CLINICAL PERIPHERALITY final report - all sections · Clinical Peripherality Characterising Remote...
117
Clinical Peripherality Characterising Remote and Rural Primary Care August 2004 This study was funded by the Scottish Executive Remote and Rural Area Resource Initiative
Transcript of CLINICAL PERIPHERALITY final report - all sections · Clinical Peripherality Characterising Remote...

Clinical Peripherality
Characterising Remote and Rural Primary Care August 2004
This study was funded by the Scottish Executive Remote and Rural Area Resource Initiative

i
Authors
Gillian M Swan RGN MSc
Research Fellow 1
Prof. David J Godden MD FRCP (Edinburgh & Glasgow)
Director 1
Kim M Walker BSc(Hons) PhD
Training and Education Manager 2
S.Selvaraj PGDCA MSc
Research Fellow/Bio-statistician 1
1
Highlands and Islands Health Research Institute University of Aberdeen The Green House Beechwood Park Inverness IV2 3BL
2
NHS Education for Scotland Forest Grove House Foresterhill Road Aberdeen AB25 2ZP
Acknowledgements The authors acknowledge and thank Helen Deasy 1 and Kay Lackie 1 for Research, Technical and Administrative support

ii
Steering group
David J Godden
Director 1
Kim M Walker
Training and Education Manager 2
Gillian M Swan
Research Fellow 1
David Pinney
Associate Adviser in General Practice 3
Josephine Stojak
LHCC General Manager 4
Angus Venters
LHCC Clinical Governance Lead 5
Ian Weatherhead
Continuing Professional Development Lead 5
1 Highlands and Islands
Health Research Institute University of Aberdeen The Green House Beechwood Park Inverness IV2 3BL
2 NHS Education for Scotland Forest Grove House Foresterhill Road Aberdeen AB25 2ZP
3 Lochaber LHCC and NHS Highland Dewar House, Highlander Way Inverness Business and Retail Park Inverness IV2 7GE
4 Argyll and Bute LHCC Lorn Medical centre Soroba Rd Oban Argyll
5 Wester Ross, S.Skye and Lochalsh LHCC Dr Mackinnon Memorial Hospital Broad ford Isle of Skye IV49 9AA

iii
EXECUTIVE SUMMARY INTRODUCTION Planning healthcare delivery and appropriate education and training for staff requires knowledge of the nature of care and the setting in which it is provided. This study describes these issues in a large remote and rural area of Scotland. The findings should be of particular relevance to providers of education and training, including NHS Education for Scotland, Royal Colleges and other professional training bodies, and Universities and further education institutions, and to healthcare providers, such as NHS Boards, who have responsibilities for funding education and training. AIM OF THE STUDY This study was designed to explore services provided by remote and rural healthcare staff and to investigate implications for training. STUDY SETTING The setting was 3 local health care cooperatives (LHCCs) in West Highland: Argyll and Bute; Wester Ross, Skye and Lochalsh; and Lochaber. Together, these LHCCS provide services in a geographic area of approximately 7,000 square miles from 53 general practices, of whom 6 have additional branch surgeries. General practices also provide cover for 9 community hospitals. METHODS A literature review of academic papers, policy and strategy documents, books and theses was performed. Appropriate consent and management approvals for data collection were obtained. Data collection took place between May and December 2003. Exploratory interviews with key personnel were carried out. A practice profile was developed for each practice community using a variety of data sources, to describe geography, demography and service provision in each practice community. These were circulated to practices for comment and correction, and the corrected profiles were used for analysis. A scoring system for the spectrum of roles provided in practice was devised, reflecting clinical services, access issues (e.g. patient access across water), additional responsibilities (e.g. helicopter escort, police surgeon) and lack of availability of specific professional support (e.g. practice nurse, midwife, community psychiatric nurse). Anonymised personal development plans from health care staff in one LHCC were analysed to describe training needs perceived by staff. A performance assessment framework was provided by each LHCC. A project officer supplied a 12-month diary summary for delivering training in one LHCC. Summary statistics were generated. Factor analysis was used to derive an index to reflect the geographic and demographic characteristics of rural practice communities,

iv
which we termed “Clinical Peripherality”. The relationship between this factor and the spectrum of roles delivered in practices was explored. RESULTS Practice Profiles Profiles were distributed to all 59 practices in the area, and 49 (83%) replied to the request for corrections and additional information. Corrections were required to only 0.39% of fields. The final practice profiles contained 115 descriptive fields per practice community. Remote practice communities were characterised by small practice list sizes, low population density, and prolonged travel times to secondary care and educational facilities, ie. greater clinical peripherality. Rural LHCCs showed higher median values and greater scatter of clinical peripherality scores compared to an urban LHCC. Numbers of visitors and temporary residents were substantial, especially when expressed in proportion to permanent residents. The spectrum of roles provided in practices was wide, and positively correlated with clinical peripherality (r=0.69) Training Needs 118 anonymised personal development plans and reviews (PDPR) were provided from one LHCC, representing 37.5% of all non-GP staff contracted to the Primary Care Trust and 50% of general practitioners in that LHCC. A wide range of training requirements was described. These could be grouped as: information technology; technical; clinical practical; clinical knowledge and management training. Particular staff groups prioritised different training needs, and there were also differences in the preferred methods of delivery: experiential, taught, personal study or method not specified. Although in interviews, managers perceived locum and “back fill” as important to allow training, this was less often mentioned in the PDPR analysis. Time and finance were commonly quoted resource needs. As well as varying across staff groups, preferred delivery methods varied with skills needed and with resources required to undertake training. Training needs perceived by individual practitioners were not necessarily aligned to institutional strategic targets. Travel distances and costs derived from the diary provided by the training officer were substantial, amounting to 76 days, 8971 miles travelled and associated costs of £3588 in one year, reflecting the reality of training provision in a remote rural geographic area.

v
SUMMARY The principal findings of the study are as follows:
?? Rural health care providers deliver a wide range of services, adopting a broad spectrum of roles.
?? The geography and demography of general practice communities can be
characterised by a “clinical peripherality” factor, which is derived from population density, GP list size, and travel time from secondary care facilities and from administrative/educational facilities.
?? Clinical peripherality and the spectrum of roles adopted by health practitioners
are positively associated, i.e. more peripheral practitioners adopt a wider spectrum of roles.
?? Clinical peripherality is associated with constraints on provision, time and
resources for training and education.
?? Training needs perceived by individuals are not necessarily aligned to institutional targets.
RECOMMENDATIONS Six main recommendations arise from this study, relating to: generic training; clinical training; delivery and scheduling of training; resources; linking personal and organisational objectives; and future research. Implementing these recommendations should be the responsibility of training organisations, such as NHS Education for Scotland and professional bodies (Royal Colleges and others), and of the Scottish Executive Health Department and individual NHS Boards, who have responsibility for prioritisation and funding of training. Some examples of such practices are already in place or in development, and that experience should be built upon.
?? GENERIC TRAINING
o Multidisciplinary rural practice management training should be available. This could include human resource management, communications, setting organisational goals, managing effectiveness, leadership and IT skills. NHS organisations should actively explore inter-sectoral training in rural communities. Consideration should be given to outsourcing non-clinical training and accessing what already exists via the local enterprise companies. Universities and Further Education organisations may wish to contribute in these areas.
?? CLINICAL TRAINING
o Multidisciplinary clinical training should be enhanced for rural health care workers.
o Rural teaching and preparation for rural teaching should be accredited as CME/CPD.

vi
?? DELIVERY AND SCHEDULING OF TRAINING
o E-health resources will be appropriate to deliver some elements of teaching and training.
o ‘Roadshow’ delivery of training is popular and should be supported, with appropriate measurement of its effectiveness.
o Innovative scheduling of training should be developed. For example, blocks of training organised on consecutive days to facilitate locum cover and minimise travel expense, appropriate timing of sessions and avoidance of peak clinical periods such as summer visitor season.
?? RESOURCES
o Allocation of resource for learning and development should align with that for rural service delivery.
?? LINKING PERSONAL AND ORGANISATIONAL OBJECTIVES
o Personal Development Plans should be linked to institutional planning and to priorities determined through patient and public involvement.
?? FUTURE RESEARCH
o Evaluation of tele-education and of the “roadshow” educational model is required.

vii
Contents
INTRODUCTION
1
THE STUDY SETTING Geography 3 History 5 Economy 6
Transport 8
GENERAL CONTEXT Rurality, Deprivation and Health 9
Influences on population 14
POLICY CONTEXT LHCC Development 15 Drivers for role development 18 Workforce policy 18 Recruitment and retention 20 Role analysis 20 Training and development 21
Profiling 22
METHODS Framing the research 23 Common elements of method 23 Profiling 28
Training and development 31
RESULTS Introduction 33 Profiling 33 Spectrum of roles in Primary Care and
General Medical Services 43
Population 45 Access 46 Factor Analysis 51 Training and development 53 Performance Assessment Frameworks 60
Rural healthcare staff training costs 61
ANALYSIS AND DISCUSSION
63
Clinical Peripherality 64 Workforce information 65 Personal development planning and
reviews 66
Resources 66 Delivery method 67 Skill requirements 67 Integrated care and development planning 68 Rural healthcare staff training 68 Critical mass 69 Strengths and weaknesses of the Study 69
viii
Limitations 70 CONCLUSIONS AND RECOMMENDATIONS
71
REFERENCES
77
ABBREVIATIONS
84
CONTRIBUTORS
85
APPENDIX 87
ix
Tables
Table 1 Settlement size classification of study area and neighbouring urban area
3
Table 2 List of engagements with stakeholders 26 Table 3 Funnelling of field codes into groups for data analysis 32 Table 4 Response rates for return of community profiles by LHCC 34 Table 5 Classification of practices by LHCC 34 Table 6 Practices and professional support by LHCC 34 Table 7 The number of practices providing dedicated clinics by LHCC 35 Table 8 The number of practices with quality assessment and teaching
commitments by LHCC 35
Table 9 The number of practices supplying unscheduled care and related services by LHCC
36
Table 10 The number of practices combining General Practice duties with associated community roles by LHCC.
36
Table 11 Example of confirmed profiles from general practices with limited nurse resource where clinical escort may be required for patient transfer by air
40
Table 12 Tourist activity figures for 1999 showing ratio of resident: visitor bed nights
42
Table 13 Scoring system for Spectrum of roles 44 Table 14 Use of ferry to access Health Board by LHCC 48 Table 15 Use of ferry to access Acute receiving hospital by LHCC 49 Table 16 Skills requirement by staff discipline 53 Table 17 Details of skill needs where respondents were greater than 10. 54 Table 18 Skill levels by staff disciplines 54 Table 19 Delivery methods identified by staff disciplines 55 Table 20 Details of delivery methods where respondents were greater than
10. 55
Table 21 Resource needs by staff disciplines 56 Table 22 Skill needs by skill levels 56 Table 23 Delivery methods and skill needs 57 Table 24 Resource needs and skill needs 58 Table 25 Delivery method and skill level 58 Table 26 Resource needs and skill levels 58 Table 27 Resource needs and delivery method 59 Table 28 Diary summary of a rural project training officer 61
Maps
Map 1 Map of the West Highland study area 4 Map 2 Highlands and Islands Enterprise map of Fragile Areas 7
x
Figures
Figure 1 Evans and Stoddart model of Public Health 10 Figure 2 Common elements of the investigation 24 Figure 3 Progress of investigation – Profiling 28 Figure 4 Progress of investigation – Training and development needs 30 Figure 5 The incidence of emergency, urgent and air transport use by
LHCC for 2002-2003 37
Figure 6 The incidence of emergency road ambulance use in each LHCC showing summer and winter frequency for 2002-2003
38
Figure 7 The incidence of urgent road ambulance use in each LHCC showing summer and winter frequency for 2002-2003
38
Figure 8 The incidence of air ambulance use in each LHCC showing summer and winter frequency for 2002-2003
39
Figure 9 The annual average of time (minutes) from emergency call to hospital care by ambulance station, broken down into response time, time on scene and travel/transfer time.
41
Figure 10 A summary of service provision for temporary and emergency patients in a sample GP practice.
41
Figure 11 Temporary residents per GP by LHCC 42 Figure 12 Spectrum of roles score for each main practice by LHCC 43 Figure 13 Population Density at the location of the GP surgery by LHCC 45 Figure 14 Population density at ward level by LHCC 46 Figure 15 Scottish Index of Multiple Deprivation: scores for ‘practice
community’ access deprivation by LHCC 47
Figure 16 Total travel time to Health Board by LHCC 47 Figure 17 Illustration of miles of single track road between GP practice
address and Health Board by LHCC 48
Figure 18 The total travel time to Acute receiving hospital by LHCC 49 Figure 19 Illustration of the length of single-track road between GP
practice address and acute receiving hospital by LHCC 50
Figure 20 Clinical Peripherality indices by LHCC 51 Figure 21 Association between Access (SIMD) and Clinical
Peripherality 52
Figure 22 Association between Spectrum of roles score and Clinical Peripherality
52
xi
Draft Report Distribution List
Eric Jespersen Argyll and Bute LHCC Colville Laird BASICS Gill MacVicar East Highland
Community Health Partnership Jim Douglas Fort William Ken Proctor NHS Highland Gillian Needham NHS Education for Scotland Annie Ingram North of Scotland Planning Group Gordon Baird Royal College of General Practitioners,
Rural Practice Group Stuart Cable Royal College of Nursing Andrew Marsden Scottish Ambulance Service


1
INTRODUCTION Principles for the delivery of health services in remote and rural areas, endorsed by the Solutions subgroup of the Remote and Rural Areas Resource Initiative 1 include patient-centred care, equity of provision, local management, and appropriate training and education for health care professionals. It has been suggested that, in the rural or remote setting, every gap in service at LHCC level is filled by other generalists, resulting in a need for broad-spectrum practice and appropriate provision of training. This study was conceived when the vehicle through which primary care services were coordinated and delivered was the Local Health Care Co-operative (LHCC). Generic training needs of LHCCs have been identified in a review by Audit Scotland 2 and more recently in Health Board Performance Assessment Frameworks (PAF) for Primary Care. This project explored the concept that remote and rural LHCCs may have particular characteristics, which would influence their provision of services and their approach to training and education of professionals. These might include their geography and demography and a need to break down traditional barriers between health care workers to allow new skill mixes to emerge. A number of remote and rural LHCCs had begun, independently, to review their service provision and to explore strategies for training and education of professionals. The project brought together 3 LHCCs from West Highland to work with managers and researchers from NHS Education for Scotland (NES) and the Highlands and Islands Health Research Institute. The initial aims were to explore: the profile of the service provision expected of a remote and rural LHCC; the training needs of a remote and rural LHCC and a strategy by which these might be met; the development of a robust and meaningful rurality index for practices. Each of the LHCCs was making progress with service definition, provision and training needs but was processing information in different ways. At the time of the study, further administrative reorganisation in the NHS was imminent. Community Health Partnerships (CHPs) were to become administrative units for integrated care, created from the building blocks of the LHCC initiative. In order to provide data that would have relevance independent of the current higher level administrative structure, this project focused on the characteristics of practice communities and the training needs of individuals within the LHCC. The principal objective of the study was refined: 'To identify the purpose and needs of remote and rural healthcare staff - implications for training' This was addressed by a literature review followed by two separate, but related strands of investigation: 1. An exploration of factors affecting service provision in remote and rural LHCCs.

2
2. A profile of the training needs of staff in a remote and rural LHCC and a strategy
by which these might be met. In addition a ‘practice community’ profiling dataset was created from a variety of national and local data sources. Information was included where it was objective, available at sub LHCC level, and capable of linkage to local practice postcodes. Performance assessments for Primary Care had been made available through the Performance Assessment Framework (PAF) model. A protocol was developed to access anonymised personal development plans. Detail was collected from analysis of the Personal Development Plans of a typical rural LHCC with management approval from the NHS Trusts involved. This report describes the historical, geographical and policy context for the study, followed by the methods and results for each strand of investigation. The findings are discussed and conclusions drawn.

3
THE STUDY SETTING The study took place within 3 LHCCs in West Highland: Argyll and Bute; Wester Ross, Lochalsh and Skye; and Lochaber (Map 1). Geography Argyll and Bute LHCC covers a geographical area of 2,600 square miles with 26 populated islands and is divided into 6 localities, each of which has a community hospital. There are 30 GP practices within the area and the practice locations date from 1912 parish boundaries, which means that practices are located approximately 15 –30 miles apart.3 Wester Ross, Lochalsh and Skye covers an area of approximately 2,388 square miles and includes the islands of Raasay and Soay. Much of the area is remote and rural with many communities being accessed by single-track roads or ferries. There are 12 GP practices and 2 community hospitals. Lochaber LHCC covers an area of 2,003 square miles. The main population base is Fort William, much of the remaining area is remote and rural with many communities being accessed by single-track roads or ferries. There are 11 GP practices and 1 Community hospitals. There is a range of settlement size in the study area. Using methodology developed by The Platform Project,4 general practice codes were linked to settlement classification defined by the Scottish Household Survey (SHoS).5 The results are shown in Table1. The vast majority of practices are in the more remote categories. Information about a neighbouring urban LHCC, Inverness (an area of 405 square miles), is shown for comparison. Table 1: Settlement size classification of study area and neighbouring urban area SHoS Level 2:
Urban areas (settlements of 10-125,000)
SHoS Level 3: Accessible small towns (settlements of 3 – 10,000 and within 30 minutes drive of a settlement of 10,000 or more)
SHoS Levels 4-7 A range of settlement sizes at varying drive times from other settlements of differing size
SHoS Level 8: Very remote rural
(settlements of <3,000 and over 60 minutes from a settlement of >=10,000)
West Highland
5% 5% 17% 73%
Inverness
84% 16% 0% 0%

4
Map 1: Map of the West Highland study areaa
a © Hugh Noble www.tartanhen.co.uk
5
History The distress of the Highland population following failure of the potato harvest in 1836 received comment in the mid 19th century Royal College of Physicians of Edinburgh report. The Royal Commission was the first formal bid to make destitution and the lack of medical aid a matter of public concern and this led to the reform of the Scottish Poor law in 1845.6 The difficulties of travel, rural depopulation, doctors’ income, inferior diet and insufficiency of the existing supply of nurses were highlighted in a report to His Majesty’s Treasury in 1912 chaired by MP for Inverness-shire, Sir John Dewar. This early qualitative research into health in the Highlands and Islands 7 included the area currently described as West Highland ‘… in which isolation, topographical and climatic difficulties, and straitened financial circumstances are found most generally in combination.’ In this manner ‘Highlands and Islands’ became something of a ‘laboratory for administrative and legislative experiment’ 8 which encompassed not only the dependence of the population on local benefactors for health care but also subsidy of doctors to improve their working conditions and encourage residency in an area of need. An example is available from estate recordsb, which describes a legal and financial agreement between landowner and doctor ‘…who was to attend free of charge all paupers, estate workers and those unable to pay fees…The doctor had to keep a horse and be in readiness day and night for emergencies.’ These early records of rural deprivation led to many changes, the most telling being the removal of the financial transactions between benefactor, doctor and patient following the Highlands and Islands Medical Grant Scheme in 1913, ultimately a pattern for the 1948 National Health Act. However, the West Highland problem did no t then simply fade away. The West Highland survey of 1955 9 describes public health issues such as low employment, supply of water and housing and includes an illustration of the distribution and role of healthcare workers. A review of acute services in the same area in 2002 10 recognised the role of local hospitals as part of the wider economic and social environment and concluded that the current acute service arrangements in West Highland were fragile and could not be sustained. In promoting a different model of health care, reference is made to remote communities in other countries where the focus shifts from locally delivered acute care to high quality primary care and emergency transport services. However Highland Care services face a growing caseload of the terminally and chronically ill, as the increasingly aged indigenous population is augmented by the in-migration of other senior citizens. 3,11 20% of Health and Social work establishments in Scotland have ‘hard to fill’ vacancies. Skye, Lochalsh, Lochaber, Argyll and the Islands feature in the top 8 of the Local Economic Fora league tables of establishments anticipating recruitment difficulties.12
b William Fraser of Kilmuir and Snizort, Skye, records lodged in Inverness Archives Office
6
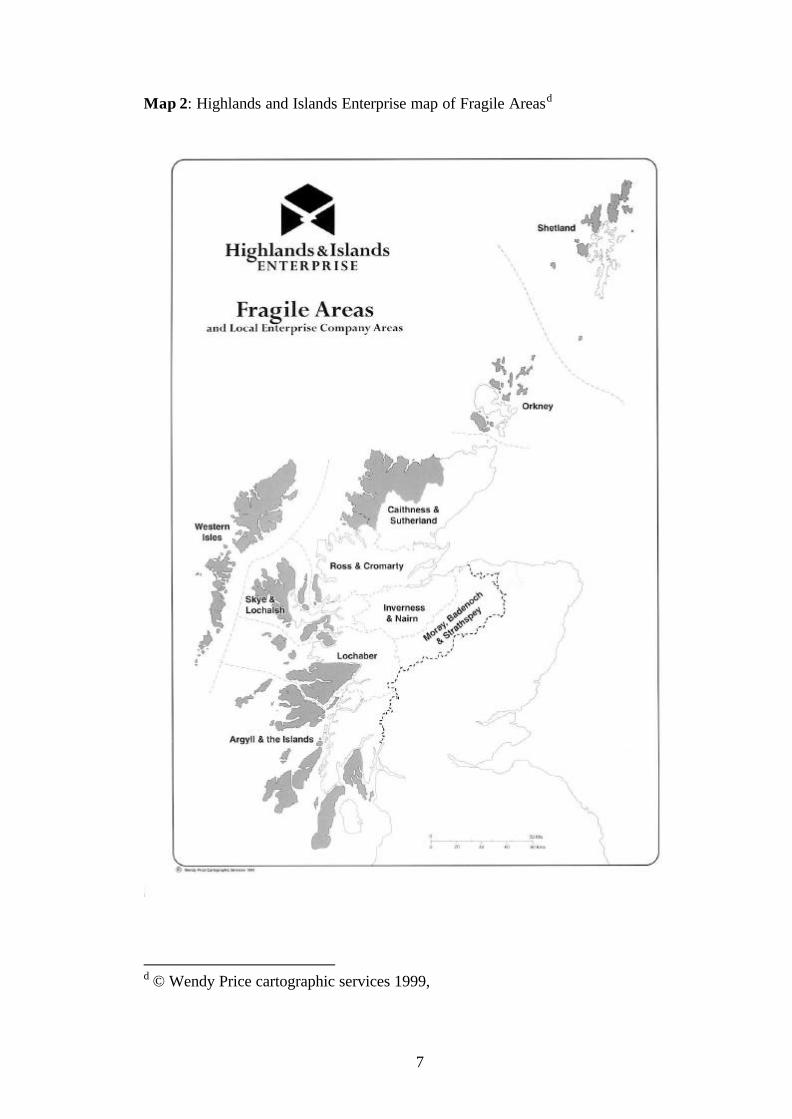
Economy The Scottish Enterprise community uses the term ‘fragile’ to describe economically and socially disadvantaged areas. Parts of the Highlands and Islands area with long term structural problems of economic declinec are classified on the basis of 12 criteria which can be broken into 3 main types: geographic, demographic, and economic. Not all criteria have to be satisfied for an area to be designated as fragile. Geographic markers of fragility include: islands that lie off other islands and are not linked by a causeway; communities at a distance of more than 50 miles from a population centre of 5000 and those areas where over 70% of roads are single track. Demographic markers of fragility include islands with populations of less than 2,500 and areas of population density less than the Highlands and Islands Enterprise (HIE) area average (9 persons per square kilometre). Also included are communities where more than 20% of the population is of pensionable age, where there has been population loss between the last 2 censuses and where in-migration of the economically active is below the HIE area average. Economic markers of fragility include economic activity rates which fall below the HIE area average, high average and/or seasonal unemployment, long term unemployment more than 25% above the HIE area average and high dependency on primary sector employment. A map compiled from the HIE collection of data demonstrates the overlap of fragile areas with the study area. (Map 2) The service sector is the major employer in the area.12 Seasonal shift of employment opportunities are most notable in the Islands, however all areas rely on seasonal activity such as tourism, fish farming, fishing, farming and forestry.
c Personal communication Highlands and Islands Enterprise June 2003
7
Map 2: Highlands and Islands Enterprise map of Fragile Areasd
d © Wendy Price cartographic services 1999,

