Compounded Medicinal Cannabis€¦ · terpenes in cannabis are also reported to influence either...
12
Compounded Medicinal Cannabis PROFESSIONAL REFERENCE ONLY. PUBLISHED NOV CONTENTS Foreword ......................................................................................................... 2 Access to Compounded Medicinal Cannabis.................................... 2 The Compounding Access Pathway ..................................................... 3 Legal Access Pathway................................................................................ 4 Medicinal Cannabis ..................................................................................... 4 The Endocannabinoid System ................................................................ 5 Clinical Pharmacology................................................................................ 6 Potential Therapeutic Applications ....................................................... 7 Other Potential Therapeutic Applications .......................................... 8 Dosage ........................................................................................................ 8-9 Precautions and Warnings ..................................................................... 10 References.....................................................................................................11
Transcript of Compounded Medicinal Cannabis€¦ · terpenes in cannabis are also reported to influence either...

CompoundedMedicinal CannabisPROFESSIONAL REFERENCE ONLY. PUBLISHED NOV!"#$%
CONTENTS
Foreword .........................................................................................................2
Access to Compounded Medicinal Cannabis ....................................2
The Compounding Access Pathway .....................................................3
Legal Access Pathway................................................................................4
Medicinal Cannabis .....................................................................................4
The Endocannabinoid System ................................................................5
Clinical Pharmacology ................................................................................6
Potential Therapeutic Applications ....................................................... 7
Other Potential Therapeutic Applications ..........................................8
Dosage ........................................................................................................ 8-9
Precautions and Warnings .....................................................................10
References .....................................................................................................11

PAGE 2 GREEN DISPENSARY COMPOUNDING: COMPOUNDED MEDICINAL CANNABIS FOR PROFESSIONAL REFERENCE ONLY
FOREWORD
New legislation introduced in Australia in 2016 brought some key amendments to the federal Narcotic Drugs Act 1967 to decriminalise the use and supply of medicinal cannabis. The Therapeutic Goods Administration (TGA) in 2017 went on to reschedule certain medicinal cannabis products to schedule 8 of the Poisons Standard, making the prescription of medicinal cannabis legal in Australia. This was later rescheduled again to allow certain products to be classified as Schedule 4 medicines.
Since these changes, Australians have been seeking both knowledge and access to medicinal cannabis, driven by ine!ectiveness of existing pharmaceutical treatments or compromised quality of life due to their side e!ects. The increase in demand for medicinal cannabis is still being significantly accommodated by the black market due to reported di"culties in facing the legal and bureaucratic barriers in place in every phase of the supply chain.
This document serves to provide an update of the legislation around current patient access to prescription medicinal cannabis products in Australia. Additionally, it provides an overview of the pharmacology, potential therapeutic applications and prescribing information for the major cannabinoids CBD and THC, found in medicinal cannabis. Although these updates are recent, they serve to enable more Australian patients an equitable, e"cient, and a!ordable means to have access to medicinal cannabis.
ACCESS TO COMPOUNDED MEDICINAL CANNABIS IN AUSTRALIA
In 2017, the TGA listed the cannabinoids THC and CBD in the Poisons Standard allowing medicinal cannabis to be prescribed by any medical practitioner in accordance with applicable federal and state laws.
Schedule 4 Cannabidiol Products (CBD)Products containing CBD with less than 2% of other cannabinoids including THC are classified as Schedule 4 (Prescription Only Medicines) which are substances that should only be used or supplied on the order of a prescriber (eg a medical practitioner) and available from a pharmacist on prescription.
Schedule 8 Delta-9-Tetrahydrocannabinol Products (THC) Products containing greater than 2% of other cannabinoids including THC are classified as Schedule 8 (Controlled drugs or drugs of dependence) which are substances that need to be available for use but manufacture, supply, possession and use need to be restricted to reduce abuse, misuse and dependence. Therefore, like all other S8 prescriptions, medical practitioners may need to apply for state or territory approvals as applicable to them.
In South Australia as an example, the prescription and supply of Schedule 8 medicines is regulated under section 18A of the Controlled Substances Act 1984. A Section 18A authority is required after 2 months of treatment or before commencing treatments where the person is already prescribed a Schedule 8 drug (for a period exceeding 2 months) and for any person the medical practitioner reasonably believes to be dependent on drugs. Some exemptions do apply, for example a Section 18A authority is not required for patients aged 70 years or older.
THE COMPOUNDING ACCESS PATHWAY
The Therapeutic Goods Regulation 1990 was updated in December 2017 to remove the restriction which prohibited pharmacists from compounding cannabinoid medicines. Since a pharmacist is not manufacturing a commercial unregistered product, TGA does not examine individual products produced by pharmacists on prescription order from medical practitioners. This jurisdiction lies with the Pharmacy Board of Australia.
