Clinical Commissioning Group Governing Body Paper … · Clinical Commissioning Group Governing...
32
Clinical Commissioning Group Governing Body Paper Summary Sheet Date of Meeting: 25 November 2014 For: PUBLIC session PRIVATE Session For: Decision Discussion Noting Agenda Item and title: GOV/14/11/10 Information Management and Technology (IM&T) Strategy for Wiltshire Clinical Commissioning Group Author: Bruce Don IM&T Consultant working for the Central Southern Commissioning Support Unit (CSCSU) Lead Director/GP from CCG: Simon Truelove Chief Financial Officer Peter Jenkins Medical Advisor and Interim Chief Clinical Information Officer Executive summary: The information management and technology strategy for Wiltshire CCG describes the drivers and outcomes that the CCG wants to commission from its current providers. The strategy that takes the desired outcomes from the CCG 5 year plan and other national strategies describes what the CCG will promote in the use of IT and information management which will benefit the patient, the organisations that provide services to our population, how the CCG commissions and how the CSCSU will support the CCG in the strategy delivery. Evidence in support of arguments: NHS England Digital Strategy, Wiltshire CCG 5 year plan Who has been involved/contributed: The clinical executive, the chief clinical information officer, CFO, representatives from providers, clinical leaders within Wiltshire Cross Reference to Strategic Objectives: Support the delivery of the Wiltshire 5 year plan and the objectives embedded within the plan Engagement and Involvement: Primary care, secondary care, Wiltshire Council and results of the engagement from the CCG 5 year plan Communications Issues: None 1
Transcript of Clinical Commissioning Group Governing Body Paper … · Clinical Commissioning Group Governing...

Clinical Commissioning Group Governing Body Paper Summary Sheet
Date of Meeting: 25 November 2014 For: PUBLIC session PRIVATE Session
For: Decision Discussion Noting
Agenda Item and title: GOV/14/11/10 Information Management and Technology (IM&T) Strategy for Wiltshire Clinical Commissioning Group
Author: Bruce Don IM&T Consultant working for the Central Southern Commissioning Support Unit (CSCSU)
Lead Director/GP from CCG:
Simon Truelove Chief Financial Officer Peter Jenkins Medical Advisor and Interim Chief Clinical Information Officer
Executive summary:
The information management and technology strategy for Wiltshire CCG describes the drivers and outcomes that the CCG wants to commission from its current providers. The strategy that takes the desired outcomes from the CCG 5 year plan and other national strategies describes what the CCG will promote in the use of IT and information management which will benefit the patient, the organisations that provide services to our population, how the CCG commissions and how the CSCSU will support the CCG in the strategy delivery.
Evidence in support of arguments:
NHS England Digital Strategy, Wiltshire CCG 5 year plan
Who has been involved/contributed:
The clinical executive, the chief clinical information officer, CFO, representatives from providers, clinical leaders within Wiltshire
Cross Reference to Strategic Objectives:
Support the delivery of the Wiltshire 5 year plan and the objectives embedded within the plan
Engagement and Involvement:
Primary care, secondary care, Wiltshire Council and results of the engagement from the CCG 5 year plan
Communications Issues:
None
1

Financial Implications:
The strategy will utilise existing resources including the Primary Care IT allocation that has been recently devolved to the CCG. Any investment in IM&T solutions will need to achieve a return on investment in order to support future business cases
Review arrangements:
Review to be undertaken annually
Risk Management: Information governance will be a key risk to manage as the objective of the single view of the client is delivered
National Policy/ Legislation:
Follows the national digital strategy from NHS England
Equality & Diversity: An equality and diversity assessment will be undertaken for each programme / project that supports the delivery of the CCG IM&T strategy
Other External Assessment:
N/A
What specific action re. the paper do you wish the Governing Body to take at the meeting?
Agree the overall IM&T strategy for the CCG, the proposed IM&T programme and the governance arrangements.
2

Information Management & Technology Strategy for Wiltshire CCG
v1.1 November 2014
Contents
A IM&T PLAN ON A PAGE ..................................................................................................................................................... 4
B INTRODUCTION AND BACKGROUND ................................................................................................................................. 5
C DRIVERS FOR CHANGE ....................................................................................................................................................... 5
C1 LOCAL HEATH ECONOMY ............................................................................................................................................................ 5 C2 WILTSHIRE CCG’S GOALS ........................................................................................................................................................... 6 C3 NATIONAL CONTEXT ................................................................................................................................................................... 7
D STRATEGIC FRAMEWORK .................................................................................................................................................. 8
D1 IM&T VISION ........................................................................................................................................................................... 8 D2 FRAMEWORK ............................................................................................................................................................................ 9
E CURRENT SITUATION AND THE GAPS TO BE BRIDGED ..................................................................................................... 11
E1 CURRENT SITUATION ................................................................................................................................................................ 11 E2 SIMILARITIES AND DIFFERENCES AMONGST GROUPS ........................................................................................................................ 13 E3 THE GAP BETWEEN VISION AND CURRENT POSITION ...................................................................................................................... 14
F MOVING FORWARD ........................................................................................................................................................ 16
F1 STRATEGIC PRINCIPLES .............................................................................................................................................................. 16 F2 OUTLINE PLANS ....................................................................................................................................................................... 16 F3 FURTHER CONSIDERATIONS ....................................................................................................................................................... 22 F4 NEXT STEPS ............................................................................................................................................................................ 24
APPENDIX A. GLOSSARY ........................................................................................................................................................... 25
APPENDIX B. PATIENT / CLIENT SYSTEMS ACROSS WILTSHIRE .................................................................................................. 26
APPENDIX C. NATIONAL IM&T TARGETS AND RELEVANT DEVELOPMENTS ............................................................................... 29
APPENDIX D. SHARED ACCESS TO PATIENT / CLIENT INFORMATION ........................................................................................ 31
3

A IM&T Plan on a Page
4

B Introduction and Background B1.1 Information management and technology (IM&T) is an essential enabler to support the
CCG’s goals, supporting diverse benefits for all stakeholders of relevance to the CCG: ♦ Commissioners – informing and supporting decision-making; ♦ Clinicians - enabling access to the right information at the right time; ♦ Patients and the public – empowering them to understand their own health, adopt
healthier lifestyles and access appropriate local services at the right time.
B1.2 This document sets out the direction of travel for IM&T to support Wiltshire CCG, and represents the current strategy and high-level implementation plans for the next 3 to 5 years. The focus is on support for the CCG / commissioning not on provider IM&T, nor on GP (provider) IT & systems issues – although clearly there is interdependency with some of the issues, hence aspects of GPIT are referred to in this report.1
B1.3 IM&T has a broad definition - covering data, information, intelligence, knowledge, systems, IT / digital technologies, supporting skills and services. This report does not go into any single issue in depth. It aims to convey the breadth of issues to be addressed and to provide pointers to the way forward.
B1.4 This is the first systematic analysis of IM&T as it relates to Wiltshire CCG’s overall strategy and priorities. The findings and preliminary conclusions are based on reviews of local and national documentation, interviews with a individuals from the CCG / primary care, and discussions with the CCG’s Clinical Executive team.
B1.5 Inevitably, this document contains many acronyms. These are expanded upon in the Glossary (Appendix A).
C Drivers for Change C1 Local Heath Economy
C1.1 Wiltshire CCG commissions services on behalf of a population of about 480,000 with an overall budget of approximately £520m, within a highly complex health system: ♦ There are 56 general practices, organised into 3 locality groups (Sarum, NEW,
WWKYD); ♦ Three different acute trusts provide the majority of services for each of the locality
groups (Salisbury Foundation Trust (SFT) for Sarum, Great Western Hospital NHSFT in Swindon (GWH) for NEW, Royal United Hospital in Bath (RUH) for WWKYD);
♦ GWH NHSFT also provide community services across Wiltshire, as well as to Bath and NE Somerset. (These services will be re-tendered next year);
♦ Avon and Wiltshire Partnership Trust (AWP) provides mental health services across Wiltshire and Gloucestershire;
♦ NHS 111 service is provided by Harmoni (who also cover Avon and Gloucestershire); ♦ Ambulance services are provided by South Western Ambulance Service NHS FT
(SWAS); ♦ Medvivo provide GP Out of Hours Services;
1 Other initiatives, outside the scope of this report, are required to take forward the specific proposals regarding delegation of responsibility to CCG’s for GP systems and IT - as set out in “Securing excellence in GP IT Services. Operating Model, 2nd edition”, NHS England, April 2014
5

