CME - Blog Tempo Cirurgia Plásticablog.tempocirurgiaplastica.com.br/wp-content/... · ipation in...
11
CME Breast Reduction Dennis C. Hammond, M.D. Michael Loffredo, M.D. Grand Rapids, Mich. Learning Objectives: After studying this article, the participant should be able to: 1. Understand the preoperative considerations that must be weighed to appropriately assess operative risk of breast reduction. 2. Have a full under- standing of the basic techniques that are available to treat the patient with macromastia. 3. Identify which patients are best suited to a particular technique. 4. Identify common complications associated with breast reduction and under- stand how to treat them. Summary: Breast reduction remains a basic plastic surgery procedure designed to alleviate upper torso complaints resulting from macromastia. Historically, the inverted-T inferior pedicle procedure was the dominant technique for the treatment of macromastia for 40 years. The past two decades have seen a reexamination of breast reduction technique in an attempt to improve on the results and minimize complications. As a result, a new genre of procedures based on different pedicles and short-scar skin management techniques has been introduced. With these new procedures, the plastic surgeon now has a variety of different techniques that can be offered for reducing the hypertrophic breast. Strategically applying the concepts inherent in these procedures to the correct patient can provide outstanding results with few complications. In this article, the concepts and results of these various procedures are discussed to give the reader a basic understanding of the options available for breast reduction. (Plast. Reconstr. Surg. 129: 829e, 2012.) PREOPERATIVE ASSESSMENT History F or any patient presenting for breast reduction, it must be remembered that a significant num- ber of women will develop breast cancer in their lifetimes. For this reason, one of the most im- portant preoperative issues to be clarified relates to the malignant potential of the breast. Although uncommon, occult breast cancer in the reduction specimen is occasionally detected. 1,2 For this rea- son, a breast history must be obtained, with special emphasis placed on the results of any previous open or percutaneous biopsies, whether any masses have been or are currently present, and when the last mammogram was obtained. A prac- tical rule of thumb regarding mammographic clearance of the breast would involve requiring such clearance for any patient older than 30 years, and lowering this threshold to 25 if there is a family history of breast cancer in any first-degree relative. For patients younger than 25 years, mam- mographic clearance would likely have such a low yield that its routine use would only rarely affect surgical planning regarding breast reduction. Other important information relates to the repro- ductive history of the patient and whether she was able to successfully breast-feed. If not, her desire to breast-feed in the future must be assessed, as breast reduction surgery can impact on this very personal choice. 3–5 Also, what effect pregnancy or weight gain had on breast size should be noted, as this can be a predictor of how the patient’s breast may change over time after the procedure if she should lose weight. This is a common concern of many patients, as they feel their breasts are a hin- From Partners in Plastic Surgery. Received for publication December 14, 2010; accepted June 29, 2011. Copyright ©2012 by the American Society of Plastic Surgeons DOI: 10.1097/PRS.0b013e31824a2efc Disclosure: The authors have no financial interest to declare in relation to the content of this article. Related Video content is available for this ar- ticle. The videos can be found under the “Re- lated Videos” section of the full-text article, or, for Ovid users, using the URL citations printed in the article. www.PRSJournal.com 829e
Transcript of CME - Blog Tempo Cirurgia Plásticablog.tempocirurgiaplastica.com.br/wp-content/... · ipation in...

CME
Breast ReductionDennis C. Hammond, M.D.
Michael Loffredo, M.D.
Grand Rapids, Mich.
Learning Objectives: After studying this article, the participant should be ableto: 1. Understand the preoperative considerations that must be weighed toappropriately assess operative risk of breast reduction. 2. Have a full under-standing of the basic techniques that are available to treat the patient withmacromastia. 3. Identify which patients are best suited to a particular technique.4. Identify common complications associated with breast reduction and under-stand how to treat them.Summary: Breast reduction remains a basic plastic surgery procedure designedto alleviate upper torso complaints resulting from macromastia. Historically, theinverted-T inferior pedicle procedure was the dominant technique for thetreatment of macromastia for 40 years. The past two decades have seen areexamination of breast reduction technique in an attempt to improve on theresults and minimize complications. As a result, a new genre of procedures basedon different pedicles and short-scar skin management techniques has beenintroduced. With these new procedures, the plastic surgeon now has a varietyof different techniques that can be offered for reducing the hypertrophic breast.Strategically applying the concepts inherent in these procedures to the correctpatient can provide outstanding results with few complications. In this article,the concepts and results of these various procedures are discussed to givethe reader a basic understanding of the options available for breastreduction. (Plast. Reconstr. Surg. 129: 829e, 2012.)
