CMDR Monograph Series No. - 51cmdr.ac.in/editor_v51/assets/mono-51.pdf6 CMDR Monograph Series No. -...
21
PEOPLE’S PARTICIPATION IN HEALTH CARE DELIVERY :AN APPRAISAL OF ACTION RESEARCH 1 CMDR Monograph Series No. - 51 PEOPLE’S PARTICIPATION IN HEALTH CARE DELIVERY : AN APPRAISAL OF ACTION RESEARCH Dr. V. B. Annigeri CENTRE FOR MULTI-DISCIPLINARY DEVELOPMENT RESEARCH Jubilee Circle, DHARWAD-580001, Karnataka, India Ph : 091-0836-2447639, Fax : 2447627 E-mail : [email protected]
Transcript of CMDR Monograph Series No. - 51cmdr.ac.in/editor_v51/assets/mono-51.pdf6 CMDR Monograph Series No. -...

PEOPLE’S PARTICIPATION IN HEALTH CARE DELIVERY :AN APPRAISAL OF ACTION RESEARCH 1
CMDR Monograph Series No. - 51
PEOPLE’S PARTICIPATION IN HEALTH CAREDELIVERY :
AN APPRAISAL OF ACTION RESEARCH
Dr. V. B. Annigeri
CENTRE FOR MULTI-DISCIPLINARY DEVELOPMENT RESEARCHJubilee Circle, DHARWAD-580001, Karnataka, India
Ph : 091-0836-2447639, Fax : 2447627E-mail : [email protected]

2 CMDR Monograph Series No. - 51
PEOPLE’S PARTICIPATION IN HEALTH CARE DELIVERY :AN APPRAISAL OF ACTION RESEARCH
Vinod B. Annigeri
The aim of the present studyconducted by the CMDR is to examine theeffects of economic reforms on the healthsector in India. The study has an actionintervention component, which aims tostrengthen the delivery of primary health carethrough the Primary Health Center (PHC)network.1
As India is a signatory to the AlmaAta declaration, we were required to achievethe goal of Health for All (HFA) by 2000A.D. It is obvious that we have not beenable to achieve this goal as enumerated inthe health policy document for variousindicators. In the wake of economic reforms,there seems to be a compression ofbudgetary resources in general, which hasreduced the share of resources for the socialsector in general and more so for the healthsector. Shrinking resources have theirimpact on the health delivery system. Fewresearch studies have documented this in theIndian context.
Methodology:
As part of our ongoing study, we collectedthe household level information in the three
selected states of Maharashtra, Orissa andKarnataka through the help of structuredquestionnaire. We tried to elicit informationregarding the socio-economic status ofhouseholds, morbidity and nutritionalprofiles, utilization pattern and the risk factorsaffecting the health status of the population.Along with this we also tried to collectqualitative information on the perceivedstatus of the community with regard to thehealth delivery system especially in thereforms period. The results from the dataindicate that, the delivery of health servicesthrough public institutions have developedcertain bottlenecks, which have resulted inlower levels of utilization by the community.Secondly, the aspirations of the communitywith regard to the public health careinstitutions are many and the present set-upis unable to meet the growing demand. Sucha situation might have been created due toinadequacy with regard to manpowersupplied as well as other inputs at the PHClevel.
Our data also reveals that, privatepractitioners are exploiting the communityunder the nose of public health careinstitutions. Sometimes as public health

