COMAJTERIZED BLOOD GAS INTERPRETATION AND REPORTING SYSTEM
7
COMAJTERIZED BLOOD GA S INTERPRETATION AND REPOR TING SYSTEM Reed M. Gardner, George H. Cannon , Alan H. Morris, Kenneth R. Olsen, W. Gary Price Departments of Biophysics & Bioengineering University of Utah and Latter-day Saints Hospital Salt Lake City, Utah Introdu ction With the increased sophisti cation of laboratOty in stru- mentation, physician and nursing staffs are being presented with large amo unt s of clinical d ata which they are expected to interpret in order to formulate proper therapy for their patients. One of the recent advances has been the development of arterial blood gas analysis. This test n ow provides reliable, accurate data on the blood gas stat us of patient s, thereby presenting information to clinical staffs which was not available before. Accompanying th ese improvements in technique has been a steady increase in knowledge and studies performed on various bl oo d gas disorders. 1 -B January 1975 Becau se new info rm at i on can be rap idly inc orporated in to a co mput e ri zed system, computers have been used to assist and e ducate staff phy s ici ans, hou se staff, and nurses by providing interpretation s of blood gas res ult s. Bleich in his work at Beth Israel Hos pit al in Boston, 9 · 1 0 Goldberg and his associates at th e University of Pennsy lvania , 1 1 and Cohan in Arizona 1 2 have been pioneers in this area. The se inves tigator s require the physician to enter raw data via punch cards , teletype s, or slow-speed video terminals. Experience indicates that ph ysicians will interact with this type of system for on ly a sh ort time. They find they can analyze the data more rapidly thr ough their own thought pro cesses with the aid of nomograms such as the one recently published by the American Thoracic Society. 13 39
Transcript of COMAJTERIZED BLOOD GAS INTERPRETATION AND REPORTING SYSTEM

COMAJTERIZED BLOOD GAS INTERPRETATION AND REPORTING
SYSTEM Reed M. Gardner, George H. Cannon, Alan H. Morris, Kenneth R. Olsen, W. Gary Price
Departments of Biophysics & Bioengineering University of Utah
and Latter-day Saints Hospital
Salt Lake City, Utah
Introduction
With the increased sophist ication of laboratOty in strumentation, physician and nursing staffs are being presented with large amounts of clinical data which they are expected to interpret in order to formulate proper therapy for th eir patients. One of the recent advances has been the development of arterial blood gas ana lysis. This te st now provides reliable, accurate data on the blood gas statu s of patients, thereby presenting information to clinical staffs which was not available before. Accompanying these improvements in technique has been a steady increase in knowledge and studie s performed on various blood gas disorders. 1 - B
January 1975
Because new info rm at ion can be rap idly incorporated in to a compute rized system , computers have been used to assist and educate staff phy sicians, hou se staff, and nurses by providing interpretation s of blood gas results. Bleich in his work at Beth Israel Hospital in Boston, 9 · 1 0 Goldberg and his associates at the University of Pennsy lvania , 1 1 and Cohan in Arizona 1 2 have been pioneers in this area. These investigators require the physician to enter raw data via punch cards, teletypes, or slow-speed video terminals. Experience indicates that physicians will interact with this type of system for only a short time. They find they can analyze the data more rapidly through their own thought processes with the aid of nom ograms such as the one recently publi shed by the American Thoracic Society. 1 3
39

To address this problem, the Latter-day Saints Hospital in Salt Lake City has undertaken the development of a system for automating the ordering, reporting, and interpretation of blood gas results. Acquisition and correction of blood gas and oxygen saturation were already semiautomated, 14 and a large computer system that recorded data on all patients admitted to the hospital was in use; hence a good deal of the groundwork for such a system had already been completed.
