
Community Acquired Pneumonia: Is Penicillin Resistance Relevant? Edward L. Goodman, MD, FACP, FIDSA,...
44
Community Acquired Pneumonia: Is Penicillin Resistance Relevant? Edward L. Goodman, MD, FACP, FIDSA, FSHEA June 30, 2008
-
Upload
cory-sanders -
Category
Documents
-
view
214 -
download
0
Transcript of Community Acquired Pneumonia: Is Penicillin Resistance Relevant? Edward L. Goodman, MD, FACP, FIDSA,...
Community Acquired Pneumonia: Is Penicillin Resistance Relevant?
Edward L. Goodman, MD, FACP, FIDSA, FSHEAJune 30, 2008

Basic Diagnostic Criteria
• History– Cough– Fever– Sputum production– Pleurisy
• Physical Exam– Altered breath sounds/percussion– Rales
• Imaging: CXR (PA/Lat if possible); CT not usually required
• Pulse Oximetry
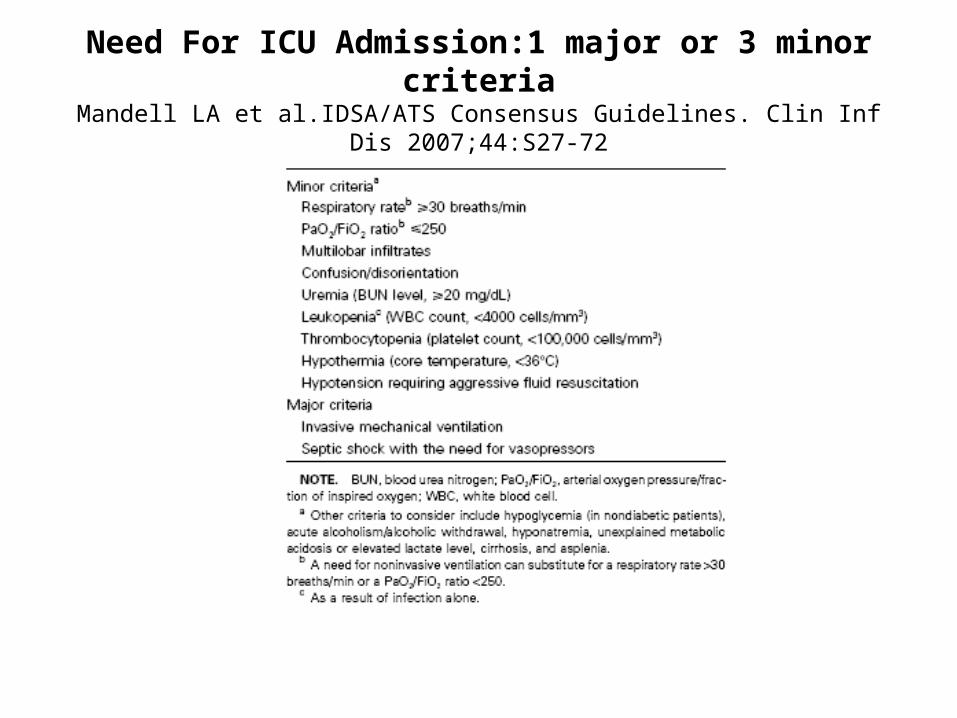
Need For ICU Admission:1 major or 3 minor criteriaMandell LA et al.IDSA/ATS Consensus Guidelines. Clin Inf Dis 2007;44:S27-72


ID Society/ATS Practice GuidelinesCID 2007;44:S45
• Recommended empirical antibiotics for community acquired pneumonia– Inpatients, non ICU treatment
• A respiratory FQ (level 1)• A beta lactam plus a macrolide (level 1)
– Inpatients, ICU treatment• A beta lactam (cefotaxime, ceftriaxone, amp/sulb) plus either
azithromycin (level 2) or respiratory FQ (level 1)• For pen allergic, aztreonam and respiratory FQ
– These Guidelines are the basis for CMS Scorecards• Failure to comply leads to diminished hospital reimbursement• Public reporting of compliance has started in 2008
Rationale for IDSA/ATS Guidelines
• Increasing Penicillin resistance
• Need for atypical coverage
• Availability of FQs which– Are highly bioavailable– Cover atypicals– Are rapidly bactericidal