PREOPERATIVE ASSESSMENT
History
For any patient presenting for breast reduction,it must be remembered that a significant num-ber of women will develop breast cancer in
their lifetimes. For this reason, one of the most im-portant preoperative issues to be clarified relates tothe malignant potential of the breast. Althoughuncommon, occult breast cancer in the reductionspecimen is occasionally detected.1,2 For this rea-son, a breast history must be obtained, with specialemphasis placed on the results of any previousopen or percutaneous biopsies, whether anymasses have been or are currently present, andwhen the last mammogram was obtained. A prac-tical rule of thumb regarding mammographicclearance of the breast would involve requiringsuch clearance for any patient older than 30 years,and lowering this threshold to 25 if there is afamily history of breast cancer in any first-degreerelative. For patients younger than 25 years, mam-
mographic clearance would likely have such a lowyield that its routine use would only rarely affectsurgical planning regarding breast reduction.Other important information relates to the repro-ductive history of the patient and whether she wasable to successfully breast-feed. If not, her desireto breast-feed in the future must be assessed, asbreast reduction surgery can impact on this verypersonal choice.3–5 Also, what effect pregnancy orweight gain had on breast size should be noted, asthis can be a predictor of how the patient’s breastmay change over time after the procedure if sheshould lose weight. This is a common concern ofmany patients, as they feel their breasts are a hin-
From Partners in Plastic Surgery.Received for publication December 14, 2010; accepted June29, 2011.Copyright ©2012 by the American Society of Plastic Surgeons
DOI: 10.1097/PRS.0b013e31824a2efc
Disclosure: The authors have no financial interestto declare in relation to the content of this article.
Related Video content is available for this ar-ticle. The videos can be found under the “Re-lated Videos” section of the full-text article, or,for Ovid users, using the URL citationsprinted in the article.
www.PRSJournal.com 829e

drance to properly exercising, and many plan tolose weight after the procedure. Basic informationregarding general health status and medicationscan identify the need for preoperative physiologicoptimization with the help of the patient’s primarycare provider. Perhaps most importantly, whetheror not the patient is a current or previous smokermust be documented. A smoking history will dou-ble the risk for developing a postoperative com-plication, and strategies designed to reduce thisrisk may be implemented, including cessation ofsmoking and alteration of technique, with per-haps a less aggressive dissection being performed.6Also, the presence of common symptoms relatedto strain on the upper torso attributable to theweight of the breasts must be documented. Thesesymptoms can include headaches, neck pain, backpain, submammary intertrigo (particularly duringthe warmer months), painful bra strap marks withgrooving and possible associated ulnar paresthe-sias caused by pressure on the brachial plexus,breast pain, difficulty wearing clothing that fitsproportionately, and emotional sequelae (partic-ularly in younger girls). This latter issue is impor-tant to identify in an adolescent patient, as peerpressure or even ridicule related to breast size canhinder social development at this very importanttime in her life. For this reason alone, breast re-duction surgery can be justified in affected pa-tients. Finally, the patient should provide someguidance as to what size breast she was hoping tohave after the procedure. Inappropriate expecta-tions are best dealt with before surgery, as dealingwith them postoperatively can be decidedly un-satisfying and unsuccessful.
Physical ExaminationThe patient is best examined in the standing
position, with the arms comfortably at the sides.Any asymmetries in the size of the breasts, theposition of the nipple-areola complex, and thelevel of the inframammary fold are noted. Mea-surements from the mid clavicle or the sternalnotch down to the nipple are obtained, and thedistance from the inframammary fold up to thenipple is noted. The latter measurement is impor-tant, as it serves as an indicator of the length of thepedicle when an inferior pedicle technique isused. The breast is palpated to assess for any po-tential masses, and the density of the parenchymais noted. This is a useful observation to make, asdense fibrous breasts that are often seen inyounger women are difficult to dissect, and thetissue remaining after resection often does not
mold together as smoothly as a breast with agreater fat content. Finally, an assessment is madeas to the estimated amount of breast tissue that willbe removed from each side. Accuracy in this de-termination is helpful in streamlining the insur-ance preauthorization status. It is also a skill thatimproves with experience.
Photographic DocumentationPhotographic documentation of the patient’s
preoperative appearance is a vital part of the pre-operative consultation. It is an important part ofthe patient’s record that can provide perspectiveif any complications or aesthetic concerns arisepostoperatively. Three views of the breast docu-menting the appearance of the breast from thefront and from each side adequately serve to re-cord the patient’s preoperative condition. Sup-plemental views, including a three-quarters view, ahands-over-head view, and a photograph with thehands lifting the breast to allow the level of theinframammary fold to be seen, can be included forfurther documentation as needed. Framing thepatient from the neck down to just below the levelof the breasts with the width extending from justoutside each arm will allow the shape, size, andposition of the breast to be visualized and yet allowperspective with regard to the rest of the torso tobe seen. As with all breast surgery, at no time is itnecessary or desirable to include the patient’s facein the photograph.