PEOPLE’S PARTICIPATION IN HEALTH CARE DELIVERY :AN APPRAISAL OF ACTION RESEARCH 3
personnel are not available in the villages,the private practitioners (who are usuallyquacks) charge heavy fees from the patients.Poor people who do not have any optionsare forced to visit such private clinics. But atthe same time we cannot afford to pass onthe blame to the public system, which is tryinghonestly to cope up with the increasedresponsibilities on the one hand and decliningbudgetary support on the other.
Rationale for Intervention:
Given this background we need toevolve new mechanisms of health caredelivery which would strengthen the publichealth delivery system. Communityinvolvement and participation in the provisionof health care services is not a new ideaaltogether. We can note that there areinnumerable experiences both within andoutside India, which have demonstrated thatcommunity participation is an effectiveresource in the provision of health careservices.
The need for such a participation inthe present day context arises firstly due toinadequate manpower at the PHC level,which seems to be over burdened. Themedical officer at the PHC is finding it hardto manage his time due to his involvement in14 programmes / schemes. Thus, patientsfind it difficult to meet him whenever theyvisit the PHC. One may ask for additionaldoctor at the PHC, but in view of changingbudgetary allocations, this may not befeasible.
Secondly, we also now observe thatmany state governments are willing toexperiment using innovative methods toimprove the situation with regard to the healthdelivery system. Recently the government ofKarnataka has announced the introductionof Rogi Kalyan Samiti (RKS) based on theexperiment of Madhya Pradesh. It needs tobe noted here that RKS is quite a novel ideain managing the public health institutions. Butthe RKS of M.P. does not go below the levelof Community Health Centers (CHCs),which means that it caters to referral ratherthan primary care. We need to experimentnew methods of strengthening the publichealth delivery system at the primary healthlevel also.
Based on the lessons of anexperiment in Karnataka involvingparticipation of Non GovernmentOrganisations (NGOs) in the delivery ofhealth care services ( Report of DeccanHerald dated 4th May 14, 2002) the Centralgovernment has made changes in the healthpolicy document 2002. The policy documentclearly encourages NGO participation in thedelivery of health services through publicoutlets.
In this background CMDR has triedto evolve an intervention package tosupplement and strengthen the public healthdelivery system. The broad objectives of thispackage are:

4 CMDR Monograph Series No. - 51
Community should actively participate inthe provision of health care services
Delivery of health care services shouldbe more community friendly
Try to inject built in mechanisms in thepackage to make it sustainable, after theinitial doses of supplements
The envisaged intervention package isoutlined as below.
CMDR would create Primary Health
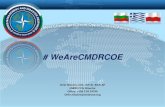
T h e fo llo w in g c h a r t w o u l d d e p ic t th e fo rm a tio n o f P H M G a n d i ts re sp o n s ib il i t ie s .
T h e P r im a ry H e a lth M a n a g e m e n t G ro u p (P H M G )
is b a s e d o n th e m o d e l o f F a m ily P ra c tic e G ro up
a sso c ia tio n s (F P G A s ) a s e x p e r i m e n te d in
K a z a k h sta n a n d K yrg yz sta n .
F o rm atio n o f P r im ar y
H e a lth M a n ag e m e n t
G r o u p (P H M G s )
D istr ic t
H e a lth
O f fic ia ls M O & O th e r S taf f o f P H C s
L o ca l T e a c h in g In s tit u tio n in M ed ic in e
N G O s in th e R e g io n
In te rve n tio n
b y P H M G
C M D R V IL L A G E P A N C H A Y A T
P urc ha sin g & M a n a g in g th e H e a lth In s u ra n c e fo r th e b e n e f it o f th e M e m b e r H H s b a se d o n S E W A m o d e l
S u p p ly o f a d d itio na l D o c to r
S u p p ly o f E q u ip m e nts
S up p ly o f n o n P H C d ru g s
T o o v e rse e th e fre e d ru g S u p p l y
fro m P H C
In s u ra n c e c o m p a n ie s to b e
in vo lv e d
D H O /M O o f P H C a n d o th e r P ro g ra m m e O ffic e r s in g o v t. se tu p to b e c o n s u lte d
T o b e a rra ng e d in c o n s u lta tio n w ith lo c a l te a c h in g in sti tu tio n i n m e d ic in e /u n it o f IM A / w it h th e h e lp o f N G O
T o b e a rra ng e d th ro u g h c o rp o ra te p a r tic ip a tio n / o th e r d o no r a g e n c ie s
T o b e a r ra n g e d th ro u g h
c o rp o ra te p a r tic p a tio n /o th
e r d o n o r a g e n c ie s
Management Group (PHMG) in theadopted village where a PHC is alsolocated.
Formation of PHMG would be throughthe active participation of District HealthOfficer (DHO) and other programmeofficers, village panchayat, CMDR andother NGOs and corporate bodies in theregion
PHMG would be registered as an NGO Initially CMDR would bear the salary
costs of additional man power supplied

