
Childhood Tuberculosis
117
-
Upload
lm-huq -
Category
Health & Medicine
-
view
20 -
download
0
Transcript of Childhood Tuberculosis



4

5

6

7
What is the diagnosis?What is the diagnosis?
CHILDHOOD CHILDHOOD
Dr Mohammad Nurul HuqDr Mohammad Nurul HuqWORLD TB DAY 24 MARCH

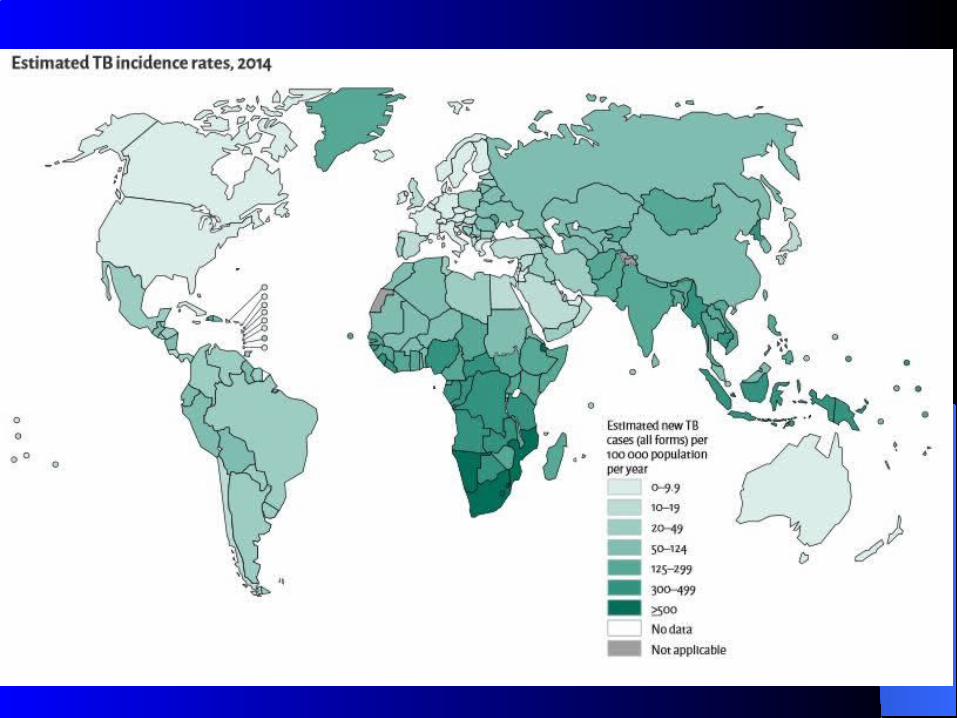
TB Key Facts: TB Key Facts: 30% world population infected!30% world population infected!
22ndnd only to AIDS as the greatest killer as single infx. only to AIDS as the greatest killer as single infx. 2015: 2015: 10.4million cases (10.4million cases (3 million "missed“)3 million "missed“)
– 1.8million (450k children) death1.8million (450k children) death– 480k had MDR-TB480k had MDR-TB
11 of top 10 killers worldwide of top 10 killers worldwide >95% cases & deaths occur in DCs>95% cases & deaths occur in DCs 1 of top 5 killers of women 15-44y1 of top 5 killers of women 15-44y HIV is x30 at riskHIV is x30 at risk
– 35% of HIV deaths35% of HIV deaths (0.4 million) (0.4 million)
multidrug resistant TB (MDR-TB). DCs: developing countriesmultidrug resistant TB (MDR-TB). DCs: developing countries

6 countries have 60% of load: 6 countries have 60% of load: India leading, India leading, f/by f/by Indonesia, China, Nigeria, Pakistan & S. Africa Indonesia, China, Nigeria, Pakistan & S. Africa Bangladesh 7Bangladesh 7thth
49million were saved by Dx & Rx between 2000-1549million were saved by Dx & Rx between 2000-15 We met MDG6 !: to reduce MR 50% by 2015We met MDG6 !: to reduce MR 50% by 2015 Incidence has fallen 1.5%/y since 2000: if 4–5%: reach Incidence has fallen 1.5%/y since 2000: if 4–5%: reach
2020 milestones of 2020 milestones of "End TB Strategy“. "End TB Strategy“. Ending TB Ending TB epidemic by 2030 is target of SDGepidemic by 2030 is target of SDG
TB Key Facts ... TB Key Facts ...

12SEAR: 95% in India, Indonesia, BD, Thailand, BurmaSEAR: 95% in India, Indonesia, BD, Thailand, Burma
2
-S.E. Asia has 38% of all TB cases
WPR25%
AFR18%
EMR8%
EUR6%
AMR5%
SEAR38%
TB can mimic any SS; TB can mimic any SS; speaks every language. speaks every language. Tb occurs Tb occurs everywhere, in everywhere, in every race, gender, ageevery race, gender, age
Malnutrition & TB go hand& in handMalnutrition & TB go hand& in hand In suspected BA, TB must be excluded In suspected BA, TB must be excluded It is It is ""a global health emergencya global health emergency”” MDR-TB: is x100 expensive (Rx x2y), often fatalMDR-TB: is x100 expensive (Rx x2y), often fatal Let no one die from PUO without trial by ATDsLet no one die from PUO without trial by ATDs
ATD: anti TB drugs. SS: symptoms & signs. MDR: multi-drug resistanceATD: anti TB drugs. SS: symptoms & signs. MDR: multi-drug resistance
TB Key Facts ... TB Key Facts ...
90% infected do not get disease90% infected do not get disease SS may be mild for many mo, & can infect 10-15/y. SS may be mild for many mo, & can infect 10-15/y.
Immunodeficiency: most at risk of active TB & dying. Immunodeficiency: most at risk of active TB & dying. The majority can be cured. It is vital that courses of The majority can be cured. It is vital that courses of Rx are completed to eradicate/reduce AB resistanceRx are completed to eradicate/reduce AB resistance
Most fatal in 1Most fatal in 1ststy of lifey of life +ve MT indicates infx., not necessarily the disease+ve MT indicates infx., not necessarily the disease BCG BCG has a high efficacy against TBM & MTB, but variable has a high efficacy against TBM & MTB, but variable
efficacy against adult PTBefficacy against adult PTB
Broadly 2 forms: Broadly 2 forms: pulmonary (90%) & extra-pulmonarypulmonary (90%) & extra-pulmonary
TB Key Facts ... TB Key Facts ...
Bangladesh ScenarioBangladesh Scenario TB is a major PH problemTB is a major PH problem 77thth among 22 high TB burden (80%) countries among 22 high TB burden (80%) countries 60% population infected; 60% population infected; 7 million diseased7 million diseased >300k new cases/y >300k new cases/y (1/every 2min)(1/every 2min) 70k die/y70k die/y (1/every 8 min)(1/every 8 min) No estimate on childhood TBNo estimate on childhood TB: : grossly underdiagnosedgrossly underdiagnosed MDR TB: 2.2%, MDR TB: 2.2%, but among previously Rx cases: 15%but among previously Rx cases: 15%
PH: public healthPH: public health
TB CARE II TB CARE II (USAID): (USAID): helps DOT, Rx of MDR-TB; works with helps DOT, Rx of MDR-TB; works with NTP in line of NTP in line of Stop TB Stop TB StrategyStrategy. . Its achievements:Its achievements:– improved access to quality servicesimproved access to quality services– lab. quality assurancelab. quality assurance– social support for MDR TB pts.social support for MDR TB pts.– effective delivery of TB services at all levelseffective delivery of TB services at all levels
DOT: directly observed therapy. MDR: multi-drug resistantDOT: directly observed therapy. MDR: multi-drug resistantNTP: national TB control programNTP: national TB control program
Bangladesh Scenario …Bangladesh Scenario …

17
Prevalence In Our Children Prevalence In Our Children
Not knownNot known Globally: Globally: 450k die/y450k die/y One of One of 1010 top U-5 killers top U-5 killers Recurrent infx., Mn., & TB go h& in handRecurrent infx., Mn., & TB go h& in hand Often under-diagnosedOften under-diagnosed
Mn: MalnutritionMn: Malnutrition
10 child killers: 10 child killers: ARI, D, Mn, malaria, AIDs, TB, LBW, B. Asphyxia, ARI, D, Mn, malaria, AIDs, TB, LBW, B. Asphyxia, drowning, accidentsdrowning, accidents

Progress in Bangladesh Progress in Bangladesh
MDG6: met already! Case detection up to 72%Case detection up to 72% Rx success 93%Rx success 93% NGO participationNGO participationTB is declining but v. slowly: TB is declining but v. slowly: incidence fell 1.5%/y incidence fell 1.5%/y
since 2000)since 2000)
MM: morbidity & mortality
HIV plus TB: HIV plus TB: Expensive & fatal !Expensive & fatal !
1/31/3rdrd HIV have TB HIV have TB Untreated:Untreated: 90% die in months90% die in months More in young peopleMore in young people More primary infx., more reactivationMore primary infx., more reactivation More MDR-TBMore MDR-TB Rapid progressionRapid progression
HIV cases should be treated freeHIV cases should be treated free

20
DefinitionDefinition
It is a chr. It is a chr. granulomatousgranulomatous ID ID c/by certain strains of c/by certain strains of Mycobacteria mainly affecting the lungsMycobacteria mainly affecting the lungs
Commonly children <5 y of age are affectedCommonly children <5 y of age are affected Less common 5-15yLess common 5-15y
Etiology Etiology
M tuberculosis (commonest)M tuberculosis (commonest) M bovis M bovis M africanusM africanus
Non-Tb. & non-leprous mycobacteria (Non-Tb. & non-leprous mycobacteria (environmentalenvironmental- - or or atypical -)atypical -) cause cause
non-Tb mycobacterial diseasenon-Tb mycobacterial disease
M bovis: M bovis: TB in cattle. Humans affected by milk; causes more TB in cattle. Humans affected by milk; causes more extrapulmonary TBextrapulmonary TB. . Typically resistant to PZATypically resistant to PZA
Synonyms/KeywordsSynonyms/Keywords
Tuberculosis, TB, consumption, phthisisTuberculosis, TB, consumption, phthisis Mycobacterial infx., primary TB, reactivation/adult TB, Mycobacterial infx., primary TB, reactivation/adult TB,
unmasked TBunmasked TB Miliary TB, MTB, TB meningitis, TBM, MDR-TB, XDR-TBMiliary TB, MTB, TB meningitis, TBM, MDR-TB, XDR-TB Pulmonary TB, endobronchial TB, extrapulmonary TBPulmonary TB, endobronchial TB, extrapulmonary TB TB lymphadenopathy, TB lymphadenopathy, scrofulascrofula, vertebral TB, vertebral TB Pott disease, TB spondylitis, bone TB, joint TB, skeletal Pott disease, TB spondylitis, bone TB, joint TB, skeletal
TB, congenital TB, etc.TB, congenital TB, etc.

