Community Resilience - Home | EMS World · voice, text, photos, data, video clips and stream live...
32
A security guard applies a tourniquet during a simulated earthquake training exercise at a Westminster (CA) mall. Visit us online at EMSWorld.com MARCH 2016 | VOL. 45, NO. 3 $7.00 Developing Community Resilience Casualty Care in the Classroom p. 20 Public Access Bleeding Kits p. 29 The First Care Provider System p. 32 When a Call Turns Violent p. 18 Permissive Hypotension in Trauma p. 44 How Community Paramedics Handle Patient Privacy p. 48
Transcript of Community Resilience - Home | EMS World · voice, text, photos, data, video clips and stream live...

A security guard applies
a tourniquet during a
simulated earthquake
training exercise at a Westminster
(CA) mall.
Visit us online at EMSWorld.com MARCH 2016 | VOL. 45, NO. 3 $7.00
Developing Community ResilienceCasualty Care in the Classroom p. 20
Public Access Bleeding Kits p. 29
The First Care Provider System p. 32
When a Call Turns Violent p. 18
Permissive Hypotension in Trauma p. 44
How Community Paramedics Handle Patient Privacy p. 48

The future of connected care is already in your hands.
Deliver real time situationalawareness for MCI triage,disaster coordination orgroup messaging
Enhance decision supportand document trauma,stroke, burns, refusals,12-leads and more
Telemedicine consults for Mobile Integrated Healthcare and CommunityParamedicine
Telemedicine is driving innovation in healthcare. Now you canenhance patient care by providing your on-scene view directlyto physicians, specialists and hospitals anywhere.
With e-Bridge™ mobile telemedicine apps, share HIPAA-securevoice, text, photos, data, video clips and stream live with confidence and ease using your smartphone, tablet or PC.
Learn how at general-devices.com or call 201.313.7075
Responsive Innovation™ for today’s connected care.
“Here’s the full picture.”
For More Information Circle 10 on Reader Service Card
For More Information Circle 11 on Reader Service Card

4 MARCH 2016 | EMSWORLD.com
Valuable Technology. Valuable Savings.
800.533.0523 www.boundtree.com
Curaplex’s brand new line of needle-free administration and
extension sets utilize innovative, new MicroClave® neutral
displacement technology. This unique needleless connector is
designed to lessen blood reflux within the catheter lumen upon
connection or disconnection to the MicroClave connector, meaning
less risk of infection and improved patient comfort and safety.
• Offers pre-pierced and injection sites
• All luer locking sites provide neutral displacement
• Tubing is standard / macrobore, DEHP-free and latex free
• Each unit is packaged in a plastic pouch
• Select sets come with built-in extension set
For more information contact your dedicated Account Manageror learn more at www.boundtree.com/curaplex-iv.asp
PARTNERS
EDITORIAL ADVISORY BOARDPeter Antevy, MDCEO & Founder, Pediatric Emergency Standards
James J. Augustine, MD, FACEPMedical Advisor, Washington Township Fire Department, Dayton, OH; Clinical Associate Professor, Department of Emergency Medicine, Wright State University, Dayton, OH; Director of Clinical Operations, US Acute Care Solutions
Raphael M. Barishansky, MPH, MS, CPMDirector, Office of Emergency Medical Services, Conn. Dept. of Public Health
Eric Beck, DO, NREMT-PAssociate Chief Medical Officer, American Medical Response
Bernard Beckerman, MD, FACEPAssociate Professor, School of Health and Behavioral Sciences, York College (CUNY), Jamaica, NY
Tom Bouthillet, NREMT-PCaptain, Town of Hilton Head Island (SC) Fire & Rescue Division
Kenneth Bouvier, NREMT-PDeputy Chief of Operations, New Orleans EMS; NAEMT President 2004–2006
Elliot Carhart, EdD, RRT, NRPAssociate Professor, Emergency Services Program, Jefferson College of Health Sciences, Roanoke, VA
Chris Cebollero, NREMT-PSenior Partner, Cebollero & Associates, St Louis, MO
Will Chapleau, EMT-P, RN, TNSDirector of Performance Improvement, American College of Surgeons
Kevin T. Collopy, BA, FP-C, CCEMT-P, NREMT-P, WEMTClinical Education Coordinator, VitaLink/AirLink, Wilmington, NC; Lead Instructor, Wilderness Medical Associates
Michael W. Dailey, MDAssistant Professor, Dept. of Emergency Medicine, Albany Medical College, NY
Thom DickEMS Educator, Brighton, CO
William E. Gandy, JD, LPEMS Educator and Consultant, Tucson, AZ
Erik S. Gaull, NREMT-P, CEM, CPPMaster Firefighter/Paramedic, Cabin John Park (MD) Volunteer Fire Department
Troy M. Hagen, MBA, NREMT-PCEO, Care Ambulance, Orange, CA
Martin Hellman, MD, FAAP, FACEPAttending Physician, Children’s Hospital of Pittsburgh, Pittsburgh, PA
Tim Hillier, Advanced Care ParamedicDirector of Professional Development, M.D. Ambulance, Saskatoon, SK Canada
Lou Jordan PIO, Fire Police Officer, Union Bridge (MD) Fire Department
C.T. “Chuck” Kearns, MBA, EMT-PEMS Consultant
G. Christopher Kelly, JDAttorney at Law, Atlanta, GA; Chief Legal Officer, EMS Consultants, Ltd.
Skip Kirkwood, MS, JD, EMT-P, EFO, CMO Director, Durham County (NC) EMS
Sean M. Kivlehan, MD, MPH, NREMT-P International Emergency Medicine Fellow, Brigham & Women’s Hospital, Harvard Medical School
William S. Krost, MBA, NREMT-PAdjunct Assistant Professor of Emergency Medicine, The George Washington University
Ken Lavelle, MD, FACEP, NREMT-P Clinical Instructor and Attending Physician, Thomas Jefferson University Hospital, Philadelphia, PA
Rob Lawrence, MCMIChief Operating Officer, Richmond (VA)Ambulance Authority
Todd J. LeDuc, MS, CFO, CEMAssistant Fire Chief, Broward Sheriff Fire Rescue, Ft. Lauderdale, FL
Mark D. Levine, MD, FACEPAssistant Professor, Dept. of Emergency Medicine, Washington University School of Medicine; Medical Director, St. Louis (MO) Fire Dept.
Tracey Loscar, NRP, FP-CBattalion Chief, Matanuska-Susitna (Mat-Su) Borough EMS, Wasilla, AK
Craig Manifold, DOEMS Medical Director, San Antonio Fire Department and San Antonio AirLIFE; Assistant Professor, University of Texas Health Science Center at San Antonio
Paul M. Maniscalco, MPA, EMT-PSenior Research Scientist & Principal Investigator, The George Washington University Office of Homeland Security
David Page, MS, NRPDirector, Prehospital Care Research Forum at UCLA; Paramedic, Allina Health EMS; Senior Lecturer, PhD candidate, Monash University
Richard W. Patrick, MS, CFO, EMT-P, FFDirector, Medical First Responder Coordination, Office of Health Affairs–Medical Readiness, U.S. DHS
Tim Perkins, BS, EMT-PEMS Systems Planner, Virginia Office of EMS, Virginia DOH, Glen Allen, VA
Michael E. Poynter, EMT-PExecutive Director, Kentucky Board of Emergency Medical Services
Vincent D. RobbinsPresident & CEO, MONOC, Monmouth-Ocean Hospital Service Corporation, Neptune, NJ
Mike RubinParamedic, Nashville, TN
Angelo Salvucci Jr., MD, FACEPMedical Director, Santa Barbara County & Ventura County EMS, CA
Scott R. Snyder, BS, NREMT-PFaculty, Public Safety Training Center, Emergency Care Program, Santa Rosa Jr. College, CA
Matthew R. Streger, Esq. Executive Director, Mobile Health Services, Robert Wood Johnson University Hospital; Fitch and Associates, LLC, New Brunswick, NJ
Dan Swayze, DrPH, MBA, MEMS Vice President/COO, Center for Emergency Medicine of Western Pennsylvania, Inc.
Cindy Tait, MICP, RN, PHN, MPHPresident, Center for Healthcare Education, Inc., Riverside, CA
John Todaro, BA, NRP, RN, TNS, NCEEEMS/CME Academic Department Coordinator, St. Petersburg College, St. Petersburg, FL
William F. Toon, EdD, NREMT-P EMS Training Manager, Loudoun County (VA) Fire, Rescue and Emergency Management; Battalion Chief - Training (ret.), Johnson County (KS) EMS: MED-ACT
David Wampler, PhD, LPAssistant Professor, Emergency Health Sciences, University of Texas Health Science Center, San Antonio, TX
Paul A. Werfel, MS, NREMT-PDirector, Paramedic Program, Clinical Asst. Professor of Health Science, School of Health Technology & Management, Asst. Professor of Clinical Emergency Medicine, Dept. of Emergency Medicine, Health Science Center, Stony Brook University, NY
Katherine West, BSN, MSEd, CICInfection-Control Consultant, Infection Control/Emerging Concepts, VA
Gerald C. Wydro, MD, FAAEMChief, Division of EMS, Temple University School of Medicine, Philadelphia, PA
Matt Zavadsky, MS-HSA, EMTDirector of Public Affairs, MedStar Mobile Healthcare, Ft. Worth, TX
Published by SouthComm Business Media, Inc PO Box 803 • 1233 Janesville AveFort Atkinson WI 53538920-563-6388 • 800-547-7377Vol. 45, No. 3PUBLISHERScott Cravens, EMT800/547-7377 x1759 [email protected]
EDITORIAL DIRECTORNancy Perry800/547-7377 x1110 [email protected]
SENIOR EDITORJohn Erich800/547-7377 x1106 [email protected]
ASSOCIATE EDITORPepper Jeter800/547-7377 x1628 [email protected]
ASSISTANT EDITORLucas Wimmer800/547-7377 [email protected]
PRODUCTION MANAGERLuAnn Hausz 800/547-7377 [email protected]
ART DIRECTOR Julie Whitty 800/547-7377 [email protected]
AUDIENCE DEVELOPMENT MANAGERJackie Dandoy800/547-7377 [email protected]
ASSOCIATE PUBLISHER - CENTRAL & MIDWESTDeanna Morgan901/[email protected]
BUSINESS DEVELOPMENT MANAGER - NORTHEAST Sandy Domin847/[email protected]
BUSINESS DEVELOPMENT MANAGER - WEST COAST John Heter 503/[email protected]
BUSINESS DEVELOPMENT MANAGER - SOUTHEASTAnn Romens800/547-7377 x1366 [email protected]
ADMINISTRATIVE ASSISTANTMichelle Lieffring 800/547-7377 x1612 [email protected]
LIST RENTALSElizabeth Jackson847/492-1350 [email protected]
Chris Ferrell, CEO Ed Tearman, CFO
Blair Johnson, C00Curt Pordes, VP, Production Operations
Eric Kammerzelt, VP, TechnologyScott Bieda, EVP, Public Safety & Security
Ed Nichols, VP, Public Safety Events
Subscription Customer Service877-382-9187; [email protected] Box 3257 • Northbrook IL 60065-3257
Article reprintsBrett PetilloWright’s Media 877-652-5295, ext. [email protected]
EMS World magazine® (USPS 947-780; ISSN 2158-7833 print) is published monthly by SouthComm Business Media, LLC. Periodicals postage paid at Fort Atkinson, WI 53538 and additional mailing offices. POSTMASTER: Send address changes to EMS World, PO Box 3257, Northbrook, IL 60065-3257. Canada Post PM40612608. Return undeliverable Canadian addresses to: EMS World, PO Box 25542, London, ON N6C 6B2.
Subscriptions: Individual subscriptions are available without charge in the U.S. to qualified subscribers. Publisher reserves the right to reject non-qualified subscriptions. Subscription prices: U.S. $52 per year, $98 two year; Canada/Mexico $72 per year, $139 two year; All other countries $103 per year, $196 two year. Student rate $19 per year. All subscriptions payable in U.S. funds, drawn on U.S. bank. Canadian GST#842773848. Back issue $10 prepaid, if available. Printed in the USA. Copyright 2016 SouthComm Business Media, LLC.
All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recordings or any information storage or retrieval system, without permission from the publisher.
SouthComm Business Media, LLC does not assume and hereby disclaims any liability to any person or company for any loss or damage caused by errors or omissions in the material herein, regardless of whether such errors result from negligence, accident or any other cause whatsoever. The views and opinions in the articles herein are not to be taken as official expressions of the publish-ers, unless so stated. The publishers do not warrant, either expressly or by implication, the factual accuracy of the articles herein, nor do they so warrant any views or opinions offered by the authors of said articles.
For More Information Circle 12 on Reader Service Card

For More Information Circle 13 on Reader Service Card

or the local hospital?Does he need a trauma center
Twenty-year-old male in a motor vehicle accident. Airbag has deployed. Car has significant front-end damage. Is he bleeding internally? Hemorrhage is the leading cause of death after injury.1
The new trauma parameters on the ZOLL X Series® help you accurately and quickly assess your patients so you can feel confident in your treatment decisions.
Insight for informed decisions.www.zoll.com/trauma
©2015 ZOLL Medical Corporation, Chelmsford, MA, USA. X Series and ZOLL are trademarks or registered trademarks of ZOLL Medical Corporation in the United States and/or other countries.
1Acosta JA, et al. Journal of the American College of Surgeons. 1998;186(5):528-533. MCN EP 1508 0110
For More Information Circle 14 on Reader Service Card8 MARCH 2016 | EMSWORLD.com
44
20
40
FEATURES
40 Response to Atypical Incidents: New Demands for EMSComplex new challenges and threats hold more danger for EMS providersBy Mac Kemp, MSs, MEd, EMT-P
44 Permissive Hypotension in Trauma Permissive hypotension can be a viable strategy in the prehospital setting when used appropriatelyBy Hawnwan Philip Moy, MD, & Abigail Cosgrove, MD
48 Protecting Patient Privacy in Community Paramedic Programs Amid HIPAA and other rules, how should you approach the need to share protected health information?By Anne M. Jensen, BS, EMT-P
53 Product Applications from the FieldInterviews with end-users of EMS products and services
COLUMNS
15 LUDWIG ON LEADERSHIPChecks and BalancesBy Gary Ludwig, MS, EMT-P
16 GUEST EDITORIALWhy You Need to Prepare for EMS 3.0By Matt Zavadsky, MS-HSA, EMT
18 CASES WITH A TWISTWhen a Call Turns ViolentBy David Page, MS, NRP, & Will Krost, MBA, NRP
58 THE MIDLIFE MEDIC9 SecondsBy Tracey Loscar, NRP, FP-C
DEPARTMENTS10 EMS World Online
12 From the Publisher
14 News Network
56 Ad Index
57 Classified Ads
LETTERS TO THE EDITOR: Letters may be edited for clarity or space. E-mail [email protected].
SUBMISSIONS: E-mail queries, manuscripts, press releases and news items to [email protected].
PERMISSIONS: E-mail requests to [email protected].
CONTAC T USfacebook.com/emsworldfans twitter.com/emsworldnews
linkedin.com/groups?gid=1853412 youtube.com/EMSWorld
MARCH 2016 VOL. 45 | ISSUE 3
Cover photo courtesy First Care Provider
20 Casualty Care in the ClassroomInside the MercyRockford Health System’s hemorrhage control program for schools
By G.B. Jones, Karen Schulte, EdD, James J. MacNeal, DO, & Christopher Wistrom, DO
29 The Argument for Public Access Bleeding KitsIf the pros can’t get there fast enough, how can we stop exsanguination?
By Peter Antevy, MD
32 The First Care Provider SystemWhy civilians should be prepared to act in mass-trauma events
By Joshua P. Bobko, MD, William J. Harris, NREMT-P, & Stuart Thomas
COVER REPORT: DEVELOPING COMMUNITY RESILIENCE

MOULAGE OF THE MONTH
NEW
VIDEOS
Bobbie Merica continues her guide to simulating injuries and illnesses through effective use of moulage. This month: Industrial explosion, impaled shrapnel.See EMSWorld.com/12166918.
FEATURES
The Narcan Monologues >> EMSWorld.com/12166441When a Weymouth, MA firefighter proposed letting drug addicts die in a Facebook post in January, responses ranged from sympathy for the firefighter to sympathy for his patients. See what Mike Rubin has to say about that in the March edition of Life Support.
Social Workers at the Station >> EMSWorld.com/12166308An innovative partnership between SourcePoint, a community support organization for seniors 60 and older, and local fire departments is helping to reduce the number of nonemergent EMS runs throughout Delaware County, OH.
Month in Review >> EMSWorld.com/12166919 If you’re looking to catch up with the latest news, most popular articles and EMS chatter on social media, check out EMS World’s new Month in Review column for a handy roundup of the top headlines.
twitter.com/emsworldnews
WEBCASTS
Visit EMSWorld.com/webca sts to register for upcoming presentations:March 2 at 2 pm ET: Maximizing Your Revenue: The Critical Link Between Documentation, Reimbursement & Compliance Find out how you can reduce your documentation errors on patient care reports to more accurately describe the patient’s condition and the care you provide, thus reducing your risk of a lawsuit. The webinar will also cover the importance of accurate and complete documentation that “paints a picture” of the patient’s condition so your organization can seek the proper level of reimbursement that is so critical to the financial health of your EMS agency.
Presented by Steve Wirth, a founding partner of Page, Wolfberg & Wirth, LLC. Sponsored by ZOLL.
www.linkedin.com/groups?gid=1853412facebook.com/emsworldfans
Real Patient Video of the Week >> EMSWorld.com/12081461ReelDx, in partnership with EMS World, offers a game-changing collection of brief real-patient videos, captured in the field by practicing EMS professionals. ReelDx videos help EMTs and paramedics keep their skills current and their training fresh through exposure to a range of conditions that may not otherwise be seen in their communities.
EMS World Expo: See What Everyone Is Saying >> EMSWorld.com/12163092The largest EMS conference and trade show in North America is coming to New Orleans, October 3-7, 2016.
10 MARCH 2016 | EMSWORLD.com
THE MOST IMPORTANT COURSE OF SOMEONE’S LIFEThe AHA’s NEW BLS offerings provide the foundation for saving lives in cardiac arrest. BLS has been updated with the latest science and education from the 2015 AHA Guidelines Update for CPR and Emergency Cardiovascular Care.
The new course teaches skills for application in both prehospital and in-facility environments, with a focus on components of high-quality CPR like chest compression fraction and team dynamics.
Master critical skills you need in emergency response situations, depicted in real-world scenarios and the varied environments you encounter.
Updated Courses. Realistic Scenarios. Adaptable Classes.
CLASSROOM
eLEARNING BLENDED
CLASSROOM
eLEARNING BLENDED
TWO WAYS TO LEARN
Instructor-Led Cognitive and psychomotor training in a classroom
BlendedA combination of eLearning and a hands-on session
Take the new BLS Course today!
©2016, American Heart Association. DS10072 2/16
Visit cpr.heart.org/BLS to learn more about the NEW BLS!
Updated to reflect
For More Information Circle 15 on Reader Service Card

