Cirrose hepática - FactorChave€¦ · refractory ascites, baseline serum albumin level, type of...
42
Cirrose hepática SOFIA CARVALHANA, LEOPOLDO MATOS
Transcript of Cirrose hepática - FactorChave€¦ · refractory ascites, baseline serum albumin level, type of...

Cirrose hepática
S O F I A C A R VA L H A N A , L E O P O L D O M ATO S

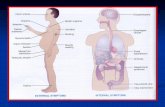
Ascite
• Definição: acúmulo de líquido livre na cavidade peritoneal
Causas de asciteGastrenterológica- HTPortal: cirrose hepática (85%), hepatite fulminante, doença veno-oclusiva,
hepatite alcoólica- Pancreatite, pseudoquisto
Cardíaca: ICC, pericardite constritiva, cor pulmonale
Infecciosa: tuberculose, schistossomíase
Neoplasia: Metástase peritoneal, mesotelioma, linfoma, pseudomixoma peritoneal
Quilosa: Obstrução linfática mesentéricas
Ginecológica: Síndrome de Meigss, endometriose
Outras: Lúpus eritematoso sistêmico, artrite reumatóide, mixedema,hipoalbuminemia

Ascite e cirrose
• 50% dos doentes com cirrosecompensada irão desenvolver asciteem 10 anos
• Complicação + frequente que leva aointernamento
• 15% morre 1ro ano e 45% aos 5 anos
Schrier et al

Ascite
• Avaliação inicial:
1. História clínica e exame objetivo
2. Ecografia abdominal +/- doppler
3. Avaliação analítica: provas hepáticas, função renal, ionogramaurinário
4. Paracentese diagnóstica
- Ascite de início recente ou causa indeterminada- Cirrose hepática com ascite pré-existente e suspeita deperitonite bacteriana espontânea (PBE)
AASLD Practice Guidelines 2012

Ascite
• Avaliação inicial:
1. História clínica e exame objetivo
2. Ecografia abdominal +/- doppler
3. Avaliação analítica: provas hepáticas, função renal, ionogramaurinário
4. Paracentese diagnóstica
5. Paracente evacuadora: desconforto abdominal, dispneia,saciedade precoce
AASLD Practice Guidelines 2012

Ascite
• Paracentese
Up to date

Ascite
• Paracentese
1. Profilaxia por rotina com PFC ou plaquetas não estárecomendado (exceto CID)
- estudo com 1100 paracenteses evacuadores não mostroucomplicações hemorrágicas
- 54% <50000 plaquetas- 75% >1,5 INR e 26% > 2,0 INR
Up to date

Ascite
• Paracentese
1. Profilaxia por rotina com PFC ou plaquetas não estárecomendado (exceto CID)
2. CI relativa – gravidez, celulite parede abdominal, globo vesical,ileus
3. Decúbito dorsal, cabeceira elevada4. Assepsia5. Seringa 20mL, agulha de 22G (diagn) vs. 16 G (evacuadora)6. Introdução do cateter/seringa perpendicular à pele, sempreaspirando até que haja saída do líquido peritoneal

Ascite
Up to date

Ascite
• Paracentese
1. Profilaxia por rotina com PFC ou plaquetas não estárecomendado (exceto CID)
2. CI relativa – gravidez, celulite parede abdominal, globo vesical,ileus
3. Decúbito dorsal, cabeceira elevada4. Assepsia5. Seringa 20mL, agulha de 22G (diagn) vs. 16 G (evacuadora)6. Introdução do cateter/seringa perpendicular à pele, sempreaspirando até que haja saída do líquido peritoneal
7. Coletar liquido para tubo de hemograma (citologia), tubo debioquímica e culturas (aerobiose, micológico e anaerobiose)
8. Pesquisa de células neoplásicas (150mL) – 60% Sens.

Ascite
• Análise do líquido ascítico
1. Aparência macroscópica
- Amarelo citrino (claro)- Turvo – infeções- Leitoso (quiloso) – neoplasia, pancreatite- Sanguinolenta – traumática, neoplasia, tuberculose (raro)- Castanho/verde – bílis, icterícia ou perfuração GI (úlceraduodenal)

Ascite
• Análise do líquido ascítico
2. Citologia
- contagem celular e diferencial
- >250 PMN = PBE
- Nota: subtrair 1PMN por cada 250 eritrócitos (punçãotraumática)

Ascite
• Análise do líquido ascítico
3. Gradiente albumina sérica e albumina do liquido ascítico(GASA)
- GASA = Albumina soro – Albumina LA
- GASA > 1,1 – HT Portal

Ascite
• Análise do líquido ascítico
3. Gradiente albumina sérica e albumina do liquido ascítico(GASA)

Ascite
• Análise do líquido ascítico
4. Bioquímica
- Glicose, proteínas totais, LDH, amílase
- Proteinas LA < 15g/L – risco de PBE
- PBS: PMN >10000, LDH LA > soro, glucose <<, ProteinasLA> 10g/L, polibacteriano ou fungos/anaerobios
- opção: TG, colesterol, ADA, Bilirrubina

Ascite
• Tratamento
1. Medidas conservadores
- Tratamento da causa subjacente – ex. abstinência
- Restrição de sódio – 2g/dia
- Restrição de líquidos – se Na <120 g/mL
- Diuréticos: obj- aumento excreção urinária Na e perda peso
• Espironolactona 100mg ----- 400mg/dia
• Furosemida 40mg ------------- 160mg/dia
• Suspender se Na<120, lesão renal, EH, caimbras graves
AASLD Practice Guidelines 2012, EASL Practice Guidelines 2013

Ascite
• Tratamento
2. Paracentese evacuadora
- Ascite refratária
AASLD Practice Guidelines 2012, EASL Practice Guidelines 2013

