Redalyc.Total gastrectomy due to ferric chloride intoxication

Gut, 1961, 2, 218
Co58B12 absorption (hepatic surface count)
after gastrectomy, ileal resection,and in coeliac disorders
D. J. FONE, W. T. COOKE, M. J. MEYNELL, AND E. L. HARRIS
From the General Hospital, Birmingham
SYNOPSIS This paper demonstrates that the hepatic surface counting technique is a reliable andsatisfactory method of estimating the absorption of radioactive vitamin B12. It does not require thecollection of faeces or urine and is therefore particularly useful in studying out-patients.
When Co58B12 is absorbed from the intestinal tract,radioactivity accumulates in the liver, reaching itsmaximum in -seven to 10 days and thereafter slowlydeclines. Glass, Boyd, Gellin, and Stephanson (1954)demonstrated that the degree of absorption ofvitamin B12 could be measured by scintillation count-ing over the surface of the liver and that hepaticsurface radioactivity was a true measure of the con-tent of radioactive B12 in the liver. Baker and Mollin(1956) demonstrated good correlation between thehepatic uptake measured by direct counting over theliver and the amount of radioactive B12 absorbed asestimated by the faecal excretion technique.The method has certain practical advantages
compared with the more widely used faecal (Heinle,Welch, Scharf, Meacham, and Prusoff, 1952) andurinary excretion methods (Schilling, 1953). It doesnot require the collection of faeces or urine andshould therefore be of particular value for the in-vestigation of out-patients, and secondly it does notrequire the administration of a large saturating doseof non-radioactive vitamin B12 which may obscurethe haematological picture and response. Despitethese advantages it does not appear to have beenadopted generally in Britain. The purpose of thispaper is to check the validity of the technique andto assess its use in three common groups of intestinaldisorders in which abnormalities of B12 absorptionmay occur, namely, post-gastrectomy states, in-testinal resection, and the coeliac group of disorders.
METHODS
CoM-labelled vitamin B12 (supplied by the RadiochemicalCentre, Amersham, England) was administered orally ina dose of 0.25 to 0.50 jug. of vitamin B12 containing0-33-0-50 ,uc. Co"8, dissolved in 20 ml. distilled water
after patients had fasted for at least 12 hours (overnight);no food or drink was allowed for the following twohours.The technique of estimating the accumulated hepatic
radioactivity was essentially similar to that described byGlass and his co-workers. The hepatic radioactivity wascounted with an EKCO cylindrically collimated scintilla-tion counter having a 1 in. thallium-activated sodiumiodide crystal. Initially, counting was performed in twoor more planes over the liver surface, but it was foundthat the variation in counts obtained in different planeswas small, and that entirely satisfactory results wereobtained by counting in one only. The majority of testswere, therefore, performed with the collimator placed incontact with the skin in the anterior axillary line in thecentre of the area of liver dullness. Counting was carriedout for five minutes, the results obtained then being cor-rected for background radiation and expressed as countsper minute per 1 ,uc. of Co"8.The liver was counted in this manner before administra-
tion of the dose, and then again between the sixth andtenth days afterwards. Initially, two counts were made ondifferent days in this period to ensure that the plateau hadbeen reached; it soon became evident that a single countwas quite satisfactory, and subsequently this wasperformed, usually on the seventh day.When the absorption of Co"8B1, was found to be
impaired, a second dose was given with 10 mg. of intrinsicfactor concentrate (Lederle) active in pernicious anaemiain 5 to 10 mg. quantities. The hepatic surface count wasthen repeated seven days later. The difference between thetwo readings (after background corrections) was takento represent the hepatic radioactivity resulting from in-creased absorption of vitamin B1, as a result of the addi-tion of intrinsic factor. On each occasion the radioactivityover the lower abdomen (just below the umbilicus) wasalso measured. If the counts in this region exceeded 50%of the liver count, the estimation was repeated after aninterval of at least three days. This was, however, onlyoccasionally necessary.