PEOPLE’S PARTICIPATION IN HEALTH CARE DELIVERY :AN APPRAISAL OF ACTION RESEARCH 5
COMPOSITION OF PHMG
All households in the village Panchayat members District Health Officer (DHO) and
other programme officers wereincluded when CMDR actually triedto operationalize PHMG. However,it was not possible to include DHOand his staff due to their non-co-operation for the whole experiment.
School teachers of the village Youth associations of the village Women’s Associations of the village Corporate bodies in the region CMDR
Providing M.B.B.S. Doctor to thePHMG clinic
Providing health cards to theHouseholds (HHs) to retain themedical history of the members
Providing telephone facility andlogistical support to the members toavail referral care
Inviting specialized doctors to thevillage for the benefit of the villagers
Organizing eye check up andtreatment camps with the help ofdonors
Educating the members aboutpreventive health care
Working out the feasibility ofproviding health insurance to themembers to avail referral care
Collaborating with charitablehospitals to avail referral care
Collecting user fees from the patientsand managing the PHMG clinic ona sustainable basis
During the course of intervention,we had to hold series of meetings and FocusGroup Discussions (FGDs) in differentvillages of the district. Same useful lessonswere learnt from the village where we firstattempted to establish a PHMG. Weconducted a baseline survey to gatherinformation about the socio-economiccondition, morbidity profile, care seekingbehavior and the cost of treatment. We alsotried to gauge the willingness of thecommunity to pay for the services to beprovided by the proposed clinic. Thoughinitially some young members of thecommunity evinced interest in the wholeaffair, gradually the euphoria subsided.When we started holding FGDs with varioussections of the community, we startedrealizing the ground realities. The elders inthe village had no interest to promote suchexperiment wherein they were required topay for the health services. One issue thatcame to the forefront in this village is that, itwas quite near to the urban center. Thepeople in the village had an easy and quickaccess to the health care institutions in theurban center, which probably acted as ademotivating factor in arousing the interestof the community to participate in such anexperiment.
By this time, we had also initiatedthe process of bringing the District Health

6 CMDR Monograph Series No. - 51
Officer into the experiment. Initial discussionswere held with DHO and other programmeofficers of the district connected with variousschemes of the health sector. The interestshown by the DHO and his team was reallyencouraging. He very much supported theidea of making the community responsiblefor the primary health care services on theirown. The prototype of action interventionwas explained to him and his team. He alsosuggested that, since health happens to be aPanchayat subject it would be better toinvolve the Zilla Panchayat in the wholeexperiment. Such a move would facilitate theinvolvement of Panchayati Raj Institutions(PRIs) in overseeing the effective deliveryof health care services. With this idea in mind,we arranged a much bigger meeting involvingChief Executive Officer of the DistrictPanchayat and Officials of HealthDepartment. The meeting focused on themodalities of community involvement, usercharges to be levied by the PHMG clinicand partnership between PHMG and PHCin the village. Partnership envisaged in thiscontext was to depute additional doctor andnurse to the PHC through the institution ofPHMG. These professionals would be basedin the premises of PHC. The communitywould get the benefit of this additionalmanpower by paying user fees. One issuewhich came up for discussion during themeeting was that, if a patient gets treated bythe Government doctor in the PHC and notby the PHMG doctor, whether he or she isrequired to pay the user fees or not. If thiswere so, no-body would opt for the PHMG
doctor for the simple reason of paying theuser fees. Hence it was decided in themeeting to collect the user fees from allpatients who would visit the PHCirrespective of the doctor that they consult.Thus user fee turned out to be an entry feeinto the PHC. The District Health Officergave his approval for this in the meeting.Chief Executive Officer of the ZP alsoendorsed this. He was of the opinion that,since PRIs are also involved in theexperiment, there should not be any problemin collecting the user fees.
When the action interventionstarted taking some definite shape with thesedevelopments, we intensified the efforts tochoose a village where such an experimentwould take place. In this context, we startedlisting those villages in the district wherePHCs are located and also such PHCswhere either one Doctor or no doctor isfunctioning. In Uppin Betageri, there wasonly one doctor at the PHC and thecommunity in that village as well as othervillages covered by that PHC felt that thereis a need of one more Doctor. Though, twoposts of Doctors were sanctioned, only oneDoctor was functioning. With this clue, wethought of choosing this village for theintervention. We approached the Panchayatand conducted the FGD. In the focus groupdiscussion the members of the villageshowed interest and were keen to participatein the action intervention. However, forcesoperating behind the scene were reallyindicative of the nature of support from

