Interpretation of arterial blood gases:Traditional versus Modern
139
-
Upload
gamal-agmy -
Category
Health & Medicine
-
view
1.954 -
download
1
Transcript of Interpretation of arterial blood gases:Traditional versus Modern


Interpretation of Arterial Blood Gases
Traditional Vs Modern
By
Gamal Rabie Agmy , MD , FCCP Professor of Chest Diseases ,Assiut University

Handerson Hasselbach
Equation
• PH= pKa+ Log HCO3/PaCo2
• PH= Log HCO3/PaCo2
• PH= HCO3
• PH= HCO3
• PH= PaCo2
• PH= PaCo2

Co2+H2o=H2co3=Hco3- + H+
Hprotein=H+ + Protein-


• PH 7.35-7.45
• HCO3 22-26 mEq/L
• PaCo2 35-45 mmHg
• PaO2 97 mmHg
• BE/BD +2 to -2
• Haemoglobin 15 gram
• A-a O2 gradient N < 15
A-a O2 gradient OLDER PERSONS
– 2.5 +0.25*AGE
– eg. AGE 60, 2.5+15=17.5
– eg. AGE 80, 2.5+20=22.5
Normal Values


Definition of Respiratory Failure
Respiratory failure is a syndrome of
inadequate gas exchange due to
dysfunction of one or more essential
components of the respiratory system

Types of Respiratory Failure
Type 1 (Hypoxemic ): * PO2 < 60 mmHg on room air.
Type 2 (Hypercapnic / Ventilatory): *PCO2 > 50
mmHg
Type 3 (Peri-operative): *This is generally a subset of
type 1 failure but is sometimes considered
separately because it is so common.
Type 4 (Shock): * secondary to cardiovascular
instability.

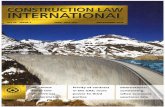
FIO2
Ventilation without
perfusion (deadspace ventilation)
Diffusion abnormality
Perfusion without
ventilation (shunting)
Hypoventilation
Normal

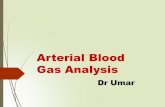
Brainstem
Spinal cord
Nerve root Airway
Nerve
Neuromuscular junction
Respiratory muscle
Lung
Pleura
Chest wall
Sites at which disease may cause ventilatory disturbance

• Type 1:
A-Acute
B-Chronic
C-Acute on top of chronic
• Type 2: A-Acute
B-Chronic
C-Acute on top of chronic
Types of RF:

• Type 1:
PaO2<60 mm Hg
PaCo235-45 mmHg
• Type 2: PaO2<60 mm Hg
PaCo2>50 mmHg
Types of RF:

Type 1: • Acute:
Pao2<60mmHg HCO3 Normal
PaCo235-45mmHg PH > 7.45
• Chronic:
Pao2<60mmHg PaCo235-45mmHg
HCO3 <22mEq/L PH=7.40-7.45
• Acute on top of chronic:
Pao2<60mmHg HCO3 <22mEq/L
PaCo235-45mmHg PH > 7.45
Types of RF:

Type 2: • Acute:
Pao2<60mmHg HCO3 Normal
PaCo2>50 mmHg PH<7.35
• Chronic:
Pao2<60mmHg PaCo2 >50 mmHg
HCO3 >26 mEq/L PH=7.35-7.40
• Acute on top of chronic:
Pao2<60mmHg HCO3 >26 mEq/L
PaCo2 >50 mmHg PH<7.35
Types of RF:


Uncompensated
Partially compensated
Compensated
Uncompensated
Partially compensated
Compensated
M acidosisM acidosis

Uncompensated
*PH < 7.35
*PaCo2 normal
*HCO3 < 22 ml eq/L

Partially compensated
*PH< 7.35
*PaCo2 < 36 mmHg
*HCO3 < 22 ml eq/L

Compensated
PH 7.35-7.40
PaCo2 < 35 mmHg
HCO3 < 22 mleq/L

Uncompensated
Partially compensated
Compensated
Uncompensated
Partially compensated
Compensated
M alkalosisM alkalosis

Uncompensated
PH > 7.45
PaCo2 normal
HCO3 >26 ml Eq/L

Partially compensated
PH >7.45
PaCo2 > 45 mmHg
HCO3 > 26 ml Eq/L

Compensated
PH 7.40-7.45
PaCo2 > 45 mmHg
HCO3 > 26 mlEq/L


Combined acidosis:
PH<7.35 PaCO2>50 HCO3<22
Combined alkalosis:
PH >7.45 PaCo2<35 HCO3>26

