
Chronic Kidney Disease - RCP London
40
Chronic Kidney Disease Maarten Taal Royal Derby Hospital and University of Nottingham United Kingdom
Transcript of Chronic Kidney Disease - RCP London

Chronic Kidney Disease
Maarten Taal
Royal Derby Hospital and University of Nottingham
United Kingdom
Outline
• CKD epidemiology update
• Estimating GFR: – CKD-EPI equation – Cystatin C
• Revised CKD Classification System (KDIGO 2012 and NICE 2104)
• Risk Prediction in CKD: – Renal – Cardiovascular
CKD Epidemiology

CKD Stage 1-5 Prevalence
Bruck K et al. JASN 2015 ePub
Health Survey for England 2009: CKD 1-5 prevalence 12.3% Fraser SDS et al. JPubHealth 36: 577–586; 2014
Variation not explained by prevalence of: • Diabetes • Hypertension • Obesity

Jha V et al. Lancet 382: 260-72; 2013
Annual incidence of ESKD

Global and regional mortality from 235 causes of death for 20 age
groups in 1990 and 2010: a systematic analysis for the Global
Burden of Disease Study 2010
Lozano R. Lancet 380: 2095 – 2128; 2013

Estimating GFR

MDRD Equation
Giles, P. D et al. BMJ 334:1198-1200; 2007
eGFR = 2.59 x (serum creatinine) -1.154 x (age) -0.203 x (0.742 if female) x (1.21 if African American)
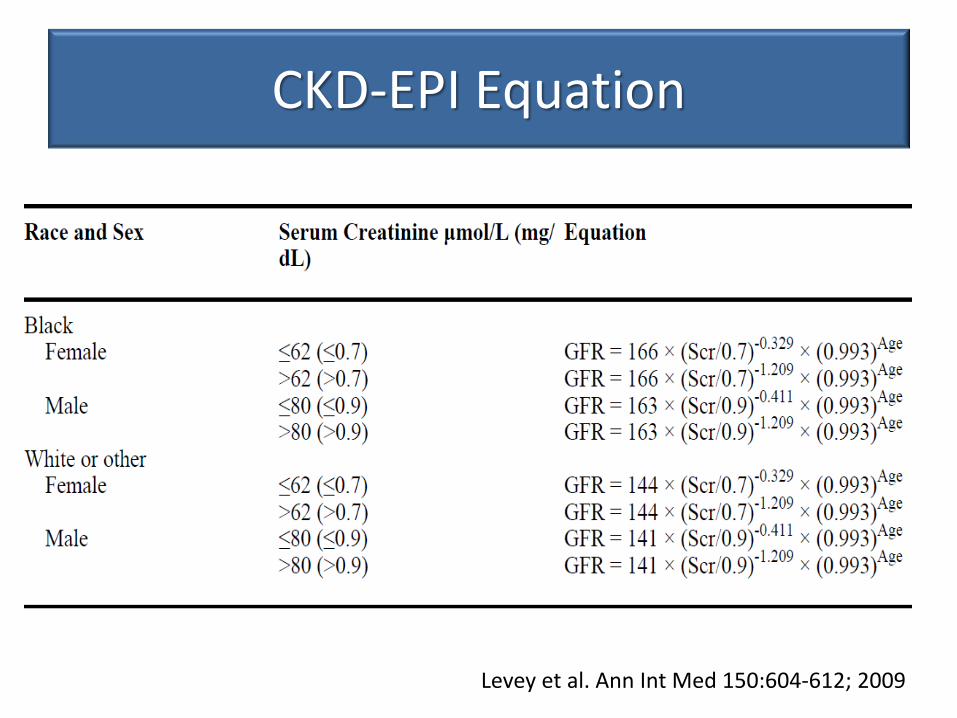
CKD-EPI Equation
Levey et al. Ann Int Med 150:604-612; 2009