Ascite
• Tratamento
2. Paracentese evacuadora
- Ascite refratária
- Ascite sob tensão ou sintomática
v Albumina: 8g/L de ascite removida >5L(cada frasco de albumina humana a 20% possui 10g )
AASLD Practice Guidelines 2012, EASL Practice Guidelines 2013

Albumina
Jalan R, J Hepatol 2013 – PMID 23954671; Levitt DG, Int J Gen Medicine 2016 – PMID 27486341
1. Modulador da distribuição de fluidosà 75% pressão oncótica
Efeito Gibbs-Donnan

no cases of hyponatremia in either study group, and sothe OR for that trial could not be computed or includedin the calculation of pooled OR. Across the other 16included trials there was no evidence of significant heter-ogeneity (P ¼ 0.97; I2, 0%) or publication bias (P ¼0.24) with respect to the hyponatremia endpoint.In the three trials comparing albumin with no treat-
ment, 13 of 79 untreated control patients (16.5%)developed hyponatremia versus 3 of 77 patients receiv-ing albumin (3.9%). Albumin reduced the odds ofhyponatremia by 80%, compared with no treatment(pooled OR, 0.20; CI, 0.05-0.74).Over all 14 trials evaluating alternative treatments, 86
of 577 control patients (14.9%) and 39 of 478 patientsallocated to albumin treatment (8.2%) experienced hypo-natremia. Among 13 of those trials with at least one caseof hyponatremia, albumin decreased the odds of hypona-tremia by 42% (Fig. 3). The effects of albumin on theodds of hyponatremia were similar across strata of age,refractory ascites, baseline serum albumin level, type ofcontrol volume expander, day of PCD assessment, para-centesis regimen, ascites volume removed, trial quality,control group mortality, and time period (Table 2).Mortality. Data on mortality were unavailable for
four trials, and in one trial,20 there were zero deaths.Across the remaining 12 trials, the mortality endpoint
did not exhibit significant heterogeneity (P ¼ 0.91; I2,0%) or publication bias (P ¼ 0.24). Only 1 of the 12trials compared albumin with no treatment,2 and therewas no significant effect of albumin on mortality inthat trial (P ¼ 0.37).In 11 trials with mortality data comparing albumin
with alternative treatments, 74 of 513 control patients(14.4%) died versus 50 of 414 assigned to albumininfusion (12.1%). The odds of death were lower by36% in the albumin group (P ¼ 0.038; Fig. 4). Differ-ences in the effect of albumin on mortality betweensubgroup strata of age, refractory ascites, baseline serumalbumin level, type of control volume expander, day ofPCD assessment, paracentesis regimen, ascites volumeremoved, trial quality, control group mortality, and timeperiod were minor (Table 2).Secondary Endpoints. Of the trials comparing albu-
min with alternative treatments, the number with avail-able data for a particular secondary endpoint and atleast one event ranged from 6 to 11 (Table 3). Albuminadministration was associated with 15%-19% reductionsin the odds of acites recurrence, renal impairment, andhospital readmission. Smaller reductions were observedfor hepatic encephalopathy and portal hypertensivebleeding. However, none of these effects with respect tosecondary endpoints were statistically significant.
Fig. 2. PCD in trials comparingalbumin with alternative treat-ments. Error bars depict CI. Pointestimates for individual trialsscaled in proportion to meta-ana-lytic weight.
1176 BERNARDI ET AL. HEPATOLOGY, April 2012
Bernardi M, Hepatology 2012 – PMID 22095893
Disfunção circulat. pós paracentese
↓ volémia efectiva
ê
↑ > 50% renina
4-6 dias pós paracentese de
grande volume
13 estudos, 857 doentes
15% vs. 31% ↓ 61%

Albumin infusion has yielded favorable results as atreatment for hyponatremia in patients with cirrhosis.40,41
In one RCT, daily albumin infusion for severe hypona-tremia in patients with refractory ascites increased serumsodium levels and reduced the incidence of infection,hepatic encephalopathy, and in-hospital mortality.41
The clinical value of albumin administration as anadjunct to LVP has been questioned because a survivalbenefit could not previously be shown.5,42 Individualtrials have not been powered to detect a survival benefit.By ‘‘borrowing strength’’ from all available RCTs, thismeta-analysis has provided evidence that albumin canindeed bestow a survival benefit, compared with alterna-tive treatments in ascites patients undergoing LVP.The mechanisms underlying the therapeutic effects
exerted by albumin in liver failure are not fully under-stood, but multiple mechanisms appear to be at work.Albumin, the most abundant circulating protein in theplasma, is endowed with an array of nononcotic prop-erties beyond its role as the predominant plasma col-loid and its capacity to expand intravascular volume.43
These include ligand binding and antioxidant andanti-inflammatory activity. Patients with ascites areusually hypoalbuminemic as a consequence of reducedhepatic synthesis and secretion, dilution by increasedintravascular and interstitial volume, and loss to theascites fluid. Moreover, the ability of albumin totransport protein-bound substances and drugs and act
as a detoxification agent is severely compromised inpatients with cirrhosis.44 The combination of hypoal-buminemia and impaired albumin function leads to amarked disturbance in the transport, metabolism, andexcretion of many endogenous and exogenous substan-ces. One consequence is alteration in the pharmacoki-netics and pharmacodynamics of many drugs, thusaffecting their efficacy and side-effect profile.45 Infu-sion of exogenous albumin in ascites patients mayserve the dual purposes of repleting the levels of circu-lating albumin and the functional activity of the albu-min pool. These are effects specific to albumin notshared by alternative treatments and may contribute tothe superior effectiveness of albumin documented inthis meta-analysis.The trials included in the meta-analysis concern
acute treatment with albumin at the time of LVP. But,albumin has also shown promise for the managementof ascites as a weekly or biweekly long-term treatment
Fig. 4. Mortality in trials com-paring albumin with alternativetreatments. Graphic conventions asin Fig. 2.
Table 3. Other Effects of Albumin Versus AlternativeTreatments
Endpoint Trials Odds Ratio (CI)
Ascites recurrence 11 0.85 (0.61-1.18)Renal impairment 10 0.83 (0.49-1.42)Hepatic encephalopathy 7 0.91 (0.50-1.66)Portal hypertensive bleeding 7 0.97 (0.45-2.11)Hospital readmission 6 0.81 (0.56-1.18)
HEPATOLOGY, Vol. 55, No. 4, 2012 BERNARDI ET AL. 1179
Bernardi M, Hepatology 2012 – PMID 22095893
Disfunção circulat. pós paracentese
11 estudos, 927 doentes
12,1% vs. 14,4% ↓ 36%