FROM THE PUBLISHER By Scott Cravens, EMT
12 MARCH 2016 | EMSWORLD.com
The Breakthrough Treatment for Non-Compressible Hemorrhage
Injectable Hemostatic Device
Now Cleared for Civilian Use
Phot
o by
: Bra
d G
ilpin
*For deep, narrow tract junctional wounds
XSTAT – For the control of severe, life threatening bleeding from junctional wounds in the groin or axilla:• Stops bleeding in seconds with rapidly expanding sponges.• Developed in collaboration with U.S. Special Operations Forces.• Recommended by the Committee for Tactical Combat Casualty
Care (CoTCCC). *
For More Information Circle 16 on Reader Service Card
A Whole Community Response A Mesa Fire and Medical Department trial is improving patient care while decreasing costs
A year and half ago the Mesa (AZ) Fire and Medical
Department (MFMD) received a $12.5 million CMS grant to
fund a three-year trial dedicated to improving care and low-
ering costs by more effectively managing low-acuity calls.
The “Mesa Community Care Response Initiative” sends a nurse
practitioner or physician assistant—along with a captain/paramed-
ic—to examine and treat patients in the field without transporting
them to the emergency department. The call center flow chart
illustrates how calls are processed. The program aims to increase
patient satisfaction, decrease ED and EMS transport costs, make
more efficient use of MFMD resources and lessen ED overcrowding.
I recently met with the architect of this innovative approach,
MFMD Medical Director Gary Smith, along with Fire Chief Harry
Beck, who is tasked to implement it.
High- or Low-Acuity?The first question is, “Is this a high-acuity call?” If yes, MFMD sends
out a four-person ALS company. If the answer is no, the call trans-
fers to an RN employed by MFMD to triage. Both Smith and Beck
believe this RN triage component will be the cornerstone of a
future telemedicine rollout. That program would involve another
partnership as well, this time with local physician groups to provide
after-hour physician calls.
“One of the things we picked up on pretty quickly,” says Beck,
is that, “anything we can do to interrupt or prevent a 9-1-1 call is a
process that we should be involved in.” An effective nurse triage
line will reduce frequent callers and improves patient care.
Unit TypesTransitional response vehicles—four units staffed with an EMT
captain and ALS firefighter—manage the low-acuity calls and
keep ALS units available for bigger emergencies.
The community care unit (CCU) is staffed by a NP or PA, while
the community care specialialists (CCS) unit is staffed by a
licensed social worker and captain/paramedic.
The CCUs are reporting a 64% diversion rate from the ED and the
CCS behavioral units are even higher. Both the CCU and CCS are a
result of non-FD community partnerships. Mountain Vista Medical
Center supplies the nurse practitioners and physician sssistants,
while CPR (Crises Preparation and Recovery, Inc.) supplies the
licensed clinical social worker who delivers the patient with a full
psychological work-up at the time of delivery to the psych center.
“By sending an advanced practice PA/NP you now have the
‘power of a prescription pad’ because they can take care of the
individual right then,” says Smith.
MFMD has also added i-STAT handheld blood analyzers to the
advanced practice ambulance, so practitioners can get an out-
patient basic metabolic panel. “We get an H&H (hemoglobin and
hematocrit) to determine if the patient is anemic. We are adding
lactate to that so we can go out on sepsis calls. Sepsis is now
a core measure for CMS, because of the high readmission rate,”
notes Smith.
The Power of PartnershipsSmith credits partnerships between healthcare entities as criti-
cal to the success of the program. His ultimate goal is to create a
model that can be reproduced throughout the healthcare system.
An added bonus to the integration with allied healthcare provid-
ers is the opportunity for current paramedics to grow into some of
the advanced healthcare roles.
For more information on the MFMD system, visit EMSWorld.
com/12167512.
© G
ary A
. Sm
ith, M
D, 2
013,
Mes
a Fi
re/M
edic
al D
epar
tmen
t
Caller Communications Center
Mid-LevelProvider
No
Yes
Treat/TransportMost Appropriate Facility Treat/Refer
AdvancedParamedic
Medical Direction
4 Person ALSCompany
BLS TransitionalResponse Vehicle
BehavioralHealth Provider
RN/SocialWorker
Scheduled
Triage RNHigh Acuity
Unscheduled
Mesa Fire and Medical Department Chief Harry Beck with Medical Director Gary Smith, MD

Advocates in Canada Demand Legislation to Stem Responder SuicidesStakeholders recently gathered to discuss solutions
Bob Baillie barely reacted when he received his
dispatch instructions. A paramedic for 13 years,
he has responded to nearly every 9-1-1 call
imaginable, but he sensed something was dif-
ferent as he approached the lobby of the hotel where a
woman had been found without vital signs. “I’m sorry
you have to see this,” Baillie recalls a police officer say-
ing to him. Upstairs, his colleague lay dead of helium
asphyxiation, a carefully planned method of suicide.
The ride back to base was silent between him and
his partner, Baillie recalls, and he felt a profound sense
of being disconnected from reality. Baillie had seen
firsthand what most paramedics, police officers and
fire fighters knew only as rumor: First responders kill
themselves in alarming numbers.
A Sense of UrgencyThirty-nine first responders died by suicide in 2015
according to the Tema Conter Memorial Trust, a Cana-
dian organization that supports first responders with
mental health illnesses such as PTSD.
“We’ve already had five first responder suicides this
year,” says Director Vince Savoia. According to data
tracked by Savoia, PTSD was diagnosed in 60% of
those who died by suicide.
While all first responders can be affected, two para-
medics took their own lives at the end of January, and a
sense of urgency has heightened within the paramedic
community, where the prevalence of PTSD is highest.
“Some employers are known to terminate paramed-
ics with PTSD, so no one comes forward and asks for
help,” says Savoia.
While the stigma around PTSD in the first responder
community is improving, Savoia states that treatment
options are expensive and recovery is slow. The Trust
is advocating for changes to legislation so that men-
tal healthcare is covered by OHIP (the Ontario Health
Insurance Plan) and the Workplace Safety and Insur-
ance Board.
Savoia asks: “Why can I go to the ED and get my
broken leg fixed, but if I need counseling, I have to pay
out of pocket?”
For seven years advocates have been calling for
presumptive causation legislation that would make
PTSD a workplace injury. “The issue of legislating pre-
sumptive causation and funding tools for taking care of
paramedics in Ontario is one of our three top priorities,”
says Geoff McBride, president of the Ontario Para-
medic Association. “It can’t happen soon enough. It
is time for people who care for others to be cared for.”
Progress, says McBride, is slow but steady. Through
education and popular media, people are realizing
that mental illness is like any other illness, like a bro-
ken bone. McBride thinks we have reached a tipping
point: “It is becoming easier to talk about mental ill-
ness among colleagues, but governments need to act.”
Stakeholders Gather for National RoundtablePoliticians seem to be taking notice. Canadian Prime
Minister Justin Trudeau has promised to develop a
suicide prevention program for the Canadian Forces,
and Public Safety Minister Ralph Goodale has a man-
date to develop a “coordinated national action plan on
post-traumatic stress disorder, that disproportionately
affects public safety officers.”
Funding has been promised for PTSD research to
the amount of $20 million and in January, stakeholders
gathered at a national roundtable in Saskatchewan to
discuss solutions.
On February 1, 2016, the Province of Ontario
announced a strategy to help reduce the incidence
of PTSD and suicide among first responders. Yasir
Navqi, minister of community safety and correctional
services, oversees first responders in Ontario. “We have
all seen the devastating and far-reaching impacts of
PTSD on our first responders” he said in a statement,
adding that the Liberal government is “sending a strong
signal today that we have a comprehensive approach”
to ensure first responder well being. That approach has
both “preventative and legislative components,” says
Minister of Labour Kevin Flynn. While unable to offer
specific details until a bill is formally introduced later
this month, the Ministry of Labour says it is taking a
very “serious look at presumptive benefits.”
Cheri DiNovo, a member of the provincial parliament
from the New Democratic Party, says, “Good intentions
aren’t what’s needed, what’s needed is action.”
People are realizing that
mental illness is like any
other illness, like a broken
bone.
cont. on page 56
NEWS NETWORK By Blair Bigham, MD, EMT-P, MSc
14 MARCH 2016 | EMSWORLD.com

Request Free Information at www.emsworld.com/e-inquiry
ADVERTISER INDEX
cont. from page 14
COMPANY PAGE INQ #
Airon Corporation 31 25
American Heart Association 11 15
Bound Tree Medical, LLC 5 12
Compression Works LLC 35 27
Emergency Medical Products 26 22
EMS World EXPO 33
ENGEL USA 38 31
Everglades University 35 28
Firehouse EXPO 52
Gaumard Scientific 60 40
GD 3 11
Graham Professional Medical 37 29
Journal Of Special Operations Medicine
2 10
Lenoir Community College 30 24
COMPANY PAGE INQ #
Mangar International 22 18
Minto Research and Development
25 21
NAEMT 17 17
Nasco 24 20
National Awards of Excellence 28
North American Rescue Products 6-7 13
Pyng Medical Corp 59 39
Rescue Essentials 23 19
RevMedX, Inc 13 16
Simulaids Inc 34 26
SWAT-T 37 30
Taylor Healthcare Products 27 23
World Trauma Symposium 39
ZOLL 9 14
NEWS NETWORK
56 MARCH 2016 | EMSWORLD.com
The sponsor of five private member bills over seven years—all
of which failed—DiNovo says that PTSD must be recognized as a
workplace injury as it is in Manitoba and Alberta. “If the govern-
ment doesn’t recognize PTSD as a problem, why would employ-
ers?” she questions when asked about municipalities terminating
paramedics with PTSD.
Less Talk, More ActionUntil legislation is passed that facilitates the delivery of mental
health services to the paramedics who need it, paramedic Natalie
Harris will continue fighting for change.
Harris was on the road in 2012 when she was dispatched to a
9-1-1 call for two women who had been brutally murdered. “I was
aware that I would see horrible things, but was not prepared for
the mental turmoil I felt when I saw firsthand the evil humans are
capable of,” she says. Harris became depressed and suicidal, turn-
ing to alcohol. The day after she testified at the murder trial, she
overdosed and stopped breathing. She spent the next year in and
out of hospitals and treatment programs. As part of her therapy,
Harris started to blog about her journey. “My blog gave me free-
dom from the grip mental health stigma had on me,” she recalls.
Harris is now a globally renowned advocate for first responders
who suffer from PTSD.
McBride is pleased to see politicians holding summits and
releasing press releases but remains skeptical.
“We’ve talked this thing to death…what we need now is less talk,
more action,” he says.
Harris and Baillie agree. They go to work on the road every day,
wondering if the next call will bring trouble for themselves or a
colleague.
“We won’t get rid of suicide,” acknowledges Savoia, “but when
we peel away the emotion, what people are truly asking for is to
be seen, heard and understood. It’s that simple.”
That’s why Savoia offers first responders a crisis line staffed by
trained professionals at 888/288-8036.
While governments talk about PTSD, DiNovo sits in her Queens
Park office, hearing about yet another paramedic who took his
own life. “I don’t know what we’re waiting for…how many deaths
will it take?” she says.
AB O U T THE AU TH O R After a decade working as a helicopter paramedic, Blair Bigham, MD, EMT-P, MSc, completed medical school in Ontario, Canada, where he is now a resident physician in the emergency department. After completing his Masters of Science at the University of Toronto, Blair worked as an associate scientist at St. Michael’s Hospital in the fields of resuscitation science, knowledge translation and patient safety. E-mail him at [email protected] or follow him on Twitter at @BlairBigham.

Any form of theft eats away at the
confidence the public has in your
organization.
Check s and BalancesAs an EMS leader, it is your responsibility to prevent theft
©Bigstock.com/ratch0013
LUDWIG ON LEADERSHIP By Gary Ludwig, MS, EMT-P
EMSWORLD.com | MARCH 2016 15
Ioften scan the headlines on websites like
EMSWorld.com to see the latest happenings
in the EMS community. In mid-January, I saw a
headline I have seen before, yet it disturbs me
every time: It concerned a former EMS director and
his wife arrested after an audit uncovered miss-
ing funds. In this case, an EMS director of a county
service in Arkansas and his wife, who served as
the bookkeeper, were accused of stealing nearly
$700,000 from the EMS service over a five-year
period. An audit discovered the missing money.
Sadly none of the 34 employees in the service had
received a pay increase in four years.
Just do a Google search and you will see this is not
an uncommon occurrence in EMS. One of the largest
I found on a search for this column was the theft of
$1.6 million over a seven-year period by the treasurer
of a volunteer EMS organization in Long Island, NY.
This averaged out to about $230,000 a year.
It appears that theft and embezzlement in EMS
organizations occurs quite often. The sad part is that
we are entrusted by the public with their confidence
and, even though those who steal are not reflective
of the entire profession, their actions form the basis
of public opinion and can erode confidence.
Former President Ronald Reagan coined the
phrase, “Trust but verify” when talking about his rela-
tionship with the Soviet
Union on nuclear
negotiations. The
same is true for those
who are allowed to
handle money for
EMS organizations.
There should be
checks and bal-
ances in place
for anyone who
handles money
in an EMS organi-
zation. If a bookkeeper or treasurer is insulted by this,
then tough! It is not a question of their honesty; it is
a question of maintaining the public trust. Besides,
if a bookkeeper or treasurer has nothing to hide, they
should not be bothered by checks and balances.
Any money that comes into an EMS organization
should be put into a checking account. If you have
someone who does your billing for you, have them
transfer the money directly into your account instead
of sending a check. The inverse is true: Any money
that leaves the EMS organization should be taken
out of a checking account. This documentation of
receivables and payables cannot be tampered with
since it is all controlled by the bank. This documenta-
tion is important later for reconciling the amount of
money an EMS organization has and can help with
auditing processes.
If possible, you should have at least two different
employees handling payments going out. Unless
they collaborate, they cannot set up a fake vendor,
authorize payments and issue checks. The same
goes for issuing payroll checks to employees. There
have been cases of paramedics being intentionally
overpaid and the difference being split between the
bookkeeper and the paramedic.
As the EMS manager, you should periodically
review your books. Randomly pull a transaction and
ask that the bookkeeper run you through the process
of how the invoice was received, paid and recorded.
Ask questions of any transactions or vendors you do
not recognize.
Finally, you should have a periodic independent
audit conducted of your financial transactions. It
does not have to be a full-blown audit, but some-
times spot audits can catch wrongdoings. Even the
knowledge that periodic audits will be done by a
third party is enough to keep people honest.
The protection of the funding that operates and
helps your EMS organization function is essential.
Any form of theft or embezzlement also eats away
at the confidence the public has in your organization.
Even though theft may not have anything to do with
patient care, any public knowledge of the theft can
transcend into the public’s confidence in all aspects
of the EMS organization.
Do all you can to prevent thefts of monies in your
EMS organization.
AB O U T THE AU TH O R Gary Ludwig, MS, EMT-P, is chief of the Champaign (IL) Fire Department. He is a well-known author and lecturer who has managed award-winning metropolitan fire-based EMS systems in St. Louis and Memphis. He has a total of 37 years of fire and EMS experience and has been a paramedic for over 35 years. Contact him at garyludwig.com.

EMSWORLD.com | MARCH 2016 1716 MARCH 2016 | EMSWORLD.com
GUEST EDITORIAL By Matt Zavadsky, MS-HSA, EMT
Market forces will dictate that we
re-evaluate every aspect of EMS
delivery through a different lens—
the lens of value.
Why You Need to Prepare for EMS 3.0Are you ready for the unprecedented transformation within our healthcare system?
For the past few years, the EMS profession
has focused on developing mobile integrat-
ed healthcare and community paramedicine
(MIH-CP) programs as a way to offer added
value to our stakeholders in a healthcare system that
is undergoing an unprecedented transformation. But
the changes necessary to survive—or even thrive—
during this healthcare transformation transcend
beyond MIH-CP. Market forces will dictate that we
re-evaluate every aspect of EMS delivery through a
different lens—the lens of value.
This healthcare transformation is being referred to
as “Healthcare 3.0.” Use of the term “3.0” by health-
care system leaders represents the understanding
that the healthcare system is in its third phase of
evolutionary transformation, and that there is likely
to be more change in the future (4.0, etc.).
Almost everything you read regarding “Healthcare
3.0” references that “the new normal” is based on a
value proposition, primarily economic value. Things
like pay-for-performance, outcome-based pay-
ments, bundled payments based on episodes of
care, accountable care organizations, shared-risk
contracting, penalties for adverse outcomes such
as readmissions or healthcare-acquired infections,
financial bonuses for reporting outcome data (and
penalties for not reporting it), and externally mea-
sured patient satisfaction scores have all had a sig-
nificant impact on hospitals, home health agencies,
skilled nursing facilities and physicians.
The rapid consolidation of healthcare payers and
healthcare providers, and mergers of managed care
giants such as Cigna with Anthem and Aetna with
Humana, will likely lead to a handful of oligopolistic
payers. Acquisition activity on the provider side of
the equation has been equally dramatic with hos-
pital system mergers, hospitals buying physician
groups, physician groups acquiring other physician
groups, hospitals buying pharmacy chains, phar-
macy chains merging and hospitals acquiring urgent
care centers.
All this activity seems centered around improv-
ing negotiating power based on larger populations
controlled by providers and payers. It may be likely
that we will eventually have a few payers negotiating
population-based shared-risk contracts with just a
few integrated providers.
Ask Tough QuestionsHow all these changes will impact EMS is relatively
predictable—all we have to do is look at what’s
happened to our fellow healthcare providers and
begin preparing ourselves for the third evolutionary
transformation for EMS, or what we could refer to
as “EMS 3.0.” And, like Healthcare 3.0, we need to
base EMS 3.0 on the value proposition we bring to
our stakeholders.
In order to do this, we have to answer some dif-
ficult questions like:
» Do we own a space in the healthcare system?
If we do, what is it? Why are we uniquely positioned
for that space?
» Is EMS safe? What is the adverse outcome rate
when EMS treats a patient? How many times when
we don’t transport a patient do they end up in the
ED hours later?
What is the economic value we bring to the
patients, payers and our healthcare partners? Are
we economically incentivized correctly to focus on
patient outcomes?
» What is the clinical value (peer reviewed and
published) we bring to the patient? Did the fact that
the patient called 9-1-1 for “x” condition make a dif-
ference in the patient’s outcome?
» Who should really be paying for EMS? And what
should they actually be paying for?
» Are our practitioners educated and credentialed
for the role they should be playing in the healthcare
system? Is a 750-hour paramedic course the right
training, or should EMS practitioners have more edu-
cation than a hairdresser?
» What does it actually cost to deliver EMS? And
if one service delivery model costs “x” and another
costs two times “x,” can they prove that the value
they bring is worth the extra cost?
» Should accreditation, or conditions of partici-
pation, be required of EMS agencies to be eligible
for reimbursement like other healthcare providers?
Is that the best way to deal with widely published
fraud and abuse issues in EMS?
Become InformedThe good news is that leaders from several EMS
associations are focusing on finding the answers
to these questions and providing specific target-
ed learning opportunities that will help keep you
informed:
» The National Association of EMTs is hosting The
EMS Transformation Summit: Welcome to “EMS 3.0”
on April 18 in Washington, D.C., preceding EMS On
The Hill Day.
» The National Association of EMS Physicians,
the National Association of EMS Educators, the
National EMS Management Association, the Ameri-
can Ambulance Association, the National Associa-
tion of EMTs and others are developing a transfor-
mation strategy to align the industry’s focus to help
our profession transform to EMS 3.0.
» The Academy of International Mobile Health-
care Integration (AIMHI) will be conducting a series
of face-to-face educational sessions and webinars
on high-performance EMS and EMS integration into
the rest of the healthcare system.
» EMS World Expo will have a dedicated EMS 3.0
Transformation track for leaders and providers to
attend and equip themselves with the knowledge
necessary to survive the next five years in EMS.
» The Promoting Innovation in EMS project,
headed by Drs. Kevin Munjal and James Dunford,
will release its work on ways to remove barriers to
innovation in EMS.
Your mission is to become a change agent. Read
everything you can, attend as many national confer-
ences as possible, subscribe to e-mail distribution
lists, join national associations and engage in the
conversation. Most of all, participate in driving the
necessary changes for EMS to thrive over the next
five years.
AB O U T THE AU TH O R Matt Zavadsky, MS-HSA, EMT, is the public affairs director
at MedStar Mobile Healthcare, the exclusive emergency and non-emergency EMS/MIH provider for Fort Worth and 14 other cities in North Texas. Matt has helped guide the implementation of several innovative programs with healthcare partners that have transformed MedStar fully as a mobile integrated healthcare provider.
Tactical Combat Casualty Care (TCCC): only TCCC course endorsed by the American College of Surgeons; uses PHTLS military textbook; 16 hours of CECBEMS credit. Two day course for MEDICAL military personnel.
NEW! Tactical Combat Casualty Care–All Combatants (TCCC-AC): 8-hour course created by the Committee on TCCC. One day course specifically for NON-MEDICAL personnel.
NEW! Tactical Emergency Casualty Care (TECC): endorsed by the American College of Surgeons; meets TECC guidelines; uses PHTLS military textbook; teaches civilian tactical EMS. 16 hours of CECBEMS credit.
Law Enforcement and First Response Tactical Casualty Care (LEFR-TCC): for all public safety first responders; based on TCCC and PHTLS. 8 hours of CECBEMS credit.
Bleeding Control for the Injured (B-Con): teaches basic lifesaving medical interventions to first responders and civilians; meets recommendations of the Hartford Consensus. 2.5 hours.
NAEMT Sets The Standard In Tactical Casualty Care Training
VISIT NAEMT.ORG/EDUCATION | EMAIL [email protected] | CALL 1-800-34-NAEMT
For More Information Circle 17 on Reader Service Card
For more information on The EMS Transformation Summit: Welcome to “EMS 3.0,” visit naemt.org.
For more information on EMS World Expo, scheduled for October 3–7 in New Orleans, LA, visit EMSWorldExpo.com.

