Clinical Significance of Low CMV DNA Levels in...
31
1 Clinical Significance of Low CMV DNA Levels in Human Plasma 1 2 Running Title: Significance of Low CMV DNA Levels in Human Plasma 3 4 Jesse Waggoner 1 , Dora Y. Ho 1 , Paolo Libiran 2 , and Benjamin A. Pinsky 1, 2,* 5 1 Department of Medicine, Division of Infectious Diseases and Geographic Medicine, Stanford 6 University School of Medicine, Stanford, CA, USA. 7 2 Department of Pathology, Stanford University School of Medicine, Stanford, CA, USA. 8 9 *To whom correspondence should be addressed. 10 3375 Hillview Ave, Room 2913 11 Palo Alto, CA 94304 12 Phone: 650-721-1896 13 Fax: 650-723-6918 14 E-mail: [email protected] 15 16 Copyright © 2012, American Society for Microbiology. All Rights Reserved. J. Clin. Microbiol. doi:10.1128/JCM.06800-11 JCM Accepts, published online ahead of print on 18 April 2012 on July 12, 2018 by guest http://jcm.asm.org/ Downloaded from
Transcript of Clinical Significance of Low CMV DNA Levels in...
1
Clinical Significance of Low CMV DNA Levels in Human Plasma 1
2
Running Title: Significance of Low CMV DNA Levels in Human Plasma 3
4
Jesse Waggoner1, Dora Y. Ho1, Paolo Libiran2, and Benjamin A. Pinsky1, 2,* 5
1Department of Medicine, Division of Infectious Diseases and Geographic Medicine, Stanford 6
University School of Medicine, Stanford, CA, USA. 7
2Department of Pathology, Stanford University School of Medicine, Stanford, CA, USA. 8
9
*To whom correspondence should be addressed. 10
3375 Hillview Ave, Room 2913 11
Palo Alto, CA 94304 12
Phone: 650-721-1896 13
Fax: 650-723-6918 14
E-mail: [email protected] 15
16
Copyright © 2012, American Society for Microbiology. All Rights Reserved.J. Clin. Microbiol. doi:10.1128/JCM.06800-11 JCM Accepts, published online ahead of print on 18 April 2012
on July 12, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from
2
ABSTRACT 17
18
The clinical significance of low copy numbers of CMV DNA detected in immune suppressed 19
patients remains unclear. In this study, we compare the artus CMV Rotor-Gene PCR, utilizing 20
automated nucleic acid extraction and assay setup (the artus CMV protocol), with COBAS 21
Amplicor CMV Monitor (our reference protocol). We then analyzed the results of all CMV PCR 22
tests ordered following the implementation of the artus CMV protocol at our institution and 23
followed 91 adult patients with a positive test result. The artus CMV protocol had a linear range 24
extending from 2.0 to 7.0 log10 copies/mL and had a lower limit of 95% detection of 57 25
copies/mL. Using archived plasma samples, it demonstrated 100% sensitivity and 94% 26
specificity for the detection of CMV DNA. Following implementation of the artus CMV 27
protocol, 320 of 1403 (22.8%) plasma samples tested positive (compared with 323/3579 (9.0%) 28
samples in the preceding six months), and 227 (16.2%) samples had copy numbers <400 29
copies/mL. Ninety-one adult patients had at least one positive test. The data was analyzed using 30
a threshold of 200 copies/mL, and in 22 episodes, the viral load increased from <200 copies/mL 31
to ≥200 copies/mL on sequential tests. In 21 of these 22 episodes, the viral load either continued 32
to increase or antiviral treatment was initiated in response to the repeat value. In summary, we 33
evaluate the performance characteristics of a protocol utilizing the artus CMV PCR and identify 34
clinically meaningful changes in CMV DNA copy number even when initially detected at a low 35
level. 36
on July 12, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from
3
INTRODUCTION 37
38
Cytomegalovirus (CMV) remains a major cause of morbidity following solid organ 39
transplantation (SOT) and hematopoietic stem cell transplantation (HSCT), and even with 40
antiviral treatment, mortality from certain forms of CMV end-organ disease, such as CMV 41
pneumonitis, remains high (14, 17, 18). Viremia has been associated with end-organ disease, 42
and an increase in CMV DNA titer in serial blood samples, typically detected using a 43
quantitative PCR assay, can predict disease development (10, 20). When used in a pre-emptive 44
treatment protocol, quantitative PCR helps decrease the incidence of CMV disease and the use of 45
antiviral therapy compared to using viral culture (9). However, despite the widespread use of 46
quantitative CMV PCR assays, thresholds for the diagnosis of disease or the initiation of pre-47
emptive therapy have not been established (9, 14, 17). This situation has resulted from the use of 48
different clinical diagnostic tests for CMV (both commercially available and lab-developed), the 49
broad range of values over which CMV disease can occur, and until recently, the lack of a 50
universal standard for CMV DNA quantitation (8, 13, 24). 51
52
The COBAS Amplicor CMV Monitor was the first commercially available quantitative CMV 53
PCR and remains commonly used in clinical virology laboratories (7). It has a lower limit of 54
detection of 400 copies/mL of plasma and a linear range from 2.78log10 to 5.0 log10 copies/mL 55
(600 to 100,000 copies/mL) (4). The limits of detection and quantitation of this assay result in a 56
large number of patients with ongoing yet unquantifiable or even undetectable viremia. 57
58
on July 12, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from