Why Add Macrolide to Beta Lactam?
• To cover atypical pathogens which Beta Lactams don’t cover– Chlamydophilia– Mycoplasma– Legionella


Why Add Macrolides?
• Added benefit beyond antimicrobial effects?– Several retrospective studies suggested
better outcomes when macrolide added to beta lactam for bacteremic Pneumococcal pneumonia
• Etiology not in doubt• Postulated immunomodulatory effect
– Recent prospective study partially confirmed:• Baddour, Yu et al 2004

Am J Respir Crit Care Med 2004;170:440

Baddour L, Yu V et al. Combination Antibiotic Therapy Lower Mortality among Severely Ill Patients with Pneumococcal Bacteremia. Am J Resp Crit Care Med 2004; 170:440
What About Increasing Resistance to Penicillin?
• In 1968 we used Procaine Pen G 600,000 IM BID for CAP (presumed pneumococcal pneumonia)
• Much data on rising MIC’s for Strep pneumoniae– FQ’s activity not related to Pen “non
susceptibility”

US Region n
Penicillin-resistant (MIC ≥2 mg/L)
Penicillin intermediate (MIC 0.12 – 1 mg/L)
Erythromycin-resistant
(MIC ≥1 mg/L)
Erythromycin intermediate
(MIC 0.5 mg/L)
NORTH-WEST
422 17.3% 10.4% 23.2% 0.5%
NORTH-CENTRAL
2106 26.3% 11.3% 31.7% 0.1%
NORTH-EAST
3708 21.7% 11.5% 26.5% 0.3%
SOUTH-WEST
1349 27.0% 15.4% 29.3% 0%
SOUTH-CENTRAL
1455 32.5% 13.8% 38.6% 0.3%
SOUTH-EAST
1063 36.4% 14.0% 40.2% 0.2%
Distribution of Streptococcus pneumoniaeAntimicrobial Resistance Across the US
Doern G et al. J Infect 2004;48(1):56-65.
Net Effect
• Every febrile patient in ED with the slightest abnormal CXR gets Levaquin or Avelox!– Heavily promoted by drug makers– IDSA Guidelines indirectly encourage it
• Resistance to FQ rising at an alarming rate among E coli and Pseudomonas
• Rising rates of C diff and MRSA can be attributed, in part, to FQ pressure
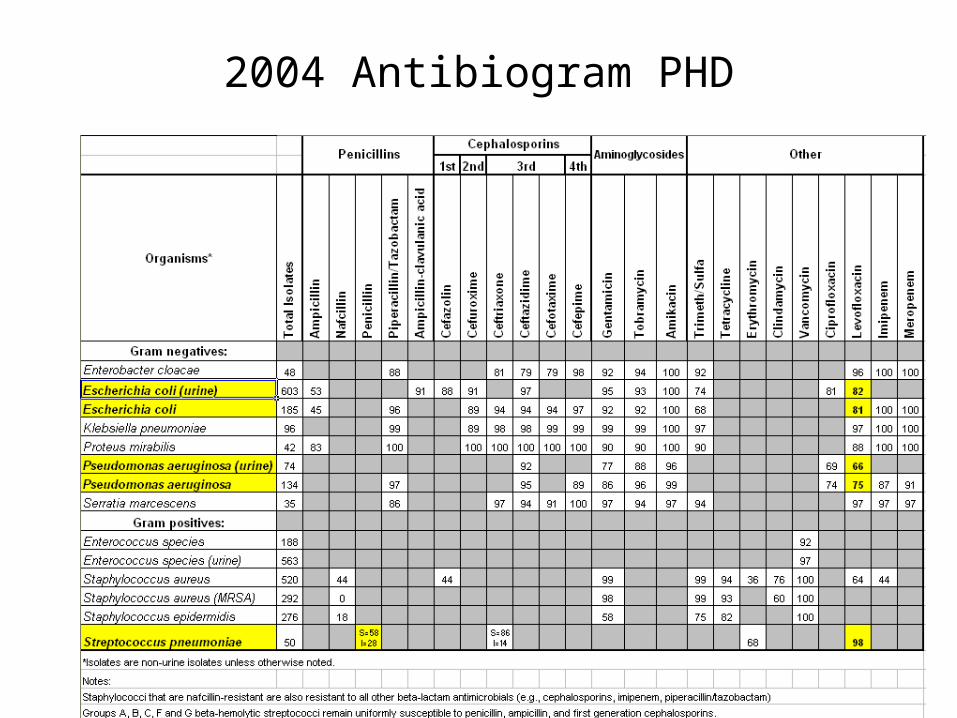
2004 Antibiogram PHD