Blood Gas Analysis &
Acid-Base Disorders
Professor Gamal Rabie Agmy, MD, FCCP
Professor of Chest Diseases , Assiut
University

Blood Gas Analysis
Arterial blood
Sea level (101.3kPa, 760mmHg)
Quiet
Anti-coagulate blood
Inspire air (Whether O2 supply)

Why Order an ABG?
• Aids in establishing a diagnosis
• Helps guide treatment plan
• Aids in ventilator management
• Improvement in acid/base management allows for optimal function of medications
• Acid/base status may alter electrolyte levels critical to patient status/care

Clinical Significance
To evaluate oxygen status
To evaluate ventilation
To evaluate acid-base disorder

How to evaluate oxygen status?
PaO2:
Partial pressure of oxygen in Arterial
blood .
Normal: 95-98 mmHg (12.6-13 kPa)
Estimate formula of age:
PaO2=100mmHg-(age×0.33) ±5mmHg

Hypoxaemia
Mild: 80-60mmHg
Medorate: 60-40mmHg
Severe: <40mmHg

Respiratory Failure
PaO2<60mmHg respiratory failure
Notice: sea level, quiet, inspire air
rule off other causes (Congenital
cyanotic heart disease and abnormal
types of Hg)

Classification of Respiratory Failure
PaCO2: The carbon dioxide partial
pressure
of arterial blood
Normal: 35-45mmHg (4.7-6.0kPa)
mean: 40mmHg

Classification of Respiratory Failure
Type Ⅰ TypeⅡ
PaO2 (mmHg) <60 <60
PaCO2 (mmHg) ≤35-45 >50

Other Parameters
SaO2: Saturation of arterial blood
oxygen
Normal: 0.95-0.98
Significance: a parameter to evaluate
hypoxaemia, but not sensitive
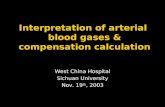
ODC ( Dissociation curve of
oxygenated hemoglobin): “S” shape

SaO2%
PO2
Oxygen dissociation curve

PH 2,3DPG temperature CO2
ODC to right deviation
Oxygenated hemoglobin release oxygen
to tissue, prevent hypoxia of the tissue.
But absorbed oxygen of hemoglobin is
decreased from the alveoli.
Bohr effect: movement of ODC place is
induced by PH.

PA-aO2: Difference of alveoli-arterial
blood oxygenic partial pressure.
Normal: 15-20mmHg (<30mmHg in the
old)
Significance: a sensitive parameter in
gas exchange

PvO2: Partial pressure of oxygen in
mixed venous blood.
Normal: 35-45mmHg
mean: 40mmHg
Significance: Pa-vO2 is to reflect the
tissue absorbing oxygen.

CaO2: The content of the oxygen of the
arterial blood.
Normal: 19-21mmol/L
Significance: a comprehensive
parameter to evaluate arterial
oxygen.

Parameters in acid-basic disorder evaluation
PH: negative logarithm of
Hydrogen ion concentration.
Normal: 7.35-7.45
mean: 7.4
PH=Pka+log 〔HCO3
- 〕
0.03PaCO2
=6.1+log 20
1

HCO3- (bicarbonate):
SB (standard bicarbonate)
AB (actual bicarbonate)
SB: the contents of HCO3- of serum of arterial
blood in 37℃, PaCO2 40mmHg, SaO2 100%.
Normal: 22-26 mmol/L
mean: 24mmol/L
AB: The contents of HCO3- in actual condition.
In normal person: AB=SB

AB and SB are parameters to reflect
metabolism, regulated by kidney.
Difference of AB-SB can reflect the
respiratory affection on serum HCO3- .
Respiratory acidosis: AB>SB
Respiratory alkalosis: AB<SB
Metabolic acidosis: AB=SB<Normal
Metabolic alkalosis: AB=SB>Normal

Buffer bases(BB):
is the total of buffer negative ion of blood.
BB: HCO3-
hemoglobin
plasma proteins
HPO42- (phosphate)
Normal: 45-55mmol/L
mean: 50mmol/L
Significance: Metabolic acidosis: BB
Metabolic alkalosis: BB

Bases excess (BE):
the acid or bases used to regulate blood PH 7.4 . ( in 38℃,PaCO2 40mmHg, SaO2 100%)
Normal: 0±2.3 mmol/L
Significance:
add acid: BE(+), BB
add base: BE(-), BB