The Computerized Blood Gas Interpretation and Reporting System, described in the fo llowing paragraphs, permits reports and interpretations to be generated from the computer data base at Latter-day Saints Hospital without direct physician interaction. Reports are generated in a serial format which makes them ideal for long-term patient follow-up.
pH 25 7.00 100
95
Methods
The Pulmonary Function or Blood Gas Laboratory is the focus of blood gas determinations. ln the Pulmonary Function Laboratory are located two Astrup blood gas machines, an Instrumentation Laboratory , Model 182, CO-oximeter, computer terminals, and a GE Terminet 30-cps printer. A technician begins the blood gas analysis procedure by entering the patient identification number through the computer terminal , whereupon the name of the patient is displayed for verification. The computer then leads the technician through procedural steps acquiring analog data from the blood gas machines at critical points during the process. As each piece of information is acquired, the data is corrected for pH and patient temperature , 1 6 where appropriate , and stored in the patient's flle .1 5
Pco2 mmHg 50 75
105 90 (HC03) mEqjL 705
85 / /
710 80 710
75 75 7.15 70 7.15
SEVERE 7.20 65
60 7.25
55
730 H•] 50
735 nrnfL
45 740 40 745 35 750
30 760 25 7.70 20 7.80 15 7.90 000 10
850 5
5 10 15 20 25 30
50
..---------/
40 45 50 5 5 60 65 70 75 80 85 ~ 95100 Pco2 mmHg
25
7.20
7.25
730
7.35
740
745
7.50
7.00
7.70
780
-r.:YJ aoo
850
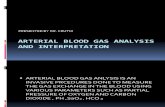
Figure 1. Blood ac id -base map used fo r clin ical interpretation of blood gas data.
40 COMPUTER

System Design The system operates on a Control Data 3300 computer through the MEDLAB system. 1 7 In addition to the terminal in the Pulmonary Laboratory , there are eight nursing divisions. three open-heart surgical operating suites, and four intensive care units with 23 beds of computer monitoring which order and receive hardcopy blood gas results from the computer.
The nursing division communicates with the computer through telephones adapted for use with a voice-response system . 1 8
'1 9 Recently the voice response system has been
implemented on a Votrax supplied by the Federal Screw Works of Troy, Michigan. Ordering is performed by a nurse or ward clerk dialing the computer extension, and then , as directed by the voice-response system , entering the patient number, room and bed number, and desired test time. When the order is complete , a status light is turned on and a request is printed in the Pulmonary Laboratory. Orders from surgical suites and computerized intensive care units are made through CRT terminals and have been designed so the staff can quickly and easily place orders.
The ordering system is convenient for the ICU staffs and laboratory staff because no phone answering is required and verbal errors are eliminated. Orders can also be placed when no technician is in the laboratory.
Interpretations Several techniques for interpreting blood acid-base and oxygen status were evaluated. The technique selected for evaluating clinical acid-base status is a combination of confidence bands for various respiratory and metabolic acid-base disorders from several authors. 1 -
8
Goldberg' s general approach was followed 1 1 with altitude corrections for Salt Lake City. The modified map is shown in Figure I. There are six major classification areas: 1) metabolic acidosis, 2) acute respiratory acidosis, 3) chronic respirat01y acidosis, 4) metabolic alkalosis, 5) acute respiratory alkalosis, and 6) chronic respiratory alkalosis. Regions between the "pure" acid-base disorders are interpreted as mixed disorders. The map is also divided into normal, mild, moderate , and severe regions. In the mild region no interpretation is specified, since nurses and physicians will usually not take any therapeutic action as a result of slight abnormalities.
Figure 2 shows the oxygen hemoglobin dissociation curve with the criteria for classification of oxygen status. The five classifications are 1) severe hypoxemia, 2) moderate hypoxemia , 3) mild hypoxemia, 4) normal, and 5) supranormal P02 . Alveolar-arterial oxygen gradients are computed from the blood gas data and inspired oxygen concentration, if available . Inspired oxygen concentration is estimated from oxygen flow rate.
Once the blood gas data is entered into the computer the results are automatically evaluated using the acid-base map of Figure I. This is automatically performed by the HELP (Health Evaluation through Logical Processing) program (Figure 3) described in the preceding paper by Pryor et al.
HELP allows logical determinations to be made from the blood gas data as well as from data entered from other sources contained in the patient' s data file. Decisionmaking criteria are stored on a separate disk in a logical format which allows easy implementation of medical decisions. HELP permits medical decision criteria to be stated in a high-level computer language, thereby simplifying the entry of the medical decision logic . Once the blood gas test is run it is automatically evaluated by the criteria logic and an
January 1975
interpretation is made. The interpretation is stored on a problem-oriented record file , and a hardcopy report is generated.
Figure 4 shows a typical serial blood gas report. All of the data is available through the computer terminals and the voice response system. This is especially convenient during the evening hours when no one is in the Pulmonary
. Laboratory to read the reports over the telephone. Reports are printed for the Pulmonary Laboratory and ICU's on video terminals and on a hardcopy printer for distribution to the patient charts. No physician involvement is required. A pulmonary technician and the computer perform quality control.