2007 PHD
Is Penicillin Resistance Relevant in Treating CAP?
• Clearly in Pneumococcal meningitis resistance is critical– Poor penetration into CSF by penicillin– Immunologically “privileged sanctuary”
• No complement• Minimal immunoglobulin
• Not relevant in pneumonia or bacteremia
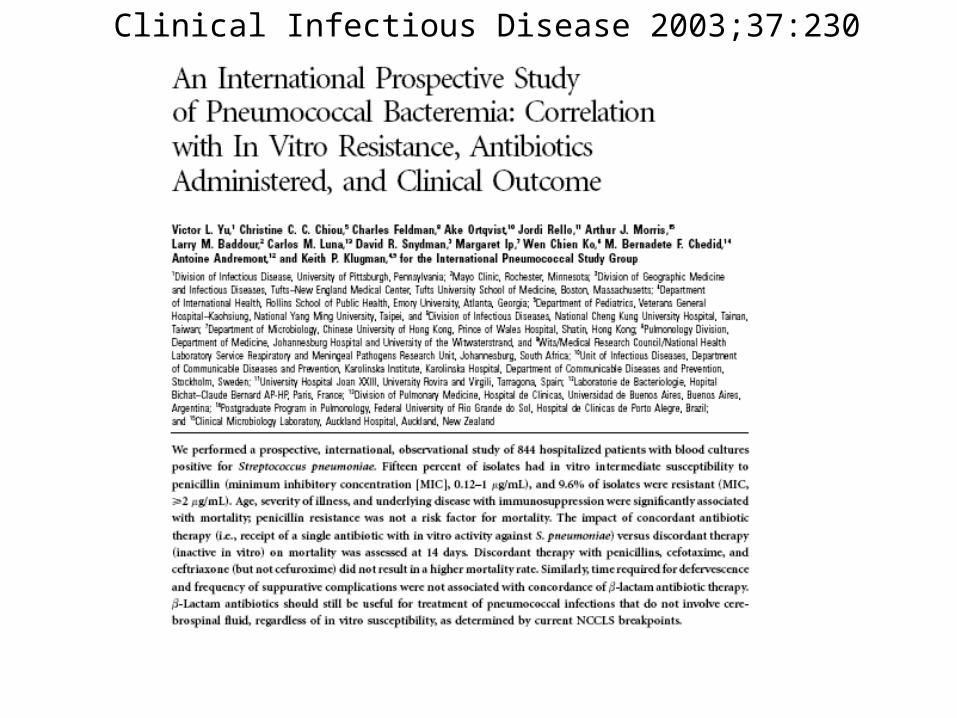
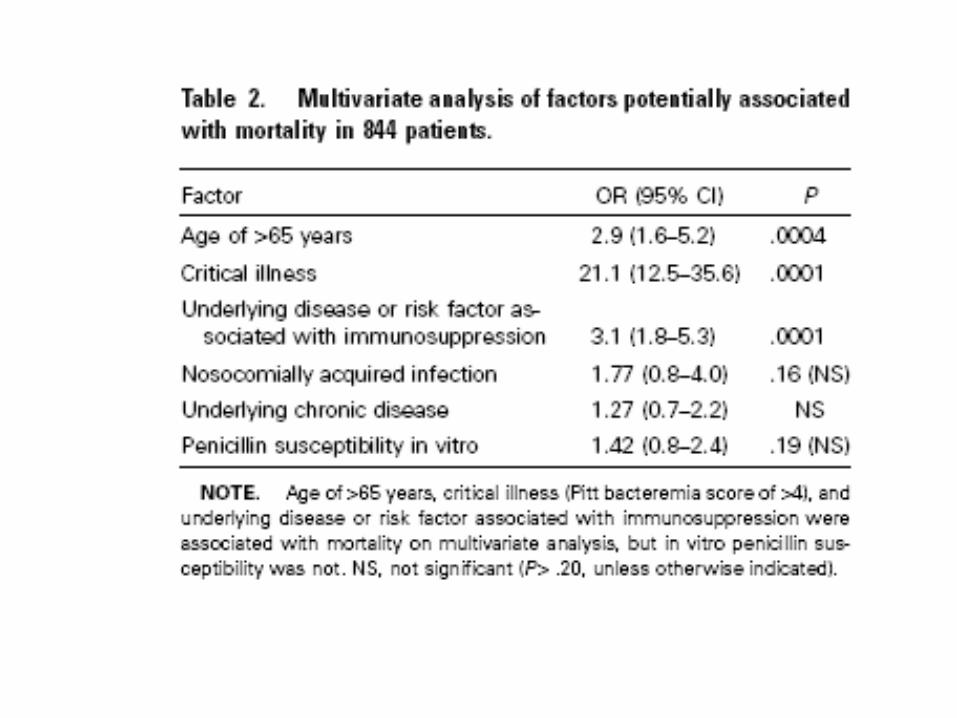
Clinical Infectious Disease 2003;37:230