MDRD vs. CKD-EPI
Levey et al. Ann Int Med 150:604-612; 2009
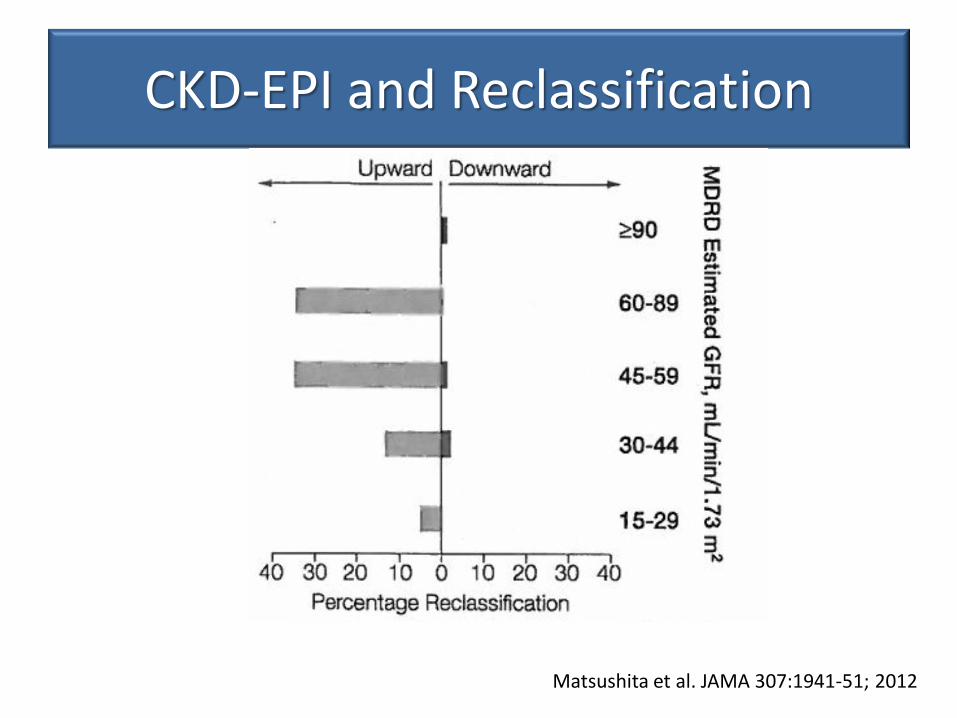
CKD-EPI and Reclassification
Matsushita et al. JAMA 307:1941-51; 2012

CKD-EPI and Risk prediction
Matsushita et al. JAMA 307:1941-51; 2012
Net Reclassification Improvements

Cystatin C
• Small protein produced by all nucleated cells
• Filtered by glomerulus
• No tubular secretion
• Almost completely reabsorbed and catabolised by tubule cells
• Not affected by muscle mass or gender
• Is affected by: obesity, thyroid status, diabetes, corticosteroids, inflammation, smoking

NICE Clinical Guideline 182: 2014
1.1.14 Consider using eGFRcystatinC at initial diagnosis to confirm or rule out CKD in
people with:
• an eGFRcreatinine of 45–59 ml/min/1.73 m2, sustained for at least 90 days and
• no proteinuria (albumin:creatinine ratio [ACR] less than 3 mg/mmol) or other marker
of kidney disease.