This new update to the improved accessibility of cannabinoid medicines provides medical practitioners with an alternative prescribing pathway which is lawful and provides patients with a tailored approach to cannabinoid medicines. This is important because manufactured products do not address tailoring and customisations treatments.
COMPOUNDING QUALITY STANDARDS
Compounded cannabis products, still need to comply to the current medicinal cannabis quality standards (Therapeutic Goods Order 93 and 100). This ensures that the starting material used in preparing the medicine is free of moulds, pesticides, heavy metals, and is tested for cannabinoid content and foreign matter. Compounding pharmacies have strict compounding guidelines that need to be adhered to for the production of high quality and safe medicines for patients. Cannabinoid medicines prepared by experienced and specialist compounding pharmacies should comply with the TGA’s medicinal cannabis quality standards (Therapeutic Goods Order 93 and 100).

FOR PROFESSIONAL REFERENCE ONLY PAGE 3GREEN DISPENSARY COMPOUNDING: COMPOUNDED MEDICINAL CANNABIS
During treatment with medicinal cannabis, a trial period may be set up between the doctor and patient to closely monitor the patient for responsiveness to treatment, risk management processes, and further investigations as required.
STEP &: MONITORING AND REVIEW (&!$" WEEKS)
During treatment with medicinal cannabis, a trial period may be set up between the doctor and patient to closely monitor the patient for responsiveness to treatment, risk management processes, and further investigations as required.
STEP &: MONITORING AND REVIEW (&!$" WEEKS)
The patient’s prescription is prepared and dispensed directly to the patient by a specialist compounding pharmacy.
STEP ': PRESCRIPTION PREPARATION
The patient’s prescription is prepared and dispensed directly to the patient by a specialist compounding pharmacy.
STEP ': PRESCRIPTION PREPARATION
ACCESS TO COMPOUNDED CANNABIDIOL (CBD ! SCHEDULE &)
ACCESS TO COMPOUNDED DELTA!%!TETRAHYDROCANNABINOL (THC ( SCHEDULE ))
THE COMPOUNDING ACCESS PATHWAY
Products containing greater than 2% of other cannabinoids including THC in the formulation, are classified as Schedule 8 medicines, and require further state health department approval. Check with individual state laws for prescribing Schedule 8 medicines in your state.
STEP "a: WRITTEN PRESCRIPTION
Products containing pure CBD or CBD with less than 2% of other cannabinoids are classified as Schedule 4 medicines (prescription-only) and can be supplied upon presentation of a standard prescription.
STEP "a: WRITTEN PRESCRIPTION
Complete relevant state health department approval or application processes for the THC prescription.
STEP "b: WRITTEN PRESCRIPTION
STEP ": WRITTEN PRESCRIPTION
A prescription is written identifying the formulation strength and dosage suitable for the patient’s health condition. (This is where an experienced, specialist compounding pharmacy can provide guidance and support.)
STEP ": WRITTEN PRESCRIPTION
A prescription is written identifying the formulation strength and dosage suitable for the patient’s health condition. (This is where an experienced, specialist compounding pharmacy can provide guidance and support.)
A clinical decision to prescribe a compounded medicinal cannabis product is made between medical practitioner and patient, documented, and patient consent provided.
STEP $: CLINICAL DECISION

PAGE 4 GREEN DISPENSARY COMPOUNDING: COMPOUNDED MEDICINAL CANNABIS FOR PROFESSIONAL REFERENCE ONLY
ALL LEGAL ACCESS PATHWAYS FOR MEDICINAL CANNABIS
Prior to December 2017, only the first three pathways allowed for the supply of unregistered cannabis products in Australia. The emergence of the compounding pathway is now another lawful means of access for doctors and patients for medicinal cannabis in Australia where it is deemed an appropriate treatment option. Therefore, the five access pathways for medicinal cannabis are now:
• Special Access Scheme (SAS-A/B/C) Schedule 5A Subregulation 12 (1A) Item 1 and 1A This scheme allows sponsors to access or import unregistered goods when the medication is not currently approved or available in Australia, when the patient has utilized all available medical treatments or when a prescriber decides to treat a patient with an unregistered medicine.
• Authorised Prescriber Schedule 5A Subregulation 12(1A) Item 1 and 1A Where a medical professional is treating a number of patients with similar disease states, they can apply for Authorised Prescriber status to bypass the requirement for individual applications to be made for each patient through the Special Access Scheme.
• Clinical Trial Schedule 5A Subregulation 12 (1A) Item 3 This scheme exists for clinical testing of new drugs in a controlled environment and requires TGA/Ethics approval.
• Contract Manufacturing Schedule 5A Subregulation 12 (1A) Item 5 This scheme allows a GMP licensed manufacturer to make batches of unregistered goods for a group of patients for a particular hospital under contract; the goods produced cannot be identical to a registered ARTG product.