To Recap
• IDSA/ATS Guidelines are basis for “scorecards” judging adequacy of therapy for CAP
• These Guidelines “favor” monotherapy with Fluoroquinolones
• FQ resistance and “collateral damage” rising
• Penicillin “resistance” redefined – irrelevant for CAP and bacteremia

Solution?
• Amoxicillin/clav (Augmentin XR) 2 gm po BID (with macrolide on admission)– ampicillin/sulbactam IV is included in
IDSA/ATS guidelines• Amox/clav microbiologically equivalent for
respiratory pathogens
– Serum levels of 2 gm amox well above MIC for Strep pneumo
• Therefore, less pressure to use FQ
Edward L Goodman

Query to Dale Bratzler, DOCMS consultant 5/14/08
• For empiric Rx of non-ICU CAP, why not use po Amoxicillin/clavulanate XR (plus an oral macrolide) for those patients who could take an oral regimen?
• For non-ICU CAP where the etiology is known with reasonable certainty, will specific therapy be a “fallout” if it is not in the IDSA/ATS Guidelines?

Responses from Dr. Bratzler
• “With the exception of oral fluoroquinolones, oral antibiotics are not recommended for the treatment of hospitalized patients with pneumonia – at least not initial therapy.”
• “I am not sure of the exact bioavailability of Augmentin, but it is not recommended in the Guidelines and will not be in the pneumonia performance measure.”
• “I think this is a fine choice for an outpatient. I am not aware of studies of treatment of inpatient pneumonia with ….Augmentin.”
Bratzler - continued
• “…if a patient has a positive test for a pathogen (and the test result is available to the physician within the first 24 hours of admission), the case is excluded from the antibiotic selection performance measure.”

Can We Refute Bratzler?
• “I think this is a fine choice for an outpatient. I am not aware of studies of treatment of inpatient pneumonia with ….Augmentin”

Augmentin XR® Package Insert
• Four randomized, controlled, double blind and one non comparative studies in adults with CAP
• In comparative studies 904 patients• In non-comparative study 1122 patients
• Dose: Amoxicillin 2 gm/clavulanate 125 mg po BID
• Results: – Comparative: 86.3% - 94.7% clinical success– Non comparative: 85.6% clinical success

Augmentin XR® Package InsertClinically Evaluable with Reduced Susceptibility to Penicillin
Penicillin MIC
n/N % 95% C.I.
All Strep pneumo
275/297 92.6% ----
MIC = 2 18/18 100% 81.5-100
MIC>2 24/25 96% 79.6-99.9
MIC>=4 6/7 85.7% 42.1-99.6