8
West Highland faces economic decline. Contributory factors are complicated by access deprivation, population shifts, out-migration of young people, ageing population and recruitment and retention difficulties of professional healthcare staff groups.1, 3, 13
Transport Roads and infrastructure Lifeline roads are defined as being roads that are the sole means of accessing particular communities, or where an alternative route would involve a considerable increase in road distance and journey time.14 The total length of lifeline roads in the study area is 1157 Km and these roads service communities with a total population of 9600. The emphasis to slow the growth of road-based transport by transferring to rail has little relevance in the Highlands and Islands as much of the region is distant from rail terminals. There has been growing attention to the possibility of sea transport. Both rail and sea terminals require connecting road transport and there is continuing reliance on road transport as the most effective and appropriate means of moving small volumes on a regular and frequent basis. Whilst car ownership in rural areas may be high,15 access can still be limited by how the car is used i.e. a car used for work will be unavailable for access to local healthcare facilities between 9 am and 5 pm. 16 Public transport The importance of having access to a public transport service is high for those who live in rural areas. ‘public transport is essential in rural areas, notably to meet the needs of the elderly, teenagers and households without a car’17 The transport choices in the study area include air, sea, road and rail transport. These services are limited by financial viability as described in the example below: Ferry provision Good sustainable transport and travel facilities are essential in supporting the fragile economies of peripheral and island communities.18 Problems for the ferry provider include: ?? Traffic volume on the ferry routes is low overall and reduces the opportunities for
economies of scale. ?? Overcapacity is unavoidable due to geographic restrictions on schedules and the
need to cope with peak periods. ?? Elements of service are maintained for social reasons rather than commercial,
including most winter service. ?? Capital outlays are high and expected returns on capital are essentially low.
9
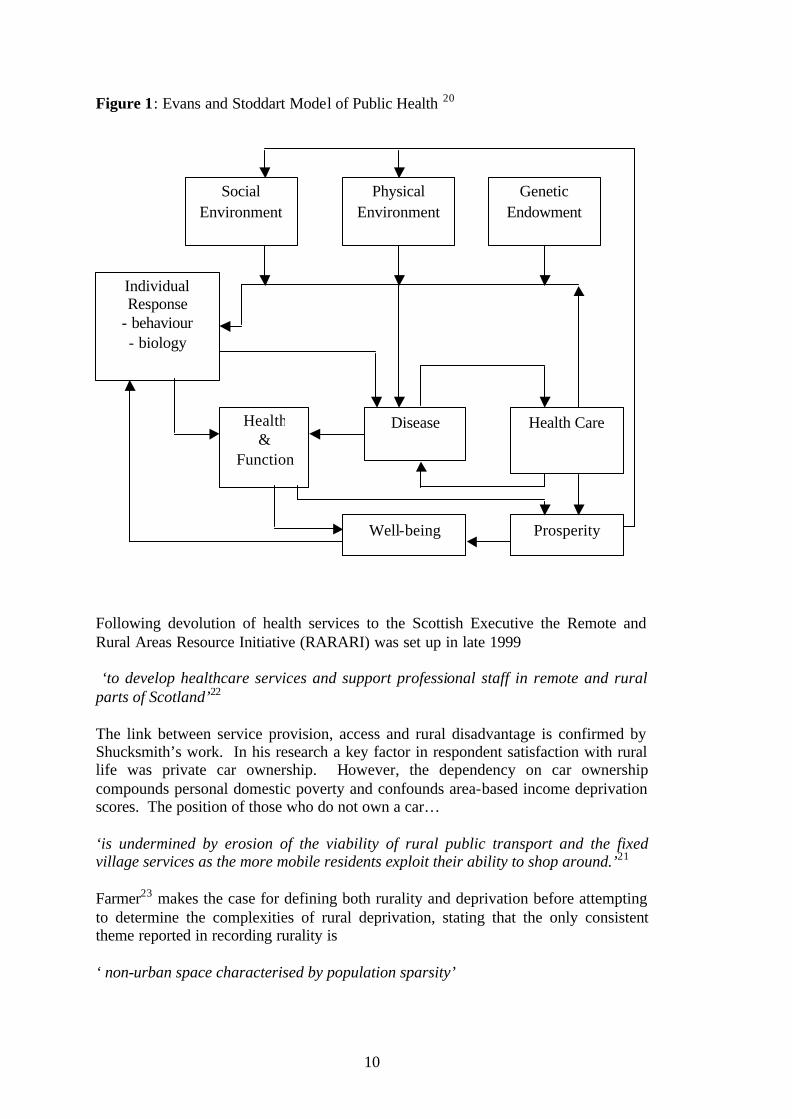
GENERAL CONTEXT Rurality, Deprivation and Health The association between socio-economic circumstances and health is well established. The World Health Organisation lists interrelated aspects of population health and it is possible to make an association with rurality. Discussion of social determinants of health includes: ?? How the social and psychological environment affects health ?? The impact of work on health ?? The problems of unemployment and job insecurity ?? The role of friendship and social cohesion ?? The dangers of social exclusion ?? The need for policies to prevent people from falling into long-term disadvantage ?? The need to ensure access to supplies of healthy food for everyone. In recent years the European Conference on Rural development, meeting in Cork, discussed sustainability of rural development. 19 Within a 10-point plan of action this aims to include: ‘…reversing rural out-migration, combating poverty, stimulating employment and equality of opportunity, and responding to growing requests for more quality, health, safety, personal development and leisure, and improving rural well-being.’ Studies in Scotland have determined that rurality and disadvantage are linked.17 The Scottish Needs Assessment Programme (SNAP) is part of the quality initiative in Scotland. 20 It focuses on assessing health, populations, need and multi-agency interventions for public health. This reflects the Evans and Stoddart model for public health, which links all relevant aspects of living, professions and services. The model shown in Figure 1 establishes the greater picture of population health and draws attention to the interdependency of relevant factors. Shucksmith 17described disadvantage as… ‘the inability of individuals or households to share in styles of life open to the majority‘ and discusses poverty ‘……as potentially both a predisposing factor and an outcome of disadvantage, outstanding factors being old age, low wages and employment opportunities.’ There is recognition of the need to understand the processes causing rural disadvantage and the uneven impact on different groups and areas. ‘…not only are rural societies and economies changing under the influence of internal and external factors, but representations of rurality are also changing…’21
10
Figure 1: Evans and Stoddart Model of Public Health 20 Following devolution of health services to the Scottish Executive the Remote and Rural Areas Resource Initiative (RARARI) was set up in late 1999 ‘to develop healthcare services and support professional staff in remote and rural parts of Scotland’22 The link between service provision, access and rural disadvantage is confirmed by Shucksmith’s work. In his research a key factor in respondent satisfaction with rural life was private car ownership. However, the dependency on car ownership compounds personal domestic poverty and confounds area-based income deprivation scores. The position of those who do not own a car… ‘is undermined by erosion of the viability of rural public transport and the fixed village services as the more mobile residents exploit their ability to shop around.’21 Farmer23 makes the case for defining both rurality and deprivation before attempting to determine the complexities of rural deprivation, stating that the only consistent theme reported in recording rurality is ‘ non-urban space characterised by population sparsity’
Social Environment
Physical Environment
Genetic Endowment
Individual Response
- behaviour - biology
Health &
Function
Disease Health Care
Well-being Prosperity

11
The Randall definition of rurality 24 is ‘those Local Authority districts which have a population density of less than 200 persons per square kilometre’; the OECD definition of rural ‘<150 persons per sq km’ and more recently the Scottish Household Survey classification of settlements are used as measures of rurality. 25, 26. However populations are better represented when their rurality and deprivation are determined by multi factor descriptions.17, 27 Many deprivation indicators in current use are produced from the large 1991 and 2001 Census datasets to produce area based measures 28 although current deprivation indicators are under review.29 The Scottish Centre for Research on Social Justice (SCRSJ) group draws attention to social cohesion and determines that social exclusion resonates with the domains included in many indices of area deprivation. The Scottish Index of Multiple Deprivation (SIMD 2001), derived from the 2001 census data set, is indexed to Council ward areas and determines multiple domains of deprivation that may more readily reflect the disadvantages of rural life in Scotland.30 These are ?? Health deprivation and disability ?? Education, skills and training ?? Income deprivation ?? Employment deprivation ?? Geographical access to services. The South West Public Health Observatory note that… ‘most commentators choose definitions and measurement systems that are best suited to their own application,’ 31 …and cite Higgs on the question of whether evidence of rural-urban differentials in health service need and utilisation has been subject to methodological artefact. In an attempt to draw together information from various data sources, the Platform Project 4aims to: maximise the use of existing data-sets collected from primary care health service; describe the relationships between the resources available; inform the choice, design and location of further studies. However Farmer recommends caution in using large area measures for the needs of small communities highlighting the difficulties inherent in… ‘…drawing of inferences about individuals directly from evidence gathered about a group… a promising area score might mask significant pockets of deprivation.’23 In recognition of this, Highland Health Board used GP populations and communities as a smaller area measure in creating a link between rural health service access factors and known population groups.32 Key to the development of understanding the costs of delivering services in rural areas was the report ‘Fair Shares for All’33 (the Arbuthnott report). That review concludes that an excess cost adjustment should be applied to a range of programmes

12
where delivery is complicated by remoteness and subdivides the range into two further components:
Services provided by travelling professional staff Services provided from fixed locations
The report recognises the increased levels of travel for community nurses: ‘…which amounts to 200 miles per week in some areas. By far the largest component of this is lost nurse time exacerbated by congestion during the tourist season.’ Continuing the theme of remoteness, commissioned researche found that ‘…providing nursing care in rural and remote areas may require higher grade nurses than in more urban areas and demand from them a wider portfolio of skills. This allows them to carry out a full range of tasks in their patch (including, for example, midwifery duties and, where a GP is located across water, basic Accident and Emergency and primary care cover) and to operate without support where the size of the local population does not justify the deployment of auxiliary and lower grade nurses. This approach raises the cost of care… but it will also be more efficient than employing under-utilised auxiliary personnel.’ …and also found that relative additional costs were incurred by remote and rural areas for education and training as a result of travel costs, accommodation costs and the costs of providing service cover during training. Discussion about the merits of quantitative and qualitative measures of rural health care provision continues, and in the September 2003 report into Maternity Service Provision in Scotland24 the authors quote Rourke whose definition of rural health care is ‘…practice in non-urban areas where most…care is provided by a small number of general practitioners with limited or distant access to specialist resources and high technology health care facilities’. Murray et al1 describe the difficulties of providing health care in rural Scotland. They list potential solutions and ongoing management issues. Discussion includes patient centred care through local management, equity of access by addressing recruitment and retention, on-call duties, time to definitive care and training and education, and having due regard for family support within the rural, social and economic infrastructure. The training and education needs of rural professionals are perceived to be different from urban colleagues; this is partly because of the generalist nature of the work. Douglas 34 makes reference to the spectrum of care and provision in remote and rural areas in his hypothesis for a scoring system for remote practice – ‘The Townsville
e National Economics Research Associates field work report in ‘Fair Shares for All – Technical report’

13
score’. There is a suggestion that as rurality increases so too does the range of care required of the isolated practitioner. The difficulties of health care provision are compounded by population sparsity and increased travel times between patients and facilities. Domains in the SIMD 2003 series 30 provide objective data on the access and health deprivation levels that conspire to increase the workload, recruitment, retention and education difficulties of rural healthcare staff. The providers of care in remote and rural areas also fall prey to the same levels of access deprivation as their clients. Influences on population Most General Practices monitor year on year trends in numbers of temporary residents.f Three types of temporary residents are recorded for treatment: people in the area for less than 24 hours (emergency treatments); for between 24 hours and 15 days; for greater than 15 days (temporary residents) who will not be joining the practice list. Not all temporary residents are tourists or visitors. For example, school children attending high school from their remote homes stay at the weekly boarding hostel. They are seen as temporary residents but are registered with their "home" GP. University students, home for the holidays might be another example, as might temporary workers (such as hotel staff - often from overseas) on medium term contracts who remain registered with a GP elsewhere. Not surprisingly tourist activity does significantly boost road accident numbers in the rural tourist areas of Scotland. In rural areas 30% of road accident casualties are fatal or serious, in urban areas (defined as a settlement of 500 people or more) only 19% are fatal or serious.35 In 2000 Northern Constabulary recorded the highest national rate of accidents involving non- local drivers. The overall casualty rate was the second highest nationally at 5.8 per 1000 population. There is a close association between casualties and traffic flow. The need for accident rescue and road casualty care is more acute in areas of population sparsity.
f Personal correspondence D. Pinney, Associate Adviser, Lochaber 2003

14

15
POLICY CONTEXT LHCC Development
The creation of Primary Care Trusts (PCTs) and LHCCs were recommendations in the white paper ‘Designed to Care’.36 LHCCs were described as ‘voluntary organisations of GPs which will strengthen and support practices in delivering care to their local communities’. The key objectives were listed: ?? Provide services to their patients within an identified level of resources including
expenditure on prescribing ?? Work with the support of public health medicine to develop plans which reflect
the clinical priorities for the area, whilst taking into account specific health needs of the registered patient population covered by the co-operative
?? Support the development of population-wide approaches to health improvement and disease prevention, which require lifestyle and behavioural change
?? Improve the quality and standards of clinical care within practices and to support clinical and professional development through education, training research and audit
?? Support the development of extended primary care teams which are formed around the practice structure, and promote the development of clinical expertise and the emergence of specialisms within primary care.
Primary Care Trusts came into being in April 1999 and the general principles for LHCC development were set out. It was stressed that there was no one model and that the scope and functions of LHCCs were to be determined by agreement with the member GP practices and the PCT. There was little guidance and doubt was expressed 37 about the effectiveness of LHCCs in achieving health gain, engagement with the acute sector, effect on patient care. LHCC development workshops were held in 2000g and the vision of the presiding Minister for Health was to: increase patient involvement and satisfaction with the health and social care they receive; increase the scale of partnership working with local authorities, the acute sector and voluntary agencies; tackle inequalities and improve access to primary care services. The Health Plan of 2000 38 reiterated the role of LHCCs as vehicles for change. The LHCC Best Practice Group was established in May 2000. Supported by the Primary Care Unit of the Scottish Executive it was composed of people working in or with primary care. It was to include a wide range of disciplinary perspectives and areas of expertise rather than representatives of particular professions or organisations.
To inform the work of the Best Practice Group a joint survey with Audit Scotland was undertaken h and reported in April 200139. At that time Audit Scotland examined 79
g http://www.show.scot.nhs.uk/lhcc/LHCC accessed April 03 h Local Healthcare Co-operatives Bulletin http://www.audit-scotland.gov.uk/publications/pdf/01h07as.pdf accessed April 03
16
LHCCs across Scotland, a series of partnerships covering 952 general medical practices. They list the minimum functions of an LHCC as: ?? Community care planning and provision with local partners ?? Management of Primary and Secondary care services for child health, mental
health and older people ?? Public involvement ?? Health Improvement ?? Community planning. Recognising that LHCCs were no longer the organisations envisaged in ‘Designed to care’ the report informed the change agenda for NHS trusts 40 and in July 2001 the new LHCC Professional Committee 41 was described as an independent committee with the same status as other area Professional Advisory Committees. Its remit included:
?? Active involvement in the service design, redesign and development agenda for
the local health care system ?? Sharing in the task of advising the NHS Board on proposals and programmes
which will improve the integration of services both within local health care systems and across health and social care
?? Contributing to the NHS Boards development of the Local Health Plan and its strategic objectives
?? Advising the NHS Board on service improvement through the development of multi-disciplinary working
?? Advising the NHS Board on service developments within primary care and their workforce implications and on achieving the right skill mix within the NHS Board area.
The same report describes PAF as a method of collecting information, through self-assessment, on the progress made towards achieving this agenda for PCTs. The LHCC Best Practice Group concluded in its report that a ‘one size fits all’ approach remains inappropriate and recommended that: LHCCs may require to merge or develop local partnership agreements with other LHCCs; LHCCs and local authorities should review boundaries to maximise alignment as a basis for joint management; NHS Boards should ensure that additional resources are devolved directly to LHCCs to address local priorities. The Primary Care Modernisation Group in March 2002 42 discussed the development of local policies to ensure that all staff, both allied and employed, have equal access to training and development to support individual and team learning and recommend that nationally there is appropriate emphasis on the needs of Primary Care multidisciplinary working and learning. LHCC development needs are listed and have since been included in the white paper ‘Partnership for Care’ 43 and in ‘The Partnership Agreement.’44 This continues the theme of single system working in health and strong collaborative approaches with communities. The white paper calls for the development of Community Health

17
Partnerships (CHPs) from the building blocks provided by LHCCs and accords with the conclusions of the Best Practice group. This is facilitated by recent legislation. ‘…to ensure that NHS Boards devolve appropriate resources and responsibilities for decision-making to frontline staff and establish CHPs as an effective basis for the delivery of healthcare services.’ 45 Thus we have moved in 4 years from a voluntary partnership agenda to a legal administrative framework.

18
Drivers for role development Workforce policy The administration of Scotland is committed to implementing the European Union regulations and the ‘Working Hours Directive’ 47 has far reaching consequences for health service provision. Specifics of holiday allowance, rest periods and shift working are at variance with the traditional image of the rural practitioner who is on call for 24 hours per day. The final provisions of the Directive state ‘-no worker is (to be) subjected to any detriment by his employer because he is not willing to give his agreement to perform such work’. The Acute Services Review of 1998 48 identified issues of concern in remote and rural healthcare provision that included lack of integration and difficulties of delivery due to historical NHS systems and diseconomies of scale. It recognised that there was no advocacy for remote and rural issues that include recruitment and retention difficulties and professional isolation. The implications of the European Union (EU) Working Time directive and clinical governance drivers for increasing professional specialism was to be balanced against a service need for generalism. Doctors The Temple report ‘Future Practice’ 49 focuses on the development of the medical workforce within a multi-professional context. Two of the key messages have relevance to those working in remote areas: ?? Team delivered care is an overarching theme ?? Travel time increases the clinical risk for emergency care but so can lack of
capacity, critical mass or experience in a small unit.
The report concludes ‘The medical workforce in Scotland is under pressure. Service demand is rising and will continue to rise; the capacity to respond is already limited and will be further restricted as the Working Time Directive is applied across the workforce and as practitioners seek and expect less demanding hours of work. The service will only survive with change’. A key objective of the new General Medical Services (GMS) contract 50 has been to address the issues of practice workload. In striving for flexibility of service provision, practices will have the opportunity to opt into a wider range of enhanced services and where recruitment problems exist, they will be able to opt out of the provision of additional services. Primary Care organisations will be responsible for ensuring that patient access to services is not compromised. There has been much debate nationally about the impact that this will have on every GP and also about the added effect of the impact on rural communities distanced from centralised Acute health services. It is anticipated that future delivery of Primary Care by GPs will: ?? Provide new flexibility to determine the range of service they wish to provide

19
?? Reward clinical and organisational quality ?? Facilitate modernisation of practice infrastructure ?? Provide guaranteed levels of investment and allocate resources on an equitable
basis. Making the best use of the skills of nurses and midwives was a principle of ‘The New Deal’ 51 and was born out of the desire to regulate the hours of work of junior doctors in training. Doctors in Acute care were the first to benefit from the guidance as the opportunity to share clinical work with nurses, midwives and allied health professionals became commonly accepted. Nurses In 1999 ‘ Towards a Healthier Scotland’ 52 recommended that there should be a review of the contribution of nurses to improving the public’s health. ‘Nursing for health’ 53 was published in 2001 and set out this agenda. A year later NHS boards were asked to comment on progress by contributing to a report summarising achievements. 54 Further effort is identified for the following topics: ?? The infrastructure to support nurse involvement in community development work ?? School nursing services are part of Primary Care Trusts and are to play a full role
in the work of LHCCs ?? GP representatives to facilitate effective teamwork and health improvement
activity around maternity care and child health through the GP contract ?? Trusts should ensure that more effective use is made of nurses with specialist
expertise ?? A mechanism for commissioning community nursing education to meet the needs
of current and future practice. The World Health Organisation proposed a new type of nurse to be based in local communities 55 and the Scottish Executive saw this as a potential solution to some of the problems of providing health care in rural Scotland.56 The role of the Family Health Nurse is summarised as: ?? A skilled generalist role encompassing a broad range of duties ?? A model based on health rather than illness ?? A role founded on the principle of caring for families ?? A concept of the nurse as first point of contact
At the end of the first year of practice in this role the evaluation team suggest that there are 2 factors that make a Family Health Nurse role work: the perceived scope and space to encourage implementing the approach; and the local presence of at least one active supporter who changes their own practice.57 It is also suggested that these factors alone are not sufficient and to develop the role further advise: ?? A programme of support and facilitation of the development at site level ?? Active team review of case loads and working practices ?? Concurrent review of nursing resources and skill mix ?? Delegation of family health nursing work.

20
Midwives Concern has been raised for the quality and sustainability of maternity services in remote and rural settings. A full scoping exercise and exploration of best practice was published in September 2003.24 Given the change agenda, the difficulties of staff recruitment and population migration, the difficulties faced by midwives are not unique.50 Pharmacists Dispensing is seen as a way of ensuring financial viability for GPs in rural areas although the scheme has caused conflict between the medical and pharmacy professions.59 ‘Our National Health’ underlines the pharmacist’s role as a member of the NHS team of care providers and more recently it is suggested that the involvement of pharmacists in 3 quality topics will be addressed through systematic approaches and closer collaboration with the Primary care team: providing effective treatments; preventing adverse reactions; reducing waste.
Dentists Both pharmacists and dental practitioners have difficulty establishing financially viable practices in remote areas with low-density populations. The ratio of General Dental Practitioners to population is low in remote and rural areas and service access and provision is further confounded by the difficulties with distance and travel.60 Allied Health Professionals Allied health professionals are involved in the planning of patient care, and anticipate full involvement in team education and training with doctors and nurses as they contribute to standards to guide practice.61 Where the population base does not justify daily access to these staff groups, nurses and doctors undertake the communication roles of triage and referral. Recruitment and retention Recruitment and retention of staff is a thread running through recent health policy in Scotland and in particular in rural health service strategy. 42, 56 Some reports have recommended a ‘golden hello’60 or relocation and incentive packages1 others encourage rural placements during training 24 Recruitment difficulties underpin many of the ambitions to develop multidisciplinary teams and flexible working 42 and will be supported in future by workforce planning officers at national, regional and local level. 63 Role analysis The ‘Agenda for Change’64 is a modernised NHS pay system for all staff groups except doctors. Described in 2003 for implementation in October 2004, this takes account of knowledge, skills and responsibilities in allocating jobs to new pay bands. At the time of reporting a full appraisal of health service roles is underway. Some assessments have been completed and community work is recognised as requiring
21
different skills. For example, the “job evaluation score” for Health Care Assistants is 185-205. In the community this rises to 199-212. The key points of difference are: increased autonomy in communication, relationships and freedom to act; physical skills of driving and use of keyboard; mental effort in driving and frequent exposure to distressing or emotional circumstances. Training and development The ‘NHS in Scotland’ human resources strategy was launched in 1998 65 and a number of policies and developments are implemented by NHS organisations. Quality care was the desired result of Learning Together, 66 a strategy for education, training and lifelong learning for the NHS in Scotland that embraces four key concepts:
Lifelong learning Learning organisations Access and opportunity Careers development
This framework also includes a challenge to staff ‘to take responsibility for their own learning’. The NHS Scotland staff governance standard was first proposed in 2000 38 and published in 2002 67 stating that: ‘Staff governance is a system of corporate accountability for the fair and effective management of all staff’ Five standards, which employers are expected to deliver, entitle staff to be: well informed; appropriately trained; involved in decisions which affect them; treated fairly and cons istently; and provided with a safe working background. ‘Working for Health’ 68 identifies the mechanisms for delivery of workforce development at local levels, and describes the responsibilities of workforce officers and the infrastructure of the NHS National Workforce Unit. The report describes an approach that secures a national focus for remote and rural workforce development.

22
Rural profiling Several studies and policies have used measures of rurality to develop strategies appropriate to rural environments.33, 49 Others have used rurality as an explanation of the difficulties of service provision 24, 57 Farmer notes that the only common explanation of rurality is based on a measurement of population density. 23 The Scottish Index of Multiple Deprivation 30 captures data on access deprivation and the 2001 census indicates the population density both at settlement and ward level. Scottish Neighbourhood Statistics 69 give indicators of population distance from essential services such as hospital, GP or Dentist. Rural clinical effectiveness studies and audit have shown that road traffic accidents are more frequently fatal, 35 presentation of outdoor activity casualties increases with the tourist season i, ambulance response is less rapid for all emergencies (ORCON standard 1974) and in the fields of chronic and acute care the specialist services are more frequently sited at more heavily populated centres. 48 Recently attention has been given to the critical mass of practice that is associa ted with clinical expertise, 24, 49 suggesting that those who practice in remote areas require training and continuing professional development over and above that of the urban practitioner. Studies have reported understanding of the excess travel, finance and time required to deliver services to remote communities which gives rise to the high GP: population ratio. 33, 49, 58 In describing the caseload and training of rural healthcare practitioners it is necessary to provide a more comprehensive profile of their ‘rurality’ than is currently available from national datasets – a rural fingerprint.
i Conversation with P.Hopkins (Information and Statistics, Highland Health Board) and Christine MacFarlane Slack (Senior Nurse, Belford Hospital)

23
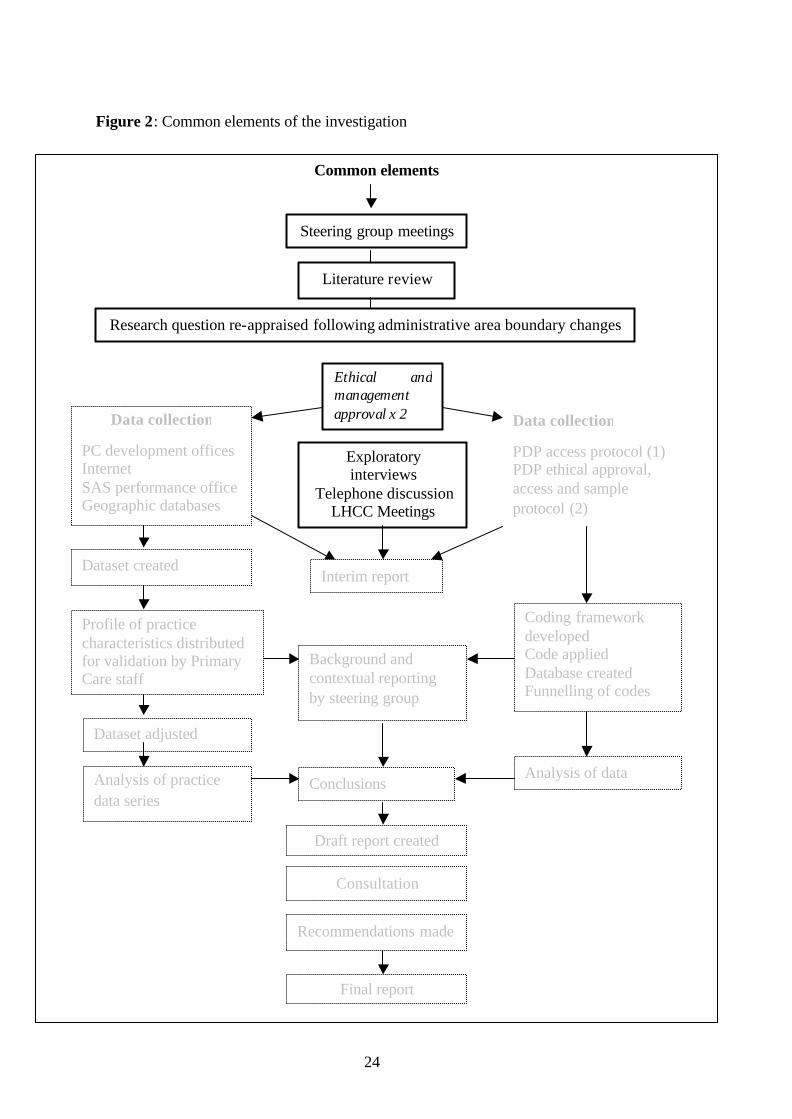
METHODS Framing the research A steering group including representatives of HIHRI, NES and the three LHCCs managed the project. A literature review was undertaken and, following appropriate management approval two separate, but related strands of investigation were undertaken. These were: an exploration of factors affecting service provision in remote and rural LHCCs; a profile of the training needs of a remote and rural LHCC and a strategy by which these might be met. These are illustrated in Figure 2. The project focused on the training needs of the individuals within the LHCCs. Methods adopted included interviews, face to face and telephone discussions, and data extraction from a variety of sources. Data collection took place during the period May 2003 to December 2003. Common elements of method Literature review
The literature review explored descriptions of rural healthcare service provision, and training and development of staff, in academic papers, policy and strategy documents, books and theses. Electronic databases were searched using a list of key works (see Appendix 1). These included BNI, CINAHL, EMBASE, HMIC, and Medline. Members of the steering group provided locally generated literature. The interview group (below) provided further literature. Reading of articles and reference lists provided detail of other associated literature.
24
Figure 2: Common elements of the investigation
Common elements
Literature review
Ethical and management approval x 2
Steering group meetings
Data collection
PC development offices Internet SAS performance office Geographic databases
Data collection
PDP access protocol (1) PDP ethical approval, access and sample protocol (2)
Exploratory interviews
Telephone discussion LHCC Meetings
Conference attendance
Profile of practice characteristics distributed for validation by Primary Care staff
Dataset created
Dataset adjusted
Analysis of practice data series
Coding framework developed Code applied Database created Funnelling of codes
Analysis of data
Interim report
Consultation
Draft report created
Final report
Conclusions
Background and contextual reporting by steering group
Research question re-appraised following administrative area boundary changes
Recommendations made