Total plasma CO2 (T-CO2):
total content of the CO2 .
Normal: HCO3- >95%

Logistics
• When to order an arterial line -- – Need for continuous BP monitoring
– Need for multiple ABGs
– COP measurement by thermodilution method
• Where to place -- the options – Radial
– Femoral
– Brachial
– Dorsalis Pedis
– Axillary

Acid Base Balance
• The body produces acids daily
– 15,000 mmol CO2
– 50-100 mEq Nonvolatile acids
• The lungs and kidneys attempt to maintain balance

Acid Base Balance
• Assessment of status via bicarbonate-carbon dioxide buffer system
– CO2 + H2O <--> H2CO3 <--> HCO3- + H+
– ph = 6.10 + log ([HCO3] / [0.03 x PCO2])

The Terms
• ACIDS
– Acidemia
– Acidosis
• Respiratory
CO2
• Metabolic
HCO3
• BASES
– Alkalemia
– Alkalosis
• Respiratory
CO2
• Metabolic
HCO3

Respiratory Acidosis
• ph, CO2, Ventilation
• Causes
– CNS depression
– Pleural disease
– COPD/ARDS
– Musculoskeletal disorders
– Compensation for metabolic alkalosis

Respiratory Acidosis
• Acute vs Chronic
– Acute - little kidney involvement. Buffering via titration via Hb for example • pH by 0.08 for 10mmHg in CO2
– Chronic - Renal compensation via synthesis and retention of HCO3 (Cl to balance charges hypochloremia) • pH by 0.03 for 10mmHg in CO2

Respiratory Alkalosis
• pH, CO2, Ventilation
• CO2 HCO3 (Cl to balance charges hyperchloremia)
• Causes – Intracerebral hemorrhage
– Salicylate and Progesterone drug usage
– Anxiety lung compliance
– Cirrhosis of the liver
– Sepsis

Respiratory Alkalosis
• Acute vs. Chronic
– Acute - HCO3 by 2 mEq/L for every 10mmHg in PCO2
– Chronic - Ratio increases to 4 mEq/L of HCO3 for every 10mmHg in PCO2
– Decreased bicarb reabsorption and decreased ammonium excretion to normalize pH

Metabolic Acidosis
• pH, HCO3
• 12-24 hours for complete activation of respiratory compensation
• PCO2 by 1.2mmHg for every 1 mEq/L HCO3
• The degree of compensation is assessed via the Winter’s Formula
PCO2 = 1.5(HCO3) +8 2

The Causes
• Metabolic Gap Acidosis – M - Methanol
– U - Uremia
– D - DKA
– P - Paraldehyde
– I - INH
– L - Lactic Acidosis
– E - Ehylene Glycol
– S - Salicylate
• Non Gap Metabolic
Acidosis
– Hyperalimentation
– Acetazolamide
– RTA (Calculate urine
anion gap)
– Diarrhea
– Pancreatic Fistula

Metabolic Alkalosis
• pH, HCO3
• PCO2 by 0.7 for every 1mEq/L in HCO3
• Causes
– Vomiting
– Diuretics
– Chronic diarrhea
– Hypokalemia
– Renal Failure

Mixed Acid-Base Disorders
• Patients may have two or more acid-
base disorders at one time
• Delta Gap
Delta HCO3 = HCO3 + Change in anion gap
Delta HCO3 >24 = metabolic alkalosis

The Steps
• Start with the pH
• Note the PCO2
• Calculate anion gap
• Determine compensation

Sample Problem #1
• An ill-appearing alcoholic male presents
with nausea and vomiting.
– ABG – 7.25 / 34 / 85 / 16
– Na- 137 / K- 3.8 / Cl- 90 / HCO3- 16

Sample Problem #1
• Anion Gap = 137 - (90 +16) =31
anion gap metabolic acidosis
• Winters Formula = 1.5(16) + 8 2
= 32 2
compensated
• Delta Gap =( 31 – 12) + 16 = 35
metabolic alkalosis

Sample Problem #2
• 22 year old female presents for
attempted overdose. She has taken an
unknown amount of Midol containing
aspirin, cinnamedrine, and caffeine. On
exam she is experiencing respiratory
distress.