23
TerminologyTerminologyPrimary TBPrimary TB: : First-time inf. First-time inf.
Mainly children. Characterized by Mainly children. Characterized by Primary ComplexPrimary Complex
Post-primary/reactivated Post-primary/reactivated or Adult-onset/ or Adult-onset/ Unmasked TBUnmasked TB
Reactivation of dormant inf. Mainly adults. Characterized Reactivation of dormant inf. Mainly adults. Characterized by by parenchymal damageparenchymal damage
Positive TST/MTLikely infection. 2-12w after primary (~3-4 wk)
24
Exposed personRecent contact with open PTB but negative TST, normal PE &
CXR
TB DiseaseCF and/or X-Ray signs of TB
Source casewho transmits M tuberculosis
Latent TB Infx (LTBI)positive MT but normal PE, CXR or healed focus (calcification in
lung, LN, or both)
Predisposing factorsPredisposing factors Smoking: Smoking: >20% of TB are attributable to smoking >20% of TB are attributable to smoking PovertyPoverty, poor housing, - hygiene, - sanitation, poor housing, - hygiene, - sanitation Overcrowding, illiteracyOvercrowding, illiteracy Mn.Mn. PollutionPollution Raw milkRaw milk Dm, Dm, HIV, HIV, immunodeficiency, chemo-immunodeficiency, chemo- Family TB, illicit drugsFamily TB, illicit drugs

26
Pathogenesis Pathogenesis
Spread: Spread: aerosol, infected milk. rarely verticalaerosol, infected milk. rarely vertical Lag period/IP: 2-12w (MT positive)Lag period/IP: 2-12w (MT positive) Mostly heal (90%)Mostly heal (90%) Any organ. PTB commonest: subpleural site, more in RULAny organ. PTB commonest: subpleural site, more in RUL
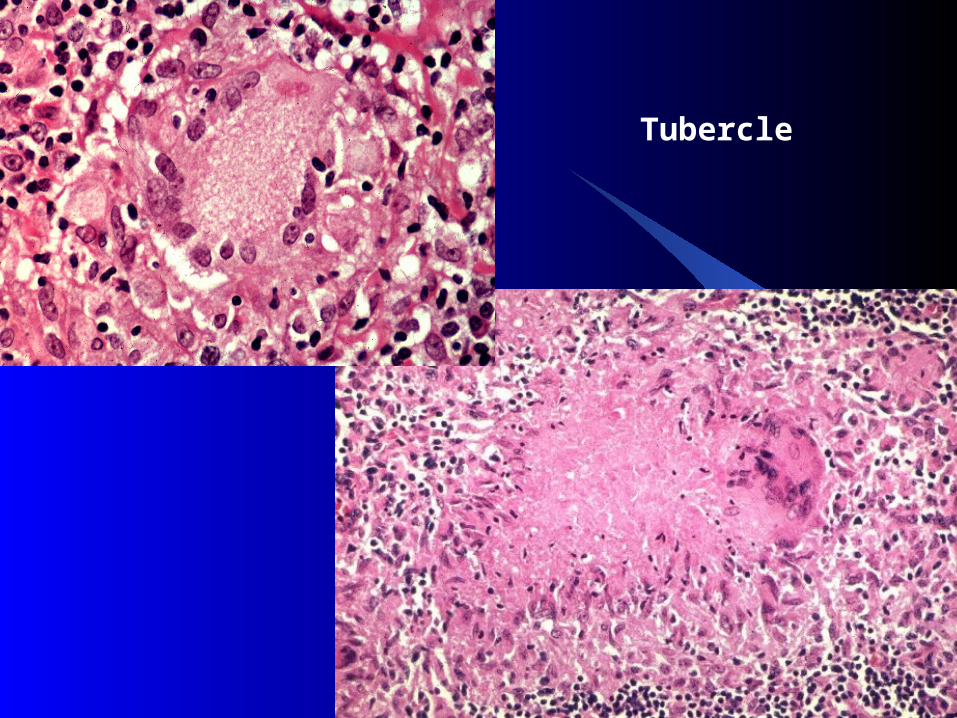
Basic lesion: Basic lesion: tubercle (central caseation); spread bytubercle (central caseation); spread by lymphohematogenous route: LN, other organslymphohematogenous route: LN, other organs
2 reactions: 2 reactions: exudative (effusion) & exudative (effusion) & granulomatous (tubercle)granulomatous (tubercle)
Mn: malnutrition. RUL Right upper lobe
27
Tubercle

28
Tubercle

29
Usual Susceptible OrgansUsual Susceptible Organs

Reactivated/unmasked TBReactivated/unmasked TB DMDM CorticosteroidsCorticosteroids Malignancy, cytotoxicsMalignancy, cytotoxics MalnutritionMalnutrition Whooping cough, measles, KA, HIVWhooping cough, measles, KA, HIV Overwhelming inf.Overwhelming inf. Immunodeficient statesImmunodeficient states

