Complications after bariatric surgery
22
COMPLICATIONS AFTER BARIATRIC SURGERY By Dr. M. Maher Khawatmi By Dr. M. Maher Khawatmi
-
Upload
mohamed-maher-khawatmi -
Category
Health & Medicine
-
view
256 -
download
2
Transcript of Complications after bariatric surgery

COMPLICATIONS AFTER BARIATRIC
SURGERY
By Dr. M. Maher KhawatmiBy Dr. M. Maher Khawatmi

1 .The The Bariatric Operations:Operations:
1.1.1. Restrictive: Restrictive:
1.1.1. Adjustable gastric banding (AGB) 1.1.1. Adjustable gastric banding (AGB) 1.1.2. Sleeve gastrectomy (SG)1.1.2. Sleeve gastrectomy (SG)
1.2. Largely Restrictive/Mildly Malabsorptive:1.2. Largely Restrictive/Mildly Malabsorptive:
1.2.1. Roux-en-Y gastric bypass (RYGB)1.2.1. Roux-en-Y gastric bypass (RYGB)
1.3. Largely Malabsorptive/Mildly Restrictive:1.3. Largely Malabsorptive/Mildly Restrictive:
1.3.1. Biliopancreatic diversion (BPD)1.3.1. Biliopancreatic diversion (BPD)1.3.2. Biliopancreatic diversion with duodenal switch (BPD-DS)1.3.2. Biliopancreatic diversion with duodenal switch (BPD-DS)

1 .The The Bariatric Operations:Operations:
1.1.1. Restrictive: Restrictive:
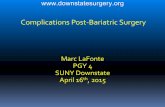
1.1.1. Adjustable Gastric Banding (AGB)AGB):
1.1.1.1. Advantages of AGBAGB:
ReversibleLeast invasiveLowest risk of deathNo malabsorption
1.1.1.2. Disadvantages of AGBAGB:
ErosionEsophageal dilationBreakSlippageFailure to lose weightLower average weight loss

Adjustable Gastric Banding (AGB)AGB)

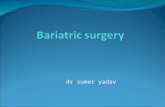
1.1.2 .Sleeve Gastrectomy (SG):
1.1.2.1. Advantages of SG:
The stomach size is reduced without loss of function.Eliminates the portion of the stomach that produces Ghrelin. Pyloric preservation prevents dumping. There are no problems with malabsorption.It is an effective first-stage procedure for super-obese patients. It is useful for patients with conditions such as anemia or Crohn’s disease, which preclude intestinal bypass. Appealing option for people who are concerned about the foreign body aspect of AGB.
1.1.2.2. Disadvantages of SG:
It is not reversible. Soft calories such as ice cream, milk shakes, etc can be absorbed and may slow weight loss. It does involve stomach stapling and therefore leaks and other
complications related to stapling may occur .

Sleeve Gastrectomy (SG)

1.21.2 . .Largely Restrictive/Mildly Malabsorptive:Largely Restrictive/Mildly Malabsorptive:
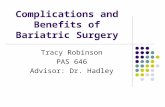
1.2.1. RYGB:
1.2.1.1. Advantages of RYGB:
Proven weight loss over 5 yearsBetter weight loss than restrictive (stomach only) operationsProven improvement in medical comorbiditiesMortality less than 1% at most centers
1.2.1.2. Disadvantages of RYGB:
MalabsorptionMarginal ulcerStomal stenosisInability to easily access distal stomachInternal herniaIron deficiency anemiaCalcium and vitamin B12 deficiencies

Roux-en-Y gastric bypass (RYGB)Roux-en-Y gastric bypass (RYGB)

1.3. Largely Malabsorptive/Mildly Restrictive:1.3. Largely Malabsorptive/Mildly Restrictive:
1.3.1. Biliopancreatic Diversion (BPD):(BPD): 1.3.1.1. Advantages of BPDBPD:
Best weight loss results of all surgeriesEating capacity is greater than other surgeriesContinued weight loss for 18-24 months post surgeryMany patients maintain a weight loss of 75-80% of excess weight 10 years post-opAdjustable and partially reversible but only with additional surgeryGood option for revision if other techniques have failedImproved health problems associated with severe obesity(i.e., diabetes, high blood pressure, sleep apnea, etc.)Improved mobility and quality of life