CASES WITH A TWIST By David Page, MS, NRP, & Will Krost, MBA, NRP
EMSWORLD.com | MARCH 2016 1918 MARCH 2016 | EMSWORLD.com
When a Call Turns ViolentThere are strategies you can take to mitigate your risk of becoming a victim of violence
Woman tries to stab Pennsylvania medic in the
chest; two Detroit paramedics stabbed and slashed in
the face; EMTs shot at, ambulance stolen in Alabama;
chief calls stabbings “near-death experience.”
All of these headlines have one thing in common—
they all happened in 2015, along with many similar
events.
Violence against police receives a lot of media
attention. What about violence against EMS provid-
ers? The public often does not view EMS as a tar-
get for violence, and event reporting and tracking is
sporadic at best. In this article we review a recent
attack and outline strategies to mitigate our risk of
becoming victims of violence.
Case PresentationOn Wednesday, November 25, 2015, at 10:38 p.m.,
an EMS crew responded to a domestic violence call.
On scene they began treating their patient when
a woman holding a knife lunged at the EMS crew
yelling, “I’m going to kill you.” She stabbed one of
the crew members in the chest and slashed at his
abdomen.
The second crew member had the presence of mind
to reach for the orange trouble button on his radio. He
pressed it, tripping the radio’s silent alarm and trans-
mitting a state of emergency to their dispatcher.
Fortunately the EMT who was attacked was wear-
ing a protective body armor vest, which is still rela-
tively uncommon in EMS. The vest blocked the knife,
and the responder did not sustain any injuries from
the initial stabbing attempt.
Unfortunately accidental trips of the orange but-
ton are common in that system, so dispatchers are
forced to check on the crew before sending help.
You can imagine the look of dismay on the crew and
assailant’s face when the radio chirped: “Ambulance
10, reset your trouble button, we are getting a false
alarm up here.”
The assailant, upon hearing the dispatcher’s radio
reply, became angry and struck the face of the crew
member holding the radio. The radio flew out of the
hands of the crew member and a struggle for surviv-
al in close quarters ensued. The lack of a follow-up
reply after two more unanswered radio transmis-
sions did eventually prompt the dispatcher to send
additional help. It is lucky neither crew member sus-
tained career- or life-ending injuries.
The FactsThe risk of non-fatal assault resulting in lost work
time among EMS workers is 0.6 cases per 100 work-
ers a year; the national average is about 1.8 per
10,000 workers. This means the relative risk of non-
fatal assault for EMS workers is roughly 30 times
higher than the national average. Over a five-year
period during which 91 line-of-duty fatalities were
identified, 10 (9%) were violence related. The rela-
tive risk of fatal assaults for EMS workers is about
three times higher than the national average.
From the first day of EMT school, we focus on
“gloves on, scene safe.” While it’s great that this is
at the top of our skills evaluations, it is often a check-
mark that is quickly and definitively answered by the
evaluator saying, “it’s safe,” and that mind-set then
never changes.
In our opening scenario, it appeared exactly that
way on arrival and the responders believed the scene
was safe. Unfortunately, scene safety is never static
or clear cut. The level of risk always varies as a call
naturally evolves. In this case, the violent action was
rapid and lethal.
Hindsight is 20/20 and the facts from
this case—along with multiple other
incidences of violence against our col-
leagues—may lead many of us to blame
the crew for letting their guard down, or
a complacent dispatcher for not react-
ing immediately to the call for help. But
in a culture of safety, a root cause analy-
sis would set up processes with multiple
redundancies that account for human
errors and ensure a systematic response
focused on safety. In this case, waiting for
or arriving with police to a high-risk event
(domestic dispute call), wearing body
armor, and maintaining radio systems
and protocols so help can be summoned
quickly are all key processes.
Current TrendsThe increase in attacks on EMS providers
is causing some systems to evaluate their
preparedness.
Cleveland EMS cited national trends
as its reason for mandating the use of
bullet-proof vests by anyone responding
to any emergency call. The use of vests is
not entirely new to Cleveland EMS; they
have had a policy in place since 1990 that
required the use of these vests in “high-risk”
responses. While not all services can afford
vests, a thorough risk assessment should be
undertaken to determine strategies neces-
sary for ensuring personnel safety.
Another example of protective strate-
gies comes from New York City, where
officials established the “Assaults Against
Paramedics and EMTs” initiative. In this ini-
tiative, legislators and city administration
have established more stringent process-
es for prosecuting those who attack EMS
personnel.
Additional strategies that mitigate the
risk of violence to EMS providers include:
» Concurrent dispatching of police in
all high-risk calls (e.g., suicide, homicide,
domestic violence, intoxication, psychiatric
illness).
» Staging at a remote location for high-
risk calls until police have secured the
scene.
» Uniforms that clearly identify EMS as
separate from law enforcement.
» Continuous education in the use of de-
escalation strategies.
» Continuous education in the use of
physical restraints if necessary (and how
to determine when necessary).
» Establishing a different set of triage
and treatment priorities if the EMS service
supports law enforcement or responds to
tactical operations.
» Advanced tactical training and defen-
sive skills for close combat encounters.
References for this article are available
online at EMSWorld.com/12166008.
ABOUT THE AUTHORS David Page, MS, NRP, is director of the Prehospital Care Research Forum at UCLA. He is a senior lecturer and PhD candidate at Monash University. He has over 30 years of experience in EMS and continues to be active as a field paramedic for Allina Health EMS in the
Minneapolis/St. Paul area.
Will Krost, MBA, NRP, is a fourth-year medical student and a faculty member at the George Washington University School of Medicine and Health Sciences in the Departments of Clinical Research and Leadership and Health Sciences. He has over 23 years of experience in EMS
operations, critical care transport and hospital administration.
CRM TipsIdentify the improbable or
unpredictable: In EMS we are constantly considering the worst-case scenario. Scene evaluation should ask that same question. In this case, responding to a domestic dispute should create more intentional situational awareness.
Post-event review: In a rapid “hot-wash” or more extensive analysis it is crucial we evaluate our performance on difficult cases. Discussing facts and identifying—in a non-blaming, non-judgmental way—different outcomes and processes that worked and those that did not will help prevent the same scenario from occurring again.
Editor’s note: Cases
are obfuscated
and amalgamated
to protect patient
privacy and provider
anonymity. While
staying as true as
possible to the actual
event, creative license
is used to better
explain the lesson(s)
in the case.
The use of de-escalation techniques is one strategy to defuse the potential for violence.
Please help us identify errors and near-miss events that affect the safety of EMS providers and patients. Report events anonymously at www.emseventreport.com.
E.V.E.N.T. is an anonymous tool designed to improve the safety, quality and consistent delivery of EMS. The data collected will be used to develop policies, procedures and training programs.
REPORT EVENTS

The audience was deliberately chosen to include not only local law enforcement, but also cross-disciplinary, multijurisdictional representatives from all stakeholders who would be impacted by a significant active-shooter event at a local elementary school.
Participants included elected and appointed city offi-cials, city and county law enforcement, emergency dis-patchers and representatives from the fire department, EMS, public works, transportation services, the district attorney’s office, the coroner’s office, public information officers, emergency managers, school district leaders and members of the local medical community.
The purpose of the exercise was to discuss, in depth, how each of the interdependent agencies would function together to prepare for and respond to an active-shooter event.
Several “do-outs” and “take-aways” were identified dur-ing the exercise, but there was perhaps nothing more significant than the exchange between Chris Wistrom,
DO, associate EMS medical director for MercyRock-ford Health System’s emergency medical services, and Yolanda Cargile, EdD, director of student services for the Janesville School District, regarding a key question: “What happens for medical care from time of injury to time safe to enter?”
A troubling answer emerged: nothing. Aside from the obligatory CPR classes, teachers and other school person-nel had not historically been exposed to lifesaving medi-cal skills training. As a community, exercise participants found this level of preparedness unacceptable. So they set about to change it.
A Multidisciplinary ApproachUnder the guidance of Wistrom and Cargile, a core cadre of volunteers was formed, including representatives of law enforcement, local fire/EMS, the school district and the local hospital.
It’s hard to read the news today without finding headlines such as these above that highlight the devastation of an active-shooter attack. A 2013 FBI document, A Study of Active Shooter Inci-dents in the United States Between 2000 and
2013, concluded active-shooter events are increas-ing and becoming more lethal.1 Significant time, resources and funds have been dedicated to training first responders to manage these events, but a gap exists in equipping other “immediate responders” for these threats.
The message above was handwritten on a white-board and displayed in the window of Columbine High School as the active-shooter incident played out during that tragic day nearly 17 years ago.
Inside the MercyRockford Health System’s hemorrhage control program for schools
The Columbine attack forever altered the law enforcement approach to active-shooter events. Police training and attitudes have been reshaped, and equip-ment and tactical procedures have evolved to adapt to the threat.
Law enforcement agencies are better prepared to respond, but there is another segment of the popula-tion impacted by active-shooter events that has not, before now, been effectively engaged to help. This article sets forth how one community chose to make a difference in preparedness by engaging and empower-ing those closest to the victims to act during a critical incident or attack.
A Troubling AnswerIn February 2014, the FBI’s Milwaukee Division facilitated an active-shooter tabletop exercise at the invitation of the Janesville (WI) Police Department.
EMSWORLD.com | MARCH 2016 2120 MARCH 2016 | EMSWORLD.com
Because local fire and police departments volunteered to help train local school staff for the Janesville casualty care project, costs were limited to those necessary to acquire the training materials and supplies for the kits.
By G.B. Jones, Karen Schulte, EdD, James J. MacNeal, DO, & Christopher Wistrom, DO

The goal was to find a program to bridge the gap from time of injury to the arrival of trained medical responders. Literature searches and best-practices reviews by all volunteers failed to identify easily imple-mented programs or universally recognized solutions. It became clear a multipronged,
multidisciplinary approach was needed. This would ensure trained EMS providers were prepared to enter the “warm zone” more quickly and efficiently, but it would also leverage and engage an entirely new resource—the people already inside the scene—to start lifesaving treatment.
The first prong of the community pre-paredness program was the full adoption of the rescue task force (RTF). RTF is not a new concept. Ironically, the framework for such a program was outlined in the Winter 2001 edition of The Tactical Edge magazine by two officers from the Beloit (WI) Police Department.2 The concepts in their article, “Confined Threat Escort Tactics,” were not widely recognized or adopted at the time.
In October 2013, however, the Interna-tional Association of Fire Chiefs (IAFC) adopted a position paper that identified sup-port for a rescue task force, and that paper is credited with significantly helping the
mangarusa.com
Safe Patient Lifting
MangarLiftingCushionsUSAmangarint
Lift aSSiStS are ChiLd’S PLay
Lifts up to
700lbs
find out how easy lifting should
be and book a demonstration.
Call 804.405.5706 or email
For More Information Circle 18 on Reader Service Card For More Information Circle 19 on Reader Service Card
The goal was to find a program to bridge the gap from time of injury to the arrival of trained medical responders.
movement progress.3 The core group set about planning to expose all first-respond-ing agencies within MercyRockford Health System’s service area to the RTF concept.
The second prong of the community-based approach was to create a training program to teach teachers, administrators and other school staff the critical lifesaving skills not found in the school handbook.
Once trained, lay personnel would become well-qualified “first” first respond-ers, a population increasingly referred to as immediate responders. With it taking only minutes to bleed to death from a severe arterial injury,4 no RTF would be able to make the difference for the most critically injured. But the immediate responders would already be there!
Once the need was identified, the chal-lenge became creation of the right program. In that quest, some age-old questions had to be answered: Who? When? Why? Where? What? And, dauntingly, how?
Identifying who to train was fairly straightforward: School personnel were the
target audience for the immediate imple-mentation of the education program. It made sense that those already inside the situation would make the ideal first line of defense. But who was best positioned to provide the training?
Almost immediately after deciding to tackle this project, the core group identified that it wanted to create a model program that could be implemented in any commu-nity. This led to the development of a train-the-trainer model that could be taught to public safety providers anywhere. After all, the ideal trainers for teachers in Anytown, USA, are the public safety providers who serve Anytown, USA.
Because many public safety providers have received some active-shooter training, the new program was designed to comple-ment other training programs that focus on the tactics of a response. The new program would not address or debate active-shooter response tactics—it would focus on what other programs didn’t address: core lifesav-ing medical skills that will make a difference prior to the arrival of skilled public safety providers.
When to conduct the training had to be considered. School district personnel iden-tified that all school districts utilized some type of staff in-service day. Some were in the fall, some were in the spring, and all had limited time due to other competing demands. The core team determined if the training could be kept to 45 minutes, it could be accomplished in nearly any in-service training window. In fact, the Janes-ville School District utilized a 45-minute window for in-service topics every week. To ensure consistency, a short video was developed that provided an overview of
EMSWORLD.com | MARCH 2016 2322 MARCH 2016 | EMSWORLD.com
From left, Yolanda Cargile, EdD, former director of student services for the Janesville (WI) School District; Christopher Wistrom, DO, emergency medicine physician at Mercy Health System; Sgt. Mike Blaser of the Janesville Police Department; and Capt. Tom Brunner of the Janesville Fire Department have worked together to bring trauma kits to Janesville’s schools.

the training program. It was designed to be made available to the target audience via an e-mail link sent the day prior to training to introduce staff to the topic. The train-ing material was streamlined so the day of training included only a 10-minute lecture, followed by 35 minutes of hands-on skill-building exercises.
The why aspect became fairly apparent following an extensive review of medical literature. The research, including a review of the Committee for Tactical Emergency Casualty Care’s TECC guidelines, showed the greatest number of preventable deaths in penetrating trauma are either directly or indirectly related to bleeding.5 The sooner massive bleeding can be slowed or stopped, the higher the likelihood of survival. With that in mind, hemorrhage control became the cornerstone of the new training program.
The group evaluated where the program should be implemented, and it made sense to start in the Janesville schools. The pro-gram had to be universally applicable, how-ever, and it was designed to work in any part
of the country and any setting—schools, hospitals, businesses, public venues—where attacks could occur. Not unlike CPR and AED training programs, the hemorrhage control program was intended to be easy to implement anywhere. The large-scale goal
was to teach as many people as possible how to stop life-threatening bleeding, whether by use of commercially available products or through improvisation with tools at hand.
In addition to hemorrhage control, the group evaluated what other training top-ics could be addressed by the program. They arrived at hemorrhage control as the primary goal, followed by management of
other preventable causes of death, including simple airway management and use of the recovery position.5
Perhaps the greatest amount of time spent in program development was deter-mining how to deliver the training content. The team had to address the realities of whether those to be instructed would be amenable to the topic. They had to identify what supplies and equipment to obtain, how to finance them, and whether there was an understanding of the need for the train-ing outside the ranks of the professional responder community. Additionally, if training materials and actual medical sup-plies could be obtained for deployment, were there practical limitations on what could be placed in the schools based on state law or school policies?
The multidisciplinary nature of the group again proved essential to resolv-ing these questions. A quick straw poll of school employees identified that they indeed wanted the education. Surprisingly, many of those asked expressed substantial
EMS1603
For More Information Circle 20 on Reader Service Card
Applying Traction Is EasyWhen you have the right splint
Use the Sager Traction Scale to set the amount of traction needed—Sager Splints do the rest. The Sager’s dynamic function permits traction to decrease automatically as the muscle spasm releases. Your patient will always have the correct amount of safe, secure, traction. It’s that easy!
One-person application. Safely treats Proximal Third and Mid-Shaft fractures. Ensures optimal patient care.
Learn how easy Sager Splints are to use / for details on Sager Splint models visit www.sagersplints.comEmail: [email protected] / Call 800.642.6468 for the name of Your Authorized Distributor.
20270 Charlanne Drive Redding, CA, 96002-9223
For More Information Circle 21 on Reader Service Card
In addition to hemorrhage control, the group evaluated what other training topics could be addressed by the program.
Kit Equipment SelectionThe initial consideration was to utilize the same type of equipment traditionally carried by SWAT operators and tactical medics. This includes Israeli bandages, SOF or C-A-T tourniquets, hemostatic gauze, chest seals and nee-dle-decompression devices. The training requirements to teach and maintain the skills to implement the equipment were problematic, however, and acquisition of the materials proved cost-prohibitive after research determined each kit would cost approximately $120!
In an effort to make the most cost- and training-effec-tive, sustainable kit possible, the core group decided the contents of the kit would at a minimum include gloves, ACE wrap, rolled gauze, SWAT-T tourniquet and instruc-tional card. Research concluded all those items could be acquired and packaged within a plastic bag for a total unit cost of under $20.
The ACE wrap combined with gauze could serve as an excellent pressure dressing and be used alone as a makeshift tourniquet. The rolled gauze is ideal for pack-ing wounds. Plastic packaging material, the plastic bag or the gloves could all be used as excellent makeshift chest seals. The SWAT-T had several advantages as well: Instructions for application are printed clearly on it, it requires no fine motor skills to apply, and it requires less
strength to apply than a SOF or C-A-T. Additionally, the SWAT-T could accommodate any size extremity (impor-tant for elementary schools with pediatric patients), be cut for use by multiple patients, and be used as an excel-lent pressure dressing. The SWAT-T was much less expen-sive than traditional windlass tourniquets and had about the same shelf life.
One identified limitation with the SWAT-T was that self-application could be difficult, especially without consistent practice. In the final analysis, however, to achieve deploy-ment of the maximum number of kits at an acceptable cost, the identified materials represented the minimal sup-plies necessary for effectiveness. Additional supplies could be added to these kits if needs or gaps were later identified.
EMSWORLD.com | MARCH 2016 2524 MARCH 2016 | EMSWORLD.com