Evaluation
Physician Experts Four pulmonary specialists and three nephrologists- all current or past members of the University of Utah faculty - were asked to participate in an evaluation of the system. Each specialist was given a list of 137 separate test results which contained pH, PC02 , HC03 , and base excess measurements. Table 1 shows the results from which the 137 test cases were randomly selected. After a consultation with the physicians, the 12 categories used by the computer were chosen as the best means of classifying the disorders.
Because not all physicians completed all 137 classifications, and some physician responses were ambiguous or obviously incorrect, there were only 49 sets of values for which the responses of all seven experts could be compared with the computer.
Analysis was difficult because none of the interpretations could be taken as absolutely correct. In comparing the responses, no interpretation was taken as a standard.
H EALTil E Vlil.I.Jt\TJO'J TIJIUG1 L (XiJCftJ.. P f«ESSES
CRITERIA ()__.
FILE (SECTORS) ~ ~-.....---'
r i..At-ruAGE TO
GENERATE lflP loo1c
PATIEI'IT DATA FILE
Figure 2. Block diagram of HELP decision-making system.
41

100
90
80 Ph= 7.40
Temp-37° C
70 c :a 0 0> 0
60 E Q)
r -0
c 50 0
~ :::> c 40 (/)
~ 0
30
~ <! ::E
20 w w a: X w 0 > a_ w >-(/) r
10-
w <! ' 1- ~ I <! w , a: X w 0 0 a_ 0 >-~ r
. . . . . . . ... . . . . . . . . . . . ~~~~ :::::::::::::::::::::::::::::::::::::::::: lf- • • • • • • • • • • • • • • • • ••••• ~ ·.·.·.·.·.·.·.·.·.·.·.·.·.·.·.·.·.·.·.·.·. . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . .... . ~ ·.·.••·••.••·.·.·.·.·••.·.•••.·.·.·.·••.·. l1 • • • • • • • • • • • • • • • • • • ••• 71 • • • • • • • • • • • • • • • • • • • • •
ll ~ ·.•.•.·.·.·••.·.·.·.•••.·.·.·.·.·.·.•.·.·. . . . . . . . . . . . . . . . . . . . . . h • • • • • • • • • • • • • • • • • • • • • ~ . . . . . . . . . . . . . . . . . . . . . ~ ......................................... . ~ ......................................... . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .... . . . . . . . . . . . . . . . . . . . . .
L.._ ').... • • • • • • • • • • • • • • • • • • •••
~ r • • • • • • • • • • • • • • • • • • • • •
~ . . . . . . . . . . . . . . . ..... . . . . . . . . . . . . . . . . . . . . . .
~ '-I • • • • • • • • • • • • • • • • • • • • •
~ r>- • • • • • • • • • • • • • • • • • • • • • . . . . . . . . . . . . . . . . . .... . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . .
~ \,\ . . . . . . . . . . . . . . . . ..... . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .... . . . . . . . . . . . . . . . . . . ... . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .... . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . .... . . . . . . . . . . . . . . . . . . ... . . . . . . . . . . . . . . . . . .... . 2 . • . • • • • • • • • • • • • • • • • • • ~ -:·:·:·:·:·:·:·:·:·:·:·:·:·:·:·:·:·:·:·:·:
~ ~ : ::: : : :: :: -oN :: :: : : ::: :: : :: ::: : :: :: :: ::: :: <l :-:·:·:·:·a.·:·:·:·:·:·:·:·:·:·:·:·:·:·:· ~ •••••••••• _J •••••••••••••••••••••••••••••
w.·.·.·.·.·<:[·.·.·.·.·.·.·.·.·.·.·.·.·.·.· X • • • • • :E • • • • • • • • • • • • • • •
':3~·-·.·.·.·.et: . ·.·.·.·.·.·.·.·.·.·.·.·.·.·. >- •••••••••• ~ .••••••••••••••••••••••••••••
I~ r ::::::::::-:-::::::::::::::::::::::::::::: . . . . . . . . . . . . . . . . ..... . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .... . . . . . . . . . . . . . . . . . .... . . . . . . . . . . . . . . , . . . ' .. .