4
The artus CMV Rotor-Gene (RG) PCR is a commercially-available, quantitative CMV PCR 59
protocol. Initial reports have demonstrated a broad linear range and a lower limit of detection 60
below that of the COBAS CMV Monitor (3). While such low copy numbers of CMV DNA as 61
those detected with the artus protocol have been reported, the clinical significance of these “low 62
positives” in a population of immune suppressed patients has not been well described (2, 11, 15). 63
64
In this study, we report the analytical performance of a protocol utilizing the artus CMV PCR 65
combined with automated sample preparation and assay set-up (SP/AS) on the QIAsymphony 66
SP/AS device (hereinafter referred to as the artus CMV protocol). Using archived human 67
plasma samples, we determined the sensitivity and specificity of the artus CMV protocol for the 68
detection of CMV DNA compared to the COBAS CMV Monitor assay following extraction on 69
the MagNA Pure LC (hereinafter referred to as the reference protocol). We document an 70
increased rate of detection of CMV in patient plasma samples following implementation of the 71
artus CMV protocol at our institution. We then followed 91 adult patients with positive tests, 72
and using a group of transplant recipients with serial testing, we identified clinically relevant 73
increases in CMV DNA copy number, even when quantified at low levels, previously 74
undetectable with the reference protocol. 75
76
on July 12, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from
5
MATERIALS AND METHODS 77
78
Samples and Control Material 79
82 archived plasma samples that had been previously tested by the reference protocol were tested 80
using the artus CMV protocol. Basematrix 53 defibrinated human plasma (DHP; SeraCare, 81
Milford, MA) was used as a negative control in all PCR runs. Stock CMV AD-169 (ATCC, 82
Manassas, VA) diluted to 5.0 and 3.0 log10 copies/mL (100,000 and 1,000 copies/mL) in DHP 83
was used as high and low positive controls, respectively. The concentration of the original stock 84
was determined using the reference protocol. 85
86
DNA Extraction and Assay Set-up 87
DNA extraction for the artus CMV protocol was performed on 1.0mL of acid citrate dextrose 88
(ACD) plasma (1.2mL of input volume required to account for instrument dead volume) using 89
the Qiagen virus/bacteria Midi Kit on the QIAsymphony SP device (both from Qiagen, Valencia, 90
CA). DNA was eluted in a final volume of 95μL. Following DNA extraction, the artus CMV 91
PCR was set-up using the QIAsymphony AS. 10µL of extracted nucleic acids, 12.5µL CMV RG 92
Master Mix, and 2.5µL of CMV magnesium solution were used, for a final reaction volume of 93
25µL. 94
95
For the reference protocol, 100µL of each specimen was extracted on the MagNA Pure LC using 96
the MagNA Pure LC DNA isolation kit with the DNA I Blood Cell High Performance protocol 97
(Roche, Indianapolis, IN). Reactions were manually set-up by pipetting 50µL out of the 100µL 98
elution into COBAS Amplicor amplification tubes (A-tubes) containing 50 µL of the COBAS 99
CMV Monitor Master Mix with Magnesium. 100
on July 12, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from

6
101
Quantitative PCR Assays 102
The artus CMV PCR (Qiagen, Valencia, CA) is a real-time, fluorescein-labeled, hydrolysis-103
probe-based PCR targeting the CMV major immediate early gene. Reactions were carried out on 104
the Rotor-Gene Q (RGQ) and underwent an initial 10 min at 95°C, then 10 cycles of touchdown 105
PCR; 95°C for 15 sec, 65°C for 30 sec, and 72°C for 20 sec, with the annealing step decreasing 106
by 1°C each cycle. This was followed by 35 cycles of 95°C for 15 sec, 56°C for 30 sec, and 107
72°C for 20 sec. Data was collected on the green and yellow channels during annealing. An 108
internal control is added to each primary sample prior to extraction, and amplification is 109
performed with specific primers and JOE-labeled, hydrolysis probes contained in the artus CMV 110
Master Mix to ensure adequate extraction efficiency and the absence of inhibitors. Positive 111
samples produced a signal above a threshold value of 0.1 in the green channel. The number of 112
CMV copies/mL was calculated by comparing the cycle number at which the fluorescent signal 113
crossed this threshold (Ct) with the four-point standard curve included on each run. The standard 114
curve was generated using four quantitation standards (Qiagen, Valencia, CA) with 115
concentrations of 10,000; 1,000; 100; and 10 copies/µL. Results were reported in copies/mL of 116
the original plasma sample. Samples with detectable virus quantified at <150 copies/mL were 117
reported as “Detected, <150 copies/mL”. 118
119
The artus CMV protocol was subsequently calibrated to the 1st WHO International Standard for 120
human cytomegalovirus for NAT based assays (NIBSC code 09/162) obtained from the National 121
Institute for Biological Standards and Controls (NIBSC; Hertfordshire, United Kingdom). The 122
WHO International Standard was diluted to 5.0, 4.7, 4.0, 3.7 and 3.0 log10 IU/mL and 6 123
on July 12, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from

7
replicates at each concentration were run on 4 separate days. The data collected in copies/mL 124
was compared to the expected IU/mL. A conversion factor was calculated by taking the mean 125
ratio of IU/mL to copies/mL for all data points. 126
127
The COBAS Amplicor CMV Monitor (Roche, Indianapolis, IN) utilized in the reference 128
protocol is a non-saturating, end-point PCR targeting the CMV polymerase UL54 gene followed 129
by quantitation with an automated enzyme-linked oligosorbent assay (ELOSA). A separate 130
internal quantitation standard is added to the primary specimen prior to extraction. 131
Amplification and detection were performed as described previously (23). 132
133
Samples that yielded discordant results by the artus CMV and reference protocols were tested 134
using the CMV R-gene real-time PCR assay (hereinafter referred to as the CMV R-gene assay; 135
Argene, Sherley, NY), which targets the pp65 UL83 gene. This assay has a reported lower limit 136
of detection (LLOD) of 50 copies/mL and a linear range extending to 7.0log10 copies/mL (6). 137
10μL of DNA extracted using the Qiagen SP device was added to 15μL of amplification premix. 138
Reaction conditions on the RGQ were 95°C for 15 min, followed by 45 cycles at 95°C for 10 sec 139
and 60°C for 40 sec. Positive samples produced a signal above a threshold value of 0.025 in the 140
green channel. The number of CMV copies/mL was calculated by comparing the cycle number 141
at which the fluorescent signal crossed this threshold (Ct) with the four-point standard curve 142
included on each run. The standard curve was generated using four quantitation standards 143
(Argene, Sherley, NY) with concentrations of 5,000; 500; 50; and 5 copies/µL. 144
145
Linearity, Lower Limit of Detection, and Accuracy 146
on July 12, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from