Sample Problem #2
• ABG - 7.47 / 19 / 123 / 14
• Na- 145 / K- 3.6 / Cl- 109 / HCO3- 14
• ASA level - 38.2 mg/dL

Sample Problem #2
• Anion Gap = 145 - (109 + 14) = 22
anion gap metabolic acidosis
• Winters Formula = 1.5 (14) + 8 2
= 29 2
uncompensated
• Delta Gap = 22 - 12 = 10
10 + 14 = 24
no metabolic alkalosis

Sample Problem #3
• 47 year old male experienced crush
injury at construction site.
• ABG - 7.3 / 32 / 96 / 15
• Na- 135 / K-5 / Cl- 98 / HCO3- 15 /
BUN- 38 / Cr- 1.7
• CK- 42, 346

Sample Problem #3
• Anion Gap = 135 - (98 + 15) = 22
anion gap metabolic acidosis
• Winters Formula = 1.5 (15) + 8 2
= 30 2
compensated
• Delta Gap = 22 - 10 = 12
12 + 15 = 27
mild metabolic alkalosis

Sample Problem #4
• 1 month old male presents with
projectile emesis x 2 days.
• ABG - 7.49 / 40 / 98 / 30
• Na- 140 / K- 2.9 / Cl- 92 / HCO3- 32

Sample Problem #4
• Metabolic Alkalosis, hypochloremic
• Winters Formula = 1.5 (30) + 8 2
= 53 2
uncompensated

SVCC Respiratory Care
Programs
ABG Analysis, Introduction
• pH, PaCO2, PaO2 are measured directly
by special electrodes contained in a
device made for that purpose
• Other indirect measurements can be
made or calculated from the above
measurements i.e., HCO3-, O2 Sat.

SVCC Respiratory Care
Programs
QA in Blood Gas Analysis
• ABG lab must be able to assure
accurate and reliable results
• The above is accomplished by applying
protocols in 3 areas:
- pre-analytic error
- calibration
- quality control

SVCC Respiratory Care
Programs
Pre-analytic Error • All factors that cause variance in lab results
prior to the sample arriving in the ABG lab.
• 4 factors assoc. with signif. P. E. are:
- air bubbles in sample
- time delay (iced sample with more than
60 min. or uniced with more
than 10 min.)
- blood clots in sample
- small sample size where excessive
anticaogulation is suspect

SVCC Respiratory Care
Programs
Calibration
• Purpose is assure consistency
• Def.: the systemic standardization of the
graduation of a quantitative measuring
instrument
• Calibrating standards for blood gas analyzers
should simulate the physical properties of
blood and meet manuf. specs.
• When 2 standards are used ---> 2-point
calibration, performed after 50 blood gases or
at least every 8 hours

SVCC Respiratory Care
Programs
Calibration (cont’d)
• A “one-point calibration” is an
adjustment of the electronic response of
an electrode to a single standard and is
performed more freq. than a 2 pt. cal.,
ideally prior to each sample analysis

SVCC Respiratory Care
Programs
Quality Control
• Refers to a system that documents the
accuracy and reliability of the blood gas
measurements and is essential to assure
accuracy in the blood gas lab
• Media available as blood gas controls
include:
- aqueous buffers
- glycerin soltn.
- human/animal serum and blood
- artificial blood
• A QC system must ID problems and specify
corrective action, document. of accept. oper.

SVCC Respiratory Care
Programs
QC (cont’d)
• Documentation of QC is usu. on Levy-
Jennings Chart which shows measured
results on the y axis versus time of
measurement on the x axis
• SD is used to summarize a mass of data: the
difference between a number in a data set
and the mean of the data set is called a
deviation. A deviation shows how much a
number varies from the mean

SVCC Respiratory Care
Programs
QC (cont’d)
• A properly functioning electrode that
repeatedly analyzes a known value will
produce results within a rel. small range, e.g.,
a PaCO2 electrode that analyzes a 40 mmHg
standard 100 times will produce results where
2/3 of the measurements are 39 - 41 mmHg
and nearly all measurements fall in 38 - 42
range
• 95% of the control measurements should fall
within 2 SD

SVCC Respiratory Care
Programs
QC (cont’d)
• Random errors indicates a value outside of 2
SD of the mean: a single random error has
minor signif., but if number increased the
machine and techniques must be evaluated
• Systematic errors is recurrent measurable
deviation from the mean
• Causes of systematic errors:
- contaminated standard
- variations in electrode temp.
- inconsistent introduction of standard