Should I Appeal to CMS?Gustave Dore 1863 Don Quixote Tilting at Windmills

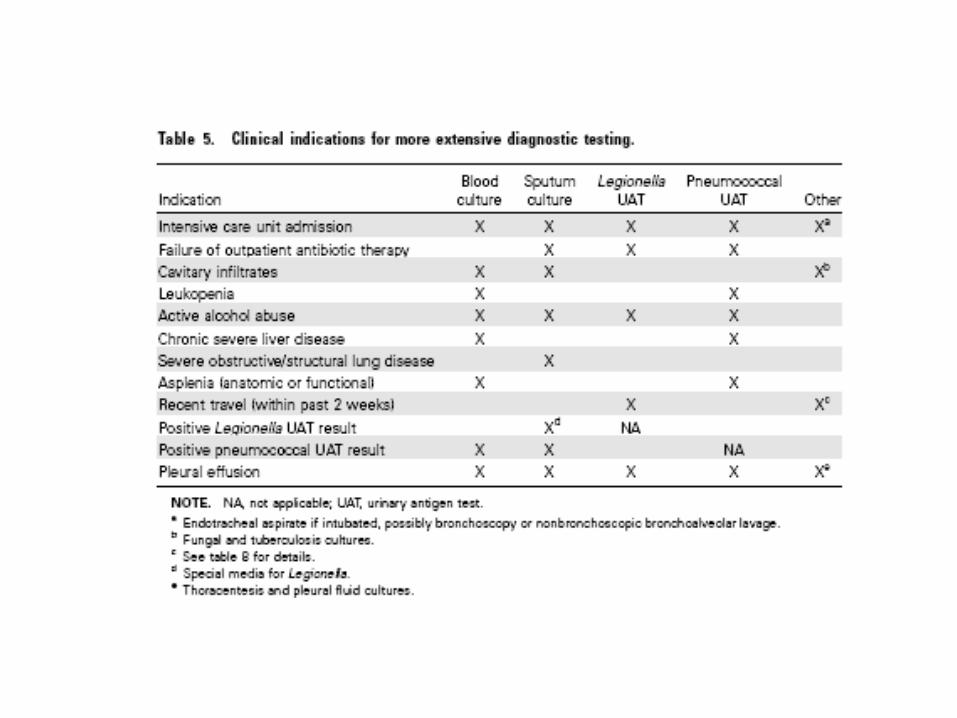
Rapid Detection of Etiology
• “…if a patient has a positive test for a pathogen (and the test result is available to the physician within the first 24 hours of admission), the case is excluded from the antibiotic selection performance measure.”– Excluded from report cards!– Less need for broad spectrum, empiric therapy – e.g.,
fluoroquinolones
• Only two current rapid diagnostic tests exist– Sputum gram stain– Urine Pneumococcal Antigen test



Musher DM et al. Diagnostic Value of Microscopic Examination of Gram-stained Sputum and Sputum Cultures in Patients with
Bacteremia Pneumococcal Pneumonia. Clin Inf Dis 2004;39:165-9
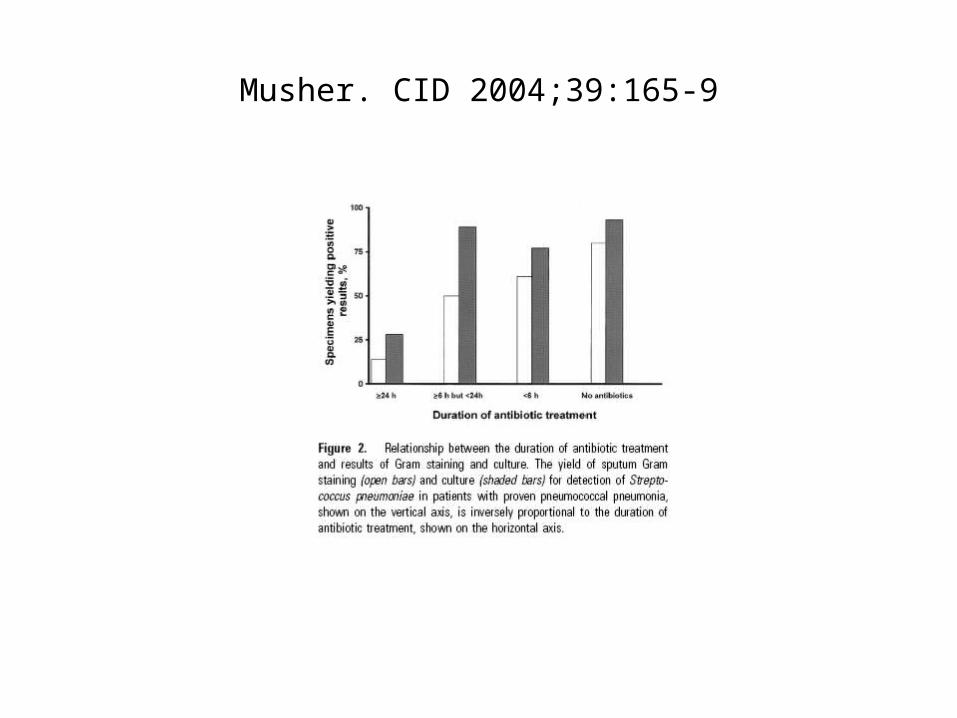
Musher. CID 2004;39:165-9
Pneumococcal Urine Antigen
• Sensitivity: 70-80%
• Specifity:>90%– False positives
• In children• Recently vaccinated • Remains positive for several weeks