PEOPLE’S PARTICIPATION IN HEALTH CARE DELIVERY :AN APPRAISAL OF ACTION RESEARCH 7
government officials. The District HealthOfficer was quietly recruiting new doctorsto the PHC of this particular village. Initiallyone doctor was appointed and gradually eventhe third doctor was installed in the PHCthough there was no provision for the thirddoctor. These developments saw the moodof the villagers change very fast as theythought it futile to participate in an experimentwherein they themselves would shoulder theresponsibility of running the clinic after theintervention support is over. They were veryhappy to have three doctors in the PHC butour efforts to enthuse them did not yield thedesired results. The DHO who perceivedour experiment as a threat professionally,was successful in foiling our experiment inthis particular village. The fact that came outfrom this experience was that, though thepublic health officials were appreciating thekind of intervention that CMDR was tryingto introduce, in actual practice they were notvery keen to support it. They were not readyto accept the fact that public health deliverysystem is not effective in providing healthservices to the people.
We chose another village whichwas willing to participate in our actionexperiment. We had discussions with themembers of the Grama panchayat of thisvillage. They were happy about the fact thatthe PHC in their village would get anadditional doctor and a nurse. The ChiefExecutive Officer (CEO) of the ZillaPanchayat (ZP) was prepared to extend hishelp for the experiment and he even directed
DHO to actively support it. As a matter ofcaution, we had similar discussions in anothervillage also so that we had an alternativeoption if again our attempt was aborted heretoo. Another reason for doing so was to seewhether we could undertake such anexperiment in the second village withoutinvolving the PHC. The joint meeting of ZP,District Health Officials, members ofrespective villages and CMDR team washeld to discuss the modalities of intervention.The people of both villages welcomed theidea of joining hands with PHC and to haveadditional staff in the premises of PHC. Theywere willing to pay for obtaining servicesfrom the PHC. During the course of themeeting the District Health Officer openlystated that he would permit the additionaldoctor and nurse to use the premises of thePHC and the new doctor would be requiredto function as per the existing governmentframework. But very soon, in almost aweek’s time we learnt that the DHO had adifferent story to narrate. He said, he wouldrequire the permission from his higher-upsin Bangalore and only if he gets the approvalfrom them, he would be in a position tohandover a portion of the PHC to the newstaff recruited under the experiment. Thiswas breaking news for the team of CMDRas well for the village that was ready toparticipate in the experiment. The villagerswere not very happy over this development.They at the same time were not very keenon undertaking such an exercise withoutinvolving the PHC. The office bearers of theGram Panchayat opined that, the villagers

8 CMDR Monograph Series No. - 51
lacked the necessary mental make-up andthe capacity to participate in such anexperiment in which public set up is notparticipating. One member felt that the drugsand other supplies to be supplied for thepeoples’ clinic would be misused by certainsections of the society and people may startsuspecting any transaction by the officebearers of the PHMG. Thus, the fate of thefirst of the two selected villages was sealed.
In the stand by village, which wehad selected as a matter of caution, we triedto experiment our prototype of actionintervention. One advantage of this particularvillage was that, it had a good backgroundof community participation in the drinkingwater supply scheme. The government ofNetherlands had initiated a rural drinkingwater and sanitation scheme in the state ofKarnataka, which tried to create theinfrastructure for the drinking water supplywith about 15 percent of the cost of theproject to be borne by the community. Afterthe expiry of the project phase, the createdinfrastructure would be handed over to thecommunity itself for maintaining andoperating the services on sustainable basis.This village named Morab, was managingthe scheme of water supply successfully. Ithad the facility to treat the water beforesupplying and couple of water tanks wereconstructed to store the water to be suppliedto the community. If a household wished toown a tap in their own home, it had to payhigher user fee than the household, whichgot water through community tap. In any
case community had to pay for the drinkingwater. The scheme was handed over to theGrama Panchayat and it has been runningthe show successfully for past seven to eightyears. We considered this as the bestpositive factor in favor of enthusing thecommunity to shoulder the responsibility ofproviding health care services also along withthe water supply and sanitation facilities. Atthe outset we informed the villagers that, weare trying our best to get the nod from thehigher-ups of the health department inBangalore to initiate the experiment in thisvillage with the effective participation of PHCset up. But if we fail to get the permission,the community has to be ready to experimenton their own. As expected the governmentmachinery did not respond at all to ourvarious requests to have discussions withthem regarding the modalities of ourproposed action intervention. More than amonth was just wasted in waiting for theofficial response. We felt that nothing wouldmove forward in this regard. Finally wemade up our mind to go ahead withoutjoining hands with the PHC set up.
The village people got convincedabout the non-cooperation of thegovernment machinery and they alsoexpressed the desire to experiment the actionintervention. When we decided to moveforward, we actually planned the details ofthe experiment with the Grama Sabhamembers as well as other prominentmembers of the community. The suggestionwhich came out during such meetings, was

