COMMUNICATING CYSTS AND DIVERTICULA OF THE RENAL PELVIS
8
COMMUNICATING CYSTS AND DIVERTICULA OF THE RENAL PELVIS By GRANT WILLIAMS, M.Sc., F.R.C.S., J. P. BLANDY, D.M., M.Ch., F.R.C.S., and G. C. TRESIDDER, F.R.C.S. From the Department of UroIogy, The London Hospital, London, E.l CYSTS communicating with the renal calyces were first described by Rayer (1841), who called them " cystes urinaires ". Since then the various names given them-calyceal cyst, calyceal diverti- culum, megacalycosis, and hydrocalycosis-all signify variations on the same theme (Fig. 1). FIG. 1 Communicating cysts and diverticula of the renal pelvis showing their variations with their alternative names. It is only necessary to make a clear distinction between these communicating cysts, and the dilatation of all the calyces which is found in hydronephrosis, for this is an entirely different entity. The cause of communicating cysts is not known, nor indeed is there necessarily only one cause. Weyrauch and Fleming (1950) had a case in a newborn baby, suggesting that some of them are congenital. Others have looked to the neck of the cyst, where it communicates with the pelvis, and suggest that the cause lies here: Beneventi (1943) considered there might be an achalasia here, on the grounds that he had a case cured by overdistension of the calyx in the course of a retrograde pyelogram. Anderson (1961) thought the neck might be narrowed as a result of inflammatory fibrosis-and termed the condition " localising obliterating pyelonephritis ". Others have suggested that an aberrant artery running across the neck of a calyx can obstruct it (Starer, 1968). Several authors have suggested that an ordinary solitary cyst of the kidney might burst into the renal pelvis (Amesur and Roy, 1963; Reiss, 1967), but if this were the case the cyst should not be lined by transitional epithelium as is the usual finding in these cases. Many authors have also pointed out the presence of stones in a number of these cases, though it is an open question whether stones are the cause or the effect of the condition (Abeshouse and Abeshouse, 1963). 163 Many different theories have been suggested.
-
Upload
grant-williams -
Category
Documents
-
view
212 -
download
0
Transcript of COMMUNICATING CYSTS AND DIVERTICULA OF THE RENAL PELVIS
COMMUNICATING CYSTS AND DIVERTICULA OF THE RENAL PELVIS
By GRANT WILLIAMS, M.Sc., F.R.C.S., J. P. BLANDY, D.M., M.Ch., F.R.C.S., and G. C. TRESIDDER, F.R.C.S.
From the Department of UroIogy, The London Hospital, London, E.l
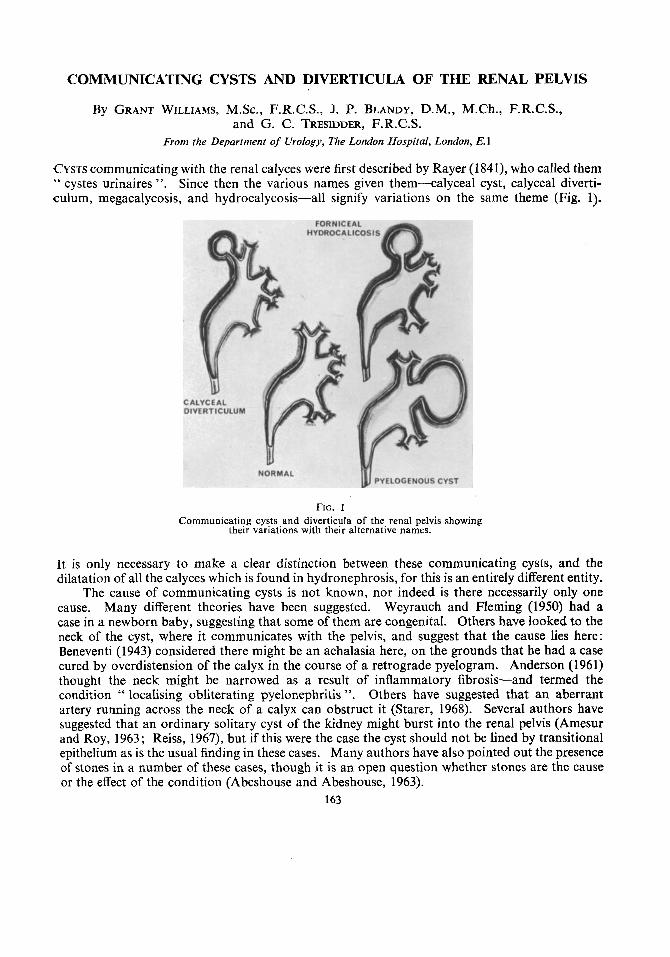
CYSTS communicating with the renal calyces were first described by Rayer (1841), who called them " cystes urinaires ". Since then the various names given them-calyceal cyst, calyceal diverti- culum, megacalycosis, and hydrocalycosis-all signify variations on the same theme (Fig. 1).