Ascite
• Tratamento
3. TIPS/Transplante hepático
- Ascite refratária
AASLD Practice Guidelines 2012, EASL Practice Guidelines 2013

Peritonite bacteriana espontânea (PBE)
• Fatores risco: Hemorragia digestiva, prot. LA<15g/L, Bil>3mg/dL
• Prevalência de 10% dos doentes internados (50% admissão)
• Tratamento
1. Antibiótico
- Cefotaxime 2g 8/8h - 5 dias
- Ceftriaxone 2g/dia – 5 dias
AASLD Practice Guidelines 2012, EASL Practice Guidelines 2013

Peritonite bacteriana espontânea (PBE)
• Fatores risco: Hemorragia digestiva, prot. LA<10g/L, Bil>3mg/dL
• Prevalência de 10% dos doentes internados (50% admissão)
• Tratamento
1. Antibiótico
2. Albumina
- 1,5g/Kg D1 (primeiras 6 horas) + 1g/Kg D3
AASLD Practice Guidelines 2012, EASL Practice Guidelines 2013

Sort P, NEJM 1999 – PMID 10432325
• Previne síndrome hepato-renal
• 126 doentes com PBE• 1,5g/Kg D1 + 1g/Kg D3
Peritonite bacter. espontânea
INTRAVENOUS ALBUMIN IN PATIENTS WITH CIRRHOSIS AND SPONTANEOUS BACTERIAL PERITONITIS
Volume 341 Number 6
·
405
ime and albumin (6 of 63 [10 percent]) than amongthose treated with cefotaxime alone (21 of 63 [33percent], P=0.002) (Table 2). On days 3, 6, and 9,the blood urea nitrogen and serum creatinine levelswere lower and the serum sodium level was higherin the cefotaxime-plus-albumin group than in thecefotaxime group (Table 3). Renal impairment de-veloped in 27 patients, and in 23 of these patients,the worsening of renal function followed a progres-sive course characterized by oliguria or anuria, markedincreases in blood urea nitrogen and serum creati-nine levels (the peak values were 94±8 mg per dec-iliter [34±3 mmol per liter] and 3.4±1 mg per dec-iliter [301±88 µmol per liter], respectively), andsevere hyponatremia (124±1 mmol of sodium perliter). For the series of patients as a whole, inde-pendent predictors of the development of renal im-pairment included base-line serum bilirubin and cre-atinine levels (P<0.001 and P=0.01, respectively)and treatment with cefotaxime alone (P=0.02; oddsratio, 4.6; 95 percent confidence interval, 1.3 to 16.1).The incidence of renal impairment among patients
with a base-line serum bilirubin level of at least 4 mgper deciliter (68 µmol per liter) was 48 percent (14of 29 patients) in the cefotaxime group, as com-pared with 12 percent (3 of 25 patients) in the cef-otaxime-plus-albumin group, regardless of the serumcreatinine level. Corresponding results in patients witha serum bilirubin level of less than 4 mg per decili-ter and a serum creatinine level of at least 1 mg perdeciliter were 32 percent (6 of 19 patients) and 14percent (3 of 21 patients), respectively. The inci-dence of renal impairment among patients with a se-rum bilirubin level of less than 4 mg per deciliter anda serum creatinine level of less than 1 mg per deci-liter was very low in both treatment groups (7 per-cent and 0 percent in the cefotaxime and cefotax-ime-plus-albumin groups, respectively).
Mortality
Mortality during hospitalization was significantlylower among patients treated with cefotaxime andalbumin than among those treated with cefotaximealone (10 percent vs. 29 percent, P=0.01) (Table 2).Independent predictors of in-hospital mortalitywere the blood urea nitrogen level (P=0.001), se-rum bilirubin level (P=0.01), and prothrombin time
*Plus–minus values are means ±SE. No significant differences werefound between the two groups in any of the characteristics. To convert thevalues for serum bilirubin to micromoles per liter, multiply by 17.1.
†The Child–Pugh score (range, 5 to 15, where 5 indicates good liverfunction and 15 indicates poor liver function) was calculated on the basisof the presence and degree of hepatic encephalopathy, the presence and de-gree of ascites, the serum bilirubin level, the serum albumin level, and theprothrombin time.
‡Organisms were isolated from ascitic fluid or blood.
T
ABLE
1.
B
ASE
-L
INE
C
HARACTERISTICS
OF
THE
126 P
ATIENTS
A
CCORDING
TO
THE
A
SSIGNED
T
REATMENT
.*
C
HARACTERISTIC
C
EFOTAXIME
(N=63)
C
EFOTAXIMEPLUS
A
LBUMIN
(N=63)
Age — yr 62±1 60±1Sex — M/F 38/25 43/20Alcoholic cirrhosis — no. (%) 19 (30) 18 (29)Hepatocellular carcinoma — no. (%) 7 (11) 10 (16)Hepatic encephalopathy — no. (%) 15 (24) 13 (21)White-cell count — per mm
3
9221±814 7883±560Ascitic-fluid polymorphonuclear cells
— per mm
3
4228±750 5223±1541
Serum bilirubin — mg/dl 6±1 4±1Serum albumin — g/dl 2.5±0.1 2.7±0.1Prothrombin time — % of control 58±2 55±2Child–Pugh score† 10±0.2 10±0.2Renal failure — no. (%) 28 (44) 25 (40)Diuretic treatment — no. (%)
Spironolactone — mg/dayFurosemide — mg/day
41 (65)73±519±1
45 (71)81±618±2
Previous prophylactic treatment with norfloxacin — no. (%)
5 (8) 6 (10)
Isolated organisms — no. (%)‡
Escherichia coli
Other gram-negative bacilliOther bacteria
36 (57)2268
32 (51)2075
*Plus–minus values are means ±SE. †The infection resolved with the initial cefotaxime therapy in 53 of the
63 patients (84 percent) in the cefotaxime group and in 57 of the 63 pa-tients (90 percent) in the cefotaxime-plus-albumin group. In the other pa-tients, the infection resolved after modification of the antibiotic therapy.
‡These patients required at least one therapeutic paracentesis for themanagement of ascites.
§The causes of in-hospital death were combined liver and renal failure(13 patients in the cefotaxime group and 5 in the cefotaxime-plus-albumingroup), massive gastrointestinal hemorrhage (2 patients in the cefotaximegroup and 1 in the cefotaxime-plus-albumin group), septic shock (2 pa-tients in the cefotaxime group), and liver failure (1 patient in the cefotax-ime group).
¶Seven patients (four in the cefotaxime group and three in the cefotax-ime-plus-albumin group) were lost to follow-up after discharge from thehospital. The three-month mortality rates were calculated as the numberof known deaths at this time divided by the total number of enrolled pa-tients in each group.
T
ABLE
2.
C
LINICAL
O
UTCOME
A
CCORDING
TO
THE
A
SSIGNED
T
REATMENT
.*
O
UTCOME
V
ARIABLE
C
EFOTAXIME
(N=63)
C
EFOTAXIMEPLUS
A
LBUMIN
(N=63)P
V
ALUE
Resolution of infection — no. (%)† 59 (94) 62 (98) 0.36Duration of antibiotic therapy
— days6±1 5±1 0.48
Paracentesis for ascites after resolution of infection — no. (%)‡
16 (25) 14 (22) 0.83
Hospital stay — days 13±1 14±1 0.48Renal impairment — no. (%) 21 (33) 6 (10) 0.002Death — no. (%)
In hospital§At three months¶
18 (29)26 (41)
6 (10)14 (22)
0.010.03
The New England Journal of Medicine Downloaded from nejm.org at INSERM DISC DOC on January 2, 2017. For personal use only. No other uses without permission.
Copyright © 1999 Massachusetts Medical Society. All rights reserved.