• Extemporaneous Compounding Schedule 5 Subregulation 12 (1) Item 6 This scheme is allows a pharmacist who is exempt from holding a manufacturing license to prepare and dispense any scheduled medicine on prescription from a medical practitioner for a specific patient.
MEDICINAL CANNABIS
What is Medicinal Cannabis?Medicinal cannabis is any pharmaceutical-grade medicine derived from the Cannabis Sativa plant used to treat or relieve a symptom, ailment or condition. Pharmaceutical-grade medicines must contain raw materials sourced from licensed manufacturers compliant to TGO93. TGO93 is a therapeutic goods standard developed by the TGA that specifies minimum quality requirements for medicinal cannabis products, and ensure sources are rigorously tested for contaminants like bacteria, fungi, pesticides and heavy metals, and standardised for active constituents.
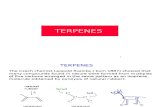
Phytocannabinoids and other active constituents in medicinal cannabisWhilst there are more than 100 di!erent phytocannabinoids found in cannabis plants, the principle and most widely studied for their potential benefits in humans are delta-9-tetrahydrocannabinol (THC) and cannabidiol (CBD). In spite of structural variances between the phytocannabinoids and the endogenous cannabinoids, similar interactions have been observed within the endocannabinoid system owing to their medicinal properties. Cannabis contains over 400 di!erent chemical constituents including a class of volatile compounds known as terpenes. Classically attributed to providing the characteristic flavor and fragrance of cannabis, the primary terpenes in cannabis are also reported to influence either the pharmacodynamics or pharmacokinetics of CBD and THC producing what is known as the “entourage e!ect”. It is reported that their inclusion in medicinal cannabis preparations may enhance the overall benefits of the primary phytocannabinoids.
Fig.1: Chemical Structure of THC Fig.2: Chemical Structure of CBD
CH3
CH3
H3C
H3C
OH
O
CH3
CH3
H3C
H3C
OH
HO

FOR PROFESSIONAL REFERENCE ONLY PAGE 5GREEN DISPENSARY COMPOUNDING: COMPOUNDED MEDICINAL CANNABIS
THE ENDOCANNABINOID SYSTEM
The Endocannabinoid System (ECS) is an ancient and evolutionarily conserved lipid-signalling system involved in a host of homeostatic functions and regulates many physiologic functions including gastrointestinal (GI) function, appetite and metabolism, pain, memory, movement, immunity, and inflammation. The ECS consists of the endogenous cannabinoids (endocannabinoids), cannabinoid receptors and the enzymes that synthesise and degrade the endocannabinoids. The receptors have distinct expression profiles, with CB1 receptors found principally (but not exclusively) at presynaptic sites throughout the peripheral and central nervous systems whilst CB2 receptors are found principally (but not exclusively) on immune cells. The endocannabinoid ligands are lipid neurotransmitters belonging to either the N-acyl ethanolamine (NAEs) class, e.g. anandamide (AEA), or the monoacylglycerol class (MAG), e.g. 2-arachidonoyl glycerol (2-AG). Both classes are short-acting transmitter substances, synthesised on demand with signalling rapidly terminated by specific enzymes. Anandamide is a partial agonist at both receptors with slightly higher a"nity for CB1 whilst 2-AG binds equally well to both. Binding at CB1 regulates neurotransmission throughout the nervous system, whilst binding at CB2 regulates the activity of immune cells giving rise to complex modulatory e!ects on immune function.
Fig.3: The Endocannabinoid System in the Nervous System (Ref: Health Canada)
Distribution of CB1 and CB2 ReceptorsCB1 receptors are abundant within the brain and spinal cord particularly within the basal ganglia, cerebellum, hippocampus and pre-synaptically on sympathetic nerve terminals, reflecting the importance of the endocannabinoid system in motor control, memory processing and pain modulation. CB2 receptors are predominant within the cells and tissues of the immune system such as the spleen and leukocytes, immune cells within the nervous system such as the microglia, and within the peripheral nervous system. To a lesser extent, both CB1 and CB2 receptors are distributed within peripheral organs and tissues including endocrine glands, the heart and liver, bone, and parts of the reproductive, urinary and gastrointestinal tracts. The potential for life-threatening overdoses due to respiratory depression are avoided due to the absence of CB1 receptors in the brainstem, medulla and thalamus.
Fig.4: The Body’s Endocannabinoid System (Ref: https://aeroflownaturals.com/education-blog/post/what-is-the-endocannabinoid-system)
Central Nervous SystemFacilitates the generation of new neurons and involved in neuroprotection, regulation of motor activity, synaptic plasticity, and control of certain memory processing.
MetabolismMaintains balance by controlling food intake and metabolic functions such as energy storage, nutrient transport and modulating insulin sensitivity.
Immune SystemRegulates immune system by suppressing proinflammatory cytokine production.
MusclesEnhances stamina by regulating blood sugar and encourages ‘runner’s high’.