FIG. 1 Communicating cysts and diverticula of the renal pelvis showing
their variations with their alternative names.
It is only necessary to make a clear distinction between these communicating cysts, and the dilatation of all the calyces which is found in hydronephrosis, for this is an entirely different entity.
The cause of communicating cysts is not known, nor indeed is there necessarily only one cause. Weyrauch and Fleming (1950) had a case in a newborn baby, suggesting that some of them are congenital. Others have looked to the neck of the cyst, where it communicates with the pelvis, and suggest that the cause lies here: Beneventi (1943) considered there might be an achalasia here, on the grounds that he had a case cured by overdistension of the calyx in the course of a retrograde pyelogram. Anderson (1961) thought the neck might be narrowed as a result of inflammatory fibrosis-and termed the condition " localising obliterating pyelonephritis ". Others have suggested that an aberrant artery running across the neck of a calyx can obstruct it (Starer, 1968). Several authors have suggested that an ordinary solitary cyst of the kidney might burst into the renal pelvis (Amesur and Roy, 1963; Reiss, 1967), but if this were the case the cyst should not be lined by transitional epithelium as is the usual finding in these cases. Many authors have also pointed out the presence of stones in a number of these cases, though it is an open question whether stones are the cause or the effect of the condition (Abeshouse and Abeshouse, 1963).
163
Many different theories have been suggested.

I64 B R I T I S H J O U R N A L OF U R O L O G Y
The condition is not common. In their comprehensive review Abeshouse and Abeshouse f o u n d 329 cases in the literature. These cysts present certain difficulties in diagnosis and treatment which have received little attention hitherto. Experience with one such problem led us to re- examine the material in the Department of Urology in this hospital, an exercise which brought Lo lieht more cases than had been expected, and revealed that surgical treatment was only rarely necessary.
Methods and Materials.-In the period 1960 to 1967 inclusive 16 patients were diagnosed with this condition in the Department of Urology at The London Hospital. During this period
FIG. 2
Fig. 2.-Communicating cyst arising from the right upper calyx (Case 1).
Fig. 3.-Communicating cyst arising from the right middle calyx (Case 4).
FIG. 3
approximately 1 1,000 new patients were referred to this department, so that communicating cysts of the kidney occur in only 0.1 5 per cent. of this already selected group of patients. Plainly, it is a rare condition.
Seven of these patients were male, nine were female: the age distribution was even, between 20 and 72 years. All but one patient had pain in the loin; 12 had recurrent urinary infection; three had hamaturia. Six were hypertensive. Plain radiographs showed stones in the cysts in four cases. The cysts took origin from the upper calyx in seven cases (Fig. 2), the middle calyx in nine (Fig. 3), and not one was related to the lower calyx.
Investigations.-Although an excretion pyelogram may outline the cyst this is not always so, as too little contrast, and that rather diluted, may find its way into the lumen of the cyst (Fig. 4). For this reason some of the cases in the present series were not diagnosed until after a considerable delay. Retrograde pyelography will usually show the cyst, which is then seen to be much larger than it appeared in the excretion pyelogram. The cysts usually empty only slowly, suggesting some hold-up at the neck of the calyx similar to the idiopathic obstruction of the pelvi-ureteric junction found in hydronephrosis (Figs. 4, 5 and 6) .