Insurance IssuesAlthough breast reduction can occasionally be
performed as a self-pay procedure, in the vast ma-jority of instances, some type of insurance is usedto pay for or help defray the costs associated withbreast reduction. As such, many insurance planshave developed a preauthorization process de-signed to assess the severity of the patient’s con-dition and determine whether or not breast re-duction would then be indicated. A commonthread that applies to many insurance plans re-lates to documentation of the functional symp-toms noted previously. Also, many plans will re-quire what are called “conservative” measures toalleviate the patient’s symptoms, including partic-ipation in physical therapy or chiropractic ther-apy, and a trial of specially fitted support gar-ments. Medical relief of symptoms with a trial oforal analgesics and/or antiinflammatory drugs isalso commonly required. Once these preliminaryadministrative details have been documented, anestimate as to the weight of tissue to be removed
Plastic and Reconstructive Surgery • May 2012
830e

is made based on the surgeon’s previous experi-ence. Typically at this point, a chart is then con-sulted that references the height and weight ofthe patient, and either the body surface area or thebody mass index is calculated. By adding in thepatient’s measurements, a minimum amount oftissue that must be removed to qualify for insur-ance coverage can then be determined. If therequirements for the symptom complex have beenmet along with the required (estimated) amountfor removal, the procedure can be considered acovered benefit. Some plans offer automatic cov-erage at this point; others still require a formalletter of preauthorization. Regardless of the de-tails, it is recommended in every circumstance todocument the patient’s symptom complex thor-oughly and make the best estimate for tissue re-moval that can be made. This information canprove very useful during the procedure to ensurenot only adequate reduction of the breast but alsoenhanced symmetry in cases of marked breast vol-ume asymmetry.
OPERATIVE STRATEGYAny procedure designed to reduce the breast
must include four cardinal elements. First, a pedi-cle must be incorporated into the design that pre-serves the vascularity and innervation to the nip-ple-areola complex. Second, and closely related topedicle choice, selected quadrants of the breastmust be removed to accomplish the desired vol-ume reduction. This is commonly accomplishedby removing tissue from around the perimeter ofthe pedicle. Third, the excessive skin envelopemust be managed in such a way as to minimizescarring as much as possible and yet allow a pro-portional relationship to be created between theremaining skin and the reduced breast volume.Fourth, an overall aesthetic breast shape must becreated either as a function of the overall op-erative strategy or secondary to defined maneu-vers designed to create a specific contour. Anyprocedure designed to reduce the breast willinclude these four elements, and analyzingthese various and sometimes diverse proceduresin this fashion will facilitate a greater under-standing of each.
Inverted-T Inferior Pedicle
Pedicle: inferiorVolume reduction: medial, superior, and lateralSkin pattern: inverted TShape: passive
The inverted-T inferior pedicle has been thepreferred method of breast reduction around theworld over the past 40 years, and it has clearlystood the test of time.7–10 The blood supply is basedon an inferior pedicle, with the redundant tissuebeing removed from around the upper hemi-sphere of the pedicle. The excess skin is removedfrom the lower pole of the breast, including aV-shaped central vertical segment. The resultingscar is that of an inverted T or anchor shape. Thishas been also commonly referred to as a Wisepattern. Shape is created passively simply as a re-sult of the wrapping of the skin flaps around theinferior pedicle that then settles under the influ-ence of gravity. (See Video, Supplemental DigitalContent 1, which highlights the marks and tech-nical features of a standard inferior pedicle in-verted-T or Wise pattern breast reduction, avail-able in the “Related Videos” section of the full-textarticle on PRSJournal.com or, for Ovid users, athttp://links.lww.com/PRS/A485.)
The main advantage of the inverted-T inferiorpedicle technique is that it can be applied in anycircumstance, from simple mastopexy to reduc-tion for gigantomastia (Fig. 1). There is no de-fined upper limit related to volume for this tech-nique. In extreme instances, the pedicle could beof such length that it outstrips the blood supply.In these circumstances, it is a simple matter toremove the nipple-areola complex, trim the pedi-cle back to a level of viability, and apply the nipple-areola complex as a skin graft. In contrast to this
Video 1. Supplemental Digital Content 1, which highlights themarks and technical features of a standard inferior pedicle invert-ed-T or Wise pattern breast reduction, is available in the “RelatedVideos” section of the full-text article on PRSJournal.com or, forOvid users, at http://links.lww.com/PRS/A485.
Volume 129, Number 5 • Breast Reduction
831e

approach of using the nipple-areola complex grafttechnique only when ischemia to the nipple-are-ola complex is identified intraoperatively, somesurgeons use this free nipple graft technique as aplanned procedure for larger breast reductionsdeemed to be over a specific amount.11–13 Com-monly used guidelines for using the free nipple-areola complex graft technique include reduc-tions of over 1500 g from each side.