8
Linearity of the artus CMV protocol was determined using serial 10-fold dilutions of CMV AD-147
169 in DHP. Replicates of each dilution were taken through the entire assay, from extraction to 148
quantitation. To determine the LLOD, Optiquant CMV Panel samples (AcroMetrix, Benicia, 149
CA) were diluted to 100, 50, and 25 copies/mL. Twenty replicates were run at each 150
concentration, and probit analysis was performed to determine the lower limit of 95% detection. 151
The quantitative results obtained with the artus CMV and reference protocols were compared 152
using 82 previously tested clinical samples. Samples that yielded discordant results were re-153
tested using the CMV R-gene assay. 154
155
Clinical Study Design 156
This research was approved by the Stanford University Institutional Review Board. We 157
analyzed the general test characteristics for plasma CMV PCR assays sent at our institution 158
during the study period, which extended from June 20, 2011, the date on which the artus CMV 159
protocol was implemented, to September 12, 2011. Adult patients with a single positive result 160
using the artus CMV protocol during this interval were then identified. We collected relevant 161
clinical data, including patient age, sex, and significant past medical history. For transplant 162
recipients, we documented the type of transplant, indication for transplantation, CMV status at 163
transplant, and antiviral prophylaxis. We also documented any treatment administered during 164
the study. The death summary was used for the documentation of cause of death where 165
applicable. 166
167
Definitions used for CMV infection and end-organ disease were consistent with previously 168
published recommendations (14, 17, 19). CMV infection was defined by the detection of CMV 169
on July 12, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from
9
DNA in patient plasma. The confirmation of CMV disease required a biopsy with consistent 170
histopathology as well as virus isolation or positive immunohistochemistry (IHC). The diagnosis 171
of “CMV syndrome” was considered only for SOT recipients. Recurrent infection was defined 172
as a rising CMV viral load following the completion of a course of antiviral treatment, with the 173
documented absence of detectable CMV DNA or CMV DNA that was detectable but <200 174
copies/mL at the completion of treatment. 175
176
Immune suppression regimens varied by transplant organ, time from transplantation, and 177
evidence of graft rejection or graft-versus-host disease. Transplant patients received antiviral 178
prophylaxis according to protocols employed by the different transplant services at our 179
institution. Two HSCT patients remained on treatment for CMV infection throughout the study 180
period and were not included in the tally of patients receiving prophylaxis. Pre-emptive therapy 181
and treatment for CMV infection or disease was initiated and the duration of therapy was 182
determined by the attending physician caring for the patient. Repeat CMV testing during therapy 183
and follow-up were performed by the clinical laboratory at the discretion of the treatment team. 184
185
Statistical Analysis 186
Agreement between the artus CMV and reference protocols was assessed using a Bland-Altman 187
plot (1). Standard statistical analyses were performed using Excel (Microsoft, Redmond, WA). 188
Probit analysis was performed using SPSS (IBM, Armonk, NY). Two-tailed Fisher’s exact tests 189
and unpaired t-tests were performed using GraphPad software (GraphPad, La Jolla, CA). 190
191
on July 12, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from
10
RESULTS 192
193
Analytical Characteristics of the artus CMV Protocol 194
The linear range of the artus CMV protocol extended from 2.0log10 to 7.0log10 copies/mL (100 195
to 10,000,000 copies/mL). Using probit analysis at 95% detection, the LLOD was found to be 196
57 copies/mL. Assay precision was further evaluated using samples with concentrations of 197
5.0log10, 3.0log10, and 2.30log10 copies/mL (100,000, 1,000, and 200 copies/mL). The mean 198
values were 5.08log10, 2.97log10, and 2.27log10 copies/mL (120,000, 933, and 195 copies/mL) 199
and the inter-run percent coefficients of variation (%COV) were 1.4, 3.7, and 5.8, respectively 200
(calculated for logarithmic values). A checkerboard experiment using 24 CMV-negative plasma 201
samples and 24 CMV AD-169 spiked plasma samples [concentration 6.0log10 copies/mL 202
(1,000,000 copies/mL)] was performed to evaluate the QIAsymphony SP/AS device; no 203
evidence of cross-contamination was observed (data not shown). 204
205
The artus CMV protocol was calibrated to the 1st WHO International Standard for human 206
cytomegalovirus for NAT based assays resulting in a conversion factor of 0.76 IU/copy of CMV 207
DNA. 208
209
Comparison of the artus CMV and Reference Protocols 210
A total of 82 archived clinical samples (42 positive, 40 negative) that had previously been tested 211
using the reference protocol were re-tested using the artus CMV protocol on the QIAsymphony 212
SP/AS/RGQ system. All 42 samples with detectable CMV DNA by the reference protocol were 213
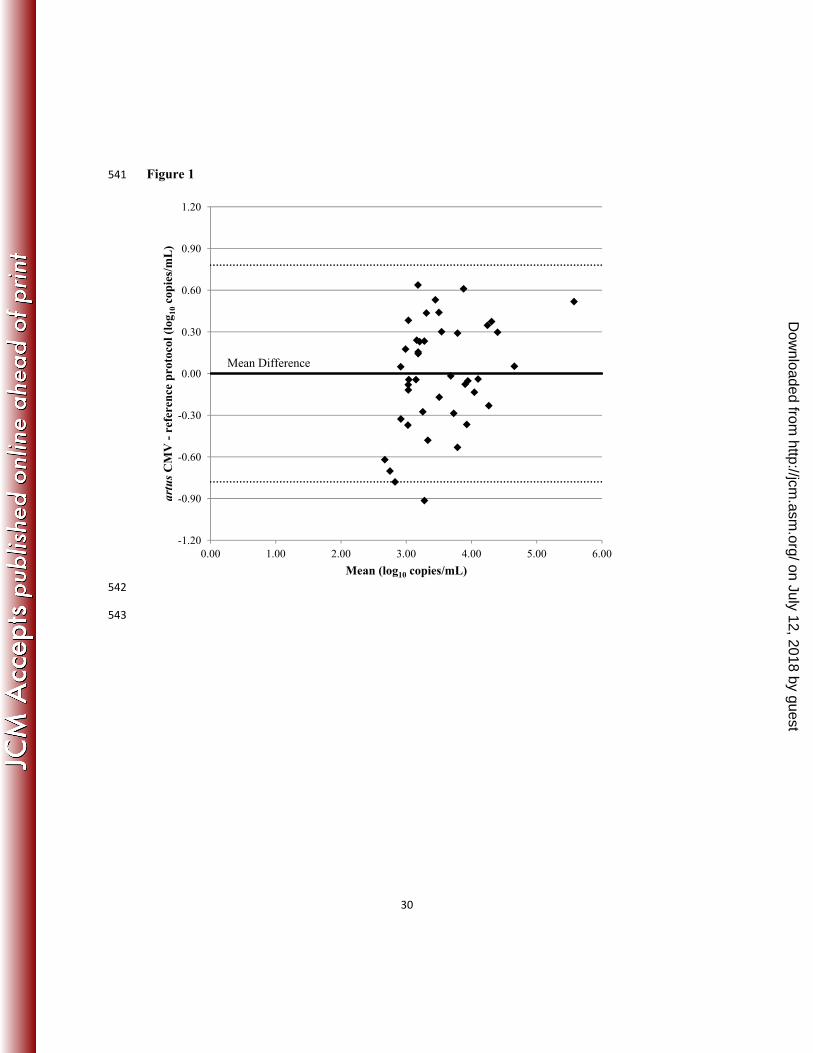
positive by the artus CMV protocol (sensitivity, 100%; Table 1). There was good agreement in 214
the quantitative results between the artus CMV and reference protocols (Figure 1). Except for 215
on July 12, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from
11
two samples (discussed below) all samples yielded results that differed by <2 SD of the mean 216
difference. 217
218
Of 40 samples with undetectable CMV DNA using the reference protocol, 10 were positive 219
using the artus CMV protocol (specificity, 75%; Table 1). The mean concentration in the 10 220
discordant samples using the artus CMV protocol was 255 copies/mL (range 13 - 986), and 8 221
samples had copy numbers <400. Seven patients had a positive CMV PCR by the reference 222
protocol prior to (4 patients) or subsequent to (3 patients) the discordant sample that was used in 223
this validation. On retesting using the CMV R-gene assay, eight of 10 discordant samples (80%) 224
had detectable CMV DNA and two remained undetectable. The revised sensitivity and 225
specificity for the artus CMV protocol, using any two positive tests as the “gold standard,” were 226
100% and 94%, respectively. 227
228
Two samples, collected from a single patient at different time points, were detected but under-229
quantitated by the artus CMV protocol compared to the reference protocol (2.82 vs. 3.73log10 230
copies/mL, and 2.44 vs. 3.22log10 copies/mL for the artus CMV and reference protocols, 231
respectively). The results differed by an amount ≥2 SD from the mean difference (Figure 2). 232
For these discordant samples, the CMV R-gene assay results were consistent with the reference 233
protocol and remained elevated compared to the artus CMV protocol. 234
235
Clinical Results 236
During the study period, 1403 plasma CMV assays were performed at our institution using the 237
artus CMV protocol. Of these, 320 had detectable CMV DNA (22.8%), with 93 quantitated at > 238
on July 12, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from