NICE Clinical Guideline 182: 2014
1.1.15 Do not diagnose CKD in people with:
• an eGFRcreatinine of 45–59 ml/min/1.73 m2
and
• an eGFRcystatinC of more than 60ml/min/1.73 m2 and
• no other marker of kidney disease.
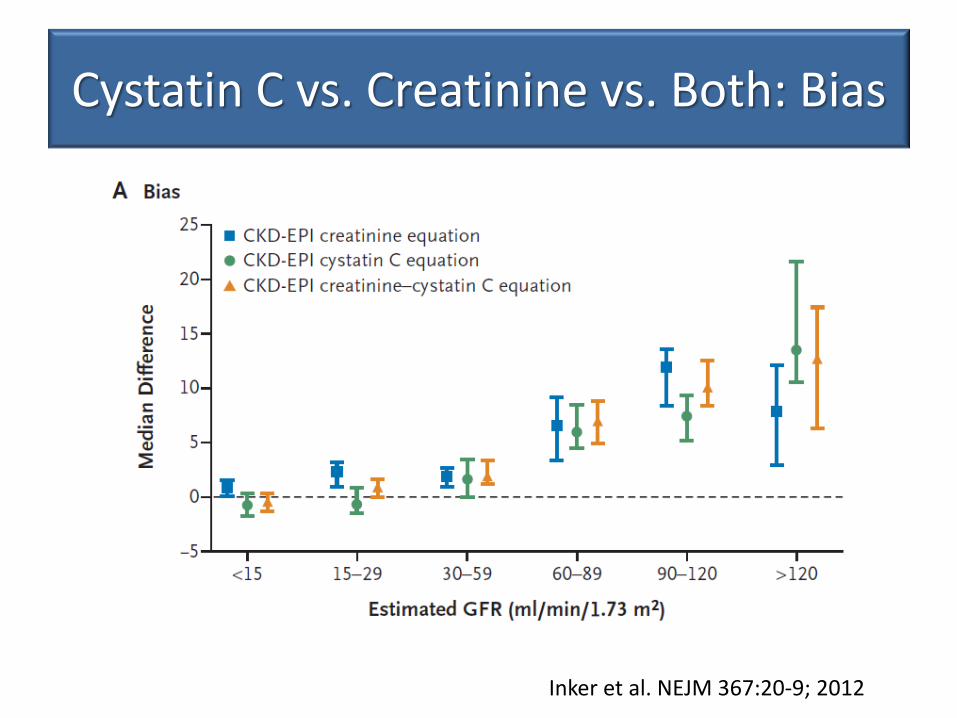
Cystatin C vs. Creatinine vs. Both: Bias
Inker et al. NEJM 367:20-9; 2012
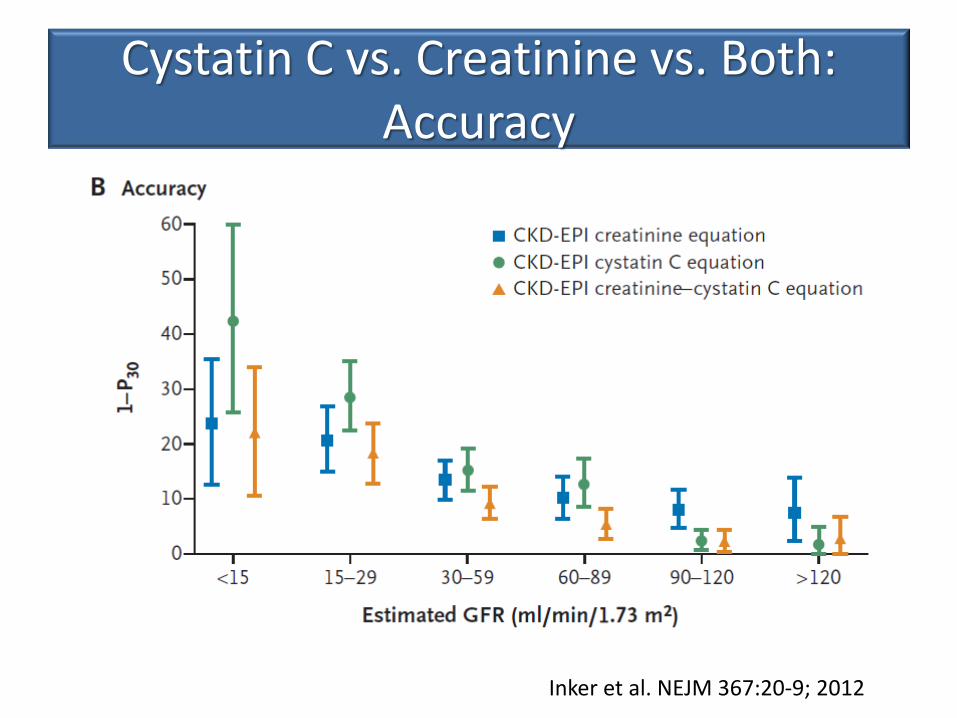
Cystatin C vs. Creatinine vs. Both: Accuracy
Inker et al. NEJM 367:20-9; 2012
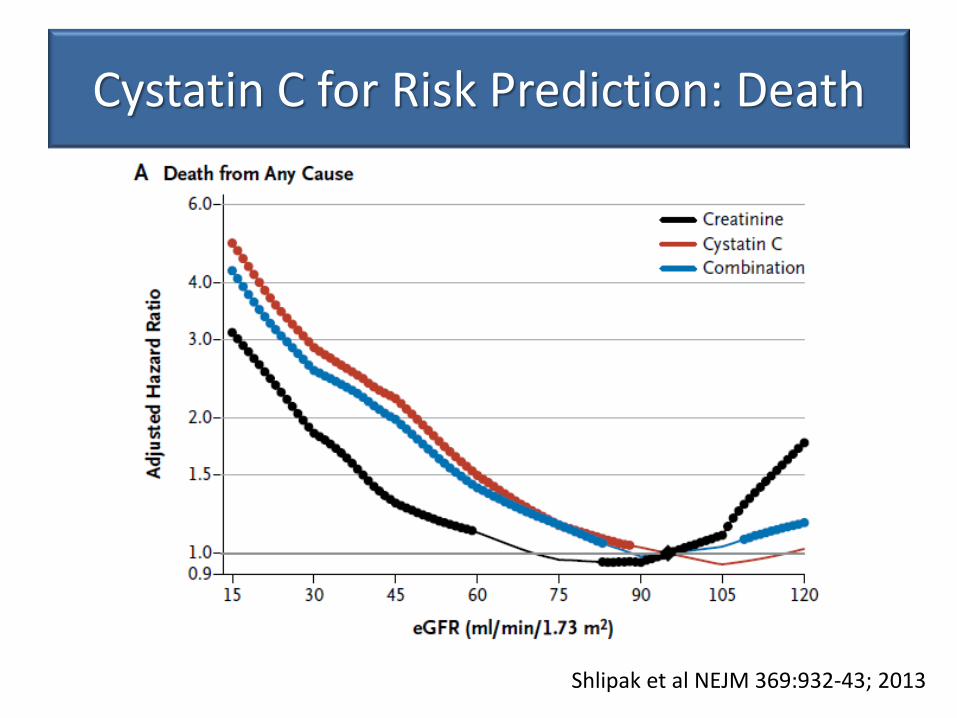
Cystatin C for Risk Prediction: Death
Shlipak et al NEJM 369:932-43; 2013