SVCC Respiratory Care
Programs
QC (cont’d)
• Causes of systematic error (cont’d)
- inconsistent calibration
technique - change in QC
standard storage or prep. - electrode
problems, e.g., protein contamin.,
membrane malfunction,
contamin. electrolyte, or electrical
problems

SVCC Respiratory Care
Programs
QC Levels
• Level 1 simulates a patient
hypoventilating
• Level 2 simulates a patient with normal
ventilatory status
• Level 3 simulates a patient
hyperventilating

HCO3- (bicarbonate):
SB (standard bicarbonate)
AB (actual bicarbonate)
SB: the contents of HCO3- of serum of arterial
blood in 37-38℃, PaCO2 40mmHg, SaO2 100%.
Normal: 22-27mmol/L
mean: 24mmol/L
AB: The contents of HCO3- in actual condition.
In normal person: AB=SB

AB and SB are parameters to reflect
metabolism, regulated by kidney.
Difference of AB-SB can reflect the
respiratory affection on serum HCO3- .
Respiratory acidosis: AB>SB
Respiratory alkalosis: AB<SB
Metabolic acidosis: AB=SB<Normal
Metabolic alkalosis: AB=SB>Normal

8 Sequential Rules:
• Rule #1
– Must know the pH; pH determines whether the
primary disorder is an acidosis or an alkalosis
• Rule #2
– Must know the PaCO2 and serum HCO3-
• Rule #3
– Must be able to establish that the available data
(pH, PaCO2, and HCO3-) are consistent

Are the data consistent?
• The Henderson Equation:
3
2
24HCO
PaCOH

Convert [H+] to pH:
• Subtract calculated [H+] from 80; this gives
the last two digits of a pH beginning with 7
– example: calculated [H+] of 24 converts to pH
of (80-24)~7.56
– example: calculated [H+] of 53 converts to pH
of (80-53)~7.27
• Refer to table 1 in handout for more precise
conversion, or if calculated [H+] exceeds 80

Relationship between [H+] & pH

Relationship between [H+] & pH
pH [H+] pH [H
+]
7.80
7.75
16
18
7.30
7.25
50
56
7.70
7.65
20
22
7.20
7.15
63
71
7.60
7.55
25
28
7.10
7.00
79
89
7.50
7.45
32
35
6.95
6.90
100
112
7.40
7.35
40
45
6.85
6.80
141
159


Simple Acid-Base Disorders:
T ype of D isorder pH PaC O 2 [H C O 3]
M etabolic A cidosis
M etabolic A lkalosis
A cute R espiratory A cidosis
C hronic R espiratory A cidosis
A cute R espiratory A lkalosis
C hronic R espiratory A lkalosis

Simple Acid-Base Disorders:
T ype of D isorder pH PaC O 2 [H C O 3]
M etabolic A cidosis
M etabolic A lkalosis
A cute R espiratory A cidosis
C hronic R espiratory A cidosis
A cute R espiratory A lkalosis
C hronic R espiratory A lkalosis

Simple Acid-Base Disorders:
T ype of D isorder pH PaC O 2 [H C O 3]
M etabolic A cidosis
M etabolic A lkalosis
A cute R espiratory A cidosis
C hronic R espiratory A cidosis
A cute R espiratory A lkalosis
C hronic R espiratory A lkalosis

Simple Acid-Base Disorders:
T ype of D isorder pH PaC O 2 [H C O 3]
M etabolic A cidosis
M etabolic A lkalosis
A cute R espiratory A cidosis
C hronic R espiratory A cidosis
A cute R espiratory A lkalosis
C hronic R espiratory A lkalosis
T ype of D isorder pH PaC O 2 [H C O 3]
M etabolic A cidosis
M etabolic A lkalosis
A cute R espiratory A cidosis
C hronic R espiratory A cidosis
A cute R espiratory A lkalosis
C hronic R espiratory A lkalosis

Simple Acid-Base Disorders:
T ype of D isorder pH PaC O 2 [H C O 3]
M etabolic A cidosis
M etabolic A lkalosis
A cute R espiratory A cidosis
C hronic R espiratory A cidosis
A cute R espiratory A lkalosis
C hronic R espiratory A lkalosis

Simple Acid-Base Disorders:
T ype of D isorder pH PaC O 2 [H C O 3]
M etabolic A cidosis
M etabolic A lkalosis
A cute R espiratory A cidosis
C hronic R espiratory A cidosis
A cute R espiratory A lkalosis
C hronic R espiratory A lkalosis