Clinical typesClinical types
Pulmonary (85%) & extrapulmonaryPulmonary (85%) & extrapulmonary OpenOpen (PTB: smear positive: 70%) (PTB: smear positive: 70%) ClosedClosed (no spread) (no spread) Primary & reinfectionPrimary & reinfection New & retreatmentNew & retreatment
Smear negativeSmear negative: when 2 sputum samples are negative: when 2 sputum samples are negative
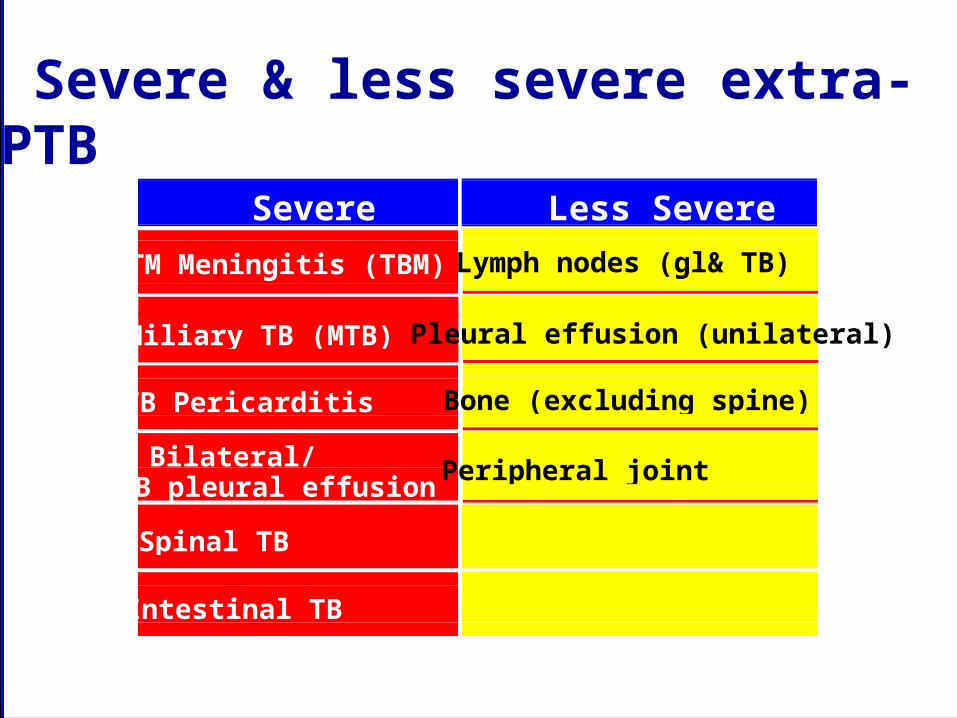
Severe & less severe extra-PTB
SevereTM Meningitis (TBM)
Less SevereLymph nodes (gl& TB)
Miliary TB (MTB)
TB Pericarditis Bone (excluding spine)
Bilateral/extensiveTB pleural effusion
Spinal TB
Intestinal TB
Pleural effusion (unilateral)
Peripheral joint
34
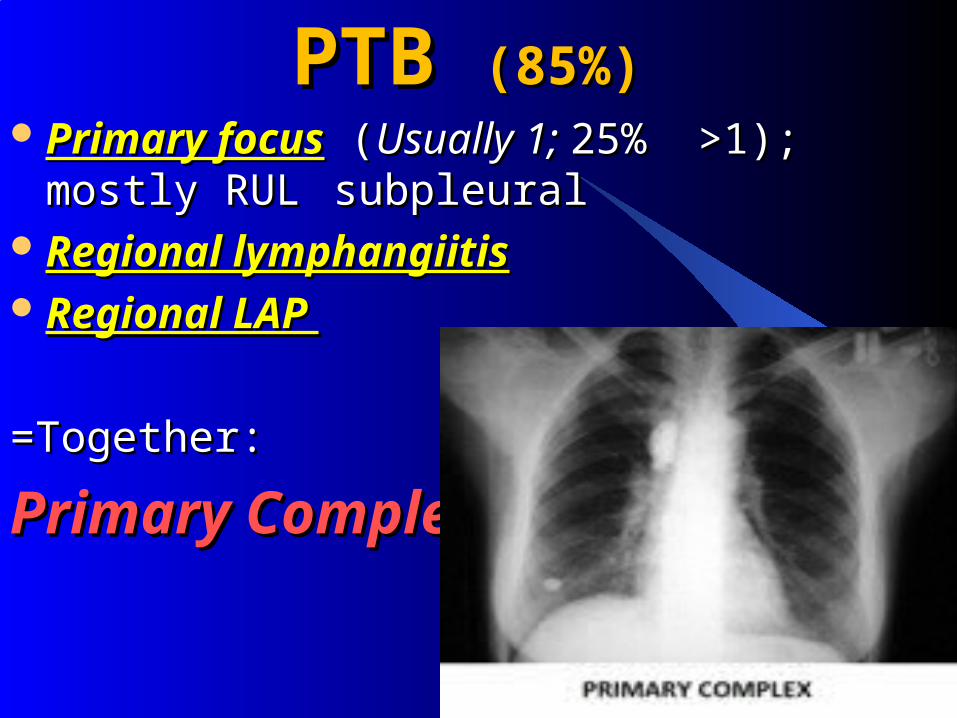
PTB PTB (85%)(85%) Primary focusPrimary focus ((Usually 1; Usually 1; 25% >1); mostly RUL 25% >1); mostly RUL
subpleuralsubpleural Regional lymphangiitisRegional lymphangiitis Regional LAP Regional LAP
=Together: =Together:
Primary ComplexPrimary Complex
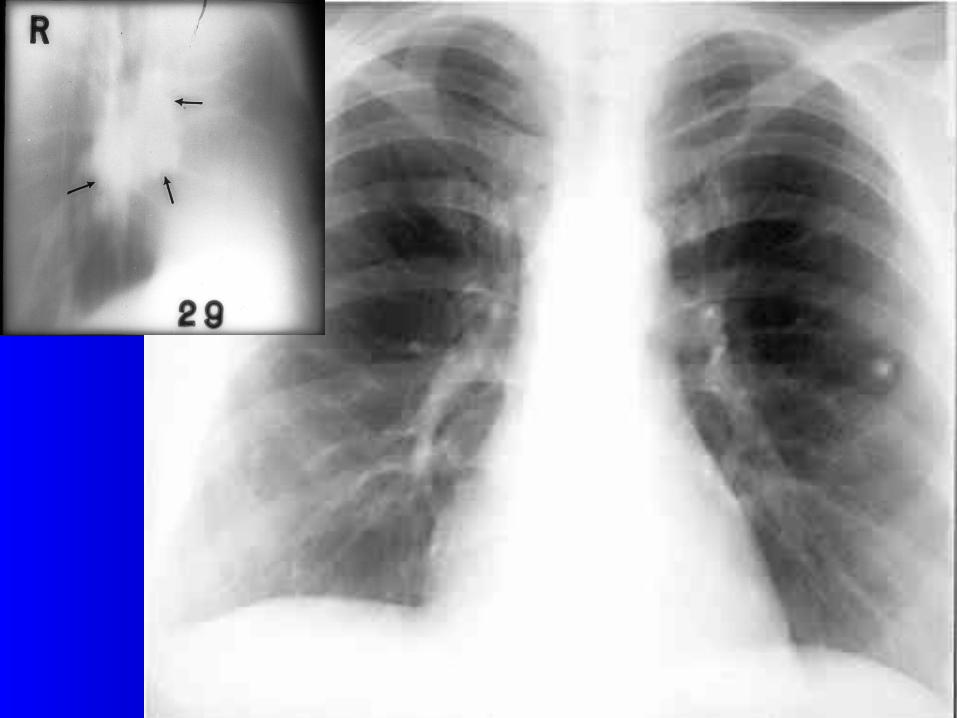
35
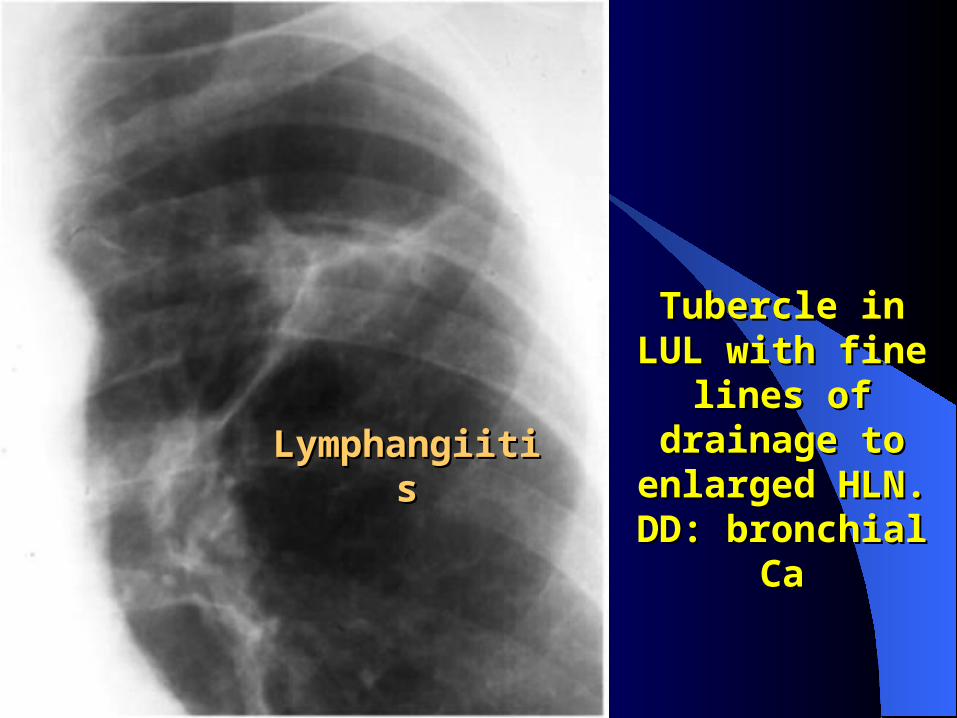
LymphangiitisLymphangiitis
Tubercle in LUL with Tubercle in LUL with fine lines of fine lines of drainage to drainage to
enlarged HLN. DD: enlarged HLN. DD: bronchial Cabronchial Ca
37
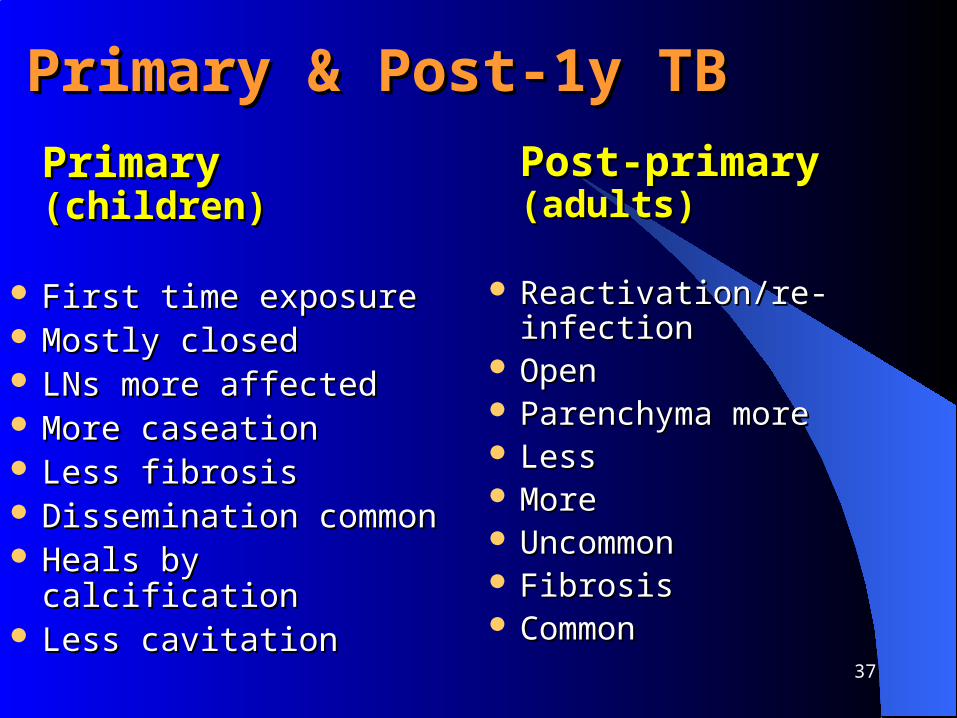
Primary & Post-1y TB Primary & Post-1y TB Primary Primary (children)(children)
First time exposureFirst time exposure Mostly closed Mostly closed LNs more affected LNs more affected More caseation More caseation Less fibrosisLess fibrosis Dissemination commonDissemination common Heals by calcificationHeals by calcification Less cavitation Less cavitation
Post-primary Post-primary (adults)(adults)
Reactivation/re-infection Reactivation/re-infection OpenOpen Parenchyma moreParenchyma more LessLess MoreMore UncommonUncommon FibrosisFibrosis Common Common