Cystatin C for Risk Prediction: ESKD
Shlipak et al NEJM 369:932-43; 2013

Cystatin C for Risk Prediction: NRI
Shlipak et al NEJM 369:932-43; 2013
Cystatin C - Problems:
• Currently available in only 3 labs in UK
• Much more expensive
• Prediction data compared Cystatin C to a single Creatinine eGFR
• More data required:
– eGFR-C study
– Renal Risk in Derby study
CKD Classification

NICE CKD Classification 2008
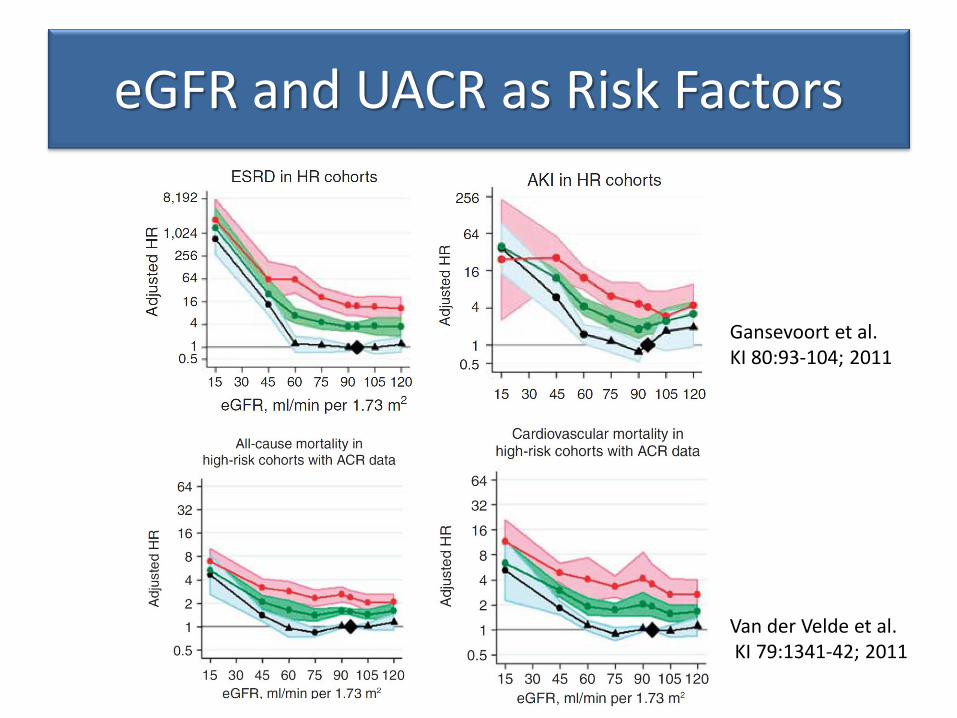
eGFR and UACR as Risk Factors
Gansevoort et al. KI 80:93-104; 2011
Van der Velde et al. KI 79:1341-42; 2011