Treatment.-All but six of the present series were treated conservatively. In the 10 case

COMMUNICATING CYSTS A N D DIVERTICULA O F R E N A L PELVIS 165
FIG. 4 Seven-year-old patient of Mr lnnes Williams showing right calyceal cyst which opacifies and a non-
opacifying portion of the collecting system in the upper pole of the left kidney.
FIG. 5 FIG. 6
Fig. 5.-Left retrograde pyelogram on the patient shown in Figure 4 showing (despite the name label) filling of the non-opacified collecting system noted in Figure 4.
Fig. 6.-Delayed emptying after the retrograde pyelograrn of Figure 5 .

I66 BRITISH J O U R N A L OF UROLOGY
not subjected to operation the urinary infections responded to antibiotics, and indeed in the ma.jority of these patients the appearance in the pyelogram was regarded as an innocent finding.
Operation was performed in six cases, either because the urinary infection could not be controlled or because there were stones, or because the patient had persisting and severe pain. In the past a number of different operations have been suggested. The most simple of all is to
FIG. I Diagram to illustrate division of the neck of the calyx in Case 5.
remove the roof of the cyst, and trust that the communication with the lumen of the renal pelvis will heal without a permanent fistula. Some writers have recommended partial nephrectomy, and others have suggested enucleation of the cyst from the kidney, with careful ligation of its neck. Experience with all these techniques suggested an alternative method.
Simple removal of the roof of the cyst was used in two of the present cases (series numbers 2 and 6). There was no permanent fistula in either case.
In two cases where the cyst arose from the upper pole a formal partial nephrectomy was performed (Cases 1 and 3). These patients healed uneventfully, but in retrospect it seems that an unnecessarily large amount of renal parenchyma may have been sacrificed.
In one case the cyst was dissected from the renal parenchyma down to its neck, and this was carefully ligated and divided. Such a dissection, however, is as unwise as it is in the case of a solitary cyst of the kidney. The kidney bleeds freely and to stop the bleeding much healthy parenchyma is compromised by the sutures used in securing hamostasis. This operation is not recommended.

C O M M U N I C A T I N G CYSTS A N D D I V E R T I C U L A OF R E N A L PELVIS
A B
167
C D FIG. 8
Deroofing of the cyst, which was then filled with perirenal fat.
Although it is possible that in most cases there is negligible risk of a urinary fistula from the neck of the calyx, it is simple to combine the safety of the unroofing operation with intrarenal division of the calyx if the approach used for extended pyelolithotomy is used (Blandy and 'J'residder, 1967) as in the following case (Case 4):
This 37-year-old woman presented with a prolonged history of recurrent episodes of urinary infection, loin pain and hypertension. Excretion pyelography with conventional technique had been performed in another hospital without showing any abnormality, but when repeated with a drip-infusion large dose technique, this showed a well-defined cyst of the renal calyx (Fig. 3).

I68 BRITISH JOURNAL OF UROLOGY
The kidney was approached through the twelfth rib incision. The pedicle was cleared. The renal sinus was then entered through the plane described by Gil-Vernet and' the parenchyma retracted so as to expose the branch of the calyx passing up towards the cyst (Fig. 7, A and B). To make certain that this was the right calyx, it was injected with saline, so as to distend the cyst. The neck of this calyx was then doubly ligated with 4-0 plain catgut and divided (Fig 8, A). The roof of the cyst was then removed, and the lip of compressed renal parenchyma forming the wall of the cyst was oversewn with plain 4-0 catgut to secure hzmostasis (Fig. 8, B). The cavity, which was much larger than the radiographs made it seem, was loosely filled with adjacent perirenal fat and the wound closed in the usual way with drainage (Fig. 8, c and D ) .
