Clinical Commissioning Group (CCG) Governing Body - … · Clinical Commissioning Group (CCG)...
34
Clinical Commissioning Group (CCG) Governing Body Date of Meeting: 21 September 2012 Agenda Item: Di 17 Subject: Performance Report Reporting Officer: Sandra Croasdale (Head of Performance) Purpose of the Paper: The purpose of this report is to update NHSHMR CCG Governing Body on NHSHMRs performance the Operating Framework requirements for 2012/2013. Performance against the 2012/2013 Business Plan is also included in the report. Governance: Link to PCT Strategic Objectives Performance reporting, and more importantly monitoring, is key to enabling the organisation to achieve its objective to becoming a high performing organisation and ensures delivery of the Strategic Objectives. Resolution: To approve To support Recommendation To review performance against the Operating Framework targets and support ongoing workstreams to drive improvements in this performance. To note the organisations performance against the business plan Key implications for the following: Financial Key Financial Implications: Has this paper been approved by the Finance Department? Yes / No / N/A N/A If YES: Name and Job Title of member of the Finance Department If NO what process has been agreed for financial sign off? Value for Money N/A Risk Potential risks of not achieving specific targets are detailed in the report Legal N/A Workforce N/A Equality Impact Assessment: Included in Paper yes no n/a Comments Patient & Public Involvement Clinical Engagement Parties/ Committees consulted Business Intelligence Indicator and Action Plan owners
-
Upload
truongdien -
Category
Documents
-
view
217 -
download
1
Transcript of Clinical Commissioning Group (CCG) Governing Body - … · Clinical Commissioning Group (CCG)...
Clinical Commissioning Group (CCG) Governing Body
Date of Meeting: 21 September 2012
Agenda Item: Di 17
Subject: Performance Report
Reporting Officer: Sandra Croasdale (Head of Performance)
Purpose of the Paper:
The purpose of this report is to update NHSHMR CCG Governing Body on NHSHMRs performance the Operating Framework requirements for 2012/2013. Performance against the 2012/2013 Business Plan is also included in the report.
Governance:
Link to PCT Strategic Objectives
Performance reporting, and more importantly monitoring, is key to enabling the organisation to achieve its objective to becoming a high performing organisation and ensures delivery of the Strategic Objectives.
Resolution:
To approve To support
Recommendation To review performance against the Operating Framework targets and support ongoing workstreams to drive improvements in this performance. To note the organisations performance against the business plan