>18
on April 17, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.2.3.218 on 1 S
eptember 1961. D
ownloaded from

Co58B12 absorption after gastrectomy, ileal resection, and in coeliac disorders
Serum levels of vitamin B12 were estimated by themethod of Meynell, Cooke, Cox, and Gaddie (1957),which gives a normal range of 105 to 672 ,gujg. per ml.with a mean normal concentration of 281 yug. per ml.The faecal excretion of the administered Co58B,2 was
estimated by counting the radioactivity appearing in thefaeces daily until none was present on each of two con-secutive days. The total faecal radioactivity was expressedas a percentage of the dose (after background corrections)obtained in the same counter.
RESULTS
CORRELATION OF HEPATIC SURFACE COUNT WITHFAECAL EXCRETION OF CoMB12
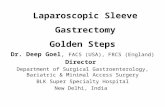
On 15 occasions the percentage absorption of theadministered dose of Co58B12 was estimated bythe faecal excretion method at the same time as thehepatic radioactivity was measured (Fig. 1). Theresults indicate good correlation between these twomethods.
CONTROL GROUPS
NORMAL SUBJECTS (FIG. 2) This group of 28 subjectsconsisted of 20 hospital patients with no gastro-
400Q
CP 3000_
W-
.< ca.
C c 2000_D._
tnE
0-
L
1000_
10 20 30 40
7% DOSE ABSORBED.
intestinal or haematological disorder, five with iron-deficiency anaemia, and three with ulcerative colitisbut with no evidence of small intestinal involvement.All had normal serum levels of vitamin B12, and noclinical evidence of B12 deficiency; hepatic radio-activity ranged from 1,600 to 4,633 counts perminute per microcurie with a mean of 2,914, S.D.828; statistical range (mean ± 2 S.D.) 1,258-4,570.The test was repeated with the addition of intrinsicfactor in six subjects. In each case the result wassimilar to that obtained by the ingestion of Co58B12alone.
PERNICIOUS ANAEMIA (FIG. 2) Nineteen patients withAddisonian anaemia were studied. In 12 the diag-nosis had previously been established on adequategrounds and confirmed by continued normal haema-tological values with liver or vitamin B12 therapyover periods of up to 10 years. In the remainingseven the test was performed as part of the initialdiagnostic investigation. None of these patients hadsteatorrhoea. Following ingestion of Co58B12 alone,hepatic surface counts varied from 0 to 720 perminute per microcurie (mean 237, S.D. 231). Whenintrinsic factor was added to the ingested Co58B12,the hepatic surface counts were increased in each
(FAECAL
FIG. 1. Hepatic surfaceradioactivity comparedwith the percentage ofCo58Bl2 absorbed as
determined by thefaecalexcretion technique.Open circles represent a
testperformed with Co58vitamin B12 alone.Closed circles representa test performed withCo58 vitamin B12 plus
intrinsic factor.
tu Ou YVU lW
EXCRETION METHOD).
0
00 0
0
0
00
0
.P ^,I A ^ C^ £^ 'M 0^ ^r In
219
in
on April 17, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.2.3.218 on 1 S
eptember 1961. D
ownloaded from

D. J. Fone, W. T. Cooke, M. J. Meynell, and E. L. Harris
case to the same range as obtained in the normalsubjects (range 1,574 to 4,268).
TOTAL GASTRECTOMY Two patients were studiedfour and 10 years after total gastrectomy. Both hadreceived regular B12 therapy since the time of opera-tion. In both the hepatic surface counts followingingestion of Co58B12 alone were very low (0 and 66),but on the addition of intrinsic factor increased tothe normal range (2,365 and 2,172).
INTESTINAL DISORDERS
PARTIAL GASTRECTOMY Twenty-four patients werestudied following partial gastrectomy, the intervalsince operation being three months to 12 years (Fig.2). In 18 the results were within the normal range.None of these patients had any clinical manifestationof B12 deficiency, and in the majority serum vitaminB12 levels have been persistently normal; occasionalmoderately low levels of serum vitamin B12 have been
encountered in three of these subjects in whomabsorption was found to be normal.