Although the inverted-T inferior pedicle tech-nique does enjoy widespread popularity, there areseveral significant drawbacks. The scar burden isextensive, particularly along the inframammaryfold. For smaller breast reductions or younger pa-tients, this scar burden can be a significant detri-ment. However, an even greater problem relatesto the change in shape that can occur over time.This phenomenon, called bottoming-out, variablyoccurs in many patients who undergo reductionusing this technique. When it occurs to excess, theaesthetics of the result can be severely compro-mised. For this reason, some surgeons have ad-
opted a strategy of using this technique for largerbreast reductions only because of its familiarityand overall track record of success. For smallerbreast reductions, one of the other short-scar tech-niques can be used.
Vertical Mammaplasty with Superior Pedicle
Pedicle: superiorVolume reduction: inferiorSkin pattern: circumverticalShape: passive
When considering the history of the verticalmammaplasty, the contribution of Claude Lassusmerits particular emphasis, as it was he who de-veloped the strategic elements of the modern op-eration that have been variably modified overtime.14–16 Also, the work of Madeleine Lejour isimportant, as it was she who brought the verticalmammaplasty concept into the mainstream ofplastic surgery.17,18 The traditional vertical proce-dure bases the blood supply to the nipple-areola
Fig. 1. (Above, left) Preoperative appearance of a 36-year-old woman in preparation for breast reduction using an inverted-Tinferior pedicle approach. (Above, right) Preoperative marks. (Below, left) Intraoperative appearance after removal of the excessbreast tissue and placement of the inferior/central pedicle into position. (Below, right) Appearance 1 year after removal of 600 gof tissue from the right breast and 650 g of tissue from the left.
Plastic and Reconstructive Surgery • May 2012
832e

complex on a superior pedicle and removes pa-renchyma from the inferior pole of the breast. Amodified circumvertical skin pattern is used thatdirectly matches up the incision length of the are-ola with the dimensions of the periareolar inci-sion. The bulk of the excessive skin envelope re-section is then taken up by the vertical segmentthat then runs straight down to the inframammaryfold. A modified version of this procedure hasbeen described by Hall-Findlay19,20 that bases thepedicle in a slightly more medial direction to easethe subsequent transposition of the nipple-areolacomplex into the periareolar defect. (See Video,Supplemental Digital Content 2, a narrated videopresented by Dr. Frank Lista that outlines themarks and technical features of a vertical mam-maplasty, available in the “Related Videos” sectionof the full-text article on PRSJournal.com or, forOvid users, at http://links.lww.com/PRS/A486.)
Despite what can be a distorted initial appear-ance, the final result for the majority of patients isquite aesthetic. The advantages of the procedureinclude rapid operative times and a reducedcutaneous scar burden with a pleasing overallbreast shape. For these reasons, the verticalmammaplasty is the most commonly used short-scar reduction technique currently in use.21
However, in many cases and particularly inlarger reductions, wound healing difficultiesand suboptimal scarring along the vertical seg-ment and at the level of the inframammary foldcan occur, resulting in shape distortion and the
need for subsequent revision.22,23 For these rea-sons, many surgeons limit the vertical mamma-plasty approach to smaller breast reductions of500 g or less (Fig. 2).
Video 2. Supplemental Digital Content 2, a narrated video pre-sented by Dr. Frank Lista that outlines the marks and technicalfeatures of a vertical mammaplasty, is available in the “RelatedVideos” section of the full-text article on PRSJournal.com or, forOvid users, at http://links.lww.com/PRS/A486.
Fig. 2. (Above) Preoperative appearance of a 48-year-old womanbefore breast reduction using a vertical mammaplasty approach.(Center) Preoperative marks. (Below) Appearance 3 years after theremoval of 98 g of tissue from the right breast and 120 g of tissuefromtheleft. [ReprintedwithpermissionfromHammondDC.Breastreduction. In: Hodgson S, ed. Atlas of Aesthetic Breast Surgery. Phila-delphia: Saunders Elsevier; 2009:155, 161, 162.]
Volume 129, Number 5 • Breast Reduction
833e

Short-Scar Periareolar Inferior Pedicle
Pedicle: inferiorVolume reduction: medial, superior, and lateralSkin pattern: circumverticalShape: active/passive
In an attempt to solve some of the problemsassociated with the vertical mammaplasty, theshort-scar periareolar inferior pedicle reduction(SPAIR) mammaplasty was developed.24–26 Thisprocedure bases the blood supply to the nipple-areola complex on an inferior pedicle and re-moves tissue from around the pedicle as in theinverted-T approach. The excessive skin envelopeis managed using a true circumvertical pattern,where the periareolar incision is larger than theareolar incision and the inferior end of the verticalsegment courses laterally along the fold as neededto effectively reduce the skin envelope of thebreast. Intraoperative shaping is performed asneeded only in selected patients by suture plicat-ing the upper pole to create upper pole fullness.(See Video, Supplemental Digital Content 3,which describes the marks and technical steps in-volved when performing the short-scar periareolarinferior pedicle reduction mammaplasty, avail-able in the “Related Videos” section of the full-textarticle on PRSJournal.com or, for Ovid users, athttp://links.lww.com/PRS/A487.)
