Closed Fractures of the Tibial Diaphysis David L. Rothberg, MD Erik N. Kubiak, MD University of Utah...
64
Closed Fractures of the Tibial Diaphysis David L. Rothberg, MD Erik N. Kubiak, MD University of Utah Original Authors: Robert V. Cantu, MD and David Templeman, MD; March 2004 Interim Authors: David Templeman and Darin Friess, MD; Revised June 2006 New Authors: David L. Rothberg, MD & Erik N. Kubiak, MD; Revised June 2010
-
Upload
alvin-robertson -
Category
Documents
-
view
219 -
download
1
Transcript of Closed Fractures of the Tibial Diaphysis David L. Rothberg, MD Erik N. Kubiak, MD University of Utah...

Closed Fractures of the Tibial Diaphysis
David L. Rothberg, MD
Erik N. Kubiak, MDUniversity of Utah
Original Authors: Robert V. Cantu, MD and David Templeman, MD; March 2004
Interim Authors: David Templeman and Darin Friess, MD; Revised June 2006
New Authors: David L. Rothberg, MD & Erik N. Kubiak, MD; Revised June 2010

Tibia Fractures
Most common long bone fracture
492,000 fractures yearly
Average 7.4 day hospital stay
100,000 non-unions per year

History & Physical
Low Energy
– Minimal soft-tissue injury
– Less complicated fracture pattern and management decisions
76.5% closed
53.5% mild soft-tissue energy

History & Physical High Energy
– High incidence of neurovascular energy and open injury
– Low threshold for compartment syndrome
– Complete soft-tissue injury may not declare itself for several days

Radiographic Evaluation
Full length AP and Lateral Views– Check joint above &
below
Oblique views may be helpful in follow-up to assess healing

Injuries Associated
30% of patients will have multiple injuries– Ipsilateral Fibula
Fracture– Foot & Ankle injury– Syndesmotic Injury– Ligamentous knee
injuries

Injuries Associated
Ipsilateral Femur Fx– “Floating Knee”
Neurovascular Injury– More Common In:
High Energy Proximal Fracture Floating Knee Knee Dislocation

Classification
Numerous systems
Important variables– Fracture Pattern
– Location
– Comminution
– Associated Fibula Fx
– Degree of soft-tissue injury

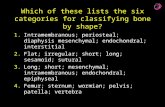
OTA Classification
Follows Johner & Wruh system
Describes relationship between fracture pattern & mechanism
Comminution is prognostic for time to union

Henley’s Classification
Applies Winquist & Hansen Femur classification to fractures of the Tibia

Tscherne Classification of Soft-Tissue Injury
• Grade 0• negligible soft tissue injury
• Grade 1• superficial abrasion or contusion
• Grade 2 • deep contusion from direct trauma
• Grade 3 • Extensive contusion and crush injury with possible
severe muscle injury, compartment syndrome

Compartment Syndrome Incidence:
– 5-15% History
– High-Energy– Crush
Exam– 4 Compartments– 6 P’s
Pain Pain with passive stretch Parasthesias Pulsless Pallor Paralysis

Compartment Anatomy
Anterior– Deep Peroneal N.
Lateral– Sup. Peroneal N.
Deep Post.– Tibial N.
Sup. Post.– Sural N.

Anterior Compartment
• Action• Ankle dorsiflexion
• Muscles• Tib. Ant. • EDL • EHL • Peroneus Tertius
• Vessels• Anterior Tibial A./V.
• Nerves• Deep Peroneal N..
1st webspace sensation

Lateral Compartment
• Action
• Foot Eversion
• Muscles
• Peroneus Brevis & Longus
• Nerves
• Superficial Peroneal N.
• Dorsal foot sensation

Deep Posterior
• Actions• Ankle plantarflexion• Foot inversion
• Muscles• FDL • FHL • Tib. Post.
• Vessels• Post Tibial A./V.• Peroneal A.
• Nerve• Tibial N.
Plantar foot sensation

Superficial Posterior
• Action• Ankle Plantarflexion
• Muslces• Gastrocnemius • Soleus• Popliteus• Plantaris
• Vessels• Greater and Lesser
Saphenous V.• Nerve
• Sural N. Lateral heel sensation