....J <! ~ a: 0 z <! a: C\J a_ 0 ~ a_
0 10 20 30 40 50 60 70 80 90 100 110 120 130
P02 (mmhg)
Figure 3. Oxygen hemoglobin dissociation curve with interpretive areas outlined.
Instead, responses were tested for agreement among themselves by noting the number and percentage of cases in which each participant agreed with the m ajority of the others. Table 2 shows these results. The compu te r ranks second among the experts, is nearly as good as the bes t expert , and is far better than the worst expert.
Most of the specialists commen ted on the difficulty of classifying acid-base disorders without clinical bedside information. Correc tive therapy of disorders can influence test resul ts. If bl ood is drawn befo re a patient has stabilized, the values can lead to an incorrec t interpretation. Also, two se ts of slightly differing values lying near the bo rder of an area on the map may give two different interpretations. These criticisms point to the need for incorporating further clin ical info rmat ion into the interpretation, which will be done as the program becomes more sophisticated. However, in its p resent state of development the program does as well as a special ist in interpreting blood gas di sorders based on laboratory results alone.
L D S H OSP ITAL B L ll 0 D G A S " E P 0 ~ T
JOHN 0 HOSPITAL NO. 3~00002 lXlCll> ~ NOT KNOn N NOV 7~ PH t> O l 2 HCOJ BE HB CO HB P02 SA.0 2 02CT
NO RMAL HIGH 7. 4 5 4 0 . 0 2':) . 0 2 • ., l 7 . o 2 .o 85 9? 23.0 RANGE L Oi'i 1 . 3~ 3 4 . 0 19.0 - 2., I 3 . U 0 .4 68 92 10 . 6
6 150 7. 39 3~ . 5 20 . 8 -I. B I 3 . 2 3 . 2 88 90 17.0
NOW MAL ARTEW I A.L A.CI D- BASE CHEM I STflY ARTER l AL P02 MAY BE LOW F(}H 02 rlD~ ~ATE
2 19 130 A 7 . 33 5 4 . 4 27 . 5 2 . 0 1 3 . 4 3.3 82 9 4 I "/ , 5
MODER ATE ACID - BASE DJSOKOER CHRON JC RES PI RA. TORY ACI DOS I S AflTEfl iAL P02 MA Y BE LOW rOR 02 FLOW RAT E
3 5 155 7. 35 45. 7 24. 6 . 5 l 3 . 7 3 . 5 9 1 96 J 8.2
MILD ACID - BASE DISORDER ARTEK I AL P02 MAY BE LOW FOR 02 fLOrl RATE
8 130 7.23 63 . 8 25 . 8 - 2 . 6 1 3. 7 3 . 0 6 4 87 16.5
SE \I dlE ACID- BASE O! SOROEH ACUTE RES}-J lt-tATOR Y ACI DOSIS MODER ATE HY}-JOXEM I A
4 9 120 7 .3~ 42. 7 22 . -j - 1. 9 I 4 . 0 3 . 0 Ol 90 I 7 . 5
MIL O ACID - BASt Dl SO HOEk MIL l) HY?OXEMIA
• I IO 5 7. 4 I 31 . 7 22 . 3 1. 1 I 4. I 2 . 9 92 97 19 . 0
MI L D ACID -~ASE DISORDER ARTEk'lAL P02 MAY BE LOr'!' t=OH 02 rLO ~ RATE
1-' h'E LI MINAh'Y INTERPRETATION -- BAS ED ONL Y ON BLOOD GAS DATA.. ***<F INAL DIAGNO:;, I S RE QU I RES CLJNI CAL O>h'RELATION l ***
I<EY - A=AHT Eh' IA L . V::MJ XEO VENOUS. C=C APILLARY , 02CT=02 CO /'ITEN T
140
·"" HERE %02
':l LIM IN
5 L/MIN
6 LI M IN
6 LIM IN
40 PO I PP
o LIM IN
The study poin ts out the need for standardization of interpretations. Eve n the best expert di sagreed with the majority 25% of the time. Standardization and verification of in terpretations are cm cial to any compu terized technique for medical decisionmaking. Before computers can be made to provide bette r inte rpretive results, these problems must be reso lved by either local or national standardization.
COHB:::zCARBOXYHEMOGUlBIN % <CC 02/ IOOCC BLOOD I
8 NOV / 4 8 136 ·**~ERMANENT RE?ORT - RET AIN ON CHART
Figure 4 . Serial blood gas report with computerized interpretations.
