for Working with Young Children and Their Families, eds, EW Lynch, MJ Hanson, Baltimore MD: Paul H. Brookes Publishing Company, 1992, p.7.

Environmental LandscapeArkansas Population
• Race/Ethnicity 1990 2000– White 82.7 80– African-American 15.9 15.7– Hispanic 0.8 3.2– Other 1.3 3.1
• Includes Asian, American Indian, Pacific Islander
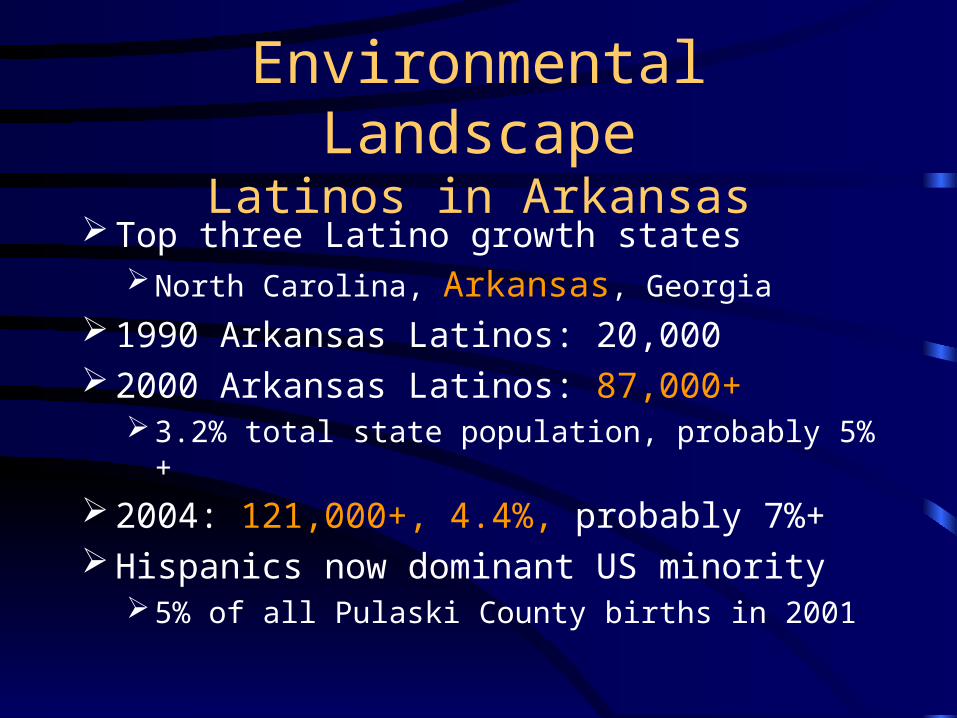
Environmental LandscapeLatinos in Arkansas
Top three Latino growth statesNorth Carolina, Arkansas, Georgia
1990 Arkansas Latinos: 20,000 2000 Arkansas Latinos: 87,000+
3.2% total state population, probably 5%+
2004: 121,000+, 4.4%, probably 7%+ Hispanics now dominant US minority
5% of all Pulaski County births in 2001

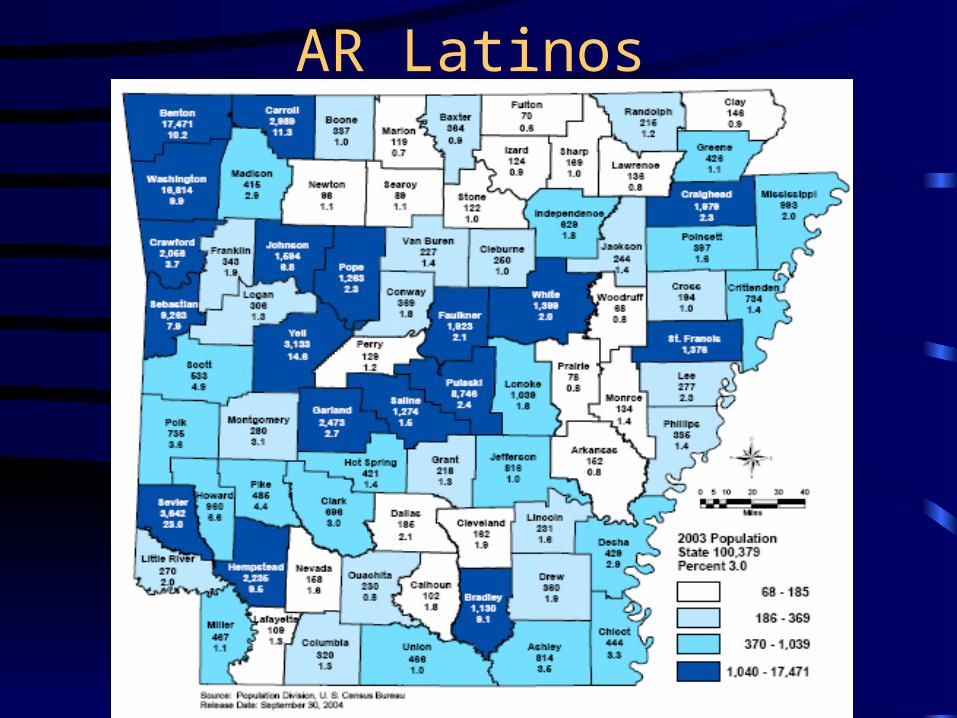
AR Latinos

Environmental LandscapeWhy Latinos Come to Arkansas
Economic opportunityRelative wage boom, available low-skill jobs
Poultry, agriculture, construction, service, factory/manufacturing
Social factorsArkansas contacts, perception of safety
“American dream” factorHome ownership, family growth, education

