Complications and Benefits of Bariatric Surgery Tracy Robinson PAS 646 Advisor: Dr. Hadley.
29
Complications and Benefits of Bariatric Surgery Tracy Robinson PAS 646 Advisor: Dr. Hadley
-
Upload
brice-sanders -
Category
Documents
-
view
215 -
download
0
Transcript of Complications and Benefits of Bariatric Surgery Tracy Robinson PAS 646 Advisor: Dr. Hadley.
Complications and Benefits of Bariatric
Surgery
Tracy Robinson
PAS 646
Advisor: Dr. Hadley
Objectives
Obesity Statistics Bariatric Surgery options Post-surgical complicatioins Nutritional consequences Improvements in co-morbidities Psychological and QOL improvements Why do PAs need to be aware?
Obesity Statistics
33% US population is obese (BMI ≥ 30 kg/m2)
8 million people in US morbidly obese (BMI ≥ 40 kg/m2)
Between 1986 and 2000…… Obesity doubled Morbid obesity quadrupled Super obesity (BMI ≥ 50 kg/m2) increased five-fold
Obesity Statistics cont…..
Men > 50% overweight = double mortality Men > 50% overweight + DM = 5x mortality Women > 50% overweight = 2x mortality Women > 50% overweight + DM = 8x
mortality
5% total healthcare costs US $60 billion
Bariatric Surgery
1990 – 2000 → 4925 to 41,000 2005 → 130,000 2010 → 218,000
Bariatric surgery criteria BMI ≥ 40 kg/m2 without co-morbid disease BMI ≥ 35 kg/m2 with concurrent co-morbid
disease
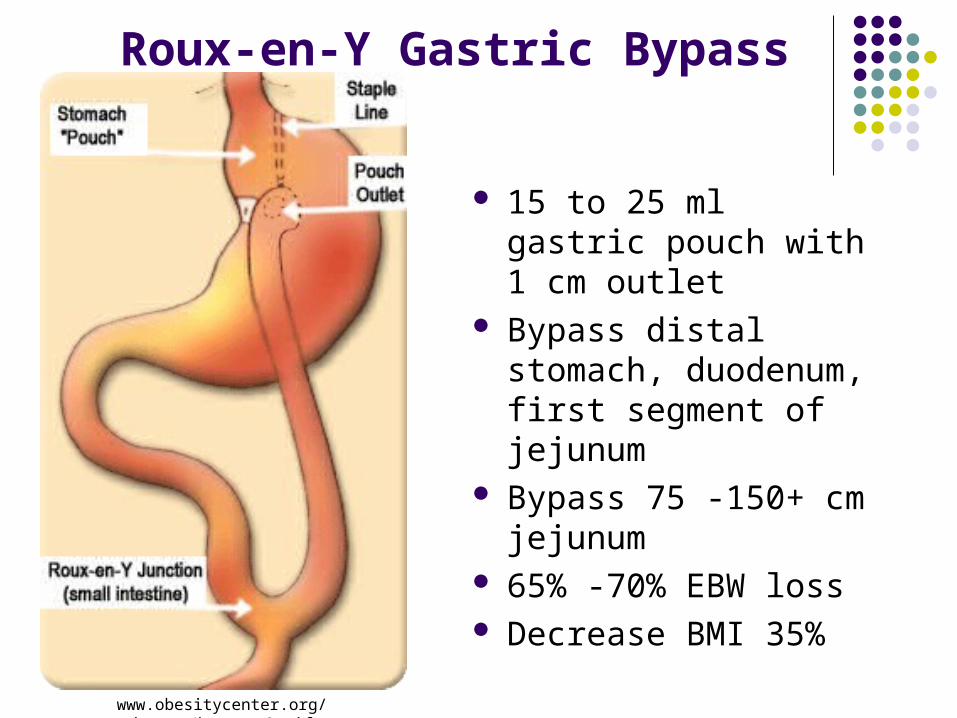
Roux-en-Y Gastric Bypass
15 to 25 ml gastric pouch with 1 cm outlet
Bypass distal stomach, duodenum, first segment of jejunum
Bypass 75 -150+ cm jejunum
65% -70% EBW loss Decrease BMI 35%
www.obesitycenter.org/ images/bg_roux2.gif
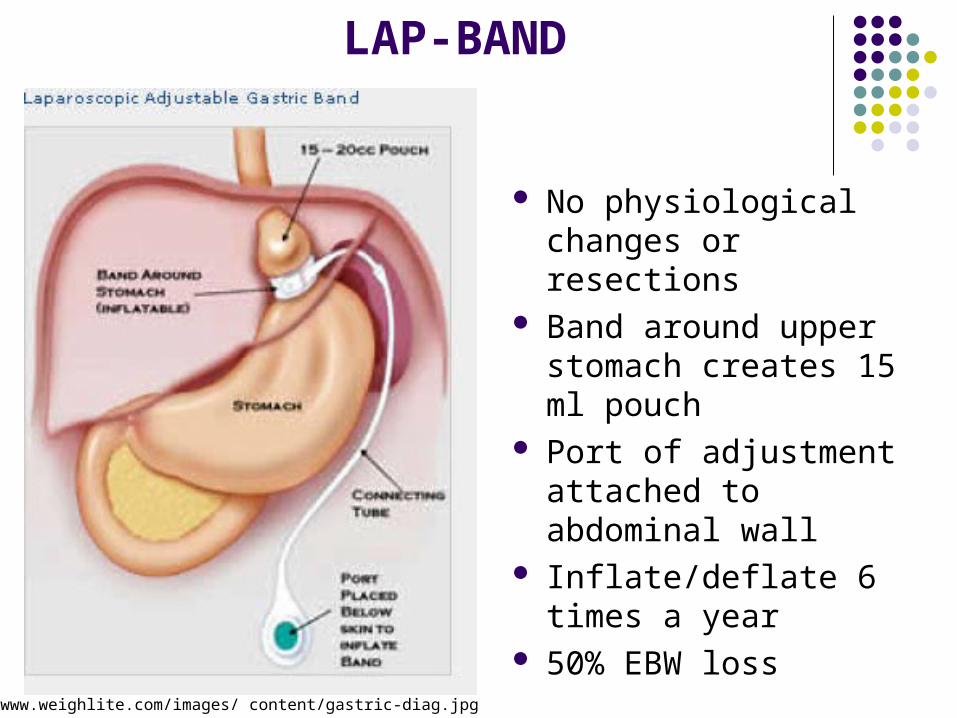
LAP-BAND
No physiological changes or resections
Band around upper stomach creates 15 ml pouch
Port of adjustment attached to abdominal wall
Inflate/deflate 6 times a year
50% EBW losswww.weighlite.com/images/ content/gastric-diag.jpg
Post-surgical Complications
Anastomosis leaks or staple line leaks PE or DVT Cholelithiasis Stomal ulceration Dumping syndrome Constipation
Anastamosis Leaks
Up to 7-10 days after surgery Most common at gastrojejunostomy,
enteroenterostomy, Roux limb stump, staple line Can lead to peritonitis, sepsis, possible death Presentation