Cannabinoid Receptor 1 (CB1) Cannabinoid Receptor 2 (CB2)
Gastrointestinal SystemHelps protect GI tract from inflammation and abnormally high gastric and enteric secretions.
HormonesPlays a signification role in the hypothalamic function which regulates metabolism, reproduction and responses to stress.
BonesPlays an important role in regulating bone mass and bone regrowth.
Postsynapticterminal
Presynapticterminal
AEA
AEA
NAPE
NAPE
NT
DAG
2-AG 2-AG
2-AG
AAGlycerol
AAEtNH2
Astrocyte
CB1R
NAPE-PLD
NAPE-PLD
DAGLa DAGLa
FAAH
MAGL

PAGE 6 GREEN DISPENSARY COMPOUNDING: COMPOUNDED MEDICINAL CANNABIS FOR PROFESSIONAL REFERENCE ONLY
Cannabidiol (CBD) Tetrahydrocannabinol (THC)
Absorption CBD has a time to maximum plasma concentration (Tmax) of 2.5 to 5 hours at steady state.
THC is almost completely absorbed (90 to 95%) after single oral doses. Due to the combined e!ects of first pass hepatic metabolism and high lipid solubility, only 10 to 20% of the administered dose reaches the systemic circulation. Concentrations of both parent drug and its major active metabolite (11-hydroxy-delta-9-THC) peak at approximately 0.5 to 4 hours after oral dosing and decline over several days. The pharmacokinetics of THC after single doses (2.5, 5, and 10 mg) and multiple doses (2.5, 5, and 10 mg given twice a day) have been studied in healthy subjects. A slight increase in dose proportionality on mean Cmax and AUC of THC was observed with increasing dose over the dose range studied.
E*ect of Food Coadministration of CBD with a high-fat/high-calorie meal increased Cmax by 5-fold, AUC by 4-fold, and reduced the total variability, compared with the fasted state in healthy volunteers.
In a published study, the e!ect of food on the pharmacokinetics of THC was studied by concomitant dosing of MARINOL® with a high-fat (59 grams of fat, approximately 50% of total caloric content of the meal), high calorie meal (approximately 950 calories). An appreciable food e!ect was observed, resulting in a 4-hour delay in mean Tmax and 2.9-fold increase in total exposure (AUC), but Cmax was not significantly changed.
Distribution The apparent volume of distribution of CBD in healthy volunteers was 20,963L to 42,849L. Protein binding of the cannabidiol and its metabolites was >94% in vitro.
THC has an apparent volume of distribution of approximately 10 L/kg, because of its lipid solubility. The plasma protein binding of THC and its metabolites is approximately 97%.
Elimination The half-life of CBD in plasma was 56 to 61 hours after twice-daily dosing for 7 days in healthy volunteers. The plasma clearance of CBD following a single CBD 1500 mg dose is 1111 L/h.
The pharmacokinetics of THC can be described using a two compartment model with an initial (alpha) half-life of about 4 hours and a terminal (beta) half-life of 25 to 36 hours. Values for clearance average about 0.2 L/kg-hr, but are highly variable due to the complexity of cannabinoid distribution.
Metabolism CBD is metabolised in the liver and the gut (primarily in the liver) by CYP2C19 and CYP3A4 enzymes, and UGT1A7, UGT1A9, and UGT2B7 isoforms. After repeat dosing, the active metabolite of cannabidiol, 7-OH-CBD, has a 38% lower AUC than the parent drug. The 7-OH-CBD metabolite is converted to 7-COOH-CBD, which has an approximately 40-¬fold higher AUC than the parent drug. Based on preclinical models of seizure, the 7-OH-CBD metabolite is active; however, the 7-COOH-CBD metabolite is not active.
THC undergoes extensive first-pass hepatic metabolism, primarily by hydroxylation, yielding both active and inactive metabolites. THC and its principal active metabolite, 11-hydroxy-delta-9-THC, a potent psychoactive metabolite, are present in approximately equal concentrations in plasma. Published in vitro data indicates that CYP2C9 and CYP3A4 are the primary enzymes in the metabolism of THC. CYP2C9 appears to be the enzyme responsible for the formation of the primary active metabolite.
Excretion CBD is excreted in faeces, with minor renal clearance. THC and its biotransformation products are excreted in both faeces and urine. Due to its re-distribution, THC and its metabolites may be excreted at low levels for prolonged periods of time. Following single dose administration, low levels of THC metabolites have been detected for more than 5 weeks in the urine and faeces.
CLINICAL PHARMACOLOGY
PharmacodynamicsDelta-9-tetrahydrocannabinol (THC) acts as a partial agonist at CB1 and CB2 receptors with greater a"nity for CB1. The CB1 receptor is highly expressed at the pre-synaptic level of neuronal synapses, where its stimulation activates potassium channels and inhibits calcium-dependent channels resulting in modulation of neurotransmitter release. The action of THC on CB1 receptors may modulate a number of neurotransmitter systems attributing to its analgesic, antispasmodic, appetite-stimulant, anti-emetic and psychoactive properties.