Key implications for the following:
Financial
Key Financial Implications:
Has this paper been approved by the Finance Department?
Yes / No / N/A N/A
If YES: Name and Job Title of member of the Finance Department
If NO what process has been agreed for financial sign off?
Value for Money
N/A
Risk Potential risks of not achieving specific targets are detailed in the report
Legal N/A
Workforce N/A
Equality Impact Assessment:
Included in Paper
yes no n/a
Comments
Patient & Public Involvement
Clinical Engagement
Parties/ Committees consulted
Business Intelligence Indicator and Action Plan owners
Performance Report
September 2012
Version 1.0
Author Sandra Croasdale, Head of Performance
Contents
1. Executive Summary ........................................................................................................ 1
2. Performance against Integrated Performance Measures ..................................................... 1
3. Performance against 2012/13 Business Plan ..................................................................... 7
4. Recommendations .......................................................................................................... 7
Appendix 1 ........................................................................................................................ 8
Appendix 2 ...................................................................................................................... 13
Appendix 3 ...................................................................................................................... 16
Appendix 4 ...................................................................................................................... 17
Appendix 5 ...................................................................................................................... 21
Performance Report September 2012
1
1. Executive Summary
1.1 The purpose of this report is to update the CCG Board on NHSHMRs performance
against national and corporate priorities. It covers performance until end July
2012, unless otherwise specified within the body of the report. The date shown for
each indicator in Appendix 1 is the date of the latest available data.
1.2 An “at a glance” Executive Summary shows performance against all Operating
Framework targets on one page. Where indictors are underperforming, and
exception report is provided in Appendix 1.
1.3 Performance to date against the 2012/13 Business Plan is also included in this
report, along with an Equality Impact Assessment of the Plan shown in Appendix
5.
2. Performance against Integrated Performance Measures
2.1 The following are presented:
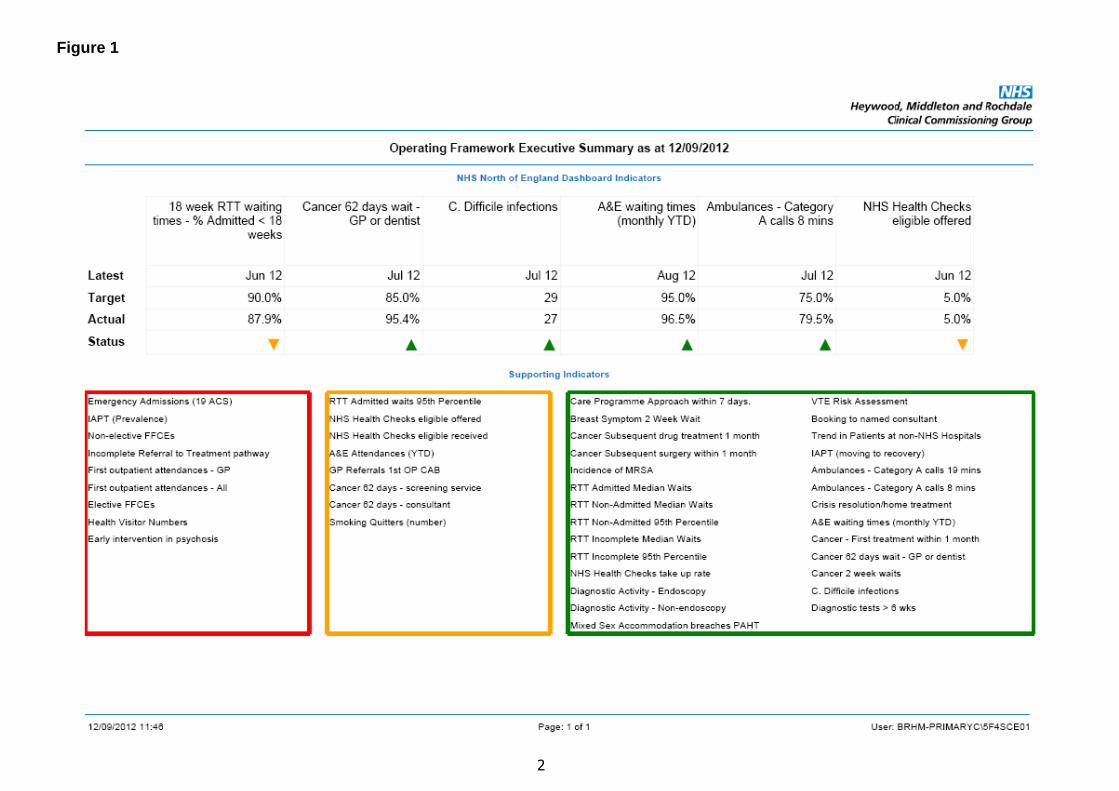
Figure 1: Executive Summary of performance against Operating Framework