One of the main advantages associated withthe short-scar periareolar inferior pedicle reduc-tion mammaplasty is that most surgeons are al-
ready familiar with the inferior pedicle; therefore,it affords an opportunity to apply a short-scar tech-nique without the need to use an unfamiliar pedi-cle as the basis for the procedure. It is a techniquethat is widely applicable for many patients, rangingfrom mastopexy and small reductions to largerreductions of 1500 g per side and more. The abilityto perform larger reductions safely relates to theincreased effectiveness of the true circumverticalpattern to reduce the excessive skin envelope. Theresults using the short-scar periareolar inferiorpedicle reduction mammaplasty are similar tothose obtained using a vertical approach. By in-corporating a vertical component into the skinpattern, the projection of the breast is enhancedand a more rounded shape is created that avoidsthe “boxy” appearance that can sometimes be seenwith the inverted-T method. Also, by canting thevertical skin removal laterally along the fold, theexcessive skin envelope can be effectively reducedin a manner that eliminates all of the complica-tions associated with the vertical scar and infra-mammary fold that are seen in the vertical mam-maplasty. Finally, because the attachments of theinframammary fold are left completely intact,there is no inordinate postoperative migration ofthe breast inferiorly, and the tendency for thebreast to bottom out is greatly minimized. There-fore, the shape seen intraoperatively is largely theshape that will be maintained during the postop-erative recovery. This allows accurate intraopera-tive adjustments to be made as needed to optimizethe aesthetic result (Fig. 3).
One technical aspect related to the use of theshort-scar periareolar inferior pedicle reductionmammaplasty is that the internal breast septum canbe easily identified and preserved. Recent anatom-ical descriptions of an internal breast septum run-ning transversely across the lower pole of the breasthave enhanced our understanding of inferior pedi-cle blood supply.27–29 Preserving the caudal leaf ofthis septum avoids injuring the direct perforatorsrunning from the muscle up to the nipple-areolacomplex within the septum. Identifying and preserv-ing this septum allows pedicles of impressive lengthto be used safely. (See Video, Supplemental DigitalContent 4, which presents the anatomical landmarksthat describe the internal breast septum, available inthe “Related Videos” section of the full-text article onPRSJournal.com or, for Ovid users, at http://links.lww.com/PRS/A488.)
The disadvantages associated with the short-scar periareolar inferior pedicle reduction mam-maplasty include the fact that it is a technicallydemanding procedure. Accurate flap dissection is
Video 3. Supplemental Digital Content 3, which describes themarks and technical steps involved when performing the short-scarperiareolar inferior pedicle reduction mammaplasty, is available inthe “Related Videos” section of the full-text article on PRSJournal.com or, for Ovid users, at http://links.lww.com/PRS/A487.
Plastic and Reconstructive Surgery • May 2012
834e

required, and skin envelope tailoring with the in-traoperative application of the circumvertical pat-tern is an acquired skill. Also, in larger reductions,the periareolar defect can be so large as to com-promise the appearance of the periareolar scarand the shape of the areola.
Liposuction Breast Reduction
Pedicle: centralVolume reduction: all quadrants
Skin pattern: not applicableShape: passive
Reducing the breast with liposuction alone of-fers the obvious advantage of relieving upper torsocomplaints without creating any significant cutane-ous scar. Volume reduction, although problematicin breasts that are particularly fibrous in nature, isusually easily performed and can effectively re-duce the fatty content of the breast simply andefficiently.30–33 Standard tumescent technique
Fig. 3. (Left) Preoperative appearance of a 58-year-old woman in preparation for breast reduction using the short-scar periareolarinferior pedicle reduction approach. (Below) Preoperative marks. (Right) Appearance at 7 months after the removal of 436 g of tissuefrom the right breast and 645 g of tissue from the left.
Volume 129, Number 5 • Breast Reduction
835e
coupled with any of the various techniques forliposuction can be applied without difficulty. How-ever, although symptom relief is certainly realized,any opportunity to reshape the breast or changethe position of the nipple-areola complex in re-lation to the breast mound is lost. Also, this ap-proach basically negates any practical opportunityto evaluate the breast parenchyma histologically,which can be an important issue for selectedpatients.