25
Ethics All research undertaken by or on behalf of or in NHS organisations is now subject to a Governance Framework.70 Research conducted within a specific NHS Trust has to be carried out with the approval of Trust Management. The 2 Trusts in the study area gave management approval. A description of the study and a confidentiality protocol was requested by both Trusts. Consent to access all available anonymised Personal Development Plans (PDPRs) was given by the local LHCC manager in one Trust, the second required consent from individuals identified through a sampling protocol. Management approval and an honorary contract were provided by both Trusts. Exploratory interviews The research sponsors and steering group provided contact details of interested parties (Table 2) In a snowballing exercise other sources were identified. Background information was also enhanced by attendance at the following meetings and conferences. ?? ‘Strength in Communities’ team - a road show in Inverness to describe the new
Scottish Deprivation Index (SIMD2001) ?? International Rural Network ‘Taking Charge’ Conference ?? LHCC Board meeting, Wester Ross, S Skye, Lochalsh ?? LHCC Locality Managers meeting, Argyll and Bute ?? LHCC Board meeting, Argyll and Bute ?? Family Health Nurse Conference, Edinburgh ?? Skills for Health – Remote and rural healthcare competences project, Edinburgh

26
Table 2: List of engagements with stakeholders External organisations
Internal organisations
Glasgow University with NHS Scotland Information and Statistics Division ‘The Platform project’
LHCC Managers Lochaber, Wester Ross, Skye and Lochalsh
The Highland Council Training and Development Manager
Scottish Centre for Research on Social Justice
Medical Director
Sabhal Mor Ostaig (Gaelic Medium College)
Primary Care Development Team
Church of Scotland National Mission
Research and Development Manager
Highland Education Dept
Highland Primary Care Trust
Workforce information HPCT
Highlands and Islands Enterprise
Manager NHS Pay Unit
Northern Constabulary
Highland NHS Board
Information Officer HHB
Argyll and Bute Council Argyll and Clyde Health Board
Primary Care Development office
BEAR Scotland Research and Development Office, Argyll and Bute
BASICS
Workforce Information Office
Scottish Ambulance Service
Argyll and Bute Primary Care Trust
Lead Nurse, Argyll and Bute LHCC

27
Profiling The main purpose of this part of the study was to develop a profile of each of the practices in the study area. The West Highland area is staffed by Primary Care staff who have a variety of contractual arrangements with NHS Highland and NHS Argyll and Clyde. Some travel between various sites, others work at a fixed address. The postcode of the GP surgery was used as an anchor point to link area measurements to the communities. Community hospital addresses were not used in profiling analysis as locations for individual staff were not representative of the area covered, and others studies were concurrently assessing hospital provision in the area. Identifiers used were as follows: The Primary Care development units provided identifying practice codes, surgery postcodes, practice names and addresses. Highland Council provided tables that linked postcodes to ward codes, ward names and Census Output Area (COA) codes. A variety of national and local data sources were employed. National Data Sources The Platform Project (www.gla.ac.uk/projects/platform) uses General Practice codes and the postcodes of registered patients to place each healthcare community within the appropriate Scottish Household Survey (SHoS) settlement classification.5 The Census data for 2001 28 describes population density at different area levels. Both Ward and COA data were captured to give the best opportunity of representing not only the population density at the surgery but also in the surrounding patient catchment area. Scottish Neighbourhood Statistics describe access to hospitals, Dentists and General Practitioners at ward level. The Scottish Index of Multiple Deprivation 30 is also presented at ward level, and is expressed as both absolute score and rank for Income, Health, Education, Access and Employment Deprivation. Geographic and transport data Transport databases and internet route planners were accessed to provide drive times, ferry crossing duration and mileage to key NHS locations from the GP postcode. Several anomalies were noticed and some road types were not represented. The results were hand searched and cross referenced to information on transport infrastructure obtained from Highlands and Island Enterprise, roads maintenance company BEAR Scotland and users forum HITrans.

28
Figure 3: Progress of investigation – Profiling
Profiling
Literature review
Ethical and management approval x 2
Steering group meetings
Data collection
PC development offices, Internet SAS performance office
Data collection
PDP access protocol (1) PDP ethical approval, access and sample protocol (2)
Exploratory interviews
Telephone discussion LHCC Meetings
Profile of practice characteristics distributed for validation by Primary Care staff
Dataset created
Dataset adjusted
Analysis of practice data series
Coding framework developed Code applied Database created Funnelling of codes
Analysis of data
Interim report
Consultation
Draft report created
Final report
Conclusions
Background and contextual reporting by steering group
Research question re-appraised following administrative area boundary changes
Recommendations made

29
NHS data sources Primary Care development units and members of the steering group were able to supply LHCC details linked to the General Practice code. These included the most accessible hospital (accepting acute admissions) and the location of the Health Board Headquarters. Scottish Ambulance Service (SAS) provided activity figures and response times linked to postcode district sector and local ambulance stations. These results were linked to GP practice at postcode district level. Both road and air ambulance activity are recorded monthly. Information on ambulance activity in the neighbouring district postcode was included to represent the potential activity of NHS staff that act as First Responders in rural areas. Air ambulance response/cover, attending SAS personnel and air transport type were also recorded. Information and Statistics Division provided records of temporary residents’ attendance at GP surgeries in the study area. Other relevant parameters Literature, discussion, interviews and meetings with staff in healthcare settings highlighted other aspects of care that represent the diversity or spectrum of skill that is required of the nurse, doctor or allied professional in remote practice. There are no centrally held records of staff associated with healthcare who are employed directly by GPs. A range of items was included in individual profiles for comment by the staff at the location. Data entry Data were entered into an Excel spreadsheet, from which a profile of each practice area could be created. A sample is shown in appendix 2. Consultation The practice profiles were disseminated for consultation and discussion to LHCC representatives. A Practice manager, Community Nurse and General Practitioner in each area received a draft profile for comment. A covering letter described the study and asked that corrections and completions be made and returned to the researchers in a prepaid envelope. Reminders were sent out to non-respondents following telephone enquiries to the Practice Managers. Returned profiles were logged and analysed. Any corrections/modifications provided by the practice representatives were recorded before the dataset was finalised for analysis.

30
Figure 4: Progress of investigation – Training and development needs
Training and development needs
Literature review
Ethical and management approval x 2
Steering group meetings
Data collection
PC development offices Internet SAS performance office Geographic databases
Data collection
PDP access protocol (1) PDP ethical approval, access and sample protocol (2)
Exploratory interviews
Telephone discussion LHCC Meetings
Conference
Profile of practice characteristics distributed for validation by Primary Care staff
Dataset created
Dataset adjusted
Analysis of practice data series
Coding framework developed Code applied Database created Funnelling of codes
Analysis of data
Interim report
Consultation
Draft report created
Final report
Conclusions
Background and contextual reporting by steering group
Research question re-appraised following administrative area boundary changes
Recommendations made

31
Training and development Personal development plans Within NHS Scotland, the Scottish Partnership forum created a staff governance standard 67 and established the Partnership Information Network (PIN) board to develop best practice human resource guidelines. The LHCCs in the study use the personal development planning and review (PDPR) proforma produced by the PIN Board ‘Guideline Development’ group.71 Consent to access anonymised PDPRs was given by management in some areas and by staff in others. The protocol to preserve confidentiality is described below. PDPR collection PDPRs were collected by Primary Care managers, copied and names blanked out. In a small community that has, for example, only one chiropodist it may still be possible to identify the staff member. A further step was therefore taken to blank out the workplace address. Coding scheme The remaining information on each anonymised PDPR was coded and recorded on an Access data base, recording staff profession, LHCC, skill need, level of training, preferred delivery method and resource needs. The information included both the agreed personal development plan and the needs identified by the individual during review and appraisal. Funnelling Many data fields were created from the PDPR coding exercise. To facilitate the analysis of large amounts of data a funnelling process was designed. For example 146 different skill needs were recorded, these were assigned to group labels giving a more manageable list of 5 groups (Table 3)

32
Table 3: Funnelling of field codes into groups for data analysis
Cod
es
Staff discipline
Skill need
Level of training
Preferred delivery method
Resource needs
Fie
lds
25 146 14 36 21
Gro
ups
1. A&C 2. AHP 3. GP 4. Nurse 5. Midwife
1. IT 2. Technical 3. Clinical -
practical 4. Clinical –
knowledge 5. Management
1. Accredited FE 2. Accredited HE 3. Professional
maintenance
1. Experiential 2. Taught 3. Personal study
1. Time 2. Equipment 3. Finance 4. Locum/backfill 5. Domestic 6. Local delivery
Analysis An analysis table was constructed and reviewed by the steering group (Appendix 3). One LHCC provided many more anonymised PDPRs than the other two. Profiling results had shown that the LHCC shared many characteristics with the other rural LHCCs in the study and analysis was therefore restricted to that LHCC. Appraisal schemes for GPs were not fully developed at the time of the study. However, an educational needs plan was collected by the Associate Adviser from each consenting GP in that LHCC. The same research information letter, confidentiality and coding protocols were employed. Performance Assessment Framework A Performance Assessment was made available by each LHCC in the study. Trainers diary The diary of a LHCC peripatetic trainer was made available to the project team.

33
RESULTS Introduction The first part of this results section concerns the practice profiles. It should be noted that within West Highland, different public bodies do not necessarily share administrative boundaries. For example, a settlement listed in the Argyll and Clyde area for health purposes may be linked to neighbouring Highland for policing or local economic measurement. In Scotland there is no single database that captures all the detail of the practice communities that are studied here. The information available in this section thus provides a uniquely comprehensive picture of the practice community. Profiling Response to the profiling exercise Fifty-three general practices and 6 branch surgeries are located in the 3 LHCC areas. The overall response rate for the return of confirmed, completed or corrected practice community profiles was 83% (Table 4) Table 4: Response rates for return of community profiles by LHCC LHCC General Practice
communities Respondents
Argyll and Bute ( A & B) 36 29 80% Lochaber ( Lochaber ) 11 8 72% Wester Ross, S.Skye and Lochalsh (WR,SS & L)
12 12 100%
Corrections to Profiles Fifty-nine profiles had been created each containing 78 fields of data, giving a total of 4602 fields. Of these, 18 (0.39%) were corrected by respondents. Three practices made a distinction between GP, Associate and Retainer by adding these descriptions in free text. Two practices described as multi-partner were corrected to single-handed and 4 GP vacancies occurred during the study period. Three respondents recorded increases in registered patients’ actual list size. The geographical access fields of distance, travel time and mode had required diligence during compilation of the individual records; researchers had already noted discrepancies and made corrections. Six more field corrections were necessary. Additions to Profiles Practices had been supplied with researcher contact details. Three telephone calls and 2 letters were received and 26 unsolicited comments from returned profiles were recorded. The topics covered seasonal population fluctuation, roles and skills travel and transport, island emergencies and ambulance provision.
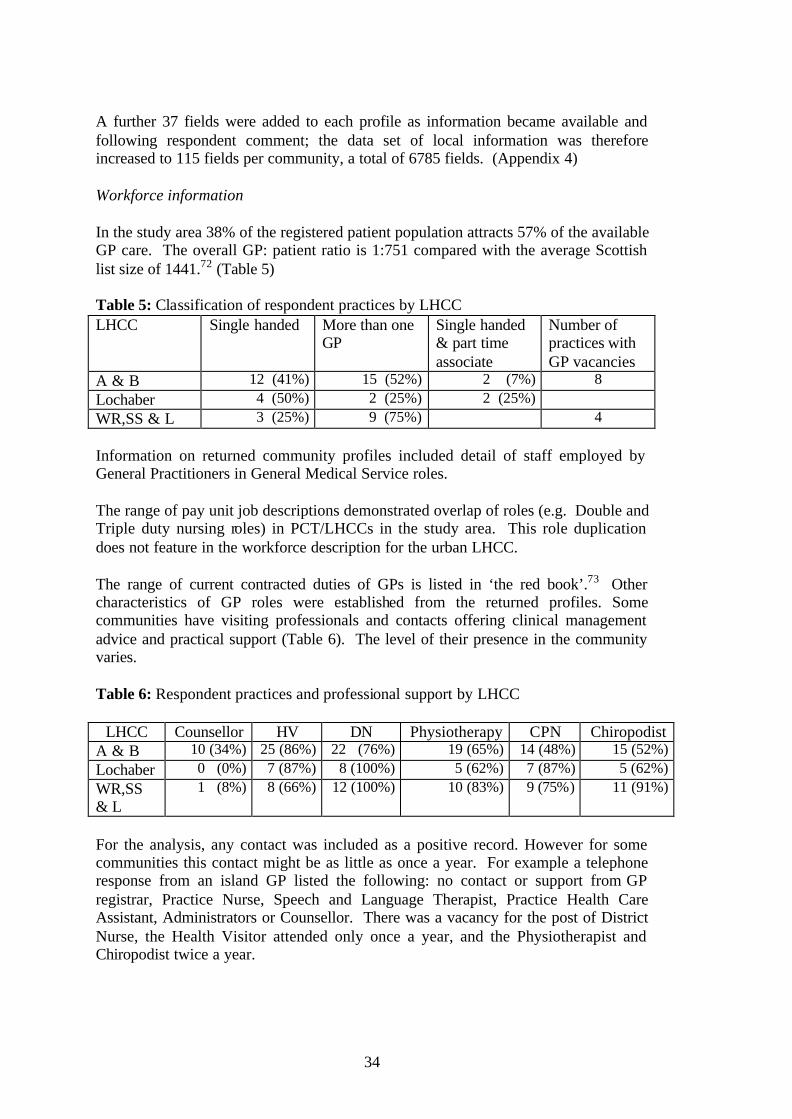
34
A further 37 fields were added to each profile as information became available and following respondent comment; the data set of local information was therefore increased to 115 fields per community, a total of 6785 fields. (Appendix 4) Workforce information In the study area 38% of the registered patient population attracts 57% of the available GP care. The overall GP: patient ratio is 1:751 compared with the average Scottish list size of 1441.72 (Table 5) Table 5: Classification of respondent practices by LHCC LHCC Single handed More than one
GP Single handed & part time associate
Number of practices with GP vacancies
A & B 12 (41%) 15 (52%) 2 (7%) 8 Lochaber 4 (50%) 2 (25%) 2 (25%) WR,SS & L 3 (25%) 9 (75%) 4 Information on returned community profiles included detail of staff employed by General Practitioners in General Medical Service roles. The range of pay unit job descriptions demonstrated overlap of roles (e.g. Double and Triple duty nursing roles) in PCT/LHCCs in the study area. This role duplication does not feature in the workforce description for the urban LHCC. The range of current contracted duties of GPs is listed in ‘the red book’.73 Other characteristics of GP roles were established from the returned profiles. Some communities have visiting professionals and contacts offering clinical management advice and practical support (Table 6). The level of their presence in the community varies. Table 6: Respondent practices and professional support by LHCC
LHCC Counsellor HV DN Physiotherapy CPN Chiropodist A & B 10 (34%) 25 (86%) 22 (76%) 19 (65%) 14 (48%) 15 (52%) Lochaber 0 (0%) 7 (87%) 8 (100%) 5 (62%) 7 (87%) 5 (62%) WR,SS & L
1 (8%) 8 (66%) 12 (100%) 10 (83%) 9 (75%) 11 (91%)
For the analysis, any contact was included as a positive record. However for some communities this contact might be as little as once a year. For example a telephone response from an island GP listed the following: no contact or support from GP registrar, Practice Nurse, Speech and Language Therapist, Practice Health Care Assistant, Administrators or Counsellor. There was a vacancy for the post of District Nurse, the Health Visitor attended only once a year, and the Physiotherapist and Chiropodist twice a year.
35
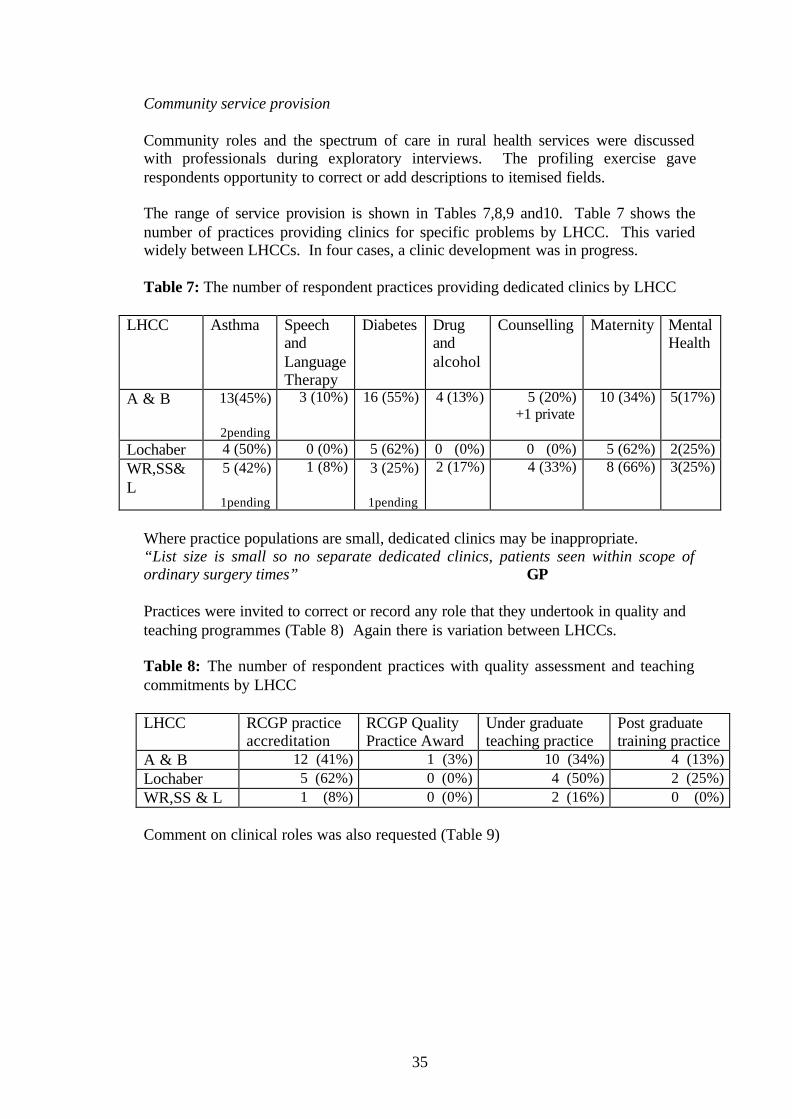
Community service provision Community roles and the spectrum of care in rural health services were discussed with professionals during exploratory interviews. The profiling exercise gave respondents opportunity to correct or add descriptions to itemised fields. The range of service provision is shown in Tables 7,8,9 and10. Table 7 shows the number of practices providing clinics for specific problems by LHCC. This varied widely between LHCCs. In four cases, a clinic development was in progress. Table 7: The number of respondent practices providing dedicated clinics by LHCC
LHCC Asthma Speech and Language Therapy
Diabetes Drug and alcohol
Counselling Maternity Mental Health
A & B 13(45%)
2pending
3 (10%)
16 (55%)
4 (13%)
5 (20%) +1 private
10 (34%)
5(17%)
Lochaber 4 (50%) 0 (0%) 5 (62%) 0 (0%) 0 (0%) 5 (62%) 2(25%) WR,SS& L
5 (42%)
1pending
1 (8%)
3 (25%)
1pending
2 (17%)
4 (33%)
8 (66%)
3(25%)
Where practice populations are small, dedicated clinics may be inappropriate. “List size is small so no separate dedicated clinics, patients seen within scope of ordinary surgery times” GP Practices were invited to correct or record any role that they undertook in quality and teaching programmes (Table 8) Again there is variation between LHCCs. Table 8: The number of respondent practices with quality assessment and teaching commitments by LHCC LHCC RCGP practice
accreditation RCGP Quality Practice Award
Under graduate teaching practice
Post graduate training practice
A & B 12 (41%) 1 (3%) 10 (34%) 4 (13%) Lochaber 5 (62%) 0 (0%) 4 (50%) 2 (25%) WR,SS & L 1 (8%) 0 (0%) 2 (16%) 0 (0%) Comment on clinical roles was also requested (Table 9)

36
Table 9: The number of respondent practices supplying unscheduled care and related services by LHCC LHCC Out of Hours
cover is by the practice only
Out of Hours cover is by single GP
Practice provides community hospital cover
Practice provides dispensing services
Practice provides minor surgery and minor injuries treatments
A & B 17 (58%) 4 (13%) 17 (59%) 27 (93%) 14 (48%) Lochaber 6 (75%) 5 (62%) 0 (0%) 6 (75%) 5 (62%) WR,SS& L 12 (100%) 3 (25%) 3 (25%) 10 (83%) 9 (75%) Some practitioners listed other commitments, for example: ‘The GPs roles include LHCC locality lead, Associate Adviser for vocational training, Local Medical Committee member, Undergraduate co-ordinator for the LHCC’ Literature and exploratory interviews had highlighted additional community roles that were listed for completion on the practice profile (Table10) Table 10: The number of practices combining General Practice duties with associated
community roles by LHCC. LHCC Occupational
Health Officer Police surgeon
Airport duties
Rescue team
Sports injury team
A & B 7 (24%) 9 (31%) 5 (17%) 3 (10%) 2 (7%) Lochaber 0 (0%) 3 (37%) 0 (0%) 2 (25%) 0 (0%) WR,SS & L 0 (0%) 4 (33%) 0 (0%) 3 (25%) 2 (16%) Useful insights into services, particularly emergency services, can be gained from Scottish Ambulance Service (SAS) data. SAS records the mode of patient transport, ambulance response times and ambulance service engagement times. These are recorded by number of incidents within a postcode district for summer and winter, for urgent, emergency and air response (Appendix 5) The number of incidents in each of these categories for the years 2002-2003 is shown in Figure 5. Argyll and Bute has the greatest number of contacts, reflecting its larger population.
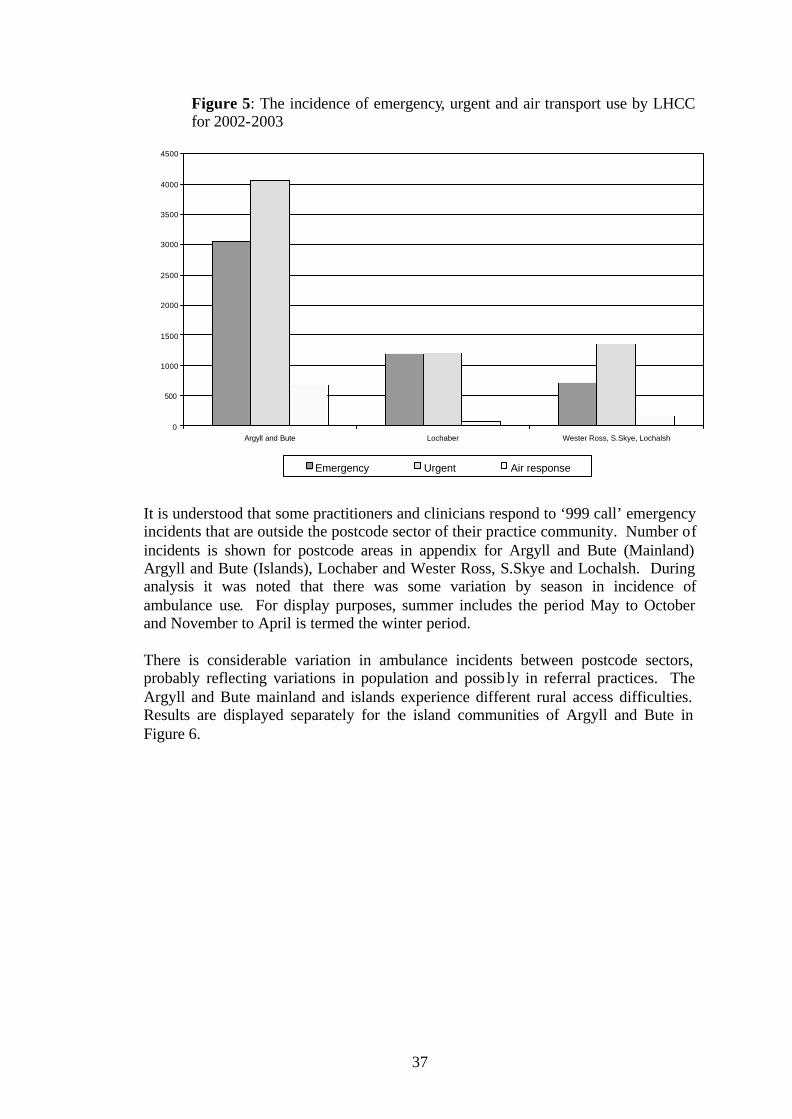
37
Figure 5: The incidence of emergency, urgent and air transport use by LHCC for 2002-2003
0
500
1000
1500
2000
2500
3000
3500
4000
4500
Argyll and Bute Lochaber Wester Ross, S.Skye, Lochalsh
Emergency Urgent Air response
It is understood that some practitioners and clinicians respond to ‘999 call’ emergency incidents that are outside the postcode sector of their practice community. Number of incidents is shown for postcode areas in appendix for Argyll and Bute (Mainland) Argyll and Bute (Islands), Lochaber and Wester Ross, S.Skye and Lochalsh. During analysis it was noted that there was some variation by season in incidence of ambulance use. For display purposes, summer includes the period May to October and November to April is termed the winter period. There is considerable variation in ambulance incidents between postcode sectors, probably reflecting variations in population and possib ly in referral practices. The Argyll and Bute mainland and islands experience different rural access difficulties. Results are displayed separately for the island communities of Argyll and Bute in Figure 6.