In four cases the hepatic surface counts were inthe same range as seen in pernicious anaemia (261,282, 292, 723), and in each increased to the normalrange upon the addition of intrinsic factor to theingested Co58B12 (2,799, 3,000, 1,907, 2,919). Thesefour patients had had a Polya type gastrectomyseven, nine, 10, and 12 years previously, in twoinstances for gastric carcinoma and in two forchronic peptic ulcer. They have all developed clinicalevidence of deficiency of vitamin B12. Threedeveloped megaloblastic anaemia (seven, nine, and 12years after operation), associated with very lowserum B12 levels and responded adequately to B12therapy. The fourth developed subacute combineddegeneration of the spinal cord 10 years after opera-tion, associated with a very low serum B12 level. He,also, responded excellently to B12 therapy.
In two patients the hepatic surface counts werebelow normal (1,028 and 1,034 counts per minute
0 0
0
0 0
0 00
0 0
0 0
0
00
0
0 0
0
0
0
0
0
0
0
7 1
0 0
0* -@0~~00 .0
0@* *0
*
a
0000
0o %^ no C00
o
0
00
0
0 IoI°10 '
o 01,
0:0
0
00
0
0
0
01
1
06
h
1to1'
1'
11;1.
111.1111.111.
>
v
0
0
0
0
0
0
0
Eo,C].
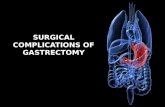
oh tej PERNICIOUS L P A R T I A L RESECTIONCONTROLS
ANAEMIA GASTRECTOMY OF ILEUMFIG. 2. Hepatic surface radioactivity in control subjects and in patients with pernicious anaemia, followinggastrectomy and resection of the ileum.Open circles represent a test performed with Col8 vitamin B12 alone.Closed circles represent a test performed with Co'8 vitamin B12 plus intrinsic factor.
400Q.
' 3000_z
Uo
u a-LU 4.U.
C~) .3cc.c= 2000_
c-.
: 1000_
220
.F
rl%
on April 17, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.2.3.218 on 1 S
eptember 1961. D
ownloaded from

Co58B12 absorption after gastrectorny, ileal resection, and in coeliac disorders
per microcurie) but not as low as those seen inpernicious anaemia. In each the count rose con-siderably after the addition of intrinsic factor to theingested dose (3,600 and 3,646 counts per minute permicrocurie). In one, megaloblastic anaemia occurredfive years after partial gastrectomy for gastric andduodenal ulcers; full response followed vitamin B12therapy, which was discontinued after three years.Two years later macrocytosis and glossitis recurred,which again responded to vitamin B12 therapy. Theother patient was seen eight years after operationwith a severe iron-deficiency anaemia and anassociated low serum B12 level of 50 g,g. per ml.Her marrow showed normoblastic erythropoiesiswith no evidence of megaloblastic change.
AFTER RESECTION OF THE ILEUM Sixteen patientswere studied after resection of a portion of the ileum(Fig. 2). In 14 this resection was performed forregional ileitis (right hemicolectomy in 11, resectionof the distal ileum alone in two, and resection of asegment of the mid-ileum in one). In one patient aright hemicolectomy was performed for carcinomaof the caecum; in one 24 in. of distal ileum wasresected for an argentaffin tumour.
In seven patients, in whom resection was per-formed from one to 14 years previously, the hepaticsurface radioactivity was within the normal range.All seven have maintained normal serum vitamin B12levels and none has developed macrocytic anaemia.
In the other nine patients in whom resection wasperformed from one to 13 years previously, thehepatic radioactivity was below normal, varyingfrom 60 to 876 counts per minute per microcurieafter the ingestion of Co58B12. When intrinsic factorwas added to the Co58B12, the counts were not sig-nificantly altered (72-1,156). In two cases a thirddose was given following the administration of tetra-cycline for five days: in neither was there any sig-nificant improvement in the absorption. These ninepatients have all had abnormally low serum vitaminB12 levels since their operation (25 to 85 ,u,ug. perml.). Six were receiving parenteral vitamin B12therapy; in three this was begun because of thedevelopment of macrocytic anaemia (the marrowwas megaloblastic in the two patients in whom it wasexamined), and in three because of persistently lowserum vitamin B12 concentrations, though anaemiawas not present. Three have not yet received vitaminB12 therapy, though they also have persistently lowserum B12 levels but no anaemia.The area of ileum resected in the patients who have
retained normal vitamin B12 absorption was theterminal ileum in six, the lengths being 6 in., 9 in.,12 in., 12 in., and 4 ft. (it was unknown in one case);the seventh patient had 16 in. of mid-ileum removed.