fear that they did not know how to act to save a life. Several shared that they’d con-sidered changing professions because the anxiety they had surrounding these crises increased significantly each time an active-shooter event was reported somewhere in the nation.
With respect to the overall cost of imple-mentation, the local fire and police depart-ments quickly volunteered the time neces-sary to do the training. As a result, costs were limited to those necessary to acquire training aids and materials, followed by costs associated with medical supplies to be deployed to the schools in casualty care kits that would be available in an emergency. The core group determined it made the most strategic sense to deploy one casualty care kit to each classroom. Placing kits in hall-ways or office areas would limit access to the lifesaving tools in a lockdown situation, and students or staff could be exposed to danger if they tried to retrieve them from a central location. The dispersed-deployment plan required substantially more kits to cover a
single school, so the over-all cost of each individual kit was an important con-sideration (see sidebar).
ImplementationTo date, the Casualty Care in the Classroom program focused on stopping life-threatening bleeding has been presented to more than 3,000 school employ-ees in Southern Wisconsin and Northern Illinois.
Surveys sent to partici-pants before, right after and at one year after training show the training to be effective. The training substantially increases confi-dence in participants’ abilities to stop the bleeding.
It has also served to better inform school personnel about the roles of law enforce-ment and EMS at the scene of active-shooter and other mass-casualty events.
Most important, the training did not
change participants’ perspectives on how likely an active-shooter event was to happen in their schools. In fact, the training reduced fear, increased confidence and relieved anxiety.
Since inception of the program, hundreds of casualty care kits have been fielded to schools throughout MercyRock-ford Health System’s service area. Funding
sources for the kits have included private donations, grant sources, community foundations, direct school funding and law enforcement seizure program funds. “We are doing this because it is the right thing to do,” says MercyRockford Health System CEO Javon Bea.
The Casualty Care in the Classroom program has proven successful because it utilized a multidisciplinary, community-
based approach to problem solving. The core group enjoyed incredible support from MercyRockford Health System and hospital administration, which partnered with the team to provide the education and materials at as low a cost as possible.
Since the inception of the Casualty Care in the Classroom program over two years ago, several significant strides have been made in immediate responder care. Two of the more notable include the Hartford Consensus Third Compendium6 and initia-tion of the White House “Stop the Bleed” campaign.7 None of these directives or pro-grams, including the Casualty Care in the Classroom program,8 can prescribe a one-size-fits-all approach to hemorrhage con-trol, but each demonstrates progress toward helping this country stop the bleeding.
Special thanks to the following for their contributions to this article: Todd Daniello, MD; Sean Marquis, MD; John Pakiella, DO; Rick Barney, MD; Rodney VanBeek, MD; Capt. Tom Brunner, EMT-P; Scott For-
mankiewicz, EMT-P; Tony Cellitti, EMT-P; Sgt. Michael Blaser; Officer Jason Kelley; Chief Deputy Scott Meyers; and Yolanda Cargile, EdD.
RE FE RE N CE S
1. Blair JP, Schweit KW. A Study of Active Shooter Incidents, 2000–2013. Texas State University and Federal Bureau of Investigation, U.S. Department of Justice, Washington, DC, 2014.2. Anderson D, Kelley J. Contained Threat Escort Tactics. The Tactical Edge, Winter 2001.3. www.iafc.org/IAFC-position-Active-Shooter-and-Mass-Casualty-Terrorist-Event.4. Blaivas M, Shiver S, Lyon M, Adhikari S. Control of hemorrhage in critical femoral or inguinal penetrating wounds—an ultrasound evaluation. Prehosp Disaster Med, 2006 Nov–Dec; 21(6): 379–82.5. Kotwal RS, Montgomery HR, Kotwal BM, et al. Eliminating preventable death on the battlefield. Arch Surg, 2011 Dec; 146(12): 1,350–8.6. Jacobs LM Jr., Joint Committee to Create a National Policy to Enhance Survivability From Mass-Casualty Shooting Events. The Hartford Consensus III: Implementation of Bleeding Control. Bulletin of the American College of Surgeons, http://bulletin.facs.org/2015/07/the-hartford-consensus-iii-implementation-of-bleeding-control/.7. Department of Homeland Security. Stop the Bleed, www.dhs.gov/stopthebleed.8. Mercy Casualty Care Program. Introducing…the Mercy Casualty Care Program, www.mercycasualtycarekits.com.
AB O U T THE AU TH O RS Special Agent G.B. Jones is currently assigned to the FBI, Milwaukee Division. As an assistant special agent in charge, Jones commanded the FBI Milwaukee SWAT and crisis management teams and oversaw the division’s active-shooter training program. He served as the FBI’s on-scene commander during the Azana Spa shooting in Brookfield,
WI, in 2012 and at a mass shooting at Northern Illinois University in DeKalb, IL, in 2008. Jones is an EMT in the FBI EMS program.
Karen Schulte, EdD, is superintendent of the Janesville (WI) School District.
James J. MacNeal, DO, is the EMS medical director for the Mercy Health System, as well as multiple EMS and TEMS agencies in both Illinois and Wisconsin. His background includes 27 years in law enforcement, fire and EMS. He is board
certified in emergency medicine and EMS.
Christopher Wistrom, DO, started his career in EMS as a volunteer in his home town. He has worked in private, hospital-based and fire-based EMS as an EMT and paramedic. He is associate EMS medical director for the Mercy Health System in Wisconsin.
*For terms and conditions please visit www.buyemp.com/customer-service.htmlBuyEMP.com You order. We ship (free).* It’s that simple.
Introducing eSeries Transport Ventilators from O-Two Medical Technologies
• Compact & Lightweight
• Easy To Use
• Quick Patient Setup
• Live Monitoring Screen
• 18+ Hour Battery Life
• Budget Friendly
• 2 Year Manufacturer’s Warranty
Built for EMS
Contact EMP for more details800.558.6270
For More Information Circle 22 on Reader Service Card For More Information Circle 23 on Reader Service Card
Hartford Consensus Third Compendium: EMSWorld.com/12165118;
Stop the Bleed: dhs.gov/stopthebleed;
MercyRockford Health System Casualty Care in the Classroom: www.mercycasualty-carekits.com.
EMSWORLD.com | MARCH 2016 2726 MARCH 2016 | EMSWORLD.com

In 2014 it became clear that the mechanisms we had in place to prevent death from exsan-guination during mass shootings and other atypical trauma were inappropriate. To our dismay, we noted that during real-life active-
assailant scenarios and full-scale drills, victims were not being addressed and treated rapidly. Implementation of the RTF (Rescue Task Force) model was supposed to address this, yet invari-ably times remained unacceptable. If we were to make a real difference in outcomes, the solution required a different distribution model.
Typically bleeding victims had no choice but to wait for emergency first responders to provide lifesaving hemostasis, yet even reorganization of the response was not able to solve the timeliness issue. By considering other life-threatening condi-tions such as sudden cardiac arrest, anaphylaxis and overdose, it became clear that the answer for hemostasis required a similar path.
AEDs are a staple of most public locations and have been pivotal in saving the lives of many victims of SCA. Epinephrine auto-injectors for anaphylaxis have become ubiquitous and in some states are required in schools. In the town of Davie, FL, Assistant Fire Chief Julie Downey and EMS medical director Peter Antevy, MD, reacted to the hemostasis problem first by training the public on bleeding control. Town employees were trained first, followed by incorporation of bleeding con-trol education into standard CPR classes in the community.
They determined that if the public could be trusted with CPR, defibrillation and intramuscu-lar injections, it could be similarly trusted with bleeding control. That decision was the first step toward allowing uninjured victims within hot zones to assist those with life-threatening bleeds.
The Argument for Public Access Bleeding KitsIf the pros can’t get there fast enough, how can we stop exsanguination?
Davie Individual Police Officer Kits (IPOKs)Contents
Chest SealGauze Pad
QuikClot (Hemostatic Dressing)SWAT Tourniquet
Severe Bleeding Kit on Town AEDS
Contents2 CAT Tourniquets2 gauze rolls2 gauze pads4 gloves (xl)
EMSWORLD.com | MARCH 2016 29
Award recipients receive• $1,000; • Three EMS World Expo core program
registrations;• $1,200 for travel and lodging at EMS World
Expo/NAEMT Annual Meeting in New Orleans, LA, Oct. 3-7, 2016.
To nominate your agency or colleague visit www.emsworld.com/awards
2015 NAEMT Military Medic of the Year, John Crowley, U.S. Navy Fleet Marine Force Corpsman
Established by
and
CALL FOR ENTRIES!NOMINATION DEADLINE: JUNE 30, 2016
NAEMT/Nasco Paramedic of the YearRecognizes a paramedic who demonstrates excellence in the performance of EMS.sponsored by
Dick Ferneau Career EMS Service of the Year Recognizes outstanding performance by a paid EMS service.sponsored by
NAEMT/Braun Industries EMT of the Year Recognizes an EMT who demonstrates excellence in the performance of EMS.sponsored by
NAEMT/North American Rescue Military Medic of the YearRecognizes a military medic who demonstrates excellence in the performance of military emergency medicine.sponsored by
ZOLL Volunteer EMS Service of the Year Recognizes outstanding performance by a volunteer EMS service.sponsored by
O
F T H E Y E A R
NAEMT/Jones & Bartlett Learning Educator of the Year Presented to an educator in recognition of their contributions to EMS.sponsored by
O
F T H E Y E A R O
F T H E Y E A R
CAREERSERVICE
By Peter Antevy, MD

Distribution of bleeding control kits from within was the most obvious way to do this. The town had put in place, years prior, a law that required large public build-ings to register their AEDs, and this allowed immedi-ate knowledge of most of the public-access AEDs. Chief Downey then constructed severe-bleeding kits using a pencil case, two tourniquets, gauze rolls and pads, scissors and a pair of gloves, using funding from the town of Davie.
By early 2015 the program was fully implemented, and members of Davie Fire Rescue continued to educate the public at health fairs, community gatherings and basic life support classes. The response was always positive, and the required training time was limited. Furthermore, the police were outfitted with a specialized kit that was purposely very thin and vacuum-sealed so it could fit easily along their chest, beneath their vest. This kit used a SWAT-T tourniquet and also added hemostatic gauze and a chest seal.
Stop the BleedAntevy presented the innovative concept at the Gathering of Eagles conference in February 2015, and it was well received by those in the EMS community. During this time Rick Hunt, MD, director of medical preparedness at the White House, was working on developing consensus on this same issue by bringing national stakeholders to the table. In October of that year the White House unveiled a new nationwide initiative—Stop the Bleed—which would provide bystanders access to bleeding control equipment, just as they have now with AEDs. The town of Davie was invited to attend the bystander “Stop the Bleed” forum at the White House. Vice Mayor Susan Starkey joined Downey and Antevy at the forum on Tuesday, October 6, 2015.
The four-hour event began to lay the groundwork for local entities to plot a course for the future. If the general public can be given sanction to take action to stop life-threatening bleeding by providing access to tourniquets and other bleeding-control equipment, many lives can be saved. The town of Davie was recognized as one of the leading municipalities in the country that has already added severe-bleeding kits to community AEDs.
In 2015 Davie already has two critical saves thanks to the public access bleeding kits. In one case a town employee severely injured himself using a power saw, and a colleague rapidly provided hemostasis using tech-niques he learned in the course. The town’s mayor and commissioners later honored the employee for his heroic actions.
AB O U T THE AU TH O R Peter Antevy, MD, is a pediatric emergency medicine physician at Joe DiMaggio Children’s Hospital in Hollywood, FL, and an associate professor of pediatrics at the Florida Atlantic University School of Medicine. He serves as medical director for several Florida agencies. He is the founder and chief medical officer of Pediatric Emergency Standards, Inc.
EMERGENCY MEDICAL SCIENCE
Paramedic Certifi cation(Hybrid Program)• Fully CAAHEP Accredited• Hybrid Paramedic program offered through LCC Continuing Education Department. Only four on-site visits required for skills training and evaluations. All coursework is done online. Tuition is $360.• Clinicals can be completed in your area. Contact LCC regarding available areas.• Different course options that allow currently
credentialed EMTs, AEMTs, or individuals with no certifi cation to train for their Paramedic certifi cation.• Graduates are eligible for the NCOEMS Paramedic exam and the National Registry Paramedic exam.
Associate Degree in EmergencyMedical Science — Bridging• All degree classes offered 100% online.• Currently credentialed state and national Paramedics earn up to 45 credits toward their degree just for being certifi ed!• Designed for demanding EMS work schedules. Complete the degree at your own pace!
Earn Your Degree Online!
231 Hwy. 58 South,Kinston, NC
www.lenoircc.edu
(252) 527-6223, ext. 115 [email protected]
For More Information Circle 24 on Reader Service Card 888.448.1238 | AironUSA.com
pNeuton™ model S ventilator with CPAP
MACS™ Stand-alone CPAP
pNeuton™ miniNeonate to pediatric ventilator with nCPAP
CPAP + VentilAtion. All in one.
With the pNeuton model S you’ll be prepared for any emergency respiratory situation. The ventilator has built-in CPAP, provides adult/pediatric volume or bi-level pressure ventilation as well as mask CPAP ventilation. Pure pneumatic technology eliminates batteries. And it’s real easy to use. Learn more about Airon’s respiratory devices for EMS. Visit AironUSA.com today.
Be PrePAred. For Anything.
Discover the pNeuton model S
ventilator with CPAP.
For More Information Circle 25 on Reader Service Card
Best Practices for Active Shooter ResponseBy Raphael M. Barishansky, MPH, MS, CPM
Unlike many other types of incidents, an active shooter/hostile event (ASHE) will almost always result in the deployment of all types of first responder. Recognizing the need for EMS, fire and law enforcement to come together for these events in a coordinated manner, the InterAgency Board recently released a broad-based document with recommendations from lessons learned and potential “best practices” for this type of event.
Improving Active Shooter/Hostile Event Response: Best Practices for Integration of Law Enforcement, Fire and EMS outlines specific recommendations across the emergency service spectrum, which include:
Integrate and improve coordinated pre-event law enforcement, fire and EMS policy development, planning, training and exercises. This is probably one of the most important lessons learned from previous events and speaks to the need for a practiced approach as a foundation for a successful response to these incidents.
Create and implement a common operating language. The need for all responders to understand each other and communicate critical, time-sensitive messages in a common language cannot be overstated.
Employ Tactical Emergency Casualty Care (TECC). This approach advocates that in areas of high threat, casualty triage should be limited only to categorizing the wounded as ambulatory, wounded or deceased. There was also mention of the need to engage in proactive pub-lic outreach as well as informing and educating a variety of specialty groups/stakeholders.
Establish evidence-based guidelines and education for medical and rescue equipment. The emphasis here is that lifesaving interventions and rapid extraction are the ONLY required medical interventions in high-threat areas. Also, it is incumbent on decision-makers to limit equip-ment to that defined by TECC, to issue individual first aid kits to law enforcement officers and to balance training and operational goals against acquisition of equipment.
Promote two-way public communication as an essential component for effective ASHE. The public is clearly identified in this document as a real first responder and a valuable resource. It was also stressed that it is essential to promptly and effectively communicate critical incident information and clear instructions on the proper public response.
For more information, see EMSWorld.com/12152344.
AB O U T THE AU TH O R Raphael M. Barishansky, MPH, MS, CPM, is a solutions-driven consultant working with EMS agencies, emergency management and public health organizations on complex issues including leadership development, strategic planning, policy implementation and regulatory compliance. E-mail [email protected].
30 MARCH 2016 | EMSWORLD.com

From hurricanes isolating segments of the population to the dynamic terrorist events in Paris and San Bernardino, the threats to our society are both complex and often overwhelm local resources. Because of their
storied success, there is a widely held regard for the availability and professionalism of our emergency medical services, and deservedly so. Accordingly, most of the financial resources dedicated to disas-ter preparedness and counterterrorism are primarily focused on improving our uniformed response.
Yet the unspoken secret of EMS is that there is a systemwide overreliance on the existing EMS struc-ture. Too often this reliance means our communities
prepare based on the assumption that medical care will be readily available. As recent events continue to prove, this is not always the case, and it suggests our current response paradigm may need improvement.1 Now is the time to educate and empower everyone to be able to bridge this gap and provide emergency care. Perhaps Amanda Ripley says it best in her book The Unthinkable: “Regular people are the most important people at a disaster scene, every time.”
Trauma is the leading cause of death from birth to nearly age 50, but there has yet to be a concerted effort to improve outcomes from traumatic injury within this population.2 Under the best circumstances, medi-cal response takes anywhere from 7–11 minutes on
By Joshua P. Bobko, MD, William J. Harris, NREMT-P, & Stuart Thomas
The First Care Provider System:
Improving Community Resilience for Unexpected Disasters
Why civilians should be prepared to act in mass-trauma events
A security guard applies
a tourniquet during a
simulated earthquake
training exercise at a Westminster
(CA) mall.
Photos courtesy First Care Provider
32 MARCH 2016 | EMSWORLD.com The Largest EMS Conference and Trade Show in North America
Where the World of EMS Converges for Education and Innovation• 130+CEU-certifiededucationalsessionsacross3daysand8tracks
• World-classfacultyandindustrythoughtleaderspresentingthelatest
techniquesandtrendsinprehospitalclinicalcare
• State-of-the-arttechnology,productsandservicesfrom350+exhibitors
• Hands-onworkshopsandinteractivelearningopportunitieswiththemost
advancedsimulators
• Moreglobalnetworkingopportunitiesthananyothernationalconference
#EMSWorldExpo Learn more at EMSWorldExpo.com