42 COMPUTER

Table 1. Distribution of Acid-Base Disorders and Oxygen Classifications
Total Blood Gas Determinations Normal Acid -base Chemistry Mild Acid-base Disorder Moderate Acid-base Disorder Severe Acid -base Disorder
DISTRIBUTION OF MODERATE AND SEVERE DISORDERS Metabolic Acidosis Mixed Metabolic and Respiratory Acidosis Acute Respiratory Acidosis Mixed Acute and Chronic Respiratory Acidosis Chronic Respiratory Acidosis Mixed Respiratory Acidosis and Metabolic Alkalosis Metabolic Alkalosis Mixed Metabolic and Respiratory Alkalosis Acute Re sp iratory Alkalosis Mixed Acute and Chronic Respiratory Alkalosis Chronic Respiratory Alkalosis Mi xed Respiratory Alkalosi s and Metabolic Acidosis
DISTRIBUTION OF OXYGEN CLASS/FICA TIONS Normal Oxygen Saturation and P02 Mild Hypoxemia Moderate Hypoxe mia Severe Hypoxem ia Supranormal P02 Arterial P02 Abnormally Low for Inspi red 0 2 Arterial P02 May Be Abnormally Low for Inspired 0 2
2130 486
1011 546
87
36 76 52
8 146 78 35 36
155 14 51
8
648 357 415
87 210 662 375
Percentage of Total
22.8 47.5 25.6
4.1
1. 7 3.6 2.4
.4 6.9 3.7 1.6 1.7 7.3
.6 2.4 0.4
30.4 16.8 19.5 4.1 9.9
31.1 17.6
Table 2 . Comparison of Interpretations of Seven Specialists with the Computer
Computer 2
% Agreement with Majority 74 .0 74.0 52.5
Rank 2 2
Staff Review and Results In order to assess the helpfulness of the computer to the physician and sample his opm10n as to the accuracy of the computerized interpretations, a survey was conducted over a 17-day period. During this time each interpretation was followed by a short evaluation note, and the physician 's attention was drawn to the note by a red stamp indicating that an evaluation was desired. Attending staff members were notified of the survey by a note in the staff newsletter, and individual letters were sent to each of the house staff members.
Results of the survey were collected by visiting the wards and looking at the charts on the day following the blood gas tests. Survey results are shown in Table 3. Due to pressing demands on physician staff members, only 68 of the 360 reports (19%) sent out were evaluated. Of those evaluated, 19 (28%) were helpful and changed patient care. We found that 80% of the responses were helpful and 20%
January 1975
8
Expert Average 3 4 5 6 7
61.0 65.5 65.0 62.5 74.5 61.1
7 4 5 6
were not helpful. In only one case did the clinician feel that the computer interpretation was incorrect.
Future Plans and Conclusions
With serial interpretations and reports already avai lable, as shown in Figure 4 , the next logical step is to have the computer make interpretations based on the time course of the laboratory results. The HELP system has recently been modified to permit time sequential interpretation. Automated entry of data from the clinical laboratory will allow check of anion gap , electrolyte levels, and other information which will broaden the data base from which interpretations will be made.
Other clinical information, such as drug information , IV solutions, and other therapeutic interventions, are entered for patients in the intensive care units. Higher-level
43

Table 3. Survey Results
Total Reports Checked for Physician Response
1. 2.
Reports Without Response Reports With Response
Breakdown of Responses
1. Helpful : Changed Patient Care 2. Helpful: Educational 3. Helpful : Interesting 3a. Not Helpful: Interesting 4. Not Helpful: No Contribution 5. Not Helpful: Incorrect Interpretation
decisions will be made from this data and suggestions will be made for clinical therapy-e.g. , changes in respirator parameters and drug administration.
Experience with the computerized interpretation system has shown that 1) computerized interpretation is accurate, and reporting of serial blood gases is accepted and appreciated by physicians and nurses; 2) interpretations aid in providing better care to a growing number of patients ; 3) quality control in the laboratories is enhanced by computer checks for internal consistency of results; 4) computerization was the catalyst for standardization of classification criteria; 5) terminology has been standardized because of computerization; 6) computerized interpretation provides an educational benefit to the staff and nurses ; and 7) turnaround time between sample withdrawal and result reporting was decreased. The time was decreased most dramatically in the critical care units where the test is most common and most urgently needed.