The nine patients with impaired vitamin B12absorption all had terminal ileum resected, thelengths in seven being 12 in., 18 in., 2 ft., 2 ft., 3 ft.,6 ft., and 'a few feet'. In one 11 in. of terminal ileumwas resected as well as a further 9 in. about 2 ft.proximally. The ninth had a right hemicolectomyfor carcinoma of the caecum.None of the 14 patients with Crohn's disease has
had clinical evidence of recurrence, and in none isthere evidence of stricture or formation of a blindloop. Only two have biochemical evidence of activedisease with increased serum seromucoid concentra-tion (Cooke, Fowler, Cox, Gaddie, and Meynell,1958). In one of these absorption is normal, in theother it is impaired. Liver function tests were normalin all.
ADULT COELIAC DISEASE AND IDIOPATHIC STEATOR-RHOEA Fifty patients were studied in whom adiagnosis of adult coeliac disease (Cooke, 1958) or'idiopathic steatorrhoea' (Cooke, Peeney, andHawkins, 1953) had been made. The results of thehepatic radioactivity are shown in Fig. 3, in whichthese patients are classified according to criteriarecently described (Fone, Cooke, Meynell, Brewer,Harris, and Cox, 1960) with special reference to thehistological appearances of the upper small intestineobtained by peroral biopsy.
In 22 patients with adult coeliac disease and a'flat' jejunal mucosa, the hepatic radioactivity waswithin the normal range in 18; in four it was belownormal (in three as low as that seen in perniciousanaemia), but was not significantly improved by theaddition of intrinsic factor.On the 28 patients with jejunal biopsies showing
'abnormal villi' (partial atrophy), eight resembledthose of adult coeliac disease in many respects butdiffered particularly in the histology of the jejunalmucosa. Hepatic radioactivity was normal in five; inthree it was below normal, but improved to thenormal range when intrinsic factor was added. Thesethree each had histamine-fast achlorhydria, and inthe two in whom gastric biopsy was performed themucosa showed severe inflammation and glandularatrophy.
In seven patients the major feature was a severemegaloblastic anaemia associated with low serumlevels of vitamin B12 which responded adequately toparenteral B12 therapy. In five hepatic radioactivitywas much below normal, but was improved to thenormal range by the addition of intrinsic factor. Allfive had histamine-fast achlorhydria, and severegastric atrophy was present in all four in whombiopsy was performed. One patient had normalhepatic radioactivity; his gastric mucosa was normal.The seventh patient had impaired absorption which
221
on April 17, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.2.3.218 on 1 S
eptember 1961. D
ownloaded from

D. J. Fone, W. T. Cooke, M. J. Meynell, and E. L. Harris
4000_
t2 3000z
W ,U o,L.cc0.c c 2000.
LM0~uJ
- 1000
0
0
0
0O*
00
o0
0 0
00
0
0
0
0
0
0
0
00
0
U l A a
0
00
0 0
0I
IIillII
II
IIII
0
II
0P00
0
* -LA
ADLT COELIAC DISEASE K IDIOPATHIC STEATORRHOEA"
GROUP I GROUP 2
was not improved by the addition of intrinsic factor.In 12 patients the major clinical feature was a
severe megaloblastic anaemia associated with normalserum vitamin B12 levels, free gastric HCl; it res-ponded adequately to folic acid therapy. In 11 thehepatic radioactivity was normal. The gastricmucosa was normal in the three examined. In onepatient hepatic radioactivity was low and not im-proved by intrinsic factor; he also had a normalgastric mucosa.