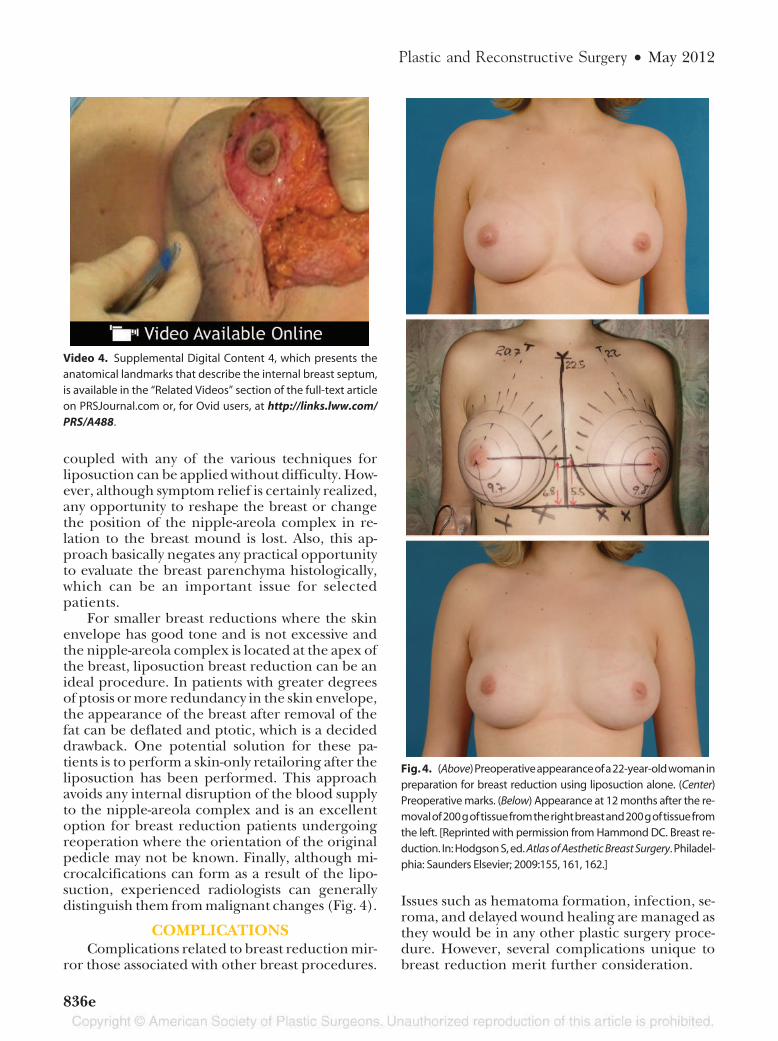
For smaller breast reductions where the skinenvelope has good tone and is not excessive andthe nipple-areola complex is located at the apex ofthe breast, liposuction breast reduction can be anideal procedure. In patients with greater degreesof ptosis or more redundancy in the skin envelope,the appearance of the breast after removal of thefat can be deflated and ptotic, which is a decideddrawback. One potential solution for these pa-tients is to perform a skin-only retailoring after theliposuction has been performed. This approachavoids any internal disruption of the blood supplyto the nipple-areola complex and is an excellentoption for breast reduction patients undergoingreoperation where the orientation of the originalpedicle may not be known. Finally, although mi-crocalcifications can form as a result of the lipo-suction, experienced radiologists can generallydistinguish them from malignant changes (Fig. 4).
COMPLICATIONSComplications related to breast reduction mir-
ror those associated with other breast procedures.
Issues such as hematoma formation, infection, se-roma, and delayed wound healing are managed asthey would be in any other plastic surgery proce-dure. However, several complications unique tobreast reduction merit further consideration.
Video 4. Supplemental Digital Content 4, which presents theanatomical landmarks that describe the internal breast septum,is available in the “Related Videos” section of the full-text articleon PRSJournal.com or, for Ovid users, at http://links.lww.com/PRS/A488.
Fig. 4. (Above)Preoperativeappearanceofa22-year-oldwomaninpreparation for breast reduction using liposuction alone. (Center)Preoperative marks. (Below) Appearance at 12 months after the re-movalof200goftissuefromtherightbreastand200goftissuefromthe left. [Reprinted with permission from Hammond DC. Breast re-duction. In: Hodgson S, ed. Atlas of Aesthetic Breast Surgery. Philadel-phia: Saunders Elsevier; 2009:155, 161, 162.]
Plastic and Reconstructive Surgery • May 2012
836e

Nipple-Areola Complex NecrosisPartial or complete loss of any portion of the
nipple or areola is perhaps the most significantpotential complication associated with breast re-duction. When this occurs, it is often accompaniedby an area of fat necrosis located in the distal end
of the pedicle. Areas of necrotic fat present asdiscrete masses that are fully mature by approxi-mately 6 months postoperatively, and simple ex-cisional biopsy effectively removes the area of con-cern. Of course, the best treatment remainsavoidance by intelligently designing pedicles, pre-
Fig. 5. (Left) Preoperative appearance of a 36-year-old woman who had previously undergone a vertical mammaplasty. She pre-sented with redundancy and shape distortion along the inframammary fold. (Below) Preoperative marks demonstrate revision usingthe circumvertical pattern. (Right) Postoperative appearance shows resolution of the distortion along the inferior pole of the breastand improved aesthetics of the nipple-areola complex.