38
Figure 6: The incidence of emergency road ambulance use in each LHCC showing summer and winter frequency for 2002-2003
0
200
400
600
800
1000
1200
1400
1600
Argyll and Bute Argyll and Bute islands Lochaber WRoss SSkye & Lochalsh
summer winter
The Scottish Ambulance Service records road ambulance use for locally generated urgent transport requests. There is little difference between summer and winter ‘urgent’ calls, these are most often generated by GP/nurses and subject to individual referral patterns. These are presented in Figure 7 and as results in appendix for summer (May-Oct) and winter (Nov-Apr) seasons for postcode areas in Argyll and Bute (Mainland), Argyll and Bute (Islands), Lochaber and Wester Ross, S.Skye and Lochalsh. Figure 7: The incidence of urgent road ambulance use in each LHCC showing summer and winter frequency for 2002-2003
0
200
400
600
800
1000
1200
1400
1600
1800
Argyll and Bute Argyll and Bute islands Lochaber WRoss SSkye & Lochalsh
summer winter

39
Helicopters are not normally considered for journeys less than 30 miles and fixed wing planes for journeys less than 100 miles, the exceptions being island or remote communities where no suitable road or land bridge exists 74. (Figure 8) Figure 8: The incidence of air ambulance use in each LHCC showing summer and winter frequency for 2002-2003
0
50
100
150
200
250
Argyll and Bute Argyll and Bute islands Lochaber WRoss SSkye & Lochalsh
summer winter
Interviewees expressed concern regarding the need to provide escorts for some urgent air flights. For example three communities have neither practice nurse nor district nurse and a single-handed GP where the air transport vehicle may be crewed by ambulance attendant only. ‘… and add the three hours that I spent on the tarmac with the patient’
Island GP Information was not available for objective measurement of air response times to initial call. Table 11 lists the type of aircraft in use for an area and the profession of the accompanying aircrew. Times shown are expected air response times once the aircraft is deployed for that mission. The need for clinical escort is dependant on the condition of the patient and the type of air transport that is available for incident response. On some occasions the escort is the only healthcare professional in the area. This implies a risk for the remaining residents.

40
Table 11: Example of confirmed profiles from general practices with limited nurse resource where clinical escort may be required for patient transfer by air
Practice name
Partners
Air ambulance response from dispatch
SAS personnel
Air transport Helicopter type and base location
Practice Nurse
DN
Applecross singlehanded up to 60 mins paramedic King Aberdeen n y
Arisaig singlehanded up to 60 mins amb attendant Islander Glasgow n y
Carbost singlehanded up to 60 mins paramedic King Aberdeen n y
Colonsay singlehanded up to 60 mins 1.amb attendant 2.paramedic
1.Islander Glasgow 2.King Aberdeen n n
Ferrindonald Sleat multipartner up to 60 mins amb attendant Islander Glasgow n y
Glenelg multipartner up to 30 mins paramedic SAS Inverness n y
Isle of Eigg singlehanded up to 60 mins amb attendant Islander Glasgow n n
Lismore multipartner up to 60 mins amb attendant Islander Glasgow n y
Lochaline singlehanded up to 60 mins amb attendant Islander Glasgow n y
Lochcarron multipartner up to 30 mins paramedic SAS Inverness n y
Lochgoilhead singlehanded up to 30 mins 1.amb attendant 2.paramedic
1.Islander Glasgow 2.King Aberdeen n n
Mallaig singlehanded up to 60 mins amb attendant Islander Glasgow n y
Port Appin multipartner up to 60 mins amb attendant Islander Glasgow n y The nature of ambulance contact with patients may differ in rural areas compared with urban. Figure 9 shows response time, time on the scene, and transfer time for patients in various locations. Response time is longer in some more remote areas, but the differences are relatively modest. Time on the scene is broadly similar across all areas. The most striking difference is in the transfer time, which may be substantial in some rural areas. Interviewees commented that this takes ambulance staff into areas of care that are most frequently addressed by nurses and doctors in Accident and Emergency Units.

41
Figure 9: The annual average of time (minutes) from emergency call to hospital care by ambulance station, broken down into response time, time on scene and travel/transfer time
0.00
20.00
40.00
60.00
80.00
100.00
120.00
INV
ER
NE
SS
Rot
hesa
y
Cam
pbel
tow
n
Dun
oon
Loch
gilp
head
Oba
n
Fort
Will
iam
Bow
mor
e
Por
tree
Bro
adfo
rd
Arr
ocha
r
Kyl
e of
Loc
hals
h
Tar
bert
Inve
rary
For
t Aug
ustu
s
Gle
ncoe
Mul
l
Ulla
pool
Mal
laig
Dun
vega
n
Str
ontia
n
Gai
rloch
Loch
carr
on
response time time on scene transfer time
In addition to the resident population, visitors and temporary residents have an impact on workload for remote rural practices. Figure 10 shows data provided by one practice within the Lochaber LHCC. Figure 10: A summary of service provision for temporary and emergency patients in a sample GP practice.
Temporary resident registration figures were made available to this study but it should be noted that there is no financial incentive for inducement practices to record these
Anonymous GP area data
0200400600800
1000
94-95
96-97
98-99
00-01
02-03
Temporary residents
Emergencytreatments

42
episodes of patient care and figures used are likely to under represent the provision by rural GPs. Boxplots are used to illustrate more than two sets of data. Figure 11 shows the number of temporary residents per annum per GP. The median, interquartile range (50% of the practices for each LHCC are shown in the grey boxes) In a boxplot outliers are marked individually as stars. Tourist activity in the study area was determined by associating local enterprise company results with LHCC boundaries. For each LHCC, the ratio of resident bed nights of the registered population (number of days resident per year i.e. 365 days less a possible 14 days holiday spent out of the area) to the estimated number of visitor bed nights was calculated. (Table12) The volume of tourist trade is likely to have a greater proportional effect in remote and rural practices than in the urban LHCC. Figure 11: Temporary residents per GP by LHCC
0 100 200 300 400 500
Table 12: Tourist activity figures for 1999 showing ratio of resident: visitor bed nights LHCC Resident
(GP registered) population
Resident bed nights (LHCC)
Visitor bed nights (LEC)
Ratio of resident: visitor bed nights
A & B 65,111 22,853,961 2,100,000 11:1 Lochaber 20,661 7,252,011 2,338,183 3:1 WR,SS & L 13,632 4,784,832 2,632,804 2:1 Inverness 60,950 21,393,450 2,190,449 10:1
Inverness
Argyll and Bute
Lochaber
Wester Ross, S.Skye, Lochalsh

43
Spectrum of roles in Primary Care and General Medical Service: A simple scoring system was developed from the primary data collection from principal practices (n.43) to record the spectrum of roles that are undertaken in rural practice (Table 13). This can be organised into four groupings:
1. Clinical 2. Access 3. Roles 4. Availability of professional support :
A positive score was given for roles undertaken outside the traditional range of care 58,
73 for example single-handed working, responsibility for branch premises and extraordinary patient access. Absence of support from other professions also attracted a positive score. A total score was calculated for each of the main practices that had supplied data. Increasing score indicates an increasing spectrum of roles. This is presented as a summary result in Figure 12 and discussed below. Figure 12: Spectrum of roles score for each main practice by LHCC
0 10 20 30 40
Argyll and Bute
Lochaber
Wester Ross, S.Skye, Lochalsh
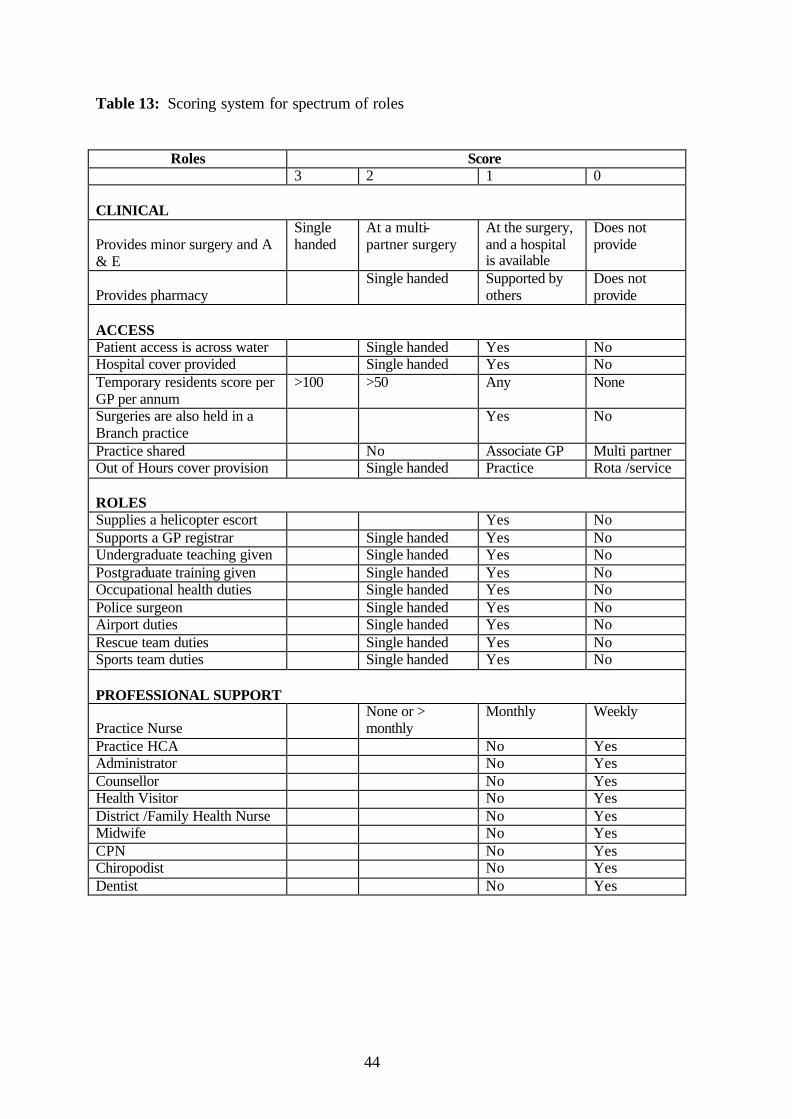
44
Table 13: Scoring system for spectrum of roles
Roles Score 3 2 1 0
CLINICAL
Provides minor surgery and A & E
Single handed
At a multi-partner surgery
At the surgery, and a hospital is available
Does not provide
Provides pharmacy Single handed Supported by
others Does not provide
ACCESS Patient access is across water Single handed Yes No Hospital cover provided Single handed Yes No Temporary residents score per GP per annum
>100 >50 Any None
Surgeries are also held in a Branch practice
Yes No
Practice shared No Associate GP Multi partner Out of Hours cover provision Single handed Practice Rota /service ROLES Supplies a helicopter escort Yes No Supports a GP registrar Single handed Yes No Undergraduate teaching given Single handed Yes No Postgraduate training given Single handed Yes No Occupational health duties Single handed Yes No Police surgeon Single handed Yes No Airport duties Single handed Yes No Rescue team duties Single handed Yes No Sports team duties Single handed Yes No PROFESSIONAL SUPPORT
Practice Nurse None or >
monthly Monthly Weekly
Practice HCA No Yes Administrator No Yes Counsellor No Yes Health Visitor No Yes District /Family Health Nurse No Yes Midwife No Yes CPN No Yes Chiropodist No Yes Dentist No Yes

45
Population Resource allocation to LHCCs is linked to resident population registered by the Practitioner Services Division of the Scottish Executive Health Department on the Community Health Index. Population density figures were derived from the 2001 Census. Figure 13 illustrates population density at the location of the GP surgery, while Figure 14 illustrates the population density at ward level to represent the nature of population distribution in the practice catchment area. This is relevant where some services are provided from fixed locations and others by travelling professional staff. Results are presented as a box and whisker plot for each LHCC in the study area. Data from Inverness LHCC provide an urban comparison. Figure 13: Population Density at the location of the GP surgery by LHCC
0 10 20 30 40
Typically, population densities at the practice locations are low in the rural LHCCS, compared to the urban LHCC. However, there is considerable variation, especially in the Argyll and Bute LHCC.
Inverness
Argyll and Bute
Lochaber
Wester Ross, S.Skye, Lochalsh

46
Figure 14: Population density at ward level by LHCC
0 10 20 30
As illustrated in Figure 14, the distinction between rural and urban LHCCs is even more pronounced when population density at ward level is examined, and scatter within the rural LHCCs is less than that seen for surgery location in Figure 13. Access As an indicator of access problems in rural areas, we examined Scottish Index of Multiple Deprivation scores for Access Deprivation, which are calculated for ward areas. The practice postcode was matched to the ward code to demonstrate access within the practice catchment area. Higher scores represent greater difficulties with access. (Figure 15) As expected, rural LHCCs are typified by greater access deprivation than the urban LHCC, but within the rural LHCCs, there is greater scatter of scores across practices. We determined total travel time of a one-way journey from each practice to the Health Board offices. As shown in Figure 16, practices within the rural LHCCs have substantial travel times to administrative and educational centres that are located within, or close to, the Health Board offices.
Inverness
Argyll and Bute
Lochaber
Wester Ross, S.Skye, Lochalsh
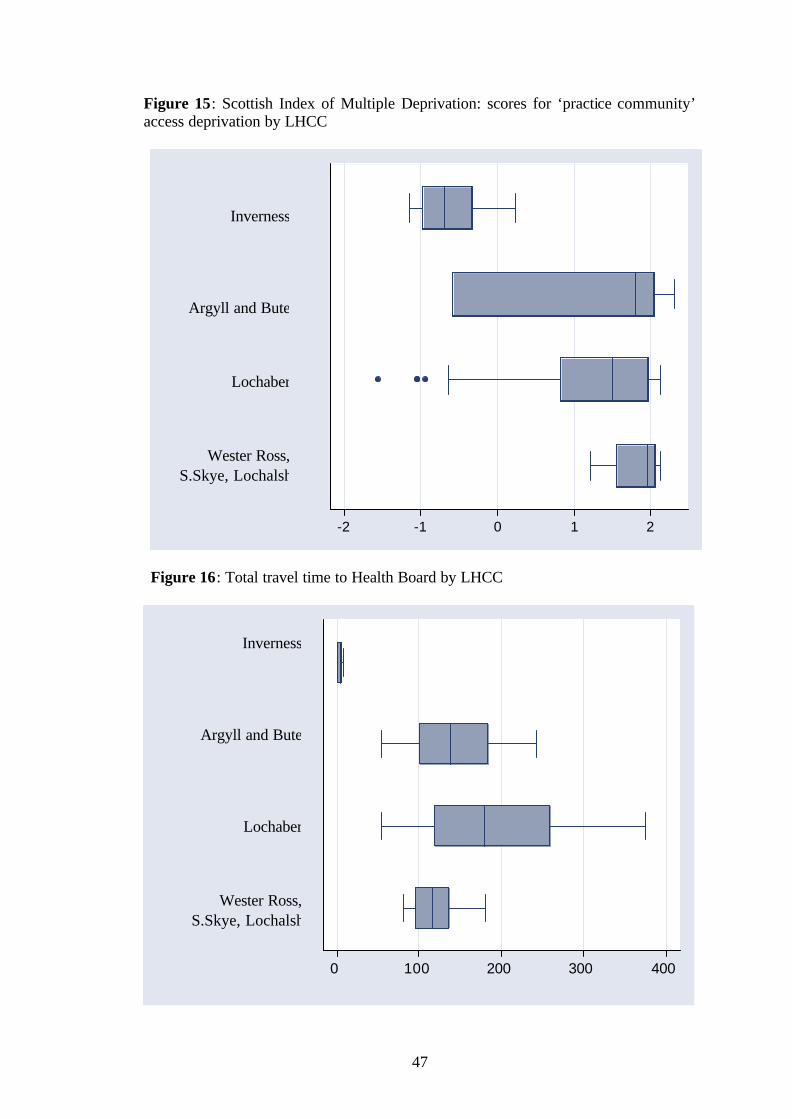
47
Figure 15: Scottish Index of Multiple Deprivation: scores for ‘practice community’ access deprivation by LHCC
-2 -1 0 1 2
Figure 16: Total travel time to Health Board by LHCC
0 100 200 300 400
Inverness
Argyll and Bute
Lochaber
Wester Ross, S.Skye, Lochalsh
Inverness
Argyll and Bute
Lochaber
Wester Ross, S.Skye, Lochalsh

48
Travel is complicated by single track road and sea crossings, and respondents noted that this makes a difference during adverse weather conditions. Figure 17 shows single track road distances to the Health Board in each LHCC. Each of the rural LHCCs has some single track roads, although the amounts differ between LHCCs, the greatest single track distances being in the Skye, Wester Ross and Lochalsh LHCC and Table14 shows that the greatest need for ferries is in the Argyll and Bute LHCC. Figure 17: Illustration of miles of single track road between GP practice address and Health Board by LHCC
0 10 20 30 40
Table 14: Use of ferry to access Health Board by LHCC LHCC Essential More than one
ferry required Preferable (land link available)
A & B 19 3 1 Lochaber 1 0 2 WR,SS & L 0 0 0 As a measure of access to secondary care we measured travel times to the nearest hospital for receipt of acute admissions. Community hospitals in the area are shown on Map 1. During the profile consultation, communities nominated their nearest hospital for receipt of acute admissions. Figure 18 shows travel time from the practices to the nearest acute hospital. As with Health Board access, the rural LHCCs have substantially greater travel times than the urban one, but the degree of remoteness among the rural LHCCs differs from the Health Board Access figures, reflecting the availability of acute services at Oban and Fort William. Travel time was assessed using the travel modes of road and ferry transport. Comment was received
Inverness
Argyll and Bute
Lochaber
Wester Ross, S.Skye, Lochalsh

49
from practitioners that, for some communities, air travel is an option, sometimes a preference and occasionally essential. Figure 18: The total travel time to Acute receiving hospital by LHCC
0 100 200 300 400
Figure 19 shows single track road length to the nearest acute hospital in each LHCC. Wester Ross, Skye and Lochalsh again has the greatest length of single track roads. The dependence of Argyll and Bute on ferry travel is shown in Table15. Table 15: Use of ferry to access acute receiving hospital by LHCC LHCC Essential More than one
ferry required Preferable (land link available)
A & B 19 3 1 Lochaber 1 0 2 WR,SS & L 0 0 0
Inverness
Argyll and Bute
Lochaber
Wester Ross, S.Skye, Lochalsh

50
Figure 19: Illustration of the length of single-track road between GP practice address and acute receiving hospital by LHCC
0 10 20 30 40
Inverness
Argyll and Bute
Lochaber
Wester Ross, S.Skye, Lochalsh

51
Factor analysis In an attempt to devise an index that would capture these geographic and demographic characteristics of rural practices, we undertook factor analysis on four candidate variables: population density, GP list size, and travel times to hospital and health board headquarters. Principal component and maximum likelihood analysis yielded a robust one-factor solution explaining 75% variance, which we termed “Clinical Peripherality”. A factor score was then generated for each practice, higher values representing greater peripherality. The factor score was further rescaled to an index of 0 to 100, based on ranking the general practices by the factor score. Summary data are shown in Figure 20. As expected, rural LHCCs show higher median values and greater scatter of clinical peripherality among their practices, compared to the urban LHCC. Figure 20: Clinical Peripherality indices by LHCC
0 20 40 60 80 100
Associations between clinical peripherality and the road access component of the Scottish Index of Multiple Deprivation and spectrum of roles offered by practices were tested using Pearson’s correlation. Clinical peripherality correlated positively with the road distance based Scottish Index of Access deprivation. (Figure 21) Interestingly, clinical peripherality also correlated strongly with spectrum of roles (Figure 22).
Inverness
Argyll and Bute
Lochaber
Wester Ross, S.Skye, Lochalsh

52
Figure 21: Association between Access (SIMD) and Clinical Peripherality
-2-1
01
2R
oad
acce
ss (
SIM
D)
-2 -1 0 1 2Clinical Peripherality
Figure 22: Association between Spectrum of roles score and Clinical Peripherality
0
10
20
30
40
Spe
ctru
m o
f rol
es
-2 -1 0 1 2 Clinical peripherality
R = 0.6854
R=0.8735
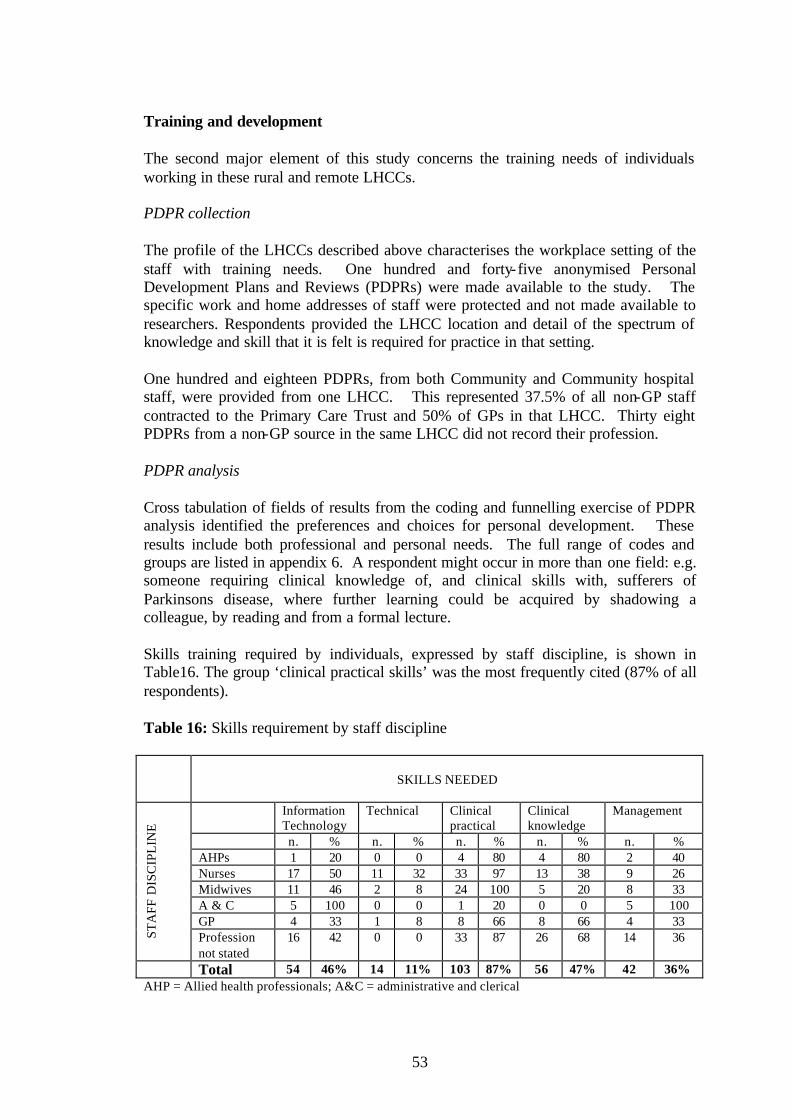
53
Training and development The second major element of this study concerns the training needs of individuals working in these rural and remote LHCCs. PDPR collection The profile of the LHCCs described above characterises the workplace setting of the staff with training needs. One hundred and forty-five anonymised Personal Development Plans and Reviews (PDPRs) were made available to the study. The specific work and home addresses of staff were protected and not made available to researchers. Respondents provided the LHCC location and detail of the spectrum of knowledge and skill that it is felt is required for practice in that setting. One hundred and eighteen PDPRs, from both Community and Community hospital staff, were provided from one LHCC. This represented 37.5% of all non-GP staff contracted to the Primary Care Trust and 50% of GPs in that LHCC. Thirty eight PDPRs from a non-GP source in the same LHCC did not record their profession. PDPR analysis Cross tabulation of fields of results from the coding and funnelling exercise of PDPR analysis identified the preferences and choices for personal development. These results include both professional and personal needs. The full range of codes and groups are listed in appendix 6. A respondent might occur in more than one field: e.g. someone requiring clinical knowledge of, and clinical skills with, sufferers of Parkinsons disease, where further learning could be acquired by shadowing a colleague, by reading and from a formal lecture. Skills training required by individuals, expressed by staff discipline, is shown in Table16. The group ‘clinical practical skills’ was the most frequently cited (87% of all respondents). Table 16: Skills requirement by staff discipline
SKILLS NEEDED
Information
Technology Technical Clinical
practical Clinical knowledge
Management
n. % n. % n. % n. % n. % AHPs 1 20 0 0 4 80 4 80 2 40 Nurses 17 50 11 32 33 97 13 38 9 26 Midwives 11 46 2 8 24 100 5 20 8 33 A & C 5 100 0 0 1 20 0 0 5 100 GP 4 33 1 8 8 66 8 66 4 33
STA
FF D
ISC
IPL
INE
Profession not stated
16 42 0 0 33 87 26 68 14 36
Total 54 46% 14 11% 103 87% 56 47% 42 36% AHP = Allied health professionals; A&C = administrative and clerical
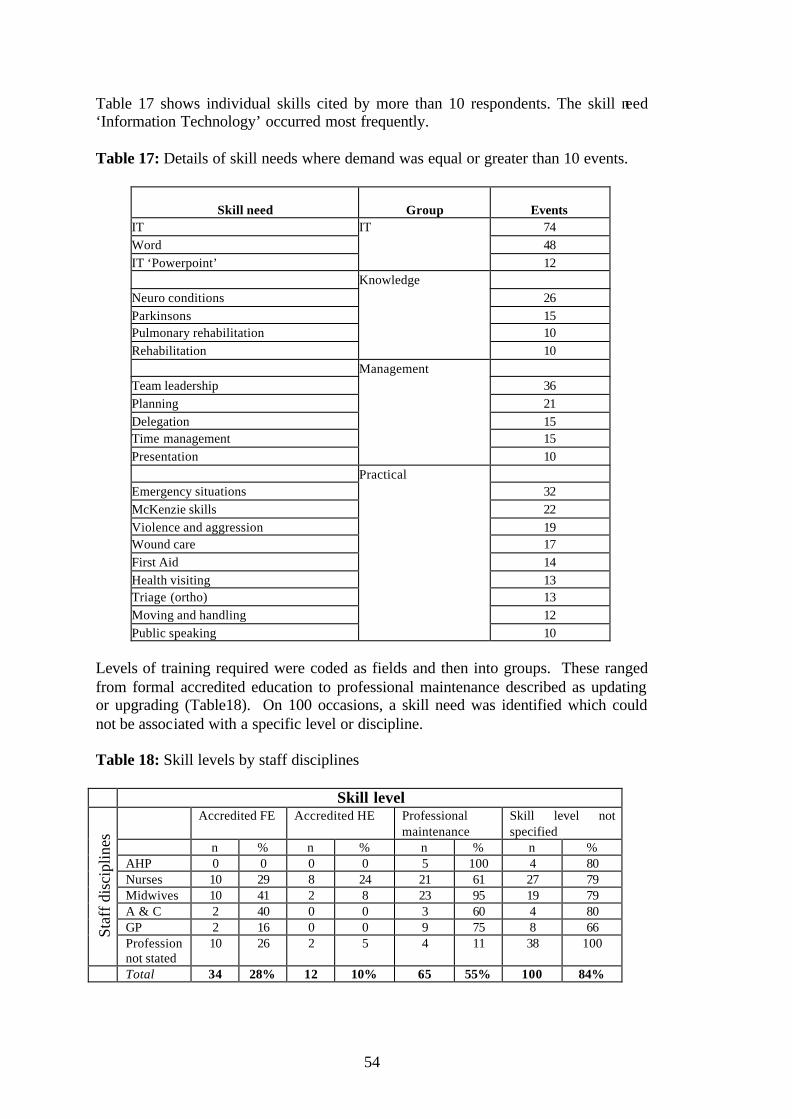
54
Table 17 shows individual skills cited by more than 10 respondents. The skill need ‘Information Technology’ occurred most frequently. Table 17: Details of skill needs where demand was equal or greater than 10 events.
Skill need Group Events
IT IT 74 Word 48 IT ‘Powerpoint’ 12 Knowledge Neuro conditions 26 Parkinsons 15 Pulmonary rehabilitation 10 Rehabilitation 10 Management Team leadership 36 Planning 21 Delegation 15 Time management 15 Presentation 10 Practical Emergency situations 32 McKenzie skills 22 Violence and aggression 19 Wound care 17 First Aid 14 Health visiting 13 Triage (ortho) 13 Moving and handling 12 Public speaking 10
Levels of training required were coded as fields and then into groups. These ranged from formal accredited education to professional maintenance described as updating or upgrading (Table18). On 100 occasions, a skill need was identified which could not be associated with a specific level or discipline. Table 18: Skill levels by staff disciplines Skill level
Accredited FE Accredited HE Professional maintenance
Skill level not specified
n % n % n % n % AHP 0 0 0 0 5 100 4 80 Nurses 10 29 8 24 21 61 27 79 Midwives 10 41 2 8 23 95 19 79 A & C 2 40 0 0 3 60 4 80 GP 2 16 0 0 9 75 8 66 St
aff d
isci
plin
es
Profession not stated
10 26 2 5 4 11 38 100
Total 34 28% 12 10% 65 55% 100 84%