Salerno F, Clin Gastro Hepatol 2013 – PMID 23178229
Meta-análise 4 estudos, 288 doentes
Peritonite bacter. espontânea
Treatment assignment was determined by computer-gener-ated sequence of random numbers in 3 trials11,18,19 and coin tossin 1 trial.17 In 3 trials, concealment of allocation to randomizedgroups was accomplished by using sealed envelopes.11,18,19 Allo-cation concealment method was unspecified for the fourthtrial.17 Thus, method of randomization was adequate for all 4included trials and of allocation concealment for 3 trials. Onthe other hand, only 1 of the 4 trials was blinded.11
In all trials, the patients of both groups received antibiotic(Table 1). Albumin was infused as a 20% solution in all trials.The treatment period with albumin was 3 days in 3 trials and 3weeks in the remaining trial. An albumin dose range of 0.5–1.5g/kg!1 was administered in 3 trials, whereas in the remainingtrial, 3 daily fixed dosages of 10 g (0.14 g/kg!1 for a 70-kgpatient) were given on the basis of National Health Insurancecoverage. Control treatment in 1 trial consisted of hydroxyethylstarch (HES) at the same dose as that of albumin. In the other3 trials, albumin was compared with no albumin. Length offollow-up was 90 days in 1 trial and unspecified in the others.
Renal ImpairmentIn 3 trials, renal impairment was defined according to
the presence or absence of renal insufficiency at baseline. Forpatients without preexisting renal insufficiency, renal impair-ment was defined as an increase from baseline in serum creat-
inine to "1.5 mg/dL!1 or, alternatively in 2 of the 3 trials, inblood urea nitrogen (BUN) to "30 mg/dL!1. In addition, in 2of the 3 trials the relative magnitude of serum creatinine orBUN increase must have been "50%. Only the "50% relativeincrease criterion was applied in cases of preexisting renal in-sufficiency. In the fourth trial, renal impairment was defined asa serum creatinine level "1.5 mg/dL!1 or BUN "25 mg/dL!1.
Across all 4 trials, 12 of 144 albumin recipients (8.3%) de-veloped renal impairment, compared with 44 of 144 controlgroup patients (30.6%). The odds ratios for renal impairment inthe 4 trials were highly consistent, ranging narrowly from 0.19 –0.30 (Figure 2). The pooled odds ratio was 0.21. There was noevidence of significant heterogeneity (P # .99; I2, 0%) or publi-cation bias (P # .11) with respect to the renal impairment endpoint.
The trials by Sort et al11 and Xue et al17 accounted for thepreponderance of meta-analytic weight. The pooled odds ratiofor renal impairment was 0.21 with 95% confidence interval (CI)of 0.08 – 0.54 after excluding the trial by Sort et al and 0.23 (CI,0.09 – 0.54) after excluding the trial by Xue et al. These resultsare the same as or closely similar to the pooled odds ratioshown in Figure 2 with no exclusion (0.21; CI, 0.11– 0.42).
For one included trial,11 outcomes were reported with strat-ification according to significant baseline predictors. Neverthe-less, in the report of that trial no formal analysis was presented
Table 1. Included Trials
Trial N Agea (SD), y Male, % Ethnicity Etiology Treatment regimen
Sort et al,11 1999 126 61.0 (7.9) 64.3 Caucasian 29.4% alcohol, 70.6%other
Cefotaxime intravenously dosed according tocreatinine without vs with 1.5g/kg!1 20%albumin within first 6 h plus 1.0 g/kg!1
on day 3Xue et al,17 2002 112 22–70b — Chinese — Ceftriaxone intravenously dosed according to
creatinine without vs with 0.5–1.0 g/kg!1
20% albumin within first 6 h and everythird day for 21 days
Fernández et al,18
200520 61.0 (9.5) 55.0 Caucasian 60.0% HCV, 40.0% other Ceftriaxone intravenously 2 g at diagnosis
and then 1 g/d plus 1.5 g/kg!1 atbaseline and 1.0g/kg!1 on day 3 of 20%albumin vs 6% HES 200/0.5
Chen et al,19
200930 56.5 (11.5) 60.0 Chinese 60.0% HBV, 23.3% HCV,
16.7% alcoholCephalosporins without vs with 50 mL 20%
albumin (0.14 g/kg!1 for a 70-kg patient)on days 1–3