The computerized blood gas laboratory presently performs more than 1800 blood gas determinations each month. The computer has aided in providing 24-hour-perday , 7-day-per-week service to intensive care and general hospital divisions. The computer has speeded response and made more legible an d usable the data from the routine clinical determinations. A computer charge of $. 75 per blood gas sample is made and is a nominal fee for the advantage of computerized interpretation and computation.
The future use of microprocessors in the acquisition and calibration of blood gas instruments will I) increase the re liability of results; 2) make the tests much less operator-dependent; 3) decrease the time required to obtain results; 4) make the test more availab le in critical care areas, since nurses can draw samples from existing arterial catheters and " inject" them into the automated machine ; and 5) possibly reduce cost of the test , which currently requires highly skilled technicians around the clock.
With the addition of better measurement methods there will be a need to improve interpretation decision criteria; therefore , a primary requirement for new systems which are designed to be used in a medical environment will be the ability to store and retrieve data for medical decisionmaking.
Acknowledgment
Supported in part by a Health Resources Administration Grant (I POl HS 01053-02).
360
292 68
19 16 19
5 8 1
References
Percentage of Slips Checked
81 % 19%
Percentage of Total Responses
28% 24% 28%
7% 12%
1%
l. Masoro, E. J. and P. D. Siegel, Acid-base Regulation: It s Physiology and Pathophysiology, W. B. Saunders Co., 1971.
2. Winters, R. W., K. Engel, and R. B. Dell, Acid-base Physiology in Medicine, The London Co., 2nd Ed. , 1969.
3. Albert , M. S., R. B. Dell, and R. W. Winters, "Quantitative Displacmenet of Acid-Base Equilibrium in Metabolic Acidosis," Annals of Internal Medicine, 66 :312-322, 1967.
4. Kessirer, J. P. and W. B. Schwartz , " The Response of Normal Man to Selective Depletion of Hydrochloric Acid: Factors in the Genesis of Persistent Gastric Alkalosis," American Journal of Medicine, 40:10-18, 1966.
5 . Goldring, et al, "Respiratory Adjustment to Chronic Metabolic Alkalo sis in Man," Journal of Clinical Investigation, 47:188-202 , 1968.
6. Brackett, N. C., Jr. , J. J. Cohan, and W. B. Schwartz, "Carbon Dioxide Titration Curve of Normal Man." New England Journal ofMedicine, 272:6-12 , 1965.
7. Arb us, G. S., et al, " Characterization and Clinical Application of the 'Significant Band' for Acute Respiratory Alkalosis," NewEnglandloumalofMedicine, 280:117-123,1969.
8. Schwartz, W. B. , W. C. Brackett, and J. J. Cohen, "The Response of Extracellular Hydrogen Ion Concentration to Graded Degrees of Chronic Hypercapnia," Journal of Oinical Invest iga tion , 44 :29 1-30 1, 1965 .
9. Bleich, H. L., "The Computer as a Consultant," New England Journal of Medicine, 28:141-147,1971.
10. Bleich, H. L., "Computer Evalu ation of Acid-Base Disorders," Journal of Clinical In vestigation, 48:1689-1696 , 1969.
11. Goldberg, M., S. B. Green, M. C. Moss, C. B. Marbach, and D. Garfinkel , "Computer-Based Instruction and Diagnosis of Acid-Base Disorders," lAMA , 223:269-275, 1973.
12. Cohan, M. L. , " A Computer Program for interpretation of Blood Gas Analysis," Computers and Biomedical Research, 2:549-557 , 1969.
13. Graphic Aids in Blood Gas Analysis, American Thoracic Society, Oct. , 1972. Cards: Oxyhemoglobin Dissociation Curve, The Alveolar Air Equat ion Nomogram , Respiratory Alterations in Acid-base Balance.
14. Clark , J. S. and R. M. Gardner, " On-Line Computerized Acid-Base Analysis," Proc. Annual Conference Engineering in Medicine and Biology, 10:17.1 , 1968.
44 COMPUTER
------------- --- ----- - ---- - -- -'·

15. Warner , H. R. and J. D. Morgan, " High Density Medical Data Management," Computers and Biomedical Research, 3:464-476, 1970.
16. Thomas, L. 1. , "Algorithms for Selected Blood Acid-Base and Blood Gas Calculations," Journal of Applied Physiology, 33:154- 15 8, 1972.