Volume 129, Number 5 • Breast Reduction
837e

serving the internal breast septum, and avoidingexcessive postoperative compression of the breast.In complicated cases such as patients who presentfor repeated reduction or have a previous historyof breast irradiation, limited undermining andwider pedicle width may help limit the potentialfor ischemia and possible necrosis. When ischemiais recognized, prompt conversion to a free nipplegraft technique can preserve an acceptable result;however, recognizing the severity of the ischemiaand deciding when to act requires thoughtfuljudgment guided by experience. Once the imme-diate changes after surgery related to cooling andepinephrine effect have subsided, the decision toproceed with removal of the ischemic nipple-are-ola complex and reapplication as a free graft canbe made. In the event of complete or partial lossof the nipple-areola complex, conservative woundmanagement with debridement and secondaryhealing are indicated followed by standard tech-niques of nipple-areola complex reconstruction,although scarring can compromise the ability tocreate a nipple of adequate projection.
ScarringExcessive or hypertrophic scarring is perhaps
one of the most potentially distressing aspects ofbreast reduction, particularly for patients under-going an inverted-T type of procedure. Once theearly postoperative scars have settled, usually 6months to 1 year postoperatively, simple scar re-vision can result in an improved appearance. Thisis because the forces on the scars stabilize overtime as the breast accommodates to its new sizeand shape. Simple revision can then greatly im-prove the appearance of the scars.
Shape ChangePostoperatively, it is very common for the skin
envelope to settle and stretch under the weight ofthe remaining breast. Also, when the attachmentsof the inframammary fold are released, the breastcan migrate below the fold, creating a new pas-sively formed fold that is positioned anywherefrom 1 to 3 cm below the inframammary fold scar.Considered together, these two changes describe
the phenomenon of bottoming-out. Treatment isdirected at tightening the skin envelope and re-pairing the fold to restore a normal breast shape(Fig. 5).
SUMMARYBreast reduction provides the plastic surgeon
with a unique opportunity to alleviate the uppertorso complaints of women affected by macromas-tia and yet incorporate strategic application ofsurgical principles to reshape and lift the breast tocreate aesthetically pleasing results. Although theinverted-T inferior pedicle technique remains thecriterion standard against which all other tech-niques are judged, recent descriptions of short-scar operations have revolutionized the treatmentof macromastia, resulting in improved shapes withless scarring. Complications are few and relief ofsymptoms is nearly universal. It remains up to theindividual surgeon to artistically apply these tech-niques to the best advantage to create the mostaesthetic results possible.
See Table 1 for Current Procedural Terminologycodes commonly used in breast reduction surgery.
Dennis C. Hammond, M.D.Partners in Plastic Surgery, Suite 202
4070 Lake Drive SEGrand Rapids, Mich. 49546
ACKNOWLEDGMENTThe authors gratefully acknowledge the contribution
of Frank Lista, M.D., who kindly provided the narratedvideo footage of the vertical mammaplasty included withthis article.
REFERENCES1. Brown MH, Weinberg M, Chong N, Levine R, Holowaty E. A
cohort study of breast cancer risk in breast reduction pa-tients. Plast Reconstr Surg. 1999;103:1674–1681.
2. Colwell AS, Kukreja J, Breuing KH, Lester S, Orgill DP.Occult breast carcinoma in reduction mammaplasty speci-mens: 14-year experience. Plast Reconstr Surg. 2004;113:1984–1988.
3. Harris L, Morris SF, Freiberg A. Is breast feeding possibleafter reduction mammaplasty? Plast Reconstr Surg. 1992;89:836–839.
4. Brzozowski D, Niessen M, Evans HB, Hurst LN. Breast feed-ing after inferior pedicle reduction mammaplasty. Plast Re-constr Surg. 2000;105:530–534.
5. Souto GC, Giugliani ER, Giugliani C, Schneider MA. Theimpact of breast reduction surgery on breastfeeding perfor-mance. J Hum Lact. 2003;19:43–49.
6. Bartsch RH, Weiss G, Kastenbauer T, et al. Crucial aspects ofsmoking in wound healing after breast reduction surgery.J Plast Reconstr Aesthet Surg. 2007;60:1045–1049.
7. Wise RJ, Gannon JP, Hill JR. Further experience with reduc-tion mammoplasty. Plast Reconstr Surg. 1963;32:12–20.
Table 1. CPT Codes Commonly Used in BreastReduction Surgery
CPT Code Descriptor
19318 Reduction mammaplasty15788 Suction-assisted lipectomy, trunkThis information prepared by Dr. Raymond Janevicius is intended toprovide coding guidance.