♦ Wiltshire residents have access to various Urgent Care Centres (UCC) and Walk in Centres (WIC);
♦ The CCG works in close partnership both with Wiltshire Council, e.g. in relation to the Better Care Fund.
C1.2 Most of these organisations have separate IT / patient record systems, from different suppliers (although 90% general practices use the same version of clinical system – TPP’s SystmOne). There are plans to replace some of the systems. Clearly this complex, mixed economy (especially being served by three main acute trusts) presents a number of challenges when considering issues such as integration and sharing of information across services. Appendix B provides further detail on systems in use across Wiltshire, and highlights some of the issues that the CCG needs to consider.
C2 Wiltshire CCG’s Goals
C2.1 IM&T is widely acknowledged to be fundamental to achieving the CCG’s goals, where it is recognised both as a key dependency and as an enabler for change. In effect, IM&T must support two rather different roles of the CCG: ♦ As commissioning organisation – what information, tools and technologies do those
working to support the commissioning process require, and how does the CCG support member practices in offering accessible healthcare?
♦ As agent of change across the whole healthcare system – where can the CCG facilitate service transformation through the deployment of IM&T?
C2.2 Many of the CCG’s strategic aims and plans, as outlined in “NHS Wiltshire CCG Five Year Strategic Plan 2014-2019”, have implications for and dependencies upon IM&T. Indeed, it is difficult to envisage how many of the goals could be achieved without further developments relating to information and technology.
C2.3 The vision, as set out in the CCG’s 5-year plan, is that health and social care services in Wiltshire should support and sustain independent living, through: ♦ Encouraging and supporting people to take more responsibility for their own health and
wellbeing; ♦ Providing fair access to a high quality and affordable system of care; ♦ Providing less care in hospitals and more care at home or in the community.
C2.4 To deliver this vision, seven workstreams have been established: Primary care, Planned care, Urgent care (UC), Intermediate care, Long term conditions (LTC), End of life (EOL) care, Community teams and services. The 5-year Plan recognises that IT is a strategic enabler “that will be pivotal in ensuring the strategic vision for Wiltshire is realised by 2019.”
C2.5 The Better Care Plan (BCP), jointly developed by the CCG and Wiltshire Council, recognises that integrated working between health and social care means “ensuring care is joined up and information shared appropriately”. For example, a fundamental part of providing person-centred services is for individuals to tell their story only once, rather than having to repeat it to different organisations. Hence the BCP contains an information systems and shared records workstream to develop solutions for data sharing and joint assessments, via the Single View of the Customer (SVoC) / Connecting Data for Life (CDfL) Project.
C2.6 Key themes which have important implications for IM&T include (with examples of IM&T dependencies or opportunities):
6

♦ Extended primary care teams, where care within local clusters is integrated between primary, community and social care services – e.g. technology to enable shared access to patient / client records, care plans, joint assessments, technology to support more effective clinician to clinician communications;
♦ Transforming primary care, through expanded services, extended hours – e.g. remote access to records within GP systems; Technology to support new modes of interaction between patients and clinicians;
♦ Shared decision making with patients - e.g. technology to enable patients to review their care options, view their health records and individualised e-care plans;
♦ Patient self-management – e.g. technology to provide support, advice and guidance, conduct online booking, online prescriptions ordering; Telehealth;
♦ Reduce inappropriate urgent hospital attendance / admission – e.g. risk stratification tool for use by care co-ordinators; Technology to educate and advise patients / carers about appropriate care pathways;
♦ Reduce unwanted variation (in referring, prescribing, acute care intervention rates and length of stay) – e.g. access to comprehensive, timely, robust information / health intelligence for benchmarking and performance monitoring; Pathway guidance and support tools for referring and prescribing clinicians;
♦ Quality and safety – e.g. strengthen reporting, including trend information and benchmarking data;
♦ Commissioning for outcomes – e.g. collection, collation, analysis of information on outcomes along the whole care pathway.
C2.7 The BCP “100 day challenge” initiative, for example, illustrates the wide-ranging nature of the dependence upon IM&T, i.e.: ♦ Referral routes – pathway guidance, directory of services, referral support tools; ♦ DTOC – shared assessments / e-communications amongst professionals before and
after discharge; ♦ Case management – risk stratification tool; ♦ Complex case / EOL management – shared personalised care plans / EOL plans; ♦ Multi-disciplinary primary care teams – e-communications and shared access to records
amongst care professionals; ♦ Monitoring performance – daily dashboard, new indicators.
C3 National Context
C3.1 Many national reports including, and since, the publication of Equity and Excellence: Liberating the NHS have emphasised the critical role of IM&T in transforming health and healthcare, in supporting transparency and in empowering citizens and patients. This has led to the establishment of several national targets that CCGs are expected to achieve. It is also leading to the development of new national information sources, systems and resources to support these over-arching goals. Relevant national IM&T targets and national IM&T-related developments are summarised in Appendix C.
C3.2 NHS England’s guidance Strategic and Operational Planning 2014 to 2019 (December 2013) highlights the importance of an outcomes focused approach, of citizen inclusion and empowerment, and of more integration between providers and commissioners and with social care – all of which have dependence upon better use of information and technology. The guidance emphasises the role of initiatives such as: ♦ Electronic personalised care plans; ♦ NHS Choices website; 7