2012/13
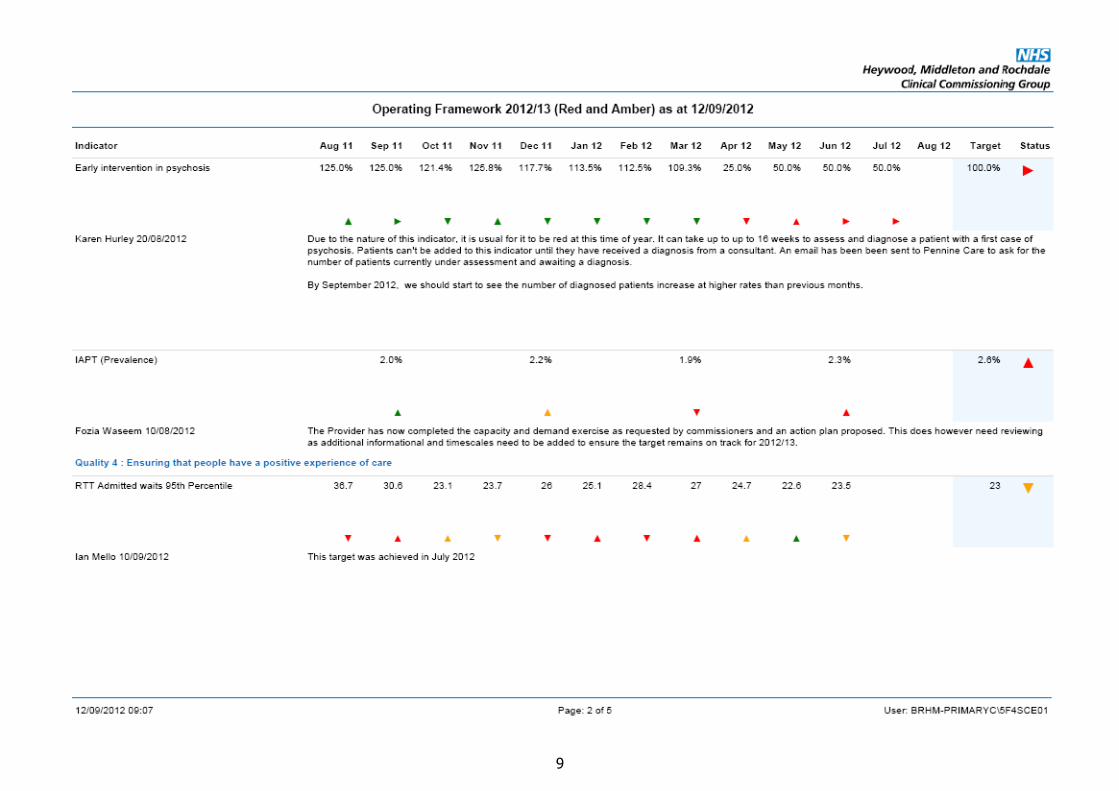
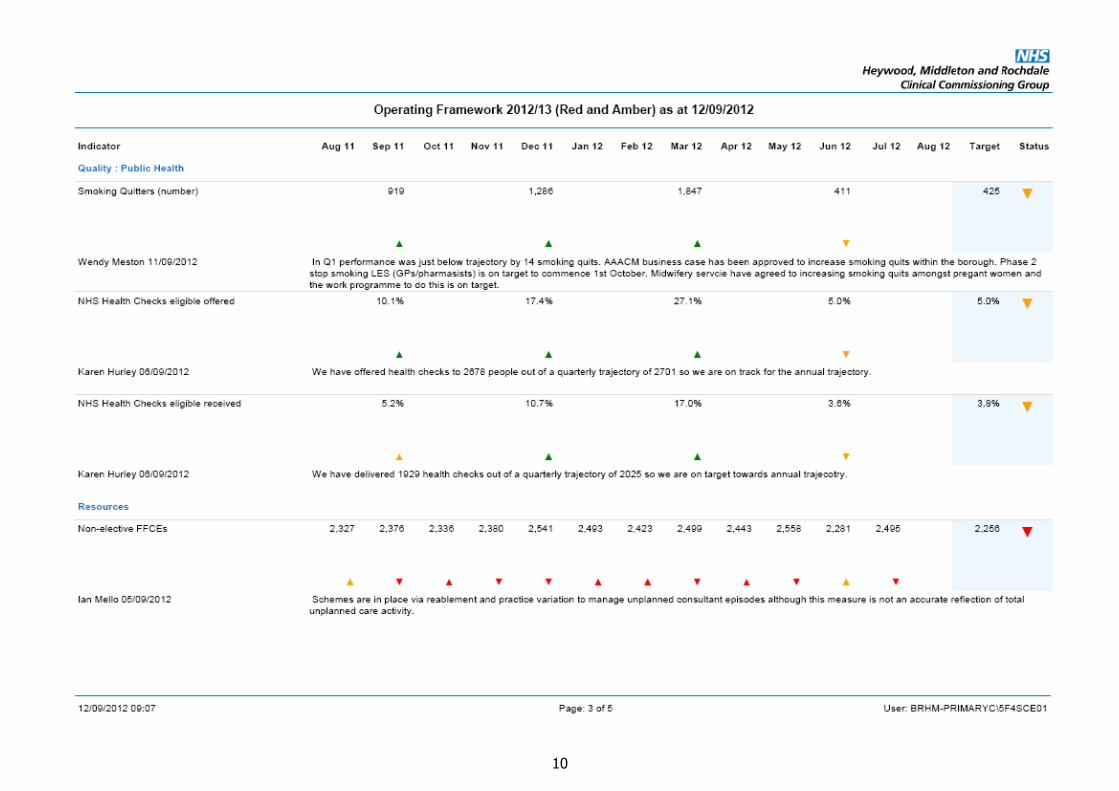
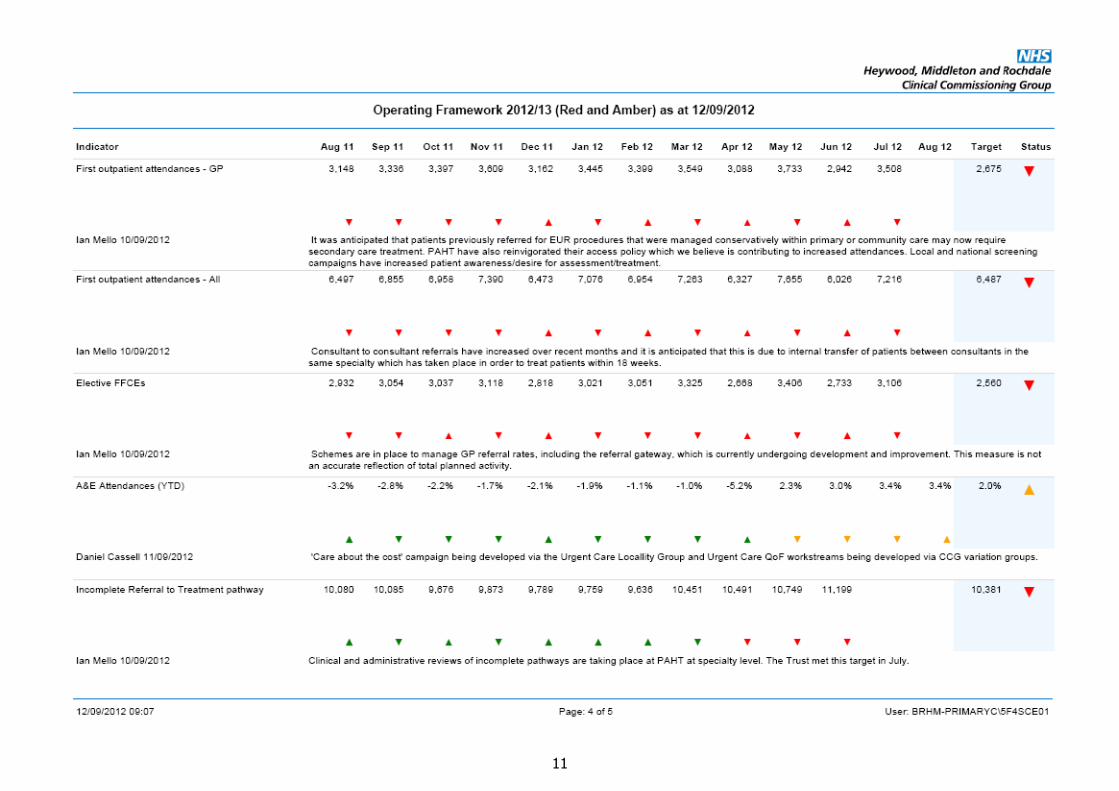
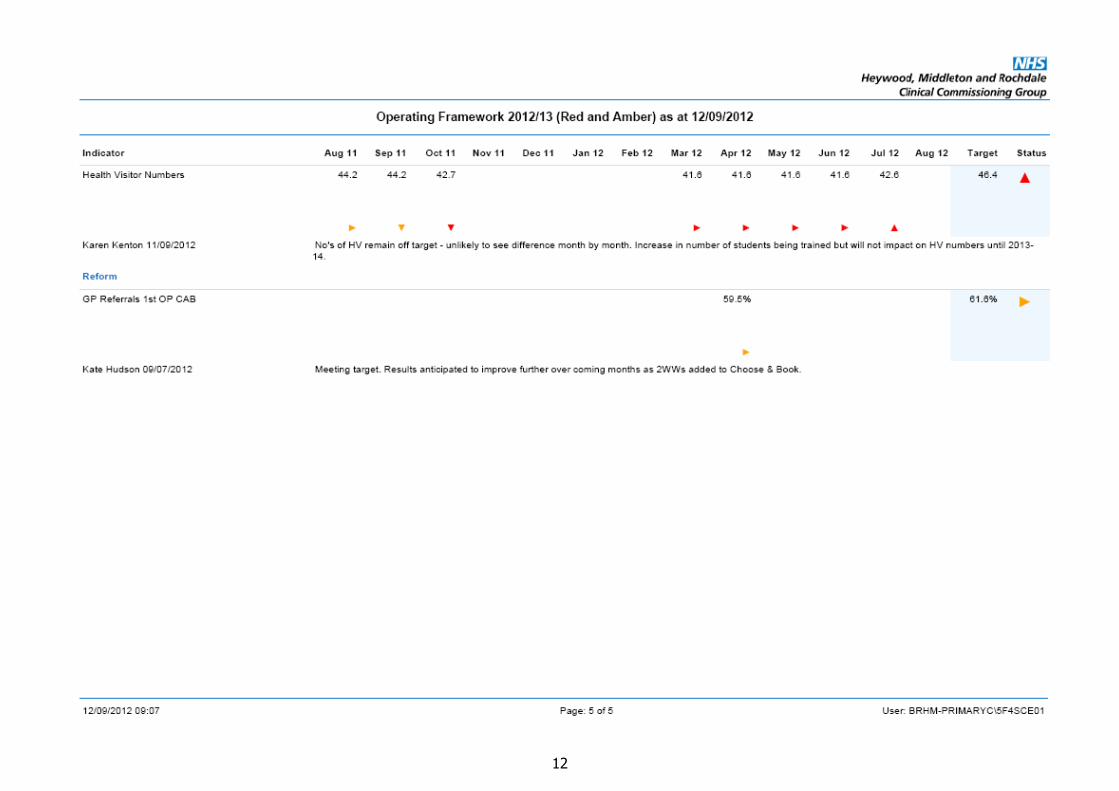
Appendix 1: Operating Framework targets by exception (12 month trend)
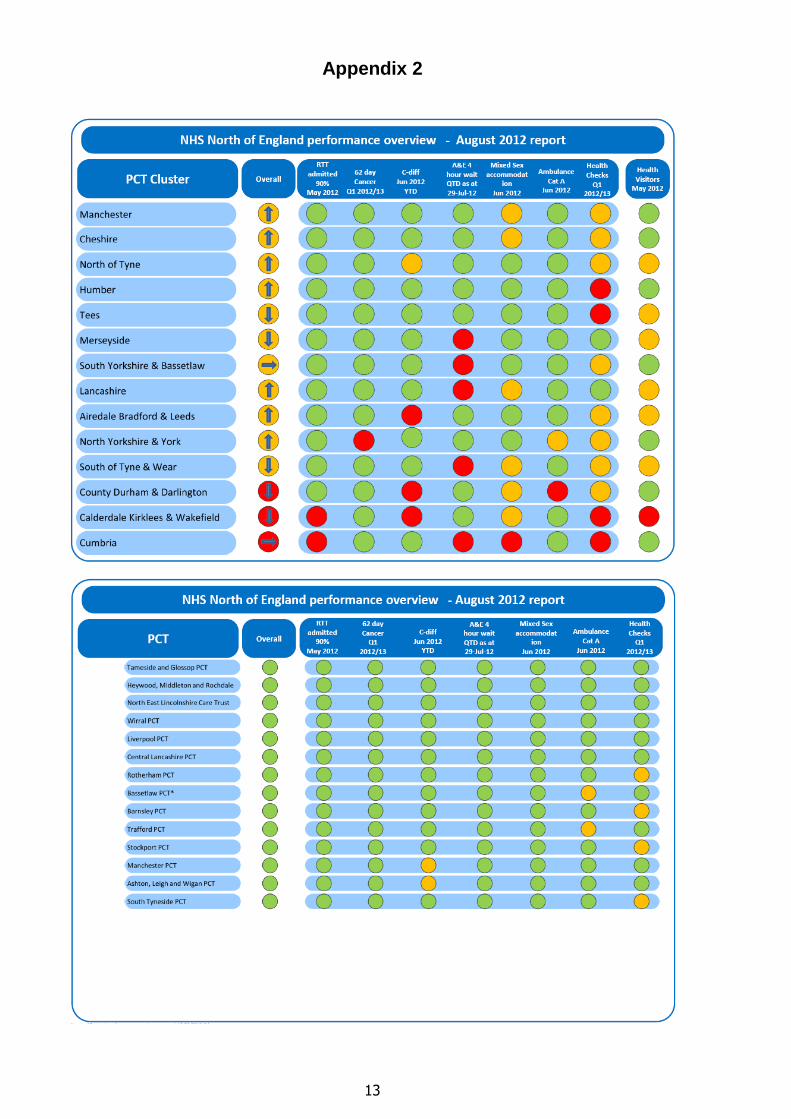
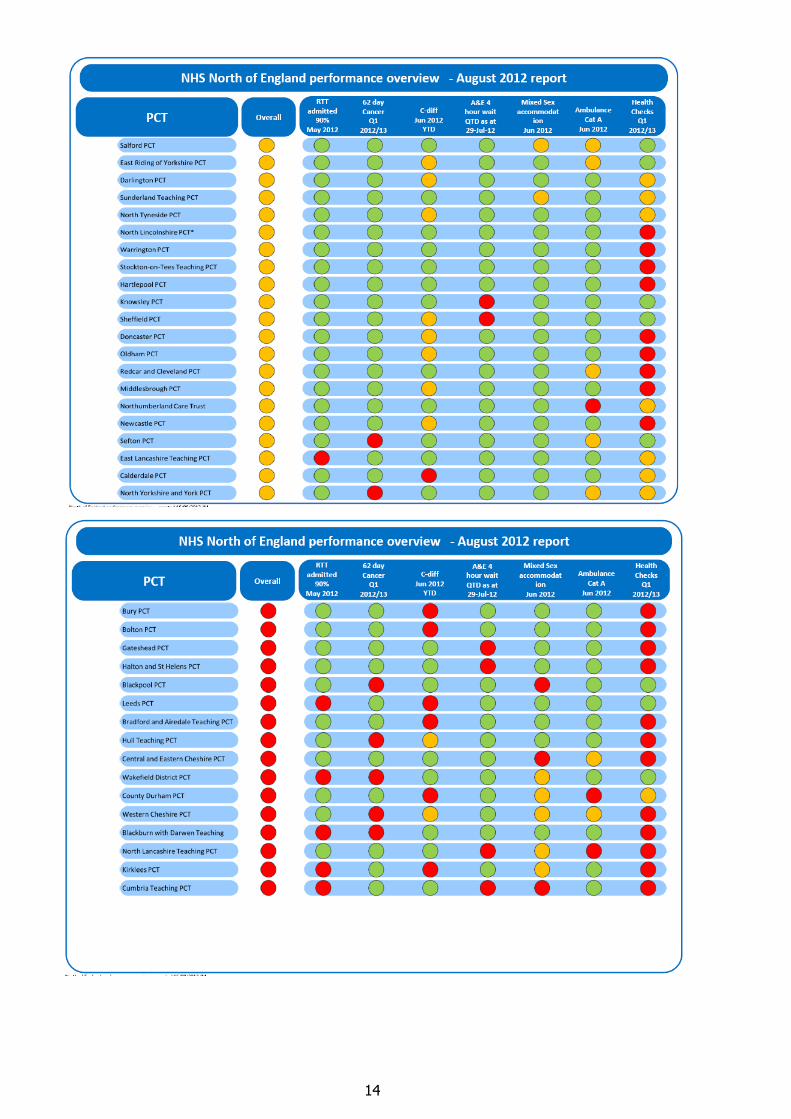
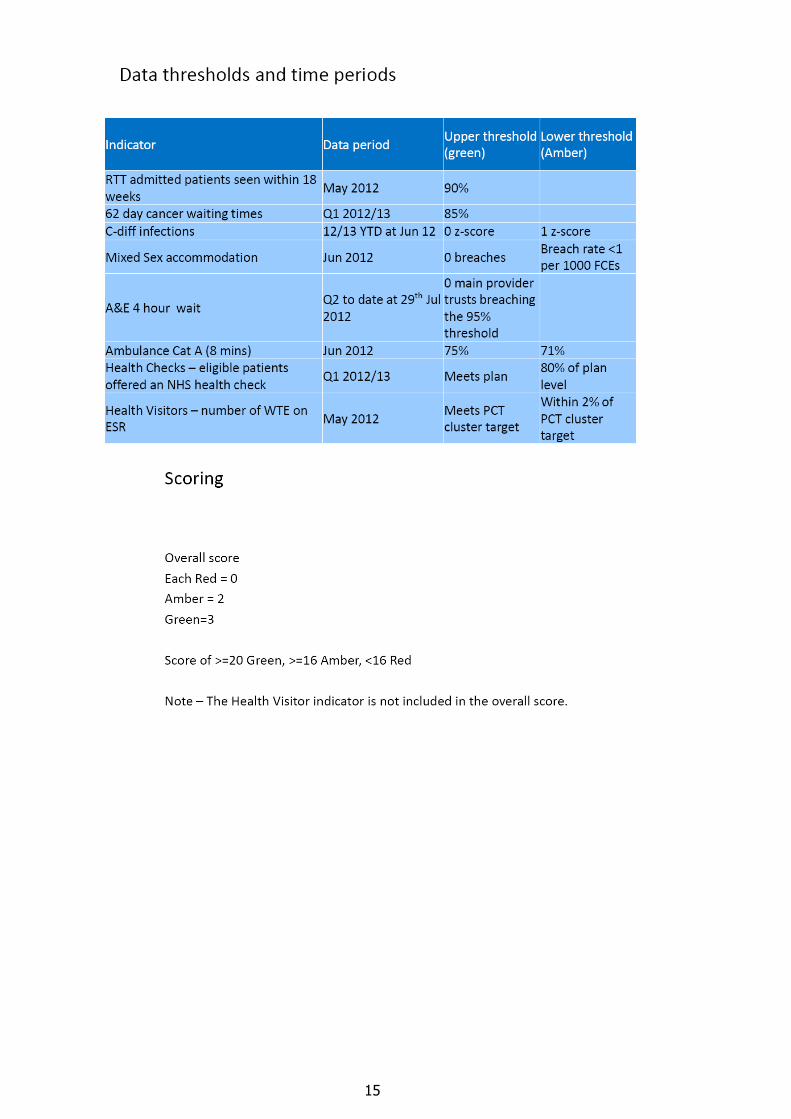
Appendix 2: NHS North of England scorecard
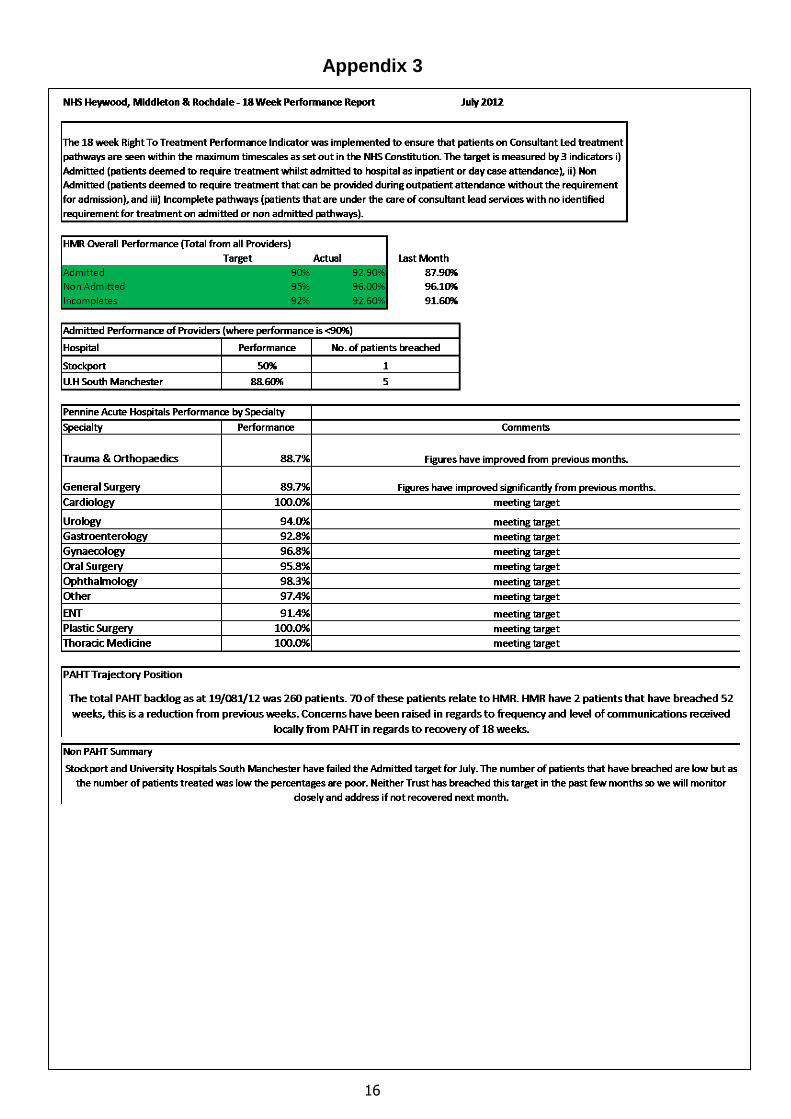
Appendix 3: RTT report
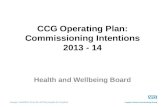
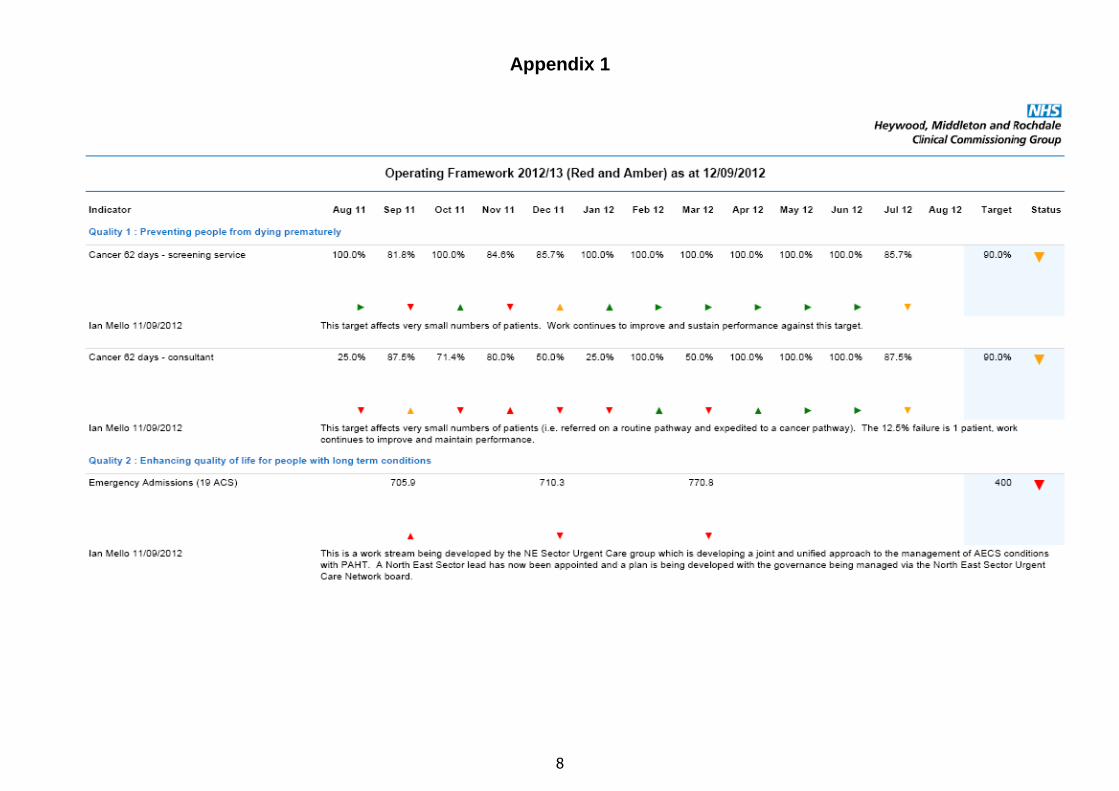
2.2 The Executive Summary against all Operating Framework targets is shown in
Figure 1 (see page 2). Key changes since last reported in July are improvements
in cancer performance which is now Green and Health Check performance
reducing to Amber. It should be noted that the Q1 2012/13 Health Checks
achieved 4.96% against a target of 5%. This equates to 23 health checks being
offered behind trajectory. NHS North of England (NoE) are reporting this
performance as Green in the NHS NoE Scorecard given in Appendix 2.
2.3 The NoE Scorecard (Appendix 2) shows significant improvement in NHS HMRs
performance. NHS HMR is rated as Green for all key performance areas, one of
only six NoE CCGs in this position.
2
Figure 1
Performance Report September 2012
3
Key performance areas:
2.4 Referral to Treatment Times
The Operating Framework for 2012/13 requires that RTT targets are monitored
and met at specialty level from April 2012. PAHT have continued to make
significant improvements in performance against this target.
Appendix 3 provides a summary of the performance as at July 2012 at both
aggregate and specialty level. Target is achieved at aggregate level (92.9%
against a target of 90%) and only two specialties are now failing – T&O (88.7%)
and General Surgery (89.7%). Agreement has been reached that delivery at
specialty level will be in place by 1 October 2012. There are robust systems in
place around each specialty. Early indications suggest RTT by specialty may be
achieved ahead of this date; however sustainability continues to be an issue and
RTT will continue to be closely monitored.
NHS HMR now has 70 patients in the backlog at PAHT, 2 of which have waited
longer than 52 weeks. This situation continues to improve and is being closely
monitored.
This target continues to carry significant risk and therefore is reviewed at the
weekly Executive Performance meeting. In addition a joint operational meeting is
held bi-weekly between PAHT and NES CCGs.
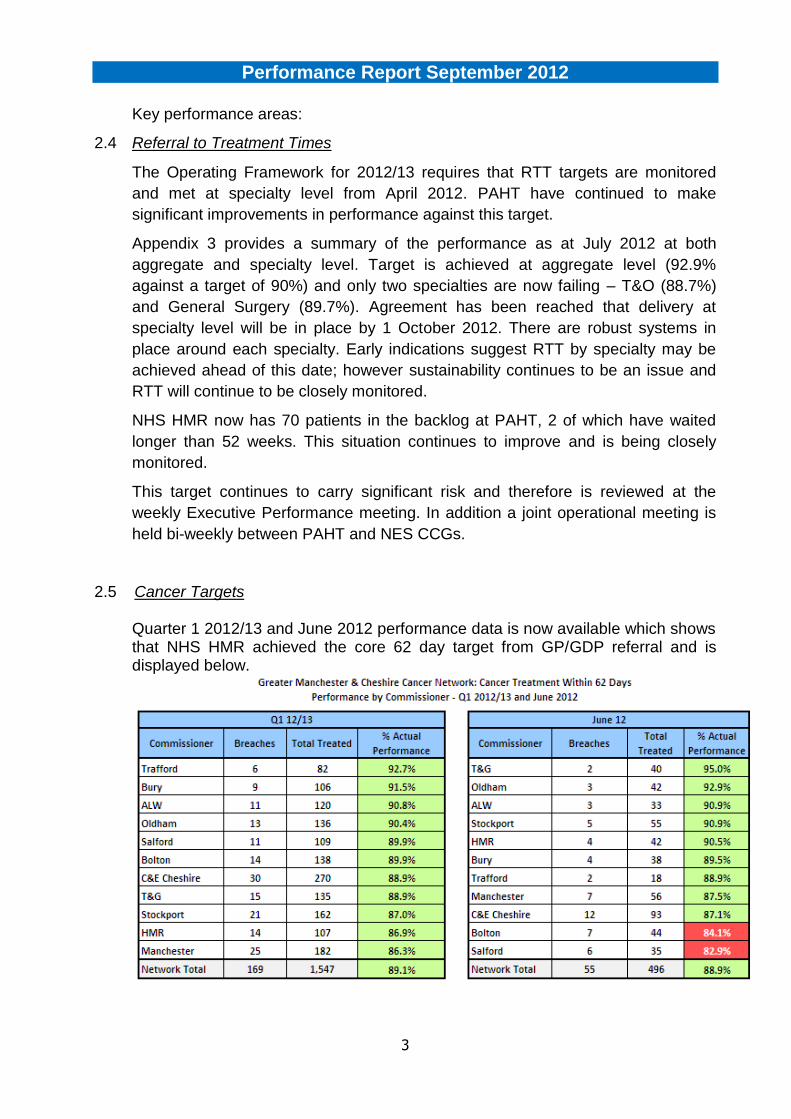
2.5 Cancer Targets
Quarter 1 2012/13 and June 2012 performance data is now available which shows that NHS HMR achieved the core 62 day target from GP/GDP referral and is displayed below.