Compartment Syndrome Remains a Clinical Diagnosis

Pressure Measurements
May be helpful in borderline cases– Basic Science
Muscle ischemia present at 20 mmHg below DBP and 30 mmHg below MAP
Various Thresholds– P = 30 mmHg– P = 45 mmHg– Whiteside’s Theory
∆ P = DBP – CP = < 30 mmHg

Pressures Not Uniform
Highest at Fracture Site
Highest Pressures in:– Deep Posterior– Anterior
Heckman JBJS ’76

Clinical Monitoring
Close Observation– Repeat Exams– Repeat Pressure
Measurements
Indwelling Monitors– Reserved for
intubated patient with high suspicion

Goals of Fasciotomy
Decompress the compartment– Minimize further soft-
tissue damage Single vs. Two incisions
– Go long No increased morbidity No difference in long-term
outcome Plan for fracture fixation Plan for wound closure Coordinate with location
of future incisions and/or internal fixation

Closed Tibial Shaft Fracture
Broad Spectrum of Injures w/ many treatments
Closed Management Intramedullary Nails Plates External Fixation

Non-Operative Treatment Indications

Fracture Brace

SarmientoUnion Rate
– 98.5%Time to Union
– 18.1 weeksShortening
– <1.4%
Initial Shortening = Final Shortnening

Natural History
Long-term angular deformities – Well tolerated without associated knee or
ankle arthrosis
– Kristensen 22 pt F/U: 20-29 yrs All patients >10 degree deformity No radiographic Ankle arthrosis
– Merchant & Dietz 37 pt F/U: 29 yrs 76% of Ankles had G/E radiographic results 92% of Knees had G/E radiographic results

Post Tibia Fracture Ankle Motion
25% Post Tibia Fracture will lose 25% of Ankle ROM

Surgical Indications Patient Characteristics
– Obesity– Poor compliance with non-
operative management– Need for early mobility
Injury Characteristics– High Energy– Moderate soft-tissue injury– Open Fracture– Compartment Syndrome– Ipsilateral Femur Fx– Vascular Injury
Fracture Characteristics– Meta-Diaphyseal location– Oblique fracture pattern– Coronal Angulation > 5°– Sagittal Angulation > 10°– Rotation > 5°– Shortening > 1cm– Comminution > 50%
cortical circumference– Intact fibula

Surgical Options
• Intramedullary Nail
• ORIF with Plate
• External Fixation
• Combination of fixation

Advantage of IM Nail Less malunion Early weight-bearing Early motion Early WB (load sharing) Patient satisfaction
L Bone, JBJS
Cost– Less expensive to society when
compared to casting
– Busse Acta Ortho ‘05

Disadvantages of IM Nail
Anterior knee pain 2/3, improve w/in year
• Risk of infection Increased hardware
failure with unreamed nails
Thermal Necrosis Medial HW
prominence

IM Nails
PRCT 62 pts
– If displacement >50% angulation >10°
– Nails superior to cast treatment
Hooper JBJS-B ‘91

IM Nails – Bone et.al.
Retrospective review 99 patients
Cast Nail
Time to union 26 wks 18 wks
SF-36 74 85
Knee score 89 96
Ankle score 84 97 Bone JBJS ‘97

Reamed vs. Nonreamed Nails
Reamings (osteogenic)
Larger Nails (& locking bolts)– Hardware failure rare w/ newer nail
designs
Damage to endosteal blood supply?– Clinically proven safe even in open fx
Forster Injury ‘05Bhandari JOT ‘00

Blachut JBJS ‘97
Reamed Non-Reamed
# pts. 73 63
Nonunion 4% 11%
Malunion 4% 3%
Broken Bolts 3% 16%
Time to Union 16.7 wks 25.7 wksLarsen JOT ‘04
Reamed vs. Nonreamed Nails

IM Nails – Interlocking Bolts
Loss of alignment w/o interlocking
Spiral 7/22Transverse 0/27Metaphyseal 7/28
Templeman CORR ‘97

Complications
Infection 1-5% Union >90% Knee Pain 56%
– w/ kneeling 90%– w/ running 56%– at rest 33%
Court-Brown JOT ‘96