Cannabidiol (CBD) stimulates antagonistic activity at both cannabinoid receptors with particular a"nity for CB2. It does this without the psychoactive side e!ects associated with THC at CB1 receptors, and can instead reduce these when taken in combination with a THC-containing formulation. Through its e!ects at the cannabinoid receptors and others including TRPV1, 5HT1, adenosine, PPAR and GPR55 receptors, CBD has been attributed with anti-inflammatory, anti-convulsant, anxiolytic, anti-oxidant, neuroprotective, anti-epileptiform, anti-nausea, tumour-inhibitory, and immunomodulatory e!ects. It also increases the concentration of the endogenous cannabinoid anandamide, due to an inhibitory e!ect on the catabolic enzyme fatty acid amide hydrolase (FAAH).
PharmacokineticsThe following table compares the Pharmacokinetics of CBD and THC.

FOR PROFESSIONAL REFERENCE ONLY PAGE 7GREEN DISPENSARY COMPOUNDING: COMPOUNDED MEDICINAL CANNABIS
Medicinal cannabis and epilepsy in paediatric and adult patients
There is some evidence to support using medicinal cannabis in the treatment of certain childhood epilepsies.
Cannabidiol (CBD) is the substance featured in most published evidence on medicinal cannabis as an epilepsy treatment. However, this evidence is when it is used as an add-on to current treatments in drug-resistant epilepsy in children and young adults up to 25 years where use of several anti-epileptic drugs has not controlled their condition. In patients with paediatric-onset drug-resistant epilepsy, CBD products reduced seizure frequency by 50 per cent or more in up to half of the patients and achieved seizure freedom in a small number of patients. Several studies have reported improved quality of life in paediatric and adult groups, but overall there are few studies of how e!ective CBD is in treating adult epilepsy. There is not enough evidence to recommend this treatment for adults.
Medicinal cannabis and multiple sclerosis (MS)
There is some low to moderate evidence to suggest that medicinal cannabis products may be e!ective for treating the pain symptoms of MS.
There is a TGA registered medicine (Nabiximols, which are an extract of cannabis plant containing roughly equal amounts of THC and CBD) for the use in MS for muscle spasticity. There is some low to moderate evidence to suggest that medicinal cannabis products may be e!ective for treating the pain symptoms of MS, although this is inconsistent. Studies di!er as to whether medicinal cannabis products can help improve bladder function, sleep, quality of life, ataxia/tremor and disability/disease progression. Treating doctors should assess people with MS after 12 weeks to re evaluate and monitor both the positive and negative e!ects of the drug.
Treating chronic and neuropathic pain
There is some evidence that cannabinoids can reduce pain in both MS-related neuropathic pain and non-MS-related neuropathic pain. There is, however, insu"cient information to make a conclusion about cannabinoids for the treatment of pain associated with arthritis and fibromyalgia.
The majority of the studies on the use of cannabinoids in pain have studied THC or THC-rich extracts. The studies are mainly where cannabinoids were “adjuvant” treatments, used in addition to other pain medicines.Most studies have been on chronic (long-term) rather than acute (short-term) pain. There is some evidence that cannabinoids can reduce pain in both MS-related neuropathic pain and non-MS related neuropathic pain, but for many people the reduction in pain may be modest. There is also some evidence that it can improve sleep. There is much interest at present as to whether cannabinoids are “opioid sparing”. While some individuals with pain have reported that their use of opioids has been reduced with concomitant use of medicinal cannabis, clinical studies in this area are still ongoing.
Preventing and managing chemotherapy-induced nausea and vomiting in cancer (CINV)
There are some reports that medicinal cannabis products (in particular THC and related substances) relieved the symptoms of CINV.
The number of studies is small and the quality of published evidence is low to moderate. THC-rich medicinal cannabis products for chemotherapy-induced nausea and vomiting should be prescribed only after standard approved treatments have failed.
Medicinal cannabis use in palliative care
There is no evidence at this time that medicinal cannabis has any anti-cancer activity or that it can slow the progression of these conditions.
While medicinal cannabis products can be used to treat nausea and vomiting due to chemotherapy, there is little evidence of any benefit to advanced cancer patients with chronic pain. The published studies in the medical literature showed little e!ect on appetite, nausea/vomiting, pain, dizziness, mental health or sleep problems. There is also no evidence that medicinal cannabis has any anti-cancer activity in human studies or that it can slow the progression of these conditions.In people without acquired immunodeficiency syndrome (AIDS), there is also no evidence that medicinal cannabis will increase their appetite, that it will help the patient gain weight or that it will enhance their mood.It is important to note that some side-e!ects from medicinal cannabis treatment may be similar to symptoms of distress often experienced by people in end-of-life care. As there are very few studies on medicinal cannabis treatment in palliative care, it should be used only after standard treatments have failed. It is possible that medicinal cannabis will interact with chemotherapy and other medications used in palliative care. More studies are needed to better understand this.