The patient made an uneventful recovery. There was no need for any blood transfusion and no post-operative leak of urine. Six months later the patient had a normal pyelogram (Fig. 9), no urinary infection, and no symptoms
FIG. 9 Intravenous pyelogram on Case 5 six months after deroofing the cyst, with intrarenal
ligation of the neck of the calyx.
DISCUSSION
In six patients of the present series who were treated by operation the wall of the cyst was found to be lined with urothelium (Fig. 10). In one of these smooth muscle was seen outside the cyst. If these cysts originated by rupture of an ordinary solitary cyst of the kidney into the renal pelvis, it is just conceivable that the flat epithelium of the cyst might be overgrown by urothelium from the renal pelvis, but it seems unlikely. More probable is the suggestion that the cyst arises by progressive dilatation of a calyx whose neck does not relax, in a way analogous to the obstruc- tion at the pelvi-ureteric junction in idiopathic hydronephrosis. The following case of Mr D. Innes Williams further illustrates this point and we would like to thank him for permission to discuss it:
This boy, aged 7, who is not included in the Table, had a history of enuresis and persistent urinary infection. His excretion pyelogram (Fig. 4) shows an obvious cyst communicating with the right upper calyx. The narrow neck was constant in all the films. Not so obvious is the fact that there is a non-opacifying upper-calyceal cyst on the left, but such a lesion was confirmed by a left retrograde pyelogram (Fig. 5 ) showing delayed emptying of this cystic lesion (Fig. 6) . The neck of this calyx was therefore explored using the technique advocated in this paper. At operation it was impossible even to pass a fine probe up the neck of this calyx and into the cystic areas (Fig.11). An upper pole partial nephrectomy was performed in this case, and the histology of the lesions showed localised pyelonephritis in relation to the neck of the cysts with scarring over the cystic areas, which were lined by transitional epithelium.
This case confirms that these lesions can occur at an early age and suggests that they arise from the pelvi- calycine system.
Differential diagnosis poses only one major difficulty, namely the exclusion of tuberculosis. In all the present cases the urine was examined on at least three occasions for tubercle bacilli by

C O M M U N I C A T I N G CYSTS A N D D I V E R T I C U L A O F R E N A L PELVIS 169
Ziehl-Neelsen staining and by culture of early morning specimens. In fact, the smooth lining of the cavity and the absence of any other features of tuberculosis help in the differential diagnosis.
I t is apparent from the follow-up of the cases with small cysts not operated on in this series
FIG. 10 Urothelial lining of the cyst wall (Case 5).
FIG. 11 Left upper pole partial nephrectomy specimen from Mr Innes Williams’s patient (Figs. 4, 5, 6).
that if control of the urinary infection can be obtained by conventional means there is no need to remove the cyst. In cases with large cysts, in whom infection persists, we suggest the simplest operation consistent with safety is the best, and we recommend either simple removal of the roof of the cyst or, where there is a large calyceal communication, adding to simple unroofing the division of the neck of the calyx within the renal sinus.