55
Table 19 shows the preferred methods of delivery. Staff most frequently required their skill to be taught to them by another person. Table 19: Delivery methods identified by staff disciplines Delivery method
Experiential Taught Personal study Delivery method not specified
n % n % n % n % AHP 5 100 5 100 3 60 1 20 Nurses 14 41 32 94 28 82 12 35 Midwives 18 75 22 91 11 46 8 33 A&C 0 0 1 20 5 100 4 80 GP 6 50 11 91 9 75 3 25 St
aff d
isci
plin
es
Profession not stated
15 39 32 84 1 3 22 57
Total 58 49% 103 87% 57 48% 50 42%
Thirty-seven training delivery methods were identified, which for ease of analysis were funnelled into 4 groups. Details of the favoured delivery methods by field are shown in Table 20. Nurses and GPs favoured personal study and taught methods. Midwives and AHPs favoured taught and experiential methods.
Table 20: Delivery methods where demand was equal or greater that 10 events Delivery method
Group Events
Course Taught 161 Internal course 65 Study days 44 Coaching 41 Seminars 10 Technology based training Personal study 75 Reading 44 Peer support 15 Shadowing 14 Distance learning 13 Job rotation 10 In service Experiential learning 59 Experience/practise 24 Practice placements 11 Not specified Not specified 84 In interviews, many managers discussed locum cover and ‘back fill’ as an important requirement to allow training to take place. However, among resource need described in PDPR analysis (Table 21), this was specifically quoted by only 6% of respondents. Time and finance resource needs appeared most frequently. Staff noted some ‘skill needs’ that did not have an identified ‘resource need.’
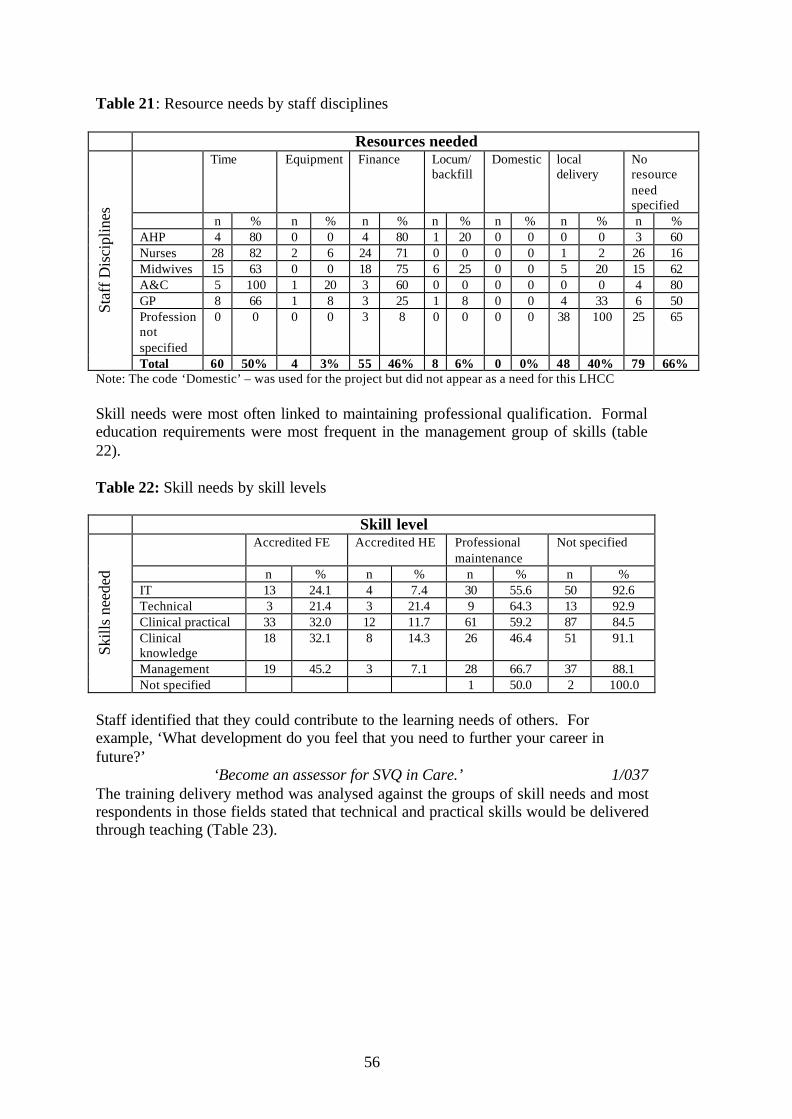
56
Table 21: Resource needs by staff disciplines
Resources needed Time Equipment Finance Locum/
backfill Domestic local
delivery No resource need specified
n % n % n % n % n % n % n % AHP 4 80 0 0 4 80 1 20 0 0 0 0 3 60 Nurses 28 82 2 6 24 71 0 0 0 0 1 2 26 16 Midwives 15 63 0 0 18 75 6 25 0 0 5 20 15 62 A&C 5 100 1 20 3 60 0 0 0 0 0 0 4 80 GP 8 66 1 8 3 25 1 8 0 0 4 33 6 50 Profession not specified
0 0 0 0 3 8 0 0 0 0 38 100 25 65
Staf
f Dis
cipl
ines
Total 60 50% 4 3% 55 46% 8 6% 0 0% 48 40% 79 66% Note: The code ‘Domestic’ – was used for the project but did not appear as a need for this LHCC Skill needs were most often linked to maintaining professional qualification. Formal education requirements were most frequent in the management group of skills (table 22). Table 22: Skill needs by skill levels Skill level
Accredited FE Accredited HE Professional maintenance
Not specified
n % n % n % n % IT 13 24.1 4 7.4 30 55.6 50 92.6 Technical 3 21.4 3 21.4 9 64.3 13 92.9 Clinical practical 33 32.0 12 11.7 61 59.2 87 84.5 Clinical knowledge
18 32.1 8 14.3 26 46.4 51 91.1
Management 19 45.2 3 7.1 28 66.7 37 88.1
Skill
s ne
eded
Not specified 1 50.0 2 100.0 Staff identified that they could contribute to the learning needs of others. For example, ‘What development do you feel that you need to further your career in future?’
‘Become an assessor for SVQ in Care.’ 1/037 The training delivery method was analysed against the groups of skill needs and most respondents in those fields stated that technical and practical skills would be delivered through teaching (Table 23).
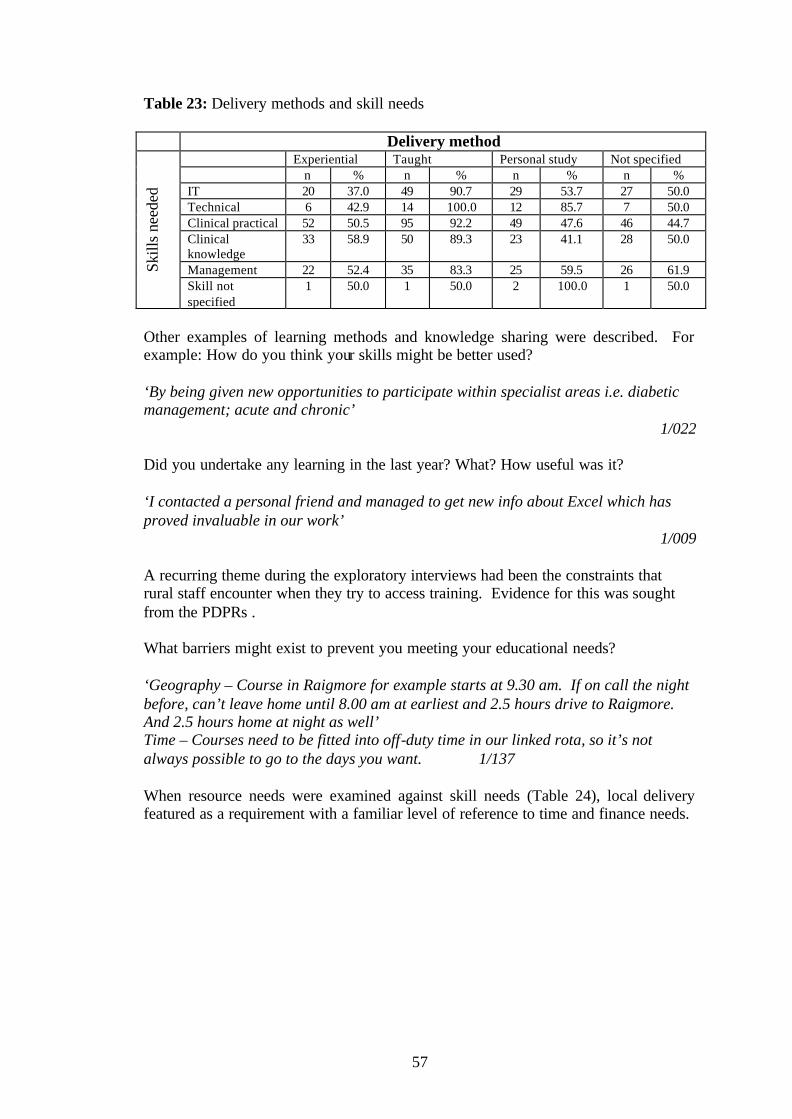
57
Table 23: Delivery methods and skill needs Delivery method
Experiential Taught Personal study Not specified n % n % n % n % IT 20 37.0 49 90.7 29 53.7 27 50.0 Technical 6 42.9 14 100.0 12 85.7 7 50.0 Clinical practical 52 50.5 95 92.2 49 47.6 46 44.7 Clinical knowledge
33 58.9 50 89.3 23 41.1 28 50.0
Management 22 52.4 35 83.3 25 59.5 26 61.9 Skill
s ne
eded
Skill not specified
1 50.0 1 50.0 2 100.0 1 50.0
Other examples of learning methods and knowledge sharing were described. For example: How do you think your skills might be better used? ‘By being given new opportunities to participate within specialist areas i.e. diabetic management; acute and chronic’
1/022
Did you undertake any learning in the last year? What? How useful was it? ‘I contacted a personal friend and managed to get new info about Excel which has proved invaluable in our work’
1/009 A recurring theme during the exploratory interviews had been the constraints that rural staff encounter when they try to access training. Evidence for this was sought from the PDPRs . What barriers might exist to prevent you meeting your educational needs? ‘Geography – Course in Raigmore for example starts at 9.30 am. If on call the night before, can’t leave home until 8.00 am at earliest and 2.5 hours drive to Raigmore. And 2.5 hours home at night as well’ Time – Courses need to be fitted into off-duty time in our linked rota, so it’s not always possible to go to the days you want. 1/137
When resource needs were examined against skill needs (Table 24), local delivery featured as a requirement with a familiar level of reference to time and finance needs.
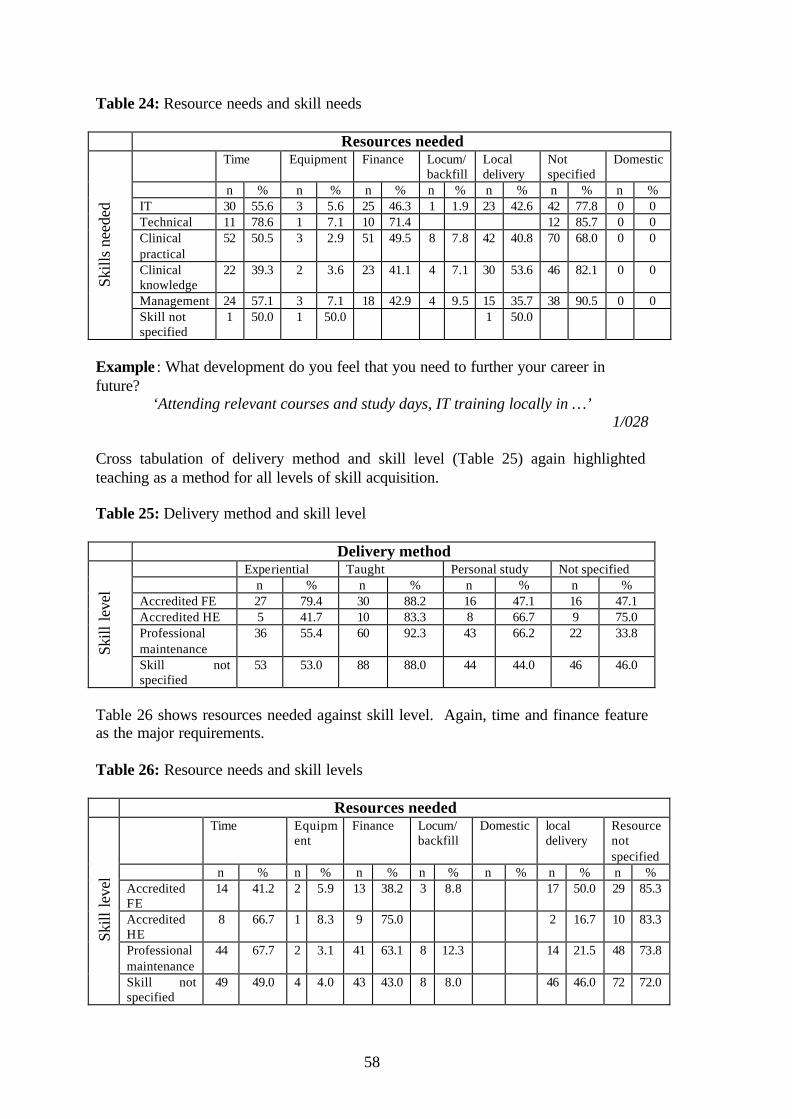
58
Table 24: Resource needs and skill needs Resources needed
Time Equipment Finance Locum/ backfill
Local delivery
Not specified
Domestic
n % n % n % n % n % n % n % IT 30 55.6 3 5.6 25 46.3 1 1.9 23 42.6 42 77.8 0 0 Technical 11 78.6 1 7.1 10 71.4 12 85.7 0 0 Clinical practical
52 50.5 3 2.9 51 49.5 8 7.8 42 40.8 70 68.0 0 0
Clinical knowledge
22 39.3 2 3.6 23 41.1 4 7.1 30 53.6 46 82.1 0 0
Management 24 57.1 3 7.1 18 42.9 4 9.5 15 35.7 38 90.5 0 0
Skill
s ne
eded
Skill not specified
1 50.0 1 50.0 1 50.0
Example : What development do you feel that you need to further your career in future?
‘Attending relevant courses and study days, IT training locally in …’ 1/028
Cross tabulation of delivery method and skill level (Table 25) again highlighted teaching as a method for all levels of skill acquisition. Table 25: Delivery method and skill level Delivery method
Experiential Taught Personal study Not specified n % n % n % n % Accredited FE 27 79.4 30 88.2 16 47.1 16 47.1 Accredited HE 5 41.7 10 83.3 8 66.7 9 75.0 Professional maintenance
36 55.4 60 92.3 43 66.2 22 33.8
Skill
leve
l
Skill not specified
53 53.0 88 88.0 44 44.0 46 46.0
Table 26 shows resources needed against skill level. Again, time and finance feature as the major requirements. Table 26: Resource needs and skill levels Resources needed
Time Equipment
Finance Locum/ backfill
Domestic local delivery
Resourcenot specified
n % n % n % n % n % n % n % Accredited FE
14 41.2 2 5.9 13 38.2 3 8.8 17 50.0 29 85.3
Accredited HE
8 66.7 1 8.3 9 75.0 2 16.7 10 83.3
Professional maintenance
44 67.7 2 3.1 41 63.1 8 12.3 14 21.5 48 73.8
Skill
leve
l
Skill not specified
49 49.0 4 4.0 43 43.0 8 8.0 46 46.0 72 72.0

59
Example from PDPR: Any additional comments? Obstacles or barriers? ‘Distance from training opportunities and lack of courses in Scotland’
1/010 The resource group of codes included opportunity as an individual field, an example is given below. Resource needs and delivery methods are compared and there is apparent willingness to undertake personal study if time is available. (Table 27). Table 27: Resource needs and delivery method Resources needed
Time Equipment Finance Locum/ backfill
Domestic local delivery
Resource not specified
n % n % n % n % n % n % n % Experiential 31 53.4 3 5.2 28 48.3 7 12.1 24 41.4 44 75.9 Taught 53 51.5 3 2.9 49 47.6 8 7.8 42 40.8 68 66.0 Personal study
43 75.4 3 5.3 35 61.4 4 7.0 6 10.5 44 77.2
Del
iver
y m
etho
d
Delivery not specified
23 46.0 4 8.0 21 42.0 3 6.0 24 48.0 43 86.0
Example from PDPR : Any additional comments? Obstacles or barriers? ‘In remote and rural areas where GPs are dispensing doctors the opportunity to use my nurse prescribing skills is extremely limited’
1/050

60
Performance Assessment Frameworks (PAF) The analysis of the PDPRs has highlighted learning issues for individuals. The following summary of performance from the 2 participating Primary Care Trusts identifies those areas of service where further organisational development is envisaged. Performance assessment summaries for all 3 LHCCs were made available to the study. j k The comments recorded here do not necessarily apply to all the LHCCs in the study and are paraphrased from the PAF fields for the recording of self-assessed important weaknesses. Targets for the PCTs are determined by the SEHD for local application. This deals with primary care modernisation and investment funding, and quality issues for practices that include accreditation and patient access. Three staff groups are identified as having a role in this modernisation and quality drive by addressing the nurse’s role in public health, a local Dental Action Plan and implementing a pharmacy strategy. The final section of the PAF reports is described in full and paraphrased only to protect the identity of the LHCCs. These comments capture areas where strength was identified but there were important areas of development for the organisations to address:
?? Collaboration between primary and secondary care through LHCCs could be closer
?? Variable governance structures related to capacity
?? The lack of widespread engagement of dentists and optometrists with
LHCCs
?? Variable understanding of LHCC function and benefit to patient care
?? The need to re-engineer LHCCs to align more closely with Local Authority boundaries and avoid duplication while building on the good work of the existing LHCCs
?? Managed Clinical Care Networks are working in some areas and not in others
?? The need to achieve greater devolution of responsibilities within a locality framework
?? The primary care perspective is inadequately represented in planning processes to date
j Primary Care performance assessment framework 2002/3 NHS Argyll and Clyde k Primary Care performance assessment framework 2002/3 NHS Highland

61
?? LHCCs need to be equipped to take on the wider responsibilities envisaged for them by the ongoing national work for joint working in support of the Community planning process.
Rural healthcare staff training costs A project officer involved in Continuing Professional Development policy initiatives supplied a 12 month diary summary for delivering training in one of the LHCCs (Table 28). This shows the considerable cost, related to mileage expenses, of delivering a training service in an area with little public transport. Table 28: A 12 month diary summary of a project officer engaged in a rural training initiative January to December 2003 Days Miles Cost
£s LHCC meetings 5 440 176.00 Training sessions (144 staff) 21 3437 1374.80 1 day Conference attendance 2 312 124.80 CPD project 48 4782 1912.80 Total
76
8971
£ 3588.40

62
63
ANALYSIS AND DISCUSSION This study defines important characteristics of practices located within rural and remote LHCCs, which distinguish them from urban LHCCs. It also provides some useful insights into the training needs of individuals working within the rural LHCC. The principal characteristics of rural and remote LHCCs are diversity and “clinical peripherality”.
Diversity is apparent in the geographic and demographic characteristics of practices, and in the roles adopted by individual professionals, who may need to fulfil a wider range of functions than would be expected in an urban setting, albeit working with a smaller practice population. Clinical peripherality is a useful way of expressing and quantifying aspects of rural practice that reflect demography, geography and transport links. In this study, we have shown that clinical peripherality is related to the spectrum of roles of rural practitioners. This, in turn, impacts on training requirements. A number of themes related to geography and demography emerge from this study. Within the rural LHCCs, population density is low but there is considerable variation between practice locations. This variation is less when density is measured at Ward area statistic level, compared to Census Output Area (COA). The former statistic more accurately reflects the sparsely populated patient catchment areas, and provides an opportunity for individual study results to be compared. Figures are available for all Scotland and similar measures could therefore be derived for the rest of the country. These rural and remote areas, in which tourism is an important part of the economy, have proportionately greater numbers of tourists in relation to the resident population compared to the urban area. This has a potential impact on health care providers, especially in terms of emergency and urgent care episodes. Visitor numbers, and their influence on NHS resource use, are recorded poorly by practitioners since the abandonment of re-charges and the Extra Contractual Referrals system. This is regarded by those interviewed to have been financially significant and is noted as a particular problem. 76 There is no incentive for inducement practices to record / keep data on temporary residents. Accident and Emergency departments in the area were not able to provide information on UK visitors. However figures for Scotland show that, on average, 30% of road traffic accidents in rural areas are serious or fatal compared to 19% in urban Scotland,35 and tourists are involved in such accidents. The impact of tourism is reflected in the ambulance figures, where summer calls are more frequent than winter calls. Variation in ambulance activity between postcode sectors may also partially reflect effects of temporary residents, as well as variations in resident populations. Both providers and users describe the impact of tourism on service provision as a burden on resource that has been formulated only with respect to the resident population.32 Population health and demography was not the remit of this study. However population shift of young people from rural to urban areas is recognised, 3, 11 and this contributes to the economic fragility of the area and staff recruitment and retention difficulties. 77

64
Clinical Peripherality The residents, both patients and staff, of West Highland experience difficulties of access to acute NHS facilities, as a result of the geographic barriers of poor roads, mountains and extensive coastline. Many practices serve areas that are peninsular in the sense of being almost surrounded by water or mountains but also by poor quality of the ‘lifeline’ access roads that serve communities and contribute to total travel times. The level of this varies greatly between practices within each rural LHCC. There are no noticeable differences in total travel time measurements between practices in the urban LHCC. Economies of scale can be achieved by providing services for population clusters 31
and is the sensible course for surgery location, although present locations are largely determined by historical factors rather then contemporary planning. Asthana notes that there is reduced scope for sharing services with neighbouring providers in a Health Board that shares only one border with another authority. Access deprivation in the study area is understandable given the population sparsity, the land mass and the peninsular nature of health communities, LHCCs and Health Boards. Peripherality influences clinical decisions by local practitioners. A lengthy journey may influence a clinician to request early transfer of patients to an acute centre before a definitive diagnosis can be made, for example in a case of croup or premature labour pains. It is considered wiser to tolerate the repercussions of sending a patient who has ‘got better’ during the journey time than to procrastinate and have a patient’s condition worsen miles away from help. Travel time is linked to risk and is therefore distinct from travel time that is merely inconvenient.49 Clinical management in the rural LHCC reflects these geographical facts and acute receiving hospitals must appreciate that different thresholds for admission exist. Road ambulance response times are longer than in urban areas and interviewees reported tourist traffic as an additional seasonal impediment to rapid patient transfer. Audit times show that following patient contact, lengthy road transfers are necessary in many parts of the study area. The nature of care required during prolonged ambulance transfers may differ significantly from that in a rapid, urban, transit. Ambulance leaders express concern that simple measures of care, for example inhaled pain relief, are not suitable over the total travel time. Patient access to emergency care is reduced, and the need for local emergency care providers is increased. Under the Helicopter Emergency Medical services (HEMS) regulations there are dedicated ambulance aircrew and detailed operational procedures; HEMS aircraft cannot be despatched to non-surveyed areas at night and can only be used in non HEMS mode for secondary transfers at night utilising dedicated landing sites with approved illumination. Air transport is considered appropriate where it is believed that there is a genuine clinical benefit that can be justified by the requesting authority. The only absolute indication is for an emergency where use of air transport has demonstrable advantages over land resources.74 Air travel choices were not included in local measurement of time, distance and mode of travel to a hospital accepting acute admissions and therefore direct comparison in total travel time can be made across practices and LHCCs.