Biliopancreatic Diversion (BPD)(BPD)

1.3.1.2 .Disadvantages of BPDBPD:
Usually performed as open surgery Risk of death 1:200 Longer recovery time, usually 6-8 weeks Malabsorptions require life long supplementation of fat soluble vitamins (A, D, E, and K), B12, calcium and iron Risk of iron deficiency anemia and osteoporosis Requires gallbladder removal during surgery due to high risk of gallstones Dumping syndrome can occur after ingesting high sugar foods Increased stool frequency Foul flatulence and diarrhea if fatty foods eaten

1.3.21.3.2 . .Biliopancreatic diversion with duodenal switch (BPD-DS):Biliopancreatic diversion with duodenal switch (BPD-DS):
Advantages of BPD-DS:BPD-DS:
Excellent weight lossIncreased food intakePreserved pylorus = less dumpingLess risk of marginal ulcers
Disadvantages of BPD-DS:BPD-DS:
Increased risk of protein malabsorptionIncreased risk of fat-soluble vitamin malabsorption (A, D, E, K)Iron deficiency anemiaDiarrhea and excess gas more commonInternal herniaHigher complication rateHigher risk of osteoporosis

Biliopancreatic Diversion with Duodenal Switch (BPD-DS)(BPD-DS)

2 .Complications Complications after Bariatric Surgery:
2.1. Early Complications:2.1. Early Complications:
The most serious early complications are anastomotic leak and The most serious early complications are anastomotic leak and pulmonary embolism. pulmonary embolism. Anastomotic leak can occur at any of the sites where the GI tract is Anastomotic leak can occur at any of the sites where the GI tract is entered or reconstructed, although it most commonly occurs at the entered or reconstructed, although it most commonly occurs at the gastrojejunostomy. gastrojejunostomy. Leaks can be extremely difficult to detect. Leaks can be extremely difficult to detect. Tachycardia, tachypnea, fever, anxiety, and leukocytosis are often Tachycardia, tachypnea, fever, anxiety, and leukocytosis are often present, although it is not uncommon for a leak to manifest as present, although it is not uncommon for a leak to manifest as unexplained persistent tachycardia in an asymptomatic patient. unexplained persistent tachycardia in an asymptomatic patient. This complication can often be confirmed with an upper gastrointestinal This complication can often be confirmed with an upper gastrointestinal series using water-soluble contrast. If the study is negative but suspicion series using water-soluble contrast. If the study is negative but suspicion
is high, the abdomen should be reexploredis high, the abdomen should be reexplored..

Pulmonary complications include pneumonia and atelectasis. Pulmonary complications include pneumonia and atelectasis. Pulmonary embolism is the second most frequent cause of death, with an Pulmonary embolism is the second most frequent cause of death, with an incidence of approximately 1%.incidence of approximately 1%. Although obstruction of the Roux limb is rare after RYGB, it may cause Although obstruction of the Roux limb is rare after RYGB, it may cause acute distention of the gastric remnant. acute distention of the gastric remnant. Internal hernias and adhesion formation are also rare causes of intestinal Internal hernias and adhesion formation are also rare causes of intestinal obstruction. obstruction.
Most wound complications occur within 1 month of surgeryMost wound complications occur within 1 month of surgery..