♦ Telehealth and telecare; ♦ Clinical outcomes data; ♦ Care.data; ♦ Summary Care Record; ♦ Friends and Family Test.
C3.3 The national GMS Contract 2014-15 requires practices to provide specific online services to their patients, as well as complying with various national information / system requirements (see Section D for further details, and Appendix C re national targets).
C3.4 The “Any Town” report and tools produced by NHS England2, and referenced in Wiltshire’s 5-year Plan, attempts to quantify the role of IM&T in cost-saving interventions - for example: ♦ Reducing unwanted variation in primary care referring and prescribing - which relies on
good practice-level data / health intelligence; ♦ Multi-disciplinary case management for the frail elderly and those suffering with a long-
term condition – which is dependent upon use of risk stratification software; ♦ Reducing the number of preventable deaths from medication-related incidents - through
use of clinical decision support tools.
C3.5 The “Any Town” report also highlights the (as yet unquantified) likely net financial benefits arising from IT systems interoperability (i.e. sharing information) across the health economy.
C3.6 NHS England’s “Good data strategy” initiative addresses the presumption that “only through the analysis of high quality data can commissioners ensure that they are securing safe, effective, and equitable care for all”. The vision3 encourages CCGs to broaden the range of data and types of analyses routinely used to support commissioning. For example, alongside more traditional flows of data from healthcare providers, it recommends much greater exploitation of information from service users and from the local population.
C3.7 NHS England recently have delegated responsibility to CCGs for general practice IT (GPIT). Whilst this strategy focuses on commissioning requirements, there are important dependencies upon GPIT, as discussed further below.
D Strategic Framework D1 IM&T Vision
D1.1 Wiltshire CCG’s IM&T vision is that better exploitation of information and technology - both within the CCG and across the whole of health and social care – is critical to achieve “the right healthcare, for you, with you, near you”. Patients will benefit from healthier outcomes, receiving co-ordinated person-centred services (“tell your story once”) that are closer to home (whenever appropriate), which are of high quality, are cost effective and sustainable. This will be achieved by: ♦ Ensuring access to the right information, in the right place at the right time; ♦ Using technology to support best clinical practice, moving to paperless working, thus
facilitating service efficiency, effectiveness and safety;
2 http://www.england.nhs.uk/ourwork/sop/plan-sup-tools/ 3 High quality datasets: Our vision, NHS England, January 2014
8
♦ Allowing greater flexibility in bringing care to the individual, rather than individuals travelling too far to receive care;
♦ Empowering patients and the public to take greater responsibility for their own health and healthcare;
♦ Enhancing commissioning decision-making.
D2 Framework
D2.1 Given this vision, and the kinds of IM&T opportunities / requirements outlined in Section C, the following broad categories will be used for further analysis, each of which responds to a different set of drivers: 1. Commissioning enablement, i.e. the support that the CCG (including its member
practices) needs to be an effective commissioner; 2. Whole system patient information sharing / interoperability, i.e. supporting integrated
patient-centred services across professional and organisational boundaries; 3. Patient / public engagement and empowerment, i.e. provision of information and tools
for direct use by citizens / patients / clients; 4. Infrastructure, i.e. the necessary enablers to support developments in the other three
categories.
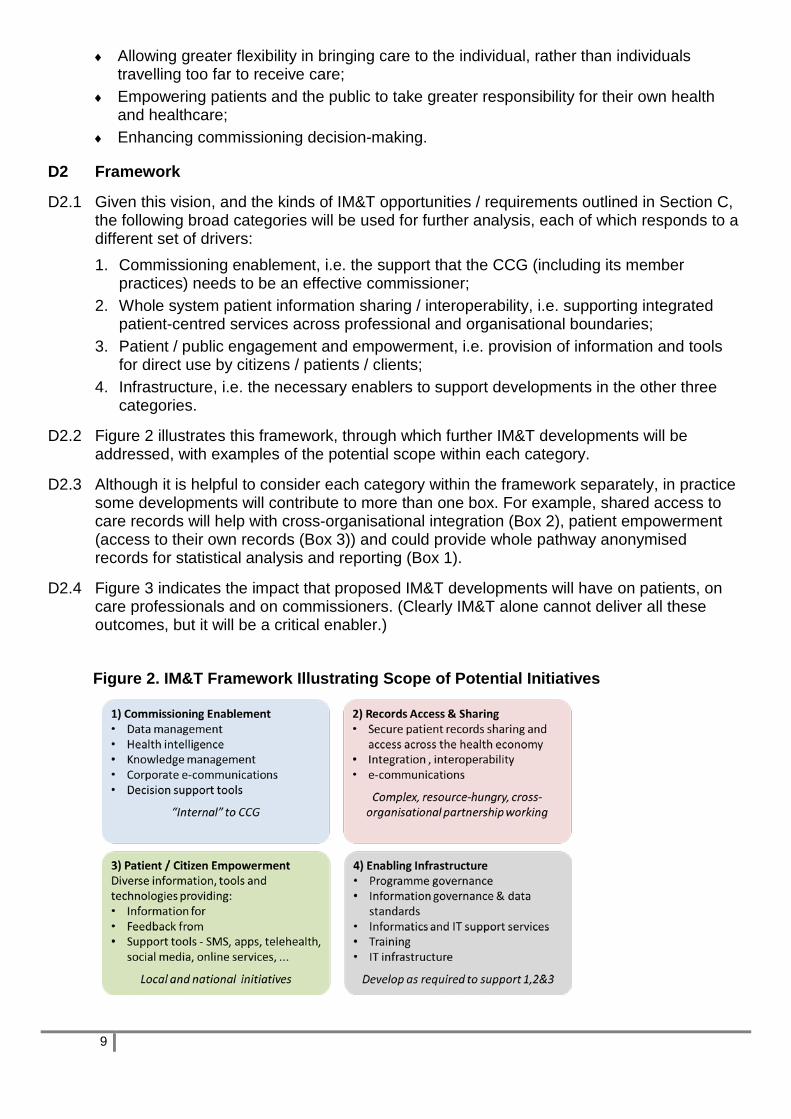
D2.2 Figure 2 illustrates this framework, through which further IM&T developments will be addressed, with examples of the potential scope within each category.
D2.3 Although it is helpful to consider each category within the framework separately, in practice some developments will contribute to more than one box. For example, shared access to care records will help with cross-organisational integration (Box 2), patient empowerment (access to their own records (Box 3)) and could provide whole pathway anonymised records for statistical analysis and reporting (Box 1).
D2.4 Figure 3 indicates the impact that proposed IM&T developments will have on patients, on care professionals and on commissioners. (Clearly IM&T alone cannot deliver all these outcomes, but it will be a critical enabler.)
Figure 2. IM&T Framework Illustrating Scope of Potential Initiatives
9
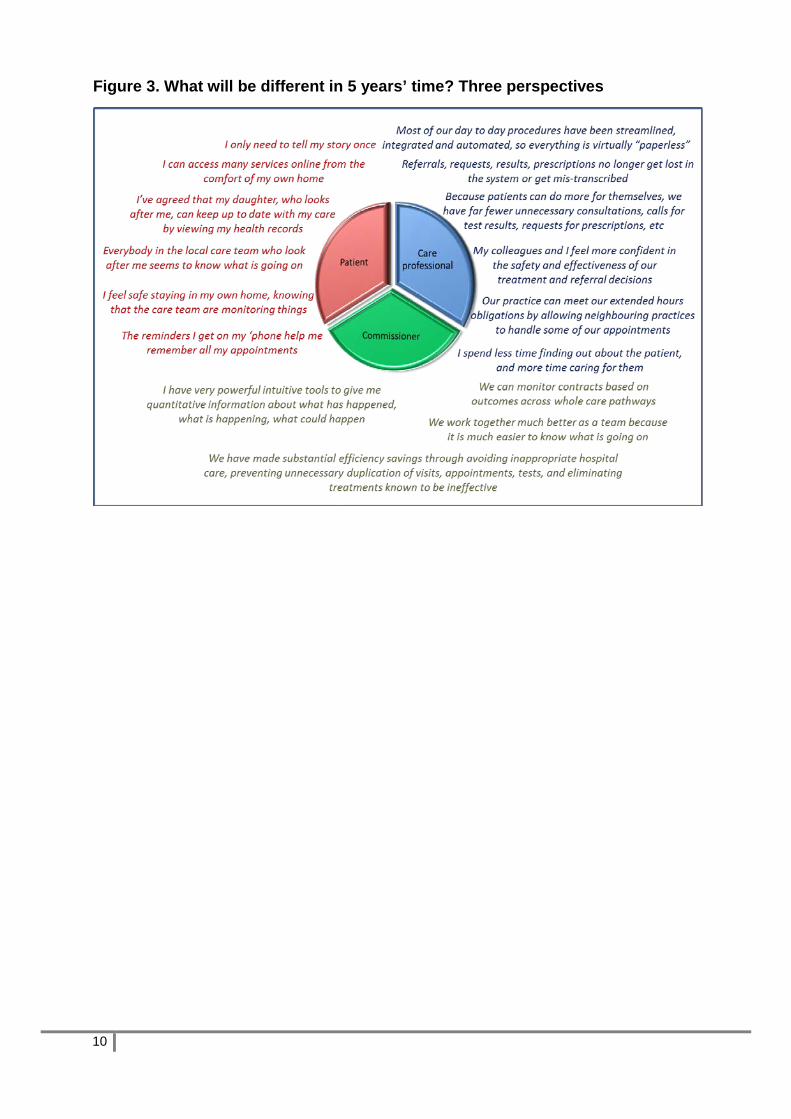
Figure 3. What will be different in 5 years’ time? Three perspectives
10
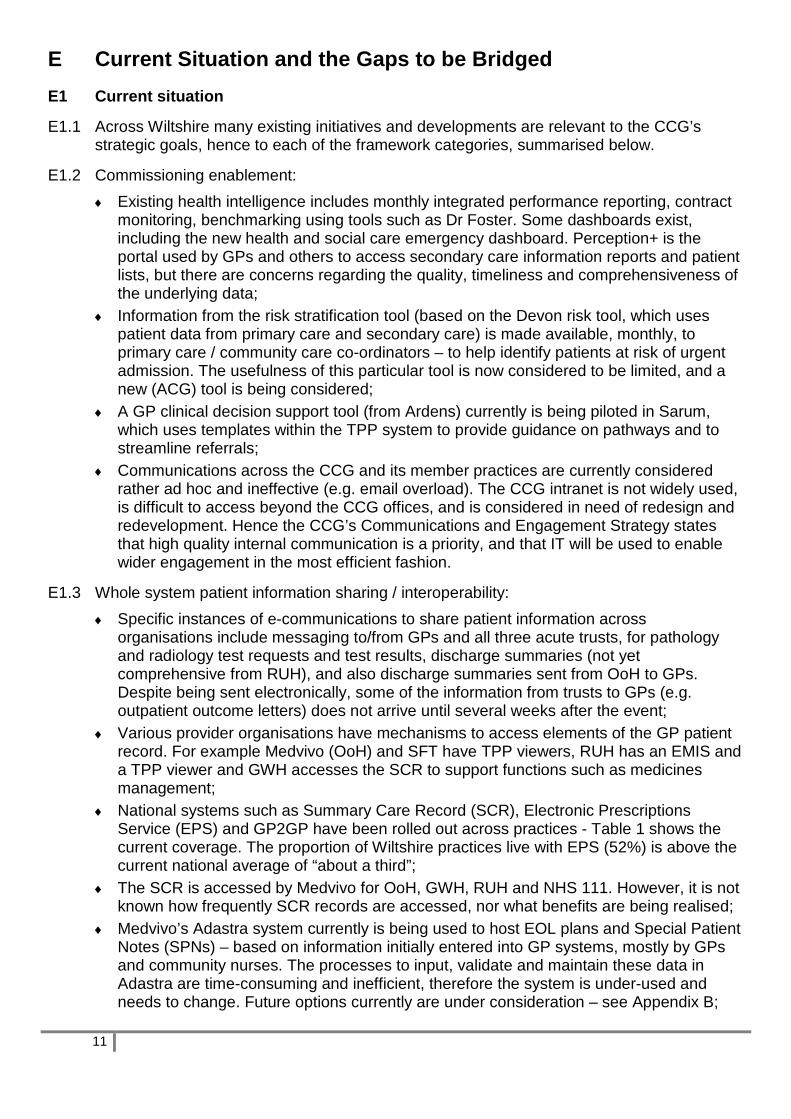
E Current Situation and the Gaps to be Bridged E1 Current situation
E1.1 Across Wiltshire many existing initiatives and developments are relevant to the CCG’s strategic goals, hence to each of the framework categories, summarised below.
E1.2 Commissioning enablement: ♦ Existing health intelligence includes monthly integrated performance reporting, contract
monitoring, benchmarking using tools such as Dr Foster. Some dashboards exist, including the new health and social care emergency dashboard. Perception+ is the portal used by GPs and others to access secondary care information reports and patient lists, but there are concerns regarding the quality, timeliness and comprehensiveness of the underlying data;
♦ Information from the risk stratification tool (based on the Devon risk tool, which uses patient data from primary care and secondary care) is made available, monthly, to primary care / community care co-ordinators – to help identify patients at risk of urgent admission. The usefulness of this particular tool is now considered to be limited, and a new (ACG) tool is being considered;
♦ A GP clinical decision support tool (from Ardens) currently is being piloted in Sarum, which uses templates within the TPP system to provide guidance on pathways and to streamline referrals;
♦ Communications across the CCG and its member practices are currently considered rather ad hoc and ineffective (e.g. email overload). The CCG intranet is not widely used, is difficult to access beyond the CCG offices, and is considered in need of redesign and redevelopment. Hence the CCG’s Communications and Engagement Strategy states that high quality internal communication is a priority, and that IT will be used to enable wider engagement in the most efficient fashion.
E1.3 Whole system patient information sharing / interoperability: ♦ Specific instances of e-communications to share patient information across
organisations include messaging to/from GPs and all three acute trusts, for pathology and radiology test requests and test results, discharge summaries (not yet comprehensive from RUH), and also discharge summaries sent from OoH to GPs. Despite being sent electronically, some of the information from trusts to GPs (e.g. outpatient outcome letters) does not arrive until several weeks after the event;
♦ Various provider organisations have mechanisms to access elements of the GP patient record. For example Medvivo (OoH) and SFT have TPP viewers, RUH has an EMIS and a TPP viewer and GWH accesses the SCR to support functions such as medicines management;
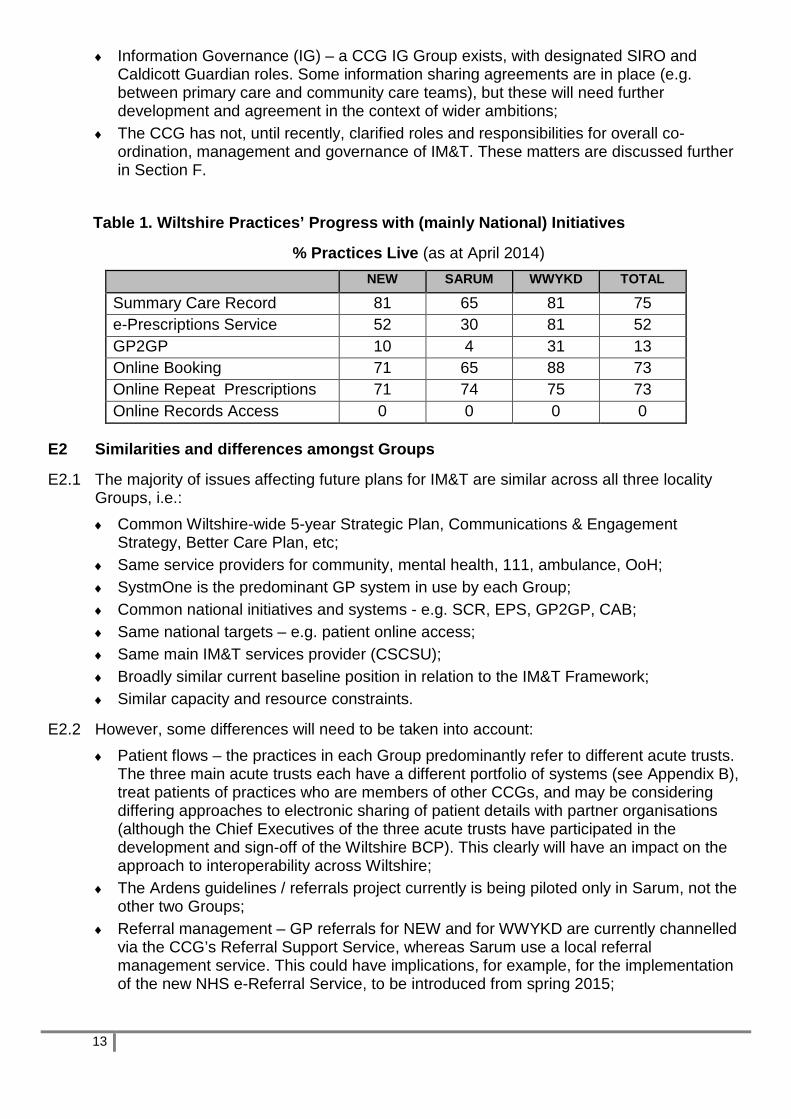
♦ National systems such as Summary Care Record (SCR), Electronic Prescriptions Service (EPS) and GP2GP have been rolled out across practices - Table 1 shows the current coverage. The proportion of Wiltshire practices live with EPS (52%) is above the current national average of “about a third”;
♦ The SCR is accessed by Medvivo for OoH, GWH, RUH and NHS 111. However, it is not known how frequently SCR records are accessed, nor what benefits are being realised;
♦ Medvivo’s Adastra system currently is being used to host EOL plans and Special Patient Notes (SPNs) – based on information initially entered into GP systems, mostly by GPs and community nurses. The processes to input, validate and maintain these data in Adastra are time-consuming and inefficient, therefore the system is under-used and needs to change. Future options currently are under consideration – see Appendix B;
11