HBV, hepatitis B virus; HCV, hepatitis C virus; SD, standard deviation.aMean, except as otherwise indicated.bAge range eligible for this trial; mean age not reported.
Figure 2. Renal impairment.CI is shown by error bars. Datapoints for individual trials sca-led according to meta-analyticweight.
February 2013 ALBUMIN IN SPONTANEOUS BACTERIAL PERITONITIS 125
on the comparative effectiveness of albumin in the subgroupsdefined by the baseline predictors. Such a subgroup analysis isshown in Table 2. The control group incidence of renal impair-ment was 14 of 29 (48%) when baseline serum bilirubin equaledor exceeded 4 mg/dL!1, as contrasted with 7 of 34 (21%) whenserum bilirubin was below 4 mg/dL!1 at baseline. The oddsratio for the prevention of renal impairment as the result ofalbumin treatment was 0.15 in patients with baseline serumbilirubin !4 mg/dL!1, compared with 0.32 in those with lowerbaseline serum bilirubin; however, this subgroup difference inthe effectiveness of albumin for averting renal impairment wasnot statistically significant (P " .47). With regard to renalimpairment, furthermore, the effectiveness of albumin was sim-ilar in the subgroup defined by either serum bilirubin !4
mg/dL!1 or serum creatinine !1 mg/dL!1 at baseline vs thesubgroup with lower values of those 2 parameters (Table 2).
MortalityTotal mortality was 23 of 144 patients allocated to
albumin treatment (16.0%) and 51 of 144 to the control regi-men (35.4%). Odds ratios for mortality in individual RCTs weresimilar, ranging from 0.16 – 0.55 (Figure 3). The pooled oddsratio was 0.34. There was no significant heterogeneity (P " .72;I2, 0%) or publication bias (P " .69) with respect to mortality.The pooled odds ratio for mortality with exclusion of either thetrial by Sort et al11 (0.28; CI, 0.12– 0.65) or by Xue et al17 (0.41;CI, 0.21– 0.80) was comparable to that with no exclusion shownin Figure 3 (0.34; CI, 0.19 – 0.60).
Table 2. Comparative Effectiveness of Albumin in Subgroupsa
Subgroup
Outcome
Odds ratio (CI) P valueb
Albumin Control
Event Total Event Total
Renal impairmentBilirubin !4 mg/dL!1 3 24 14 29 0.15 (0.04–0.63)Bilirubin #4 mg/dL!1 3 39 7 34 0.32 (0.08–1.36)Ratio of odds ratios (CI) 0.48 (0.06–3.58) .47Bilirubin !4 mg/dL!1 or creatinine !1 mg/dL!1 6 46 20 48 0.21 (0.07–0.59)Bilirubin #4 mg/dL!1 and creatinine #1 mg/dL!1 0 17 1 15 0.27 (0.01–7.28)Ratio of odds ratios (CI) 0.76 (0.02–23.8) .88
Hospital mortalityBilirubin !4 mg/dL!1 3 24 13 29 0.18 (0.04–0.72)Bilirubin #4 mg/dL!1 3 39 5 34 0.48 (0.11–2.19)Ratio of odds ratios (CI) 0.36 (0.05–2.88) .34BUN !30 mg/dL!1 6 23 13 28 0.41 (0.12–1.34)BUN #30 mg/dL!1 0 40 5 35 0.07 (0.00–1.28)Ratio of odds ratios (CI) 5.97 (0.25–142) .27Bilirubin !4 mg/dL!1 or BUN !30 mg/dL!1 6 39 18 43 0.25 (0.09–0.73)Bilirubin #4 mg/dL!1 and BUN #30 mg/dL!1 0 24 0 20 —c
Bilirubin !4 mg/dL!1 and BUN !30 mg/dL!1 3 8 8 14 0.45 (0.08–2.67)Bilirubin #4 mg/dL!1 or BUN #30 mg/dL!1 3 55 10 49 0.23 (0.06–0.87)Ratio of odds ratios (CI) 2.00 (0.21–18.7) .54
aData from included trial of Sort et al.11 Subgroups defined in terms of baseline levels for serum bilirubin, serum creatinine, or BUN. Inmultivariate analyses reported by Sort et al, independent predictors of renal impairment were baseline levels of serum bilirubin (P # .001) andserum creatinine (P " .01) and antibiotic treatment without albumin (P " .02). Independent predictors of hospital mortality included baselinelevels of serum bilirubin (P " .01) and BUN (P " .001) and antibiotic treatment without albumin (P " .05).bDifference in effectiveness of albumin between the subgroups by test of interaction.cOdds ratio inestimable for 0 events in both groups.
Figure 3. Mortality. CI is shownby error bars. Data points for in-dividual trials scaled accordingto meta-analytic weight.
126 SALERNO ET AL CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Vol. 11, No. 2
8,3% vs. 30,6%
16% vs. 35,4%