2.22.2 . .Late Complications:Late Complications:
2.2.1. Vomiting:2.2.1. Vomiting:
Vomiting is common after bariatric surgery. Causes include inadequate Vomiting is common after bariatric surgery. Causes include inadequate chewing, food impaction, stomal stenosis after RYGB, obstruction at the chewing, food impaction, stomal stenosis after RYGB, obstruction at the jejunojejunal anastomosis, internal herniation, and bowel obstruction jejunojejunal anastomosis, internal herniation, and bowel obstruction secondary to adhesion formation. secondary to adhesion formation. Patients should be encouraged to eat slowly, over at least 20 minutes, Patients should be encouraged to eat slowly, over at least 20 minutes, and to make sure that meal volume is less than 60 ml at each sitting. and to make sure that meal volume is less than 60 ml at each sitting. They should be alsoThey should be also instructed to drink between meals to minimize the instructed to drink between meals to minimize the risk of gastric pouch overfilling. risk of gastric pouch overfilling. Patients who gradually develop intolerance to both solids and liquids Patients who gradually develop intolerance to both solids and liquids may have developed stomal stenosis after RYGB. The problem is quite may have developed stomal stenosis after RYGB. The problem is quite successfully treated with endoscopic or fluoroscopic balloon dilation. successfully treated with endoscopic or fluoroscopic balloon dilation. Patients who fail to respond may require surgical intervention. Patients who fail to respond may require surgical intervention. The sudden onset of vomiting may herald bezoar or food impaction. The sudden onset of vomiting may herald bezoar or food impaction. Emergency esophagogastroscopy may be required to extract the Emergency esophagogastroscopy may be required to extract the obstructing material. Obstruction at the jejunojejunal anastomosis is a obstructing material. Obstruction at the jejunojejunal anastomosis is a
less common cause of vomitingless common cause of vomiting . .

2.2.22.2.2 . .Diarrhea:Diarrhea:
Patients who undergo BPD typically have 4-6 bowel movements per day Patients who undergo BPD typically have 4-6 bowel movements per day that may be steatorrheic. that may be steatorrheic. Patients who experience diarrhea after RYGB may have dumping Patients who experience diarrhea after RYGB may have dumping associated with ingestion of hyperosmolar food substances.associated with ingestion of hyperosmolar food substances.
2.2.3. Gastroesophageal Reflux: 2.2.3. Gastroesophageal Reflux:
Gastroesophageal reflux is frequently observed after AGB. Gastroesophageal reflux is frequently observed after AGB. Some patients will need to have their gastric bands removed.Some patients will need to have their gastric bands removed. In this instance, conversion to a RYGB may be indicated, especially if In this instance, conversion to a RYGB may be indicated, especially if weight loss has been unsatisfactoryweight loss has been unsatisfactory..

2.2.42.2.4 . .Cholelithiasis:Cholelithiasis:
The rapid weight loss increases the likelihood of gallstone formation. The rapid weight loss increases the likelihood of gallstone formation. As many as 36% of patients may develop sludge or cholelithiasis within As many as 36% of patients may develop sludge or cholelithiasis within 6 months of gastric bypass operations.6 months of gastric bypass operations. Some surgeons recommend prophylactic cholecystectomy at the time of Some surgeons recommend prophylactic cholecystectomy at the time of bariatric surgery; others perform cholecystectomy only if sonographic bariatric surgery; others perform cholecystectomy only if sonographic evidence of gallstones is identified. evidence of gallstones is identified. Ursodeoxycholic acid, 300 mg orally twice daily for 6 months following Ursodeoxycholic acid, 300 mg orally twice daily for 6 months following gastric bypass, reduces the cholelithiasis risk to 2%.gastric bypass, reduces the cholelithiasis risk to 2%.Compliance with this medication can be difficult secondary to adverse Compliance with this medication can be difficult secondary to adverse side effects (nausea, diarrhea, and pruritus).side effects (nausea, diarrhea, and pruritus). Access to the common bile duct can be difficult in patients who have Access to the common bile duct can be difficult in patients who have
undergone undergone RYGBRYGB..

2.2.52.2.5 . .Stomal Ulceration:Stomal Ulceration:
Stomal ulceration is more common after RYGB in which the distal Stomal ulceration is more common after RYGB in which the distal stomach is not transected. Endoscopy is the diagnostic procedure of stomach is not transected. Endoscopy is the diagnostic procedure of choice and biopsies should be performed to rule out Helicobacter pylori.choice and biopsies should be performed to rule out Helicobacter pylori. Prophylaxis is key. Patients are treated with proton pump inhibitors Prophylaxis is key. Patients are treated with proton pump inhibitors during the immediate postoperative period. Many centers continue such during the immediate postoperative period. Many centers continue such treatment for several months.treatment for several months.Stomal stenosis can occur following RYGB. Outpatient endoscopic Stomal stenosis can occur following RYGB. Outpatient endoscopic dilatation is usually successful in patients with gastric bypass, although dilatation is usually successful in patients with gastric bypass, although more than one treatment may be necessarymore than one treatment may be necessary..