12
400 copies/mL (6.6%) and 227 (16.2%) detected at <400 copies/mL. In the six months prior to 239
this change, using the reference protocol, 323 out of 3579 tests had detectable CMV DNA (9.0%, 240
p<0.0001). All of these samples had copy numbers ≥400 copies/mL. The number of patients 241
with at least one positive test also increased with the use of the artus CMV protocol over the 242
same time interval (17.8% vs. 6.9% of patients per month, p<0.0001). The average number of 243
tests did not vary significantly throughout this period (593 vs. 539 tests per month, respectively, 244
p=0.052). 245
246
We identified and collected clinical information on the 91 adult patients who had at least one 247
plasma sample with detectable CMV DNA using the artus CMV protocol. The mean age for 248
patients was 51.2 (standard deviation 14.8), and 53 patients were male. The majority of patients 249
had received a transplant (n = 82, 90.1%), of which 55 (60.4%) had an HSCT and 27 (29.7%) 250
had an SOT (lung, 9; renal, 6; heart, 5; liver 3; combined transplants, 4). Table 2 shows 251
characteristics of the transplant recipients, including CMV status at the time of transplantation 252
and antiviral prophylaxis following transplantation. 253
254
The number of tests per patient during the study period (June 20, 2011 through September 12, 255
2011) varied significantly based on their underlying condition. HSCT recipients had a mean of 256
7.0 tests performed per patient (standard deviation 3.8), whereas non-HSCT patients had a mean 257
of 2.7 tests per patient (standard deviation 2.5; p<0.0001). 258
259
Treatment Outcomes and Recurrence 260
on July 12, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from
13
Forty-five patients (49.5%) received antiviral treatment for CMV infection or disease. There 261
was no difference in the proportion of patients treated for CMV based on the type of transplant 262
(58.2% for HSCT vs. 40.7% for SOT, p=0.163). All patients received valganciclovir or 263
ganciclovir as treatment. Four patients also received foscarnet during the study (8.9%). Twenty-264
eight treatment episodes were started and completed during the study. The average duration of 265
antiviral therapy for these episodes was 30.5 days (standard deviation 15.7, range 10-78). 266
Twenty-one patients had at least two weeks of follow-up off therapy, and eight patients had 267
recurrent CMV infection. The rate of recurrence was not significantly different if CMV DNA 268
remained detectable but <200 copies/mL at the end of treatment (50%, n = 10) or if it had 269
become undetectable (27%, n = 11; p=0.387). 270
271
Two patients had confirmed end-organ disease. The first patient, without a transplant, presented 272
with DKA and odynophagia and was found to have esophageal ulcerations positive for CMV by 273
IHC. The serum viral load was 3.78log10 copies/mL (6,020 copies/mL). The second patient 274
received a renal transplant (R-/D+) 17 months before presenting with abdominal pain and 275
diarrhea. Serum CMV showed 5.41log10 copies/mL (259,000 copies/mL), and colon biopsies 276
revealed viral inclusions positive for CMV stain by IHC. Three other patients received treatment 277
for possible CMV disease [colitis (2) and CMV syndrome (1)]. One patient with possible colitis 278
did not undergo a colonoscopy until after treatment had started. The second patient had a 279
colonoscopy at an outside facility, the results of which were not available to us. The patient with 280
possible CMV syndrome improved with antiviral treatment; a limited work-up did not reveal 281
other possible causes for his illness. 282
283
on July 12, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from