Conclusions
• Urine Antigen on all cases of CAP– If positive
• consider treatment with amoxicillin 1 gm po TID or IV ampicillin 1 gm Q6H
• Not included in calculation of score cards
– If negative• Follow IDSA Practice Guidelines
• Obtain induced sputum for gram stain and culture– Lower sensitivity requires initial adherence to IDSA/ATS
Guidelines– Allows potential for pathogen identification
• allows sensitivity tests• Allows switch to narrow spectrum therapy – i.e., amoxicillin

ID Society/ATS Practice GuidelinesCID 2007;44:S45
• Recommended empirical antibiotics for community acquired pneumonia– Inpatients, non ICU treatment
• A respiratory FQ (level 1)• A beta lactam plus a macrolide (level 1)
– Inpatients, ICU treatment• A beta lactam (cefotaxime, ceftriaxone, amp/sulb)
plus either azithromycin (level 2) or respiratory FQ (level 1)
• For pen allergic, aztreonam and respiratory FQ
Bibliography
• Baddour LM, Yu VL et al. Combination Antibiotic Therapy Lowers Mortality among Severely Ill Patients with Pneumococcal Bacteremia. Am J Resp Crit Med 2004;170:440.
• Mandell LA, Wunderlink RG et al. Infectious Diseases Society of America/American Thoracic Society Consensus Guidelines on the Management of Community Acquired Pneumonia in Adults. Clin Infect Dis 2007;44:S27-42.
Bibliography
• Musher DM, Montoya R, Wanahita,A. Diagnostic Value of Microscopic Examination of Gram-Stained Sputum and Sputum Cultures in Patients with Bacteremia Pneumococcal Pneumonia. Clin Infect Dis 2004;39:165.
• Werno AM, Murdoch Dr. Laboratory Diagnosis of Invasive Pneumococcal Disease. Clin Infect Dis 2008;46:926.
• Woodhead M. Community-Acquired Pneumonia Guidelines an International Comparison: A View from Europe. Chest 1998;113:183.

Bibliography
• Williamson, S (Personal Communication May 15, 2008).
• Bratzler, D (Personal Communication May 15, 2008)






![Business Case for ASP.pptx [Read-Only] - Home - SHEA€¦ · MAKING THE BUSINESS CASE FOR ASP: TAKING IT TO THE C-SUITE Gary R Kravitz MD FACP FIDSA FSHEA St. Paul Infectious Disease](https://static.fdocuments.in/doc/165x107/5ac64ebb7f8b9a220b8dd366/business-case-for-asppptx-read-only-home-making-the-business-case-for-asp.jpg)









![Business Case for ASP.pptx [Read-Only] · MAKING THE BUSINESS CASE FOR ASP: TAKING IT TO THE C-SUITE Gary R Kravitz MD FACP FIDSA FSHEA St. Paul Infectious Disease …](https://static.fdocuments.in/doc/165x107/5ac65e007f8b9aa0518e85cc/business-case-for-asppptx-read-only-the-business-case-for-asp-taking-it-to-the.jpg)