brief insight into the success of a reproduc-ible model for organizations constrained by limited resources.
The First Care Provider ConceptOrganizations and agencies across the world now conduct regular active-shooter exer-cises. While many of these programs teach familiarization with the DHS-recommend-ed “run, hide, fight” approach, the “first care provider” concept creates an all-hazard approach to situations where life may be compromised yet medical care is unavail-able.9 This was the next critical step in the trauma chain of survival, considering that current trauma education programs are not designed for a civilian audience. Further, the situational response and prioritization of care differs dramatically from civilian medi-cal programs (first aid, CPR) but adheres to the consensus guidelines recommended by C-TECC. Finally, the universality of the first care model makes it an appropriate subject to be included as a part of all ongoing safety programs and new-employee orientations, or as a stand-alone course.
Some of the most impressive outcomes were achieved in Westminster, CA, through a community-led effort to improve resilien-cy. As a small city (pop. 90,000) with limited resources, Westminster’s pilot project was launched through a public-private endeavor to improve preparation for mass-casualty disasters, including acts of terrorism, vio-lence and natural disasters. In partnership with FirstCareProvider.org, the commu-nity sought to reach areas of community interface that have substantial public use or risk for traumatic injury but are often completely reliant on the 9-1-1 system (such as schools, city hall, city maintenance, non-sworn police personnel and local business-es). Following an active-shooter curriculum administered by the Westminster Police Department, the First Care Provider model was introduced to create a communitywide network of trauma-trained individuals capable of providing lifesaving interventions to trauma and potentially augmenting the capabilities of first responders.10
This model proved the key to success. Acting Chief of Police Daniel Schoonmaker summarized the program by saying, “Some treatments are covered in other courses
EMS1603S
For More Information Circle 26 on Reader Service Card
For More Information Circle 27 on Reader Service Card
For More Information Circle 28 on Reader Service Card
DEGREESBachelorCrisis and Disaster Management
MasterBusiness Administration
– Aviation Management
– Construction Management
– Project Management
Public Health Administration
Aviation Science
– Aviation Operations
– Aviation Security
Recognized as a 2016Military Friendly® School
Boca Raton | Orlando | Sarasota | Tampa | Online
888.854.8308
SCAN HERE
LEARN MORE
average during non-surge operations, and departments around the country are self-identifying their own inability to meet NFPA 1710 standards.3,4 Given this reality, there have been outstanding efforts highlighting the science of civilian survivability, particu-larly from hemorrhage. The Committee for Tactical Emergency Casualty Care (C-TECC) has made great strides synchronizing civilian-based prehospital guidelines for medical providers across the world. Subsequently the Hartford Consensus, convened follow-ing the Sandy Hook massacre, has effectively pushed the need for improving hemorrhage control within communities.5 Following on the success of these groups, the federal government has attempted to make recommendations for civilian actions (DHS active shooter pamphlet) and recruit the community with the “Stop the Bleed” program.6,7
While these efforts are critically important, what has been miss-ing until now is a unifying solution to meet these new mandates. Recent publication of the First Care Provider white paper (http://firstcareprovider.org/#white-paper) has provided a foundation for this effort, combining the currently supported TECC guidelines with systemic lessons learned from a fully operationalized public education model.8 In this paper (excerpted on page 36) we share a
The public can be trained to deliver immediate lifesaving care. In this photo, a construction worker applies an improvised tourniquet to his leg after he was impaled on a metal bar.
EMSWORLD.com | MARCH 2016 3534 MARCH 2016 | EMSWORLD.com

currently offered to the public, but there is no bystander-led trauma system that combines both action and treatment, particularly in the time from onset to response.” Therefore, the supporting literature, prioritization of care and nuances of public education that make up this system are markedly different from other programs. While “Stop the Bleed” supports one of the major tenets of the civilian TECC guidelines and the Hartford Consensus, public access to hemostatic devices without educational outreach may not suf-ficiently address the needs of our communities.
First Care Provider OutcomesThis concern was evident during the Westminster exercise. “I felt myself panic,” says Patricia Singer, one of the volunteers who braved the study without prior preparation. This hesitancy was one of the primary barriers the First Care Provider model sought to overcome. Its evolution over the past several years and ongoing contact with our communities have extracted several lessons particular to public trauma education.
One of those is that the reluctance to act is possible to overcome once the root cause of this reluctance is identified and an easily retainable model that integrates with existing emergency procedures is provided. The success of this approach was made evident by Berri Williams, a teacher who had completed FCP training almost two months prior to the exercise. “They taught us exactly what to care about first,” Williams says, “so we knew exactly what to look for.” This familiarization and recognition of the preventable causes of death can be imparted to the layperson and must be included in any civilian course.
Second, in the untrained population there is a tendency to con-gregate in times of emergency, and a hesitancy to take individual
action. With a brief familiarization, First Care-trained members of the public demonstrate a notable willingness to operate indepen-dently, recognize critical injuries and properly allocate resources for maximal benefit. This type of outreach effort may actually encourage independent thinking in times of disaster. This becomes critical given that recent events (e.g., Tucson, Aurora, Boston) have shown that rapid evacuation to medical care can be as important as hemorrhage control.11 Therefore, bystander safety training, rec-ognition of critical injury and rapid evacuation should be the key objectives in civilian training, with the preventable causes of death as a secondary objective.
Finally, one of the most notable observations was ironically captured by one of the participants who had the most medical education. “We are so used to having equipment to rely on that you don’t know what to do in a situation like that,“ says Hiram Diaz, a registered nurse. The reality is that there must be a mandate within our medical educational system to highlight this developing skill set and prepare providers to face the threats of terrorism, active-violence incidents and disaster medicine. There has been dramatic support preparing first responders, but there has not been a parallel effort to educate “first receivers.”
Recommendations and Future DirectionReluctance to change is perhaps the most critical barrier that must be overcome for a successful community resiliency program. This will require leadership to move beyond a complete reliance on traditional 9-1-1 response and hesitance to introduce medical policy into the broader population. However, the evolving threats facing our society make it necessary to recognize the gap left by
For More Information Circle 29 on Reader Service Card
Code #72657
800.558.6765GrahamMedical.com
The MegaMover® Select™ Goes Where Stretchers Can’t
Move with Speed & Safety
EMS Products from Graham Medical
• Transfer, transport, and rescue patients that can’t be reached by stretchers
• 14 multi-positioned handles provide ergonomic lifting
• Pull straps for situations when pulling a patient is safer than lifting
• Durable, nonwoven design holds up to 1000 lbs.
• Light, space-saving, and portable
New
For More Information Circle 30 on Reader Service Card
Arming the First Care ProviderAn educated populace can help produce a seamless transition of care for victims of traumatic injuryThe following is excerpted from Building Community Resilience to
Dynamic Mass Casualty Incidents: A Multi-Agency White Paper in
Support of the First Care Provider, authored by the Committee for
Tactical Emergency Casualty Care, FirstCareProvider.org and the
Koshka Foundation for Safe Schools. Find the whole document at
http://www.firstcareprovider.com/#white-paper.
Natural and manmade disasters are creating increasingly complex response challenges. The current U.S. emergency response model relies heavily upon the availability and expertise of highly trained public safety agencies. Too often this leads the public and our leaders to assume profession-al emergency medical care will be immediately available. Unfortunately there are often delays in first responders accessing victims, especially in complex high-threat events.
Initiatives such as the Rescue Task Force model and the 3-ECHO program are creating “warm zone/indirect threat care” operational paradigms for first responders and are an important first step in shortening the time from injury to first medical intervention. However, despite aggres-
sive and expedient deployment of professional medical providers, there remains a time gap from point of injury to lifesaving intervention that only First Care Providers—empowered and trained community members—can address.1
The First Care Provider represents the first link in the trauma chain of survival from point of wounding through definitive care.3,4 A First Care Provider-empowered sys-tem offers a universal, flexible bystander-initiated trauma protocol. This shared language, based on the principles of Tactical Emergency Casualty Care, empowers the FCP and the arriving medical/rescue assets to integrate effec-tively and work off the “same sheet of music.”
There are four key requirements to the development and implementation of a successful community First Care Provider program:
1. Administrative leadership and operational policy devel-opment—Successful FCP integration requires grassroots initiatives and national public policy leadership. Leaders must evolve past the complete reliance on traditional 9-1-1
response and overcome the wide-spread reluctance to introduce poli-cies that empower medical action in the broader population. Non-medical leadership is critical to creating an effective whole-of-community system that reduces potentially preventable trauma mortality.7
2. Public access trauma kits—Many government build-ings and public businesses in the United States are grossly underprepared to support FCP interventions for traumatic injuries during targeted violence events. The deployment of public access trauma kits serves two critical roles. First, they provide a visual cue to prompt First Care Providers to action. Second, if properly equipped, they can provide critical material to support lifesaving interventions for more than just hemorrhage control. Public access to read-ily available medical equipment should be part of a multi-pronged approach to community safety.
3. First responder training—The training of professional first responders currently focuses on unified command, operational coordination and direct lifesaving interven-tions. This traditionally marginalizes the bystanders and uninjured persons on scene. This must change. First
responders must be familiar with the capabilities of the FCP as well as have operational plans that incorpo-rate these available providers as force multipliers in the response.
4. First Care Provider training—Data from across the globe demonstrates that training individuals empowers action and improves survival from medical and traumatic emergencies.8–10 Trained First Care Providers demonstrate a willingness to operate independently, are able to recog-nize critical injuries and can properly allocate resources for maximal benefit.11
External hemorrhage control is a critical skill for many traumatic type injuries; however, it is not a panacea. Recent events reveal that access to the wounded, recog-nition of significant injury and rapid evacuation to medical care are at least as important as immediate hemorrhage control. Education on all of the preventable causes of death12 in penetrating and blast trauma should be the ultimate goal and can be accomplished with a limited time investment. In addition to reducing mortality through application of TECC, this training will improve resilience by empowering individuals to take action in times of crisis.
EMSWORLD.com | MARCH 2016 3736 MARCH 2016 | EMSWORLD.com

our current disaster planning assumptions and existing medical curricula. There are currently no common protocols for EMS services or law enforcement to provide medical care in what has become known as the “hot zone.”12,13
This is a crucial gap for those affected by crisis or conflict, for whom the “how to respond” decisions have already been made. The victims of trauma can neither wait for help nor consult others away from the incident. Therefore, the only care provided for the victims of those events will be self-aid and by the unharmed bystander. The First Care Provider concept was created specifically for the nonmedi-cal civilian needing to provide care for those injured in trauma. It
adheres to the latest medical guidelines and the recommendations of both Hartford and “Stop the Bleed.” The FCP model prioritizes decisions based on the expected resources available to the nonuni-formed civilian population and dispels the common fear of how to recognize and appropriately treat critically injured victims.
In a time where limited budgets and reduced personnel make operating emergency response systems increasingly challenging, agencies must realistically consider return on their investment when it comes to public safety. A synchronized strategy for improving community resilience will include fire prevention, cardiac arrest and traumatic injury. As departments continue to face escalating expectations of service as well as soft mandates from multiple orga-nizations, creating a first care provider network becomes a realistic and achievable goal with limited time investment.
RE FE RE N CE S
1. Bobko JP, Kamin R. Changing the paradigm of emergency response: The need for first-care providers. J Bus Contin Emer Plan, 2015 Autumn; 9(1): 18–24.2. Centers for Disease Control and Prevention. WISQARS, http://webappa.cdc.gov/sasweb/ncipc/leadcaus10_us.html.3. NFPA 1710: Standard for the Organization and Deployment of Fire Suppression Operations, Emergency Medical Operations, and Special Operations to the Public by Career Fire Departments.4. Green E. City ambulance response times improving, study shows. San Francisco Chronicle, Nov. 19, 2015.5. Jacobs L, Carmona R, McSwain N, et al. The Hartford Consensus III: Implementation of Bleeding Control. Bulletin of the American College of Surgeons, http://bulletin.facs.org/2015/07/the-hartford-consensus-iii-implementation-of-bleeding-control/.6. Department of Homeland Security. Active Shooter How to Respond, https://www.dhs.gov/xlibrary/assets/active_shooter_booklet.pdf.7. Department of Homeland Security. Stop the Bleed, http://www.dhs.gov/stopthebleed.8. Callaway D, Bobko JP, Shapiro G, Anderson K, Smith E, Sarani B. Building Community Resilience to Dynamic Mass Casualty Incidents: A Multi-Agency White Paper in Support of The First Care Provider. J Trauma Acute Care Surg, pending publication April 2016.9. Fisher AD, et al. The Ranger First Responder Program and Tactical Emergency Casualty Care Implementation: A Whole-Community Approach to Reducing Mortality From Active Violent Incidents. J Spec Oper Med, 2015; 15: 46–53.10. Fletcher JL. Active shooter ready: Westminster PD trains city staff, local teachers on being first-care providers. Behind the Badge, http://behindthebadgeoc.com/cities/wpd/active-shooter-ready-westminster-pd-trains-city-staff-local-teachers-first-care-providers/.11. System Planning Corp., TriData Division. Aurora Century 16 Theater Shooting: After-Action Report for the City of Aurora, https://www.courts.state.co.us/Media/Opinion_Docs/14CV31595%20After%20Action%20Review%20Report%20Redacted.pdf.12. U.S. Fire Administration. Fire/Emergency Medical Services Department Operational Considerations and Guide for Active Shooter and Mass Casualty Incidents.13. International Association of Fire Fighters. IAFF Position Statement: Rescue Task Force Training, http://www.iaff.org/Comm/PDFs/IAFF_RTF_Training_Position_Statement.pdf.
AB O U T THE AU TH O RS Joshua P. Bobko, MD, FAAEM, is a board-certified emergency physician and adjunct assistant professor of emergency medicine at Loma Linda University in California. He is a medical team manager for California USAR Task Force 5 and the medical drector for the Westminster (CA) Police Department. His company, Valiant Research, provides training and operational medical support for the Los Angeles FBI. Recognizing the gap in traditional EMS response, Bobko started the nonprofit FirstCareProvider.org with the goal of improving community resilience
by expanding trauma education into our communities. He is on the Board of Directors for the Committee for Tactical Emergency Casualty Care.
William J. “Bill” Harris, NREMT-P, is a 20-year veteran of the U.S. Navy. His deployments include Iraq, Afghanistan, Kuwait and Africa, as well as serving in Iceland. He spent eight years serving beside U.S. Marines as a Fleet Marine Force corpsman, and seven years at the Naval Special Warfare Development Group. Since retirement in 2010 he has trained military members, law enforcement, firefighters and other government agency personnel in Tactical Combat Casualty Care (TCCC), Tactical Emergency Casualty Care (TECC) and active-shooter tactical response.
Stuart Thomas is codirector of MARCH Tactical Training Ltd. and owner of Line9Medic Ltd. (TangoMikeTM) in the U.K. He also serves on the board of advisors for the Committee for Tactical Emergency Casualty Care (C-TECC).
For More Information Circle 31 on Reader Service Card
PORTABLE TOP LOADING EMS FRIDGESAs first-responders, you know keeping your cool can be a matter of life or death, and that’s why you can rely on Engel.
The Engel fridges are designed to meet the needs of the EMS market for the transport of temperature-sensitive saline and medications.
For those long shifts, introducing our new vacuum insulated, high performance 30oz Tumbler - your partner in cool.
30oz Tumbler
Phone 561-743-7419 • enge lcoo le rs .com
A LEGEND IN RELIABILITY
*New
38 MARCH 2016 | EMSWORLD.com
Hosted by NAEMT’s PHTLS Committee and EMS World Expo
Presenting the latest research and information on prehospital trauma care from internationally recognized experts around the globe, the 5th annual World Trauma Symposium will expand your medical knowledge and improve your clinical care, ultimately improving your patients’ outcomes. A 1-day educational event that will change the way you practice.
All attendees will receive 8 hours of CECBEMS-accredited CE, CME or nursing CE.
WorldTraumaSymposium.com
OCTOBER 4, 2016 NEW ORlEANS, lA ERNEST N. MORiAl CONvENTiON CENTER
Registration Opens
April 1st
The premier education event for
ALL providers of out-of-hospital
trauma care.
#WorldTrauma16 Learn about PHTLS at naemt.org
Acting Chief Dan Schoonmaker of Westminster (CA) Police Department briefs the community on his vision for an integrated first responder/First Care Provider program.
For More Information Circle ?? on Reader Service Card

Members of the Tactical Medic Program that is embedded into the Leon County Sheriff’s Office SWAT team train for active shooter situations.
those incidents, the officer immediately neutralized the threat.1,2
For law enforcement, the Columbine school shootings were the sentinel event that changed their response to active shooter incidents. A lesson learned was the immediate need for first-arriving officers to engage the perpetrators rather than contain the incident and wait for SWAT teams.
For EMS, the Aurora, CO, movie theater shootings were the sentinel event. Due to several issues in communication and coordination, such as misunderstandings between agencies regarding EMS entry and scene safety, fire and EMS assets were unable to gain access to the critically injured, resulting in many severely injured patients being transported by law enforce-ment. These gaps in communication left some responders without situational aware-ness of current circumstances and immedi-ate needs.3
A review of the incident revealed that EMS and law enforcement must better coor-dinate and begin to practice and respond differently when these types of incidents occur. Citizens are demanding that law enforcement, fire and EMS find alternatives to rescue and improve outcomes for severely traumatized patients. The fact is that many of these critical trauma patients can be saved if EMS is aggressive in its approach and clearly understands and mitigates the risks as much as possible.
With the most recent Paris and San Ber-nardino incidents, EMS personnel must rec-ognize another, higher-risk threat level than an active shooter. These types of attacks are coordinated and complex events that have been planned and perpetrated by terrorists whose intent is to kill as many citizens as possible, including response personnel, and to gain as much media attention as achiev-able for their cause. This is a game changer for EMS response. For these types of events, EMS agencies can no longer remain siloed with an insulated response from other community resources. Overall commu-nity response, particularly among all first responder agencies, is key to success in such atypical incidents.
The Traditional ResponseTraditionally in EMS, when a violent inci-dent of any type has occurred, personnel
have staged their response at a safe dis-tance. Since EMS providers are not armed or trained to confront a violent incident, this model should remain intact for all typical violent incidents. EMS should not confront a violent incident under normal circumstances without law enforcement clearing the scene. Once law enforcement has contained the threat, EMS providers can enter the scene and treat the injured. The types of incidents discussed here are dif-ferent from a normal response and require a different approach.
The Response to Atypical IncidentsResponse to an atypical incident must be planned and practiced before an actual incident occurs.4 Risk is involved in every EMS response; however, the response to an atypical event contains higher-risk elements, thus preplanning and careful training must occur to lessen the risks faced by responders. EMS providers should clearly understand how they need to interact with other public safety entities and how this coordinated interaction can reduce their exposure to danger and improve patient outcomes. This is not to be taken lightly because in these types of incidents, the intent of terrorists is to cause as much death and destruction as possible, including public safety resources. The per-petrators have the advantage of surprise; however, public safety has the advantage of superior training, preplanning and the pool-ing of community resources to improve their approach.
As in active shooter events, law enforce-ment officers should directly engage the perpetrators upon arrival. The first four arriving law enforcement officers should eventually form an initial contact team that directly confronts the perpetrators, attempting to neutralize the threat and end the carnage. The fifth-arriving law enforce-ment officer should assume a position of incident command and begin organizing other arriving resources to adequately meet the needs of this very fluid incident. The incident commander should begin report-ing the situation to dispatch, requesting additional resources as needed, collect-ing information about the current status
of the incident, and forming additional initial contact teams of law enforcement officers and rescue task forces, consisting of arriving EMS, fire and law enforcement as they arrive on the scene. This incident com-mander should utilize situational awareness to determine where initial contact teams and rescue task forces are needed to engage the enemy and evacuate victims.
The rescue task force is a team with a minimum of one law enforcement officer and one EMS and/or fire personnel. However, two law enforcement officers per team is optimal. The configuration may be larger, depending on the immediately available personnel and the needs at the incident. The mission of the rescue task force is to enter the warm zone behind the initial contact teams to begin hemorrhage control and rapid evacuation.5 Ideally, this would include tourniquets and
blood-clotting pressure bandages and any means of rapid evacuation of the injured. With limited personnel, particularly in the beginning stages of an incident, there may not be time to set up formal triage areas. In lieu of triage, patients should be moved to casualty collection points, where they can then be moved by additional personnel to the cold zone for rapid transport.
Going into warm and hot zones in an active and dangerous event with shooting and violent threats represents a new thought process for fire and EMS personnel.6 Fire may be familiar with operating in warm and hot zones of hazardous materials, but the actively violent threat is different and requires a dif-ferent approach. EMS is very familiar with the golden hour of trauma; however, these severely injured patients lacking that hour need immediate evacuation and transport to survive. Injuries this catastrophic require that these patients be transported to a trau-ma center or surgery to save lives.
EMS has always faced the possibility of responding to acts of violence, but as the world changes, new challenges and threats are presented that are more complex and hold more danger for EMS providers.
Recent events such as the terrorist attacks in Paris and San Bernardino make it imperative that EMS providers understand and adapt their response to these threats accordingly, to save the lives of victims and fellow first responders. New procedures must be adopted that reflect coordination within each com-munity for the most effective response for its citizens.
EMS providers are accustomed to responding to violent incidents where guns, knives and other
weapons have been utilized. However, over the past decade, EMS has faced a growing number of higher-level incidents—those involving active shooters, and also heavy weapons, terrorist attacks and the pos-sibility of additional attacks that include explosives and hazardous materials. This trend demands not just a simple shift in response, but an entirely new thought dynamic for EMS.
According to the FBI, from 2000 to 2013, 18 incidents met the criteria for an active shooter incident in which a single law enforcement offi-cer arriving on the scene was clearly documented engaging the perpetrators immediately. Of those 18 incidents, 13 were still in progress and in 12 of
Response to Atypical Incidents: New Demands for EMSComplex new challenges and threats hold more danger for EMS providers
By Mac Kemp, MSs, MEd, EMT-P
EMSWORLD.com | MARCH 2016 4140 MARCH 2016 | EMSWORLD.com

