Common variable immune deficiency syndrome
2
CASE REPORT Common variable immune deficiency syndrome Ahmed A. El-Masry, Ibrahim Dwedar, Hesham A. Abdel-Halim * , Riham Hazem Faculty of Medicine, Ain Shams University, Egypt Received 26 December 2013; accepted 5 January 2014 KEYWORDS Common variable immune deficiency; IgG; IgM; Pneumonia Abstract A male patient 40 years old, non smoker, presented with fever, cough and expectoration of greenish sputum and diarrhea of 1 week duration. The condition started 3 years ago, by cough and expectoration of about cup/day of greenish sputum, not related to posture, along with fever up to 39 °C with loss of weight about 12 kg in one month and associated with diarrhea and mucus shedding. The patient sought medical advice and received empirical antibiotics and symptomatic treatments with partial clinical improvement. The patient showed multiple relapses of same respi- ratory and gastro-enterology symptoms every 3–4 weeks with 4 hospital admissions. CT-chest was done and revealed emphysematous changes with basal inflammatory reaction (Fig. 1); sputum workup showed no acid fast bacilli and growth of normal flora, fasting blood glucose was 102 mg/ dl. A second CT-chest was done after one year and showed right sided pneumonic consolidation, bilateral pneumonic reaction with multiple mediastinal lymphadenopathy, bilateral pleural thicken- ing and right encysted pleural effusion (Fig. 2). ª 2014 Production and hosting by Elsevier B.V. on behalf of The Egyptian Society of Chest Diseases and Tuberculosis. Fibro-optic bronchoscopy was done and showed mucosal ulceration of the right lower lung segments with purulent dis- charge from that segments, BAL C&S showed gram stain mixed g-ve bacilli (proteus and pseudomonas), after 4 months, sputum C&S showed a growth of candida. There was no past or family history of relevant significance (Figs. 1 and 2). Physical examination There was a fever of 38–39.5 °C during the first 9 days of hos- pital course, chest clinical examination showed inspiratory coarse crackles all over chest. Laboratory data ABG on room air was (PH = 7.47, PaCO 2 = 28 mmHg, PO 2 = 73 mmHg, HCO 3 22 mEq/l, ABE 3.2, SO 2 = 96%), ECG showed sinus tachycardia, CBC revealed (WBC 22.200 (Neutrophils 82.2%), Hb 9.1 (normocytic normochromic), platelets (446.000), hypokalemia (K 2.0) which was corrected by IV potassium, fasting blood glucose, liver, kidney and coag- ulation profiles were normal. Sputum workup revealed no acid fast bacilli nor any pathogenic organisms, stool analysis showed entameba histolytica cysts, stool C&S revealed normal * Corresponding author. Tel.: +20 1224474750. E-mail address: [email protected] (H.A. Abdel-Halim). Peer review under responsibility of The Egyptian Society of Chest Diseases and Tuberculosis. Production and hosting by Elsevier Egyptian Journal of Chest Diseases and Tuberculosis (2014) xxx, xxx–xxx The Egyptian Society of Chest Diseases and Tuberculosis Egyptian Journal of Chest Diseases and Tuberculosis www.elsevier.com/locate/ejcdt www.sciencedirect.com Please cite this article in press as: A.A. El-Masry et al., Common variable immune deficiency syndrome, Egypt. J. Chest Dis. Tuberc. (2014), http://dx.doi.org/10.1016/j.ejcdt.2014.01.002 0422-7638 ª 2014 Production and hosting by Elsevier B.V. on behalf of The Egyptian Society of Chest Diseases and Tuberculosis. http://dx.doi.org/10.1016/j.ejcdt.2014.01.002
Transcript of Common variable immune deficiency syndrome

Egyptian Journal of Chest Diseases and Tuberculosis (2014) xxx, xxx–xxx
The Egyptian Society of Chest Diseases and Tuberculosis
Egyptian Journal of Chest Diseases and Tuberculosis
www.elsevier.com/locate/ejcdtwww.sciencedirect.com
CASE REPORT
Common variable immune deficiency syndrome
Ahmed A. El-Masry, Ibrahim Dwedar, Hesham A. Abdel-Halim *, Riham Hazem
Faculty of Medicine, Ain Shams University, Egypt
Received 26 December 2013; accepted 5 January 2014
*
E-
Pe
D
PT
04
ht
KEYWORDS
Common variable immune
deficiency;
IgG;
IgM;
Pneumonia
Corresponding author. Tel.:mail address: Heshamatef71@
er review under responsibil
iseases and Tuberculosis.