65
Peripherality also applies to administrative and educational requirements of remote and rural LHCCs. Administrative and educational outreach initiatives require long journeys, often complicated by more than one transport mode, to practices in rural LHCCs. This is further discussed in the analysis of training requirements. Working within resource and geographic constraints, staff in rural areas must be able to evaluate what health care intervention is of value, reliable, convenient and accessible. In rural life, the mode of knowledge/healthcare acquisition is influenced both by the “what” of staff and patients needs and the “how” of getting it. A pattern of rural health care emerges that is demonstrably different from urban care and must be responsive to local circumstances. This caut ions ‘against an international trend for government medical/clinical governance policy that contradicts community empowerment strategy’. l Workforce Information The Seeking Solutions conference of March 2000 hypothesised that the more remote the community, the fewer the health services that can be found and delegates noted that this position should be made ‘explicit and transparent’ 62 This characteristic is evident in all rural LHCCs in the study, but there is great diversity in composition of the healthcare team, and individual roles within that team, in rural areas. A recent Australian study concludes that the more rural or remote the area the more likely a GP is to be regularly engaged in complex care and, most importantly, the findings have implications for the workload, responsibility, vocational satisfaction, need for professional education and support, and costs and remuneration of practice.78 The impact of changes in the team may therefore be much greater in rural areas. Individual community profiles show that removal of one member of staff from an area for a time period can deplete the healthcare provision by up to 100% in areas such as islands and remote communities. Two island communities of low population reported that the GP ‘does everything’, other populated islands without a surgery are staffed by single-handed nurses who ‘do everything’. This finding is consistent with a study of the range of General Practice curative services in Europe, which found that rural practices provided more comprehensive services than urban practices regardless of the healthcare system. 79 As many work with small populations the level of support from allied professions and peers is limited in isolated areas and certain fields of care. For all staff the lack of ‘critical mass’ of practice within small populations confers a greater need for refresher training and this is discussed below. As small populations limit the representation of health professionals, the health role of other public servants and community members may become more prominent. Consider the example of mental health problems. In the last twenty years male suicide rates in Highland have been consistently higher than Scotland as a whole, even excluding non-residents. 80 However, there are few community psychiatric nurses for the geographic area. This impacts on generalists and indicates the need for a broad-spectrum knowledge base for isolated practitioners. Many remote and rural
l Conference proceedings, Mueller K, International Rural Network Conference, Inverness, June 2003

66
staff deal with patients with significant mental health problems because there is no other resource. There may be close collaboration with the local constabulary who, in one of the LHCC areas, stated that one third of their time is spent dealing with mental health issues. This involvement in healthcare by individuals employed in other sectors has also been observed in other countries. For example, in remote Canadian communities the ‘paraprofessional’ is an acknowledged and valued role, although conflicts and differences of opinion over management may occur between these individuals and more orthodox professionals. 81 This type of activity is described by some as inter-sectoral working (see below). 82 Flexibility of local staff in responding to a broad spectrum of need given sparse numbers of health practitioners and patients was demonstrated in these rural LHCCs. Not only do practitioners conduct their normal paid work but they also contribute to the social environment of their communities by acting as volunteers for rescue services and sports teams etc. Unscheduled and out of hours care is often provided by the local practice alone and there may be high dependency on one or two individuals. Diagnostic and clinical management skills employed might not be distinguishable from urban practice, however travel issues (for example private boat), and weather conditions (for example snow that closes the short cut over a mountain pass) may add considerably to the time spent on care delivery that is measured as one patient contact. The location of ‘A&E’ and ‘Acute admission’ hospitals was established after consulting the local health workforce. Community hospital facilities, supported by GPs, cater for other areas of care. This description of hospital proximity and the way in which Primary Care organisations combat access deprivation is not apparent in national surveys of drive time. 48 Personal development planning and reviews There is only limited literature on the subject of assessing GPs educational needs. 83 Myers highlights the difficulties and notes resentment at being assessed by teacher-centred and top-down methods, emphasising the need to link the relevance of educational material to GPs actual practice. This current study undertook a simple exercise to establish current GP educational needs in the run-up to more sophisticated evaluation. As new policies take hold quality assessments may begin to provide Postgraduate Centres with evidence of training needs. 50 Resources All staff groups reported that protected time was required for learning, acknowledging that there were fees and costs associated with the location of the training. Study leave for staff is considered necessary to support the development of a wide range of skills 76 and is the key to promoting effective and appropriate care 84, 85 Respondents associate time allocation for learning with the delivery method. Evidence was available from PDPR analysis and the community profiling exercise to demonstrate the excess requirement for time allocation to account for overnight accommodation; rail, air and ferry links; and adverse weather conditions affecting road and sea travel.
67
Delivery method The preferred method of delivery for all groups was through teaching, while nurses and doctors also recorded personal study as an option, and midwives and allied health professionals recorded a need for experiential learning opportunities. Preference for interactive delivery methods are reported for rural practitioners in America and Australia 86, 87 The LHCC selected for PDPR analysis had not had exposure to the BASICS course but did name other ‘taught’ emergency courses. The work of Kiger et al, in exploring the development of maternity skills in remote areas found that interviewees had a clear preference for emergency and scenario-based training.24 Self directed learning is reported as an appropriate method of meeting continual educational needs of rural nurses in their efforts to overcome the many obstacles to professional growth in rural practice. 88 In rural Canada family physicians rated funding for learner-driven continuing medical education and limiting on-call duty as the most important education and practice solutions. 89 Skill requirements Named skills were analysed by group and the most common group was ‘clinical practical’ skills. Some detail was lost in this funneling exercise and it was necessary to list the frequency of skills requirement separately. IT, from the management group of skill needs, was listed as the single most common skill requirement. Technology based learning is listed as a delivery method and has been found to be an effective medical education tool.90 This suggests that IT skills training is a priority if the preference for personal study through technology based learning 43 is to become a reality. Muellerm suggests that preferences for services are based on ‘security needs’, i.e. a safety net, not necessarily proven healthcare needs. Hopton et al have posed a question: ‘Where is patient care in all this?’ 37 Discussion of local training needs in rural areas have a focus around priorities of healthcare provision confirmed by patient and public involvement initiatives. 10, 32 These are listed for rural communities in the area as ?? Life threatening conditions ?? Short term acute conditions ?? Long term treatable conditions ?? Lifelong conditions Emergency clinical skills appear in the analysis of more frequently requested skills training and with needs identified at LHCC level. These are discussed below.
m Conference proceedings, Mueller K, International Rural Network Conference, Inverness, June 2003 Mueller – IRH conference 24th June 2003

68
Integrated care and development planning The LHCC Best Practice group and other literature refer to the need to address LHCC infrastructure difficulties and also refer to the essential development of multidisciplinary and multi-agency participation if the potential for local working is to be fulfilled.39,42 Lessons learned elsewhere list philosophical and professional barriers to collaboration and consider that agreed aims, agendas, project ownership and leadership are important features of multi agency working. 91 Whilst Munro et al argue that the case for multidisciplinary learning remains unproven 92 this type of collaboration is set to feature more often in future community care planning in Scotland. 45, 93 LHCC leaders have suggested at interview that difficulties are in clinical leadership and not management. Managers list protected time,1 local/contextual application,76 investment and accessibility issues in training and development planning and this is supported by the completed PAF and results of PDPR analysis. Managers report that identifying staff training needs is the easy part and that staff are generally reasonable about their needs; they recognize the enormous practical difficulties of accessing training. Clinical skills training is the most difficult to access and staff are encouraged to be innovative/imaginative with placements, rotation and job swaps. LHCC leaders report that the uptake of the BASICS Scotland courses run nationally by the team at BASICS Education Scotland indicate the need for courses dealing with clinical emergencies. This course was not named in the PDPR analysis and it was suggested that some GPs have a different view of immediate care (e.g. ambulance staff do it, not GPs). Given the large mileage covered and distance from any central site, all health care professionals might expect to encounter emergencies such as road traffic accidents. Douglas et al remind us that in a rural clinical emergency it is likely to be the frontline generalist who responds and refer to advanced planning and multidisciplinary team training for unexpected clinical emergencies. 94 BASICS course evaluations show high appreciation of this type of ‘fire fighting’ course; ‘taught’ methodology delivered locally may account for its apparent success as an educational model. This programme has not had external evaluation and would benefit from an analysis of the relevance of course content and its applicability to rural practice. Rural healthcare staff training The SIMD 2001 domain for Education, Skills and Training deprivation 30 in Scotland was analysed. Diversity was demonstrated in results for both urban and rural LHCC. The SIMD score refers to non-vocational primary, secondary and tertiary education and does not suggest significant education deprivation in the area. However this does not reflect the difficulties of rural professionals aiming to maintain, up date and increase their professional standards of care.24,60,88, 95,96
69
Critical mass In some areas of West Highland population based resource is unable to support the minimum team required for specialisation. Specialisation tends to ‘squeeze out generalist healthcare skills which look at the whole person’,62 and reduce flexibility. The Acute Services Review found that a quality outcome from low volume activity ‘may seem counter intuitive to clinicians’. Possible explanations for any volume-quality relationships which do exist include the skill and experience of individual clinicians through sub-specialisation, working to protocols, overcoming ‘learning curve’ effects, adoption of ‘best’ techniques, quality of facilities, skill of supporting staff, inter-specialty links and team working. 48 In their study of the impact of practice size, Campbell et al conclude that some markers of practice performance are related to the total number of patients cared for but an over simplistic approach that fails to account for the views of patients as well as health professionals is likely to be disadvantageous to service planning.97 National policy for flexibility of care provision puts emphasis on managed clinical care ne tworks and comments on the policy driver for ‘training specialists within primary care and generalists within secondary care’ 50 other reports suggest that the primary care specialty is ‘generalism’. 62, 98 Formal accreditation to practice is required of some staff groups, e.g. midwives, and this also applies to those who take on dual or triple nursing duties where one of those duties is midwifery. There is growing recognition that triple duty nursing is not feasible in some areas 57 and experience of births is reduced due to the multiplying factor on roles and reduced fertility rates in parts of the study area. 11, 24 Strengths and Weaknesses of the Study Data gathering was focussed at the level of individual practice communities and individual practitioners. National data were used where appropriate in generating practice profiles, but these were then subjected to validation by local consultation. The 86% response to this exercise lends credibility to the findings. The response rate compares favourably with other profiling studies. 78, 79, 97 We are unaware of previous work at this level of detail in Scotland and this has provided valuable insight into what constitutes a ‘Rural LHCC’. Lessons learned from Local Authority planning, National Health Service and Primary Care health information management 99 have been applied to the creation of unique sets of characteristics of rural health communities. Many of the markers are available nationally and data on population density, settlement size and access to public and retail services form the basis of rural definitions. Ease of access to, and use of postcodes by, national databases influenced some data collection. The model used to assess the degree of Clinical Peripherality is readily transferable to other Scottish Health Boards. The aim of the study was to describe the rural profile of West Highland LHCCs and the impact on staff development. The definition of rurality has important implications for the way in which service needs and problems of access are interpreted.31 Rurality contributes to deprivation where it restricts access to a commodity and so it was necessary to add total travel times to establish understanding of the rural barriers to patient care and how those same barriers influence the development of staff. Ward level generic deprivation indices are unlikely to provide

70
a true reflection of levels of deprivation in rural practices.100 This study has employed measurements that are specific to each practice area. Following discussion with local stakeholders and public service providers a more specific local data collection was developed. Transport consultants and ferry operators provided information on sea journeys that illustrated the frequency of sea crossing, the influence of adverse weather conditions and seasonal timetables. Nationally accessible geographic databases were found to be reliable in description of length of road journeys but did not account for single-track road travel time. Despite increased sophistication, some geographic detail such as a sea crossing is lost in public databases that give advice on proximity of services by linear measurement. Martin et al anticipate that it will be possible to assemble comprehensive public transportation data in the future and that it will no longer be appropriate to use indirect measures on the basis that they are the best proxies for real transport information in the planning of service delivery.101 The complexities of travel in the region are augmented with information from the Scottish Ambulance Service. Acknowledging the need for sufficiently detailed results to avoid anomalies arising from nationally aggregated data 102 and the dangers of application of large area measurements to small communities 23 it has been possible to add objective seasonal data for the incidence of ambulance use in the area. Tourist data from the Highlands and Islands Enterprise supports comment from health care staff in popular tourist zones.75 Douglas notes the difficulties arising from heterogeneity of boundaries in data aggregation103 but in the absence of any other guide it is useful to include an estimate of tourist activity. Additions were made to the main dataset following respondent comment. Geographic and travel data were hand searched and corrections were made to nationally available data. An analysis was made of all data fields and graphs have been displayed in results where differences between rural and urban LHCCs can be demonstrated. Limitations The work was undertaken during a period of policy adjustment for staff in the NHS and implementation coincides with the completion of this project. It is particularly difficult to measure the different representations of rural expertise given the number of policy changes that are contributing to ‘change fatigue’ in the study area. Evidence from communication with GPs suggests that the new GMS contract and Out Of Hours care opt-out may have influenced some of the replies. It would have been useful to include a PDPR analysis for the two other LHCCs in the study, however one LHCC was undertaking a major change initiative and the other was heavily committed to PDPR training and did not have representative information available at the time.

71
CONCLUSIONS AND RECOMMENDATIONS The ambition to deliver quality care within a constrained financial resource is a driver for modernisation that is shared by rural healthcare workers. Each working environment requires different skill sets and the rural health practitioner requires a wide-ranging array of knowledge and skill to deliver care to the patient and access clinical and educational support for themselves. In rural communities, potential gaps in health service delivery due to lack of specific personnel are filled by other generalists. This results in: ?? Increased pressure for broad spectrum practice ?? Increased pressure on training provision ?? Increased time resource requirements This study has described the diversity of practice required of all staff groups in the rural setting. Given the public access to health information that is available through the Internet and other sources, the health professionals’ uniqueness is no longer in holding knowledge but in so-called ‘knowledge skill’ (appraising it for general validity and patient specific relevance) as well as practical skill. 104 Communities have visiting professionals and tele-contacts offering clinical management advice and practical support. The level of presence in the community may vary but communications channels exist for ‘local generalists supported by distant specialists’.n Extensive national exercises in job analysis 64 and appraisal are currently taking place and job descriptions will become formalised as part of ‘Agenda for Change’. Clinical skills acquisition is linked to models of care and intervention designed by various healthcare professions. Until the fairly recent development of healthcare partnerships the development needs addressed by local staff managers and professional colleges lacked coherence. Rural roles are multifaceted and experience shifts in focus to enable service provision during times of contractual change and revision of administration structures. This results in the learning and development needs of staff being met from multiple sources and is a flexibility that can be preserved. Whilst the needs of the professions are unique the skills of managing diversity of health care practice in rural areas are generic.108 Recommendation Multidisciplinary rural practice management training should be available. This would include human resource management, communications, setting organisational goals, managing effectiveness and leadership.
n Strasser Conference International Research Network – Inverness 24th June 2003
72
Local communities are tolerant of ‘rural’ difficulties and the communication chain between patients and the NHS is short. There is felt to be an increased public involvement. There are close links in these rural areas with other public service sectors. The business plans of the NHS are closely associated with the needs of patients and public and in a two way communication process it is the individuals closest to the public interface who act as catalysts for change. These professionals, practitioners and clinicians create and maintain the necessary conditions to achieve public health objectives for residents by: identifying who they are; knowing what it is that they require; offering choices, as far as possible; facilitating their contribution to proposed service changes. Economy of scale in public health orientated, non-clinical training is now feasible through the Joint Futures project where local community care schemes, social services and privately run care homes would jointly undertake some forms of training. Inclusion of NHS staff may help with the economics of training delivery to small groups; multi-organisational group training is another way to link the NHS to local services and communities Training opportunities can be shared with police, nursing, medicine, social work, housing and education in, for example: mental health awareness; substance dependency; moving and handling (people, without hospital aids), fire; IT; accident and ‘events’ behaviour; child protection; driving; aggression; teaching and presentation; management – time management, recruitment, selection etc.
There are concerns that some staff miss out on staff governance issues and NHS learning development because they are employed directly by the GMS GP. Each Local Enterprise Company has a skills lead and generic skills training that could be made available to employees of the NHS. A GP learning IT skills with someone from a local small/medium business enterprise, e.g. the manager of a fish farm, would allow NES resource to be focussed more clinically. IT skills to support personal learning are a priority for the NHS and a priority for making global connections for the Highlands and Islands Economic community.105 Shared IT training and collaboration between organisations represents efficient and economical use of training resources. Increased levels of IT knowledge in the healthcare community have been shown through PDPR analysis to enhance the opportunity for personal study through technology-based learning.
Recommendation NHS organisations should actively explore inter-sectoral training in rural communities. Consideration should be given to outsourcing non-clinical training and accessing what already exists via the local enterprise companies.

73
Lengthy ambulance response times suggest that First Responders (public or staff) require skills that will support them through the initial period of ‘first aid’ and into some paramedic fields of care, for example defibrillation. Lengthy transfer times increase the need for extended transport care, e.g. nurse escorts on military air transport, analgesia administration by paramedics. In rural Australia an ambulance medical officer has been able to facilitate co-operative relationships between rural ambulance staff and rural health practitioners through shared teaching.106. Participants welcome clinical ‘fire-fighting’ courses and their models of delivery as interventions. This ‘multidisciplinary taught’ model might be considered for grouping other skills requirements. Where solo healthcare workers ‘do everything’ it is appropriate to offer nursing skills training for example wound care, to GPs. GPs are beginning to be supported by nurses with extended skills and given the issues of workforce sparsity this is to be encouraged by supporting those who are facing a cultural change in the healthcare hierarchy. Recommendation Multidisciplinary clinical training should be enhanced for rural health care workers The LHCC has a teaching role in communicating local knowledge of risk management to the receiving hospital. There is suggestion that some departments, distanced from the LHCC, are probably not aware of LHCC needs, claims are also made that there is little understanding of the role of some Trust departments at LHCC level. The organisation is ‘a bit of an irrelevance to staff on the ground’. Where specialism is defined as a field of care management rather than a disease topic for example nursing, management, physiotherapy or chiropody etc., the practitioner takes on a leadership role and may require appropriate training such as the Royal College of Nursing Clinical Leadership course and the Xceed programme. 107 Clinical isolation and population sparsity contribute to the lack of learning opportunity. The act of preparing for and giving training is an example of how a rural clinician might up-date their own knowledge. This is supported by the results of PDPR analysis, which show that there is a demand for teaching and presentation skills. It is argued that staff registration as a training resource and facility development as a training site limits the availability of staff for clinical contact time. However there is potential for local recruitment of trainers that can be supported by resource allocation. Recommendation Rural teaching and preparation for rural teaching should be accredited as CME/CPD

74
Resources to reduce barriers of geography include telemedicine, video links, telephone peer support, while resources to reduce barriers to opportunity include protected time, locum cover, local venue and sensitive scheduling. Access to training can be expressed as = 1 / Barriers. Multidiscip linary protocol teaching, delivered locally will address economy and reduce strain on backfill. Awareness of rural issues will be raised as teachers discuss their experiences and ‘take the message back’ to central offices. Recommendation Use should be made of e-health resources to deliver teaching and training. Particular consideration should be given to ‘Roadshow’ delivery of training Motivational issues are addressed by linking training to risk management, business goals, personal need and social needs. Hidden costs to those who are highly motivated include spending their social hours on professional and business development. Recognition of this commitment through increased resource will support policies to recruit and retain rural healthcare staff. Recommendation The constraints on resources of time and finance for learning and development should be addressed in the same spirit as the allocation of resource for rural service delivery. Comparisons of urban and rural access at local and ward level will support programme planning by flagging up the potential difficulties of enrolment to centralised training courses. The scheduling and design of training provision requires innovative solutions as traditionally designed courses can act as a barrier to course enrolment for the rural practitioner. For example ?? Solo workers: one fortnight a year away for all training – locum provision more
straightforward, time protected ?? Distance issues addressed by travel sensitive timing for example a 1pm start, 1
overnight stay and an early afternoon finish ?? Traffic congestion and increased caseload commitment avoided by planning
sessions outside the tourist season in spring and autumn Recommendation Innovative scheduling of training should be developed

75
Our analysis has shown that rurality has two key impacts on the quality of health service delivery: practitioner access to training is reduced and the need for emergency training is increased. In evaluation participants have expressed satisfaction with ‘firefighting’ courses such as the BASICS, ALS, ALSO, APLS courses. What is less clear is how these skills are utilised post-course and how the skills are retained; use of new skills, if required, is likely to have high impact but skill retention suffers from low frequency of practise. Recommendation Evaluation should be performed of short accelerated clinical emergency courses and their educational models The diversity of delivery methods suggests alternative choices for addressing learning needs in rural areas. Interactive teaching and its association with networking, peer contact and connectivity with the ‘outside world’ emerged as the most sought after educational delivery method. Motivation may also be linked to the clinical isolation experienced by rural healthcare workers. Feeling part of the ‘big picture’, and having protected time, contribute to perceptions of one’s value to an organisation. In-depth study of these factors could inform future educational planning strategy. Recommendation Further research is required to explore whether isolation from peers influences the choice for ‘taught’ methodology in remote and rural CME/CPD There is increased need to link training and development planning to the public prioritisation of patient care needs. There is apparent mismatch in the perceived training needs described by individuals and those expressed by LHCC representatives. The PDPRs analysis showed that personal plans are not as rigorous in aligning with NHS business plans as one might have hoped. Two aspects of PDPR that were identified at analysis are professional need linked to business planning, and personal need associated with recruitment/retention of staff Recommendation Personal Development Plans should be linked to business planning and to patient and public involvement

76

77
REFERENCES
1. Solutions Group. Solutions for the provision of health care in the remote and rural areas of Scotland in the 21st Century. January 2002.
2. Audit Scotland. Paying Dividends. Edinburgh: Audit Scotland; April 2001.
3. Argyll and Bute Local Health Care Co-operative. A New Model of Integrated Rural health Care within Argyll and Bute. Argyll and Clyde: NHS; April 2002.
4. A Platform for Primary Care Research in Scotland: Project Summary. Available at: www.gla.ac.uk/projects/platform/. Accessed 30 November 2003.
5. Scottish Household Survey: 8 fold urban rural classification. Available at: http://www.scotland.gov.uk/library5/rural/asrs-23.asp.
6. Blackden S. From Physicians' Enquiry to Dewar Report: A Survey of Medical Services in West Highlands and Islands of Scotland, 1852-1912: Part 1. ; Proc.R.Coll.Physicians Edinb 1998; 28:51-66
7. Highlands and Island Medical Services Committee. Report to the Lords Commissioners of His Majesty's Treasury. ; 1912.
8. McLachlan G. Improving the Common Weal: Aspects of Scottish Health Services 1900-1984 Edinburgh University Press for The Nuffield Provincial Hospitals Trust, Edinburgh, 1985
9. Fraser Darling F. North Highland Survey: An essay in Human Ecology. ; 1955.
10. Clark J, Shapiro J, Spurgeon, P. and Willetts, J. West Highland Project: Final Report. Birmingham: Health Services Management Centre, School of Policy, University of Birmingham; February 2003.
11. Douglas I, Hopkins P, Stone G. Highland 2016: Population, Age and Reasons. Inverness: Highland Health Board; 2002.
12. Futureskills Scotland. The Scottish Labour Market 2002: Summary. Glasgow and Inverness: Futureskills Scotland; 2002.
13. Facing the Future: Nursing and Midwifery Recruitment and Retention Issue 2 January 2003. Available at: www.scotland.gov.uk/library5/health/ffnl-00.asp. Accessed 2/27, 2004.
14. EKOS Limited. Socio-Economic Impact of Traffic Restrictions on Lifeline Roads in the Highlands and Islands. ; April 2001.
15. Research Findings No 53: Car Dependence in Rural Scotland. Available at: www.scotland.gov.uk/cru/documents/rs53-01.htm. Accessed 01/03, 2004.
16. Shucksmith M, Philip L. Social Exclusion in Rural Areas: A Literature Review and Conceptual Framework. Scottish Executive Central Research Unit; 2000.

78
17. Shucksmith M, Chapman P, Clark M, Black S, Conway E. Disadvantage in Rural Scotland: How it can be experienced and how it can be tackled. Aberdeen: ; August 1994.
18. Jackson T. Transport and Economic Development in the Highlands and Islands; Occasional Paper No 47. ; 1994.
19. European Commission The Cork Declaration. The European Conference on Rural development, 9th November 1996; Cork, Ireland
20. Hanlon P, Possible Scotland. The Scottish Council Foundation; 2002.
21. Disadvantage in Rural Areas, The Rural Development Commission, Rural research report number 29, 1996
22. The RARARI Factfile. Available at: www.rarari.org.uk.
23. Farmer J, Baird G, Iversen L. Rural Deprivation: reflecting reality. British Journal of General Practice June 2001;51:486-91.
24. Kiger A. Sustainable Maternity Service Provision in Remote and Rural Areas of Scotland. Aberdeen: NHS Education for Scotland; September 2003.
25. Stroke Outcomes in Northern Scotland: Does Rurality Really Matter? Rural and Remote Health 3. Available at: http://rrh.deakin.edu.au.
26. Bromley C, Curtice J, Attitudes to Discrimination in Scotland. Available at: www.natcen.ac.uk/publications/b32483%attitudes.PDF.
27. Bailey N, Spratt J, Pickering J, Goodlad R, Shucksmith M. Deprivation and Social Exclusion in Argyll and Bute. Report to the Community Planning Partnership. Aberdeen: Scottish Centre for Research on Social Justice; February 2004.
28. Scotland's Census Results Online. Available at: www.scrol.gov.uk/scrol/analyser/. Accessed June, 2003.
29. Bailey N, Flint J, Goodlad R, Shucksmith M, Fitzpatrick, S. and Pryce, G. Measuring deprivation in Scotland: developing a long-term strategy. Scottish Centre for Research on Social Justice: May 2003.
30. Scottish Index of Multiple Deprivation. Available at: http://www.scotland.gov.uk/library5/social/siod-22.asp. Accessed 6/10/2003.
31. Asthana S, Halliday J, Brigham P, Gibson A. Rural deprivation and service need: a review of the literature and an assessment of indicators for rural service planning. University of Plymouth: South West Public Health Observatory; 2002.
32. Stone G, Swan G, Ludbrook A, Hopkins P. Designing Our Future. Inverness: Highland Health Board; December 2002.
33. Arbuthnott J. Fair Shares For All. Edinburgh: Scottish Executive; 1999.