38
Big Big tuberculomatuberculoma
39
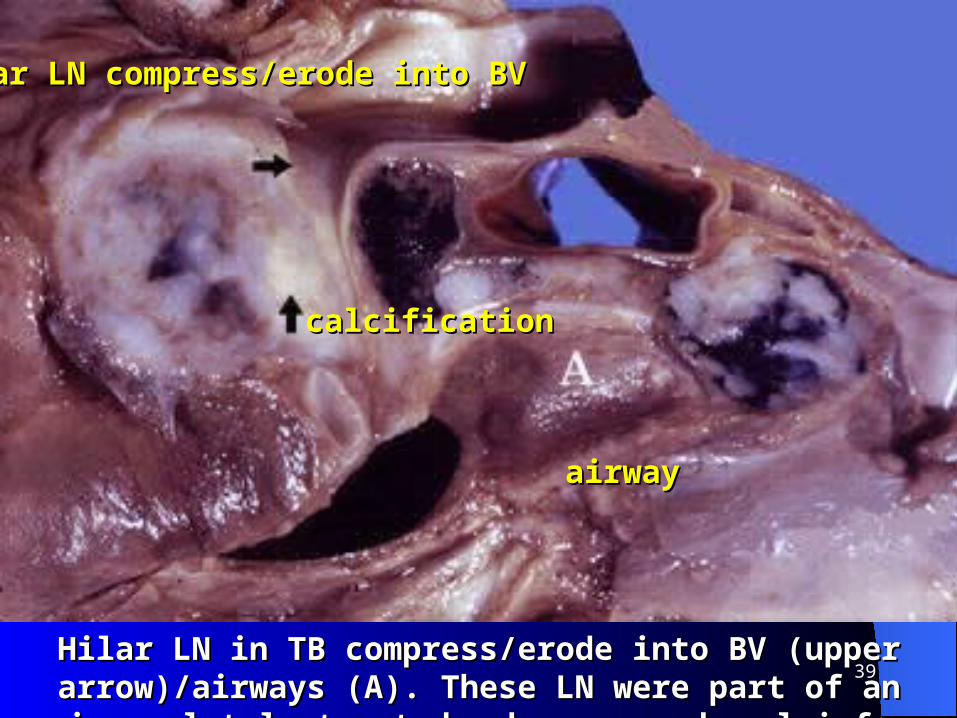
airwayairway
calcificationcalcification
Hilar LN compress/erode into BV Hilar LN compress/erode into BV
Hilar LN in TB compress/erode into BV (upper arrow)/airways (A). Hilar LN in TB compress/erode into BV (upper arrow)/airways (A). These LN were part of an incompletely treated, chr. parenchymal inf.These LN were part of an incompletely treated, chr. parenchymal inf.
40
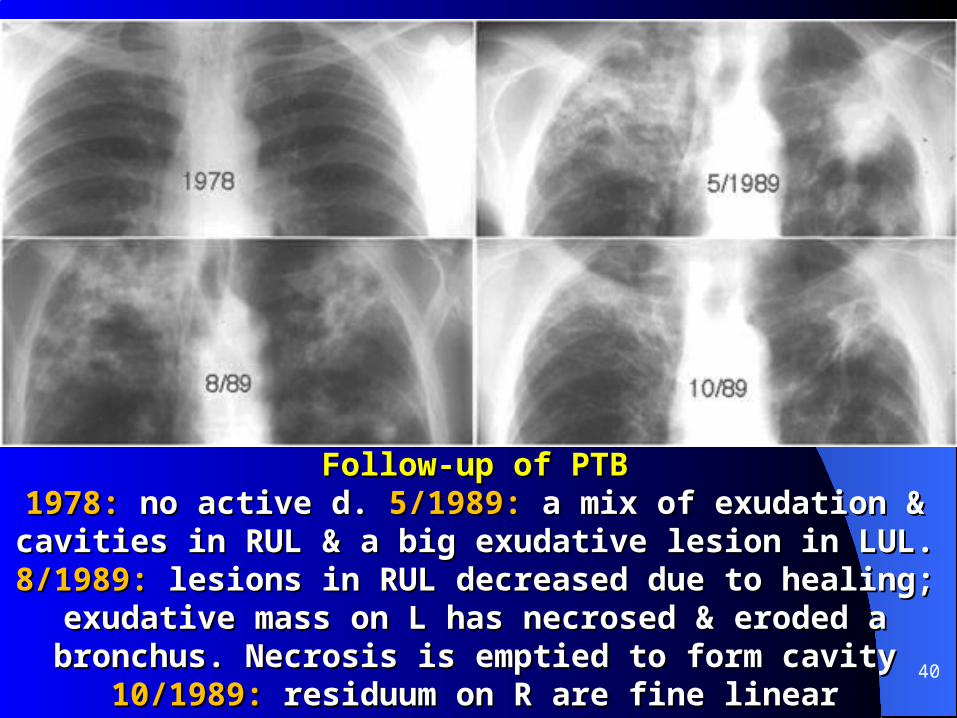
Follow-up of PTBFollow-up of PTB1978: 1978: no active d. no active d. 5/1989: 5/1989: a mix of exudation & cavities in RUL & a big a mix of exudation & cavities in RUL & a big
exudative lesion in LUL. exudative lesion in LUL. 8/1989: 8/1989: lesions in RUL decreased due to lesions in RUL decreased due to healing; exudative mass on L has necrosed & eroded a bronchus. healing; exudative mass on L has necrosed & eroded a bronchus.
Necrosis is emptied to form cavityNecrosis is emptied to form cavity10/1989: 10/1989: residuum on R are fine linear opacities. L cavity shrunk & the residuum on R are fine linear opacities. L cavity shrunk & the
surrounding consolidations have resolved surrounding consolidations have resolved

41
““Tree in` bud"Tree in` bud"
CT: CT: ill-defined small nodules adjacent to peripheral bronchi: ill-defined small nodules adjacent to peripheral bronchi: calledcalled tree in bud tree in bud

42CXR & CT of a cavity CXR & CT of a cavity in the apical segment of RUL (K). The draining in the apical segment of RUL (K). The draining
bronchus is visible (arrow). CT (2mm slice)bronchus is visible (arrow). CT (2mm slice)
43
Immunity in TB Immunity in TB
Immunity is complex & Immunity is complex & incompleteincomplete:: CMICMI Humoral: Humoral: many antibodiesmany antibodies MO may stay viable inside healed LN for decades; MO may stay viable inside healed LN for decades;
unmasks when immunity fallsunmasks when immunity falls
44
Fate of Primary ComplexFate of Primary Complex
Best described in PTBBest described in PTB
Primary focus: mostly Primary focus: mostly healsheals (70%; calcified). If (70%; calcified). If progress progress cavity, bronchiectasis, bleed cavity, bronchiectasis, bleed
DiseaseDisease from focus & LNfrom focus & LN DisseminationDissemination within 6mowithin 6mo ComplicationsComplications:: LAP & 1y focusLAP & 1y focus

45PTB with large cavitationPTB with large cavitation

46
CXR & CT of productive TB with multiple nodules (nodules of CXR & CT of productive TB with multiple nodules (nodules of MTB are smaller)MTB are smaller)

47
PressurePressure by enlarged LN by enlarged LN Stridor, wheeze, hoarsenessStridor, wheeze, hoarseness DysphagiaDysphagia Bronchiectasis, collapse, emphysemaBronchiectasis, collapse, emphysema
Discharge Discharge of Caseous Materialsof Caseous Materials Into BV, lymphatics: Into BV, lymphatics: disseminated TBdisseminated TB Into bronchus: Into bronchus: TB Br.Pn. (endobronchial TB)TB Br.Pn. (endobronchial TB) Fistula, pl. effusion, pneumothoraxFistula, pl. effusion, pneumothorax Severe hgeSevere hge
Complications: LNComplications: LN
Caseation LN (matted)Caseation LN (matted)
48
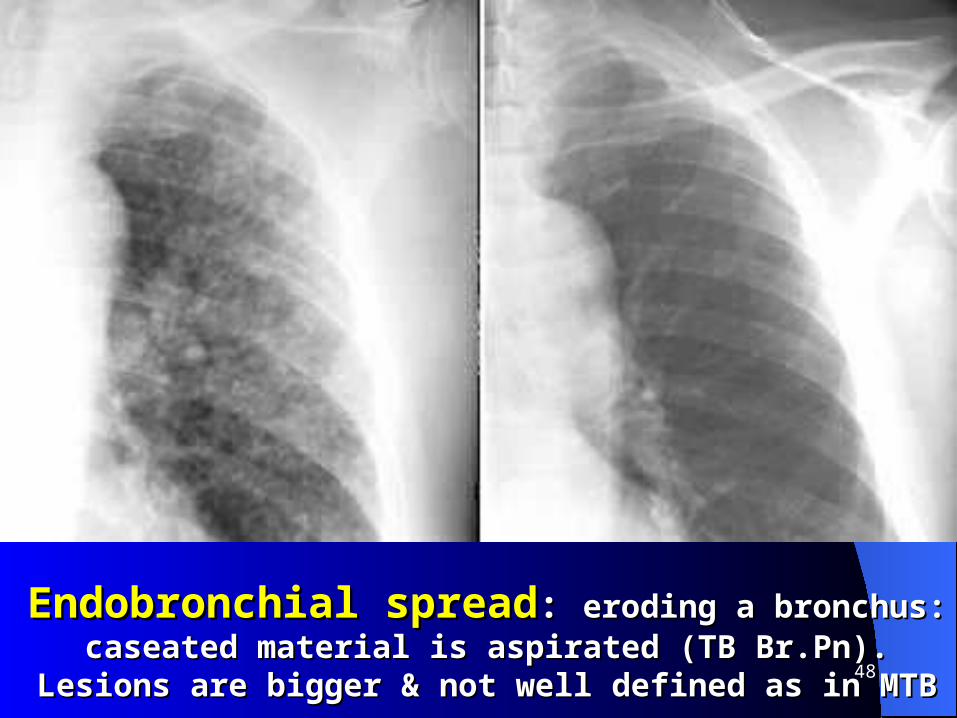
Endobronchial spreadEndobronchial spread: : eroding a bronchus: caseated material is eroding a bronchus: caseated material is aspirated (TB Br.Pn). Lesions are bigger & not well defined as in MTBaspirated (TB Br.Pn). Lesions are bigger & not well defined as in MTB