Peritonite bacteriana espontânea (PBE)
• Fatores risco: Hemorragia digestiva, prot. LA<10g/L, Bil>3mg/dL
• Prevalência de 10% dos doentes internados (50% admissão)
• Tratamento
1. Antibiótico
2. Albumina
3. Paracentese 48h
- Redução >25% PMN em relação à paracentese inicial;- Ausência de redução - escalar ATB e excluir PBS (TC Abdominal)
AASLD Practice Guidelines 2012, EASL Practice Guidelines 2013

Peritonite bacteriana espontânea (PBE)
• Profilaxia primária
1. Cirrótico + hemorragia digestiva – paracentese + ATB
2. Prot. LA<1,5g/dL
- Creatinina > 1,2 mg/dL- Ureia > 25 mg/dL- Na >130- Child >=9 e bil. >=3
• Profilaxia secundária: norfloxacina 400mg/dia ou cotrimoxazol400/80mg/dia
AASLD Practice Guidelines 2012, EASL Practice Guidelines 2013

Lesão renal aguda
• Cr ≥ 50% ou ≥ 0.3mg/dL em relação ao baseline em <48 h
• ↑ mortalidade se Cr >1.5mg/dL
• 50% cirróticos hospitalizados tem LRA
• Causas: Hipovolemia, SHR, infeção, fármacos
AASLD Practice Guidelines 2012, EASL Practice Guidelines 2013

Síndrome hepato-renal
• Diagnóstico:
Bernardi M, J Clin Exp Hepatol 2014 – PMID 25755577

Síndrome hepato-renal
• Diagnóstico:
• Cirrose e ascite
• LRA
• Exclusão de outras causas de LRA
• Ausência de resposta após suspensão diuréticos e expansão com
albumina (100g/dia) em 48h
• Tipo Ià em 2 semanas: Cr x2/ >2,5mg/dL (desencadeante)
• Tipo IIà Cr> 1,5mg/dL, gradual (progressão da doença)
Bernardi M, J Clin Exp Hepatol 2014 – PMID 25755577

Síndrome hepato-renal
• Albumina e terlipressina
Bernardi M, J Clin Exp Hepatol 2014 – PMID 25755577