17. Pryor, T. A., R. M. Gardner, and W. C. Day, "Computer Systems for Research and Clinical Application to Medicine," AFIPS Conference Proceedings, 33:809, 1968.
18. Johnson, D. K., "A Computer-Based Audio Response System for Clinical Medicine," PhD Thesis, University of Utah , 1969.
19. Gardner, R. M., G. H. Cannon, A. H. Morris, K. R. Olsen, and W. G. Price, "Computerized Blood Gas Interpretation," Medical Instrumentation, 8(2): 126, 197 4.
20. Cannon, G. H. and R. M. Gardner, "Accuracy and Usefulness of Comp uterized Interpretation of Blood Gas Determinations," Clinical Research, 22(2):175A, 1974.
21. Warner, H. R., C. M. Olmsted , and B. D. Rutherford, "HELP- A Program for Medical Decision-Making," Computers and Biomedical Research, 5:65-74 , 1972.
Reed M. Gardner is the guest ed itor of this issue . His biography appears with his introduction on page 19.
January 1975
George H. Cannon is a third-year medical student at the University of Utah. He is a member of Phi Beta Kappa and recently presented a paper at the student seminar of the Western Meetings of the American Federation for Clinical Research. He received his BA degree in medical biology from the University of Utah in 1973.
Alan H. Morris is an assistant professor in the College of Medicine at the University of Utal1 , and Medical Director of the Pulmonary Laboratory at the Latter-day Saints Hospital. His current research interests fall within the general category of clinical or applied pulmonary phy sio logy. Dr. Morris received his BA degree in chemistry from Princeton University and his MD degree from Yale University .
Kenneth R. Olsen is associated with the University of Utal1 , Depar tment of Biophysics & Bioengineering, as a systems programmer, with special inte rest in operating systems and use of computers in solving mathematical problems, and was responsible for implementing the programming for the Pulmonary Function Laboratory and the blood gas analysis system. Olsen received his BS degree in political science from Utah State University.
W. Gary Price is working towards his PhD degree in the Department of Biophysics and Bioengineering on a voice response system for hospital use. He is presently employed by MEDLAB Computer Services with special interest in computer application to patient care. Price received his BA degree in electrical engineering from the University of Utah.
Computerized Imaging Techniques Seminar Proceedings Meeting hetdJune 26-27,1967 .
Washington, D.C. 165 pages- Price $18.00 Vol.10
Many new types of system s and ap pli ca tions were di sc ussed in a se ri es of seventeen papers presented during th is two -day meeting. Th ese top1cs included computer analysis of ph otog raphic images for earth resources studies, fin gerprin t cla ssi fi cat ion, high ene rgy physics I bubbl e chamber data] and chromosome studies. Also covered was computer enhancement of pictures re cord ed by the Surveyor moon craft and weather sa tellites and the com puter restoration of images degraded by air tu rbulance and other ca uses. The prese nta tion of computer gene rated data in pictorial fo rm was shown to be hi gh ly effective. Finally this material was sum · marized and analyzed by a panel of experts.
Numerical Mapping Applications • 01g1tal Image Process1ng at JPL • Automatu: Readmg ol Recon naissance Film Code Blocks • A Computerized 3-D Ploltmg Program • Socrates - Adaptive Image Processor • Image Feature ExtractiOn for Automatic Terrain ClassificatiOn • Cond1!1 omng of Dlg1!11ed Tires and £ssa Sate ll ite Vidicon Data • Image Process ing by Compute1 Generated B1nary F11ters • Two-Dimensional Image Prediction and Enhan cement • See ing Solid • lnvestigatmns m the ldent1 fi cal ion of f ingerprint Pa tterns by Machne Methods • A Multichannel Image Data Handlmg System for Agncultural Remote Sensing • Pattern Recognition in Bubble Chambers • The Ch rom osome Scanning Program at lawrence Radiation laboratory • Computer Process1ng of Atmosphencally Degraded Images · D1g1tal Image format1on from Electronica lly Detected Holograms • The Com · bined Use of Dig1tal Computers and Coherent Optics 1n Image Processing.
ALL ORDERS MUST BE PREPAID. Price includes shipping and handling.
Within California add 6% sales tax.
~~fE~~eco"Fs t~~":'6e~~~ICAL INSTRUMENTATION ENGINEERS. P.O. Box 1146, Palos Verdes Estates, California 90274 . Telephone: (213) 378·1216.
Reader Service Number 127