79
34. Douglas JDM, Farmer J, Gillies G, Richardson K, West C, Macleod J, et al. "What can Scotland learn from Australia's experience of remote and rural healthcare policy?”. Scotland: RARARI; August 2002.
35. Sharples J, Fletcher J. Tourist Road Accidents in Rural Scotland. Edinburgh: Scottish Executive; 2001. Report No.: T2953.
36. The Scottish Office. Designed to Care: Renewing the National Health Service in Scotland. Available at http://www.scotland.gov.uk/library/documents1/care-axb.htm Accessed April 2003.
37. Hopton, J. and Heaney, D. Towards Primary Care groups: The development of local healthcare cooperation in Scotland. BMJ May 1999;318(7192).
38. Scottish Executive Health Department. Our National Health: A plan for action, a plan for change. Edinburgh: Scottish Executive Health Department; 2001.
39. Hopton, J. and Hill, M. Connecting Communities with the NHS. April 2001 (in press).
40. Scottish Executive Health Department. Rebuilding our National Health Service. Edinburgh: NHS Scotland; May 2001.
41. Wilson H, Brock J. LHCC Development: The Next Steps. Scottish Executive Health Department: ; July 2001.
42. The Primary Care Modernisation Group. Making the Connections. NHS Scotland; March 2002.
43. Scottish Executive Health Department. Partnership for Care: Scotland's Health White Paper. Edinburgh: Scottish Executive; February 2003.
44. Scottish Executive Health Department. A Partnership for a Better Scotland. ; May 2003.
45. Scottish Executive. National Health Service Reform (Scotland) Bill. 2003. Report No. SP Bill 6.
46. Scottish Executive Health Department. Community Health Partnerships: Consultation Paper on Guidance. Edinburgh: Scottish Executive; 2002. Report No.: AMI01607.
47. EUR-Lex. Working Hours Directive. Official Journal November 1993;L307.
48. Scottish Office Department of Health. Acute Services Review. ; May 1998.
49. Scottish Executive Health Department. Future Practice: A Review of the Scottish Medical Workforce. ; July 2002.
50. The Department of Health. Investing in General Practice: The New General Medical Services Contract. ; 2003.
80
51. NHS Management Executive. Junior Doctors: The New Deal. Management Executive: NHS; 1991.
52. The Scottish Office. Towards a Healthier Scotland - A White Paper on Health. ; February 1999.
53. Scottish Executive Health Department. Nursing for Health. ; March 2001.
54. Scottish Executive Health Department. Nursing for Health: Two years on. Edinburgh: Stationery Office; 2003.
55. WHO Europe. The Family Health Nurse: context, conceptual framework and curriculum. ; January 2000. Report No.: EUR/00/5019309/1300074.
56. Jarvie A. Family Health Nursing in Scotland: A report on the WHO Europe pilot. St Andrews House, Edinburgh: Scottish Executive; 2003.
57. MacDuff, C. and West, B.J.M. Evaluating Family Health Nursing Through Education and Practice. Edinburgh: Scottish Executive; 2003.
58. Deaville J. The Nature of Rural General Practice in the UK - Preliminary Research. Newtown, Powys: Institute of Rural Health; 2001.
59. Scottish Executive Health Department. The Right Medicine: A Strategy for Pharmaceutical Care in Scotland. Edinburgh: Scottish Executive; 2001.
60. NHS Education for Scotland. Education and Training for the Dental Team in Remote and Rural Regions of Scotland: Report of a Working Group. NHS Scotland; January 2003.
61. Scottish Executive Health Department. Building on Success: Future Directions for the Allied Health Professions in Scotland. Edinburgh: The Stationery Office; 2003.
62. Scottish Council. Seeking Solutions: Education and Training for Remote and Rural Health Professionals. March 2000.
63. Scottish Executive Health Department. Planning Together: Final Report of the Scottish Integrated Workforce Planning Group. 2002 Available at http://www.scotland.gov.uk/library3/health/ptfr-00.asp Accessed May 2003
64. Department of Health. Agenda for Change. Department of Health; March 2003.
65. The Scottish Office. Towards a New Way of Working - The Plan for Managing People in the NHS in Scotland. ; April 1998.
66. Scottish Executive Health Department. Learning Together. Scottish Executive Health Department; 1999.
67. Scottish Executive Health Department. Staff Governance Standard for NHSScotland employees. Scottish Executive Health Department; 2002.

81
68. Scottish Executive Health Department. Working for Health: The Workforce Development Action Plan for NHSScotland. ; August 2002.
69. Scottish Neighbourhood Statistics. Available at: www.sns.gov.uk/.
70. Chief Scientist Office. The Research Governance Framework for Health and Community Care. ; 2003.
71. Partnership Information Network (PIN) Board: Guideline Development Group. Personal Development Planning and Review. Scottish Executive Health Department. 2003
72. General Practitioner Workload. Available at: http://www.rcgp.org.uk/rcgp/information/publications/information/rcf0003/Rcf0003.asp. Accessed 3/14, 2002.
73. Making sense of The Red Book. Available at: http://www.redbook.i12.com/rb/Docs/rb692.htm. Accessed Sept 2003.
74. Scottish Ambulance Service. Your Guide to Air Ambulance Services 2002;(April).
75. EKOS Limited. Volume and Value of Tourism in the Host/Moray Areas. EKOS Ltd; October 1999.
76. Argyll and Bute Local Health Care Co-operatives. Integrating Primary and Community Emergency Care Services within Argyll and Clyde. Argyll and Bute LHCC; May 2001.
77. Futureskills Scotland. Skills in Scotland 2002: The employers' view. Glasgow and Inverness: Futureskills Scotland; 2002.
78. Humphreys JS, Jones JA, Jones MP, Mildenhall D, Mara PR, Chater B, et al. The influence of geographical location on the complexity of rural general practice activities. Medical Journal of Australia 2003; Oct 20;179(8):416-20.
79. Boerma W, Groenewegen, PP. and Van der Zee, J. General practice in urban and rural Europe: The range of curative services. Social Science and Medicine 1998;47(4):445-53.
80. PION Economics. Accounting for Rural Deprivation. ; August 2000. Report No.: Ref pe493.doc: Ver 1.3.
81. Minore B, Boone M. Realizing Potential: Improving Interdisciplinary Professiona/Paraprofessional Heath Care Teams in Canada's Northern Aboriginal Communities Through Education. Journal of Interprofessional Care 2002;16(2).
82. Scottish Consumer Council. Access to Primary Care services in Scotland: Final Summary report. Scottish Consumer Council; 2001.
83. Myers P. The Objective assessment of general practitioners' educational needs: an under-researched area?. British Journal of General Practice 1999;49:303-7.

82
84. British Association of Medical Managers. Clinical Governance in the new NHS. Cheshire: British Association of Medical Managers; 1998.
85. Bloor K, Maynard A. Clinical Governance: Clinician, heal thyself? Management policy in the new NHS. Institute of Health Service Managers. London 1998
86. Stancic N, Mullen PD, Prokhorov AV, Frankowski RF, McAlister AL. Continuing medical education: what delivery format do physicians prefer?. Journal of Continuing Education in the Health Professions 2003; Summer;23(3):162-7.
87. Wise AL, Hays RB, Adkins PB, Craig ML, Mahoney MD, Sheehan M, et al. Training for rural general practice. Medical Journal of Australia September 1994;161(5):314-8.
88. St Clair, C. and Brillhart, B. Rural nurses as self-directed learners: overcoming obstacles to continuing education. Journal of Continuing Education for Nursing October 1990;21(5):219-23.
89. Rourke JT, Incitti F, Rourke LL, Kennard M. Keeping family physicians in rural practice. Solutions favoured by rural physicians and family medicine residents. Canadian Family Physician 2003; Sep;49:1142-9.
90. Davis DA. The science and practice of continuing medical education: A study in dissonance. ACP Journal Club April 1993;118.
91. van Eyk, H. and Baum, F. Learning about Interagency Collaboration: trialling collaborative projects between hospitals and community health services. Health and Social Care in the Community July 2002;10(4):262-9.
92. Munro N, Felton, A. and MacIntosh, C. Is multidisciplinary learning effective among those caring for people with diabetes?. Diabetic Medicine 2002;10:799-803.
93. Scottish Executive Health Department. Report of the Joint Future Group. ; November 2000.
94. Douglas JDM, Laird C. Clinical fire drills and skill decay: can we develop an evidence base for policy and a language for training?. Medical Education 2004;38:14-6.
95. Cudney SA. Making gerontic continuing education accessible for rural nurses. Journal of Gerontological Nursing July 1991;17(7):29-34.
96. Cox, J. and Mungall, I. Rural Healthcare. Abingdon: Radcliffe Medical Press; 1999.
97. Campbell JL, Ramsay, J. and Green, J. Practice size: impact on consultation length, workload, and patient assessment of care. British Journal of General Practice 2001;51(469):644-50.
98. Worley P, Silagy C, Prideaux D, Newble DaJ,A. The Parallel Rural Community Curriculum: an integrated clinical curriculum based in rural general practice. Medical Education 2000;34:558-65.

83
99. Hopkins P, Douglas, I. and Swan, G. Healthy, Wealthy and Wise?: A Feasibility Study. Inverness: Highland Health Board; January 2003.
100. Barnett S, Martin, D. and Diamond, I. A multilevel analysis of the effects of rurality and social deprivation on premature limiting long term illness. Epidemiol Community Health January 2001;55(1):44-51.
101. Martin D, Wrigley S, Barrett, S. and Roderick, P. Increasing the sophistication of access measurement in a rural healthcare study. Health & Place 8: 3-13; 2002
102. Quantifying Access to Health Facilities. Available at: http://www.ruralhealth.org.au/fifthconf/bamfordpaper.htm. Accessed 11/5, 2001.
103. Douglas I. Estimating tourist numbers in Highland May 2003;.
104. Professional behaviour and access to care. Available at: www.rdd-phru.cam.ac.uk/access/access.htm. , 2001.
105. A Smart, Successful Scotland - the Highlands and Islands dimension. Available at: http://www.show.scot.nhs.uk/sehd/nlp/MainFrame.htm.
106. O'Meara P, Strasser R, Marrow, P. and Le Leivre, P. An integrated approach to the role of the ambulance medical officer in rural Australia. Pre-Hospital Immediate Care 2001;5:24-6.
107. National Leadership Development Programme: Xceed. Available at: http://www.show.scot.nhs.uk/sehd/nlp/MainFrame.htm.
108. Skills for Health: Map of Competences for Remote and Rural Healthcare, RARARI, Bristol, June 2004
84
ABBREVIATIONS A & B Argyll and Bute A & C Administration and Clerical AHP Allied Health Professional BASICS British Association of Immediate Care courses CHP Community Health Partnerships COA Census Output Area CPN Community Psychiatric Nurse DN District Nurse FE Further Education GMS General Medical Services GP General Practitioner HE Higher Education HEMS Helicopter Emergency Medical Service HHB Highland Health Board HIE Highlands and Islands Enterprise HIHRI Highlands and Islands Health Research Institute HITrans Highlands and Islands Transport forum HPCT Highland Primary Care Trust HV Health Visitor IT Information Technology LEC Local Enterprise Community LHCC Local Health care Co-operative NES NHS Education Scotland NHS National Health Service OECD Organisation for Economic Co-operation and Development PAF Performance Assessment Framework PC Primary Care PCT Primary care Trust PDP Personal Development Plan PDPR Personal Development Plan and Review PIN Partnership Information Network RARARI Remote and Rural Areas Resource Initiative SAS Scottish Ambulance Service SCRSJ Scottish Centre for Research on Social Justice SEHD Scottish Executive Health Department SHoS Scottish Household Survey SIMD Scottish Index of Multiple Deprivation SNAP Scottish Needs Assessment Prograramme WHO World Health Organisation WR,SS & L Wester Ross, South Skye and Lochalsh
85
CONTRIBUTORS
ORGANISATION ORGANISATION Neil Greg AA Head of motoring policy Eric Jespersen Argyll and Bute PCT
Paul Anfield, Argyll & Isles Enterprise Pat Tyrrell Argyll and Bute PCT
Verona Stockman BASICS Karen Fryer NHS Argyll and Clyde
Dr Colville Laird BASICS/GP Fiona Corcoran NHS Argyll and Clyde
John McFadyen BEAR Scotland Cathy Fox NHS Argyll and Clyde
Rev Ian Sutherland Church of Scotland Catherine Sinclair NHS Highland
Dr Jim Douglas GP/RARARI Leslie Ann Smith NHS Highland
Claire Macdonald Highlands and Island Enterprise Ian Douglas NHS Highland
Andy Sargeant Highlands and Island Enterprise Paddy Hopkins NHS Highland
Shona Cline Highlands and Island Enterprise Alasdair MacLennan NHS Highland
Stephen Boyle Highlands and Island Enterprise John Palmer NHS Highland
Howard Brindley HITRANS Ken Proctor NHS Highland
Dr Ian Smith Kinlochbervie Academy Sasha Railton NHS Highland
Chris Meacher Lochaber LHCC Fiona Duff NHS Highland
Laura Fisher Northern Constabulary Jane McKay NHS Highland
Matt Sutton Platform Project Maureen Thomson NHS Highland
Mike Allan Scottish Ambulance Service Jim McKay NHS Highland
Ian Donald Scottish Ambulance Service Lynn Marsland NHS Highland
David Currie Scottish Ambulance Service Brian Houston NHS Highland
Christine MacLeod The Highland Council Sarah McLeod NHS Highland
John MacFadyen The Highland Council Gill Keel NHS Highland
Hugh Logan The Highland Council
Christine Macfarlane-Slack
NHS Highland
Alison Dix Sabhal Mor Ostaig, Gaelic Medium College, Skye
James McNally ISD Scotland
Jenny Spratt Scottish Centre for Research on Social Justice
Lindsay Mitchell Skills for Health Dr M.Elder GP
Gill Keel W Ross, S Skye, Lochalsh LHCC Dr Jeremy Philips GP
Alison Hudson W Ross, S Skye, Lochalsh LHCC Dr Hanna GP
Morag Greenshield W Ross, S Skye, Lochalsh LHCC Dr Boyd GP

86

87
APPENDIX

88

89
APPENDIX 1 – SEARCH STRATEGY Databases: BNI, CINAHL, EMBASE, HMIC, Pre-medline, Medline, Index to theses – May 2003
serv
ice
prof
ile
desc
riptio
n
eval
uatio
n
Prim
ary
care
train
ing
educ
atio
n
need
s as
sess
men
t
need
s an
alys
is
heal
thca
re w
orke
rs
trai
ning
nee
ds a
naly
sis
capa
city
bui
ldin
g
staf
f
Loc
al H
ealth
car
e co
oper
ativ
es
educ
atio
n
GP
trai
ning
Prac
tice
nurs
e tr
aini
ng
rura
l
service * * * *
Profile * *
service profile *
Description *
service description *
Evaluation *
service evaluation *
Primary care * * *
Training * *
Education * *
Primary care training * *
Primary care education * *
needs assessment *
needs analysis *
healthcare workers * * * training needs analysis * * capacity building * * * * Staff * * Local Health care cooperatives * * Education * * staff education * GP training * Practice nurse training * Rural *
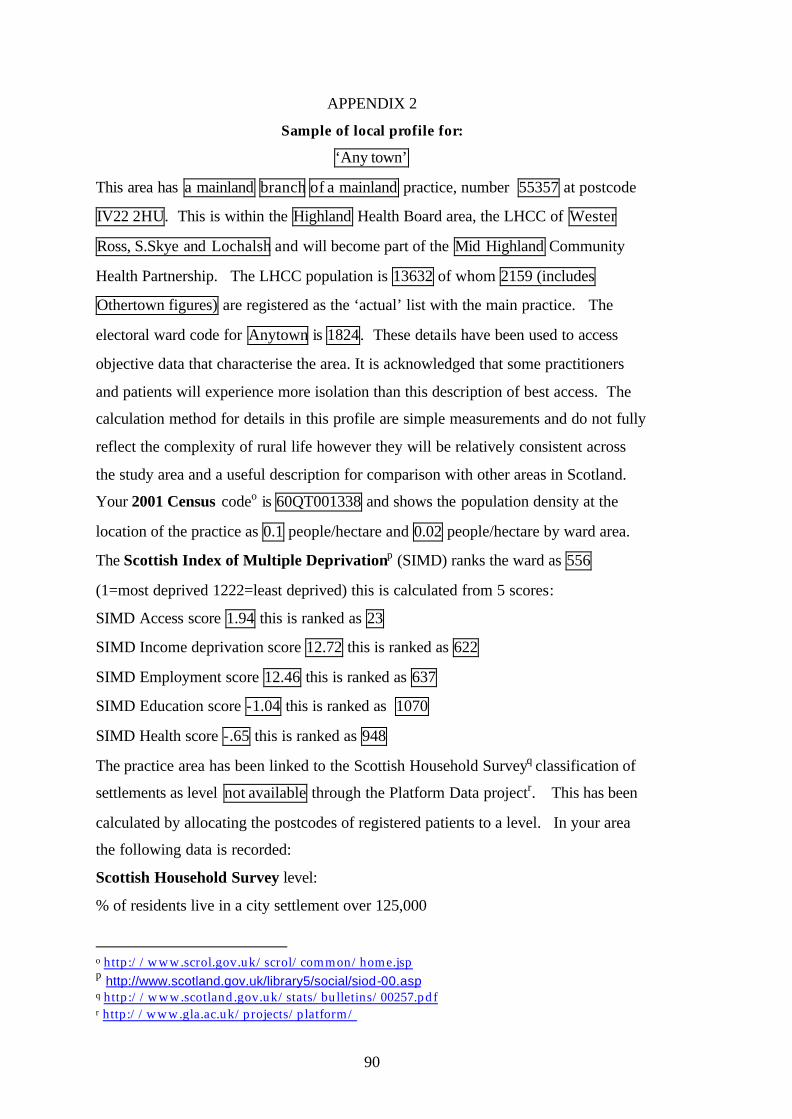
90
APPENDIX 2
Sample of local profile for:
‘Any town’
This area has a mainland branch of a mainland practice, number 55357 at postcode
IV22 2HU. This is within the Highland Health Board area, the LHCC of Wester
Ross, S.Skye and Lochalsh and will become part of the Mid Highland Community
Health Partnership. The LHCC population is 13632 of whom 2159 (includes
Othertown figures) are registered as the ‘actual’ list with the main practice. The
electoral ward code for Anytown is 1824. These details have been used to access
objective data that characterise the area. It is acknowledged that some practitioners
and patients will experience more isolation than this description of best access. The
calculation method for details in this profile are simple measurements and do not fully
reflect the complexity of rural life however they will be relatively consistent across
the study area and a useful description for comparison with other areas in Scotland.
Your 2001 Census codeo is 60QT001338 and shows the population density at the
location of the practice as 0.1 people/hectare and 0.02 people/hectare by ward area.
The Scottish Index of Multiple Deprivationp (SIMD) ranks the ward as 556
(1=most deprived 1222=least deprived) this is calculated from 5 scores:
SIMD Access score 1.94 this is ranked as 23
SIMD Income deprivation score 12.72 this is ranked as 622
SIMD Employment score 12.46 this is ranked as 637
SIMD Education score -1.04 this is ranked as 1070
SIMD Health score -.65 this is ranked as 948
The practice area has been linked to the Scottish Household Surveyq classification of
settlements as level not available through the Platform Data projectr. This has been
calculated by allocating the postcodes of registered patients to a level. In your area
the following data is recorded:
Scottish Household Survey level:
% of residents live in a city settlement over 125,000
o http://www.scrol.gov.uk/scrol/common/home.jsp p http://www.scotland.gov.uk/library5/social/siod-00.asp q http://www.scotland.gov.uk/stats/bulletins/00257.pdf r http://www.gla.ac.uk/projects/platform/
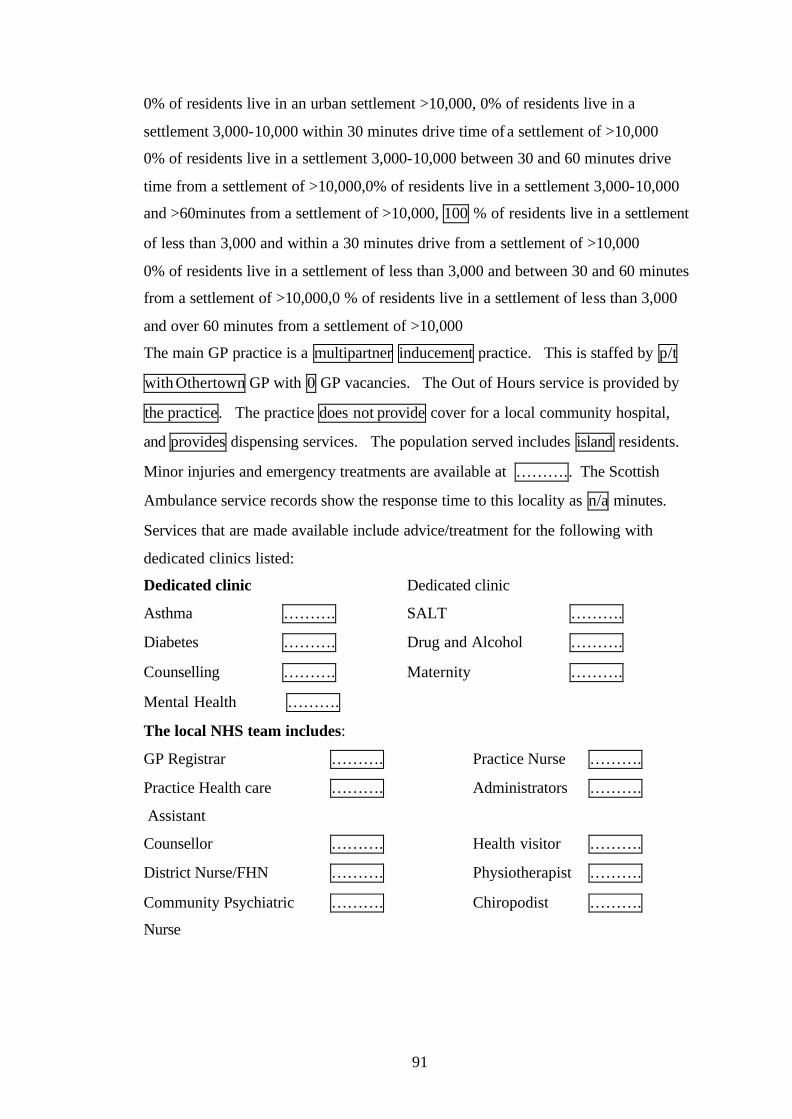
91
0% of residents live in an urban settlement >10,000, 0% of residents live in a
settlement 3,000-10,000 within 30 minutes drive time of a settlement of >10,000
0% of residents live in a settlement 3,000-10,000 between 30 and 60 minutes drive
time from a settlement of >10,000,0% of residents live in a settlement 3,000-10,000
and >60minutes from a settlement of >10,000, 100 % of residents live in a settlement
of less than 3,000 and within a 30 minutes drive from a settlement of >10,000
0% of residents live in a settlement of less than 3,000 and between 30 and 60 minutes
from a settlement of >10,000,0 % of residents live in a settlement of less than 3,000
and over 60 minutes from a settlement of >10,000
The main GP practice is a multipartner inducement practice. This is staffed by p/t
with Othertown GP with 0 GP vacancies. The Out of Hours service is provided by
the practice. The practice does not provide cover for a local community hospital,
and provides dispensing services. The population served includes island residents.
Minor injuries and emergency treatments are available at ……….. The Scottish
Ambulance service records show the response time to this locality as n/a minutes.
Services that are made available include advice/treatment for the following with
dedicated clinics listed:
Dedicated clinic Dedicated clinic
Asthma ………. SALT ……….
Diabetes ………. Drug and Alcohol ……….
Counselling ………. Maternity ……….
Mental Health ……….
The local NHS team includes:
GP Registrar ………. Practice Nurse ……….
Practice Health care
Assistant
………. Administrators ……….
Counsellor ………. Health visitor ……….
District Nurse/FHN ………. Physiotherapist ……….
Community Psychiatric
Nurse
………. Chiropodist ……….

92
The practice is listed as:
RCGP accredited ……….
RCGP Quality Practice Award ……….
An undergraduate teaching practice ……….
A postgraduate training practice ……….
Additional GP roles include:
Occupational Health Officer ………. Police surgeon ………. Airport duties ……….
Rescue team ………. Sports injury team ……….
The most accessible General Hospital accepting acute admissions is Raigmore.
Access to acute in-patient care for registered patients is characterised by:
76.4 road miles between the GP surgery and the General hospital, 109 minutes road
time between the GP surgery and the General hospital, 0 miles of single track road
complicate the journey. Ferry travel is not necessary and requires 0 ferry journey
lasting 0 minutes. The total one-way travel time with good connections and in perfect
conditions is 109 minutes. The Health Board headquarters is based in Inverness.
Access to the Health Board is characterised by: 76.4 road miles between the GP
surgery and the Health Board, 109 minutes road time between the GP surgery and the
Health Board, 0 miles of single track road complicate the journey. Ferry travel is not
necessary. The crossing takes 0 minutes and requires 0 ferry. The total one-way
travel time with good connections and in perfect conditions is 109 minutes.
Rural practitioners describe seasonal population shifts. In your Local Enterprise
Council area the Scottish Tourist board and Highlands and Island Enterprise board
have recorded n/a resident bed nights: n/a tourist bed night per annum. Incidence
shows fluctuation coinciding with the winter snow sports/climbing season and
summer touring/water sports/hill sports visitors. The average age of summer visitors
is n/a years and winter visitors n/a years.