Síndrome hepato-renal
Ortega R, Hepatol 2002 – PMID 12297842
Patients treated with terlipressin and albumin showedsignificant improvement in renal function and increasesin serum sodium concentration, arterial pressure, centralvenous pressure, and atrial natriuretic peptide levels, andsignificant and marked suppression of the activity of therenin-aldosterone system and sympathetic nervous system(Tables 1 and 2). By contrast, treatment with terlipressinalone was not associated with statistically significantchanges in any of these parameters except for a significantreduction in plasma norepinephrine levels. Individual val-ues of serum creatinine levels before and at the end oftherapy are shown in Fig. 1.
To assess the predictive factors of response to therapy,we analyzed the differences among responders and non-responders (including the 2 patients with partial re-sponses). No differences were found between these 2
groups with respect to the severity of renal failure (base-line serum creatinine levels 3.5 ! 0.5 mg/dL vs. 3.6 ! 0.3mg/dL, respectively; P " .46) or liver failure (baselineChild-Pugh score 10.4 ! 0.6 vs. 11.2 ! 0.6, respectively;P " .34). By contrast, the response rate was significantlyrelated to the administration of albumin in associationwith terlipressin. Ten of the 12 responders received albu-min (83%) as compared with 3 of the 9 nonresponders(33%) (P " .03). By using logistic regression analysis,albumin administration was the only variable with inde-pendent predictive value of complete response.
Recurrence of HRSDuring the 3-month follow-up period, HRS recurred
in only 2 of the 12 patients (17%) with complete response(1 treated with terlipressin and albumin and 1 treatedwith terlipressin alone). Both patients were treated withthe same therapeutic schedule used as initial therapy (for 7and 10 days, respectively) and a complete response wasobserved in the 2 patients. The probability of HRS recur-rence after complete response was 5% at 1 month and37% at 3 months.
Side Effects and Complications of CirrhosisOne of the 21 patients (5%) included (receiving terli-
pressin alone) showed signs of finger ischemia at thefourth day of treatment, which disappeared after terli-pressin withdrawal. Most patients had abdominal cramps,associated with increased bowel movements in some ofthem, after the first dose of terlipressin was given. Thesesymptoms resolved within a few hours despite the admin-istration of subsequent doses of terlipressin. No adverseeffects related to intravenous albumin were seen.
Table 2. Effects of Treatment on Renal Function, Systemic Hemodynamics, and Activity of Neurohumoral Systems in PatientsReceiving Terlipressin and Albumin and in Those Receiving Terlipressin Alone
Terlipressin and Albumin (n ! 13) Terlipressin (n ! 8)
Baseline End of Treatment Baseline End of Treatment
Serum creatinine level (mg/dL) 3.6 ! 0.5 1.5 ! 0.2* 3.4 ! 0.3 3.4 ! 0.7Glomerular filtration rate (mL/min) 10 ! 2 30 ! 8* 4 ! 3 7 ! 4Urine volume (mL/d) 571 ! 54 1,057 ! 27* 719 ! 113 739 ! 108Serum sodium (mEq/L) 123 ! 1 131 ! 1* 120 ! 2 121 ! 3Serum potassium (mEq/L) 4 ! 0.3 3.7 ! 0.1 4 ! 0.3 4.4 ! 0.3Urine sodium (mEq/d) 3 ! 0.6 9 ! 3* 3 ! 1 6 ! 3Mean arterial pressure (mm Hg) 70 ! 2 79 ! 2* 64 ! 4 60 ! 4Central venous pressure (cmH2O) 10 ! 12 14 ! 1* 10 ! 3 12 ! 1Plasma renin activity (ng/mL ! h) 20 ! 8 4 ! 1* 25 ! 8 14 ! 3Aldosterone (ng/dL) 289 ! 55 72 ! 19* 263 ! 80 157 ! 38Norepinephrine (pg/mL) 1,359 ! 274 448 ! 161* 1,030 ! 171 449 ! 46*Atrial natriuretic peptide (fmoL/mL) 156 ! 34 189 ! 31* 112 ! 39 80 ! 17
NOTE. Values are mean ! SEM. No significant differences were found between patients receiving and not receiving albumin in any of the parameters obtained beforetreatment. Normal values of plasma renin activity and plasma concentrations of aldosterone, norepinephrine, and atrial natriuretic peptide in our laboratory in healthysubjects on a low sodium diet are: 1.2 ! 0.1 ng/mL ! h, 24 ! 2 ng/dL, 233 ! 17 pg/mL, and 6 ! 0.5 fmol/mL, respectively.
*P # .05 with respect to baseline values in the same treatment group.
Fig. 1. Individual values of serum creatinine before the initiation oftreatment and at the end of treatment in patients receiving terlipressinand intravenous albumin (left) and patients receiving terlipressin alone(right).
944 ORTEGA ET AL. HEPATOLOGY, October 2002
• Estudo com 25 doentes: terlipressina vs terlipressina + albumina
Two patients treated with terlipressin and albumin (1nonresponder) and 4 treated with terlipressin alone (all 4being nonresponders) developed severe bacterial infec-tions and/or upper gastrointestinal bleeding during ad-mission (P ! .15).
SurvivalAt the end of the first month after the inclusion in the
study, 11 patients were alive (9 treated with albumin), 7had died (1 treated with albumin), and 3 had been trans-planted (all 3 treated with albumin). At the end of thefollow-up period (3 months), 13 patients had died (6treated with albumin), 5 had been transplanted (all 5treated with albumin), 2 were alive (1 treated with albu-min), and 1 was lost to follow-up evaluation. The mediansurvival time in the whole series was 40 days. Main causesof death were bacterial infections in 8 patients, liver fail-ure in 3 patients, and gastrointestinal hemorrhage in 2patients.
To assess the existence of predictive factors of survival,we analyzed the following 3 parameters: renal and liverfunction at baseline, as estimated by serum creatinine lev-els and Child-Pugh score, respectively, and administra-tion of albumin. All 3 parameters were associated withprognostic value in the univariate analysis. However, inthe multivariate analysis, only baseline Child-Pugh scoreand administration of albumin were associated with inde-pendent prognostic value (Fig. 2). The reversal of HRS(complete response) was associated with an improved sur-vival. In the whole series, median survival of patientsshowing complete response to therapy was 50 days com-pared with only 14 days for patients who did not show acomplete response to therapy (P ! .0057) (Fig. 3, upperpanel). Corresponding figures for patients with type 1HRS were 46 days and 12 days, respectively (Fig. 3, lowerpanel).
Comparison Between Patients With Type 1 andType 2 HRS
Table 3 shows the comparison of complete response totherapy, recurrence of HRS, and outcome in patients di-vided according to the clinical type of HRS, type 1 versustype 2.
DiscussionThe results of the current investigation indicate that
terlipressin alone does not seem to be very effective in thetreatment of HRS in patients with cirrhosis, whereas theaddition of albumin seems to improve the outcome. Inthe overall series of patients (treated and not treated withalbumin), the rate of complete response was close to 60%.
This response rate is much higher than the response ratesreported with classic therapies, including renal vasodila-tors, such as dopamine, or peritoneovenous shunting, orthe rate of spontaneous resolution of HRS, which arebelow 10% in all cases.4,13-16 The only therapy that hasbeen reported to induce a response rate similar to thatobtained in the current study is the transjugular intra-hepatic portosystemic shunt. Although the informationavailable on the effect of transjugular intrahepatic porto-systemic shunts in HRS is very limited, the response rateobtained ranges between 40% and 70%.17,18
In the current study, the response rate in patients withtype 2 HRS was similar to that of patients with type 1HRS, which suggests that not only patients with type 1HRS but also patients with type 2 HRS may be candidatesfor vasoconstrictor therapy. Moreover, the survival rateand the number of patients reaching liver transplantationwas higher among patients with type 2 HRS comparedwith patients with type 1 HRS. However, the results ofthese comparisons should be taken with caution becausethe survival of untreated patients with type 2 HRS islonger than that of untreated patients with type 1 HRS1
and the number of patients with type 2 HRS included inthis study was very low.
Fig. 2. Probability of survival after entry into the study of all patientsincluded classified according to the baseline Child-Pugh score (upperpanel) and treatment with terlipressin with or without intravenous albu-min (lower panel).
HEPATOLOGY, Vol. 36, No. 4, 2002 ORTEGA ET AL. 945
Efeito na função renal Efeito na sobrevida
Resposta: 77% vs 25%, p=0.03