14
Eight patients died during the study; causes of death included intra-cerebral hemorrhage, end-284
stage liver disease (2), graft versus host disease (2), pulmonary embolism and pneumonia, 285
congestive heart failure, and AML with blast crisis. None of these patients had confirmed CMV 286
disease. Three patients were receiving treatment for CMV infection at the end of life. 287
288
Patients with Detectable CMV DNA at Low Levels 289
To determine the clinical significance of low positive CMV DNA levels we evaluated our data 290
based on a threshold of 200 copies/mL. This threshold was chosen after initial review of our 291
data for 91 patients with a positive test. 80% (4/5) of patients with quantified viral loads 292
between 150 and 200 copies/mL had a spontaneous decline in the viral load below 150 293
copies/mL, whereas 21/22 patients with viral loads that increased to ≥200 copies/mL had viral 294
loads that continued to increase or received treatment (p=0.0014). 295
296
As shown in Figure 2, 86 (94.5%) patients in this study had at least one CMV level detected at 297
<200 copies/mL. Five (5.5%) of the patients always had elevated CMV DNA levels >1000 298
copies/mL during the study period and were not further evaluated. Sixteen (17.6%) patients had 299
samples with viral loads >200 copies/mL at the beginning of the study period (median viral load 300
1348 copies/mL, range 354-9320 copies/mL). Fifteen of these patients received antiviral 301
treatment. A single patient had an increased viral load in the setting of a disseminated varicella-302
zoster infection, and the CMV copy number declined with high dose acyclovir treatment. The 303
transition from a viral load of <200 to >200 copies/mL was not captured during the study period 304
for these 16 patients. 305
306
on July 12, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from

15
Forty-nine (53.8%) patients only had samples with CMV DNA detected but <200 copies/mL. Of 307
these 49 patients, 16 had a single test performed during the study period. Of the 33 patients with 308
multiple tests, the rate of positive tests per patient varied from 8.3% to 81.8% (1 out of 12 to 9 309
out of 11 samples). None of these patients received treatment during the study period, though 15 310
had been treated for CMV infection or disease previously. 311
312
Twenty-one patients developed 22 clinical episodes during which the CMV DNA copy number 313
increased from a level <200 copies/mL (either undetected or detected but <200 copies/mL) to a 314
level ≥200 copies/mL on sequential tests (Table 3). All 21 patients had received an HSCT 315
(R+/D+, n=10; R+/D-, n=9; R-/D+, n=2). The median time between sequential tests was 7 days 316
(range 1-27 days). 317
318
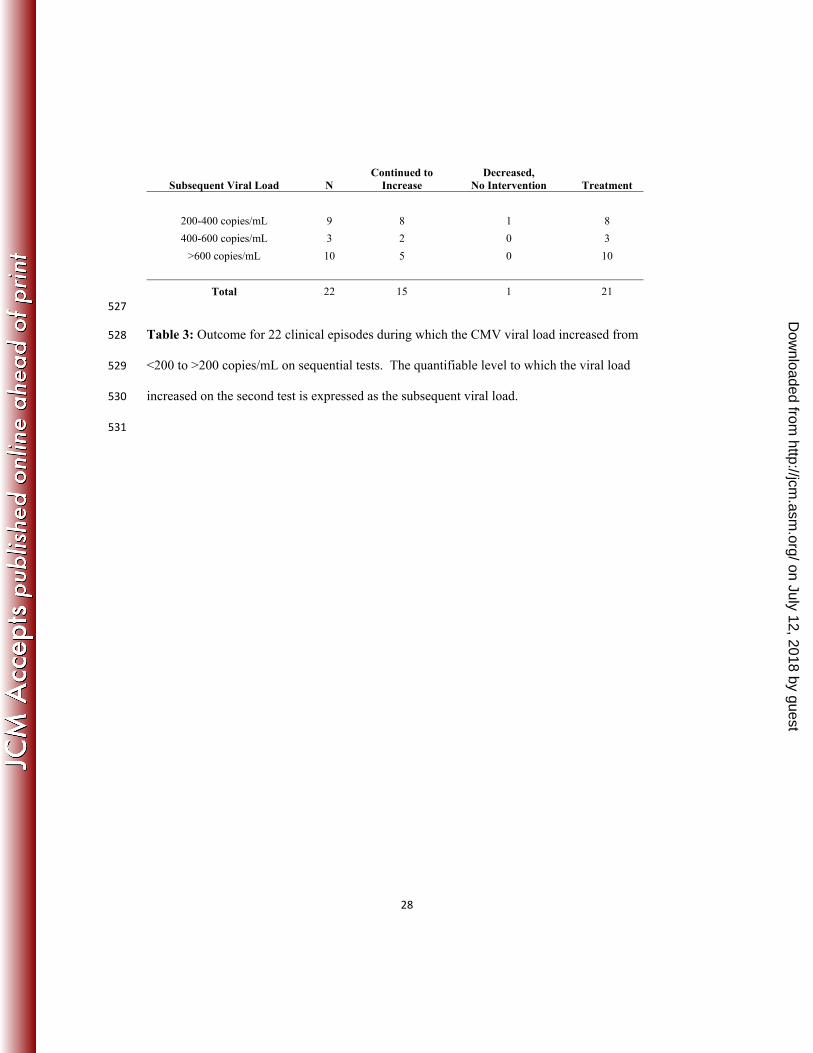
We further categorized these 22 episodes based on quantification of the subsequent tests. In 319
45.5% (10/22) of episodes the subsequent viral load was ≥600 copies/mL, levels quantifiable by 320
the reference assay. In five of these episodes antiviral treatment was initiated in response to this 321
viral load (median viral load 999 copies/mL, range 937-8390 copies/mL). In the other five 322
episodes, the CMV level continued to increase, and all five were eventually treated (median viral 323
load at the start of treatment 946 copies/mL, range 763-2570 copies/mL). In 13.6% (3/22) of 324
episodes the subsequent viral load was 400-600 copies/mL, a range detectable but not 325
quantifiable by the reference method. A CMV level of 541 copies/mL prompted antiviral 326
treatment during one episode. In two episodes, the viral load continued to increase and both 327
episodes were subsequently treated (viral load at the start of treatment 1160 and 761 copies/mL, 328
respectively). 329
on July 12, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from
16
330
In 40.9% (9/22) of episodes the subsequent viral load ranged from 200-400 copies/mL, a range 331
that was not detectable by the reference method. In 8 of these episodes, the viral load continued 332
to increase. Seven of these episodes were ultimately treated with antivirals and one was treated 333
with reduced immune suppression (median viral load at the start of treatment 888 copies/mL, 334
range 323-7950 copies/mL). There was a single episode in which the viral load increased from 335
<200 to >200 copies/mL on sequential tests (262 copies/mL) and then decreased without 336
intervention. 337
338
In 72.2% (16/22) of episodes, patients did not immediately receive treatment in response to their 339
subsequent CMV viral load. In fifteen of these clinical episodes CMV levels continued to 340
increase and ultimately required antiviral therapy or reduced immune suppression. 341
342
on July 12, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from