Tachycardia, tachypnea Fever Ab pain/back pain Pelvic pressure or rebound tenderness
Anastamosis Leaks
Order Gastrograffin upper GI series Subclinical cases
Bowel rest Parenteral nutrition IV antibiotic if H. pylori
Clinically suspect leak Laparoscopic evaluation and leak repair
Failure to evaluate is the most common cause of preventable, major long-term disability or death in bariatric surgical patients
Pulmonary Embolism
Sudden cause of death up to one month after surgery
20%-30% mortality rate High risk may have vena cava filter
placement prior to surgery Prophylaxis with compression stockings and
LMWH Early ambulation imperitive
Pulmonary Embolism
Presentation Profound hypoxia Hypotension Signs of sepsis
Immediate spiral chest CT Abdominal exploration if too large for
machine No pathology start anticoagulation Too large…….NO SURGERY
Cholelithiasis
Up to 36% of patients within 6 months post-op Bile stasis leads to increased sludge and
gallstones Prophylactic cholecystectomy prior to surgery if
evidence of existing sludge or stones Prevent post-operative disease with concurrent
bariatric surgery and cholecystectomy Prophylactic use of urosidol
Expensive and unpalatable
Stomal Ulceration
12%-15% within 2-4 mos. Post-surgery Etiology
Overabundant acid in pouch leads to excessive acid passing through stoma
Pouch tension and staple line breakdown NSAID use
Presentation Dyspepsia, vomiting Epigastric or retrosternal pain
Stomal Ulceration
Treatment PPI, carafate Antibiotics if H. Pylori Avoid NSAIDS, alcohol, smoking
If no response to treatment Endoscopy Back to surgery for pouch revision or staple
line repair
Dumping Syndrome
More than 15% patients Hypotention Tachycardia Lightheadedness, syncope Flushing Abdominal cramping and diarrhea Nausea and vomiting
Dumping Syndrome
Occurs with high dose simple sugar ingestion Sugar in small intestine causes osmotic overload
and fluid shift from blood to intestine Increased intestinal volume leads to watery diarrhea Decreased blood volume leads to systemic changes Patient education
Eat slowly Avoid drinking before, during and not until 30 minutes after
meals.