♦ General practices have access to the Active Patient Log (APL) which provides a near real-time list of patients admitted to and discharged from hospital – but have no routine information flows on post-discharge care;
♦ A pilot is underway with a few GPs, giving access to a ‘cut down’ view of the adult social care record via a system called Multi Agency View (MAV);
♦ GP2GP is used by some practices (see Table 1) to transfer records between practices when patients move, but there are some practical / technical constraints in obtaining wider take-up, yet to be resolved;
♦ The SVoC / CDfL initiative, which thus far has primarily been led by Wiltshire Council offers potential to address several of the CCG’s integration needs – see below and Appendix D.
E1.4 Patient / public engagement and empowerment: ♦ The CCG’s Communications and Engagement Strategy identifies the important potential
role of e-communications channels, such as social media, webcasting and blogs, for engaging with patients and the public;
♦ The CCG’s website holds content pertinent to the CCG, has links to information on local services and some links to external sites, and a link to Twitter. However, as with the intranet, this is considered in need of redesign and redevelopment. Issues to address include the underlying IT platform and support, synergy and avoiding duplication with other local public-facing websites (e.g. Council, trusts, practices) and establishing clear responsibilities for maintaining specific elements of content and links with other sites;
♦ Table 1 summarises the extent to which practices have implemented online repeat prescriptions, online booking and online records access (which now form part of the national GMS contract) – showing that the majority of practices now offer online booking and ordering of repeat prescriptions but no practices currently offer online access to their records. No statistics are available regarding the extent to which these facilities are being used by patients;
♦ Many practices provide automated patient texting for appointment reminders, results reporting, and more general health promotion campaigns;
♦ To date here have been very limited telehealth initiatives in Wiltshire (although Medvivo provide support for fairly widespread telecare services on behalf of the Council).
E1.5 GP IT and wider Infrastructure: ♦ All general practices have N3 connectivity and wifi throughout their premises; ♦ There is poor 3G/mobile broadband signal coverage across many of the rural areas in
Wiltshire, which currently is restricting more ambitious plans for mobile access to systems and records (e.g. by community care co-ordinators). SystmOne has the capability to be accessed via any internet connection, or records can be downloaded / uploaded when a connection is available, thus supporting, for example, reviewing and recording notes when GPs visit patients in their homes or in care homes;
♦ Some GPs use BT’s secure home working service to connect to their clinical system, via N3;
♦ A current frustration amongst GPs is lack of integration of the user interface between the clinical system and other systems / external information sources, such as emails or guidance tools, which impacts on overall practice efficiency and effectiveness, and ability to move towards paperless working. A single user login solution is required;
♦ CSCSU provide the majority of the CCG’s IM&T-related support services, including data management , health intelligence, project management, IT services, governed through an SLA. Operational GPIT support service contracts across the whole CSCSU area currently are under review, with the intention of re-tendering shortly;
12
♦ Information Governance (IG) – a CCG IG Group exists, with designated SIRO and Caldicott Guardian roles. Some information sharing agreements are in place (e.g. between primary care and community care teams), but these will need further development and agreement in the context of wider ambitions;
♦ The CCG has not, until recently, clarified roles and responsibilities for overall co-ordination, management and governance of IM&T. These matters are discussed further in Section F.
Table 1. Wiltshire Practices’ Progress with (mainly National) Initiatives
% Practices Live (as at April 2014) NEW SARUM WWYKD TOTAL
Summary Care Record 81 65 81 75 e-Prescriptions Service 52 30 81 52 GP2GP 10 4 31 13 Online Booking 71 65 88 73 Online Repeat Prescriptions 71 74 75 73 Online Records Access 0 0 0 0
E2 Similarities and differences amongst Groups
E2.1 The majority of issues affecting future plans for IM&T are similar across all three locality Groups, i.e.: ♦ Common Wiltshire-wide 5-year Strategic Plan, Communications & Engagement
Strategy, Better Care Plan, etc; ♦ Same service providers for community, mental health, 111, ambulance, OoH; ♦ SystmOne is the predominant GP system in use by each Group; ♦ Common national initiatives and systems - e.g. SCR, EPS, GP2GP, CAB; ♦ Same national targets – e.g. patient online access; ♦ Same main IM&T services provider (CSCSU); ♦ Broadly similar current baseline position in relation to the IM&T Framework; ♦ Similar capacity and resource constraints.
E2.2 However, some differences will need to be taken into account: ♦ Patient flows – the practices in each Group predominantly refer to different acute trusts.
The three main acute trusts each have a different portfolio of systems (see Appendix B), treat patients of practices who are members of other CCGs, and may be considering differing approaches to electronic sharing of patient details with partner organisations (although the Chief Executives of the three acute trusts have participated in the development and sign-off of the Wiltshire BCP). This clearly will have an impact on the approach to interoperability across Wiltshire;
♦ The Ardens guidelines / referrals project currently is being piloted only in Sarum, not the other two Groups;
♦ Referral management – GP referrals for NEW and for WWYKD are currently channelled via the CCG’s Referral Support Service, whereas Sarum use a local referral management service. This could have implications, for example, for the implementation of the new NHS e-Referral Service, to be introduced from spring 2015;
13