17
DISCUSSION 343
344
In this study, we evaluated a CMV testing method that involves automated sample preparation, 345
assay set-up, and real-time, quantitative PCR using the artus CMV PCR. This protocol showed 346
good numerical agreement when compared with the reference protocol, and the artus CMV 347
protocol has a broader linear range and lower LLOD. In addition, we also report the finding of a 348
significant increase in the rate of positive tests following the implementation of the artus CMV 349
protocol for the detection and monitoring of CMV in patient plasma samples at our institution. 350
This increase appears to be accounted for by the detection of patients with viral loads 351
undetectable by the reference method, though this cannot be confirmed without testing all 352
samples by both methods. 353
354
The artus CMV PCR has been evaluated in a number of previous studies (3, 5, 7, 12, 22). Our 355
results agree with the findings of the only previous report to compare artus CMV PCR reagents 356
to the COBAS Amplicor CMV Monitor (3). However, we demonstrate a lower LLOD and 357
extend the previous results to include the use of a different DNA extraction protocol and smaller 358
reaction volumes. 359
360
We did identify two specimens that amplified poorly in the artus CMV protocol. These samples 361
were drawn at separate times from a single patient, and repeat testing using the reference 362
protocol and CMV R-gene assay showed consistent and elevated quantitative results. The three 363
assays used in this study target different regions of the CMV genome. One potential explanation 364
for the discrepant quantitation is that the CMV isolate from this patient contains a mutation in the 365
on July 12, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from

18
proprietary major immediate early gene sequences targeted by the artus CMV PCR. Such 366
mutations have been reported to cause decreased amplification in other assays that target this 367
gene, but they have not previously been reported for the artus CMV PCR (5, 16). 368
369
Recently, the WHO approved an international quantitation standard for CMV in an effort to 370
address concerns regarding the agreement of quantitative results for CMV PCR testing between 371
centers (14, 21, 24). Our results were generated using a commercially available set of 372
quantitation standards, and a conversion factor of 0.76 IU/copy of CMV DNA was subsequently 373
calculated by calibrating the artus CMV protocol to the 1st WHO International Standard for 374
human cytomegalovirus. To our knowledge, this is one of the first reports to provide such a 375
conversion factor. Reporting clinical results in IU/mL should allow for more accurate 376
comparisons of quantitative results generated using different assays. 377
378
Previous studies have documented the ability of PCR assays to detect CMV DNA copy numbers 379
below 100 copies/mL, though the clinical significance of such values remained unclear (2, 15). 380
Boeckh et al. designed a sensitive real-time PCR assay and reported on two patients diagnosed 381
with CMV disease who had viral loads detectable in stored samples from up to seven weeks prior 382
to diagnosis (2). Kaiser et al. modified the COBAS Amplicor CMV Monitor such that they 383
could detect CMV DNA down to 20 copies/mL of patient plasma (15). They then identified 16 384
HSCT recipients with detectable CMV DNA by their new protocol. Three patients in that study 385
had low detectable viral loads that resolved without therapy. However, most patients received 386
treatment following the detection of CMV DNA, making it difficult to draw conclusions 387
regarding changes in the viral load from this report. 388
on July 12, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from

19
In HIV-positive patients with low CD4 counts, Erice et al. studied the use of a CMV antigen 389
assay (limit of detection reported as 200 copies/mL), and the reference protocol used in our study 390
(11). In univariate analysis after adjusting for HIV viral load and CD4 count, an increase in the 391
CMV copy number to >200 copies/mL during the study was significantly associated with 392
decreased survival. While the numerical cut-off used in their study cannot be generalized to our 393
population given the significant differences in testing modalities, these results support the 394
conclusion that increases in CMV viral load are significant even when initially detected at a very 395
low level. 396
397
During our study, 94.5% (n = 86) of patients had a CMV viral load that was detectable but <200 398
copies/mL, and many patients had repeatedly detectable viral loads at <200 copies/mL. The 399
finding of detectable virus at this level is difficult to interpret in isolation. However, the CMV 400
viral load continued to rise or antiviral treatment was initiated in 21 out of 22 clinical episodes 401
during which the viral load increased from <200 to >200 copies/mL. Twenty of these patients 402
eventually received antiviral treatment (Table 3), and in only a single episode did the viral load 403
decline without any intervention (from 262 to <200 copies/mL). All 21 patients in this sub-404
group had received an HSCT and were being followed using a pre-emptive treatment protocol; 405
none of them developed confirmed CMV disease. 406
407
Recommendations for the duration of treatment for CMV infection and disease are available, but 408
these have not been studied in a randomized setting (14, 17). Detectable CMV viral loads at the 409
end of treatment have been shown to predict recurrence in SOT patients, though this report 410
utilized a less analytically sensitive assay than the test used here (23). In our patients, the rates 411
on July 12, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from