PEOPLE’S PARTICIPATION IN HEALTH CARE DELIVERY :AN APPRAISAL OF ACTION RESEARCH 9
that, there is a need to place the details ofthe experiment before the general public ofthe village in a open meeting which is knownas Grama Sabha or Village Meet. TheCMDR team attended such a meeting in thevillage and the details of the actionintervention were explained to the people.To our surprise the health related matterswere taken up at the outset of the meetingand people expressed a desire to have adoctor at the PHC. They made this requestbecause the post of doctor had remainedvacant for many years. There had been manyad-hoc arrangements, which never fulfilledthe requirements of the PHC. Incidentally,the District Health Officer made one moreadhoc posting for the vacancy of doctor, andthe concerned doctor had come on the dayof meeting to convince the people thatgovernment has done something for theirvillage by sending the doctor. When thedoctor informed the people that he had takenthe charge of Medical Officer of PHC forthe past one month or so, the people couldnot believe it. They asked the office bearersof the panchayat and other people as towhether they noticed the presence of thisdoctor at the PHC at any time. It meant thatthe doctor had taken charge only on paperand had no time to visit the PHC to deliverthe services. This event actually benefitedus to a great extent. We explained the detailsof the experiment. The idea of formation ofPHMG and establishing a clinic by it in thevillage appealed to the people. There was aunanimous agreement for this idea. Whenwe also explained about the introduction of
user fees at the clinic there was no oppositionto such an idea, in fact people were in favorof this, because getting a M.B.B.S. doctorfor their village involves certain expenditurewas the message from their discussion. Thevillage meet finally gave an unanimous YESfor our experiment. After this meet, weintensified our efforts towards the formationof PHMG. A series of meetings were heldwith Grama Panchayat members and othervillage leaders, social activists, womenorganizations and youth associations. Ourintention was to involve the panchayat setup in the organization of PHMG on an officialbasis. This would help the process ofdecentralization in the provision andmanagement of health care services. But theopinion of the office bearers of the panchayatwas that, the decentralized set-up has beenreeling under the effects of “Red Tape” andhence it would not be proper to bring PHMGalso under a system which suffered onaccount of many socio-political factors. Weconsidered their argument and finallydecided to keep PHMG out of thedecentralized set up, but we inducted someof the panchayat members as the membersof PHMG also.
Thus the formation of PHMGtook place in the village. The members ofPHMG included, Panchayat members,school teachers, representatives of womenorganizations, other prominent members ofthe community and of course CMDR wasalso a member of this group. The doctor andnurse were appointed for the clinic. We were