I70 BRITISH JOURNAL OF U R O L O G Y
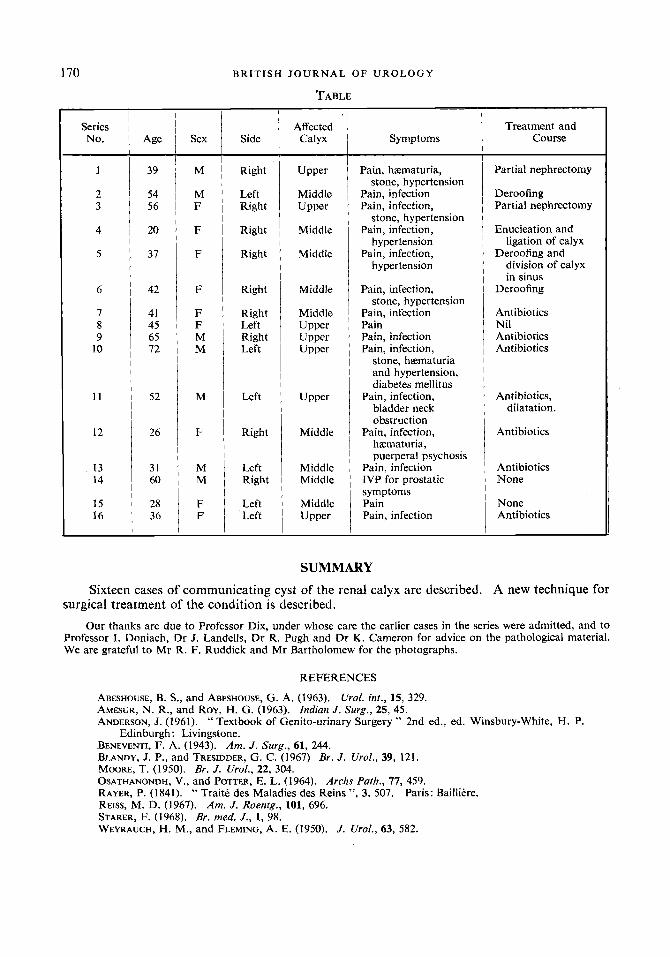
TABLE
Series No.
1
2 3
4
5
6
7 8 9
10
11
12
13 14
15 16
Age
39
54 56
20
37
-
42
41 45 65 12
52
26
31 60
28 36
Sex
M
M F
F
F
F
F F M M
M
F
M M
F F
Side
Right
Left Right
Right
Right
Right
Right Left Right Left
Left
Right
Left Right
Left Left
Affected Calyx
Upper
Upper
Middle
Middle
Middle
Middle
Middle Upper Upper Upper
Upper
Middle
Middle Middle
Middle Upper
Symptoms
Pain, hzematuria,
Pain, infection Pain, infection,
stone, hypertension Pain, infection,
hypertension Pain, infection,
hypertension
Pain, infection,
Pain, infection Pain Pain, infection Pain, infection,
stone, hypertension
stone, hypertension
stone, hzemat uria and hypertension, diabetes mellitus
Pain, infection, bladder neck obstruction
Pain, infection, hzematuria, puerperal psychosis
Pain, infection IVP for prostatic symptoms Pain Pain, infection
Treatment and Course
Partial nephrectomy
Deroofing Partial nephrectomy
Enucleation and
Deroofing and ligation of calyx
division of calyx in sinus
Deroofing
Antibiotics Nil Antibiotics Antibiotics
Antibiotics, dilatation.
Antibiotics
Antibiotics None
None Antibiotics
SUMMARY
Sixteen cases of communicating cyst of the renal calyx are described. A new technique for surgical treatment of the condition 1s described.
Our thanks are due to Professor Dix, under whose care the earlier cases in the series were admitted, and to Professor I. Doniach, Dr J. Landells, Dr R. Pugh and Dr K. Cameron for advice on the pathological material. We are grateful to Mr R. F. Ruddick and Mr Bartholomew for the photographs.
REFERENCES
ABESHOUSE, B. S., and ABESHOUSE, G. A. (1963). AMESUR, N. R., and ROY, H. G. (1963). Indian J . Surg., 25, 45. ANDERSON, J. (1961). ‘‘ Textbook of Genito-urinary Surgery ” 2nd ed., ed. Winsbury-White, H. P.
BENEVENTI, F. A. (1943). Am. J. Surg., 61, 244. BLANDY, J. P., and TRESIDDER, G. C. (1967) Br. J. Urol., 39, 121. MOORE, T. (1950). Br. J . Urol., 22, 304. OSATHANONDH, V., and POTTER, E. L. (1964). Archs Path., 77, 459. RAYER, P. (1841). “ Trait6 des Maladies des Reins ”, 3, 507. REISS, M. D. (1967). Am. J. Roenfg., 101, 696. STARER, F. (1968). Br. med. J., 1, 98. WEYRAUCH, H. M., and FLEMING, A. E. (1950). J. Urol., 63, 582.
Urol. int., 15, 329.
Edinburgh: Livingstone.
Paris: Baillitre.