Production an
lease cite this article in pruberc. (2014), http://dx.d
22-7638 ª 2014 Production
tp://dx.doi.org/10.1016/j.ejcd
+20 122yahoo.c
ity of Th
d hostin
ess as: Aoi.org/1
and hosti
t.2014.01
Abstract A male patient 40 years old, non smoker, presented with fever, cough and expectoration
of greenish sputum and diarrhea of 1 week duration. The condition started 3 years ago, by cough
and expectoration of about cup/day of greenish sputum, not related to posture, along with fever up
to 39 �C with loss of weight about 12 kg in one month and associated with diarrhea and mucus
shedding. The patient sought medical advice and received empirical antibiotics and symptomatic
treatments with partial clinical improvement. The patient showed multiple relapses of same respi-
ratory and gastro-enterology symptoms every 3–4 weeks with 4 hospital admissions. CT-chest
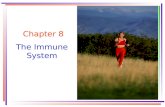
was done and revealed emphysematous changes with basal inflammatory reaction (Fig. 1); sputum
workup showed no acid fast bacilli and growth of normal flora, fasting blood glucose was 102 mg/
dl. A second CT-chest was done after one year and showed right sided pneumonic consolidation,
bilateral pneumonic reaction with multiple mediastinal lymphadenopathy, bilateral pleural thicken-
ing and right encysted pleural effusion (Fig. 2).ª 2014 Production and hosting by Elsevier B.V. on behalf of The Egyptian Society of Chest Diseases and
Tuberculosis.
Fibro-optic bronchoscopy was done and showed mucosalulceration of the right lower lung segments with purulent dis-charge from that segments, BAL C&S showed gram stain
mixed g-ve bacilli (proteus and pseudomonas), after 4 months,sputum C&S showed a growth of candida. There was no pastor family history of relevant significance (Figs. 1 and 2).
4474750.om (H.A. Abdel-Halim).
e Egyptian Society of Chest
g by Elsevier
.A. El-Masry et al., Common0.1016/j.ejcdt.2014.01.002
ng by Elsevier B.V. on behalf of T
.002
Physical examination
There was a fever of 38–39.5 �C during the first 9 days of hos-
pital course, chest clinical examination showed inspiratorycoarse crackles all over chest.
Laboratory data
ABG on room air was (PH = 7.47, PaCO2 = 28 mmHg,PO2 = 73 mmHg, HCO3 22 mEq/l, ABE �3.2, SO2 = 96%),
ECG showed sinus tachycardia, CBC revealed (WBC 22.200(Neutrophils 82.2%), Hb 9.1 (normocytic normochromic),platelets (446.000), hypokalemia (K 2.0) which was correctedby IV potassium, fasting blood glucose, liver, kidney and coag-
ulation profiles were normal. Sputum workup revealed no acidfast bacilli nor any pathogenic organisms, stool analysisshowed entameba histolytica cysts, stool C&S revealed normal
variable immune deficiency syndrome, Egypt. J. Chest Dis.
he Egyptian Society of Chest Diseases and Tuberculosis.

Figure 1 CT-chest showing emphysematous changes with basal
inflammatory reaction.
Figure 2 CT-chest showing Right sided pneumonic consolida-
tion, bilateral pneumonic reaction with multiple mediastinal
lymphadenopathy, bilateral pleural thickening and right encysted
pleural effusion.
2 A.A. El-Masry et al.
flora. Colonoscopy was done up to cecum, examination re-
vealed normal mucosa and vascular pattern with no evidenceof ulcers, polyps or masses. ESR-1st hr 30, CRP 24, HIV-Ab, HBsAg, and HCV-Ab were negative. IGg < 50 mg/dl
(N. 658-1837) and IGA was 36 mg/dl (N. 71-360). Chest radio-graph revealed bilateral basal hetrogenous opacity (pneumo-nia), CT-chest showed Bilateral basal lung consolidative
patches involving the lingual and right middle lobe and Bilat-eral minimal pleural effusion and thickening, pelvi-abdominalU.S. showed calcular gall bladder and mild splenomegaly,Echocardiogram revealed normal LV internal dimensions
and normal systolic function, with estimated EF = 62%.
Please cite this article in press as: A.A. El-Masry et al., CommonTuberc. (2014), http://dx.doi.org/10.1016/j.ejcdt.2014.01.002
Immunology consultation suggested the diagnosis of ‘‘com-mon variable immune deficiency’’ and adviced prophylactictherapy in the form of long acting penicillin/2 weeks, SeptrinDS tab twice daily for 15 days, oral Ketrax 3tab every other
day for 15 days and follow up in outpatient clinic.Other tests recommended including C3, C4, Circulating im-
mune complex, and Immunefixation, IgM, IgE titers.
Conflict of interest
None declared.
variable immune deficiency syndrome, Egypt. J. Chest Dis.