Simple Acid-Base Disorders:
T ype of D isorder pH PaC O 2 [H C O 3]
M etabolic A cidosis
M etabolic A lkalosis
A cute R espiratory A cidosis
C hronic R espiratory A cidosis
A cute R espiratory A lkalosis
C hronic R espiratory A lkalosis

Simple Acid-Base Disorders:
T ype of D isorder pH PaC O 2 [H C O 3]
M etabolic A cidosis
M etabolic A lkalosis
A cute R espiratory A cidosis
C hronic R espiratory A cidosis
A cute R espiratory A lkalosis
C hronic R espiratory A lkalosis

Simple Acid-Base Disorders:
T ype of D isorder pH PaC O 2 [H C O 3]
M etabolic A cidosis
M etabolic A lkalosis
A cute R espiratory A cidosis
C hronic R espiratory A cidosis
A cute R espiratory A lkalosis
C hronic R espiratory A lkalosis

Simple Acid-Base Disorders:
• The compensatory variable always changes
in the SAME DIRECTION as the
primarily deranged variable
• Compensation is always more pronounced
in CHRONIC RESPIRATORY disorders
than in acute respiratory disorders

8 Sequential Rules:
• Rule #4:
– must know if compensation is appropriate
– compensation never overshoots
• Must have known “rules of thumb” to
interpret appropriateness of compensation

Rules of Compensation:
• Metabolic Acidosis
– PaCO2 should fall by 1 to 1.5 mm Hg x the fall
in plasma [HCO3]
• Metabolic Alkalosis
– PaCO2 should rise by .25 to 1 mm Hg x the rise
in plasma [HCO3]

Rules of Compensation:
• Acute Respiratory Acidosis
– Plasma [HCO3] should rise by ~1mmole/l for
each 10 mm Hg increment in PaCO2
• Chronic Respiratory Acidosis
– Plasma [HCO3] should rise by ~4mmoles/l for
each 10 mm Hg increment in PaCO2

Rules of Compensation:
• Acute Respiratory Alkalosis
– Plasma [HCO3] should fall by ~1-3 mmole/l for
each 10 mm Hg decrement in PaCO2, usually
not to less than 18 mmoles/l
• Chronic Respiratory Alkalosis
– Plasma [HCO3] should fall by ~2-5 mmole/l for
each 10 mm Hg decrement in PaCO2, usually
not to less than 14 mmoles/l

Case #1:
• A 24 years old with chronic renal failure
presents to ER with history of increasing
azotemia, weakness, and lethargy. Exam
reveals the patient to be modestly
hypertensive, and tachypneic. Labs reveal
BUN=100 mg, and Creatinine=8 mg.

Case #1:
• Steps 1&2: must know pH, PaCO2, HCO3
• pH=7.37, PaCO2=22, and HCO3=12
• Step 3: are the available data consistent?
3
2
24HCO
PaCOH

Case #1:
• [H+]=44, equates to pH~7.36; data are thus
consistent
• What is the primary disorder?
• “_________Acidosis”
• Which variable (PaCO2, HCO3) is deranged
in a direction consistent with acidosis?
• Primary disorder is “Metabolic Acidosis”

Is compensation appropriate?
• HCO3 is decreased by 12 mmoles/l
• PaCO2 should decrease by 1 to 1.5 times the
fall in HCO3; expect PaCO2 to decrease by
12-18 mm Hg or be between 22-28 mm Hg
• Since PaCO2 is 22 mm Hg, compensation is
appropriate, and the data are consistent with
a simple metabolic acidosis with respiratory
compensation

8 Sequential Rules:
• Rule #5:
– If the data are consistent with a simple disorder,
it does not guarantee that a simple disorder
exists; need to examine the patient’s history
• Rule #6:
– When compensatory responses do not lie within
the accepted range, by definition a combined
disorder exists.

Case #2:
• A 16 year old male with sickle cell anemia,
hemochromatosis, & subsequent cirrhosis,
presents with a several day history of
emesis. At presentation to the pedes ER, he
is hypotensive, orthostatic, and confused.
• What acid-base disorders might be
anticipated based on the above information?