POTENTIAL THERAPEUTIC APPLICATIONS
There are many studies reporting on the therapeutic e!ects of medicinal cannabis, and we will cover some of the key benefits here. However, evidence is continually emerging for further potential applications. What is evident is that cannabinoids may provide broad benefits across several health conditions, either with symptom management, disease progression or quality of life. As a legal treatment, medicinal cannabis where appropriate may form part of a multi-therapy approach or as a further option to other medications where their e!ects have been limited.
TGA Therapeutic Guidelines

PAGE 8 GREEN DISPENSARY COMPOUNDING: COMPOUNDED MEDICINAL CANNABIS FOR PROFESSIONAL REFERENCE ONLY
DOSAGE
As medicinal cannabis does not follow the traditional “single molecule, single target” pharmacological model for drugs, dosing information can be highly variable and is best determined based on titration within suggested dosage guidelines.
The Variables• The complex pharmacology of cannabinoids
• Genetic di!erences in cannabinoid receptor structure and function
• Genetic di!erences in cannabinoid metabolism a!ecting cannabinoid bioavailability
• Prior exposure
• Pharmacological tolerance to cannabinoids
• Changes to cannabinoid receptor distribution/density/function as a consequence of a medical condition
• The variable potency of raw material and ratios of di!erent cannabinoids
• The di!erent dosing regimens and routes of administration used in di!erent research studies
All these contribute to the di"culty in prescribing precise doses or establishing uniform dosing schedules for cannabis and cannabinoids.
Dosage TitrationThe best method of determining the most appropriate dose for an individual patient is through the process of titration (i.e. finding the right dose where potential therapeutic e!ects are maximised while adverse or harmful e!ects are minimised). The most prudent approach to dosing in the absence of evidence-based guidelines is to start with a low dose and titrate the dose up slowly.
Starting with a low dose is particularly important for people with memory and thinking di"culties, liver and kidney disease, and weakness and wasting of the body due to severe chronic illness. It is also important for young people and the elderly. Consumption of oral cannabis should proceed slowly, waiting an absolute minimum of 30 minutes, but preferably 3 hours, between doses of cannabis-based oral products to gauge for strength of e!ects (or possible overdosing). Dose escalation should be done slowly, once the subjective e!ects and tolerability are fully appreciated. If intolerable adverse e!ects appear without significant benefit, dosing should be tapered and stopped.
OTHER POTENTIAL THERAPEUTIC APPLICATIONS
Arthritis and musculoskeletal disorders• Pre-clinical studies suggest stimulation of CB1 and CB2 receptors alleviates symptoms of osteoarthritis (OA), and both THC and
CBD alleviate symptoms of rheumatoid arthritis (RA).
• Observational studies in patients with fibromyalgia suggest a modest benefit in symptoms of pain, sti!ness, somnolence, and in their perception of wellbeing.
Movement disorders• Dystonia: Evidence from small placebo-controlled or open-label clinical trials suggests improvement in symptoms of dystonia with
oral CBD whilst oral THC provided mixed results.
• Tourette’s Syndrome: Limited evidence from small clinical studies suggests that oral THC improves certain symptoms of Tourette’s syndrome such as tics.
Stress and psychiatric disorders• Sleep disorders: Human experimental data suggests THC has a dose-dependent e!ect on sleep with lower doses appearing to
decrease sleep-onset latency and increase sleep quality while high doses appear to cause sleep disturbances.
• Post-traumatic stress disorder: Pre-clinical and human experimental studies suggest a role for certain cannabinoids in alleviating post-traumatic stress disorder (PTSD)-like symptoms.
• Alzheimer’s disease and dementia: Pre-clinical studies suggest that THC and CBD may protect against excitotoxicity, oxidative stress and inflammation in animal models of Alzheimer’s disease (AD). Limited case, clinical and observational studies suggest that oral THC are associated with improved in AD-associated symptoms such as nocturnal motor activity, disturbed behaviour and agitation.
Gastrointestinal system disorders• Irritable bowel syndrome (IBS): Pre-clinical studies in animal models of IBS suggest that certain synthetic cannabinoid receptor
agonists inhibit colorectal distention-induced pain responses and slow GI transit.
• Inflammatory bowel disease (Crohn’s disease, ulcerative colitis): Pre-clinical studies in animal models of inflammatory bowel disease (IBD) suggest that certain cannabinoids such as THC, CBD, CBG and CBC may limit intestinal inflammation and disease severity.