10 CMDR Monograph Series No. - 51
able to search an experienced M.B.B.S.doctor, who had several years of practice inrural areas. We had a series of meetings tocomplete the modalities of opening the clinicin the village. A bank account was openedin the village in the name of PHMG and threepeople were authorized to operate theaccount. The doctor of the clinic, thepresident of the PHMG and the presidentof the Gram Panchayat were to manage thefinancial matters of the PHMG. In any case,CMDR had taken the responsibility ofshouldering the doctor’s and nurse’s salary,supply of medicines and 50 percent of therent for the premises of the clinic. TheCMDR had intimated to the PHMGmembers that such financial support fromCMDR would be for a period of six monthsonly. After the expiry of such period, thePHMG will have to take over theresponsibility of running the PHMG clinic onits own. A suitable place in the village waschosen to start the clinic. The members ofPHMG named the clinic as SamudayaArogya Kendra (SAK) which meansCommunity Health Center. Before theinauguration of the clinic, CMDR suppliedthe minimum of equipments and other smallrequirements of the SAK. The following tableshows the kind of materials supplied andtheir value.
Type of assets Amount (Rs)
Medical Instruments 8825.5
Furniture 4242Other materials 1055Total 14122.5
The clinic was opened on the 19th ofSeptember 2002. The PHMG had agreedto collect the user fees from the patientsvisiting the clinic. The fee structure consistedof two slabs. An examination along withsupply of minimum tablets and medicinewould cost the patient Rs 5/- whereas thefee would be Rs 10/- if the patient receivedan injection. From day one the patientsshowed interest to visit the clinic. The moodon the opening day in the village was quiteeuphoric with villages and members of thePHMG feeling contented as they wereinstrumental in bringing a M.B.B.S. doctorto the village. They had put up a small boardfor the clinic with the working hours of theclinic mentioned on it. The clinic was tofunction from 9 a.m. to 5 p.m.
The clinic started functioning, andthe staff of CMDR used to visit the villageto give publicity to the clinic. They also usedthe occasion to elicit the views of the patientsregarding services offered by the PHMGclinic as well as the PHC situated in thevillage. The following table shows the month-wise income and expenditure of the PHMGclinic.
Table 1: Assets given to the SAK

PEOPLE’S PARTICIPATION IN HEALTH CARE DELIVERY :AN APPRAISAL OF ACTION RESEARCH 11
The clinic was opened on the 19th ofSeptember 2002. The PHMG had agreedto collect the user fees from the patientsvisiting the clinic. The fee structure consistedof two slabs. An examination along withsupply of minimum tablets and medicinewould cost the patient Rs 5/- whereas thefee would be Rs 10/- if the patient receivedan injection. From day one the patientsshowed interest to visit the clinic. The moodon the opening day in the village was quiteeuphoric with villages and members of thePHMG feeling contented as they wereinstrumental in bringing a M.B.B.S. doctorto the village. They had put up a small boardfor the clinic with the working hours of theclinic mentioned on it. The clinic was tofunction from 9 a.m. to 5 p.m.
The clinic started functioning, and thestaff of CMDR used to visit the village togive publicity to the clinic. They also usedthe occasion to elicit the views of the patients
Month
No.of patients
@ Rs. 5 Amount
No.of patients
@ Rs. 10 Amount
Total No.of
patients Amount2-Sep 28 140 96 960 124 1100
2-Oct 140 700 439 4390 579 50902-Nov 145 725 431 4310 576 5035
2-Dec 79 395 355 3550 434 39453-Jan 135 675 380 3800 515 4475
3-Feb 179 895 299 2990 478 38853-Mar 554 2770 0 * 0 * 554 2770
Total 1260 6300 2000 20000 3260 26300
* Note: In view of the non-availability of break up of patients, we have
included all under Rs.5 category.
regarding services offered by the PHMGclinic as well as the PHC situated in thevillage. The following table shows the month-wise income and expenditure of the PHMGclinic.
The receipts of the clinic for theperiod September 2002 to March 2003shows that, a total of 3,280 patients visitedthe clinic, generating an income of Rs.26,300. Certainly this amounts to asignificant sum for the PHMG of Morab. Butat the same time, we also need to look atthe expenditure. The CMDR was paying Rs.10,000 as salary plus Rs. 3,000 asallowances to the doctor. The nurse used toget Rs. 5,000 as salary and Rs. 680 by wayof allowances. Apart from this CMDR had
also spent on non-recurring items like,equipments and furniture for the clinic andrecurring expenditure on medicines. This isshown in the table below.