49Gross emphysema
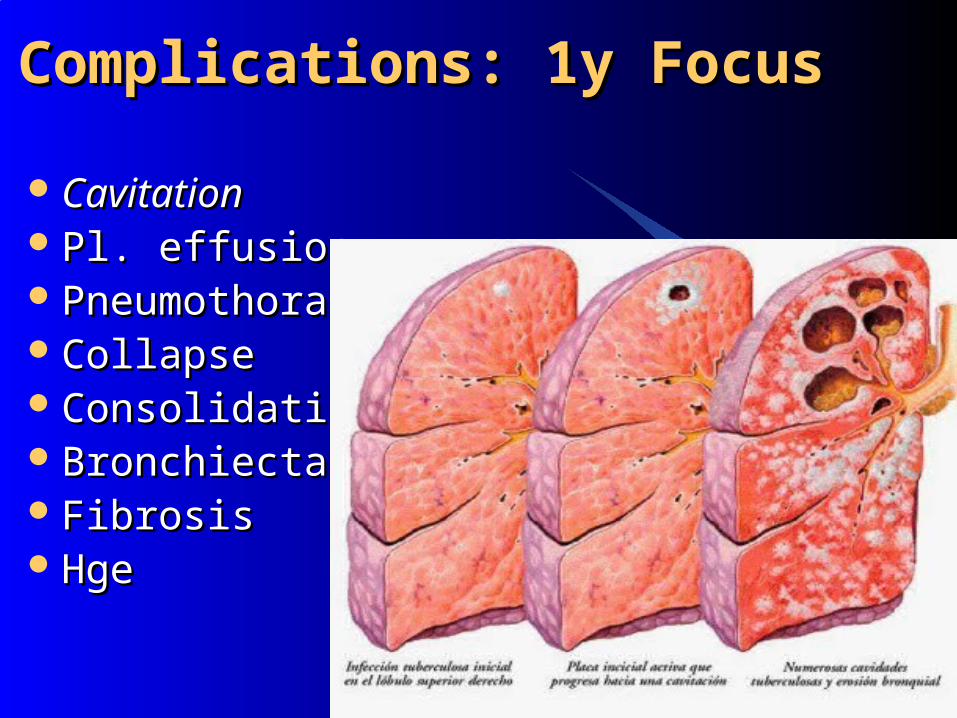
Complications: 1y FocusComplications: 1y Focus
CavitationCavitation Pl. effusionPl. effusion PneumothoraxPneumothorax CollapseCollapse ConsolidationConsolidation BronchiectasisBronchiectasis FibrosisFibrosis HgeHge

51
PTB PTB pneumothoraxpneumothorax
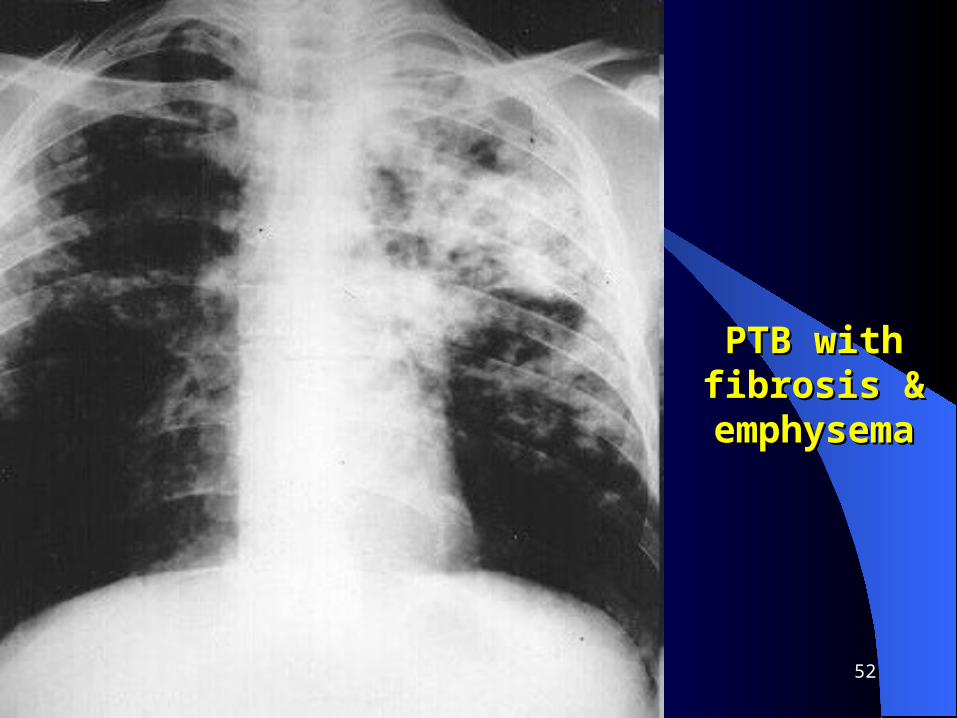
52
PTB with fibrosis PTB with fibrosis & emphysema& emphysema
53
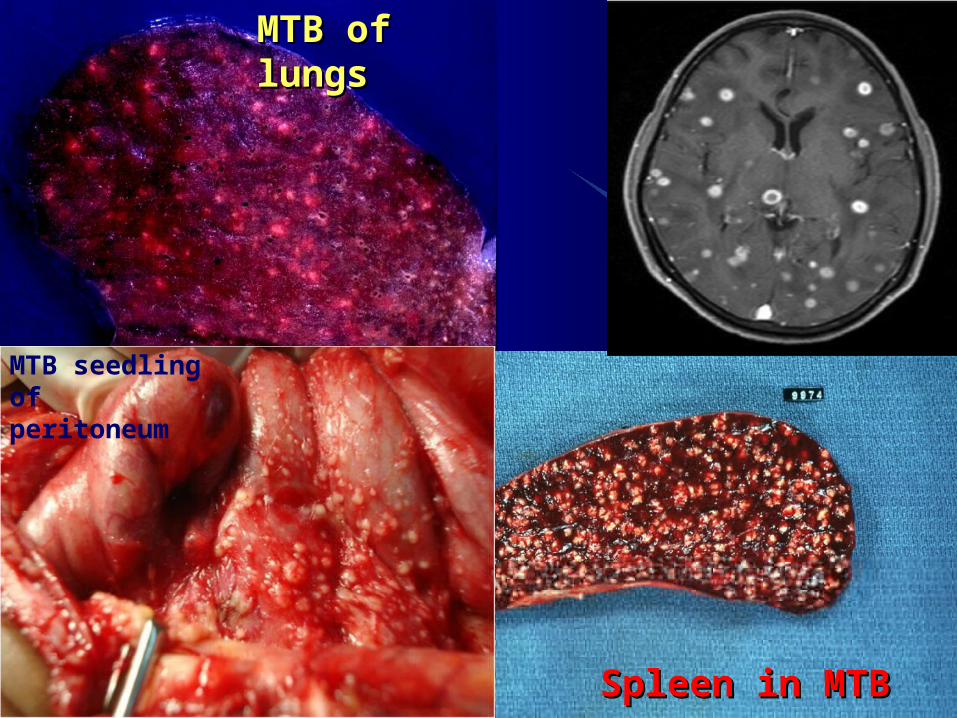
Disseminated TB Disseminated TB
Within 2-6mo of 1y inf.Within 2-6mo of 1y inf. Commonly venous; occasionally arterial Commonly venous; occasionally arterial ((local MTB)local MTB) Endobronchial:Endobronchial: ac. TB Br.Pn ac. TB Br.Pn May be asymptomatic: May be asymptomatic: balance of inf.balance of inf.~~defencedefence 2 gravest forms: ac. MTB & TBM2 gravest forms: ac. MTB & TBM Multi-organMulti-organ features. M features. Mainly liver, kidneys, other parts ainly liver, kidneys, other parts
of lungs, skin, LN, brain, etc. of lungs, skin, LN, brain, etc.
Bone, uro-genital involvement very latelyBone, uro-genital involvement very lately