Environmental LandscapePublic Schools
Microcosm of state situationAll issues intersect: poverty, health,
immigration, hunger, housing
Explosion of language minority students’93-’94: 4,071; ’03-’04: 23,626 480%
5.2% K-12 studs,80% Spanish-speaking3/4 of Limited English Proficiency

Impact on Health
Barriers to health and health care accessLanguage, language, languageLack of knowledge about care systemsImmigration factorsPoverty, educational attainmentProvider workforce insufficiencyAlternative vs. Traditional US systemLack of health insurance

Impact on Health CarePublic Health
• Of all patients served by ADH, 8.2% Latino in 2001
• 50% of ADH clientele in Sevier county (DeQueen) and >30% in Benton and Washington counties Latino in 2001
• WIC, prenatal, immunization services highly utilized
• Partnerships formed to deliver services

Impact on Healthcare
• US public and private health workforce– US 15% Latino, 3.5% US MDs Latino– CA 31% Latino, 4% CA MDs Latino– 6.1% 2001 Med School Graduates Latino
• 7% African American (13% US population)
– 3.2% 2000 medical school faculty Latino– 1.9% UAMS COM Latino faculty– Largely without culture or language training

Impact on Healthcare
• Language– 39% of Spanish-speaking adults speak
English “not well” or “not at all”– Inability to cross language barrier affects
all health and social service delivery– Agencies have few, if any, bilingual staff– Federal mandate to improve service to LEP
persons-Executive Order 13166

Impact on Health

Impact on HealthNew Immigrants
• Unfamiliar US care systems– Not accustomed to making appointments– Difficult to navigate large medical centers– Little help available in Spanish– Unsure how to apply for, use and renew
health insurance– Not accustomed to preventive care,
screenings, disease surveillance

Impact on Health and Healthcare
• Immigration Issues– Many mixed status and separated families– 1996 welfare reform laws bar even
documented from benefits for 5 years– No documents=Invisible=Vulnerable– Fear of being asked for documents– Mobility across border– Possible comprehensive reform

Immigration
Impact on Health
• Traditional methods of care– Herbal remedies– Alternative caregivers
• curanderas, parteras, sobadoras, hierbistas
– Availability of prescription drugs– Family-centered decisions about health– Cultural beliefs about health and disease
• “sugar” vs. diabetes, etc.

Culturally Competent Encounter
• Country of origin-not all from Mexico– Reasons for leaving native country
• First or native language
• Education attained, literacy issues– Informed consent issues
• Religion-not all Catholic– End of life considerations

Latino Cultural Concepts
• La Familia-The Family, Gender roles
• Respeto-Respect– Social modesty; sensitivity in HC encounter
• Confianza-Confidence
• Personalismo-Personal Familiarity
• Spiritual Impact-role of faith and religion– Fatalismo, espiritismo

Latino Cultural Concepts
• Other beliefs about disease– Empacho, Bilis– Mal Ojo– Envidia – Mal Aire
• Traditional Healers
• Non-licensed providers

The Culturally Competent Encounter
• National Standards for Culturally and Linguistically Appropriate Services in Health Care– HHS Office of Minority Health, March 2001– 14 standards organized by themes
• Culturally Competent Care, Language Access Services, Organizational Supports for Cultural Competence

The Culturally Competent Encounter
• Realms for cultural competence– Organizational
• Minority leadership recruitment, development, promotion; community involvement
– Systemic• Community assessment, data collection, quality
– Clinical• Awareness of sociocultural influences, training
of staff, patient empowerment

The Culturally Competent Encounter
• Understand community or client being served and what social and cultural influences impact health and behavior
• Understand how these factors interact with the system in ways that prevent quality care access
• Identify barriers and intervene• Monitor outcomes

The Culturally Competent Encounter
• Avoid stereotyping – Vast heterogeneity among racial and
ethnic subgroups• Differences by national origin, educational
attainment, socioeconomics, religion
• Engage in dialogue– Linguistically appropriate communication
and negotiation is the key

Connection to Disparities
• Access to health information, services
• Language access
• Quality measurements, data collection
• Workforce education
• Community education
• Systems change

Connection to DisparitiesCurrent Efforts
• Community– La Casa Health Network– Community Health Center expansion
• Multi-partner effort: ADHHS, JCCSI, ACH, Baptist Health, La Casa, LULAC, Pulaski County, City of LR
• UAMS– Chancellor’s Racial and Ethnic Health
Disparities Taskforce