Performance Report September 2012
4
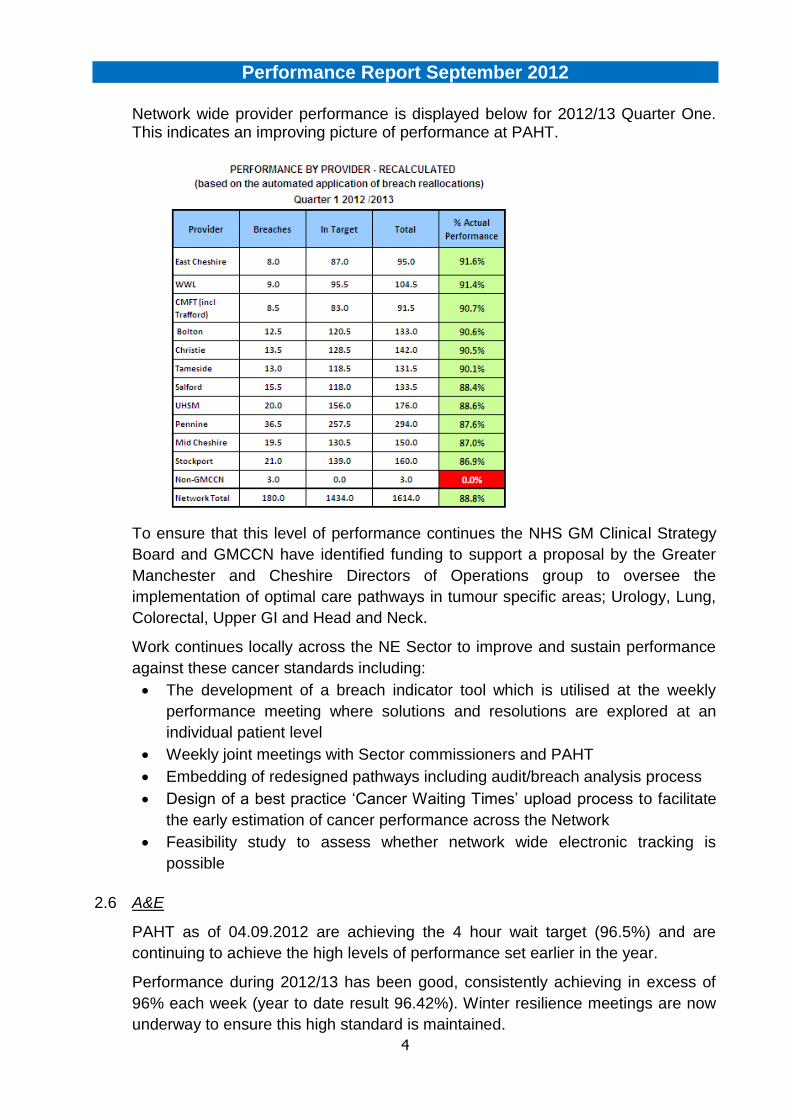
Network wide provider performance is displayed below for 2012/13 Quarter One. This indicates an improving picture of performance at PAHT.
To ensure that this level of performance continues the NHS GM Clinical Strategy
Board and GMCCN have identified funding to support a proposal by the Greater
Manchester and Cheshire Directors of Operations group to oversee the
implementation of optimal care pathways in tumour specific areas; Urology, Lung,
Colorectal, Upper GI and Head and Neck.
Work continues locally across the NE Sector to improve and sustain performance
against these cancer standards including:
The development of a breach indicator tool which is utilised at the weekly
performance meeting where solutions and resolutions are explored at an
individual patient level
Weekly joint meetings with Sector commissioners and PAHT
Embedding of redesigned pathways including audit/breach analysis process
Design of a best practice „Cancer Waiting Times‟ upload process to facilitate
the early estimation of cancer performance across the Network
Feasibility study to assess whether network wide electronic tracking is
possible
2.6 A&E
PAHT as of 04.09.2012 are achieving the 4 hour wait target (96.5%) and are
continuing to achieve the high levels of performance set earlier in the year.
Performance during 2012/13 has been good, consistently achieving in excess of
96% each week (year to date result 96.42%). Winter resilience meetings are now
underway to ensure this high standard is maintained.
Performance Report September 2012
5
2.7 CAT A 8 and 19 Minute Ambulance
NWAS has achieved both the 8 and 19 minute performance target for July 2012.
8 min (July 2012) 19 min (July 2012)
HMR 78.70% 94.62%
GM 77.24% 94.87%
Northwest 77.94% 95.11%
At local level NHS HMR achieved the 8 minute target but under performed against
the 19 minute target. It is worth noting however that 94.62% is a significant
improvement against May‟s performance of 92.45%.
A GM Urgent Care transport group has been formed and had an initial meeting to
begin to have overview of both the local and GM Ambulance performance has
taken place with performance being a standing item on the agenda. These
meetings currently take place monthly and are led by NHS GM.
High turnaround times continue to have an adverse effect on NWAS‟ ability to
deliver the performance standard and are coming under increased scrutiny by
NHS North of England. Turnaround times are influenced by both NWAS and acute
providers, therefore reciprocal penalties on handover and turnaround were agreed
and supported by the SHA. The penalty clause is now included in both the NWAS
and acute contracts. There will be a phased approach to implementing the penalty
in 2012/13 to take account of Hospital Arrival Screens (HAS) being installed and
reporting systems being developed. Detailed reports on handover will be provided
to commissioners and acute trusts in Q1 and Q2 2012/13 with full implementation
of the penalty commencing in Q3.
NHS HMR met with NWAS and PAHT to discuss HAS screen compliance and
turnaround times and is assured at this point that the 2 trusts are working closely
to improve both compliance and turnaround time. PAHT are currently on track for
delivering 50% compliance by the end of Q2 and 95% compliance by end of
2012/13. NHS HMR will continue to attend the meetings and support the providers
where possible.
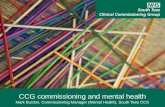
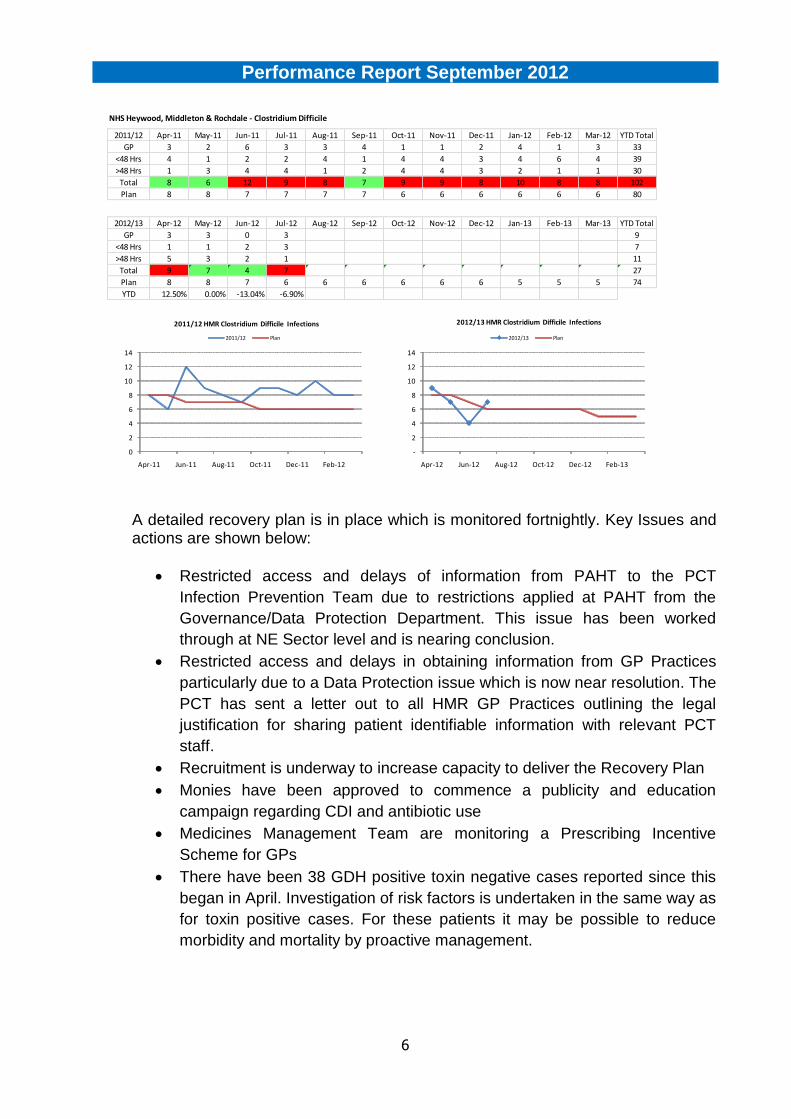
2.8 Clostridium Difficile
Current performance against trajectory places NHS HMR 2 cases under the year-
to-date plan.
There have been 8 cases of CDI in July; the eighth case has not yet been entered
correctly onto the national HCAI data collection system and therefore this has not
been incorporated into the table below. This means that the real position for NHS
HMR is 1 case under the year-to-date plan as of the end of July.
To date, only 1 case has been reported for the month of August. This data is
provisional.
Performance Report September 2012
6
A detailed recovery plan is in place which is monitored fortnightly. Key Issues and actions are shown below:
Restricted access and delays of information from PAHT to the PCT
Infection Prevention Team due to restrictions applied at PAHT from the
Governance/Data Protection Department. This issue has been worked
through at NE Sector level and is nearing conclusion.
Restricted access and delays in obtaining information from GP Practices
particularly due to a Data Protection issue which is now near resolution. The
PCT has sent a letter out to all HMR GP Practices outlining the legal
justification for sharing patient identifiable information with relevant PCT
staff.
Recruitment is underway to increase capacity to deliver the Recovery Plan
Monies have been approved to commence a publicity and education
campaign regarding CDI and antibiotic use
Medicines Management Team are monitoring a Prescribing Incentive
Scheme for GPs
There have been 38 GDH positive toxin negative cases reported since this
began in April. Investigation of risk factors is undertaken in the same way as
for toxin positive cases. For these patients it may be possible to reduce
morbidity and mortality by proactive management.