54Newborn with MTB (mother had active TB)Newborn with MTB (mother had active TB)
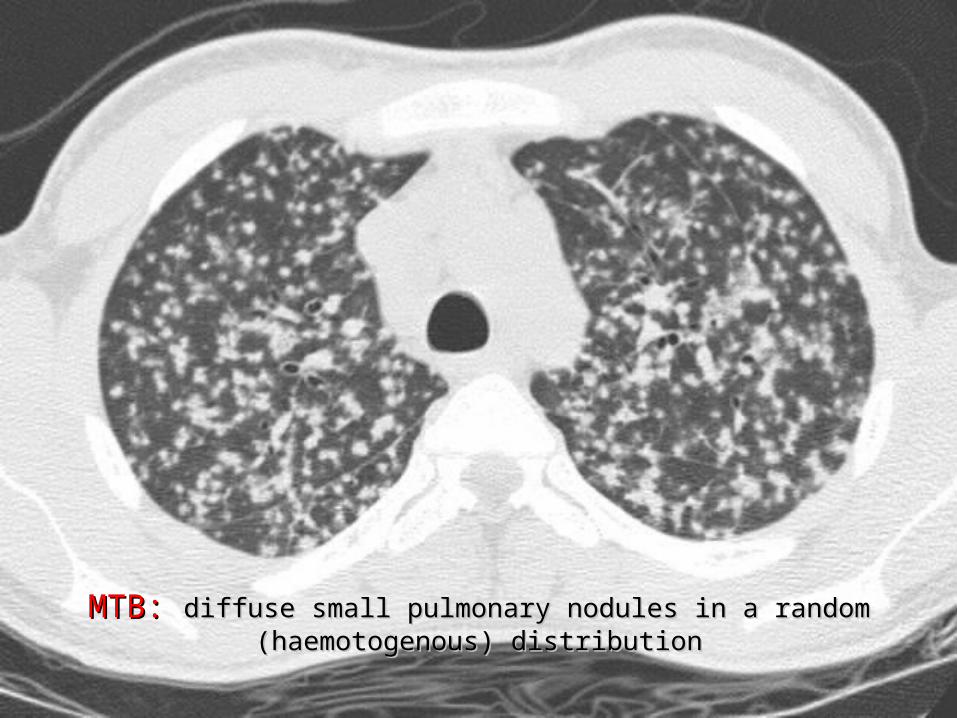
MTB: MTB: diffuse small pulmonary nodules in a random (haemotogenous) distributiondiffuse small pulmonary nodules in a random (haemotogenous) distribution
56
MTB of lungsMTB of lungs
Spleen in MTBSpleen in MTB
MTB seedling of peritoneum
57
TB Pleural Effusion TB Pleural Effusion (exudative)(exudative)
Localized PE is part of primary TBLocalized PE is part of primary TB Huge exudation may occurHuge exudation may occur Ac. onset, fever, chest pain, SoBAc. onset, fever, chest pain, SoB Diminished chest movement & B. SoundDiminished chest movement & B. Sound Stony dull percussion noteStony dull percussion note
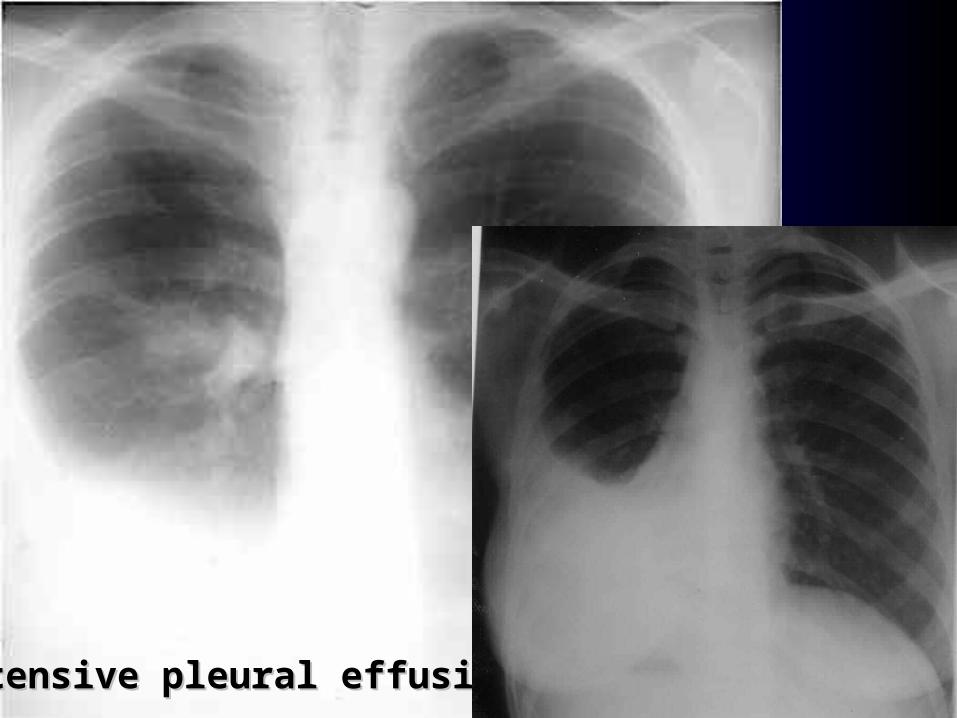
58Extensive pleural effusionExtensive pleural effusion

59
Clinical Features TBClinical Features TB
Predisposing factors Predisposing factors Age U-5, 15-45 Age U-5, 15-45 General features: General features: Organ specific features:Organ specific features:

60
GeneralGeneral Evening F, night sweatsEvening F, night sweats ANV, wt. loss, fatigue, lassitude,ANV, wt. loss, fatigue, lassitude, loss of initiativeloss of initiative HA, irritability, chr. ill health, GLAP, etc.HA, irritability, chr. ill health, GLAP, etc.
Organ specificOrgan specific PTB: PTB: chr. cough, hemoptysischr. cough, hemoptysis Abdo. TB: Abdo. TB: RAP, distension, diarrhea, constipationRAP, distension, diarrhea, constipation Bone TB: Bone TB: arthritis, gibbousarthritis, gibbous CNS TB: CNS TB: HA, epilepsy. HA, epilepsy. Skin: Skin: L. vulgarisL. vulgaris Renal TB: Renal TB: hematuria, etchematuria, etc TBM: TBM: slow onset of meningitisslow onset of meningitis
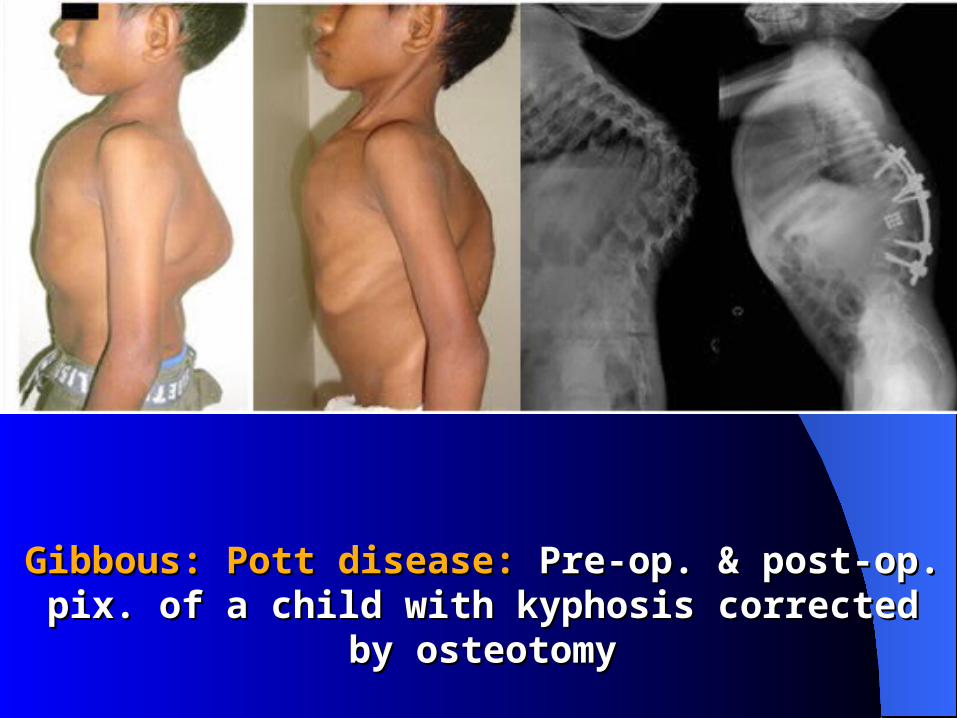
Gibbous: Pott disease: Gibbous: Pott disease: Pre-op. & post-op. pix. of a child with Pre-op. & post-op. pix. of a child with kyphosis corrected by osteotomykyphosis corrected by osteotomy