and at each different incident. Local and state law should be reviewed to determine if these resources can be utilized in a disaster situation.
Intelligence GatheringLaw enforcement personnel are accustomed to gathering information to eventually develop an intelligence product to help guide response efforts and to feed into an investigation after an incident has conclud-ed. EMS personnel should be aware how the information they are presented may influ-ence how the response unfolds or directs decision making. EMS personnel should understand that something they see at the scene or hear over the radio may be impor-tant information that could help mitigate the situation or shed light on how a response could be better coordinated. Responding personnel should clearly understand how and to whom to forward that information if it seems to be important for the success of the incident. There should be a constant flow of information to the incident com-manders to evaluate all information from all sources.
ConclusionAn atypical incident, such as a terrorist attack, may prove to be the most challenging response to any EMS agency. However, with careful thought and planning, the ability to respond as a community-based team uti-lizing all community-based resources can improve outcomes for injured patients and for responders.
The Department of Homeland Security has begun work on training courses related to atypical incidents. The Louisiana State University National Center for Biomedical Research and Training is in the process of developing courses for these types of attacks. Many courses exist for law enforcement on active shooter incidents and EMS personnel should seek this same type of training.
While there is risk responding to these incidents, planning a coordinated approach, critical thinking, risk-based decision mak-ing, unconventional approaches and the creative use of resources can make the outcomes successful and save lives.
RE FE RE N CE S
1. U.S. Department of Justice, Federal Bureau of Investigation. A study of active shooter incidents in the United States between 2000 and 2013. Sept. 16, 2013, Washington, D.C.
2. Blair JP, Nichols T, Burns D, Curnutt JR. 2013. Active Shooter Events and Response. Boca Raton, FL: CRC Press.3. Johnson KH. Changing the paradigm: Implementation of combined law enforcement, fire, and emergency medical service (EMS) cross-disciplinary response to hostile events. Naval Postgraduate School, Monterey, California Thesis, 2014.4. The Interagency Board. Integrating Law Enforcement, Fire, and Emergency Medical Services During Active Shooter/Hybrid Targeted Violence Incidents, August 2015.5. Morrissey J. EMS response to active-shooter incidents. EMS World 40:7,42–48.6. Macesker B, Myers JJ, Guthrie VH, Walker DA, Schoolcraft SG. Quick-reference Guide to Risk-based Decision Making (RBDM): A Step-by-step Example of the RBDM Process in the Field. Air University, 2002.7. United States Coast Guard, U.S. Department of Homeland Security. Risk-Based Decision Making Guidelines. June 11, 2015.8. Ergenbright CE, Hubbard SK. Defeating the Active Shooter: Applying facility upgrades in order to mitigate the effects of active shooters in high occupancy facilities. Naval Postgraduate School, 2012, PhD diss., Monterey, CA.
AB O U T THE AU TH O R Mac Kemp, MSs, MEd, EMT-P, is deputy chief of clinical affairs at Leon County EMS in Tallahassee, FL. He has over 39 years of EMS experience and has worked for county, hospital and private EMS systems. He began his career at a funeral home that provided ambulance services. He currently holds a master’s degree in Health
Education from Florida State University in Tallahassee, FL, and a master’s degree of Security Studies from the United States Naval Postgraduate School, Center for Homeland Defense and Security in Monterey, CA. He also designs and teaches homeland security courses for the Louisiana State University Center for Biomedical Research and Training.
New Command StructuresWhile conventional incident command works in normal disaster situations, in an atypical incident there are not enough per-sonnel or enough time to set up this formal structure. Rapidly moving events, the pos-sibility of multiple attack sites and limited resources call for a new approach to com-mand structures. Each individual incident has an incident commander. However, with multiple simultaneous incidents, coordina-tion of available resources is key to meet the needs of each individual incident. The answer is Area Command.
Area Command is not a new concept, but it works in rapidly changing events with the potential for multiple sites of response and operations. Once there is recognition of a coordinated terrorist series of incidents or atypical incident, the first-arriving supervi-sor should find a location that is safe and located appropriately far enough away from all incidents to establish an Area Command for coordination of community resources for all incidents. The Area Command may need to be moved if the threat shifts toward the command post. Commanders must always consider security at the Area Command since terrorists may plan second-ary attacks on command posts once they are established. This includes setting up an Area Staging spot for initial response of resources to be directed as needed to each individual incident. Remember, the incident command at each scene and Area Command are abbreviated command structures to operate until a full incident command setup can be established, once enough personnel arrive on all scenes. The supervisor setting up Area Command can be from any response discipline.
All responding personnel should be ready, through cross training and temporary role exchange, to perform whatever duties may be needed for the incident. Obviously, only armed law enforcement can engage the perpetrators; law enforcement can treat vic-tims while in the hot and warm zones if they are trained and appropriately equipped with tourniquets and pressure bandages. Fire and EMS could provide perimeter control or guard evidence if immediate medical or hazard control is not needed. A successful outcome is helped if all response personnel are willing to fill whatever roles need to
be filled at the moment and shift with the changing stages of the event. All responders should be ready to function outside of their normal lane of activities and play the role that is immediately needed.
New Agency RequirementsFor new approaches to succeed, critical thinking is required by leadership, with the use of resources that may not be utilized in a traditional response.
All public safety agencies and other potential resources should plan and train together for these types of incidents. Pre-planning is one of the greatest advantages public safety has in dealing with of these types of attacks. EMS should play a large role in bringing all community partners, regardless of local politics or jurisdictions, to the table for input and coordination.
Agency protocols should be coordinated to reflect the enhanced roles of the agency and its personnel responding in these types of incidents. Accordingly, mutual aid agree-ments should be in place before an incident occurs so that incident and area command-ers are aware of available resources in a given situation.
Unconventional ResourcesMany times in an atypical event all resourc-es will be strained and possibly unavailable. Responders should be aware of possible resources that could help them to complete their mission. Unconventional resources for extreme atypical incidents can include:
» Private businesses and entities; » Public works personnel; » Correctional personnel; » National Guard and Civil Air Patrol; » Private security guards.
Many of these resources may have sur-prising answers to the problems that present themselves.
Needed specialized equipment may also be in short supply. Thinking creatively can help alleviate equipment shortages. Use of barricades and dump trucks from public works can assist in establishing a perimeter. Plywood, tables and chairs may be used to assist moving patients. When ambulances are in short supply, could other trucks or buses be used to move patients to hospi-tals with medical personnel on board? The answers will be different in each location
Glossar y of TermsArea Command: A command
structure that is particularly beneficial to incidents that are typically not site-specific, are not immediately identifiable, are geographically dispersed and evolve over longer periods of time (e.g., public health emergencies, earthquakes, tornadoes, civil disturbances, terrorism).
Area Staging: Any area or place serving as a point of assembly or preparation on the way to a destination or multiple destinations allowing overall coordination of available resources.
Atypical EMS Incident: An incident that is outside of the normal response parameters of EMS agencies such as terrorist attacks or active shooter incidents that require a modified approach.
Casualty Collection Point: Location within a jurisdiction that is used for the assembly, triage (sorting), medical stabilization and subsequent evacuation of casu-alties. In the context of atypical incidents, the CCP in most circum-stances may be used as an assem-bly point to move patients rapidly to waiting transport.
Initial Contact Teams: Consists of the first arriving law enforcement officers at an active shooter or terrorist incident who immediately and directly confront and engage the perpetrators of the incident.
Rescue Task Force: The Rescue Task Force is an aggressive response to an active shooter inci-dent that provides rapid medical treatment at the point of injury to those who have been injured. The RTF is a joint response between police and fire/EMS departments, but can be adapted to any agency large or small, rural or urban. It usually consists of at least one or more EMS/fire personnel to treat and evacuate patients and at least two law enforcement officers to protect the victims and EMS/fire personnel.
Critical Thinking & Risk-Based Decision MakingWith these new challenges for EMS comes the need for critical thinking and decision making that reduces risk as much as possible for responders. Since the attackers have designed these incidents to overwhelm local resources, it is imperative that EMS personnel be aware of potential threats and be prepared to look for unconventional approaches to miti-gate the situation.
Critical thinking involves being open-minded to alternatives, judging source credibility when information is received, asking clarifying questions, forming a hypothesis and drawing conclusions based on available infor-mation. Critical thinking is also being cautious about conclusions, under-standing that conclusions can change based on new information. The good news is that EMS providers use criti-cal thinking on everyday responses. Now they need to use their critical thinking skills in an expanded manner
to encompass larger and more complex incidents. Critical thinking is not making uninformed snap decisions; rather, it requires making the best decision quickly based on current information.
Everyone, every day makes risk-based decisions,7 but with the higher stakes in an atypical incident, risk-based decision making is a criti-cal component of good outcomes. To make a risk-based decision, EMS per-sonnel should ask these questions:
» What can go wrong? » How likely is it that it will go
wrong? » Is the risk of the potential prob-
lem tolerable? What can be done to lessen the risk of the problem?
This process helps respond-ers evaluate current information to make informed choices that lead to improved outcomes. This process
involves a decision structure, risk assessment, risk management, and impact assessment that should lead to appropriate risk communica-tion. Basically by asking the above questions, then applying the answers to the risk assessment, you can then make decisions to manage the risk and anticipate possible impacts of your decision. Once you have worked through this process, you then com-municate what steps need to occur and then reassess the situation.8
EMSWORLD.com | MARCH 2016 4342 MARCH 2016 | EMSWORLD.com

It’s another busy Friday night for your medic unit when you are dispatched to a motorcycle collision on the highway.
You arrive on scene to find a 32-year-old male lying on the highway moaning
in pain. He has a significant amount of road rash on his right side and an obvious open right lower extremity deformity. The patient does not believe he lost consciousness, but cannot precisely recall the events surround-ing the crash. He was helmeted and has no obvious external signs of head trauma.
You splint his leg and get him into the ambulance for a secondary assessment. His initial vital signs are: heart rate of 115, blood pressure of 95/65, a respiratory rate of 24 and an oxygen saturation of 97% on room air. He appears anxious and has dif-fuse abdominal pain on palpation.
While en route, you place a 16-gauge IV, hang a liter of normal saline and run it wide open. A repeat blood pressure taken five minutes later is 80/60 and the patient has become slightly confused. You are con-cerned he is in hemorrhagic shock and you grab another liter of normal saline. While starting your second bag, you remember hearing about “permissive hypotension,” but are unsure what blood pressure param-eters are considered safe for this patient or whether this patient is even a candidate for this treatment.
IntroductionThe theory behind permissive hypotension in the actively hemorrhaging trauma patient is not new. The idea dates back to the early 20th century when a group of captains in the Army Medical Corps described their experience managing injuries during World War I, noting, “Injection of a fluid that will increase blood pressure has dangers in itself. If the pressure is raised before the surgeon is ready to check the bleeding that may take place, blood that is sorely needed may be lost.” 1
Unfortunately, these recommendations were largely forgotten for most of the 20th century despite several animal studies per-formed in the 1950s and 1960s.2
The most current debate regarding hypo-tensive versus normotensive resuscitation strategies for trauma patients was sparked by a landmark randomized controlled trial (RCT) in 1994, which demonstrated a sig-nificantly lower mortality rate in hypoten-sive patients with penetrating torso trauma who received no or very little fluid resuscita-tion prior to the operating room.3
The theory behind permissive hypoten-sion is that overly aggressive crystalloid administration leads to worsened outcomes via clot disruption (“popping the clot”), dilu-tional coagulopathy, dilutional anemia and hypothermia, all of which contribute to the
“lethal triad” of coagulopathy, acidosis and hypothermia.
In theory, permissive hypotension main-tains a careful balance between organ per-fusion and the risk of bleeding or rebleed-ing. It should be understood that permissive hypotension is neither a treatment nor a substitute for surgery or definitive hemor-rhage control, and it currently only applies to trauma patients who are actively exsan-guinating in the prehospital or ED setting while awaiting resuscitation with blood products and emergent damage control sur-gery. Per the permissive hypotension theory, only once the bleeding is controlled should aggressive attempts be made to restore nor-mal physiology.
Animal StudiesIn the early 1990s numerous animal studies using rats, swine and sheep were performed to compare techniques for fluid resuscita-tion in uncontrolled hemorrhage.
In 2003, a systematic review of 52 RCTs in animal models included nine trials that compared a normotensive (mean arterial pressure >80 mmHg) versus hypotensive resuscitation strategy.4 Five of these trials used rat models, while four used a porcine model. Uncontrolled hemorrhage was induced under anesthesia. When compared to normotensive resuscitation, animals who received hypotensive resuscitation had a 67% lower risk of mortality. The obvious limitation of this study was the use of ani-mal subjects, as well as the use of a wide variety of anesthetics with different hemo-dynamic properties.
A more recent animal study in 2011 attempted to determine an ideal target mean arterial pressure (MAP) and maximal tolerable duration of hypotension during uncontrolled hemorrhagic shock in rats.5 After splenic parenchyma and splenic artery transection, uncontrolled hemorrhage continued for 20–30 minutes. Afterward, rats (who, coincidentally, have the same MAPs as humans) were fluid-resuscitated with different target MAPs for one hour. Hemostasis was then achieved by splenic artery ligation. Animal survival and sur-vival time in the 50- and 60-mmHg target MAP groups were higher than in all other groups, including the no-treatment group. This was statistically significant. Therefore,
Permissive Hypotension in TraumaPermissive hypotension can be a viable strategy in the prehospital setting when used appropriately
By Hawnwan Philip Moy, MD, & Abigail Cosgrove, MD
EMSWORLD.com | MARCH 2016 4544 MARCH 2016 | EMSWORLD.com
Photos courtesy of the Richmond Ambulance Authority, raaems.org