Knee Pain after IMN
Incidence– Varied in lit. 10-86%
Attributed to:– Skin Incision– Approach– Insertion Site– Quad weakness– Nail Prominence
Removal– 27% resolved– 69% marked
improvement– 3% worse Court-Brown JOT ‘96

Neurologic Complications

Expanded Indications
Proximal 1/3 fractures Beware Valgus and Procurvatum
Distal 1/3 fractures Beware Varus or valgus Beware of intraarticular extension

Proximal Tibia Fracture
Entry site is critical
Reference– Lateral Tibial
Spine

Too Low! Too Medial!Procurvatum Valgus

Semiextended Position
Neutralize quadriceps pull on proximal fragment
Medial parapatellar approach – subluxate patella laterally
Use handheld awls to gently ream through the trochlear groove
Tornetta CORR ‘96

Hyperextended position
Pulls patella proximally to allow straight starting angle
Universal distractor
Beuhler JOT ‘97

Blocking (Poller) Screws
Functionally narrows IM canal– Increases strength and rigidity of fixation– Place on concave side of deformity
21 patients– All healed within 3-12 months– Mean alignment 1° valgus, 2° procurvatum
Krettek JBJS ‘99

Technique
Screws placed on concave side of deformity
Proximal or distal fractures


Distal Tibial Fractures
Reduction before reaming
Distractor Fibula plate/nail Joy Stick Calcaneal Traction

Universal Distractor Reduction
Beuhler JOT ‘97

Plate Fibula

Distal Tibial Joystick

Outcomes of IM Nailing
• 859 closed tibia fractures• 92.5% union rate• 18.5 weeks to union• 1.9% infection rate• 4.4% aseptic nonunion
• “Reamed intramedullary nailing will probably continue to be the best method of treating tibial diaphyseal fractures.”
Court-Brown JOT ‘04

Plating of Tibial Fractures
• 3.5 mm or Narrow 4.5mm DCP plate can be used for shaft fractures
• Newer periarticular plates available for metaphyseal fractures

Subcutaneous Tibial Plating
• Newer alternative is use of limited incisions and subcutaneous plating- requires indirect reduction of fracture and hybrid screw fixation options

Advantages of Plating
Anatomic reduction usually obtained
In low energy fractures– 97% G/E results
reported• Ruedi Injury

Disadvantages of Plating
• Increased risk of infection and soft tissue problems, especially in high energy fractures
• Higher rate hardware failure than IM nail
• Delayed WB (load bearing) Johner CORR ‘83

External Fixation
• Generally reserved for open tibia fractures or periarticular fractures

AO Technique of Tibia Plating• Anterior longitudinal incision
• 1 cm lateral to tibial crest• Maintain AT paratenon and periosteum
• Plate on medial border of tibia
• 3.5 mm or 4.5mm LCDCP plate secured to bone on distal fragment
• Butterfly fragment can be secured with interfragmentary screw
• The AO articulating tension device can be secured to proximal part of plate to aid reduction
• With fracture reduced, screws placed through plate on either side of fracture

Technique of External Fixation
• Unilateral frame with half pins
• 5mm half pins• near-near and far-far• Stay out of zone of injury
• Pre-drilling of pins recommended
• Fracture held reduced while clamps and connecting bar applied

Advantages of External Fixator
• Can be applied quickly in polytrauma patient
• Allows easy monitoring of soft tissues and compartments
• Modifiable• No long term deep HW

Outcomes of External Fixation
Anderson CORR ‘74Edge JBJS ‘81
95% union rate for group of closed and open tibia fractures
20% malunion rate Loss of reduction
associated with removing frame prior to union
Risk of pin track infection

Conclusions
Common fracture w/ several treatment options
Closed stable fx can be treated in a cast
Unstable fx often best treated by intramedullary nail

Acknowledgments
1st Edition lecture R. Cantu M.D.Cases Courtesy R. Winquist M.D.
E. Kubiak M.D.
Return to Lower Extremity
Index
E-mail OTA about
Questions/Comments
If you would like to volunteer as an author for the Resident Slide Project or recommend updates to any of the following slides, please send an e-mail to [email protected]