Spina ventosa

TB of hip jointTB of hip joint

Skin TB: lupus vulgarisSkin TB: lupus vulgaris
TB of Skin (verrucosa cutis)TB of Skin (verrucosa cutis)
Scrofuloderma: chr. effect of skin overlying Scrofuloderma: chr. effect of skin overlying a TB process, typically LAP, osteoarticular d. a TB process, typically LAP, osteoarticular d.
or epididymitis. Subcut. TB leads to cold or epididymitis. Subcut. TB leads to cold abscessabscess
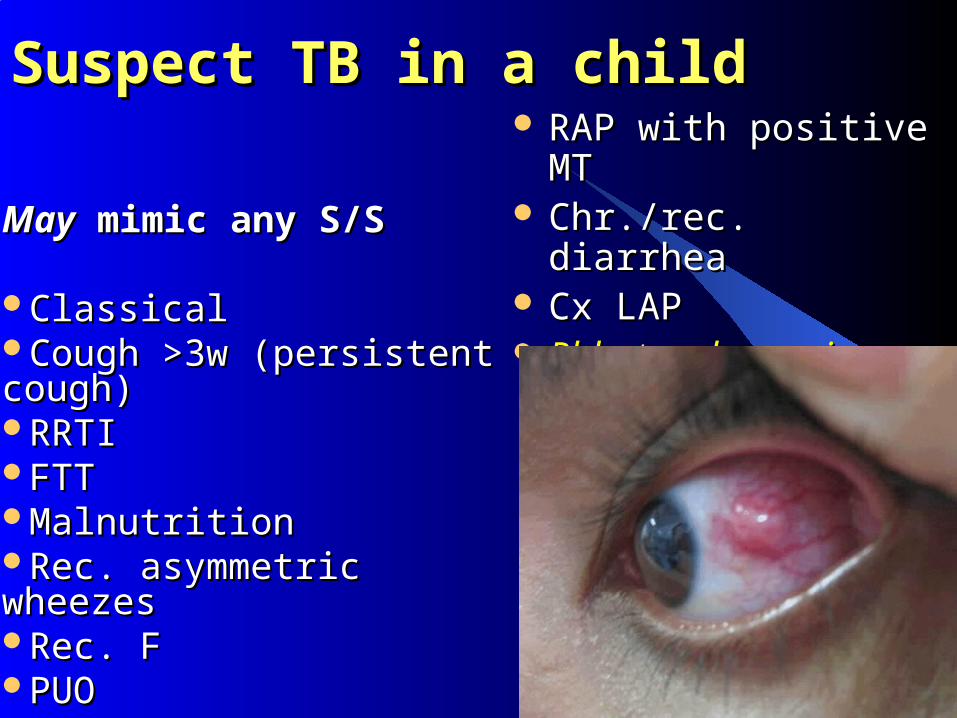
Suspect TB in a child Suspect TB in a child
MayMay mimic any S/S mimic any S/S
ClassicalClassicalCough >3w (persistent cough)Cough >3w (persistent cough)RRTIRRTIFTTFTTMalnutrition Malnutrition Rec. asymmetric wheezesRec. asymmetric wheezesRec. FRec. FPUOPUO
RAP with positive MTRAP with positive MT Chr./rec. diarrhea Chr./rec. diarrhea Cx LAP Cx LAP Phlyctenular conj.Phlyctenular conj.
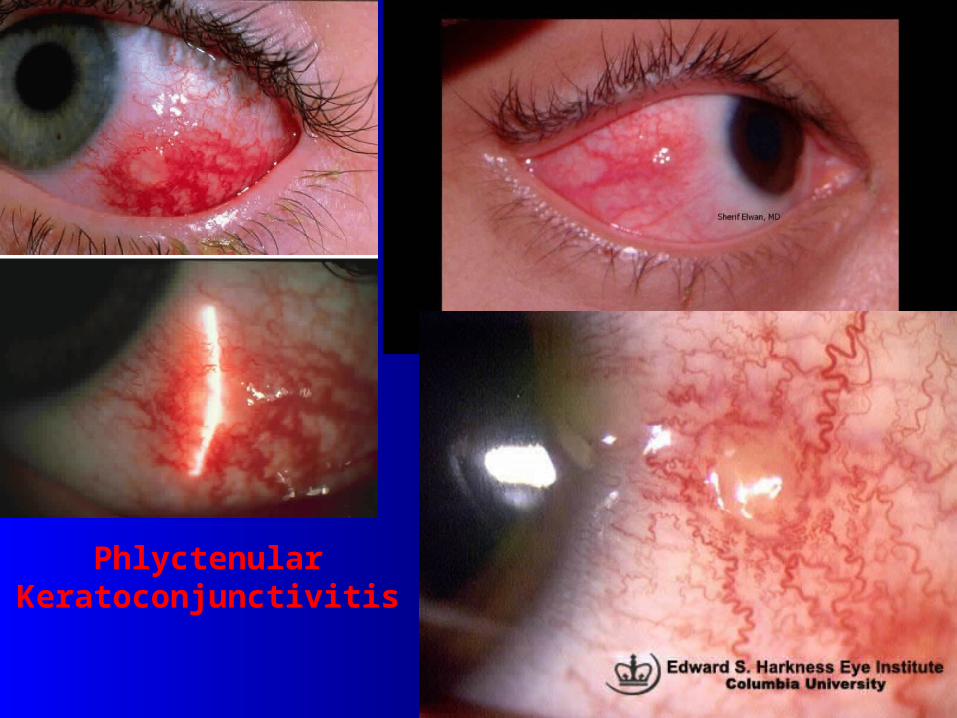
Phlyctenular Keratoconjunctivitis
67
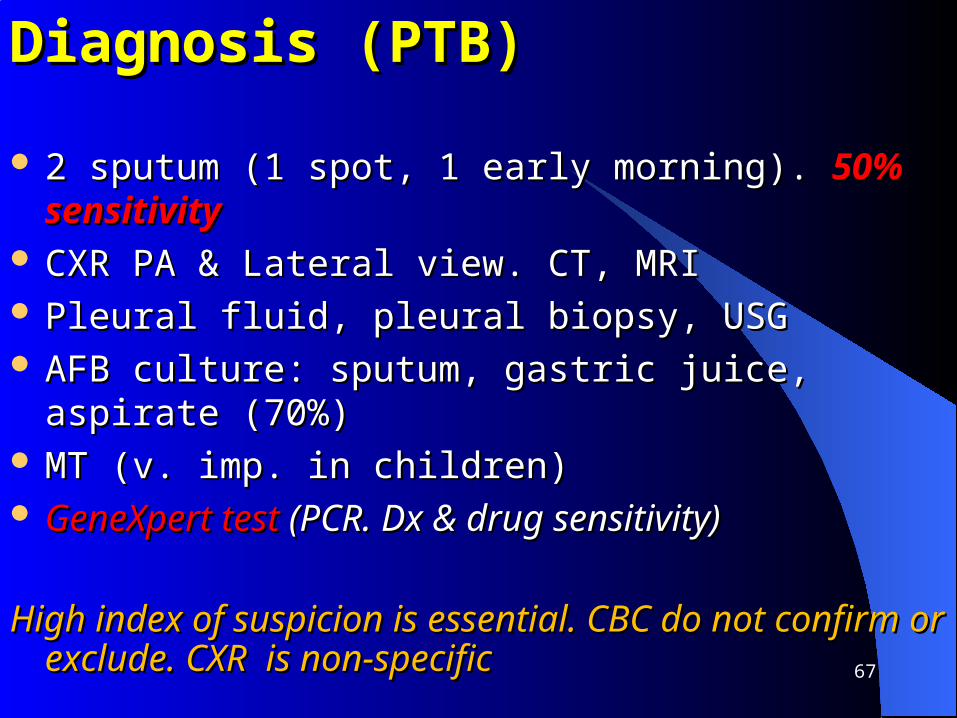
Diagnosis (PTB)Diagnosis (PTB)
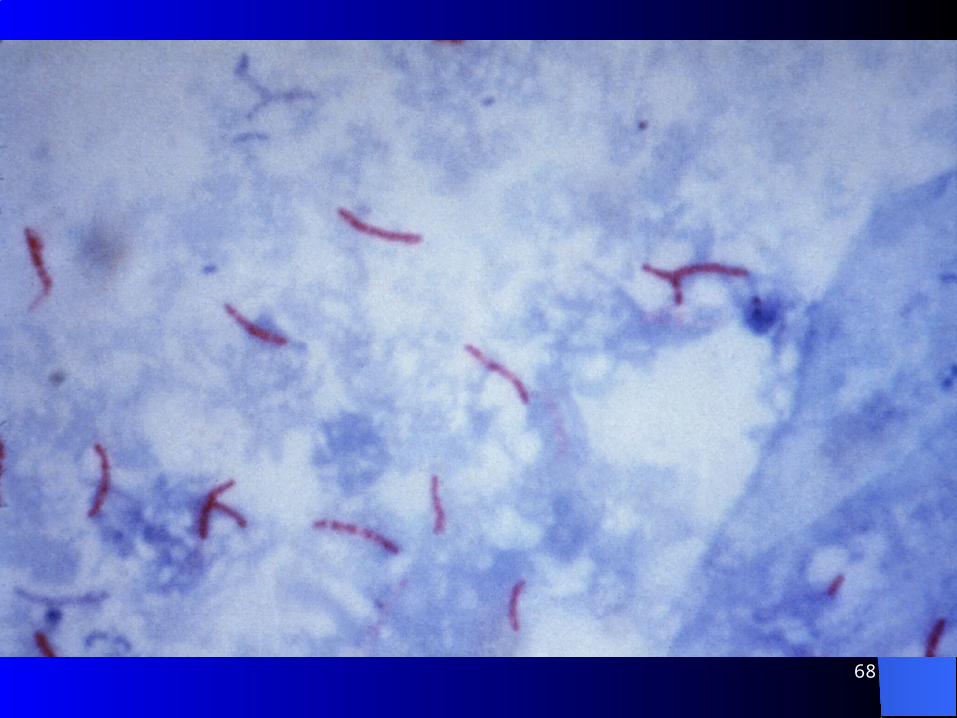
2 sputum (1 spot, 1 early morning). 2 sputum (1 spot, 1 early morning). 50% sensitivity50% sensitivity CXR PA & Lateral view. CT, MRICXR PA & Lateral view. CT, MRI Pleural fluid, pleural biopsy, USGPleural fluid, pleural biopsy, USG AFB culture: sputum, gastric juice, aspirate (70%)AFB culture: sputum, gastric juice, aspirate (70%) MT (v. imp. in children)MT (v. imp. in children) GeneXpert test GeneXpert test (PCR. Dx & drug sensitivity)(PCR. Dx & drug sensitivity)
High index of suspicion is essential. CBC do not confirm or High index of suspicion is essential. CBC do not confirm or exclude. CXR is non-specificexclude. CXR is non-specific
68