20
of recurrent infection in patients with a detectable viral load at the end of therapy did not differ 412
significantly from rates in patients with undetectable CMV at the end of therapy. The number of 413
patients in this analysis was small (n = 21), however, and this merits further study in a larger 414
population. 415
416
Limitations of our study include the retrospective design and the reliance on treating physicians 417
to determine when to initiate antiviral therapy during periods of viremia. Despite these 418
limitations, we were able to demonstrate that episodes of CMV viremia eventually treated with 419
antiviral therapy can be detected earlier using a more sensitive testing method. A prospective 420
study would better define clinical benefits that may result from using the CMV threshold 421
identified here (i.e. shorter duration of antiviral therapy or decreased toxicity). While the 422
incidence of end-organ disease would provide a more rigorous end-point, its occurrence is likely 423
too rare for it to be used in this fashion. 424
425
In summary, we report the performance characteristics of an automated protocol using the artus 426
CMV PCR in comparison with a widely used reference protocol and report our findings from the 427
study of a cohort of immune compromised patients monitored with this test. In a subgroup of 428
HSCT recipients, we observed clinically meaningful increases in the viral load, even when 429
quantified at levels previously undetectable in our reference protocol. These findings support the 430
use of a low threshold for the initiation of pre-emptive therapy in transplant patients. 431
432
on July 12, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from

21
ACKNOWLEDGEMENTS 433
We thank the staff of the Stanford Clinical Virology Laboratory for their hard work, support, and 434
technical expertise. Qiagen provided the artus CMV RG PCR reagents and QIAsymphony 435
SP/AS extraction kits and consumables used for assay evaluation. 436
437
on July 12, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from
22
REFERENCES 438
1. Bland, J. M., and D. G. Altman. 1986. Statistical methods for assessing agreement between 439
two methods of clinical measurement. Lancet. 327:307-310. 440
2. Boeckh, M., M. Huang, J. Ferrenberg, T. Stevens-Ayers, L. Stensland, W. G. Nichols, and L. 441
Corey. 2004. Optimization of quantitative detection of cytomegalovirus DNA in plasma by real-442
time PCR. J Clin Micobiol. 42:1142-1148. 443
3. Caliendo, A. M., J. Ingersoll, A. M. Fox-Canale, S. Pargman, T. Bythwood, M. K. Hayden, J. 444
W. Bremer, and N. S. Lurain. 2007. Evaluation of real-time PCR laboratory-developed tests 445
using analyte-specific reagents for cytomegalovirus quantification. J Clin Micobiol. 45:1723-446
1727. 447
4. Caliendo, A. M., K. St. George, S. Kao, J. Allega, B. Tan, R. LaFontaine, L. Bui, and C. R. 448
Rinaldo. 2000. Comparison of quantitative cytomegalovirus (CMV) PCR in plasma and CMV 449
antigenemia assay: clinical utility of the prototype AMPLICOR CMV MONITOR test in 450
transplant recipients. J Clin Micobiol. 38:2122-2127. 451
5. Chou, S. 1992. Effect of interstrain variation on diagnostic DNA amplification of the 452
cytomegalovirus major immediate-early gene region. J Clin Micobiol. 30:2307-2310. 453
6. CMV R-gene product information. 2012. Argene, Inc. 454
7. College of American Pathologists. 2011. VLS-A, viral load participant summary. Surveys and 455
Anatomic Pathology Education Programs. 456
8. Cope, A. V., C. Sabin, A. Burroughs, K. Rolles, P. D. Griffiths, and V. C. Emery. 1997. 457
Interrelationships among quantity of human cytomegalovirus (HCMV) DNA in blood, donor-458
recipient serostatus, and administration of methylprednisolone as risk factors for HCMV disease 459
following liver transplantation. J Infect Dis. 176:1484-1490. 460
on July 12, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from

23
9. Einsele, H., G. Ehninger, H. Hebart, K. M. Wittkowski, U. Schuler, G. Jahn, P. Mackes, M. 461
Herter, T. Klingebiel, J. Loffler, S. Wagner, and C. A. Muller. 1995. Polymerase chain reaction 462
monitoring reduces the incidence of cytomegalovirus disease and the duration of side effects of 463
antiviral therapy after bone marrow transplantation. Blood. 86:2815-2820. 464
10. Emery, V. C., C. A. Sabin, A. V. Cope, D. Gor, A. F. Hassan-Walker, and P. D. Griffiths. 465
2000. Application of viral-load kinetics to identify patients who develop cytomegalovirus disease 466
after transplantation. Lancet. 355:2032-2036. 467
11. Erice, A., C. Tierney, M. Hirsch, A. M. Caliendo, A. Weinberg, M. A. Kendall, and B. 468
Polsky. 2003. Cytomegalovirus (CMV) and human immunodeficiency virus (HIV) burden, CMV 469
end-organ disease, and survival in subjects with advanced HIV infection (AIDS clinical trials 470
group protocol 360). Clin Infect Dis. 37:567-578. 471
12. Forman, M., A. Wilson, and A. Valsamakis. 2011. Cytomegalovirus DNA quantification 472
using an automated platform for nucleic acid extraction and real-time PCR assay setup. J Clin 473
Micobiol. 49:2703-2705. 474
13. Gor, D., C. Sabin, H. G. Prentice, N. Vyas, S. Man, P. D. Griffiths, and V. C. Emery. 1998. 475
Longitudinal fluctuations in cytomegalovirus load in bone marrow transplant patients: 476
relationship between peak virus load, donor/recipient serostatus, acute GVHD and CMV disease. 477
Bone Marrow Transplant. 21:597-605. 478
14. Humar, A., D. Snydman, and and the AST Infectious Diseases Community of Practice. 2009. 479
Cytomegalovirus in solid organ transplant recipients. Am J Transplant. 9:S78-S86. 480
15. Kaiser, L., L. Perrin, B. Chapuis, K. Hadaya, L. Kolarova, C. Deffernez, S. Huguet, C. Helg, 481
and W. Wunderli. 2002. Improved monitoring of cytomegalovirus infection after allogeneic 482
on July 12, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from
24
hematopoietic stem cell transplantation by an ultrasensitive plasma DNA PCR assay. J Clin 483
Micobiol. 40:4251-4255. 484
16. Lengerova, M., Z. Racil, P. Volfova, J. Lochmanova, J. Berkovcova, D. Dvorakova, J. 485
Vorlicek, and J. Mayer. 2007. Real-time PCR diagnostics failure cause by nucleotide variability 486
within exon 4 of the human cytomegalovirus major immediate-early gene. J Clin Micobiol. 487
45:1042-1044. 488
17. Ljungman, P., R. de la Camara, C. Cordonnier, H. Einsele, D. Engelhard, P. Reusser, J. 489
Styczynski, and K. Ward. 2008. Management of CMV, HHV-6, HHV-7, and Kaposi-sarcoma 490
herpesvirus (HHV-8) infections in patients with hematological malignancies and after SCT. 491
Bone Marrow Transplant. 42:227-240. 492
18. Ljungman, P., D. Engelhard, H. Link, P. Biron, L. Brandt, S. Brunet, C. Cordonnier, L. 493
Debusscher, A. de Laurenzi, H. J. Kolb, Messina C., A. C. Newland, H. G. Prentice, C. Richard, 494
T. Ruutu, H. Tilg, and L. Verdonck. 1992. Treatment of interstitial pneumonitis due to 495
cytomegalovirus with ganciclovir and intravenous immune globulin: experience of European 496
bone marrow transplant group. Clin Infect Dis. 14:831-835. 497
19. Ljungman, P., P. Griffiths, and C. Paya. 2002. Definitions of cytomegalovirus infection and 498
disease in transplant recipients. Clinical Infectious Diseases. 34:1094-1097. 499
20. Meyers, J. D., P. Ljungman, and L. D. Fisher. 1990. Cytomegalovirus excretion as a 500
predictor of cytomegalovirus disease after marrow transplantation: importance of 501
cytomegalovirus viremia. J Infect Dis. 162:373-380. 502
21. National Institute for Biological Standards and Control. 2010. 1st WHO international 503
standard for human cytomegalovirus for nucleic acid amplification techniques. NIBSC Code 504
09/162. 1-2. 505
on July 12, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from