2.2.62.2.6 . .Upper Gastrointestinal Bleeding:Upper Gastrointestinal Bleeding:
Upper gastrointestinal bleeding is rare. Upper gastrointestinal bleeding is rare. Possible causes include bleeding at the gastrojejunal anastomosis, at the Possible causes include bleeding at the gastrojejunal anastomosis, at the gastric pouch staple line, stomal ulceration, or bleeding at the gastric pouch staple line, stomal ulceration, or bleeding at the jejunojejunal anastomosis. jejunojejunal anastomosis. Endoscopy can identify and treat many sources of bleeding. Access to Endoscopy can identify and treat many sources of bleeding. Access to the bypassed stomach may be obtained percutaneously or may require the bypassed stomach may be obtained percutaneously or may require operative exposure. operative exposure.
2.2.7. Dumping Syndrome:2.2.7. Dumping Syndrome:
Dumping syndrome most commonly occurs after RYGB. Dumping syndrome most commonly occurs after RYGB. Typical symptoms include diarrhea, abdominal colic, nausea, and Typical symptoms include diarrhea, abdominal colic, nausea, and vomiting, as well as systemic effects of hypotension, tachycardia, vomiting, as well as systemic effects of hypotension, tachycardia, lightheadedness, flushing, and syncope, and are believed to be caused lightheadedness, flushing, and syncope, and are believed to be caused
by hyperosmolar foods or liquidsby hyperosmolar foods or liquids . .

2.2.72.2.7 . .Vitamin BVitamin B12 12 , Folate, and Iron Deficiencies;, Folate, and Iron Deficiencies;
Patients who undergo RYGB or BPD may develop vitamin BPatients who undergo RYGB or BPD may develop vitamin B1212 deficiency. deficiency. The mechanisms include achlorhydria, suboptimal vitamin consumption, The mechanisms include achlorhydria, suboptimal vitamin consumption, and reduced production of intrinsic factor, which is required for vitamin and reduced production of intrinsic factor, which is required for vitamin BB1212 absorption in the distal ileum. absorption in the distal ileum. Folate deficiency is seen in association with decreased absorption of Folate deficiency is seen in association with decreased absorption of vitamin Bvitamin B1212, which is needed for conversion of inactive to active folate., which is needed for conversion of inactive to active folate.Folate deficiency may also occur secondary to achlorhydria.Folate deficiency may also occur secondary to achlorhydria.Iron deficiency anemia is common after RYGB. The mechanisms include Iron deficiency anemia is common after RYGB. The mechanisms include suboptimal iron consumption and reduced absorption of iron in suboptimal iron consumption and reduced absorption of iron in association with achlorhydria and a bypassed duodenumassociation with achlorhydria and a bypassed duodenum..

2.2.82.2.8 . .Fat-Soluble Vitamins:Fat-Soluble Vitamins:
Patients who undergo a long-limb RYGB or BPD may have significant Patients who undergo a long-limb RYGB or BPD may have significant steatorrhea with loss of the fat-soluble vitamins. Daily supplementation of steatorrhea with loss of the fat-soluble vitamins. Daily supplementation of vitamin D may be required. vitamin D may be required.
2.2.9. Thiamine:2.2.9. Thiamine:
Thiamine is normally absorbed in the proximal small bowel.Thiamine is normally absorbed in the proximal small bowel. Thiamine deficiency can result in Wernicke-Korsakoff syndrome, Thiamine deficiency can result in Wernicke-Korsakoff syndrome, characterized by ophthalmoplegia, ataxia, and mental status alterations. characterized by ophthalmoplegia, ataxia, and mental status alterations. 2.2.10. Calcium:2.2.10. Calcium:
Calcium is normally absorbed in the duodenum. Calcium is normally absorbed in the duodenum. Long-term consequences of RYGB or BPD include osteoporosis Long-term consequences of RYGB or BPD include osteoporosis and therefore calcium supplementation is recommended postoperatively at supplementation is recommended postoperatively at
doses of 1500–2000 mg per daydoses of 1500–2000 mg per day..