NHS Heywood, Middleton & Rochdale - Clostridium Difficile
2011/12 Apr-11 May-11 Jun-11 Jul-11 Aug-11 Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 YTD Total
GP 3 2 6 3 3 4 1 1 2 4 1 3 33
<48 Hrs 4 1 2 2 4 1 4 4 3 4 6 4 39
>48 Hrs 1 3 4 4 1 2 4 4 3 2 1 1 30
Total 8 6 12 9 8 7 9 9 8 10 8 8 102
Plan 8 8 7 7 7 7 6 6 6 6 6 6 80
2012/13 Apr-12 May-12 Jun-12 Jul-12 Aug-12 Sep-12 Oct-12 Nov-12 Dec-12 Jan-13 Feb-13 Mar-13 YTD Total
GP 3 3 0 3 9
<48 Hrs 1 1 2 3 7
>48 Hrs 5 3 2 1 11
Total 9 7 4 7 #N/A #N/A #N/A #N/A #N/A #N/A #N/A #N/A 27
Plan 8 8 7 6 6 6 6 6 6 5 5 5 74
YTD 12.50% 0.00% -13.04% -6.90%
0
2
4
6
8
10
12
14
Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Feb-12
2011/12 HMR Clostridium Difficile Infections
2011/12 Plan
-
2
4
6
8
10
12
14
Apr-12 Jun-12 Aug-12 Oct-12 Dec-12 Feb-13
2012/13 HMR Clostridium Difficile Infections
2012/13 Plan
Performance Report September 2012
7
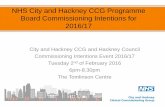
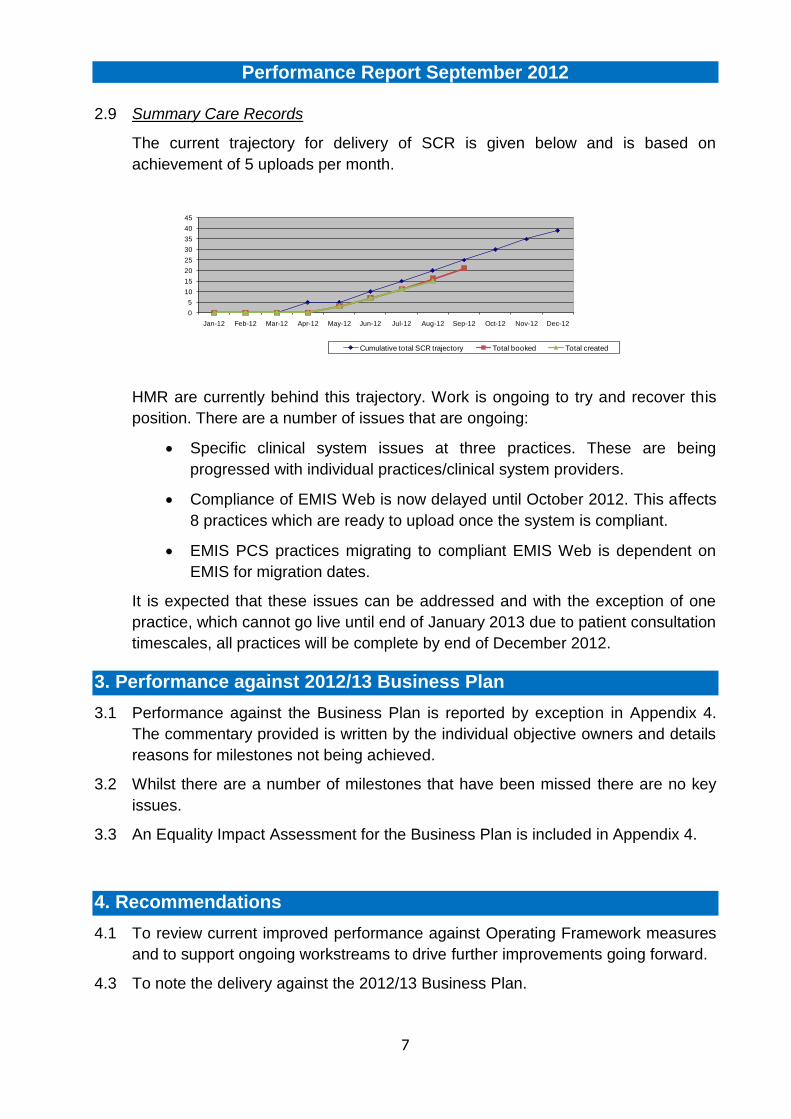
2.9 Summary Care Records
The current trajectory for delivery of SCR is given below and is based on
achievement of 5 uploads per month.
HMR are currently behind this trajectory. Work is ongoing to try and recover this
position. There are a number of issues that are ongoing:
Specific clinical system issues at three practices. These are being
progressed with individual practices/clinical system providers.
Compliance of EMIS Web is now delayed until October 2012. This affects
8 practices which are ready to upload once the system is compliant.
EMIS PCS practices migrating to compliant EMIS Web is dependent on
EMIS for migration dates.
It is expected that these issues can be addressed and with the exception of one
practice, which cannot go live until end of January 2013 due to patient consultation
timescales, all practices will be complete by end of December 2012.