25
22. Raggam, R. B., M. Bozic, H. J. F. Salzer, S. Hammerschmidt, C. Homberg, K. Ruzicka, and 506
H. H. Kessler. 2010. Rapid quantitation of cytomegalovirus DNA in whole blood by a new 507
molecular assay based on automated sample preparation and real-time PCR. Med Microbiol 508
Immunol. 199:311-316. 509
23. Sia, I. G., J. A. Wilson, C. M. Groettum, M. J. Espy, T. F. Smith, and C. V. Paya. 2000. 510
Cytomegalovirus (CMV) DNA load predicts relapsing CMV infection after solid organ 511
transplantation. J Infect Dis. 181:717-720. 512
24. Wolff, D. J., D. LaMarche-Heaney, P. D. Neuwald, K. A. Stellrecht, and R. D. Press. 2009. 513
Multi-site PCR-based CMV viral load assessment - assays demonstrate linearity and precision, 514
but lack numeric standardization. J Mol Diagn. 11:87-92. 515
516
on July 12, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from

26
Reference Protocol Total artus C
MV
P
roto
col Pos Neg
Pos 42 10 52 Neg 0 30 30
Total 42 40 82
517
Table 1. Comparison of the artus CMV protocol to the reference protocol using 82 clinical 518
samples. The 10 samples positive by the artus CMV protocol and negative by the reference 519
protocol were retested using the CMV R-gene assay. Eight of 10 samples were positive by the 520
CMV R-gene assay. 521
522
on July 12, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from

27
Transplant Recipients Patients (%)
Total 82 (100) SOT 27 (32.9) CMV status at transplant R+/D+ 15
R+/D- 5 R-/D+ 6 R+/D unknown 1 Prophylaxis
Acyclovir 3 Valganciclovir 15 None 9 HSCT 55 (67.1) Allogenic 53 Autologous 2 CMV status at transplant R+/D+ 29 R+/D- 22 R-/D+ 4 Prophylaxis 53 Acyclovir 51
Valganciclovir 0 None 2
523
Table 2. Characteristics of 82 transplant recipients with a positive plasma CMV PCR during the 524
study period. The two autologous HSCT transplants were CMV positive (R+) at transplant. 525
526
on July 12, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from
28
Subsequent Viral Load N Continued to
Increase Decreased,
No Intervention Treatment
200-400 copies/mL 9 8 1 8
400-600 copies/mL 3 2 0 3
>600 copies/mL 10 5 0 10
Total 22 15 1 21 527
Table 3: Outcome for 22 clinical episodes during which the CMV viral load increased from 528
<200 to >200 copies/mL on sequential tests. The quantifiable level to which the viral load 529
increased on the second test is expressed as the subsequent viral load. 530
531
on July 12, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from

29
FIGURE LEGENDS 532
533
Figure 1. Bland-Altman plot for the comparison of the artus CMV and reference protocols 534
using 42 clinical samples. The mean difference was zero (labeled, bold-faced line); dashed lines 535
indicate mean +/- 2 standard deviations. 536
537
Figure 2. Flowchart of the 91 adult patients with at least one positive plasma CMV PCR during 538
the study period. 539
540
on July 12, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from
30
Figure 1 541
542
543
-1.20
-0.90
-0.60
-0.30
0.00
0.30
0.60
0.90
1.20
0.00 1.00 2.00 3.00 4.00 5.00 6.00
artusC
MV
-re
fere
nce
pro
toco
l (lo
g 10
cop
ies/
mL
)
Mean (log10 copies/mL)
Mean Difference
on July 12, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from

31
Figure 2544
545
Patients with positive CMV PCR during study period
n=91
≥1 CMV viral load detected at <200 copies/mL
n=86
Viral load always <200 copies/mL
n=49
Viral load increased from <200 to >200 copies/mL
n=21
Viral load initially >200 copies/mL
n=16
Viral load always >1000 copies/mL
n=5
on July 12, 2018 by guesthttp://jcm
.asm.org/
Dow
nloaded from