93
APPENDIX 3 Analysis table for PDPRs Analysis table for PDPs
IT
Tech
nica
l
Clin
ical
- p
ract
ical
Clin
ical
- k
now
ledg
e
Man
agem
ent
Acc
redi
ted
FE
Acc
redi
ted
HE
Pro
fess
iona
l m
aint
enan
ce
Exp
erie
ntia
l
Tau
ght
Per
sona
l stu
dy
Tim
e
Equ
ipm
ent
Fin
ance
Locu
m/b
ackf
ill
Dom
estic
Loca
l del
iver
y
LHCC Lochaber ? ? ? ? ? ? ? ? ? ? ? ? ? ? ? ? ? WRSL ? ? ? ? ? ? ? ? ? ? ? ? ? ? ? ? ? Argyll and Bute ? ? ? ? ? ? ? ? ? ? ? ? ? ? ? ? ?Disciplines AHP ? ? ? ? ? ? ? ? ? ? ? ? ? ? ? ? ? Nurses ? ? ? ? ? ? ? ? ? ? ? ? ? ? ? ? ? Midwives ? ? ? ? ? ? ? ? ? ? ? ? ? ? ? ? ?
Admin and Clerical ? ? ? ? ? ? ? ? ? ? ? ? ? ? ? ? ?
GP ? ? ? ? ? ? ? ? ? ? ? ? ? ? ? ? ?Skills needed IT ? ? ? ? ? ? ? ? ? ? ? ? Technical ? ? ? ? ? ? ? ? ? ? ? ?
Clinical - practical ? ? ? ? ? ? ? ? ? ? ? ?
Clinical - knowledge ? ? ? ? ? ? ? ? ? ? ? ?
Management ? ? ? ? ? ? ? ? ? ? ? ?Skill level Accredited FE ? ? ? ? ? ? ? ? ? Accredited HE ? ? ? ? ? ? ? ? ?
Professional maintenance ? ? ? ? ? ? ? ? ?
How delivered Experiential ? ? ? ? ? ? Taught ? ? ? ? ? ? Personal study ? ? ? ? ? ?Resource need Time Equipment Finance Locum/backfill Domestic Local delivery
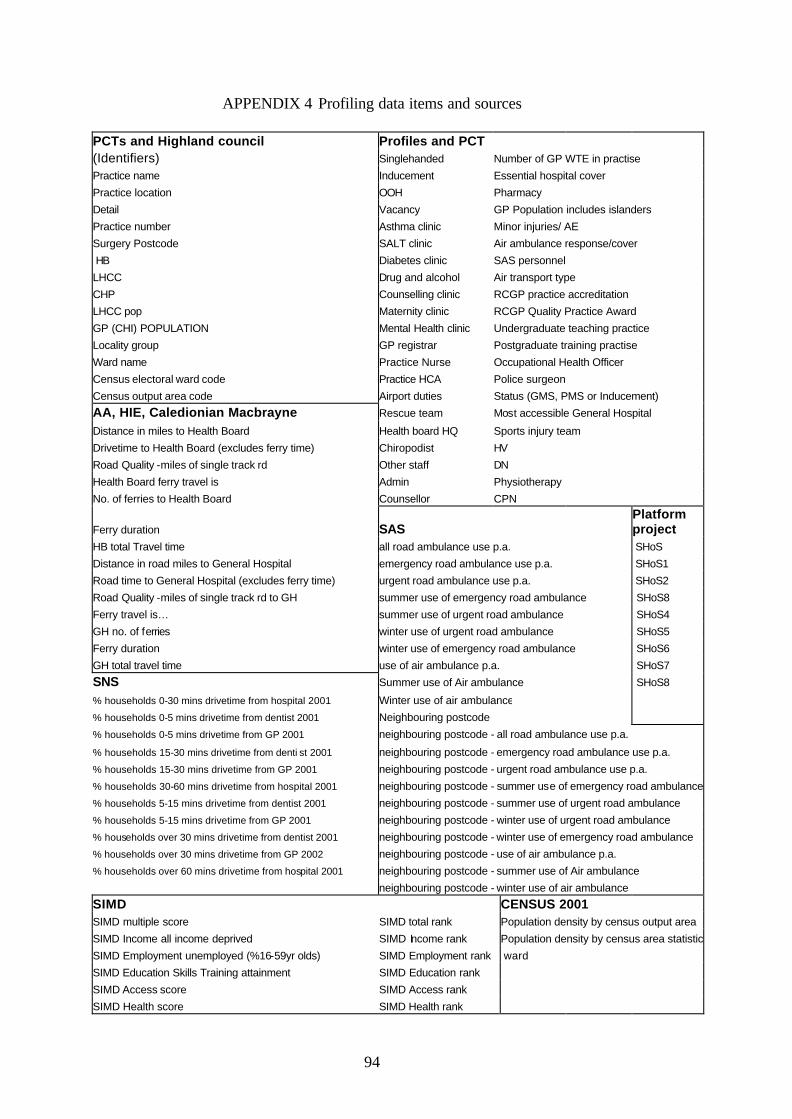
94
APPENDIX 4 Profiling data items and sources PCTs and Highland council Profiles and PCT (Identifiers) Singlehanded Number of GP WTE in practise
Practice name Inducement Essential hospital cover Practice location OOH Pharmacy Detail Vacancy GP Population includes islanders
Practice number Asthma clinic Minor injuries/ AE Surgery Postcode SALT clinic Air ambulance response/cover
HB Diabetes clinic SAS personnel LHCC Drug and alcohol Air transport type CHP Counselling clinic RCGP practice accreditation
LHCC pop Maternity clinic RCGP Quality Practice Award
GP (CHI) POPULATION Mental Health clinic Undergraduate teaching practice Locality group GP registrar Postgraduate training practise Ward name Practice Nurse Occupational Health Officer Census electoral ward code Practice HCA Police surgeon Census output area code Airport duties Status (GMS, PMS or Inducement)
AA, HIE, Caledionian Macbrayne Rescue team Most accessible General Hospital
Distance in miles to Health Board Health board HQ Sports injury team Drivetime to Health Board (excludes ferry time) Chiropodist HV Road Quality -miles of single track rd Other staff DN Health Board ferry travel is Admin Physiotherapy No. of ferries to Health Board Counsellor CPN
Ferry duration SAS Platform project
HB total Travel time all road ambulance use p.a. SHoS
Distance in road miles to General Hospital emergency road ambulance use p.a. SHoS1
Road time to General Hospital (excludes ferry time) urgent road ambulance use p.a. SHoS2
Road Quality -miles of single track rd to GH summer use of emergency road ambulance SHoS8 Ferry travel is… summer use of urgent road ambulance SHoS4 GH no. of ferries winter use of urgent road ambulance SHoS5 Ferry duration winter use of emergency road ambulance SHoS6 GH total travel time use of air ambulance p.a. SHoS7 SNS Summer use of Air ambulance SHoS8 % households 0-30 mins drivetime from hospital 2001 Winter use of air ambulance % households 0-5 mins drivetime from dentist 2001 Neighbouring postcode % households 0-5 mins drivetime from GP 2001 neighbouring postcode - all road ambulance use p.a.
% households 15-30 mins drivetime from denti st 2001 neighbouring postcode - emergency road ambulance use p.a.
% households 15-30 mins drivetime from GP 2001 neighbouring postcode - urgent road ambulance use p.a.
% households 30-60 mins drivetime from hospital 2001 neighbouring postcode - summer use of emergency road ambulance
% households 5-15 mins drivetime from dentist 2001 neighbouring postcode - summer use of urgent road ambulance
% households 5-15 mins drivetime from GP 2001 neighbouring postcode - winter use of urgent road ambulance
% households over 30 mins drivetime from dentist 2001 neighbouring postcode - winter use of emergency road ambulance
% households over 30 mins drivetime from GP 2002 neighbouring postcode - use of air ambulance p.a.
% households over 60 mins drivetime from hospital 2001 neighbouring postcode - summer use of Air ambulance
neighbouring postcode - winter use of air ambulance
SIMD CENSUS 2001 SIMD multiple score SIMD total rank Population density by census output area
SIMD Income all income deprived SIMD Income rank Population density by census area statistic
SIMD Employment unemployed (%16-59yr olds) SIMD Employment rank ward SIMD Education Skills Training attainment SIMD Education rank SIMD Access score SIMD Access rank SIMD Health score SIMD Health rank

95
APPENDIX 5 Ambulance activity ( Source: Scottish Ambulance Service October 2002 – October 2003)
per a
nnum
per a
nnum
per a
nnum
Sum
mer
Sum
mer
Win
ter
Win
ter
per a
nnum
Sum
mer
Win
ter
All
road
am
bula
nce
calls
All
emer
genc
y am
bula
nce
calls
All
urge
nt
ambu
lanc
e ca
lls
Em
erge
ncy
calls
Urg
ent c
alls
Eem
erge
ncy
calls
Urg
ent c
alls
air
air
air
IV 21 89 28 61 22 44 6 17 5 4 1
IV 22 100 43 57 34 33 9 24 7 6 1
IV 23 50 29 21 20 12 9 9 0 0 0
IV 26 186 77 109 57 58 20 51 9 6 3
IV 40 216 83 133 59 67 24 66 4 4 0
IV 41 62 37 25 24 8 13 17 0 0 0
IV 42 21 15 6 8 3 7 3 0 0 0
IV 43 15 7 8 5 5 2 3 0 0 0IV 44 18 9 9 6 8 3 1 0 0 0
IV 45 24 7 17 7 14 0 3 0 0 0
IV 46 2 1 1 1 1 0 0 0 0 0
IV 47 18 14 4 14 1 0 3 0 0 0
IV 48 12 3 9 2 5 1 4 0 0 0
IV 49 261 43 218 23 124 20 94 117 69 48
IV 51 608 149 459 93 232 56 227 28 20 8
IV 52 27 14 13 10 7 4 6 0 0 0
IV 53 3 1 2 1 2 0 0 0 0 0
IV 54 114 43 71 32 30 11 41 4 3 1
IV 55 136 38 98 19 53 19 45 0 0 0
IV 56 16 4 12 4 11 0 1 0 0 0
IV 63 108 79 29 56 11 23 18 2 2 0
PH 30 1 1 0 0 0 1 0 0 0 0
PH 31 32 26 6 12 4 14 2 0 0 0
PH 32 63 30 33 19 18 11 15 7 4 3
PH 33 1667 779 888 466 448 313 440 31 14 17
PH 34 65 50 15 35 8 15 7 0 0 0
PH 35 19 13 6 12 2 1 4 5 5 0
PH 36 73 25 48 14 27 11 21 5 5 0
PH 37 18 16 2 15 0 1 2 0 0 0
PH 38 18 17 1 11 1 6 0 0 0 0
PH 39 50 24 26 18 14 6 12 2 0 2
PH 40 12 8 4 4 4 4 0 0 0 0
PH 41 110 56 54 36 34 20 20 5 3 2
PH 42 0 0 0 0 0 0 0 13 10 3
PH 43 0 0 0 0 0 0 0 0 0 0
PH 44 0 0 0 0 0 0 0 1 1 0
PH 49 157 85 72 54 38 31 34 0 0 0
PH 50 126 64 62 38 35 26 27 1 1 0
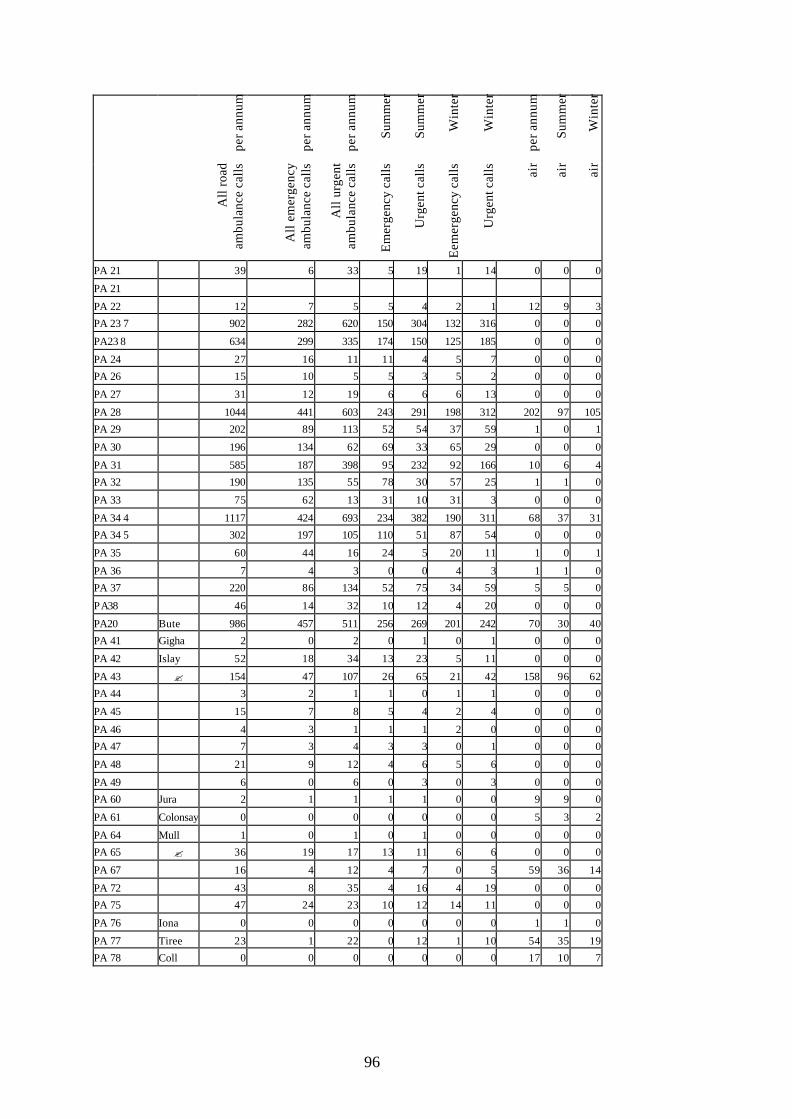
96
per a
nnum
per a
nnum
per a
nnum
Sum
mer
Sum
mer
Win
ter
Win
ter
per a
nnum
Sum
mer
Win
ter
All
road
am
bula
nce
calls
All
emer
genc
y am
bula
nce
calls
All
urge
nt
ambu
lanc
e ca
lls
Em
erge
ncy
calls
Urg
ent c
alls
Eem
erge
ncy
calls
Urg
ent c
alls
air
air
air
PA 21 39 6 33 5 19 1 14 0 0 0
PA 21
PA 22 12 7 5 5 4 2 1 12 9 3
PA 23 7 902 282 620 150 304 132 316 0 0 0
PA23 8 634 299 335 174 150 125 185 0 0 0
PA 24 27 16 11 11 4 5 7 0 0 0
PA 26 15 10 5 5 3 5 2 0 0 0
PA 27 31 12 19 6 6 6 13 0 0 0
PA 28 1044 441 603 243 291 198 312 202 97 105
PA 29 202 89 113 52 54 37 59 1 0 1
PA 30 196 134 62 69 33 65 29 0 0 0
PA 31 585 187 398 95 232 92 166 10 6 4
PA 32 190 135 55 78 30 57 25 1 1 0
PA 33 75 62 13 31 10 31 3 0 0 0
PA 34 4 1117 424 693 234 382 190 311 68 37 31
PA 34 5 302 197 105 110 51 87 54 0 0 0
PA 35 60 44 16 24 5 20 11 1 0 1
PA 36 7 4 3 0 0 4 3 1 1 0
PA 37 220 86 134 52 75 34 59 5 5 0
PA38 46 14 32 10 12 4 20 0 0 0
PA20 Bute 986 457 511 256 269 201 242 70 30 40
PA 41 Gigha 2 0 2 0 1 0 1 0 0 0
PA 42 Islay 52 18 34 13 23 5 11 0 0 0
PA 43 ? 154 47 107 26 65 21 42 158 96 62
PA 44 3 2 1 1 0 1 1 0 0 0
PA 45 15 7 8 5 4 2 4 0 0 0
PA 46 4 3 1 1 1 2 0 0 0 0
PA 47 7 3 4 3 3 0 1 0 0 0
PA 48 21 9 12 4 6 5 6 0 0 0
PA 49 6 0 6 0 3 0 3 0 0 0
PA 60 Jura 2 1 1 1 1 0 0 9 9 0
PA 61 Colonsay 0 0 0 0 0 0 0 5 3 2
PA 64 Mull 1 0 1 0 1 0 0 0 0 0
PA 65 ? 36 19 17 13 11 6 6 0 0 0
PA 67 16 4 12 4 7 0 5 59 36 14
PA 72 43 8 35 4 16 4 19 0 0 0
PA 75 47 24 23 10 12 14 11 0 0 0
PA 76 Iona 0 0 0 0 0 0 0 1 1 0
PA 77 Tiree 23 1 22 0 12 1 10 54 35 19
PA 78 Coll 0 0 0 0 0 0 0 17 10 7

97
The incidence of mainland emergency road ambulance use in Argyll and Bute LHCC 2002-2003
0
50
100
150
200
250
300
Summer Winter
The incidence of island emergency road ambulance use in Argyll and Bute LHCC 2002-2003
0
50
100
150
200
250
300
Islay Mull Bute Jura Tiree
Summer Winter

98
The incidence of emergency road ambulance use in Lochaber LHCC 2002-2003
0
50
100
150
200
250
300
350
400
450
500P
H 3
0
PH
31
PH
32
PH
33
PH
34
PH
35
PH
36
PH
37
PH
38
PH
39
PH
40
PH
41
PH
42
PH
43
PH
44
PH
49
PH
50
Summer Winter
The incidence of emergency road ambulance use in Wester Ross, S. Skye and Lochalsh LHCC 2002-2003
0
10
20
30
40
50
60
70
80
90
100
IV 2
1
IV 2
2
IV 2
3
IV 2
6
IV 4
0
IV 4
1
IV 4
2
IV 4
3
IV 4
4
IV 4
5
IV 4
6
IV 4
7
IV 4
8
IV 4
9
IV 5
1
IV 5
2
IV 5
3
IV 5
4
IV 5
5
IV 5
6
IV 6
3
Summer Winter

99
Incidence of mainland urgent road ambulance use in Argyll and Bute LHCC 2002-2003
0
50
100
150
200
250
300
350
400
450
PA
21
PA
22
PA
23
7
PA
23 8
PA
24
PA
26
PA
27
PA
28
PA
29
PA
30
PA
31
PA
32
PA
33
PA
34
4
PA
34
5
PA
35
PA
36
PA
37
PA
38
Summer Winter
Incidence of island urgent road ambulance use in Argyll and Bute LHCC 2002-2003
0
50
100
150
200
250
300
Islay Mull Bute Jura Tiree
Summer Winter
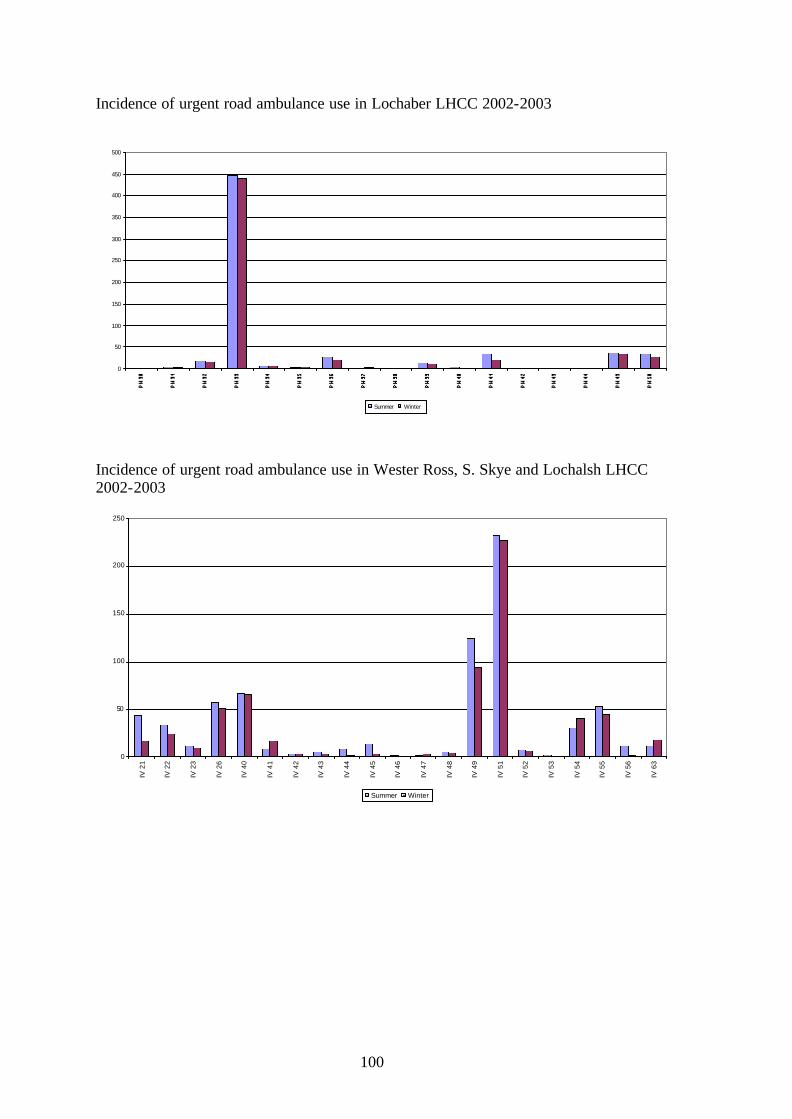
100
Incidence of urgent road ambulance use in Lochaber LHCC 2002-2003
0
50
100
150
200
250
300
350
400
450
500
Summer Winter
Incidence of urgent road ambulance use in Wester Ross, S. Skye and Lochalsh LHCC 2002-2003
0
50
100
150
200
250
IV 2
1
IV 2
2
IV 2
3
IV 2
6
IV 4
0
IV 4
1
IV 4
2
IV 4
3
IV 4
4
IV 4
5
IV 4
6
IV 4
7
IV 4
8
IV 4
9
IV 5
1
IV 5
2
IV 5
3
IV 5
4
IV 5
5
IV 5
6
IV 6
3
Summer Winter

101
APPENDIX 6A
FUNNELLING EXERCISE FOR PDPR CODING AND ANALYSIS
Knowledge Practical Management Alternative therapies Acupuncture Administration Assertiveness Administrat ion of medicines Anger management Autism Advanced driving Appraisal Breast Feeding ALSO Audit care pathways Anaphylaxis CHI system Changing patient behaviour Antenatal/parentcraft Clinical leadership Chest diseases Asthma Coaching Child protection BASICS Communication Child psychology Bereavement counselling Delegation Childrens act BP monitoring Documentation and record keeping common conditions Cannulation IV Group facilitation Copd Cardiac rehab facilitator Leadership Dementia Child development Local knowledge Diabetes Complementary therapy Management Dysphagia consultation technique Medical record updating and filing protocol Eneuresis Continence Mentoring Falls prevention Counselling PAS Fire Defibrillation Planning Food Hygiene dispensing Practice accreditation General Medicine District/Comm. Nursing Presentation Genetics Ear Syringing Recruitment Gerontology Emergency Life support/ CPR Retirement Health Promotion Emergency situations revalidation skills Incapacity Act Examination of the newborn Single shared assessment Infertility Family planning Stress management integrated care First Aid Supervisors Marie Curie course First Responder SVQ Assessor medico legal Hands intrapartum Team leadership Mens health health care Team nursing Mental Health Health visiting Time management Mental Health Act Heart disease PEAK chiropody system Multiple sclerosis Hypnosis Technical Neuro conditions Immediate Life support Hearing tests Nutrition Immunisation Sign Language Obesity Injection Technology (new) Orthopaedic medicine Leg ulcer management Vision Parenting Male catheterisation IT Parkinsons Massage IT Post natal depression McKenzie skills IT ‘Access’ Public Health Midwifery IT ‘Excel’ Pulmonary rehabilitation Minor Illness IT ‘Powerpoint’ Rehabilitation Moving and handling IT ‘Word’ Research techniques Nurse practitioner Word Sexual health Nursing not specified
Smoking cessation Pain management social science Palliative care Stroke Study skills Physiotherapy Syringe drivers Terminal Care Pilates exercise Teaching Tissue viability Prescribing teleradiology unfamiliar conditions Public speaking Triage (ortho) Webster Stratton prog. Respiratory skills Venepuncture Social activities in rehab Violence and aggression Sports injuries Wound care

102
APPENDIX 6A continued
Further Education Experiential learning Equipment
Accredited Case study Equipment - OHP
certificate Experience/practise Equipment – CD player
Diploma In service Equipment – Computer
ECDL Job rotation Equipment – Desk
Foundation Liaison with Acute trust Equipment – Flip chart
NVQ NVQ Modern apprenticeship Equipment – Laptop
SVQ Observation Own Office
Higher Education Peer group meetings Finance
Degree Practice placements Fees for study -materials
MSc Secondment Fees for tuition
Professional Shadowing Finance
Advanced Supervision Financed travel
Basic SVQ Self funding
Maintenance Personal study Time
Update Professional Book access Opportunity
Upgrade Professional CD ROM Own time
Distance learning Practise
Taught Home study Study time
By GP Internet access Travel time
Coaching Journal access Domestic
Conference Open learning Childcare / Family friendly
Course Peer support Locum
Internal course Phone a friend
Residential study Reading Not specified
Seminars Reflection
Study days Research place
Technology training Studying delivered in Scotland
Workshop/training day Technology based training Delivered Locally

103
APPENDIX 6B
GROUPING FOR PDPR CODING AND ANALYSIS Administration and Clerical Clinic Secretary
Medical records clerk
Receptionist
Secretary
Allied Health professional Chiropodist
Physiotherapisst
Radiographer
Speech Therapist
GP GP
Midwives District Nurse / Midwife
Family Health Nurse/ Midwife
Health Visitor/School Nurse/Midwife
Midwife
Midwifery assistant
Triple duty (HV/M/DN)
Not stated Not stated
Nurses Auxiliary /Health Care Assistant (Community)
Community Nurse (bank)
Community Nurse Learning Disability
Community Staff Nurse
Community Nurse
District Nursing Sister
Family Health Nurse
Health Visitor
Health Visitor/School Nurse
School Nurse