In patients with penetrating injuries and short transport times (less than 30 minutes), fluids should be withheld in the prehospital setting in patients who are alert or have a palpable radial pulse. Fluids (in the form of small boluses, i.e., 250 mL) should be given to return the patient to a coherent mental status or palpable radial pulse. In the setting of trau-matic brain injury, however, fluids should be titrated to maintain systolic blood pressure greater than 90 mmHg (or mean pressure greater than 60 mmHg).”15 The most cur-rent Advanced Trauma Life Support (ATLS) guidelines now recommend limiting initial resuscitation to 1 liter of crystalloid, which is an update from their prior recommendation of 2 liters.16 However, these guidelines do not provide blood pressure goals.
The Europeans have been advocating per-missive hypotension for over a decade. As early as 2002, expert consensus guidelines from the United Kingdom stated: “Fluid should not be administered to trauma vic-tims before haemorrhage control if a radial pulse can be felt. Judicious aliquots of 250 mL should be titrated for other patients. If the radial pulse returns, fluid resuscitation can be suspended for the present and the situation monitored. In penetrating torso trauma the presence of a central pulse should be considered adequate.”17
Additionally, it was recommended that transfer never be delayed due to attempts to obtain IV access. These guidelines were rein-forced two years later by the National Institute for Health and Clinical Excellence (NICE).18
Finally, the most updated European con-sensus guidelines published in 2010 recom-mend “a target systolic blood pressure of 80 to 100 mmHg until major bleeding has been stopped in the initial phase following trauma without brain injury (Grade 1C).”19 The guidelines also state, “A controlled hypotensive fluid resuscitation should aim to achieve a mean arterial pressure of 65 mmHg or more.”
Bottom LinePermissive hypotension for uncontrolled hemorrhage is the first major component of damage control resuscitation that seeks to avoid excessive fluid administration in the actively exsanguinating trauma patient. Potential benefits include the prevention of clot disruption, hemodilution, hypothermia,
and metabolic acidosis. However, it is impor-tant to recognize that permissive hypoten-sion is neither a treatment nor a substitute for definitive hemorrhage control.
As there is significant heterogeneity among trauma patients with regard to mechanism (blunt vs. penetrating) and injury severity, this strategy must be care-fully selected for and is often presented as a contraindication in certain patient popula-tions, such as those with traumatic brain injury or long transport times. Regardless, it is imperative that the prehospital provider not miss non-hemorrhagic causes of hypo-tension such as tension pneumothorax.
While there is a paucity of well-conduct-ed RCTs comparing hypotensive with nor-motensive resuscitation strategies, all stud-ies have demonstrated either improved or, worst-case scenario, unchanged outcomes for blunt or penetrating trauma patients who have been managed with permissive hypotension in the prehospital setting. The question remains if we should be titrating to blood pressure at all (as opposed to men-tal status or strength of peripheral pulses), and if so, what the optimal blood pressure should be. Current guidelines have trended toward recommending small fluid boluses with minimum MAP goals cited anywhere between 50–65 mmHg, SBP between 70–90 mmHg, or titration to return of a radial pulse or cerebration.
Until future RCTs demonstrate that this approach is truly harmful to the actively exsanguinating trauma patient, permissive hypotension can be a viable strategy in the prehospital setting when used appropriately in the right patient, setting, and if an option in your protocols.
Case ConclusionAfter administering 500 mL of normal saline, you are able to palpate a radial pulse on your motorcycle collision patient. You decide to hold on further fluid administra-tion and pull into the ambulance bay with-in five minutes. On arrival, your patient’s blood pressure remains 80/60, and resus-citation with blood products is initiated. The patient ultimately goes to the operating room with orthopedic surgery for fixation of pelvic fractures and a femur fracture. He does well post-operatively and leaves the hospital three days later.
RE FE RE N CE S
1. Cannon WB, Fraser J, Cowell EM. The preventive treatment of wound shock. JAMA, 1918; 70:618–21.2. Wiles MD. Blood pressure management in trauma: from feast to famine? Anaesthesia, 2013; May;68(5):445–93. Bickell WH, et al. Immediate versus delayed fluid resuscitation for hypotensive patients with penetrating torso injuries. N Engl J Med, 1994; 331:1105–1109.4. Mapstone J, Roberts I, Evans P. Fluid resuscitation strategies: a systematic review of animal trials. J Trauma, 2003; Sep;55(3):571–89.5. Li T, Zhu Y, Hu Y, et al. Ideal permissive hypotension to resuscitate uncontrolled hemorrhagic shock and the tolerance time in rats. Anesthesiology, 2011; 114(1):111–119.6. Turner J, Nicholl J, Webber L, Cox H, Dixon S, Yates D. A randomised controlled trial of prehospital intravenous fluid replacement therapy in serious trauma. Health Technol Assess, 2000; 4:1–57.7. Dula DJ, et al. Use of prehospital fluids in hypotensive blunt trauma patients. Prehosp Emerg Care, 2002; 6(4):417–420.8. Sampalis JS, et al. Ineffectiveness of on-site intravenous lines: is prehospital time the culprit? J Trauma, 1997; 43(4):608–615.9. Kwan I, Bunn F, Roberts I. Timing and volume of fluid administration for patients with bleeding. Cochrane Database Syst Rev 2003, CD002245.10. Talmor D, et al. Treatment to support blood pressure increases bleeding and/or decreases survival in a rat model of closed head trauma combined with uncontrolled hemorrhage. Anesth Analg, 1999; 89:950–956.11. Bourguignon PR, Shackford SR, Shiffer C, Nichols P, Nees AV. Delayed fluid resuscitation of head injury and uncontrolled hemorrhagic shock. Arch Surg, 1998; 133:390–8.12. Chesnut RM, et al. The role of secondary brain injury in determining outcome from severe head injury. Journal of Trauma, 1993; 34: 216–2213. Bratton SL, et al. Guidelines for the management of severe traumatic brain injury. I. Blood pressure and oxygenation. J Neurotrauma, 2007; 24(Suppl 1):S7–13.14. Berry C, et al. Redefining hypotension in traumatic brain injury. Injury, 2012; 43: 1833–7.15. Cotton BA, et. al. Guidelines for prehospital fluid resuscitation in the injured patient. Eastern Association for the Surgery of Trauma (EAST) practice management guideline. J Trauma, 2009; 67(2):389–402.16. American College of Surgeons, Committee on Trauma. ATLS: Advanced Trauma Life Support Student Course Manual 9th ed. Chicago, IL: American College of Surgeons, 2012.17. Revell M, Porter K, Greaves I. Fluid resuscitation in prehospital trauma care: a consensus view. Emerg Med J, 2002; 19:494–498.18. National Institute for Health and Clinical Excellence. Pre-hospital initiation of fluid replacement therapy in trauma. Technology appraisal 74. January 2004.19. Rossaint R, et al. Management of bleeding following major trauma: an updated European guideline. Critical Care, 2010; 14: R52.
AB O U T THE AU TH O RS Hawnwan Philip Moy, MD, is an assistant medical director of the St. Louis City Fire Department, emergency medicine clinical instructor and core faculty of the EMS Section of the Division of Emergency Medicine at Washington University in St. Louis, MO.
Abigail Cosgrove, MD, is a second-year emergency medicine resident at Washington University in St. Louis, MO. She currently serves on the board of directors for the Emergency Medicine Residents’ Association and is the editor in chief of EM Resident magazine. Her interests include prehospital medicine, cardiovascular emergencies and pediatric emergency medicine.
researchers concluded that 50–60 mmHg may be the ideal hypotensive resuscitation target MAP in uncontrolled hemorrhage.
Using a new target MAP of 50 mmHg, they found that when comparing a 60-, 90- or 120-minute duration of permissive hypotension, rats subjected to 120 minutes of hypotension had significantly lower sur-vival times, as well as worsened renal and hepatic mitochondrial function. Addi-tionally, they concluded that more than 90 minutes of hypotensive resuscitation could cause severe organ damage and should be avoided. Obviously, the most fundamental limitation of these studies is that the appli-cability of animal models to human injury remains unclear.
Human StudiesWhile the previously mentioned landmark prospective RCT in 1994 compared fluid resuscitation strategies in hypotensive patients with penetrating torso injuries,3 an RCT from the United Kingdom in 2002 looked at the effect of two different prehos-pital fluid protocols on overall mortality for 1,309 trauma patients, of whom more than 90% suffered blunt trauma.6
Paramedics in two ambulance services were randomly allocated to one of two treat-
ment protocols. Protocol A required that IV fluids be administered on scene to all adult trauma patients who, under current procedures, would have had fluids started. Protocol B required that fluid be withheld until arrival to the hospital, unless time of transport was greater than one hour.
Overall there was no difference in six-month mortality between the groups. However, this study has been criticized for its questionable randomization technique, poor protocol compliance and poor alloca-tion concealment.
An additional—albeit retrospective—study evaluating resuscitation strategies in patients with blunt trauma compared 150 hypotensive (SBP < 90 mmHg) patients who received either more than 500 mL fluid or
no fluid at all in the prehospital setting.7 They were matched by Injury Severity Score (ISS) and SBP on scene, with primary out-come being SBP on arrival to the ED. While the group who received fluids had a signifi-cantly higher SBP on arrival, there was no difference in survival to hospital discharge after adjusting for age, SBP and ISS.
Another prehospital study sought to determine if there was an association between mortality and the act of simply initiating on-site intravenous fluid replace-ment in prehospital trauma patients suf-fering from blunt or penetrating trauma.8 It compared 217 patients who had on-site intravenous fluid replacement (IV group) with an equal number of matched patients without IVs (no-IV group) and found sig-nificantly higher seven-day mortality in the IV group (23% vs 6%, p < 0.001).
After adjusting for variables including age, gender, ISS, mechanism of injury and prehospital time, the use of on-site IV fluid replacement was associated with a signifi-cant increase in mortality. Additionally, when evaluating the association between prehospital transport times and mortal-ity, researchers found that for prehospital times of less than 30 minutes, the use of IV fluid replacement provided no benefit. For
prehospital times exceeding 30 minutes, it was associated with an increased risk of mortality.
Regardless, a Cochrane Review in 2003 (with a most recent search run in 2014) found insufficient evidence for
or against the use of early or larger volumes of IV fluid administration in uncontrolled hemorrhage.9 The review evaluated six trials including two discussed above3,6 in order to examine the effect of early versus delayed fluid administration, as well as larger versus smaller volume of fluid for the treatment of uncontrolled hemorrhage. It is important to note that this review was not restricted to trauma patients.
Traumatic Brain InjuryDiscussion of permissive hypotension in actively hemorrhaging trauma patients usually excludes patients with traumatic brain injury (TBI) due to concern for the risk of inadequate cerebral perfusion pres-sure. Unfortunately, the diagnosis of TBI
can be a difficult distinction to make in the prehospital setting, as altered levels of consciousness are often seen in polytrauma patients suffering hemorrhagic shock from major extracranial injuries, the administra-tion of opioid analgesia or the ingestion of alcohol or illicit drugs.
Most but not all studies on permissive hypotension in trauma patients exclude those with TBI. Interestingly, animal mod-els looking at effects of fluid resuscitation in rats and swine with both head injury and active exsanguination found that rats who underwent low-volume resuscitation had better neurologic outcomes and that pigs who were aggressively resuscitated had increased intracranial pressure and worse cerebral oxygen delivery, presumably sec-ondary to cerebral edema.10,11
This being said, a retrospective obser-vational study in 1993 showed that a single episode of hypotension (SBP < 90 mmHg) in severely brain-injured patients was asso-ciated with a doubling of mortality and a parallel increase in morbidity rates among survivors.12 Furthermore, patients whose hypotension was not corrected in the field had a worse outcome than those whose hypotension was corrected by time of ED arrival.
Guidelines published by the Brain Trau-ma Foundation in 2007 advocate maintain-ing SBP above 90 mmHg in severe TBI, but do not specifically state whether this applies to actively hemorrhaging patients.13 A more recent retrospective review actually recom-mended that the threshold for hypotension in TBI be redefined as SBP < 110 mmHg.14 Regardless, the Brain Trauma Foundation guidelines ultimately conclude, “Clinical intuition suggests that correcting hypoten-sion and hypoxia improves outcomes; how-ever, clinical studies have failed to provide the supporting data.”
Current GuidelinesTrauma guidelines in the United States are largely influenced by the Eastern Associa-tion for the Surgery of Trauma (EAST) Prac-tice Management Guideline Committee.
Its most recent set of guidelines for pre-hospital fluid administration from 2009 con-clude: “There is insufficient data to suggest that blunt or penetrating trauma patients benefit from prehospital fluid resuscitation.
It is imperative that the prehospital provider not miss non-hemorrhagic causes of hypotension such as tension pneumothorax.
EMSWORLD.com | MARCH 2016 4746 MARCH 2016 | EMSWORLD.com

be discouraged. An agency willing to engage in a systematic approach to policy development will find good news; these laws aren’t as set on thwarting your patient care attempts as you thought.
MIH-CP at the IntersectionJust like the general EMS discipline, MIH-CP pro-grams operate at the intersection of healthcare, public health and public safety. For example:
» A healthcare version of MIH-CP might deal primarily with chronic disease management or post-hospital discharge follow-up.
» A public health version of MIH-CP might include prevention, communicable disease moni-toring or immunization programs.
» A public safety version of MIH-CP might be involved in crisis intervention, frequent-user care coordination, or alternative destinations to preserve response readiness.
» A single MIH-CP program might operate in any combination of these.
Healthcare agencies and MIH-CP programs focused solely on healthcare often have straight-forward approaches to patient privacy because the majority of their transactions occur under the medi-cal umbrella. However, if your MIH-CP program
extends beyond the medical umbrella, chances are you have struggled, or are struggling, to make sense of privacy laws.
Medical privacy laws do address non-medical disclosures. For example, the Health Insurance Portability and Accountability Act (HIPAA) allows for disclosures for reasons other than healthcare activities, like public health interests, oversight and safety issues. A series of these permitted disclosures under HIPAA is contained in Title 45 of the Code of Federal Regulations, parts 160 and 164. Figure 1 shows samples of permitted disclosures (a majority drawn from §164.512 of HIPAA) organized to illustrate the types of disclosures with possible applications to the different MIH-CP categories.
The mission of the MIH-CP program will deter-mine what specific policies and procedures are need-ed for client care. Understanding the landscape of disclosures can help you identify and prioritize the order in which you choose to tackle the accompany-ing policies and procedures.
Consent Forms: The Catchall SolutionOne of the first and most important actions for your MIH-CP program is to develop a consent or autho-rization form to obtain permission from the client to disclose information for purposes of care. It is relatively uncomplicated to work with an attorney to create or modify a consent form. Additionally, an attorney should determine if your agency is able to operate with one form, or if you need any additional authorization forms for sensitive health issues.
Once the program has a consent form, the simplest, most conservative route to privacy compliance is to require that CPs use this form to gain consent from every client. In this case the CP is obtaining consent at times where the agency may not necessarily need it. On the other hand, it can give the CP authorization
Amid HIPAA and other rules, how should you approach the need to share protected health information?
Mobile integrated healthcare and community paramedic (MIH-CP) programs face a seemingly complex landscape when it comes to sharing and receiving protected health infor-
mation (PHI). With an expanded role in the com-munity, EMS operations are finding they may not have policies and procedures to guide community paramedics as they engage in this workflow. However, the decisions community paramedics make in regards to information-sharing can carry greater responsi-bility, require greater discretion or self-control, and introduce greater risk. For this reason administrators
are right to be concerned about developing policies, procedures and training for patient privacy in their MIH-CP programs.
This article focuses on a theoretical approach to patient privacy, rather than a technical approach. As it stands now, no single standard can indicate what is permitted and not permitted for the broad spectrum of MIH-CP programs. Each program must perform its own needs assessment and work with its legal teams to determine any relevant state law or additional requirements in place due to program funding, structure or treatment operations. If the idea of patient privacy feels overwhelming, don’t
By Anne M. Jensen, BS, EMT-P
The mission of the MIH-CP program will determine what specific policies and procedures are needed for client care.
FIGURE 1: PERMITTED DISCLOSURES
Healthcare » Disclosures for treatment
» Disclosures for payment
» Disclosures for healthcare operations
Public Health » Disclosures for public health and oversight activities
» Disclosures for public health research
» Disclosures to address a threat to health
Public Safety » Disclosures for abuse, neglect, domestic violence
» Disclosures for law enforcement/judicial purposes
» Disclosures to avert a threat to safety
EMSWORLD.com | MARCH 2016 4948 MARCH 2016 | EMSWORLD.com
Once your program has a comprehensive set of privacy standards, implement training, compliance and ongoing assessments and revisions.Lee Swanson
If your program requires additional policies to supplement a consent form, a systematic approach can make policy development less intimidating.Lee Swanson

Refine the list into categories. For example: » Information category—Medical information,
mental health information, substance abuse infor-mation, social information, service utilization.
» Recipient category—Coresponder on an incident; law enforcement; covered entity; noncovered entity.
Use the category lists to create a disclosure matrix. For an example, see Figure 3.
Step #3: Complete the Disclosure MatrixThe next step is to complete the privacy matrix.
The agency may already have policies for some of the boxes. For the remaining boxes, it is best to involve the agency’s legal team.
For each box, answer the question “Under what ethical and legal circumstances can I provide this disclosure?” Privacy law usually settles down into the following categories:
» Permitted without authorization from the client; » Permitted when disclosed to a partner or busi-
ness associate under a formal agreement; » Permitted with authorization from the client; » Required by law.
There may be times when your agency chooses to be more stringent than privacy laws. In that case you could add other categories. For example:
» Never; » Permitted without client authorization but
requires management approval.This may be especially relevant for disclosures that
require discretion. For example, disclosures to avert a serious threat require that the threat be credible and that the disclosure is expected to lessen the threat. It may be that management wants to exercise discre-tion and assess credibility before allowing the CP to make the disclosure.
With the matrix complete, the privacy concepts are ready to be written into policy.
Policies in ActionOnce the MIH-CP program has a comprehensive set of privacy standards, administrators should imple-ment training, compliance and ongoing assessments and revisions of the policies and procedures. Addi-tionally, as a closing concept, there is a cultural com-ponent to this new set of rules: CPs need training to
deal with the casual, and sometimes inappropriate, exchanges of information that take place in a com-munity setting that is not isolated to a 9-1-1 incident. The CP should be prepared with helpful scripts or otherwise understand that awkward social exchang-
es are normal when upholding the agency’s privacy standards. With a comprehensive set of policies and procedures, along with cultural preparedness, MIH-CP programs can eliminate a majority of the ambi-guity associated with privacy compliance and focus on other aspects of the new MIH-CP discipline.
AB O U T THE AU TH O R Anne M. Jensen, BS, EMT-P, is the Resource Access Program coordinator for San Diego Fire-Rescue Department and Rural/Metro of San Diego. With an inclination toward technology, she emphasizes meaningful patient care, using technology to expand capacity to serve and mitigate risk. E-mail [email protected].
Examples of these situations include care for clients with cognitive disabilities from dementia or men-tal illness, cognitive impairment due to substance abuse, or when the client is a threat to the safety of self or others. In other words, CP programs with a crisis intervention component, or those that deal with cognitively vulnerable individuals, may not be as effective without policies and procedures to cover disclosures in these cases.
Going Further With Policy DevelopmentIf the program requires additional policies to supple-ment a consent form, a systematic approach will make policy development less intimidating. The following instructions represent one approach to building a comprehensive set of policies and procedures, though it is certainly not the only approach.
Step #1: Perform a Gap AnalysisA gap analysis may sound formal or arduous, but
a person familiar with the workflow of the CP could perhaps accomplish this in less than a day. In this case a gap analysis involves comparing existing policies and forms to a list of desired policies (see Figure 2).
The goal of this process is to create a wish list of disclosures. If the disclosure doesn’t seem permitted under current law, include it anyway. The resulting list should contain items that seem both possible and
impossible, not to get away with as much as possible but to create tools that will help the CP be the best advocate for the patient.
Step #2: Create a Disclosure Matrix FormDivide the list from Step #1 into two parts: one list
for the type of information disclosed, and another for the recipient. For example:
» Information type—Medical information, number of hospital visits, mental health diagnosis, etc.
» Recipient types—Law enforcement, hospitals, primary care physicians, etc.
FIGURE 3: SAMPLE DISCLOSURE MATRIX
Covered Entity Noncovered Social Entity
Law Enforcement
Coresponder Family/Friends
Demographics/svc. util.
Medical info.
Mental health info.
Substance abuse info.
Communication Comple xitiesAs mobile integrated healthcare and community paramedic (MIH-CP) programs create new services to help patients, one of the challenges they will face is how best to develop important policies and procedures to guide CPs in their new roles. One critical consideration will be how to provide patients the new types of assistance they need while maintaining the patient’s privacy. This month community paramedic innovator Anne Jensen describes a comprehensive approach to developing those policies and procedures that will help CPs and their administrators think through the various ways patients’ information will need to be exchanged.
Community paramedics conduct a broad assessment of the patient that reveals medical, mental health, social, economic, environmental and other factors that influence the patient’s health. To provide the variety of resources needed to help the patient, CPs not only need to share these new types of information with healthcare entities, but with mental health, social service agencies, police and others that may not be covered by the agency’s current privacy-related policies and procedures. Anne’s framework for defining the types of information and entities that might be involved is an incredibly useful tool for agencies and attorneys to understand the complex but mission-critical nature of these communications. Thanks to Anne for sharing her experience and guidance in navigating these new regulatory areas.
—Dan Swayze, MIH-CP Advisor
More Than HIPA AHIPAA may not be the only privacy standard that’s applicable to your MIH-CP program, though it is the most dominant. Other laws and situations may apply:
» State privacy laws—States may have their own privacy laws to consider. HIPAA has specific text to define the relationship between federal and state laws, and an attorney is best suited to interpret this relationship.
» Privacy requirements associated with federal funding—MIH-CP programs that anticipate receiving federal funds for targeted efforts, such as substance abuse or mental health efforts, may need to look at additional privacy standards.
» Privacy requirements associated with organizational structure—If you employ care providers other than CPs, like certain licensed mental health professionals, your organization may be subject to a higher level of confidentiality.
A summary of selected federal laws and regulations addressing confidentiality, privacy and security can be found at https://www.healthit.gov/sites/default/files/privacy-security/federal-privacy-laws-table2-26-10-final.pdf.
to disclose information to any entity specified on the consent or authorization form. This could include entities to which HIPAA provides no provisions or where there is ambiguity.
This is certainly a valid approach, and some agen-cies may be able to operate fully with a 100% consent policy. However, some programs require the CP to initiate care prior to any opportunity for consent.
EMSWORLD.com | MARCH 2016 5150 MARCH 2016 | EMSWORLD.com
Have your CP clients sign a consent or authorization form that allows you to disclose their information to other caregivers.Lee Swanson
FIGURE 2: EXAMPLE GAP ANALYSIS
Existing:
Policies » Field disclosures to ER
» Field disclosures to law enforcement
Authorization forms » Disclosures to media
Needs development:
Policies » Field disclosures to primary care
» Field disclosures to substance abuse
treatment center
» Nonmedical disclosures during a crisis
» Disclosures to family