12 CMDR Monograph Series No. - 51
Doctor Nurse2-Sep 5200 5676 6943 17819
2-Oct 13000 5676 1390 20066
2-Nov 13000 5676 18676
2-Dec 13000 5676 2783 21459
3-Jan 13000 5702 18702
3-Feb 8000 5624 13624
3-Mar 13000 5676 18676
Total 78200 39706 11116 129022
Table 3: Recurring Expenses of the Clinic (Rs.)
MonthSalary
Medicines Total
The average income and expenditure perpatient would give us the overall scenario ofthe finances of the clinic. It would alsoindicate the gap that exists with the present
user fee structure as well as compensationstructure for the staff employed. Thefollowing table gives us the average incomeand expenditure per patient.
Months
Income /
Patient
Expenditure /
Patient Difference2-Oct 8.8 34.7 -25.9
2-Nov 8.7 32.4 -23.7
2-Dec 9.1 49.4 -40.4
3-Jan 8.7 36.3 -27.6
3-Feb 8.1 28.5 -20.4
3-Mar 5 33.7 -28.7
Total 8.1 39.6 -31.5
Table 4: Per Patient Income & Expenditure

PEOPLE’S PARTICIPATION IN HEALTH CARE DELIVERY :AN APPRAISAL OF ACTION RESEARCH 13
The average income per patient variesbetween Rs. 5 to about Rs. 8 whereas theaverage expenditure is between Rs. 28 toRs 40. This only means that the cost ofproviding medical care services is quiteburdensome and if the community is madeto shoulder this responsibility, it may not befeasible for it to do so. What could be thealternatives before us to deal with a situationlike this? If one considers increasing the userfees, the community may not support it. Evenif some segment of the community supportsit, it may severely affect the equity aspectsof the services rendered by the clinic, leavingout the poorer sections in the cold. In sucha situation, the best thing would be to reducethe operating costs of the clinic by reducingthe salary of the doctor and by a reductionof other manpower support. In this particularexperiment it was found that, as the clinicwas catering to the needs of the communitywith regard to the treatment of commondiseases and injuries, the services of thenurse was not considered to be veryessential. The clinic had no facilities toprovide the MCH services, which also madethe nurse less useful for the clinic. Thepremise of the clinic was rented at the rateof Rs 600 per month. There was scope toshift the clinic to cheaper premises to saveon the costs. The various permutations andcombinations of the viability aspects of theclinic showed that, at least 35 to 40 patientsmust visit the clinic and it must generate anincome of Rs. 7,000 to 7,500 per month.The clinic must then find a doctor who iswilling to serve for Rs. 5,000 per month.
Rest of the amount could be utilized for thepurchase of medicines and payment of rentand salary of the helper, with of course someminimum savings for the PHMG. Under suchcircumstances the take over of the clinic bythe PHMG would be quite smooth andsustainable, after CMDR’s withdrawal fromthe intervention.
Views of the Community Aboutthe Clinic:
When the clinic startedfunctioning in the village, the news startedspreading slowly within the village as well asto the neighboring villages. Thanks to theefforts of the CMDR field team which wasinstrumental in canvassing the opening up ofthe clinic as well as services rendered by itfor the benefit of the community. The doctorof the clinic was also effective in renderingthe services as required by the communityand his interpersonal skills helped in gainingthe confidence of the community. Aspromoters of the clinic, CMDR was keento know how the community viewed theclinic vis-à-vis the PHC that was alsofunctioning in the village. Exit interviews,discussions with the people and patientswere conducted at regular intervals to elicitthe information.
Young and old, male andfemale rich and poor patients visited thePHMG clinic. Usually more patients visitedthe clinic in the morning hours (between 10a.m. to 1.30 p.m.) and in the evenings i.e.