Case #3:
• 16 yo male with sickle cell anemia, hemo-
chromatosis, & subsequent cirrhosis, and
several days of emesis. In the pedes ER, he
is hypotensive, orthostatic, and confused.
• Emesis-loss of H+ (HCl)-metabolic alkalosis
• Orthostatic hypotension-?lactic acidosis
• SCD-decreased O2 delivery-?lactic acidosis
• Cirrhosis-decreased lactate metabolism

Case #3:
• What baseline information is available?
• pH=7.55, PaCO2=66
• „lytes: Na+=166, K+=3.0, Cl-=90, HCO3=56
• Are the data internally consistent?
3
2
24HCO
PaCOH

Case #3:
• [H+]~28, equates to pH~7.55; consistent
• What is the primary abnormality?
• “_________ Alkalosis”
• PaCO2ed, HCO3 ed, therefore…….
• “Metabolic Alkalosis” presumed due to
emesis
• Is compensation appropriate?

Case #3:
• Metabolic Alkalosis
– PaCO2 should rise by .25 to 1 mm Hg x the rise
in plasma [HCO3]
• HCO3 ed by 32; PaCO2 should by 8-32
• PaCO2 ed by 26, so compensation appears
appropriate
• What about multiple risk factors for lactic
acidosis?

Case #3:
• Could there be a concealed lactic acidosis?
• What is the anion gap?
• Na+- (Cl- + HCO3), normally 12-14
• Anion gap here is 166 - (90 + 56) = 20
• ed anion gap implies metabolic acidosis
• Combined metabolic alkalosis &
metabolic acidosis therefore present

8 Sequential Rules:
• Rule #7: Always calculate the anion gap
• Often it is the only sign of an occult
metabolic acidosis
– acidotic patients partially treated with HCO3
– acidotic patients with emesis
• May be the only sign of metabolic acidosis
“concealed” by concomitant acid-base
disorders

Causes of Anion Gap Acidosis:
• Endogenous acidosis
– Uremia (uncleared organic acids)
– Ketoacidosis, Lactic acidosis (increased organic
acid production), Rhabdomyolosis
• Exogenous acidosis
– ingestions: salicylate, iron; paraldehyde use
• Other Ingestions:
– Methanol toxicity, Ethylene Glycol toxicity

Causes of normal Anion Gap Acidosis:
• Diarrhea
• Isotonic saline infusion
• Renal tubular acidosis
• Acetazolamide
• Ureterocolic shunt

Anion Gap:
• Based on the concept of electroneutrality; the
assumption that the sum of all available cations=
the sum of all available anions. Restated as:
• Na+ + Unmeasured Cations (UC) = Cl- + HCO3 +
Unmeasure Anions (UA); conventionally restated:
• Na+-(Cl-+HCO3)=UA-UC=Anion Gap=12 to 14

Anion Gap:
• Na+-(Cl-+HCO3)=UA-UC
• Serum albumin contributes ~1/2 of the total anion
equivalency of the “UA” pool. Assuming normal
electrolytes, a 1gm/dl decline in serum albumin
decreases the anion gap factitiously by 3 mEq/L.
Therefore an anion gap of 12 mEq/L is corrected
to 17-18 mEq/L when the serum albumin is half of
normal; this is an important correction factor in
settings of chronic illness or malnourished patients

Case #3:
• A 3 year old is brought to the pedes ER at
~3am, stuporous and tachypneic. History is
remarkable for his parents having cleaned
out their medicine cabinet earlier that day.
An ABG and electrolytes have been
accidentally drawn by the nurse.

Case #4:
• Available data: pH=7.53, PaCO2=12;
Na+=140, K+=3.0, Cl-=106, HCO3=10
• Are the data internally consistent?
3
224HCO
PaCOH

Case #4:
• [H+]~29, so pH~7.51; data consistent
• What is the primary disturbance?
• “__________ Alkalosis”
• Which variable (PaCO2, HCO3) is deranged
in a direction consistent with alkalosis?
• ed PaCO2, ed HCO3; so “Respiratory
Alkalosis”

Case #4:
• Is compensation appropriate?
• Acute respiratory alkalosis
– Plasma [HCO3] should fall by ~1-3 mmole/l for
each 10 mm Hg decrement in PaCO2, usually
not to less than 18 mmoles/l
• PaCO2 ed by ~30 mm Hg; HCO3 should
fall by 3-9 mmole/l; HCO3 is too great, so
superimposed metabolic acidosis

Case #4:
• What is the anion gap?
• 140 - (106 + 10) = 24; elevated anion gap
consistent with metabolic acidosis
• What is the differential diagnosis?
• Combined (true) respiratory alkalosis and
metabolic acidosis seen in sepsis, or
salicylate intoxication