DISCUSSION
An intrinsic factor defect was clearly demonstratedin all our patients with pernicious anaemia, whilstthe complete lack of intrinsic factor secretion ex-pected to follow total gastrectomy was confirmed inour two patients. As was shown by Baker andMollin (1956), there is good correlation with thefaecal excretion method of Heinle et al. (1952), hencethe hepatic radioactivity after an oral dose of radio-active vitamin B12 appears to be closely related to theamount absorbed. Our results in the control groupsconfirm previous observations that the hepaticsurface counting technique is a reliable method of
0
0
6
0
0
@1
* II
1iI
II
II161
00i
0
FIG. 3. Hepatic surfaceradioactivity in patientswith 'idiopathic steatorr-hoea'.Open circles represent atestperformed with Co58vitamin B12 alone.Closed circles representa test performed withCo58 vitamin B12 plusintrinsic factor.
estimating the degree of absorption of radioactivevitamin B12.A varying degree of impairment of intrinsic factor
secretion is a recognized, but uncommon, sequel ofpartial gastrectomy (Badenoch, Evans, Richards, andWitts, 1955; MacLean, 1957; Loewenstein, 1958)and was seen in six of our 24 patients. Each of thesesix had developed evidence of B12 deficiency. Asthese cases did not form an unselected series, theresults do not reflect the true incidence of B12deficiency as a result of partial gastrectomy whichhas been estimated as 0.6% (MacLean, 1957).
Since partial gastrectomy does not remove muchof the intrinsic factor secreting area of the mucosa-fundus and body-as does total gastrectomy, someother factor must be involved. Badenoch et al. (1955),on the basis of gastric biopsy studies in five patients,suggested that persistence of gastritis with mucosalatrophy in the gastric remnant is the explanation ofthe intrinsic factor defect. A similar conclusion wasreached by MacLean (1957) in a study of the mucosaof resected stomachs; he suggested that the develop-ment of megaloblastic anaemia following partialgastrectomy might be predicted by such study.The observation of moderately low serum B12
222
on April 17, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.2.3.218 on 1 S
eptember 1961. D
ownloaded from

Co"B12 absorption after gastrectomy, ileal resection, and in coeliac disorders
levels despite normal B12 absorption in three patientsfollowing partial gastrectomy is of interest. Asreported by Cox et al. (1959), the serum levels insuch patients do return to normal with the ad-ministration of iron. A possible explanation mightbe that although the B12 is absorbed when givenunder the 'ideal' conditions of the test, it may not beabsorbed as well when presented in food. Thisphenomenon has been demonstrated with theabsorption of iron (Baird and Wilson, 1959), andmay apply to B12 as well. Glass et al. (1960) havefound low serum B12 levels in some cases of gastritiswith histamine-fast anacidity in which absorption ofradioactive B12 was normal. They conclude that theexplanation for these inter-relationships must awaitmore complete knowledge of the natural history ofgastric atrophy and B12 deficiency.Impaired absorption which was not corrected by
the addition of intrinsic factor was demonstrated innine of the 16 cases following resection of ileum. Inall 16 cases the degree of absorption of vitamin B12was in excellent agreement with other features ofvitamin B12 metabolism. All seven patients in whomnormal absorption was demonstrated had main-tained normal serum B12 levels and normal bloodpictures since operation: the nine with impairedabsorption had all developed low serum vitamin B12levels with macrocytic anaemia in three. It is generallybelieved that in man vitamin B12 is absorbed in thedistal small intestine. Booth and Mollin (1959)found that absorption of vitamin B12, with andwithout intrinsic factor, was invariably subnormal inthe patients who had had more than 6 to 8 ft. ofileum resected or short circuited; the terminal ileumwas involved in each of their cases. In general, thelength of resected ileum was greater in our patientswith impaired absorption than in those in whomabsorption remained normal. It is of particularinterest, however, that absorption was impaired intwo patients in whom only 12 in. and 18 in. ofterminal ileum was resected. All but two of our grouphad had the resection performed for Crohn's disease;there was no significant difference between thosewith normal and those with abnormal absorption asregards severity of the lesion before operation orincidence of recurrence after operation. The diminu-tion in absorption appears more closely related tothe extent of involvement by the disease process thanfrom intestinal stasis or blind loops. These casesprovide further evidence that the distal ileum is themost important site for absorption of vitamin B12 inman. They also emphasize the need for constantobservation for the occurrence of vitamin B12deficiency or alternatively the routine prophylacticadministration of vitamin B12 after resection of evenshort lengths of ileum.