Risk Prediction in CKD
Renal Risk
• eGFR 51 (CKD 3)
• 84y female
• No previous illness
• BP 125/65
• UACR 1.6mg/mmol
• Category G3a A1
• eGFR 51 (CKD 3)
• 52 year male
• Type 2 DM
• BP 160/95
• UACR 365mg/mmol
• Category G3a A3


Renal Risk Scores
• Patients with CKD stage 3-5
• Risk Factors:
– Age
– Gender
– eGFR
– Albuminuria
– Albumin
– Calcium
– Phosphate
– Bicarbonate
• Outcome: ESKD
• AUC 0.917
Tangri N, JAMA 305:1553-9, 2011

KFRE Validation
Tangri N et al. JAMA. 2016;315(2):164-174.
External validation: • 31 cohorts • 721,357 people • 30 countries • 4-Variable KFRE • C statistic = 0.88 • Correction factor to
improve calibration for non-N.American populations

KFRE Risk Calculator
http://kidneyfailurerisk.com/

Renal Risk
• eGFR 51 (CKD 3)
• 84y female
• No previous illness
• BP 125/65
• UACR 1.6mg/mmol
• 5Year ESKD risk = 0.2%
• eGFR 51 (CKD 3)
• 52 year male
• Type 2 DM
• BP 160/95
• UACR 365mg/mmol
• 5Year ESKD risk = 7.5%

CV Risk Prediction in CKD
• Framingham underestimates CV risk in CKD
• QRISK2 includes CKD but as a binary variable
• Meta-analysis: 637 315 individuals from 24 cohort studies
• Selected participants without CVD at baseline
• Considered eGFR and UACR as risk factors in addition to Framingham risk factors
• Risk assessed over 5 years

Matsushita K. Lancet Diabetes Endocrinol 2015

Matsushita K. Lancet Diabetes Endocrinol 2015
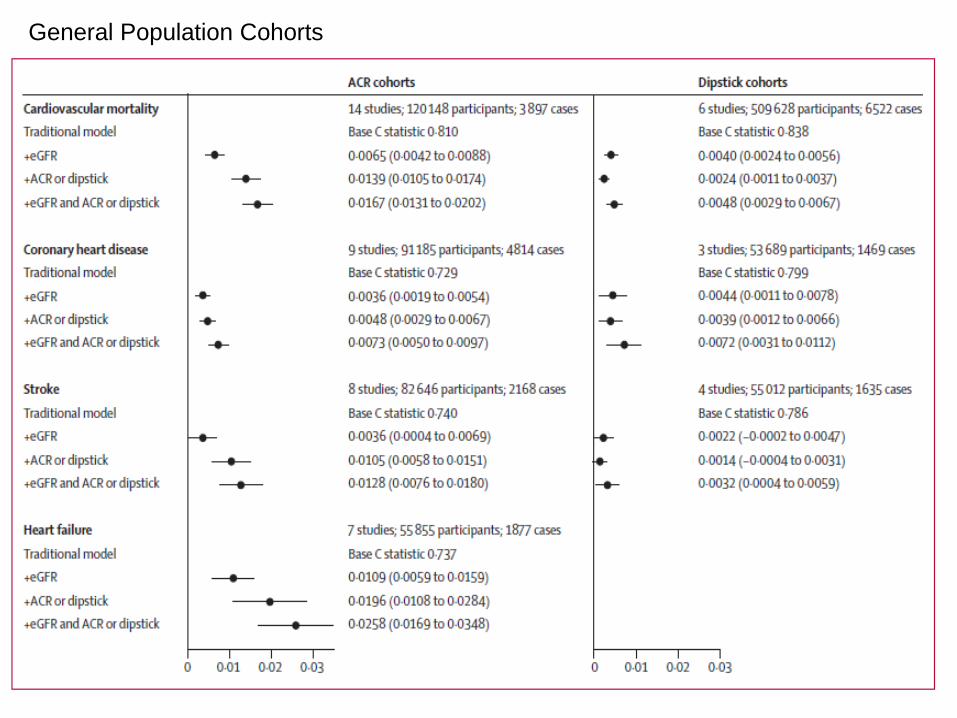
General Population Cohorts


CKD Cohorts

Summary
• CKD remains prevalent in 10-20% of adults • The CKD-EPI equation is more accurate and has
less bias than the MDRD equation • The role of cystatin C for estimating GFR is not yet
clear • The new CKD classification promotes a risk-based
approach to management • The KFRE provides an evidence-based tool for
ESKD risk prediction • GFR and UACR add predictive value to traditional
Framingham cardiovascular risk factors