Case #5:
• A 5 year old with Bartter‟s Syndrome is
brought to clinic, where she collapses. She
has recently been febrile, but history is
otherwise unremarkable. An ABG and
serum electrolytes are obtained: pH=6.9,
PaCO2=81; Na+=142, K+=2.8, Cl-=87,
HCO3=16

Case #5:
• Are the data consistent?
• [H+]=122, pH~6.9; data are consistent
3
224HCO
PaCOH

Case #5:
• What is the primary disturbance?
• “_________ Acidosis”
• Which variable (PaCO2, HCO3) is deranged
in a direction consistent with acidosis?
• Both; pick most abnormal value--
• “Respiratory Acidosis”
• Is compensation appropriate?

Case #5:
• Acute Respiratory Acidosis
– Plasma [HCO3] should rise by ~1mmole/l for
each 10 mm Hg increment in PaCO2
• Since HCO3 is inappropriately depressed,
compensation is not appropriate, and there
is a concomitant metabolic acidosis as well
• What is the anion gap?
• AG=39, confirms metabolic acidosis

Case #5:
• Combined Respiratory Acidosis and
Metabolic Acidosis; are there other
disorders present?
• What about the dx of Bartter‟s Syndrome?
• Bartter‟s Syndrome characterized by
hypokalemic metabolic alkalosis
• Does this patient have a concealed
metabolic alkalosis?

Case #5:
• Anion gap is 39, or 25-27 greater than
normal
• Typically, increases in anion gap correlate
with decreases in HCO3
• Assuming a 1:1 relationship, as anion gap
increases by 25, HCO3 should fall by 25
• Starting HCO3 must have been 16 + 25 = 41

Case #5:
• Therefore, starting HCO3 was ~41 mmol/l,
consistent with expected chronic metabolic
alkalosis. This metabolic alkalosis was
“concealed” by the supervening profound
metabolic and respiratory acidoses
associated with her arrest event.
• Final diagnosis: Metabolic alkalosis,
metabolic acidosis, & respiratory acidosis

8 Sequential Rules; Rule #8
• Rule #8: Mixed Acid-Base Disorders
• Coexistant metabolic acidosis and
metabolic alkalosis may occur. Always
check the change in the anion gap vs.
decrement in bicarbonate to rule out a
concealed metabolic disorder.

Case #6:
• A 3 year old toddler is brought to the ER at
3 am after being found unarousable on his
bedroom floor, with urinary incontinence.
EMS monitoring at the scene revealed sinus
bradycardia. One amp of D50W and 5 mg
of naloxone were given IV without
response. Vital signs are stable; respiratory
effort is regular, but tachypneic. He is
acyanotic.

Case #6:
• Initial lab studies (lytes, ABG & urine tox
screen) are sent. Initial dextrostick is >800.
• Initial available data are:
• Na+=154, K=5.6, Cl=106, HCO3=5,
BUN=6 creatinine=1.7, glucose=804,
PO4=12.3, Ca++=9.8, NH4=160, serum
osms=517
• pH=6.80, PaCO2=33, PaO2=298

Case #6:
• What is the primary disturbance?
• ________ Acidosis
• Metabolic Acidosis
• Is compensation appropriate?
• No; PaCO2 level is inappropriately high
• Are other disorders present?
• Respiratory acidosis (due to evolving coma)

Case #6:
• What is our differential thus far?
– Anion gap vs. non-anion gap metabolic acidosis
– DKA, lactic acidosis, renal failure, ingestion
• The urine tox screen comes back negative
– What does urine tox screen actually screen for?
• The patient‟s IV falls out. He then has a
seizure, is incontinent of urine, and fills the
specimen bag you placed on ER arrival.

Case #6:
• What is the calculated serum osmolality,
and does an osmolal gap exist?
• 2(Na) + BUN/2.8 + Glucose/18
– Calculated=355, Measured=517
• What is the most likely diagnosis?
• How can this be confirmed definitively?
– Review of urinalysis
– Serum ethylene glycol level

Case #6:
Anion gap metabolic acidosis
Osmolal gap
Methanol, ethylene glycol
ethyl alcohol, isopropyl alcohol

Gap-Gap
*AG excess/HCO3 deficit=
(Measured AG-12)/ (24-measured HCO3)
*Ratio <1 in presence of high AG acidosis means coexistance of normal AG metabolic acidosis
*Ratio >1 in presence of high AG acidosis means coexistance of metabolic alkalosis