♦ National initiatives – as Table 1 shows, there is some variation between Groups in the proportion of practices currently offering patients online access and in the take-up of national initiatives. In general Sarum appears to have a slightly lower take-up than the other two Groups.
E3 The Gap between Vision and Current Position
E3.1 This initial analysis has highlighted that many initiatives across Wiltshire have relevance to the IM&T vision and goals set out above. However, several important gaps exist. Furthermore, as indicated, there are acknowledged shortcomings in relation to some of the existing systems, infrastructure and initiatives. Some of the more important of these are identified below.
E3.2 Interoperability – Wiltshire is a long way from achieving the strategic goal of “right information, right place, right time” with shared access to patient / client information across the major social and healthcare organisations. This is now recognised to be a potential limiting factor in meeting many of the strategic ambitions within the CCG’s seven workstreams, hence it needs to be addressed as a priority. Appendix D outlines some of the issues and some of the proposed initiatives to address the information sharing gaps.
E3.3 Shared personalised care plans are required to support at risk patients with complex LTCs or in need of EOL care. The current arrangements for sharing EOL plans are cumbersome and not sustainable in the longer term. Hence new solutions are required for creating, sharing, accessing and updating care plans / SPNs / EOL plans.
E3.4 Digital technology to communicate with patients and citizens – given the high priority assigned to better engagement with patients and the public (so that they are better able to take responsibility for their own health and healthcare), much more could be done using e-communications – both to inform and to receive feedback from individuals. Current initiatives are somewhat “hit and miss”, and their current / potential benefits have not yet been evaluated. There is scope to work more closely with the Council in using common channels for certain public-facing e-communications.
E3.5 Data quality and scope – whilst there are undoubtedly shortcomings in the various data sources used by the CCG and by GPs, some perceptions of poor data quality may arise from user-misunderstanding of data sources, definitions, etc – indicating a need for greater awareness / training, especially amongst GPs and practice staff. Furthermore, the range of data routinely available is limited, with the main focus on acute providers. As more services are delivered through integrated teams, with greater focus on outcomes, new datasets will be required – including from general practice, community and social care – joining together data currently collected by different organisations.
E3.6 Health intelligence and decision support tools - are considered critical to meeting the CCG’s goals. As well as tools for monitoring activity and outcomes, and “drilling down” into the data, there is a need for predictive tools and associated skills – both for (near) “real time” tracking and prediction of service demand and for longer-term predictive modelling. As the range of information sources used by the CCG grows, so will the need for a wider range of comparative datasets and benchmarking tools.
E3.7 Early identification of at-risk individuals is a key element of the BCP. The current risk stratification tool is no longer considered fit for purpose, and will probably be replaced by the ACG tool. It is also intended, as part of the BCP, that social care data (e.g. the frailty index) should be incorporated into the risk stratification process.
14
E3.8 Internal sharing and communications within the CCG / with member practices could be improved by systematising file management and by rationalising the intranet, i.e. a comprehensive knowledge management and communications strategy is required, which should examine the potential of initiatives such as communications with member practices via online discussion forums, and virtual meeting tools such as video-conferencing.
E3.9 Pathways, guidelines and referral decision support tools are required to help avoid inappropriate referrals, improve patient safety, ensure consistency of clinical practice and to streamline referrals processes. Only the Sarum practices which are part of the Ardens pilot currently have access to relevant tools. Whatever the conclusions from and evaluation of the Ardens pilot, a consistent approach should be taken across Wiltshire (other local CCGs are implementing commercially available solutions). Whichever tool is used, existing local and national clinical guidelines will need to be rationalised and maintained.
E3.10 National patient information access targets – as indicated above, several practices are not yet meeting the requirements set out in the GMS contract, especially regarding patient online records access.
E3.11 National initiatives – further work is required to complete the roll-out of EPS, and to a lesser extent SCR, but the main challenge is to ensure the potential patient care benefits from these developments are realised. For example, EPS should prevent a patient having to go to the surgery to request medication and wait for their prescription to be generated. Practices should benefit from reduction in prescription requests, enabling front line staff to deal with more complex problems. Other national systems will need to be implemented locally - such as the NHS e-Referrals Service replacing the existing Choose and Book (CAB) service.
E3.12 Information governance – IG solutions are needed to underpin the wider sharing of records across organisations. The development and agreement of information sharing protocols, with full engagement of local partners / stakeholders, must be a key part of further plans in these areas.
E3.13 As the CCG’s primary care strategy is further developed and implemented, the requirements for IT and for IT support will change – e.g. more reliance on mobile technologies (especially amongst members of the integrated primary care team), use of own devices and 24/7 support cover (a pan-CSCSU GPIT support service contract currently is under consideration), shared records access amongst practices, shared e-care plans, technology to support different modes of consultation.
E3.14 The level of resource allocated to IM&T by the CCG, including contracts for services with CSCSU, will need to be reviewed in the context of this strategy.
15
F Moving Forward F1 Strategic Principles
F1.1 The IM&T Strategy for Wiltshire CCG should be to ensure: ♦ Progress is made across all four categories of the framework, with the whole being
managed and controlled as a structured, planned, resourced IM&T Programme; ♦ There is cohesion across the Programme, rather than a series of ad hoc / piecemeal
developments. Any proposed IM&T development should be subject to approval by the CCG’s IM&T governance arrangements (see below);
♦ There are clear and explicit links between the IM&T programme and the prioritisation of developments, and the CCG’s mainstream workstreams (i.e. EOL, LTC, UC, Primary Care, etc) – where each workstream identifies its future requirements;
♦ There is meaningful ongoing engagement with relevant internal and external stakeholders;
♦ Objectives and benefits from each specific initiative are framed in terms of anticipated health / healthcare outcomes, not just information or technological outcomes, and these benefits will be evaluated;
♦ Plans for major resource commitments will be based on appraisal of the evidence for benefits and on robust business cases;
♦ Many developments (e.g. interoperability, use of social media) will be incremental, with defined milestones, interim benefits and appraisal of lessons learnt;
♦ Wherever appropriate, intelligence will be captured / lessons will be learnt from elsewhere, and opportunities for sharing ideas, procurements and developments with other health economies will be maximised;
♦ End-user awareness, training, change management and sufficient ongoing support for new ways of working should be seen as fundamental to the success of any project / change programme.
F2 Outline Plans
F2.1 Bridging the gap between the current situation and the CCG’s aspirations over the coming years will present several challenges in terms of resources and effort, and also in terms of professional and organisational cultures. Table 2 summarises some of the key developments that need to occur, over the coming months and years.
F2.2 Further analysis and decisions are required to determine overall priorities, but Figure 3 provides an initial indication as to which elements will be needed in the short, medium and the longer term. Table 3 identifies the key initiatives to be progressed throughout the remainder of 2014/15 and during 2015/16. A more detailed Programme Plan will need to be developed once this broad Strategy has been agreed.
F2.3 With regard to plans for shared access to patient / client records, Figure 4 illustrates the overall approach and priorities, and contrasts this with the current situation.
16
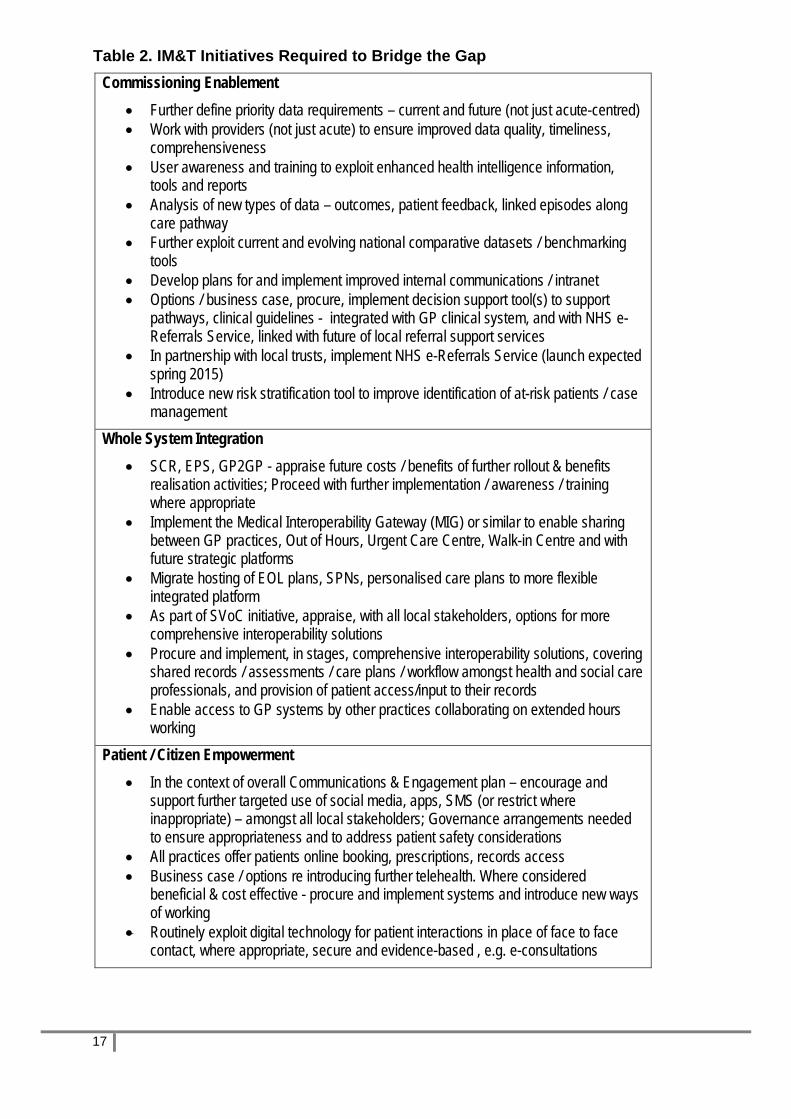
Table 2. IM&T Initiatives Required to Bridge the Gap Commissioning Enablement
• Further define priority data requirements – current and future (not just acute-centred) • Work with providers (not just acute) to ensure improved data quality, timeliness,
comprehensiveness • User awareness and training to exploit enhanced health intelligence information,
tools and reports • Analysis of new types of data – outcomes, patient feedback, linked episodes along
care pathway • Further exploit current and evolving national comparative datasets / benchmarking
tools • Develop plans for and implement improved internal communications / intranet • Options / business case, procure, implement decision support tool(s) to support
pathways, clinical guidelines - integrated with GP clinical system, and with NHS e-Referrals Service, linked with future of local referral support services
• In partnership with local trusts, implement NHS e-Referrals Service (launch expected spring 2015)
• Introduce new risk stratification tool to improve identification of at-risk patients / case management
Whole System Integration • SCR, EPS, GP2GP - appraise future costs / benefits of further rollout & benefits
realisation activities; Proceed with further implementation / awareness / training where appropriate
• Implement the Medical Interoperability Gateway (MIG) or similar to enable sharing between GP practices, Out of Hours, Urgent Care Centre, Walk-in Centre and with future strategic platforms
• Migrate hosting of EOL plans, SPNs, personalised care plans to more flexible integrated platform
• As part of SVoC initiative, appraise, with all local stakeholders, options for more comprehensive interoperability solutions
• Procure and implement, in stages, comprehensive interoperability solutions, covering shared records / assessments / care plans / workflow amongst health and social care professionals, and provision of patient access/input to their records
• Enable access to GP systems by other practices collaborating on extended hours working
Patient / Citizen Empowerment • In the context of overall Communications & Engagement plan – encourage and
support further targeted use of social media, apps, SMS (or restrict where inappropriate) – amongst all local stakeholders; Governance arrangements needed to ensure appropriateness and to address patient safety considerations
• All practices offer patients online booking, prescriptions, records access • Business case / options re introducing further telehealth. Where considered
beneficial & cost effective - procure and implement systems and introduce new ways of working
• Routinely exploit digital technology for patient interactions in place of face to face contact, where appropriate, secure and evidence-based , e.g. e-consultations
17