PRODUCT APPLICATIONS Interviews with end users of EMS products
ADVERTORIAL
Connecting Rural Care ProvidersWhen the nearest hospital is miles away,
advanced communications can shorten the
distance between the patient and lifesav-
ing care.
Matt Tatum, MA, NREMT-P, FF, director of
public safety for Henry County, VA, knows
this firsthand. For the past year, emergency
services in his rural community have been
using the GD e-Bridge system. Often, he
says, “When we pick up the patient and get
them to the ambulance, we’re still 20 or 25
minutes from the closest hospital.”
With the e-Bridge system, EMS crews
now send secure text, photos, videos, ECGs
and other data from the scene to the hos-
pital emergency department. “It allows the
ED to be more prepared for what’s coming
in,” he says.
In other cases, Tatum says, the ED phy-
sician has used the system to alert a car-
diologist, who was at the hospital when
the patient arrived. And the ability to send
video clips has allowed EMS teams to get
physician input when assessing patients
for stroke or other conditions.
Tatum says the e-Bridge system also
helps improve care in a community that
relies on a combination of career and vol-
unteer EMS services.
“A lot of our volunteers are trained as
EMT-Basics only,” he says. “When they
get that critical patient, the career depart-
ments will bring them a paramedic if they
need it. With the e-Bridge system, the EMT
can send images or messages to the para-
medic before he or she gets on scene.”
It’s also helpful that the technology
requires little training.
Another advantage for Tatum’s commu-
nity: compatibility with the varied 12-lead
ECG technology used among nine first-
responder agencies in the region. “The GD
product is universal. It works with any of
them,” says Tatum.
As a next step, Tatum plans to trial
the live-streaming video capabilities of
e-Bridge and hopes to implement that
with a mobile integrated healthcare service
in the future. Plans are still in their early
stages, but Tatum foresees it as a way to
extend care into the community through
both scheduled patient visits and non-life-
threatening 9-1-1 calls.
Visit general-devices.com.
Circle 32 on the Product Information Card
EMSWORLD.com | MARCH 2016 53
Safe Patient LiftingEvery day EMS professionals are called to
lift assist fallen patients, meaning agencies
face the daily challenge of workforce safety.
The repetitive nature of lifting can cause
injury and subsequently lost work days.
Mangar’s ELK lifting cushion reduces
injury risk by minimizing the amount of
manual handling required. The compact,
portable and battery-powered lifting
cushion inflates at a push of a button,
raising patients from the floor to a seated
position. This makes it easy for them to be
transferred off or stand.
Chris Mulberry, assistant chief para-
medic of Platte Valley Ambulance Service
in Colorado, says his agency uses the lift-
ing cushion and is very satisfied with the
results.
“The nice part is that it’s not big or heavy,
and can be used anywhere,” Mulberry says.
The ELK can be used to lift patients of
any age and weighing up to 1,000 lbs. It
provides a comfortable, stable and most
importantly, dignified lift.
Chris Lokits of Louisville Metro EMS says
the lifting cushions has been “a blessing.”
“When doing a lift assist by myself I am
confident that I can successfully get the
patient up without hurting them or myself,”
he says.
Mulberry says the cushion is especially
useful when handling older patients.
“With elderly patients some have more
fragile skin because of the medications
they take. The cushion makes the lift safer
and more comfortable because we don’t
need to grab or yank the patient.”
Lokits says some elderly patients had
concerns at first that the cushion was not
stable but after a short explanation those
concerns subsided.
The ELK can be used indoors or out-
doors, and it is particularly useful if some-
one has fallen in a confined space. Provid-
ers can shimmy or roll a patient onto the
cushion, and once correctly positioned,
the ELK is inflated using a handset. Pro-
viders no longer have to dead-lift patients,
reducing the risk of injury.
Even though some contact with the
patient is still required, Lokits says the
product increases safety for both the
patient and the provider.
“With a decrease in IODs and workman’s
compensation claims, I believe this device
will soon pay for itself. It’s invaluable”
Prior to using the ELK lifting cushion,
Mulberry says his agency lifted patients
manually. He’s been extremely pleased
with the results and says, “EMS people
are hard on equipment, but this product
is durable and stands up to any EMS use.”
Visit mangarusa.com.
Circle 33 on the Product Information Card
What’s New in 2016 at Firehouse Expo:
Historic Opening Ceremony with a MUST SEE keynote address and the presentation of the Michael O. McNamee Valor Award.
More than 100 conference sessions presented by the nation’s most well-known and respected instructors.
All new hands-on training program, including live fire, RIT, engine and ladder company operations, high-rise operations, meth lab response, vehicle extrication, apparatus rodeo and more.
Second-annual Legends & Icons celebration, including the induction of the 2016 Firehouse Hall of Fame Class.
FIREHOUSECelebrating 40 years
of Service to America’s Bravest
For more information and registration rates, visit FirehouseExpo.com.Book Your Hotel Early! Rooms are filling up fast! #FHExpo16
®®

PRODUCT APPLICATIONS Interviews with end users of EMS products
ADVERTORIAL
The Right Tool for the JobIn EMS, it’s essential to have the right tools
for the job. Airon Corporation, based in
Florida, helps provide those tools to EMS
agencies across the country.
For Ronald Bray, of Nature Coast EMS,
this product was Airon’s pNeuton model
S ventilator with CPAP.
The pNeuton model S ventilator allows
you to start with mask CPAP and, if the
patient needs it, provide ventilation as well.
The product is completely pneumatic, so
battery or electrical power is not required.
Providers can choose between 100%
FiO2 or 65% using the device.
Bray says the products he had used before
didn’t have the ability to alter the FiO2. As a
rural agency, this caused some issues.
“The other product we had used was
completely oxygen generated,” Bray says.
“Some transports would be an hour long,
and you would need a trailer of oxygen
tanks to keep them that far.”
Bray says another big benefit of the
pNeuton model S is the ability to have the
ventilator. “We use the ventilator during
cardiac arrests, and it frees up a person
for resources,” Bray says. “It’s kind of like a
force multiplier. When we put the patient
on a ventilator, the paramedic is free to
work on other aspects of the patient.”
Bray says ease of use is another reason
the product has worked so well for his
organization, and he says it was easy to
implement as well.
“We did an in-service and made a lami-
nated card with bullet points for setting it
up and we were off and running,” Bray says.
“I don’t believe we’ve had any significant
operator error with the product.”
Bray says he would “very much” recom-
mend the product to other organizations.
Visit AironUSA.com.
Circle 34 on the Product Information Card
EMSWORLD.com | MARCH 2016 5554 MARCH 2016 | EMSWORLD.com
Quality Education for EMS StudentsA quality education is a big part of a suc-
cessful career in EMS, and Lenoir Commu-
nity College helps provide that education to
its students. Equally as important is provid-
ing an education that leadership currently
in place finds useful.
Mark LaMont, battalion chief, paramedic
and training officer at Idyllwild Fire Protec-
tion District in California, says his organi-
zation has worked with Lenoir Community
College since 2010.
LCC offers paramedic training to stu-
dents beyond its service area of Lenoir,
Jones, and Greene Counties in North
Carolina. It is one of only two CAAHEP-
accredited distance education paramedic
programs in the country.
“The Lenoir student’s knowledge, patient
care and ability to build patient rap-
port are outstanding,” LaMont says. “We
have found that Lenoir students are very
well-rounded.”
The college offers multiple EMS pro-
grams, including paramedic training, EMT-B
training, AEMT training and multiple out-
reach programs and bridge programs.
LCC also offers programs to enhance
EMS personnel’s existing knowledge, such
as advanced trauma education, critical
care education, EMS refresher courses,
pharmacology for paramedics and more.
LaMont says the process the students
go through leaves them aptly prepared for
their careers.
“Through the outreach programs, these
students are rotating through clinical and
hospital settings at the same time, and we
believe this provides the students with a
practical application during their studies,”
LaMont says. “This is rarely found in other
programs.”
LaMont also praises the administration
at Lenoir Community College.
“The administration is a pleasure to work
with, and is always helpful,” LaMont says.
LaMont says his organization has ben-
efitted greatly from working with LCC.
“The process of partnering with the col-
lege has allowed our paramedic employees
a unique opportunity to receive feedback
from their students, and it keeps our para-
medics on top of their skills,” LaMont says.
Visit lenoircc.edu.
Circle 36 on the Product Information Card
Top Notch Customer ServiceIn every field, customer service is of the
utmost importance.
Taylor Healthcare Products, Inc. places
an emphasis not just on their products, but
how they deliver them as well. In the eyes
of Taylor Healthcare, product quality and
customer service are equally important.
Lisa Gray of MedStar Mobile Healthcare
in Texas says Taylor Healthcare’s products
and customer service are top notch. “We
are extremely satisfied with their prod-
ucts,” Gray says.
“We have looked
at other products
in the past, but
have found these
to be superior in
quality and the
most cost effec-
tive products on the market.”
Gray raves about their customer service
as well. “The customer service is amaz-
ing,” Gray says. “We have had a mishap
or two with FedEx mishandling our pal-
lets, and Taylor Healthcare loaded vans
Staying Current on Tactical EMSContinuing to learn about your craft is nec-
essary to be the best. This concept does
not exclude paramedicine. With a new
focus in the profession on active shooter
situations and tactical EMS, the goals of
paramedics are changing to an extent.
The Journal of Special Operations Medicine
helps its readers accomplish these goals.
Established in 2000 and privately pub-
lished since 2011, JSOM aims to improve
quality of care by promoting education
among special operations forces medi-
cal personnel. The peer-reviewed journal
promotes the examination of the latest
advancements in unconventional medicine
and provides information and debate on
medical issues surrounding tactical emer-
gency medical support.
Bridging the gap between
military and civilian medicine,
JSOM provides practical and
sensible ideas and tech-
niques to the civilian TEMS
provider who operates in a tac-
tical environment.
The articles take real-world informa-
tion and present it for medical personnel
to implement in real time.
Robert Miller, a former Ranger medic,
now chief innovation officer at North
American Rescue, says this is a big part of
why he has been reading JSOM since the
publication’s beginnings. Miller says out
of the other educational publications on
the subject, he prefers JSOM. “It is a peer-
reviewed publication with content focused
on improving knowledge and
a skill set for tactical health-
care professionals world-
wide,” Miller says, explaining
his preference.
Miller says JSOM is innova-
tive and cutting edge in the way it
approaches the issues.
“The publication is on the leading edge,
providing not necessarily what is relevant
now, but what thought leaders envision
will be important in the near future and
on the horizon,” Miller says.
Because of this, Miller says he recom-
mends JSOM to others, and encourages
others to read it.
Visit jsomonline.org.
Circle 35 on the Product Information Card
Gray says they mainly
use the fleece blankets and
G-Force fitted sheets pro-
duced by Taylor Healthcare.
Taylor Healthcare provides
a wide array of products,
including its featured Tay-
lor Titan Soft Stretcher and
the Taylor G-Force SureFit
Disposable Stretcher Sheet
Series. Its products enhance
the patient experience by providing infec-
tion control, product performance and
comfort.
Gray says that compared to other compa-
nies, Taylor’s product and service are supe-
rior. “As a purchaser, I have looked at other
items in the past 10 years that I have been
associated with MedStar, and I have yet to
find any products that come close to their
quality that are cost effective,” Gray says.
Gray says she would certainly recom-
mend Taylor Healthcare’s products to any
other agencies, and she has in the past.
“We have not had any issues in all the
years we have used them,” Gray says.
Visit TaylorHealthcare.com.
Circle 38 on the Product Information Card
with pallets and drove them up from
Houston to Fort Worth. That’s what cus-
tomer service is all about.”
Great Products, Great ServiceAs a company, Bound Tree Medical focuses
on the quality of their service along with
the quality of their products.
Carl Flores, deputy director and chief of
New Orleans EMS, has experienced this
firsthand. Flores says they have contract-
ed with Bound Tree for nearly five years,
and have been pleased with the decision.
“The service and the variety of resourc-
es they provide has been the biggest ben-
efit,” Flores says. “For example, there have
been multiple times where they might
have been out of a product in one area,
but had it in another area and were able
to get it in.”
New Orleans EMS gets nearly all of their
products through Bound Tree, and Flores
says the quality of the products has been
exceptional.
Flores says one of the most impressive
things about Bound Tree, headquartered in
Ohio, is the ability of their local and mana-
gerial representatives to demonstrate their
commitment to every customer. “I would
have no problem recommending their com-
pany to other agencies,” Flores says.
Flores says Bound Tree has went above
and beyond for New Orleans EMS, espe-
cially in terms of customization.
In 2013, there was a shooting during
Mardi Gras on Bourbon Street. Flores says
looking back, one thing he noticed was
the inability to distinguish his paramed-
ics from the mass of people around the
ambulances.
Flores says Bound Tree helped him come
up with a solution to the problem, and his
paramedics’ bags and backpacks are now
a fluorescent yellow color to help identify
them in crowds. “Bound Tree works with
agencies to help provide solutions that you
might not even be aware exist,” Flores says.
Visit boundtree.com.
Circle 37 on the Product Information Card

58 MARCH 2016 | EMSWORLD.com
Pyng Medical www.pyng.com • (+1) 604-303-7964 • [email protected] • @pyngmedical • facebook.com/pyngmedical
Download the Clinical Review Papergo.pyng.com/Sternal-IO
ALL INTRAOSSEOUS SITES ARE NOT EQUAL
Clinical Studies Suggest the Sternal IO Route Improves Patient Outcomes
The quotes above are taken from three of the four important studies reviewed in the Clinical Review Paper by Dr. Alan Moloff. To download the full paper and access references (1), (2), and (3), visit
go.pyng.com/sternal-IO
Hoskins, Stephen L, et al: “Based on the present data, we recommend that sternal IO route be considered as the first choice of drug delivery during CPR when IV access has not been established…” (1)
Pasley, Jason, et al: “...the sternal IO site provided the highest flow rates compared with the humeral and tibial insertion sites. The sternal site was also associated with a 100% success rate for initial placement facilitated by its consistent anatomy.” (2)
Burgert, James, et al: “There may also be a relationship between the anatomical location of the IO device and serum drug concentrations; the more distal the IO infusion site is from the sampling site, the longer concentrations of drug take to rise.” (3)
1
2
3
THE MIDLIFE MEDIC By Tracey Loscar, NRP, FP-C
For More Information Circle 39 on Reader Service Card
EMS is a tough
lifestyle to maintain.
SecondsThere’s no time like today to fix your fitness
“When it comes to eating right and
exercising, there is no ‘I’ll start tomorrow.’
Tomorrow is a disease.”
—Terri Guillemets
One question I am often asked is,
“How did you end up in Alaska?”
A more appropriate question
might concern how I almost did
NOT end up in Alaska, and why.
During the interviews for my current position as bat-
talion chief I was told that I would have to take a physical
agility test (PAT). There would be no job offer if I did not
pass it, no matter how well I did on the interview. It was a
straightforward expectation. It included carrying equip-
ment, climbing stairs, performing CPR and executing a
proper lift with two 45-pound dumbbells.
These are all tasks I have done over the course of my
career, so...piece of cake, right? Except for the fact that
I had not done them all together, at one time, in years.
I am not small, never have been, but my size comes
with varying degrees of fitness depending on the when.
Driving a desk for the last few years, even the built-in
exercise you get from climbing in and out of an ambu-
lance with equipment had worn thin. The innate upper
body strength I had throughout my 20s and 30s has
eroded, and I let it.
EMS is a tough lifestyle to maintain. The hours are
long, the exercise irregular, the food choices impractical,
and the hormonal spikes caused by responding to calls
leave little souvenirs in your bloodstream in the form of
cholesterol and insulin. “Average” calls do not generally
require you to put in a lot of extra physical effort. Add to
this long hours and fatigue, and it is an easy thing to fall
(or stay) out of good physical shape.
After the panel interview the Chief took me to my PAT.
I was briefed on the details—walk so many feet, climb so
many stairs, carry this many pounds, do this much CPR,
etc. Oh, and I had to do it in full turnout gear. Wait, what?
I never wear turnout gear. At the agency I was from,
I was not required to wear it. I do not have my own set,
nor have I have ever practiced in it. Yet here I was, in a
mismatched set of gear with boots too big, coat too long,
no suspenders, and looking very much like Paddington
Bear. I did my best and finished each of the tasks exactly
as asked, 9 seconds too slow. I had failed the test they
told me nobody fails.
I stood on the apron, gulping air and water and looking
up at a slate grey sky over a foreign mountainous land-
scape. What am I doing here? Maybe I’m too old, too out
of shape. I was 4,000 miles from my home and family
and my dream was evaporating because I had allowed
myself to become a liability.
I am an excellent paramedic. I am who you want
making those critical clinical decisions for your loved
one when nobody else can. Trouble is, how can I call
the shots if after climbing some stairs I cannot catch
my breath long enough to speak? If this is not you then I
guarantee you’ve worked with someone for whom you’ve
made that exact observation, where you wondered how
they could do their job effectively in the shape they are in.
I was allowed to retake the test, this time with appro-
priately fitting equipment and better orientation with the
equipment being used. It was my last chance. I beat the
time by a full minute and 27 seconds. I refused to waste
this opportunity—if I am to do the job that I still love then
I need to function at the best of my ability. I am back in
the gym, back in the kitchen, and back to reprioritizing
my time and energy.
Eating well and exercising should be cultural norms,
not hobbies or side interests. Bring a cooler, make bet-
ter choices and do the research. Websites like www.fit
responder.com or www.555fitness.com have great
matching apps and offer strongly supportive programs
that anyone can do. Functional fitness is not a catch
phrase, it is a very real part of your job performance and
ability to remain in this field for the long term.
Recently my preceptor was briefing me on icy-road
procedures: Dispatch notified when on and off, number
of people (souls) on board, no seat belt, no USAR gear,
window open, no idling. My initial amusement faded as
I realized that what he was saying was that on these
calls there was an actual chance of a potentially lethal
incident occurring. That if the truck went through the
ice I would have to be able to get out and up in a hurry
—or else.
What if I was 9 seconds too slow?
AB O U T THE AU TH O R Tracey Loscar, NRP, FP-C, is a battalion chief for Matanuska-Susitna (Mat-Su) Borough EMS in Wasilla, Alaska. Her adventures started on the East Coast, where she spent the last 27 years serving as a paramedic, educator and supervisor in Newark, NJ. She is also a member of the EMS World editorial advisory board. Contact her at [email protected] or www.taloscar.com.

Visit www.Gaumard.com and learn why more educators use Gaumard solutions to train emergency and trauma care skills.
Toll Free USA | 800.882.6655 Worldwide | 305.971.3790 Sales Inquiries / Customer Service [email protected]
Trauma HAL lets you train triage, care, and transport with the highest degree of realism. Thanks to a fully wireless and tetherless design you can
simulate scenarios without interruptions, which improves communication and teamwork.
Meet the latest technology in active shooter and mass casualty simulation-based training.
Trauma HAL® S3040.100 · Rugged and splash proof · Active eyes, seizures, and programmable secretions · Difficult airway with surgical access · eCPRTM – Real-time CPR Monitoring · Use real monitoring devices: ECG, Defib, Oximetry, EtCO2, BP
· Bleeding trauma limbs (Quadruple amputee) · Tourniquet sensors · Pressure sensitive bleeding wounds and arterial sites · 1.5 Liter internal blood reservoir · Wireless and tetherless up to 900 ft. · Up to 10 hour battery life
For More Information Circle 40 on Reader Service Card
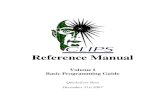









![Untitled-1 [g-devices.com]](https://static.fdocuments.in/doc/165x107/61b19288b1e60579ff4f0eb4/untitled-1-g-.jpg)







![Untitled-1 [g-devices.com]g-devices.com/site-content/uploads/2015/07/Suture-Instruments-Needle… · Directors and Probes A GLOME "Supporting Globally" 02-3962 02-3962 02-3963 02-3964](https://static.fdocuments.in/doc/165x107/60628c873141ee23591200e8/untitled-1-g-g-directors-and-probes-a-glome-supporting-globally.jpg)