3. Performance against 2012/13 Business Plan
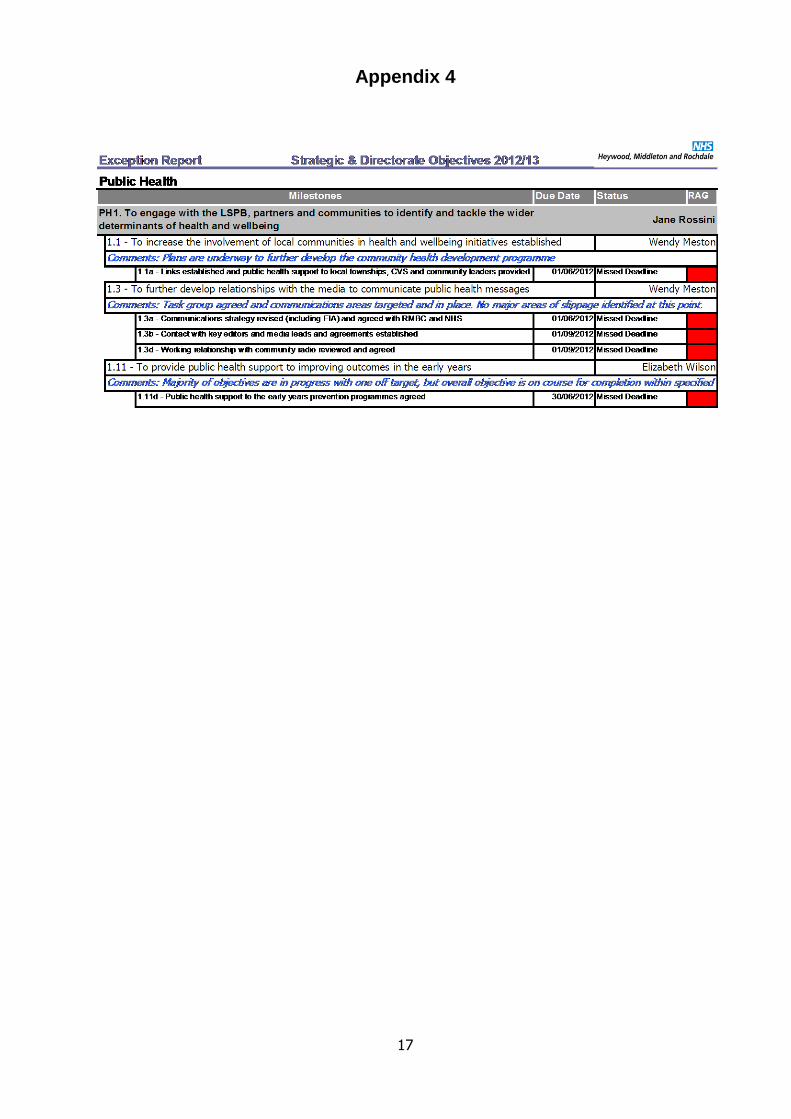
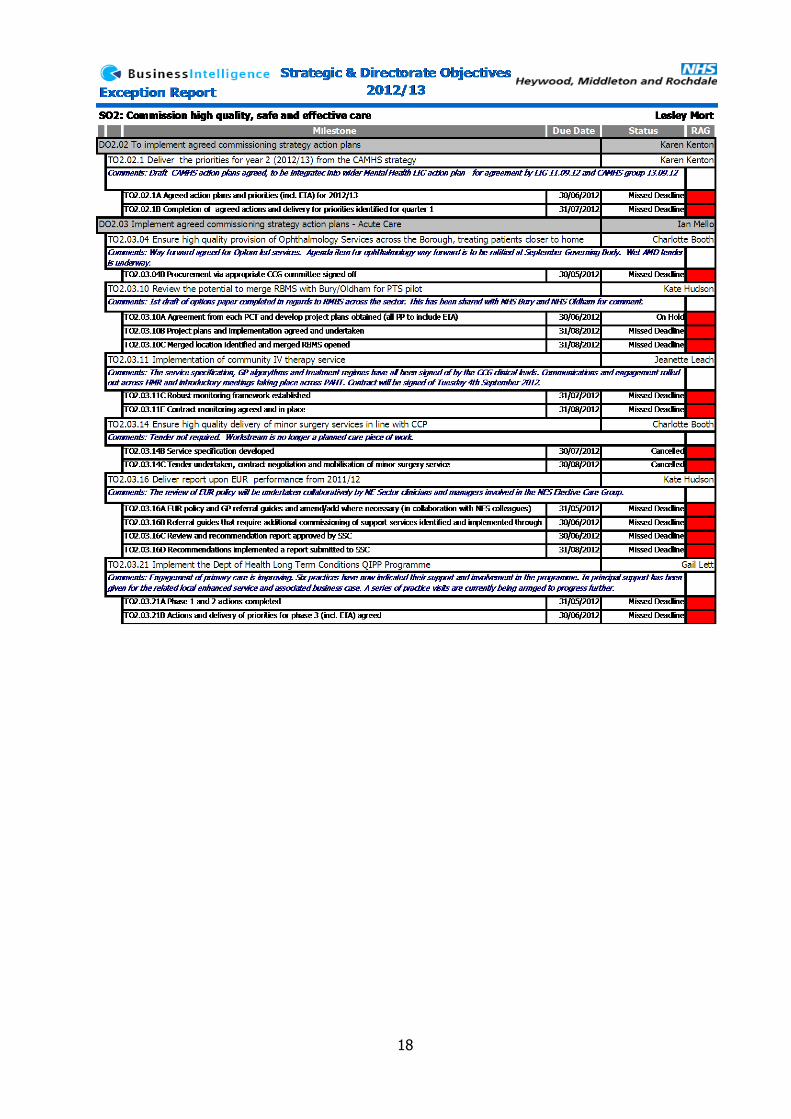
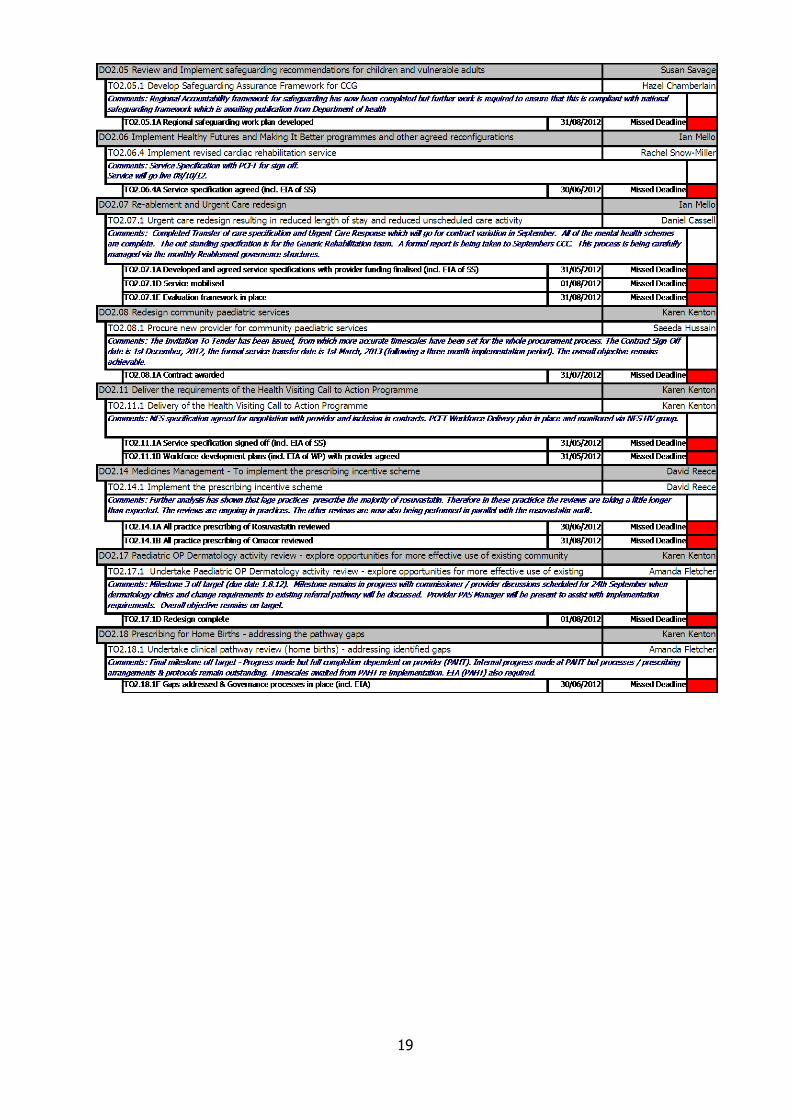
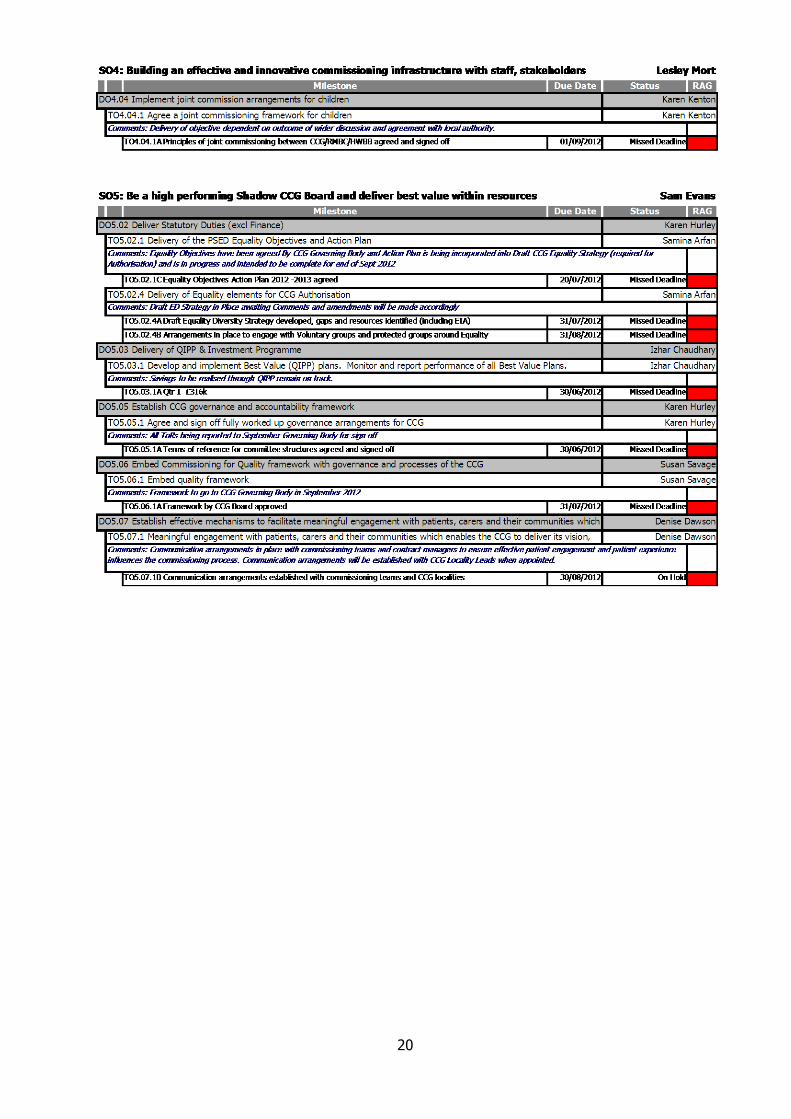
3.1 Performance against the Business Plan is reported by exception in Appendix 4.
The commentary provided is written by the individual objective owners and details
reasons for milestones not being achieved.
3.2 Whilst there are a number of milestones that have been missed there are no key
issues.
3.3 An Equality Impact Assessment for the Business Plan is included in Appendix 4.
4. Recommendations
4.1 To review current improved performance against Operating Framework measures
and to support ongoing workstreams to drive further improvements going forward.
4.3 To note the delivery against the 2012/13 Business Plan.
0
5
10
15
20
25
30
35
40
45
Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-12 Sep-12 Oct-12 Nov-12 Dec-12
Cumulative total SCR trajectory Total booked Total created
8
Appendix 1
9
10
11
12
13
Appendix 2
14
15
16
Appendix 3
17
Appendix 4
18
19
20
21
Appendix 5
Equality Impact Assessment Template & Human
Rights Screening
March 2011
22
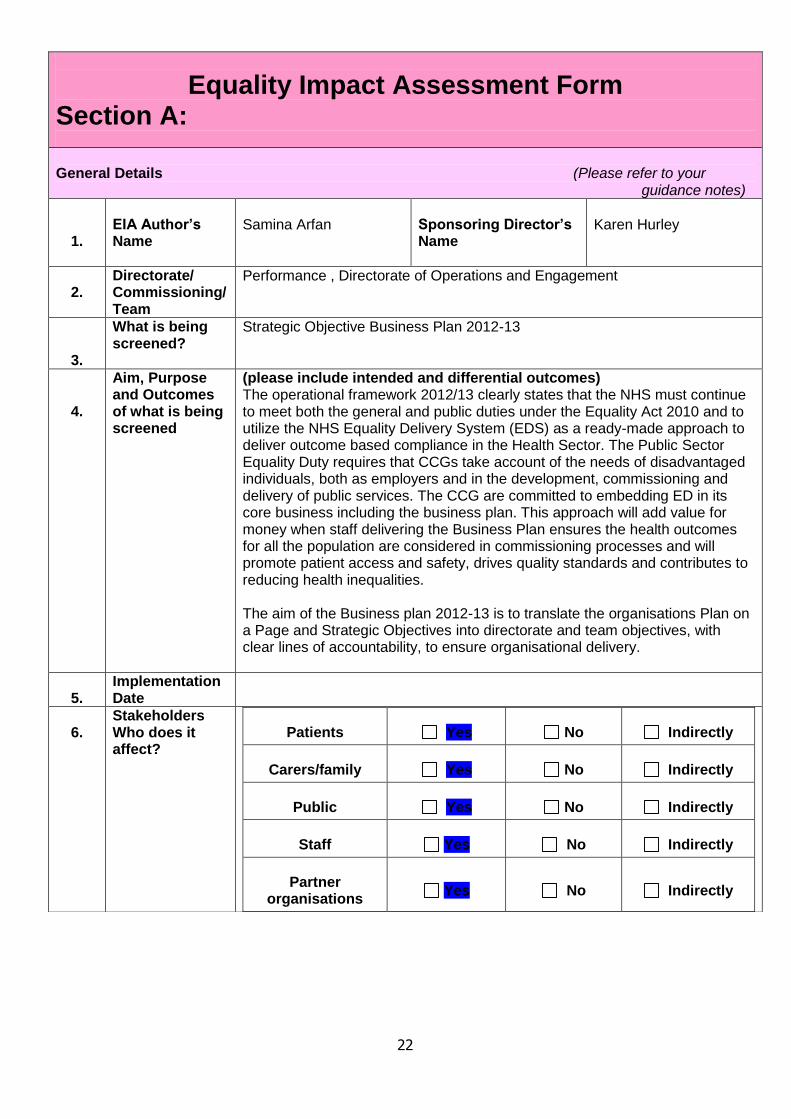
Equality Impact Assessment Form Section A:
General Details (Please refer to your guidance notes)
1.
EIA Author’s Name
Samina Arfan
Sponsoring Director’s Name
Karen Hurley
2.
Directorate/ Commissioning/ Team
Performance , Directorate of Operations and Engagement
3.
What is being screened?
Strategic Objective Business Plan 2012-13
4.
Aim, Purpose and Outcomes of what is being screened
(please include intended and differential outcomes) The operational framework 2012/13 clearly states that the NHS must continue to meet both the general and public duties under the Equality Act 2010 and to utilize the NHS Equality Delivery System (EDS) as a ready-made approach to deliver outcome based compliance in the Health Sector. The Public Sector Equality Duty requires that CCGs take account of the needs of disadvantaged individuals, both as employers and in the development, commissioning and delivery of public services. The CCG are committed to embedding ED in its core business including the business plan. This approach will add value for money when staff delivering the Business Plan ensures the health outcomes for all the population are considered in commissioning processes and will promote patient access and safety, drives quality standards and contributes to reducing health inequalities. The aim of the Business plan 2012-13 is to translate the organisations Plan on a Page and Strategic Objectives into directorate and team objectives, with clear lines of accountability, to ensure organisational delivery.
5.
Implementation Date
6.
Stakeholders Who does it affect?
Patients Yes No Indirectly
Carers/family Yes No Indirectly
Public Yes No Indirectly
Staff Yes No Indirectly
Partner organisations
Yes No Indirectly
23
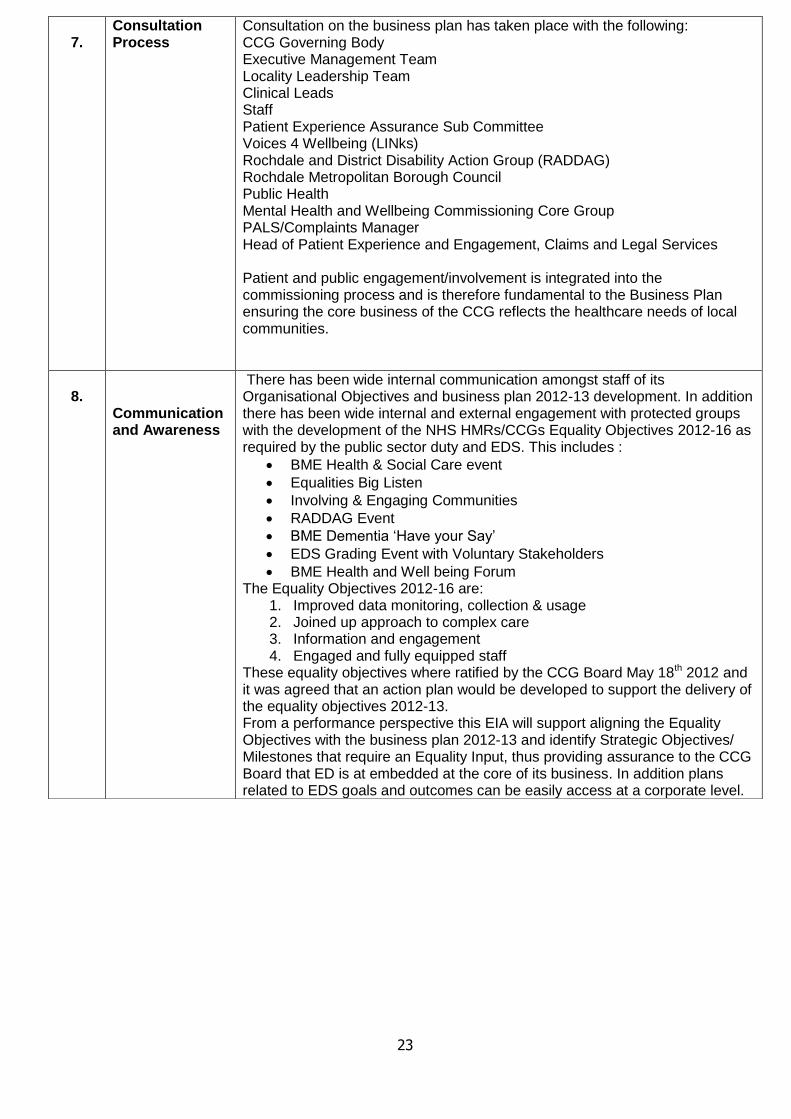
7.
Consultation Process
Consultation on the business plan has taken place with the following: CCG Governing Body Executive Management Team Locality Leadership Team Clinical Leads Staff Patient Experience Assurance Sub Committee Voices 4 Wellbeing (LINks) Rochdale and District Disability Action Group (RADDAG) Rochdale Metropolitan Borough Council Public Health Mental Health and Wellbeing Commissioning Core Group PALS/Complaints Manager Head of Patient Experience and Engagement, Claims and Legal Services Patient and public engagement/involvement is integrated into the commissioning process and is therefore fundamental to the Business Plan ensuring the core business of the CCG reflects the healthcare needs of local communities.
8.
Communication and Awareness
There has been wide internal communication amongst staff of its Organisational Objectives and business plan 2012-13 development. In addition there has been wide internal and external engagement with protected groups with the development of the NHS HMRs/CCGs Equality Objectives 2012-16 as required by the public sector duty and EDS. This includes :
BME Health & Social Care event
Equalities Big Listen
Involving & Engaging Communities
RADDAG Event
BME Dementia „Have your Say‟
EDS Grading Event with Voluntary Stakeholders
BME Health and Well being Forum The Equality Objectives 2012-16 are:
1. Improved data monitoring, collection & usage 2. Joined up approach to complex care 3. Information and engagement 4. Engaged and fully equipped staff
These equality objectives where ratified by the CCG Board May 18th 2012 and it was agreed that an action plan would be developed to support the delivery of the equality objectives 2012-13. From a performance perspective this EIA will support aligning the Equality Objectives with the business plan 2012-13 and identify Strategic Objectives/ Milestones that require an Equality Input, thus providing assurance to the CCG Board that ED is at embedded at the core of its business. In addition plans related to EDS goals and outcomes can be easily access at a corporate level.