14 CMDR Monograph Series No. - 51
around 5 p.m. or at the time of closure ofthe working hours. The community responseto the services provided by the clinic wasquite positive which was mainly due to theabsence of a M.B.B.S. doctor in the village,for the past several years. Most of thequacks who did function in the village werenot very impressive. The doctor at the PHCwho was a M.B.B.S. was not available formost of the time.
People said that the clinic waslocated in a convenient place, in the centerof the village. Space within the clinic wasquite sufficient, both for the patients to waitin queue and for the doctor to examine thepatients. The doctor of the clinic, accordingto the patients, was receptive and humanein his approach. The views of the patientsabout the clinic are summarized below:
Need for the doctor to stay in the clinicduring night time also
Patients felt that the user fee of Rs. 10and Rs. 5 was affordable for the membersof the community
Quality of the services rendered wasfound satisfactory by the patients
Patients preferred the services of PHMGclinic due to poor quality of servicesprovided by the PHC
People expressed the need to includematernity services in the clinic
The poor expressed a desire to get freeservices from the clinic
Need was also expressed to have specialhealth check-up camps
It was also brought out from our surveythat more publicity for the clinic needsto be provided in some areas of thevillage as well as the surrounding villages
The clinic started by the PHMG hada positive impact on the functioning of thePHC located in the village. As the PHMGclinic started providing good service on aregular basis, the sleeping governmental set-up woke up and started responding in areactive way to the initiatives of the peoples’clinic. The DHO came out of his routine styleof functioning and tried to match the ‘PatientFriendly’ services of the peoples’ clinic.Where there was no doctor for years in thePHC, we could see a doctor visiting thePHC daily. Even holidays saw a doctor atthe PHC, which was a rare scene in thevillage. The PHC geared up its activities byvisiting households in the village and providingservices at their doorsteps. This change inattitude put the villagers in confusion whoslowly started thinking that, there was noneed to continue with the PHMG clinic asthings are quite satisfactory at the PHC.Fortunately, this view was held by a smallgroup of people. The villagers were ultimatelyconvinced that things at the PHC improvedonly because of the CMDR experiment, andonce the experiment is over and the PHMGclinic is closed, there is every possibility thatthe PHC would revert back to its old status.So people were cautious enough to safe-guard the interest of the community bycontinuing to support CMDR led actionintervention.
The views of the community andthe support extended by the villagers reallyenthused us because we had sensed the urgein the community to carry on with theexperiment even after the withdrawal of

PEOPLE’S PARTICIPATION IN HEALTH CARE DELIVERY :AN APPRAISAL OF ACTION RESEARCH 15
CMDR. As mentioned earlier, we were busyidentifying a less expensive doctor to beposted in the clinic, so that the finances ofthe clinic would be managed within the limitsof the PHMG. When we finally found adoctor who was ready to work for Rs. 5,000per month, CMDR handed over the clinicto the PHMG by withdrawing the staffrecruited earlier. Thus, from the seventhmonth of its inception, the peoples’ clinicstarted functioning in the village as peoples’own initiative.
The experiment hashighlighted the fact that there is a potential inthe community to participate in experimentswhich calls for their participation. In mattersrelated to health, the need for communityparticipation is still more crucial and villagersare looking for outside help for initial doses
of supplements. Even the working hours ofthe PHC are not in tune with the requirementsof the people. A clinic of their own is certainlya boon to them. Our experiment supportedthe community clinic for just six months. Thecommunity felt that it needs to be extendedby about a year or so, in order to encouragethe community to shoulder the responsibilityof running the clinic. The people were alsonot able to contribute seed money on accountof drought situation for the past couple ofyears. Capacity building in the communityand getting a clear vision of sustaining suchexperiments on long-term basis are time-consuming factors. A long-term experimentwould certainly be more beneficial toevaluate the sustainability aspect.Nevertheless the community has now takenchange of the clinic and the health servicesare reaching the people in a smooth manner.
End Notes:1 * CEO – Chief Executive Officer
CHC – Community Health CenterDHO – District Health OfficerFGD – Focus Group DiscussionHFA – Health For AllPHC – Primary Health CenterPHMG – Primary Health Management GroupPRI – Panchayati Raj InstitutionsRKS – Rogi Kalyan SamitiZP – Zilla Panchayat

16 CMDR Monograph Series No. - 51

PEOPLE’S PARTICIPATION IN HEALTH CARE DELIVERY :AN APPRAISAL OF ACTION RESEARCH 17

18 CMDR Monograph Series No. - 51

PEOPLE’S PARTICIPATION IN HEALTH CARE DELIVERY :AN APPRAISAL OF ACTION RESEARCH 19

20 CMDR Monograph Series No. - 51

PEOPLE’S PARTICIPATION IN HEALTH CARE DELIVERY :AN APPRAISAL OF ACTION RESEARCH 21