Síndrome hepato-renal
Bernardi M, J Clin Exp Hepatol 2014 – PMID 25755577USE OF ALBUMIN IN PATIENTS WITHCIRRHOSIS: CURRENT INDICATIONS(FIGURE 4)
Prevention of Post-Paracentesis CirculatoryDysfunctionAscites is the most frequent complication of cirrhosis, andis associated with a poor prognosis, the 5-year survival be-ing as low as 40% after its development.
Current guidelines indicate therapeutic paracentesis asthe first line of treatment for patients with tense and refrac-tory ascites. It has to be outlined, however, that the removal
of large ascitic fluid volumes leads to a sharp drop in intra-abdominal pressure, boosting venous return to the heartand, therefore, cardiac output. However, because of anexcessive drop in peripheral vascular resistance, effectivevolume further declines. Thus, large volume paracentesiscan ultimately lead to arterial hypotension, renal impair-ment, dilutional hyponatremia, hepatic encephalopathyand reduced survival (Figure 2). Such a condition, namedpost-paracentesis circulatory dysfunction (PPCD), isdefined by a rise of more than 50% in the basal plasmarenin activity 4–6 days after paracentesis, indicating a wors-ening of effective volemia.18
MarƟn-Llahiet al. 2008
Albumindosage
1 g/kg 20-40 g/day(based on CVP)
20-40 g/day(based on CVP)
20-40 g/day(based on CVP)
Terlipressindosage
1 mg/4h i.v. 1 mg/4h i.v.
- If sCr decreaseat least 25% from baseline,conƟnue 1 mg/4h i.v.
- If sCr decrease<25% from baseline,dose doubles to 2 mg/4h i.v.
ConƟnue dose established on
day 4
Sanyalet al. 2008
Albumindosage
100 g 25 g/day 25 g/day 25 g/day
Terlipressindosage
1 mg/6h i.v. 1 mg/6h i.v.
- If sCr decreaseat least 30% from baseline,conƟnue 1 mg/6h i.v.
- If sCr decrease<30% from baseline,dose doubles to 2 mg/6h i.v.
ConƟnue dose established on
day 4
Albumin
dose doubles to 2 mg/4h i.v.dose doubles to 2 mg/4h i.v.
Alb i
Days from diagnosis 1 2-3 4 5-15
STOP if:HRS reverse
(sCr<1.5 mg/dl)or side eīects
occur
Figure 3 Dose schedules of terlipressin and albumin derived from the two main controlled clinical trials devoted to the treatment of patients withcirrhosis and hepatorenal syndrome (i.v.: intravenous; CVP: central venous pressure; sCr: serum creatinine; HRS: hepatorenal syndrome).
Figure 4 Summary table of the current uses of albumin in hepatology, according to the main international guidelines and looking at futureperspectives (PPCD: post-paracentesis circulatory dysfunction; SBP: spontaneous bacterial peritonitis; HRS: hepatorenal syndrome; HE: hepatic en-cephalopathy; ACLF: acute-on-chronic liver failure).
ALBUMIN IN THE MANAGEMENT OF COMPLICATIONS OF CIRRHOSIS BERNARDI ET AL
306 © 2014, INASL
LiverCirrhosis

Hiponatremia na cirrose
• 50% Na <135• Sintomas <110/115
• Hipovolémica – sem ascite ou edemas
• Hipervolémica – extracelular
1. Vasodilatação esplancnica
2. Tratamento
- Balanço negativo de água- Restrição de fluídos – 1L/dia- Reduzir diuréticos (Na<120)
AASLD Practice Guidelines 2012, EASL Practice Guidelines 2013

Bernardi M, J Clin Exp Hepatol 2014 – PMID 25755577
Indicações Albumina na cirrose
Complicação da cirrose Utilização da albumina
Pós paracentese 8g/L de ascite removida (>5L)
GuidelinesPBE 1,5g/Kg D1 e 1g/Kg D3
S. Hepato-renal 1g/Kg D1, 20-40g id D2-15+ terlipressina
Infecções não-PBE 1 estudo: melhoria renal e circulatória; sem melhoria sobrevida
Em estudo (controverso)
Encefalopatia 2 estudos (discordantes)
Ascite Estudo ANSWER em curso
ACLF MARS e Prometheus

• Alterações cerebrais despoletadas por insuficiência hepática e/ou
shunts portosistémicos (SPS)
• 3 tipos
• A – IHA
• B – SPS
• C – Cirrose
• Fatores desencadeantes: infeção, hemorragia digestiva, excesso
de diurético, obstipação, desidratação, alterações hidroeletrolíticas,
fármacos
Encefalopatia hepática
AASLD Practice Guidelines 2014

Encefalopatia hepática

• Tratamento
• Exclusão de outras causas de alteração do estado de
consciência
• Identificar e corrigir os fatores precipitantes
• Proteínas (1-1,5g/Kg/dia)
• Lactulose 3xdia (titular de forma a 2/3 dej/dia)
• Rifaximina 1200mg/dia
Encefalopatia hepática
AASLD Practice Guidelines 2014

Referenciação para transplante hepático
Evaluation for Liver Transplantation in Adults: 2013 Practice Guideline by the AASLD

Referenciação para transplante hepático
Evaluation for Liver Transplantation in Adults: 2013 Practice Guideline by the AASLD

• A paracentese diagnóstica deve ser realizada em todos
doentes com ascite, independentemente da sua
etiologia.
• A peritonite bacteriana espontânea é uma complicação
comum na ascite
• Peritonite bacteriana espontânea >250 PMN no LA
• Excluir infeção, incluindo PBE, em todos os doentes com
cirrose e hemorragia digestiva, febre, choque, EH,
agravamento da função renal ou hepática
Mensagens finais