24
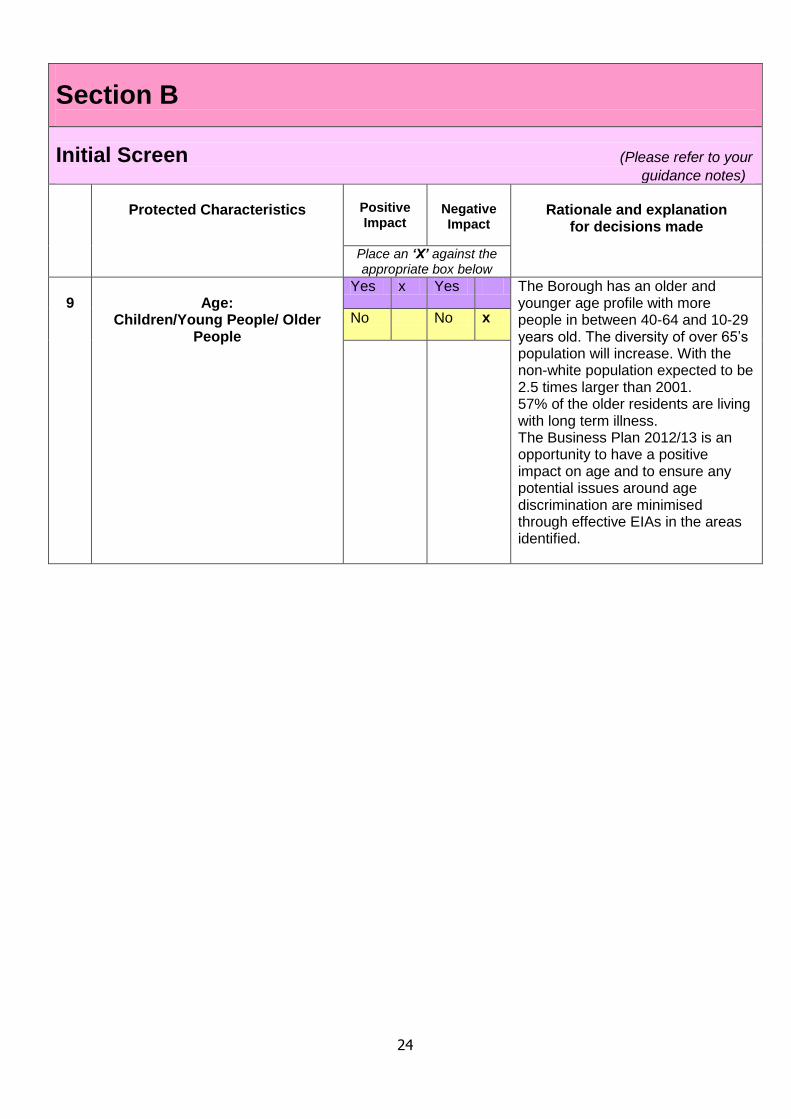
Section B
Initial Screen (Please refer to your
guidance notes)
Protected Characteristics
Positive Impact
Negative Impact
Rationale and explanation
for decisions made
Place an ‘X’ against the appropriate box below
9
Age:
Children/Young People/ Older People
Yes x Yes The Borough has an older and younger age profile with more people in between 40-64 and 10-29 years old. The diversity of over 65‟s population will increase. With the non-white population expected to be 2.5 times larger than 2001. 57% of the older residents are living with long term illness. The Business Plan 2012/13 is an opportunity to have a positive impact on age and to ensure any potential issues around age discrimination are minimised through effective EIAs in the areas identified.
No No x
25
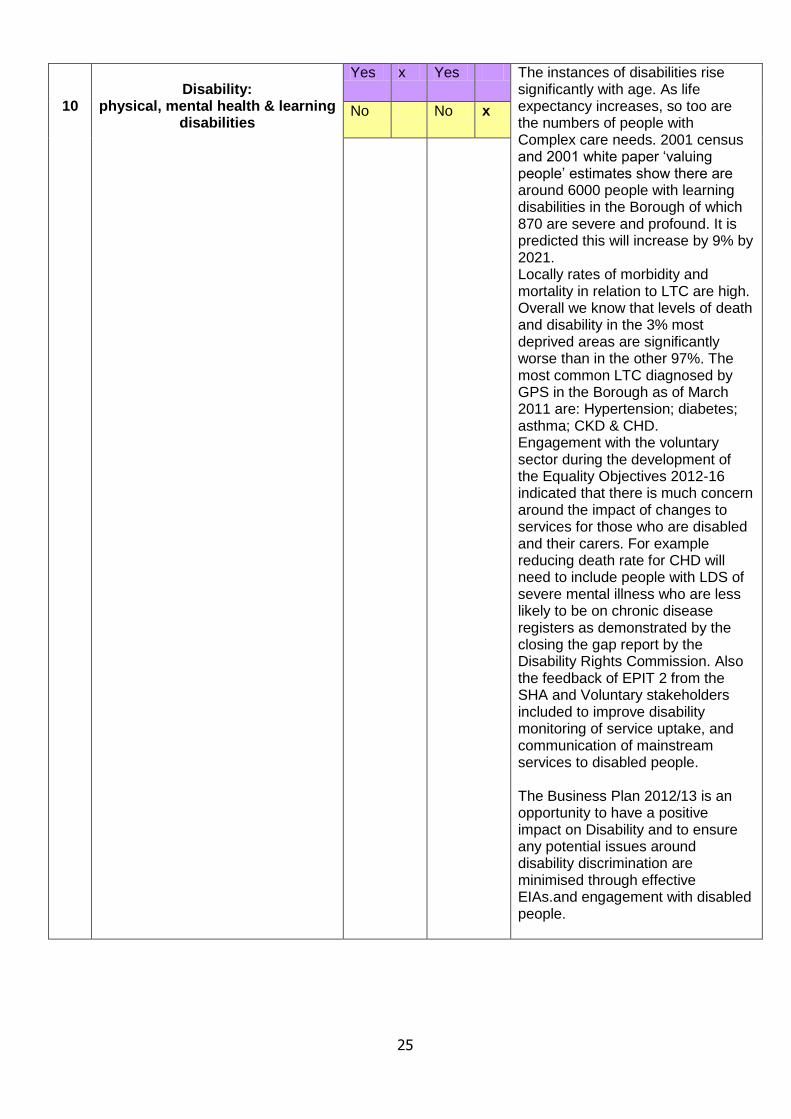
10
Disability:
physical, mental health & learning disabilities
Yes x Yes The instances of disabilities rise significantly with age. As life expectancy increases, so too are the numbers of people with Complex care needs. 2001 census and 2001 white paper „valuing people‟ estimates show there are around 6000 people with learning disabilities in the Borough of which 870 are severe and profound. It is predicted this will increase by 9% by 2021. Locally rates of morbidity and mortality in relation to LTC are high. Overall we know that levels of death and disability in the 3% most deprived areas are significantly worse than in the other 97%. The most common LTC diagnosed by GPS in the Borough as of March 2011 are: Hypertension; diabetes; asthma; CKD & CHD. Engagement with the voluntary sector during the development of the Equality Objectives 2012-16 indicated that there is much concern around the impact of changes to services for those who are disabled and their carers. For example reducing death rate for CHD will need to include people with LDS of severe mental illness who are less likely to be on chronic disease registers as demonstrated by the closing the gap report by the Disability Rights Commission. Also the feedback of EPIT 2 from the SHA and Voluntary stakeholders included to improve disability monitoring of service uptake, and communication of mainstream services to disabled people. The Business Plan 2012/13 is an opportunity to have a positive impact on Disability and to ensure any potential issues around disability discrimination are minimised through effective EIAs.and engagement with disabled people.
No No x
26
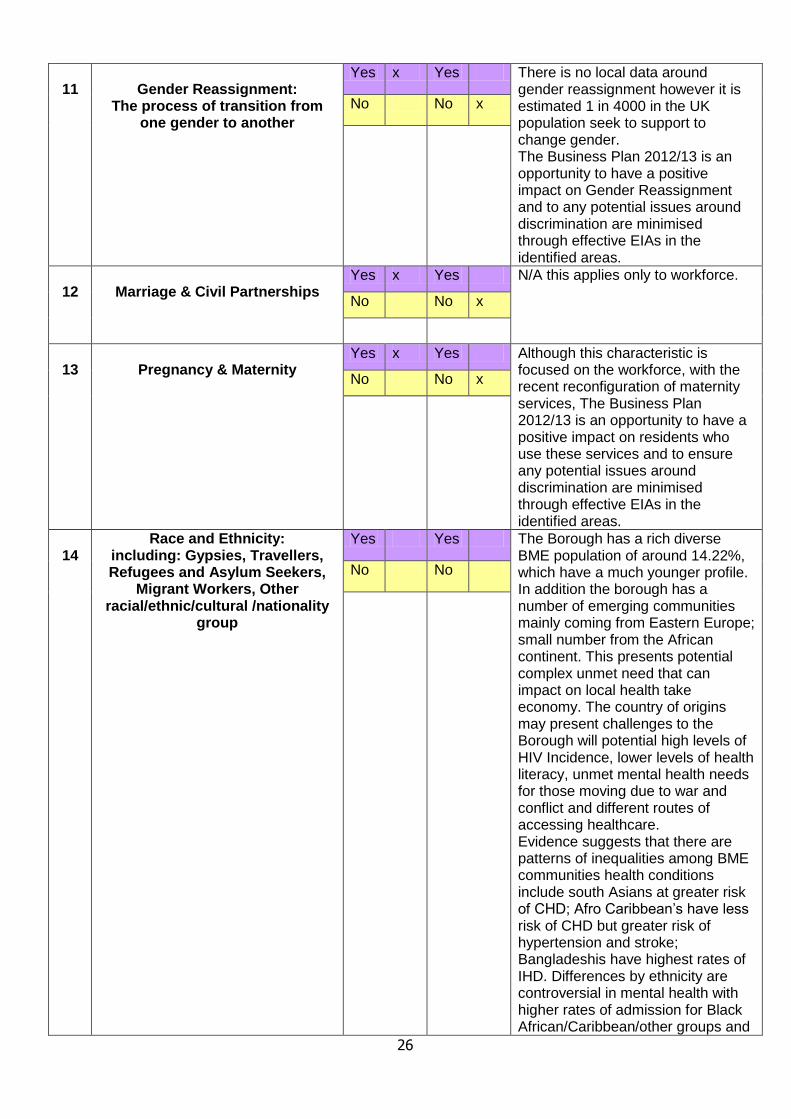
11
Gender Reassignment:
The process of transition from one gender to another
Yes x Yes There is no local data around gender reassignment however it is estimated 1 in 4000 in the UK population seek to support to change gender. The Business Plan 2012/13 is an opportunity to have a positive impact on Gender Reassignment and to any potential issues around discrimination are minimised through effective EIAs in the identified areas.
No No x
12
Marriage & Civil Partnerships
Yes x Yes N/A this applies only to workforce.
No No x
13
Pregnancy & Maternity
Yes x Yes Although this characteristic is focused on the workforce, with the recent reconfiguration of maternity services, The Business Plan 2012/13 is an opportunity to have a positive impact on residents who use these services and to ensure any potential issues around discrimination are minimised through effective EIAs in the identified areas.
No No x
14
Race and Ethnicity: including: Gypsies, Travellers, Refugees and Asylum Seekers,
Migrant Workers, Other racial/ethnic/cultural /nationality
group
Yes Yes The Borough has a rich diverse BME population of around 14.22%, which have a much younger profile. In addition the borough has a number of emerging communities mainly coming from Eastern Europe; small number from the African continent. This presents potential complex unmet need that can impact on local health take economy. The country of origins may present challenges to the Borough will potential high levels of HIV Incidence, lower levels of health literacy, unmet mental health needs for those moving due to war and conflict and different routes of accessing healthcare. Evidence suggests that there are patterns of inequalities among BME communities health conditions include south Asians at greater risk of CHD; Afro Caribbean‟s have less risk of CHD but greater risk of hypertension and stroke; Bangladeshis have highest rates of IHD. Differences by ethnicity are controversial in mental health with higher rates of admission for Black African/Caribbean/other groups and
No No

27
more likely to enter psychiatric care through the criminal justice system. The Government review „No patient left behind‟ 2008, showed a widespread dissatisfaction with Access to GP services and made recommendations for improvements. BME engagement during the equality objective development indicated that ethnicity monitoring needs to improve to be able to demonstrate that BME communities are equitably access services and that future needs can be met. In addition better communication about how they can improve their health. The Business Plan 2012/13 is an opportunity to have a positive impact on Race and to ensure any potential issues around Race discrimination are minimised through effective EIAs in the identified areas.