Infrastructure • GPIT - Complete Windows 7 upgrades and associated hardware refresh • Implement single login solution across multiple systems for practice users, and
others • Further define and start to address current and future mobile working needs,
especially for all members of integrated primary care teams • Develop and agree information sharing protocols amongst all major stakeholders • Ensure IM&T support services and IT infrastructure are sufficiently robust and flexible
to meet growth in demand and user expectations • Widespread IM&T awareness and training linked to services developments • Plan future IT infrastructure changes as technology evolves • Establish new IM&T governance and IM&T clinical leadership arrangements (see
below)
18

Figure 3. Schematic Overview of Proposed IM&T Programme
19
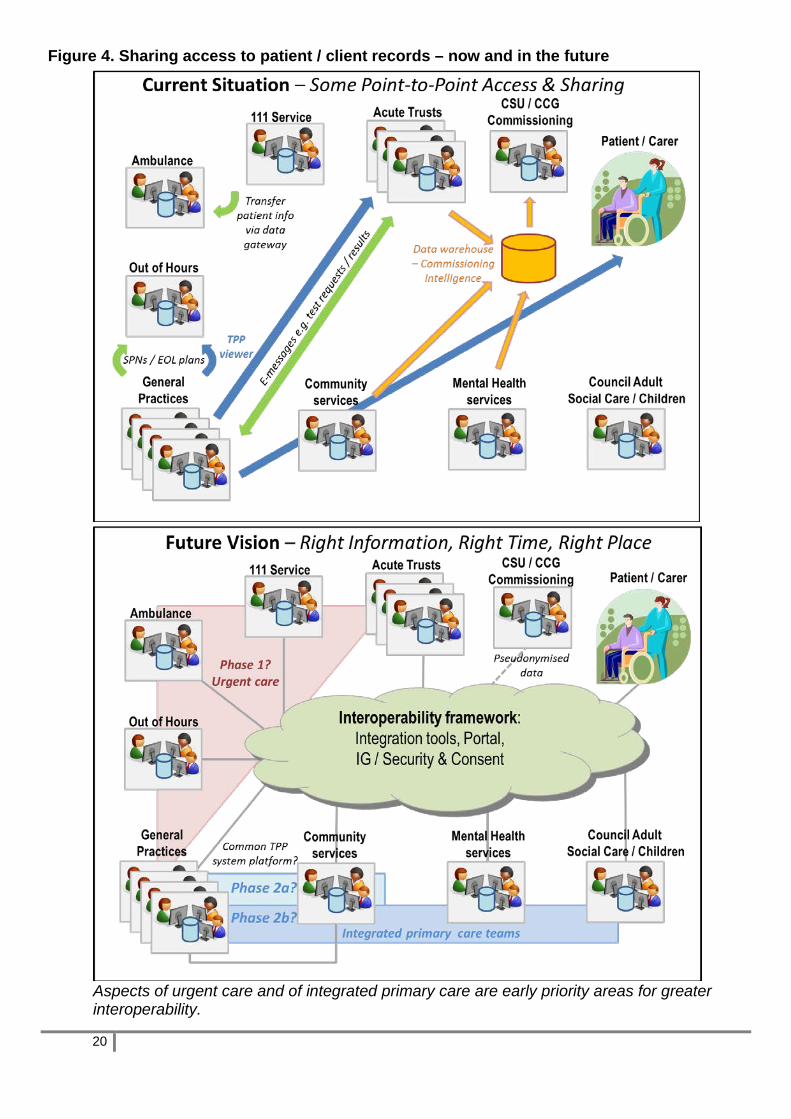
Figure 4. Sharing access to patient / client records – now and in the future
Aspects of urgent care and of integrated primary care are early priority areas for greater interoperability.
20

Table 3. Main Priorities for 2014/5 – 2015/16 (National indicates National requirement; Colour coding as for Figure 3) Initiative 2014/15 2015/16 Benefits Data and information usage
Phase in usage of new CSCSU Health Intelligence reports & tools Practice awareness and training re data, tools, interpretation Commence migration to ACG risk stratification tool (or alternative?)
Use by CCG / practices of new HI tools & reports Complete implementation of new risk stratification tools; Enhance with social care data Develop modelling tool to examine need, demand, provision, capacity and outcomes based on range of health and social care data
Better decision-making, based on better intelligence
Clinical pathways decision support tools
Evaluate Ardens pilot; Consider alternative options Rationalise existing guidelines
Develop business case, procure and commence implementation across all practices
All practitioners follow same, evidence-based guidelines. Less variation in clinical referral and treatment decisions – better outcomes, greater efficiency
e-Referrals Plan for NHS e-Referral Service (from spring 2015) - replaces current Choose & Book service
Implement across whole health system. Integrate user interface with pathways tool
Potential improvements to efficiency and safety, improved referrals data National
Internal document management & communications
Rationalise existing shared files & intranet – to minimise duplication & improve access
Evaluate further tools for sharing and two-way communications (e.g. online forums, video conferencing)
Improved communication and information sharing across CCG and member practices; CCG efficiency
Interoperability – sharing access to health records (tactical)
Evaluate MIG, develop business case (considering alternatives) to support early priorities - urgent care, primary care teams, care plans Develop information governance / consent policies and guidelines
Solution operational across all partners in urgent care pathway and key elements of integrated primary care team
Better coordination / reduce pressure on urgent services Better coordination across primary care teams
Interoperability – sharing access to health and social records (strategic)
Engage with partner organisation, through the BCP CDfL project, to define scope, use cases, priorities, plans – see Appendix D
Business cases(s), procurement(s), development(s) as determined by plans Further develop information governance / consent policies and guidelines
Joined up patient-centred services across care pathways Greater efficiency, effectiveness, safety National (development of plans)
EOL / Care Plans
Migrate from current Adastra-hosted solution to
Use MIG (or alternative solution) to access /
Meet requirements for EOL & shared care plans
21
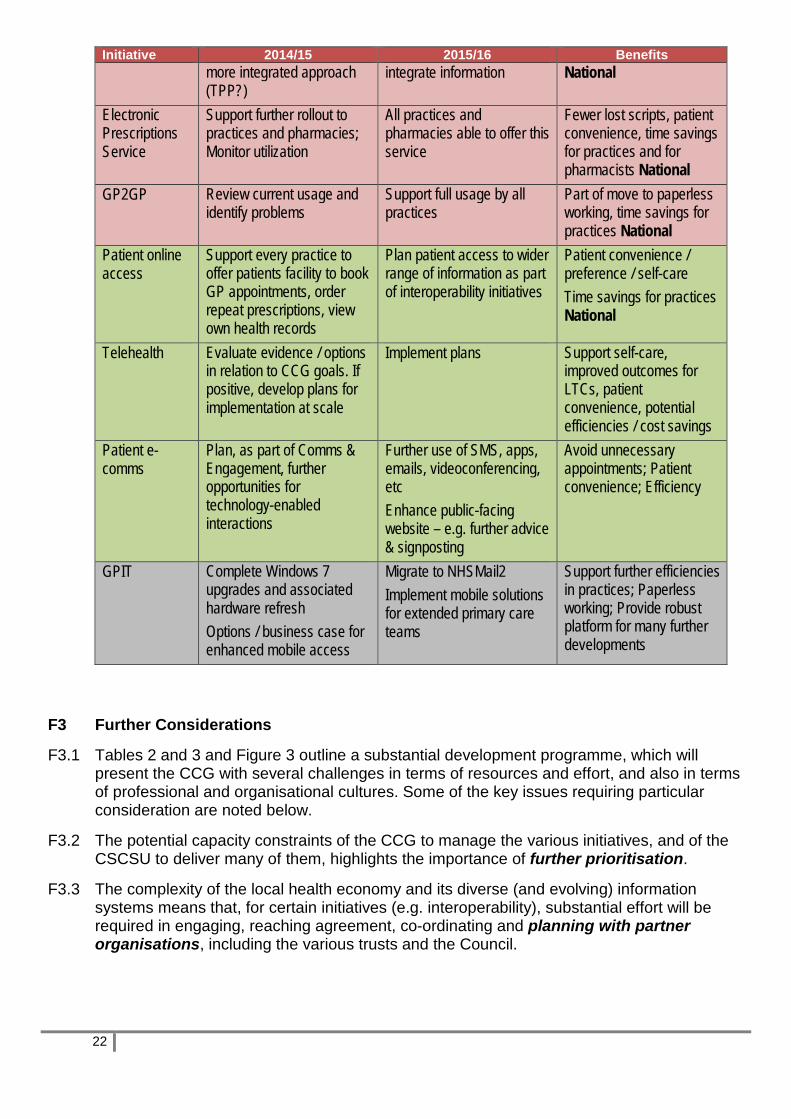
Initiative 2014/15 2015/16 Benefits more integrated approach (TPP?)
integrate information National
Electronic Prescriptions Service
Support further rollout to practices and pharmacies; Monitor utilization
All practices and pharmacies able to offer this service
Fewer lost scripts, patient convenience, time savings for practices and for pharmacists National
GP2GP Review current usage and identify problems
Support full usage by all practices
Part of move to paperless working, time savings for practices National
Patient online access
Support every practice to offer patients facility to book GP appointments, order repeat prescriptions, view own health records
Plan patient access to wider range of information as part of interoperability initiatives
Patient convenience / preference / self-care Time savings for practices National
Telehealth Evaluate evidence / options in relation to CCG goals. If positive, develop plans for implementation at scale
Implement plans Support self-care, improved outcomes for LTCs, patient convenience, potential efficiencies / cost savings
Patient e-comms
Plan, as part of Comms & Engagement, further opportunities for technology-enabled interactions
Further use of SMS, apps, emails, videoconferencing, etc Enhance public-facing website – e.g. further advice & signposting
Avoid unnecessary appointments; Patient convenience; Efficiency
GPIT Complete Windows 7 upgrades and associated hardware refresh Options / business case for enhanced mobile access
Migrate to NHSMail2 Implement mobile solutions for extended primary care teams
Support further efficiencies in practices; Paperless working; Provide robust platform for many further developments
F3 Further Considerations
F3.1 Tables 2 and 3 and Figure 3 outline a substantial development programme, which will present the CCG with several challenges in terms of resources and effort, and also in terms of professional and organisational cultures. Some of the key issues requiring particular consideration are noted below.
F3.2 The potential capacity constraints of the CCG to manage the various initiatives, and of the CSCSU to deliver many of them, highlights the importance of further prioritisation.
F3.3 The complexity of the local health economy and its diverse (and evolving) information systems means that, for certain initiatives (e.g. interoperability), substantial effort will be required in engaging, reaching agreement, co-ordinating and planning with partner organisations, including the various trusts and the Council.
22
F3.4 The likely complexity of several of these initiatives and the need to link in with wider change programmes, means many (but not all) should be managed as structured projects – with clearly defined deliverables, milestones, responsibilities, resources. Some initiatives really are extensions of business as usual. Some initiatives will be IM&T-led projects, others will be projects with an IM&T component. All should be overseen by an IM&T Steering Group / Programme Board (see below).
F3.5 Concerns about confidentiality, particularly in relation to interoperability, amongst health / social care professionals as well as patients and the public, have the potential to delay or halt projects. Therefore information governance issues – developing sharing agreements, considering opt-in / opt-out policies, with widespread awareness and consultation – must be given sufficient focus and resource from the outset.
F3.6 This review has not identified any major differences between the three locality Groups. (Those differences that have been identified are listed in Section E2). Therefore it is assumed that for the majority of issues the three Groups will work together on common priorities.
F3.7 It is essential that roles and responsibilities for management and governance of the IM&T Programme are agreed. It is proposed that to oversee the local implementation and further development of this strategy: ♦ Two (part-time) CCG roles are formalised: a) a senior manager with oversight
responsibility for IM&T, to ensure links with wider CCG plans, QIPP, budgets, CSCSU SLAs, etc, b) a Chief Clinical Information Officer (CCIO), to ensure developments focus on clinical and patient benefits, and are practical and achievable from a clinical perspective. These individuals should, ideally, be on the CCG’s Governing Body, to ensure IM&T has the appropriate profile and is considered at the outset of any development plans;
♦ A Wiltshire CCG IM&T Steering Group is established with, in addition to the above two roles, representation from other disciplines, and the CCG’s Caldicott Guardian and attended by a local CSCSU representative. Figure 5 shows the governance structure for this Group. Terms of reference for the Group have been developed, and the terms of reference, representation and accountabilities of other existing relevant local groups (e.g. the Primary Care IT Forum, the IG Group) should be reviewed in the light of this Strategy.
23