Plastic and Reconstructive Surgery • May 2012
838e

8. Wise RJ. A preliminary report on a method of planning themammaplasty. Plast Reconstr Surg. 1956;17:367–375.
9. Courtiss EH, Goldwyn RM. Reduction mammaplasty by theinferior pedicle technique: An alternative to free nipple andareola grafting for severe macromastia or extreme ptosis.Plast Reconstr Surg. 1977;59:500–507.
10. Georgiade NG, Serafin D, Morris R, Georgiade G. Reductionmammaplasty utilizing an inferior pedicle nipple-areolarflap. Ann Plast Surg. 1979;3:211–218.
11. Adams WM. Free transplantation of the nipples and areolae.Surgery 1944;5:186–195.
12. Gradinger GP. Reduction mammoplasty utilizing nipple-are-ola transplantation. Clin Plast Surg. 1988;19:641–654.
13. Karsidag S, Akcal A, Karsidag T, Yesiloglu N, Yesilada AK,Ugurlu K. Reduction mammaplasty using the free-nipple-graft vertical technique for severe breast hypertrophy: Im-proved outcomes with the superior dermaglandular flap.Aesthetic Plast Surg. 2011;35:254–261.
14. Lassus C. A technique for breast reduction. Int Surg. 1970;53:69–72.
15. Lassus C. Breast reduction: Evolution of a technique. A singlevertical scar. Aesthetic Plast Surg. 1987;11:107–112.
16. Lassus C. A 30-year experience with vertical mammaplasty.Plast Reconstr Surg. 1996;97:373–380.
17. Lejour M. Vertical mammaplasty and liposuction of thebreast. Plast Reconstr Surg. 1994;94:100–114.
18. Lejour M. Vertical mammaplasty: Early complications after250 personal consecutive cases. Plast Reconstr Surg. 1999;104:764–770.
19. Hall-Findlay EJ. A simplified vertical reduction mammaplas-ty: Shortening the learning curve. Plast Reconstr Surg. 1999;104:748–759; discussion 760–763.
20. Hall-Findlay EJ. Vertical breast reduction with a mediallybased pedicle. Aesthet Surg J. 2002;22:185–194.
21. Lista F, Ahmad J. Vertical scar reduction mammaplasty: A15-year experience including a review of 250 consecutive
cases. Plast Reconstr Surg. 2006;117:2152–2165; discussion2166–2169.
22. Berthe JV, Massaut J, Greuse M, Coessens B, De May A. Thevertical mammaplasty: A reappraisal of the technique and itscomplications. Plast Reconstr Surg. 2003;111:2192–2199; dis-cussion 2200–2202.
23. Adham M, Sawan K, Lovelace C, Jaeger NJ, Adham C. Un-favorable outcomes with vertical reduction mammaplasty:Part II. Aesthet Surg J. 2011;31:40–46.
24. Hammond DC. Short scar periareolar inferior pedicle re-duction (SPAIR) mammaplasty. Plast Reconstr Surg. 1999;103:890–901; discussion 902.
25. Hammond DC. The SPAIR mammaplasty. Clin Plast Surg.2002;29:411–421.
26. Hammond DC, Alfonso D, Khuthaila DK. Mastopexy usingthe short scar periareolar inferior pedicle reduction tech-nique. Plast Reconstr Surg. 2008;121:1533–1539.
27. Wuringer E, Mader N, Posch E, Holle J. Nerve and vesselsupplying ligamentous suspension of the mammary gland.Plast Reconstr Surg. 1998;101:1486–1493.
28. Wuringer E. Refinement of the central pedicle breast reduc-tion by application of the ligamentous suspension. Plast Re-constr Surg. 1999;103:1400–1410.
29. Wueringer E, Tschabitscher M. New aspects of the topo-graphical anatomy of the mammary gland regarding its neu-rovascular supply along a regular ligamentous suspension.Eur J Morphol. 2002;40:181–189.
30. Teimourian B, Massac E Jr, Wiegering CE. Reduction suctionmammaplasty and suction lipectomy as an adjunct to breastsurgery. Aesthetic Plast Surg. 1985;9:97–100.
31. Matarasso A, Courtiss EH. Suction mammaplasty: The use ofsuction lipectomy to reduce large breasts. Plast Reconstr Surg.1991;87:709–717.
32. Courtiss EH. Reduction mammaplasty by suction alone. PlastReconstr Surg. 1993;92:1276–1284; discussion 1285–1289.
33. Moskovitz MJ, Baxt SA. Breast reduction using liposuctionalone. Semin Plast Surg. 2004;18:225–229.
Volume 129, Number 5 • Breast Reduction
839e