FOR PROFESSIONAL REFERENCE ONLY PAGE 9GREEN DISPENSARY COMPOUNDING: COMPOUNDED MEDICINAL CANNABIS
Therapeutic Use Recommended Dosage
Anxiety 2.5mg BD, titration double dose Q3 days up to max 300mg BD
Chronic pain and Neuropathic pain 10-100mg BD
Endometriosis 2.5mg titration up to 25mg QID reg or prn
Fibromyalgia 2.5mg titration up to 25mg QID reg or prn
Migraine 2.5mg titration up to 25mg QID reg or prn
Epilepsy 2.5-20mg/kg/day in divided doses (based on clinical studies with Epidiolex®, an oil-based extract of cannabis containing greater than 98% CBD)
Sleep quality 2.5mg nocte, titration to max 50mg
Inflammatory Bowel Disease (Crohns) 2.5mg titration up to 25mg QID reg or prn
PTSD 50-100mg bd
Schizophrenia 25mg BD, titration to 1200mg per day (consider QID dosing)
CBD Daily Dosage5-500mg before food depending on condition (start with a low dose and titrate up slowly as required waiting a minimum of 30 minutes and preferably 3 hours between doses).
Tetrahydrocannabinol (THC)Information obtained from the monograph for Marinol® (dronabinol (THC); indicates that a daily oral dose as low as 2.5mg #9-THC is associated with a therapeutic e!ect (e.g. treatment of AIDS-related anorexia/cachexia).
Naturally, dosing will vary according to the underlying disorder and the many other variables mentioned above. Dosing ranges for Marinol® (dronabinol) vary from 2.5mg to 40mg #9-THC/day (maximal tolerated daily human dose = 210mg #9-THC/day).
Average daily dose of dronabinol is 20mg and maximal recommended daily dose is 40mg. Doses less than 1mg of THC per dosing session may further avoid incidence and risks of adverse e!ects. Dosing ranges for Sativex® (nabiximols) vary from one spray (2.7mg #9-THC and 2.5mg CBD) to 16 sprays (43.2mg #9-THC and 40mg CBD) per day.
THC Daily Dosage2.5-40mg before food depending on condition (start with a low dose, and titrate up slowly as required waiting a minimum of 30 minutes and preferably 3 hours between doses).
Suggested Treatment Plan for Compounded Medicinal Cannabis• Set a time-limited trial (4-12 weeks) to monitor for e"cacy of medicinal cannabis treatment and manage risks.
• Insert monitoring intervals (weekly/fortnightly/monthly reviews), any follow-up testing or investigations required and treatment goals.
• Consider an exit strategy for situations where treatment is not helping to manage symptoms, adverse e!ects cannot be tolerated or goals of treatment are not reached.
o If a patient has been on THC treatment for several months, gradually taper the dose over 4-8 weeks to avoid discontinuation symptoms
o Sleep problems such as vivid dreams or insomnia, depressed mood and irritability or anxiety may be symptoms experienced during tapering of treatment.
o These may emerge 1-2 days after the last dose, and may peak within 2-6 days with most symptoms resolving between 1-2 weeks.
DOSAGE (continued)
Cannabidiol (CBD)The following information is a guide to CBD dosing:

PAGE 10 GREEN DISPENSARY COMPOUNDING: COMPOUNDED MEDICINAL CANNABIS FOR PROFESSIONAL REFERENCE ONLY
PRECAUTIONS AND WARNINGS
The risk/benefit ratio of medicinal cannabis (especially THC-predominant cannabis) should be carefully evaluated in patients. This is due to individual variations in response and tolerance to its e!ects, as well as the di"culty in dosing.
• Age: Cannabinoid products containing primarily THC should not be used in any person under the age of 25 unless the risk/benefit ratio is considered by the medical practitioner to be favourable. The adverse e!ects of THC-predominant medicinal cannabis on mental health are greater during development, particularly during adolescence (ages 10 to 24) with risks increasing with younger age, frequent use and THC potency.
• Hypersensitivity: Cannabinoid products should not be used in any patient who has a history of hypersensitivity to any cannabinoid (from previous exposure).
• Cardiovascular/Cerebrovascular Disease: Cannabinoid products should not be used in patients with severe cardiovascular or cerebrovascular disease because of occasional hypotension or possible hypertension, tachycardia, myocardial infarction and stroke.
• Liver/Renal Disease: Cannabinoid products should not be used in patients with severe liver or renal disease.
• Psychiatric Disorders: Cannabinoid products containing primarily THC (and especially higher levels of THC) should not be used in patients with a personal history of psychiatric disorders (i.e. psychosis, schizophrenia, anxiety and mood disorders) or a familial history of schizophrenia.
• Substance Abuse: Cannabinoid products should not be used in patients with a history of substance abuse.
• Neurological Conditions: Patients with neurological conditions may be more likely to experience negative e!ects from the use of cannabinoid products.
• Pregnancy and Lactation: THC readily crosses into the placenta and cannabinoids are excreted in human milk.