Figure 5. IM&T Steering Group Governance and Accountability
F4 Next Steps
F4.1 Some of the activities required in the short term to progress the IM&T Programme include: ♦ Strategy and Planning - Further develop IM&T Programme Plans, e.g. further
prioritisation, defining links with other initiatives, further detail on what, when, how, how much, development of Benefits Register and Risks Register;
♦ Projects - Formalise existing initiatives as projects, initiate new formal projects, with involvement of partner organisations where appropriate;
♦ Governance – Establish the governance and management arrangements proposed above; The role of the PMO should be considered in supporting matrix working between IM&T and other workstreams;
♦ Awareness and consultation – develop effective two-way internal and external communications about the strategy, and key elements of the plan. In particular engage further over information governance issues and address some of the cultural issues e.g. regarding information access and sharing;
♦ Resources – identify capital and ongoing resource requirements (funding and effort) arising from each element of the IM&T Programme. Identify potential sources of external / additional funding. Align resource commitments with resource requirements.
24

Appendix A. Glossary A&E Accident & Emergency Department ACG Adjusted Clinical Groups (tool for risk stratification / predictive modelling) APL Active Patient Log AWP Avon and Wiltshire Partnership Trust BCF / BCP Better Care Fund / Plan BT British Telecommunications CAD Computer Aided Dispatch system CCG Clinical Commissioning Group CCIO Chief Clinical Information Officer CDfL Connecting Data for Life project CITHS Commodity IT Hardware & Software framework CSCSU Central Southern Commissioning Support Unit CSU Commissioning Support Unit DTOC Delayed transfer of care EOL End of Life EPS(r2) Electronic Prescription Service (Release 2) GMS General Medical Services GP General Practice / Practitioner GP2GP Electronic transfer of patient records between general practices GPIT IT and systems to support general practices GPSoC GP Systems of Choice (national framework for GPIT solutions) GWH NHSFT Great Western Hospital NHS Foundation Trust, in Swindon HL7 Health Level 7 messaging standards IG Information Governance IM&T Information Management and Technology IT Information Technology LTC Long-term Condition MAV Multi Agency View MIG Medical Interoperability Gateway N3 NHS secure broadband service NEW North and East Wiltshire locality group OoH Out of Hours primary care services PDS Personal Demographics Service RUH Royal United Hospital, in Bath SCR Summary Care Record SFT Salisbury Foundation Trust SLA Service Level Agreement SMS Short Messaging Service (mobile phone texting) SPN Special Patient Note SVoC Single View of the Customer SWAS South Western Ambulance Service UCC Urgent Care Centre WIC Walk in Centre WWKYD West Wiltshire, Yatton Keynell and Devizes locality group
25

Appendix B. Patient / Client Systems Across Wiltshire This information is presented subject to confirmation. Organisation Current System(s) Issues General practices All but 5 of the 56 practices use TPP’s
SystmOne Although there would be benefits from all being on SystmOne, the remaining practices have choice. The one remaining Vision practice is considering moving to SystmOne
GWH NHSFT Community Services
EPEX is core system, plus other systems for certain services – see below. EPEX is hosted by GWH and is not HL7 compliant
Systems need replacing, but services contract to be re-tendered shortly - see below
Medvivo Out of Hours service
Adastra, hosted by CSCSU. Have access to SCR
Considering systems options to provide more connectivity - see below
GWH NHSFT Acute Services
EPR covers PAS, clinical departments, order comms, PACS. Core system, from Medway, implemented several years ago, upgraded last year. Anglia’s ICE for requesting / results reporting. SCR accessed for medicines management and plans in place to implement SCR viewing in A&E and admissions wards
Swindon OoH and WIC sited on hospital site. Strong links with Swindon CCG and their IT plans
Salisbury Foundation Trust
iSOFT PAS. Records shared with Hampshire GPs and others through Hantsnet (based on Graphnet system). TPP GP records viewer in e.g. A&E, podiatry. Indigo4 for messaging with GPs.
Trust developing plans to replace core PAS / EPR
Royal United Hospital Cerner Millennium PAS/EPR (have recently migrated from national contract). Anglia’s ICE for requesting / results reporting. Widespread access to TPP viewer and SCR throughout the hospital
Avon and Wiltshire Partnership Trust - mental health services
RiO implemented about 2 years ago
NHS 111 service provided by Care UK
Adastra (not the same instance as used by Medvivo or SWAS). Access to Adastra is variable, depending where patient call is taken (calls may be re-directed to different call centres). Access to SCR
No direct connectivity with other organisations systems. Faxes sent to GPs and OoH
South Western Ambulance Service
999 service currently uses the Intergraph Computer Aided Dispatch system (CAD). N3 connected, but do not access national PDS. Have data gateway link with 111 service. Plans in place to enable SCR access on board vehicles from Autumn 2015.
Plan to migrate to MIS Systems Engineering’s C3 CAD system in April 2015. Have data links between OoH and CAD in Gloucestershire, and wish to expand connectivity across care pathways in Wiltshire
Wiltshire Council - Adult social services and Children’s services
Carefirst – modules cover both Children’s and Adult services. The Council access the NHS PDS (spine), and 84% of all current social care customer records have a validated NHS
Pilot underway to provide GPs with access to limited social care record via Multi Agency View (MAV) system.
26

number. N3 utilised when sharing data with health partners.
See Appendix D re SVoC.
Care homes Most have no client IT system Continuing Healthcare team use the Care Home Selection system, which is not N3 compliant
Proposal developed to offer TPP module (free) to all local care homes, based on their mobile working app. It does not require N3 connectivity
General Issues
♦ Highly complex and evolving systems landscape ♦ Wiltshire CCG is not the only commissioner for each acute trust, nor for several of the
other services, hence records sharing solutions must be consistent with approaches being taken elsewhere (i.e. standards-based, portal-based)
♦ Some records sharing solutions already established, e.g. HantsNet used by SFT ♦ Dialogue about interoperability / records sharing with all partner organisations essential.
GWH NHSFT Community Services Business case submitted to CCG for replacement of core community system. TPP is the favoured option. Some services currently use systems other than EPEX. Decisions needed as to whether all of these migrate to the replacement system:
♦ MIU use Windmill system, developed and supported by CSCSU; ♦ Child Health (covers five different services, plan is to rationalise and consolidate these) –
core system is McKesson’s CarePlus, on the same hub as Sirona (Bath) and Gloucester Community Services, both of whom are moving / have moved onto SystmOne. System re-procurement for Wiltshire is underway, independent of core community system replacement (above);
♦ Podiatry use TPP SystmOne.
Issues: ♦ Have a requirements / Output-based Specification been produced, including
interoperability requirements for either proposed new system? ♦ Business justification for single supplier procurement for core Community? ♦ Timing of system change in relation to community services re-procurement? ♦ Relationship between Child Health procurement and core Community system
procurement?
Medvivo Out of Hours Service Adastra now effectively fulfils two functions: a) Patient records system for OoH, b) Database for holding SPNs and EOL plans for, potentially, sharing more widely. In terms of the first, the system supports most of the OoH functions required, but has limited ability to inter-operate with other organisations’ systems (GP, 111, A&E, ambulance). In terms of the second, the lack of connectivity means that data input and maintenance is time-consuming and Adastra is unable to act as an Electronic Palliative Care Coordination System (EPaCCS), linking with care providers across a locality.
27