15
Religion and Belief - Faith Groups
Yes x Yes Most people in the Borough follow a religion, around 75% are Christian, around 10% are Muslim and around 7% state they have no religion. The Muslim population reports poor health in line with the national picture. The Business Plan 2012/13 is an opportunity to have a positive impact on Religion and belief and to ensure any potential issues around religious/belief discrimination are minimised through effective EIAs.
No No x
16
Sex:
Man/Woman
Yes x Yes The Borough has estimated 50.6% female and 49.4 % male population. On average men and women in the Borough live shorter lives that in the NW. The JSNA shows that the biggest killers for men are CHD, respiratory disease and digestive disease including cirrhosis; for women it is CHD, digestive disease including cirrhosis and lung cancer, it is understood that better treatment, earlier detection and risk management, prevention will positively impact on these outcomes. Such intervention will need to also consider barriers because of cross cutting issues such as age, race, and disability. The Business Plan 2012/13 is an opportunity to have a positive impact on gender and to ensure any
No No x
28
potential issues around gender discrimination and cross cutting issues are minimised through effective EIAs.
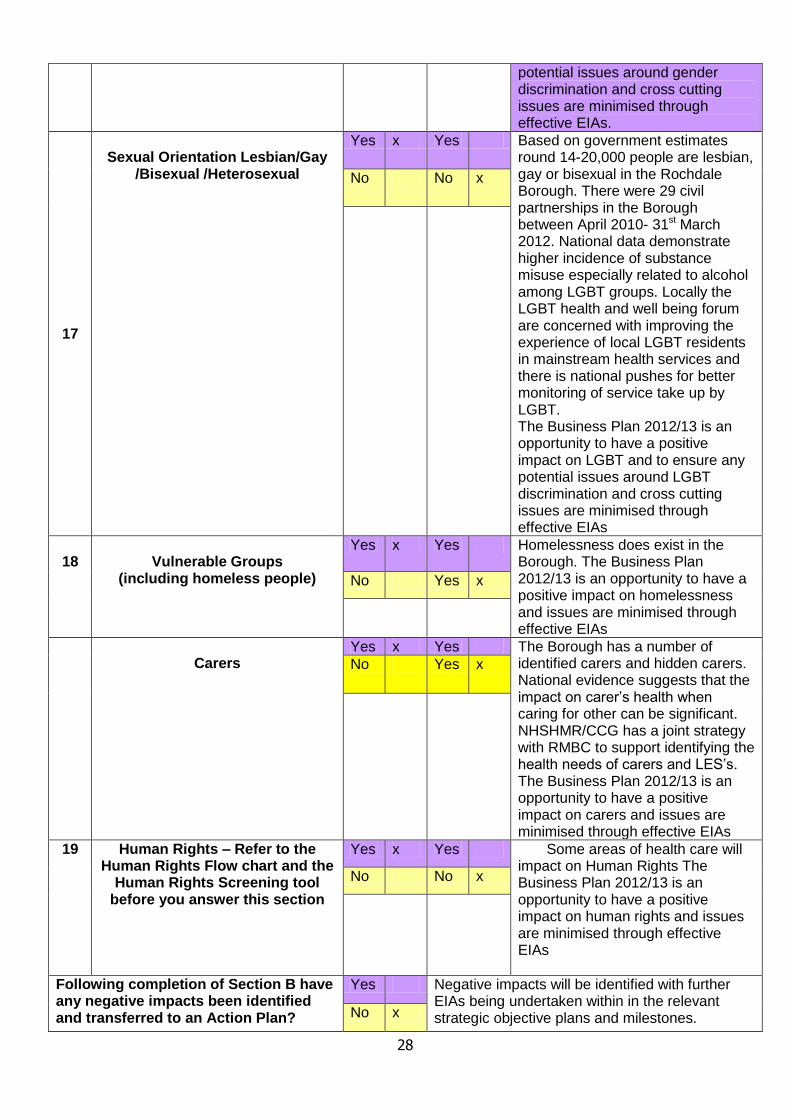
17
Sexual Orientation Lesbian/Gay
/Bisexual /Heterosexual
Yes x Yes Based on government estimates round 14-20,000 people are lesbian, gay or bisexual in the Rochdale Borough. There were 29 civil partnerships in the Borough between April 2010- 31st March 2012. National data demonstrate higher incidence of substance misuse especially related to alcohol among LGBT groups. Locally the LGBT health and well being forum are concerned with improving the experience of local LGBT residents in mainstream health services and there is national pushes for better monitoring of service take up by LGBT. The Business Plan 2012/13 is an opportunity to have a positive impact on LGBT and to ensure any potential issues around LGBT discrimination and cross cutting issues are minimised through effective EIAs
No No x
18
Vulnerable Groups
(including homeless people)
Yes x Yes Homelessness does exist in the Borough. The Business Plan 2012/13 is an opportunity to have a positive impact on homelessness and issues are minimised through effective EIAs
No Yes x
Carers
Yes x Yes The Borough has a number of identified carers and hidden carers. National evidence suggests that the impact on carer‟s health when caring for other can be significant. NHSHMR/CCG has a joint strategy with RMBC to support identifying the health needs of carers and LES‟s. The Business Plan 2012/13 is an opportunity to have a positive impact on carers and issues are minimised through effective EIAs
No Yes x
19 Human Rights – Refer to the Human Rights Flow chart and the
Human Rights Screening tool before you answer this section
Yes x Yes Some areas of health care will impact on Human Rights The Business Plan 2012/13 is an opportunity to have a positive impact on human rights and issues are minimised through effective EIAs
No No x
Following completion of Section B have any negative impacts been identified and transferred to an Action Plan?
Yes Negative impacts will be identified with further EIAs being undertaken within in the relevant strategic objective plans and milestones. No x

29
Date Completed: 28th June 2012 Signature of person completing EIA and Human Rights Screen: Sandra Croasdale
Please send a copy of all completed Sections A & B and any supporting evidence and/or policy to the ED Program Manager for scrutiny and audit purposes
Date received by ED: 28 June 2012
Signature of Senior manager or Commission lead or Executive Director: Karen Hurley
EIA Action Plan
Insert question numbers highlighted Red/ Amber below
State what actions are required to reduce any negative/ adverse impacts on Protected
Characteristics: By whom By when
Please state any
implications on resources
1 The work areas within the Business plan 2012-13 have been highlighted where further EIAs or equality considerations are required. These areas need to be incorporated as part of the performance reporting systems within the organisations
CCG to agree
July Board meeting
2 Identified staff responsible to deliver the business plan milestones, where an EIA /equality consideration has been highlighted, are required ensure they report through performance manager the progress of the EIA, and to seek support from the Equality lead if required.
Identified action Plan leads
Dates identified within the business plan
Upon undertaking an EIA it may be identified that support measures may need to be included to ensure potential challenge is avoided and that due regard is given to protected groups. For example communication plan for a service redesign and or decommission
3 EIAs are not a tick box exercise but a tool to improve health outcomes, quality, access and experience of users from protected groups, EIA action plans need to be adequately completed and forwarded to the equality lead for quality assurance and or for further support.
Identified action Plan leads
Dates identified within the business plan
30
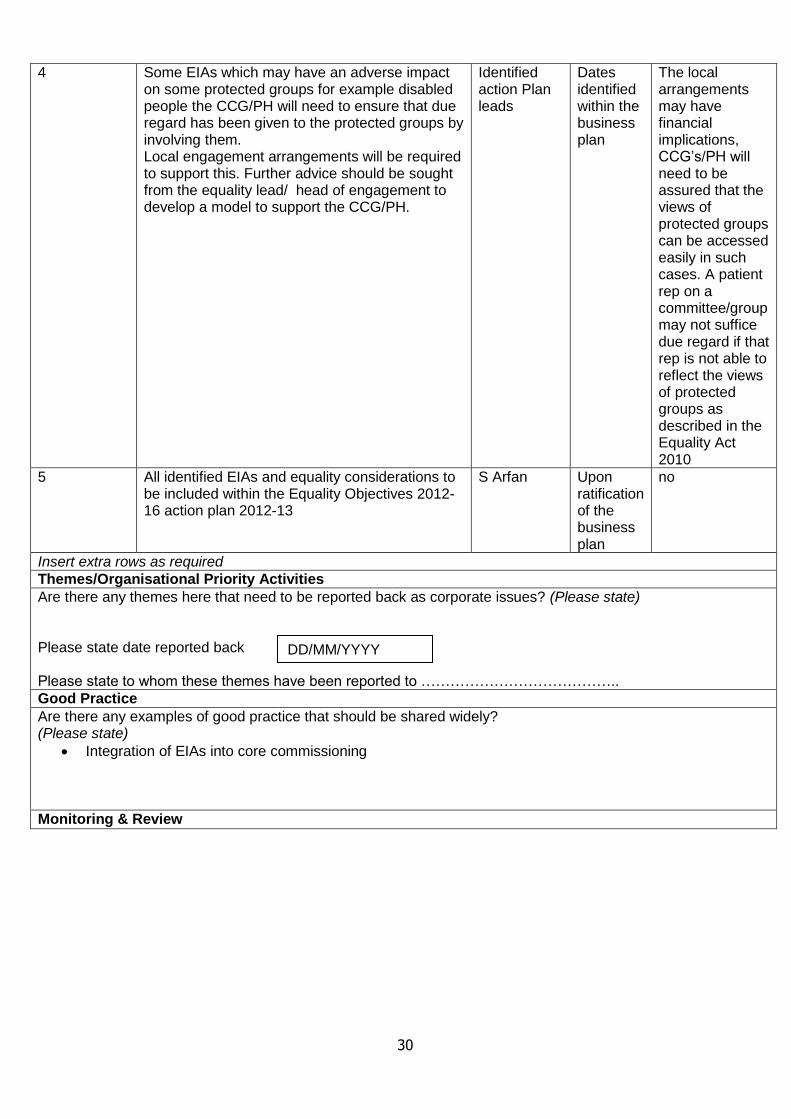
4 Some EIAs which may have an adverse impact on some protected groups for example disabled people the CCG/PH will need to ensure that due regard has been given to the protected groups by involving them. Local engagement arrangements will be required to support this. Further advice should be sought from the equality lead/ head of engagement to develop a model to support the CCG/PH.
Identified action Plan leads
Dates identified within the business plan
The local arrangements may have financial implications, CCG‟s/PH will need to be assured that the views of protected groups can be accessed easily in such cases. A patient rep on a committee/group may not suffice due regard if that rep is not able to reflect the views of protected groups as described in the Equality Act 2010
5 All identified EIAs and equality considerations to be included within the Equality Objectives 2012-16 action plan 2012-13
S Arfan Upon ratification of the business plan
no
Insert extra rows as required
Themes/Organisational Priority Activities
Are there any themes here that need to be reported back as corporate issues? (Please state) Please state date reported back Please state to whom these themes have been reported to …………………………………..
Good Practice
Are there any examples of good practice that should be shared widely? (Please state)
Integration of EIAs into core commissioning
Monitoring & Review
DD/MM/YYYY
31
(a) How will the implementation (proposed) and delivery (existing) of the service be monitored? Through performance indicators and patient experience evaluation/provider service evaluation
The implementation will be monitored by performance manager system and the mitigation action plans of the EIAs will be monitored by the Equality Assurance Committee. Identified leads will monitor the impact of any mitigation
plans they put in place.
Final Sign of by Commissioning Lead or Ex Director Karen Hurley
Date Equality Impact Assessment started: March 2012
Date completed: 28 June 2012
Summary of outcome of Impact Assessment Adverse effect not found [ x ] Please ‘X’ adverse impact can only be mitigated with further EIAs undertaken as identified within the Business Plan Adverse effect found [ ] Please indicate with a ‘X’ Are the proposed changes adequate to mitigate any adverse effects?
Date due for review: April 2013
Type of review: Full EIA/Action Plan only Action plan review
Person responsible for arranging review: Samina Arfan
Date: 28 June 2012
Initials: SC
Yes
Yes