A similar type of absorptive defect was found inonly six of 50 patients with adult coeliac disease and'idiopathic steatorrhoea'. Contrary to the findings ofOxenhorn, Estren, Wasserman, and Adlersberg(1958) and Glass (1959), absorption of radioactiveB12 was found to be normal in the majority of ourcases of adult coeliac disease, and these observationscorrelate well with the maintenance of normal serumB12 levels in the majority and the absence in thisgroup of any instance of megaloblastic anaemia dueto vitamin B12 deficiency.A total of 11 patients with 'idiopathic steator-
rhoea', i.e., with abnormal jejunal villi or 'partialatrophy', had a megaloblastic anaemia due tovitamin B12 deficiency; in all but one the deficiencywas due to impaired secretion of intrinsic factor.The combination of intrinsic factor defect andsteatorrhoea has been previously described byMollin, Booth, and Baker (1957), Jarvinen andLatvalahti (1958), Williams, Coghill, and Edwards(1958), and Doig and Girdwood (1960). We considerthese patients to be a group distinct from adultcoeliac disease. They also differ from patients withpernicious anaemia, whom they resemble clinicallyin that dysfunction of the small intestine can bedemonstrated (Fone, Cooke, Meynell, and Cox,1961).One patient, a man of 39 years, was seen with
megaloblastic anaemia, low serum vitamin B12, andnormal gastric mucosa in whom B12 absorption wasfound on two occasions to be normal. Haemato-logical response to B12 therapy was complete. Therewas no history of anticonvulsant therapy. We haveno adequate explanation for this finding at present,and he is the only patient in this series in whom thehepatic radioactivity could be considered incon-sistent with other features of vitamin B12 metabolism.
SUMMARY AND CONCLUSIONS
The hepatic surface counting technique is a reliableand satisfactory method of estimating the absorptionof radioactive vitamin B12. It does not require collec-tion of faeces or urine, or the administration of aflushing dose of non-radioactive vitamin B12. It istherefore particularly useful for the study of out-patients, and its convenience and accuracy justifymore general use.
Results in patients following partial gastrectomywere comparable to those reported by others. Nineof 16 patients who had undergone ileal resectionmainly for regional ileitis had impaired absorption ofCo58B12, not improved with the addition of intrinsicfactor. There was some general relationship betweenthe degree of impairment and the amount of intestineresected. In contradistinction to other reports, only
223
on April 17, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.2.3.218 on 1 S
eptember 1961. D
ownloaded from

224 D. J. Fone, W. T. Cooke, M. J. Meynell, and E. L. Harris
six out of 50 patients with adult coeliac disease and'idiopathic steatorrhoea' showed this type of im-paired absorption of Co58B12 but 10 with abnormalvilli (partial atrophy) demonstrated an intrinsicfactor deficit as the cause for their failure to absorbCo58B12.
We are indebted to the Endowment Research Fund ofthe United Birmingham Hospitals for a grant for equip-ment and for the financial support of a research associate(D.J.F.).
REFERENCES
Badenoch, J., Evans, J. R., Richards, W. C. D., and Witts, L. J. (1955).Megaloblastic anaemia following partial gastrectomy andgastroenterostomy. Brit. J. Haemat., 1, 339-344.
Baird, I. M., and Wilson, G. M. (1959). The pathogenesis of anaemiaafter partial gastrectomy. II. Iron absorption after partialgastrectomy. Quart. J. Med., n.s. 28, 35-41.
Baker, S. J., and Mollin, D. L. (1956). The relationship betweenintrinsic factor and the intestinal absorption of Vitamin B1l.Brit. J. Haemat., 1, 46-51.