Therefore options for the replacement of the system are being considered. They include: ♦ Continue with Adastra as now for both functions ♦ Continue with Adastra plus the MIG for both functions ♦ Continue with Adastra (with or without MIG) for a. but procure/implement a separate
replacement system (e.g. TPP) for b. ♦ Procure/implement replacement system for both a. and b.
Issues: ♦ Options appraised as part of a business case? ♦ Rationale / business justification for possible single supplier (TPP) procurement for
replacement system? ♦ Definition of requirements (including interoperability) for replacement system.
28

Appendix C. National IM&T Targets and Relevant Developments The NHS Mandate (November 2012) defines specific IM&T delivery targets, which build on goals set out in the previously published NHS Operating Framework for 2012/13, and “The Power of Information”. The GMS Contract 2014-15 also includes several of these targets, since they must be actioned within general practice. The targets are:
By March 2015 ♦ Everyone who wishes will be able to get online access to their own health records held
by their GP (from April 2014, GMS Contract); ♦ Everyone will be able to book GP appointments and order repeat prescriptions online
(from April 2014, GMS Contract); ♦ Everyone will be able to have secure electronic communication with their GP practice,
with the option of e-consultations becoming much more widely available; ♦ All referrals to be made electronically (not explicit in NHS mandate, but announced by
Secretary of State for Health and the NHS Commissioning Board’s Director of Patients and Information in speeches in January 2013);
♦ Clear plans will be in place to enable secure linking of electronic health and care records wherever they are held, so there is as complete a record as possible of the care someone receives;
♦ Clear plans will be in place for those records to be able to follow individuals, with their consent, to any part of the NHS or social care system.
The GMS Contract 2014/15 also states that practices should put in place as soon as possible after 1 April 2014 (and must, by 30 September 2014, publicise its plans to enable it to achieve these requirements by no later than 31 March 2015) the following requirements:
♦ Include the NHS Number as the primary identifier in all NHS clinical correspondence; ♦ Enable successful automated uploads of any changes to a patient’s summary
information, at least on a daily basis, to the Summary Care Record (SCR) or have publicised plans in place to achieve this;
♦ Utilise the GP2GP facility for transfer of all patient records between practices, when a patient registers or de-registers (not for temporary registration), or have publicised plans in place to achieve this.
Also, it expected that CCG’s will be required, by NHS England, to ensure that practices implement the NHS e-Referrals Service (“re-launch” of the current Choose & Book) once it is available (expected spring 2015), as part of the move to 100% paperless referrals.
By 2017 ♦ Significant progress will be made towards three million people with long-term conditions
being able to benefit from telehealth and telecare. (This requirement is re-enforced in planning guidance for 2013/14 from the Commissioning Board which states “we will expect commissioners to promote the benefits of technology in improving outcomes with a particular emphasis on much more rapid take up of telehealth and telecare in line with patient need.”)
By April 2018
♦ Digital information [i.e. patient records] to be fully available across NHS and social care services, barring any individual opt outs.
29

CCG IM&T Responsibilities In addition, “Securing excellence in GP IT Services. Operating Model, 2nd edition”, NHS England, April 2014 details those areas where NHS England has delegated responsibility for operational management of GP IT and associated funding to CCGs. In turn, CCGs will be expected to commission GP IT support services (including the management of the associated assets) from appropriate providers, for example CSUs or other IT providers, or they may choose to deliver these services themselves. The “Core” services include:
♦ Service Desk ♦ General Infrastructure Service ♦ Local Clinical Server Support ♦ Desktop Maintenance and Support Service ♦ Disaster Recovery and Business Continuity Support Service ♦ Asset Management & Software Licencing Service ♦ Supplier Management and Procurement Service ♦ On-going Support for GP Clinical Systems ♦ Technology Infrastructure Refresh Service ♦ Training Service ♦ National Strategic System Implementation Service * ♦ Routine Project and Change Management Service ♦ Client Relationship Management Service * Covers national programmes such as Summary Care Record, Electronic Prescription Service, e-referrals, GP2GP and Patient Online that promote and support greater use of digital technologies in primary care and underpin local strategies for integrated care.
The “Add-on” services (which are discretionary, to align with CCG strategies) include: ♦ Additional Infrastructure and Hardware Services ♦ Additional Service Provision ♦ Additional GPSoC Services ♦ Informatics Strategy Support and Planning ♦ Estates Strategy Service ♦ Exploitation and Optimisation of Core Clinical systems ♦ Primary Care Data Quality Service.
30
Appendix D. Shared Access to Patient / Client Information Introduction The main report has highlighted that several of the CCG’s strategic goals are dependent upon improved cross-organisational shared access to patient / client records – so-called “interoperability” amongst patient / client systems. The vision is “right information, right time, right place”, but there are several ways in which this vision may be realised. This section summarises some of the requirements, issues and relevant current initiatives. Requirements Interoperability covers a range of approaches which all have the objective of allowing users to access information that originated outside of their own local system. The most appropriate approach will be determined by the users’ data and functional requirements, and the approaches are not mutually exclusive. They include:
a) “Point to point” messaging and storage, e.g. as now for pathology results sent from lab systems to GPs, and filed in the patient’s clinical record in the GP system;
b) View only access of one particular system, e.g. as now for A&E departments presented with a view of patient information based on records held in EMIS or TPP or SCR;
c) View only access of information derived from several systems, i.e. through use of an integration engine and portal;
d) Access and local storage of information derived from several systems, i.e. as for c) but with key elements of the data transferred to and stored in, the user’s local system, as in a);
e) Smart forms and workflow, i.e. as for c) with ability to use e-forms for collecting additional data not held in provider systems and / or tools to send messages, alerts or reminders triggered by data in the shared record, as part of a systematic workflow across a multi-disciplinary team;
f) Interactive access, e.g. by a GP in practice A who has a consultation with a patient from practice B, needing to view the detailed patient record, and to update it and use system B to make a referral, prescribe, etc;
As the main report illustrates, the CCG has many examples of specific requirements, e.g.:
♦ Primary care extended hours – example f) above; ♦ EOL – development of an electronic palliative care coordination system (EPaCCS); ♦ Shared personalised care plans – as required by the Avoiding Unplanned Admissions
DES, for all patients on the case management register; ♦ DTOC – shared assessments and workflow amongst health and social care
professionals, before and after discharge; ♦ Integrated primary care teams / Better Care Plan– shared access to patient-centred
record, e-comms to support workflow amongst health and social care professionals. Patient access to their own records is also an important requirement. Robust and secure mobile working solutions are a key part of delivering the “right information, right time, right place”. Issues There is a diversity of requirements - each requires fuller definition, through consideration of “use cases” and analysis of care pathways, leading to clarity about scope.
31

Some requirements are needed in the short to medium-term, and may be addressed with tactical solutions. Others are more complex and may take several years to evolve. Hence the CCG’s approach to interoperability should involve structured projects, with clear staging, yielding phased deliverables and phased benefits. There is a diversity of systems which need to interoperate - see Appendix B. In general, the CCG should not be looking for single system solutions, but for different levels of integration between systems. The portal model is most likely for most applications. Different organisations are at different levels of maturity re internal systems, and may have different approaches to external integration. The CCG and the Council need to actively engage on these issues with all partner organisations, initially to establish common assumptions and core principles. Several neighbouring health economies already have (partial) interoperability solutions in place, or are actively developing them, e.g. Bristol’s Connecting Care, using the Orion portal; Swindon is using Black Pear software to provide cross-practice links; Salisbury acute trust uses Hantsnet based on Graphnet; Oxfordshire use the OCS, which is based on the MIG and CaseNotes software; IG / Information Sharing Agreements / secure modes of access are critical to success. Unless these are addressed early on, it is likely to cause project delays or even abandonment. The lessons from elsewhere are that this takes time. Therefore internal and external communications, including with patients / public, need to be managed carefully. Security is likely to be handled through the roles based access (RBAC) framework, based on the “need to know” principle. Relevant current and proposed initiatives Single View of the Customer / Connecting Data for Life Project (CDfL) The aim of this interoperability project is to “share and use information to integrate services and meet the needs of individuals and communities.” This project aims to extend across all NHS health providers in Wiltshire and to ensure records are accessible remotely. The project will use a middleware solution for data cleansing and data mapping, making it fairly independent of specific IT solutions in other organisations. The project is at an early stage, needing further scoping and definition of priorities and requirements. Some funding has been allocated via the BCF, and external funding has been sought from the NHS Integrated Digital Care Fund. A structured project approach is now needed to further define scope, requirements, phasing, business justification, procurement model, plans, and to start addressing some of the data sharing / IG / personal consent issues. Medical Interoperability Gateway (MIG) There is a proposal to implement the MIG to enable records sharing amongst GP practices, Out of Hours, Urgent Care Centre, Walk-in Centre in the short-medium term. The MIG could also support the creation and maintenance of shared EOL plans / Care Plans (see Appendix B on options regarding Adastra, TPP). In the longer term, the MIG should be able to provide interoperability between these systems and future whole-system strategic platforms (i.e. as required by the Connecting Data for Life Project). A business justification and plan are now required to allow decisions to be made on how and when this enabling piece of work could be taken forward.
32