Constipation
Most common complaint Causes
Dehydration and decreased fluid intake post-operatively
Increased metabolic water needs Calcium and iron supplement use following
surgery Treat with increased fluids and stool
softeners
Nutritional Consequences
Iron deficiency anemia B12 deficiency Folate deficiency Calcium and Vitamin D deficiency
Not seen with purely restrictive surgeries
Iron deficiency and anemia
Common following RYGB As high as 49% of patients Multifactorial cause
Low gastric acid levels prohibit iron cleavage from food Absorption inhibited because no nutrient exposure to
duodenum or proximal jejunum Decrease in iron-rich food consumption due to intolerance
Treat with oral supplementation of ferrous sulfate or ferrous gluconate
Vitamin B12 deficiency
Up to 70% of patients Lack of hydrochloric acid and pepsin in
stomach Prevents B12 cleavage from food Affects secretion of intrinsic factor, thus B12
absorption Intolerance to meat and milk Oral supplementation usually adequate,
otherwise, IM injections used
Folate Deficiency
40% of gastric bypass patients Complete absorption requires B12 Absorption dependent on HCl and upper 1/3
stomach Deficiency generally caused by decreased
consumption Oral supplementation
Vitamin D and Calcium Deficiency
Vitamin D deficiency is common among obese people
Calcium absorption decreased because duodenum is bypassed
Intolerance to dairy, foods high in calcium Vitamin D is required for Ca++ absorption Prolonged deficiencies lead to
Bone resorption, osteomalacia, osteoporosis Treat with calcium citrate supplementation and 2
weekly doses of Vitamin D
Improvements of Co-morbidities
Type 2 diabetes mellitus Hypertension Hyperlipidemia Degenerative joint disease Sleep apnea GERD
5% to 10% weight reduction is associated with significant decrease in risk
Weight loss from surgery reduces or eliminates medications
Improves severity or resolves co-morbid disease
Improvements of Co-morbidities
2 years after surgery diabetes mellitus was resolved in 83% of pre-operative diabetic patients (Sugerman et. al 2005)
2 years following surgery 69% had resolution of hypertension 8 years post-surgery there was complete relapse
in those with gastric banding 25% decrease in total cholesterol and 40%
decrease in triglycerides 6 to 12 months after surgery
Psychological and Psychosocial Improvements
Depression Low self-esteem and self-appraisal Poor interpersonal relationships Feelings of failure and dissatifaction with life
Subject to prejudice and discrimination
Psychological and Psychosocial Improvements
“ Most obese patients consider impaired QOL the most crippling aspect of their disease, and after surgery consider enhanced QOL the greatest benefit” (Puzziferri 2005).
“Obese individuals would rather have a normal weight with a severe disability such as be deaf, have heart disease, have an amputation and others rather than be obese without any of these conditions” (Livingston 2003).
Psychological and Psychosocial Improvements
Significant improvement in QOL with all types of surgery
New vocational and social activities Improved interpersonal relationships Better moods, self-esteem More employable, get paid more, work more
and take less sick days.
Why do PAs need to know this?
We will be the long-term healthcare provider Consequences and complications last a
lifetime Initial provider assessing signs and
symptoms Track improvements Medication changes Stay educated in all specific needs and
concerns of bariatric surgery patient!