• Driving and Operating Machinery: Patients should not drive* or operate machinery while being treated with medicinal cannabis. In addition, measurable concentrations of THC can be detected in urine many days after the last dose. It may take up to five days for 80 to 90 per cent of the dose to be excreted.
• Workplace policies: Consider ‘zero tolerance’ drug policies in places of employment for patients.
Adverse ReactionsThere is generally more information in the medical literature on the adverse reactions associated with the use of non-medicinal cannabis than there is with therapeutic or medicinal cannabis. The available information about medicinal cannabis is predominantly on the short-term adverse e!ects.
• CBD: Some reported side e!ects of oral cannabidiol include dry mouth, vomiting, diarrhoea, light headedness, and drowsiness at doses greater than 300mg.
• THC: The adverse e!ects oral tetrahydrocannabinol may include asthenia, confusion, disorientation, dizziness, drowsiness, vertigo/balance problems, dry mouth, anxiety, paranoid thoughts, memory problems, somnolence, euphoria and hallucinations.
There is limited evidence about the health risks of long-term medical use of cannabinoids, but in general those reported are similar to those reported for short-term use. Some of the harms reported among long-term users of recreational cannabis could possibly apply to the long-term medical use of cannabis and cannabinoids, but more research is needed to draw evidence-based conclusions.
Drug Interactions
CBD • CBD concentrations increase with CYP3A4 and CYP2C19 inhibitors (i.e. azole antifungals, macrolide antibiotics, verapamil/diltiazem, omeprazole, fluoxetine, etc.).
• CBD concentrations decrease with CYP3A4 and CYP2C19 inducers (i.e. St. John’s Wort, carbamazepine, etc.).
• CBD + Sodium Valproate increases liver enzymes.
• CBD + Clobazam increases Clobazam metabolite.
THC • Additive drowsiness and CNS depression when combined with barbiturates, benzodiazepines, ethanol, lithium, opioids, buspirone, antihistamines, muscle relaxants, other depressants.
OverdosingOverdosing usually presents as acute psychological complications (e.g. panic attacks, severe anxiety, psychosis, paranoia, hallucinations, convulsions, hyperemesis etc.) and can be managed with conservative measures, such as reassurance in a quiet environment, and/or administration of benzodiazepines (5 to 10 mg diazepam p.o.) or i.v. fluids, if required. As is stated in the case of overdose with Marinol®, the signs and symptoms observed are an extension of the psychotomimetic and physiologic e!ects of THC. Individuals experiencing psychotic reactions should stop using cannabis or cannabinoids immediately and seek prompt medical/psychiatric attention. Lethal overdoses due to respiratory depression do not occur due to the lack of cannabinoid receptors in the areas of the brainstem controlling respiration. The estimated lethal human dose of intravenous THC is 30mg/kg (2100mg/70kg).
*Roadside drug testing in Australia tests for THC in saliva. It is a criminal offence to drive: with the presence of THC in oral fluid, blood or urine; or (b) under the influence of THC. There is no medical defence to these offences for using a prescribed cannabis medicine. There may also be insurance implications for patients who are convicted of these offences.

FOR PROFESSIONAL REFERENCE ONLY PAGE 11GREEN DISPENSARY COMPOUNDING: COMPOUNDED MEDICINAL CANNABIS
REFERENCES
• National Guidance on medicinal cannabis: Therapeutic Goods Administration, Australia https://www.tga.gov.au/medicinal-cannabis-guidance-documents
• Access to unapproved therapeutic goods: Therapeutic Goods Administration, Australia https://www.tga.gov.au/accessing-unapproved-products
• Poisons Standard October 2019 https://www.legislation.gov.au/Details/F2019L01197
• Therapeutic Goods Regulation 1990 https://www.legislation.gov.au/Details/F2019C00739
• Information for Health Care Professionals: Cannabis and the cannabinoids. Health Canada, 2013 http://www.hc-sc.gc.ca/dhp-mps/marihuana/med/index-eng.php
• Cannabinoids for Medical Use: A Systemic Review and Meta-analysis. Whiting et al. JAMA 2015; 313(24)2456-2473
• Victorian Law Reform Commission: Medicinal Cannabis Report August 2015 http://lawreform.vic.gov.au/sites/default/files/VLRC_Medicinal_Cannabis_Report_w eb.pdf

FOR PROFESSIONAL REFERENCE ONLY
STIRLING 28 Mount Barker Road, Mount Barker (08) 8339 1347
BLACKWOOD 202 Main Road, Blackwood (08) 8278 2388
ERINDALE 361 Kensington Road, Kensington Gardens (08) 8431 6727
COMPOUNDING 211 Payneham Road, St Peters (08) 8363 7322
greendispensarycompounding.com.au
FOR PROFESSIONAL REFERENCE ONLY. PUBLISHED NOV$%&'(