Booth, C. C., and Mollin, D. L. (1959). The site of absorption ofVitamin B12 in man. Lancet, 1, 18-21.
Cooke, W. T. (1958). Adult coeliac disease and other disordersassociated with steatorrhoea. Brit. med. J., 2, 261-265.
-, Fowler, D. I., Cox, E. V., Gaddie, R., and Meyneli, M. J. (1958).The clinical significance of seromucoids in regional ileitis andulcerative colitis. Gastroeneterology, 34, 910-919.Peeney, A. L. P., and Hawkins, C. F. (1953). Symptoms, signsand diagnostic features of iodopathic steatorrhoea. Quart. J.Med., 22, 59-77.
Cox, E. V., Meynell, M. J., Gaddie, R., and Cooke, W. T. (1959).Inter-relation of vitamin B1, and iron. Lancet, 2, 998.
Doig, A., and Girdwood, R. H. (1960). The absorption of folic acidand labelled cyanocobalamin in intestinal malabsorption.Quart. J. Med., n.s. 29, 333-374.
Fone, D. J., Cooke, W. T., Meynell, M. J., Brewer, D. B., Harris,E. L., and Cox, E. V. (1960). Jejunal biopsy in adult coeliacdisease and allied disorders. Lancet, 1, 933-939.,-, - P,and Cox, E. V. (1961). To be published.
Glass, G. B. Jerzy (1959). Deposition and storage of vitamin B,, inthe normal and diseased liver. Gastroenterology, 36, 180-192.Boyd, L. J., Gellin, G. A., and Stephanson, L. (1954). Uptakeof radioactive vitamin B,, by the liver in humans: test formeasurement of intestinal absorption of vitamin B1, andintrinsic factor activity. Arch. Biochem. Biophys., 51, 251-257.
, Speer, F. D., Nieburgs, H. E., Ishimori, A., Jones, E. L.,Baker, H., Schwartz, A., and Smith, R. (1960). Gastric atrophy,atrophic gastritis, and gastric secretory failure. Gastroenter-logy, 39, 429.
Heinle, R. W., Welch, A. P., Scharf, V., Meacham, G. C., andPrusoff, W. H. (1952). Studies of excretion (and absorption ofCo'° labelled vitamin B1, in pernicious anaemia). Trans. Ass.Amer. Phycns, 65, 214-222.
Jarvinen, K. A. J., and Latvalahti, J. (1958). Some observations onnon-tropical sprue: A case with hypocalcemia, intrinsic factordeficiency, anaemia and diabetes mellitus. Ann. Med. intern.Fenn., 47, 3946.
Loewenstein, F. (1958). Absorption of cobalt"° labelled vitamin B1,after sub-total gastrectomy. Blood, 13, 339-347.
MacLean, L. D. (1957). Incidence of megaloblastic anaemia aftersub-total gastrectomy. New Engl. J. Med., 257, 262-265.
Meynell, M. J., Cooke, W. T., Cox, E. V., and Gaddie, R. (1957).Serum cyanocobalamin level in chronic intestinal disorders.Lancet, 1, 901-904.
Mollin, D. L., Booth, C. C., and Baker, S. J. (1957). The absorptionof vitamin B,l in control subjects, in Addisonian perniciousanaemia and in the malabsorption syndrome. Brit. J. Haemat.,3, 412-428.
Oxenhorn, S., Estren, S., Wasserman, L. R., and Adlersberg, D. (1958).Malabsorption syndrome: intestinal absorption of vitamin B,,.Ann. intern. Med., 48, 30-38.
Schilling, R. F. (1953). Intrinsic factor studies. The effect of gastricjuice on the urinary excretion of radioactivity after the oraladministration of radioactive vitamin B,,. J. Lab. clin. Med.,42, 860-866.
Williams, A. W., Coghill, N. F., and Edwards, F. (1958). The gastricmucosa in pernicious anaemia: biopsy studies. Brit. J. Haemat.,4, 457-464.
on April 17, 2020 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.2.3.218 on 1 S
eptember 1961. D
ownloaded from