Tuberculin Skin Testing (TST)/Mantoux TST (MT) Tuberculin Skin Testing (TST)/Mantoux TST (MT)
Standard method to know inf. with Standard method to know inf. with M tbM tbV. imp. in children. Stronger MT: more active TBV. imp. in children. Stronger MT: more active TB0.1 ml PPD i.d.:0.1 ml PPD i.d.: needle bevel facing up needle bevel facing up (pale wheal 6-10mm)(pale wheal 6-10mm)Read 48-72h later. If pt. does not return: repeatRead 48-72h later. If pt. does not return: repeatMeasure induration, Measure induration, not erythema in mm. in long axisnot erythema in mm. in long axisCI: CI: severe reaction (necrosis, blistering, anaphylaxis, or severe reaction (necrosis, blistering, anaphylaxis, or
ulcerations) to a previous TSTulcerations) to a previous TSTBCG:BCG: reacts up to 3yreacts up to 3y
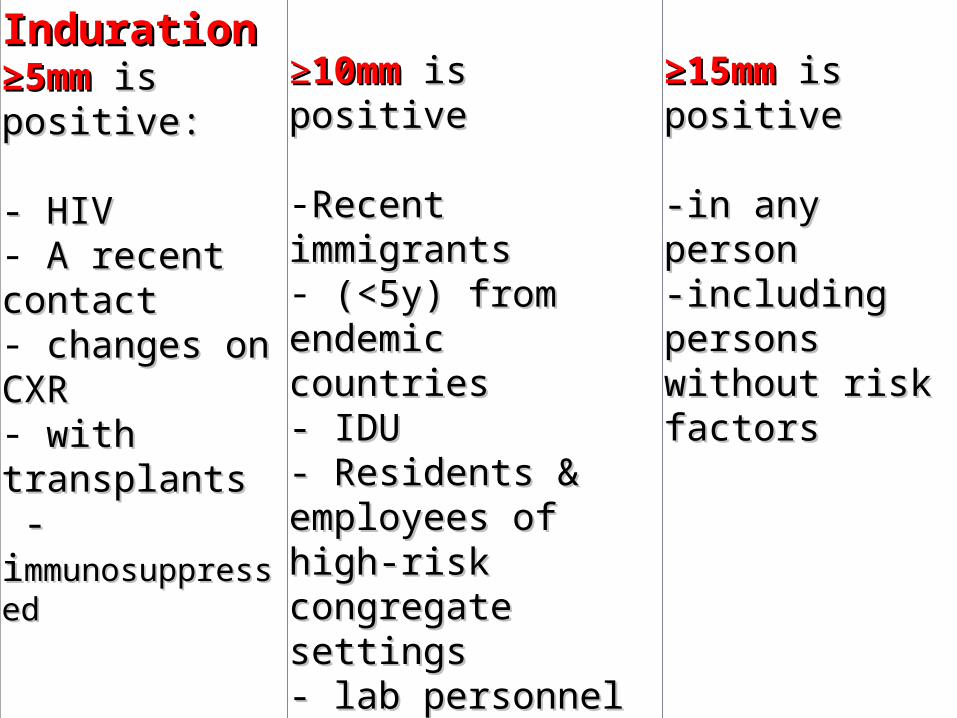
IndurationInduration≥≥5mm5mm is positive: is positive:
- HIV- HIV- A recent contactA recent contact- changes on CXRchanges on CXR- with transplantswith transplants -i-immunosuppressedmmunosuppressed
≥≥10mm10mm is positive is positive
-Recent immigrantsRecent immigrants- (<5y) from endemic (<5y) from endemic countriescountries- IDU- IDU- Residents & - Residents & employees of high-risk employees of high-risk congregate settingscongregate settings- lab personnel- lab personnel- Infants, children, & - Infants, children, & adolescents exposed to adolescents exposed to adults in high-risk adults in high-risk categoriescategories
≥≥15mm 15mm is positive is positive
-in any person-in any person-including persons -including persons without risk without risk factorsfactors

False-Positive ReactionsFalse-Positive ReactionsNon-TB mycobacteriaNon-TB mycobacteriaBCG vaccinationBCG vaccinationIncorrect method, - interpretation, - antigenIncorrect method, - interpretation, - antigen
False-Negative ReactionsFalse-Negative ReactionsFaulty tech.(Faulty tech.(commonest), commonest), anergy, malnutrition, anergy, malnutrition, First 6–10w of inf.First 6–10w of inf.Severe sys. d., immunosuppression Severe sys. d., immunosuppression V. old TB inf. (many years)V. old TB inf. (many years)<6mo age; overwhelming d<6mo age; overwhelming disseminated TBisseminated TBRecent live-virus vax (measles & smallpox)Recent live-virus vax (measles & smallpox)Some viral illnesses (measles & chicken pox)Some viral illnesses (measles & chicken pox)
How Often Can TSTs Be Repeated? How Often Can TSTs Be Repeated? NNo risk to repeato risk to repeatWhat is a Boosted Reaction?What is a Boosted Reaction?Reaction to PPD may wane over time (false-negative). But, Reaction to PPD may wane over time (false-negative). But,
TST may stimulate the immune sys, causing a boosted TST may stimulate the immune sys, causing a boosted reaction later (2-step testing)reaction later (2-step testing)
It is useful for HCW/nursing home residentsIt is useful for HCW/nursing home residents
Can TSTs Be Given To Persons Receiving Vax?Can TSTs Be Given To Persons Receiving Vax?Vax–live-viruses may interfere with TSTVax–live-viruses may interfere with TSTDo it either on the same day of vax or 4-6w laterDo it either on the same day of vax or 4-6w laterDo it at least 1mo after smallpox vaxDo it at least 1mo after smallpox vax

73

74
75
Other testsOther tests
Gastric aspirateGastric aspirate ICTICT Inflammatory fluidInflammatory fluid PCRPCR FNACFNAC BiopsyBiopsyALSALS
ALSALS (Antibodies in lymphocyte secretion)(Antibodies in lymphocyte secretion)
AdvantagesAdvantages Sensitivity >93 %; correlate clinically; an early biomarker Sensitivity >93 %; correlate clinically; an early biomarker
of active infectionof active infection Rapid detection of active TBRapid detection of active TB Diseased specimen not requiredDiseased specimen not required May be preserved for long timeMay be preserved for long time
DisadvantagesDisadvantages Cannot be applied if MT done within 40dCannot be applied if MT done within 40d It is a complementary test to other testsIt is a complementary test to other tests Rx is not given if only ALS is positiveRx is not given if only ALS is positive

77
TreatmentTreatmentAIMSAIMS To cure, prevent disabilityTo cure, prevent disability To prevent relapse, drug resistance & toxicityTo prevent relapse, drug resistance & toxicity To prevent transmissionTo prevent transmission RehabilitationRehabilitation
RxRx Specific Specific Supportive Supportive Rx of complications Rx of complications
MDR Rx costs x100MDR Rx costs x100. . Right dosage, duration & combination of drugs are Right dosage, duration & combination of drugs are essential essential
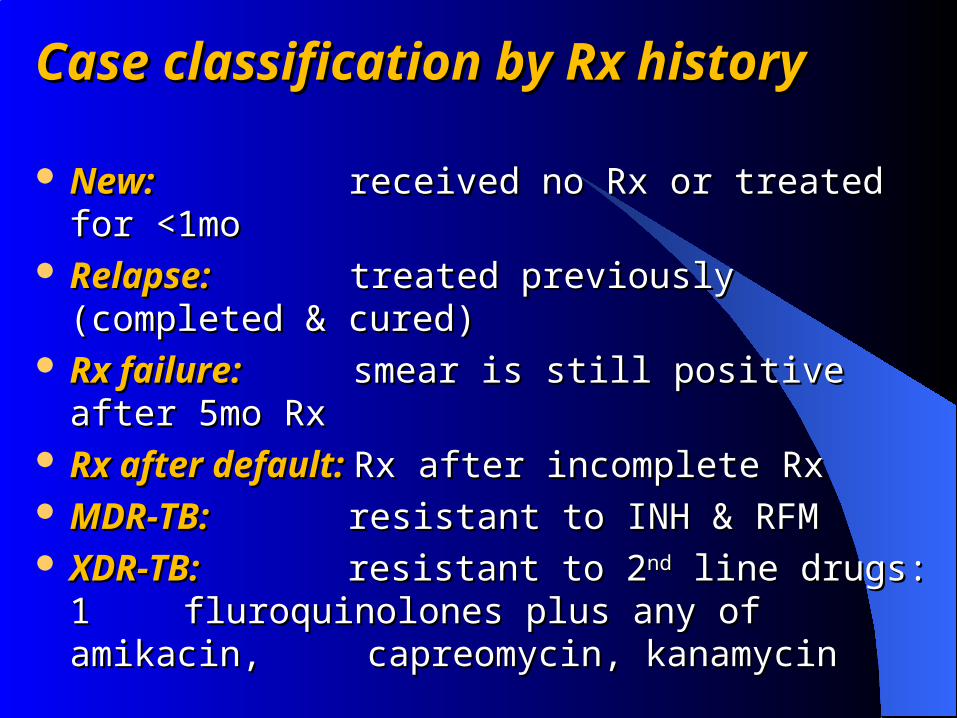
Case classification by Rx historyCase classification by Rx history
New: New: received no Rx or treated for <1moreceived no Rx or treated for <1mo Relapse: Relapse: treated previously (completed & cured)treated previously (completed & cured) Rx failure: Rx failure: smear is still positive after 5mo Rxsmear is still positive after 5mo Rx Rx after default: Rx after default: Rx after incomplete RxRx after incomplete Rx MDR-TB: MDR-TB: resistant to INH & RFMresistant to INH & RFM XDR-TB: XDR-TB: resistant to 2resistant to 2ndnd line drugs: 1 line drugs: 1
fluroquinolones plus any of amikacin, fluroquinolones plus any of amikacin, capreomycin, kanamycin capreomycin, kanamycin

79
Directly Observed Therapy (DOT)Directly Observed Therapy (DOT) ATD are given directly to the pt. by HW ATD are given directly to the pt. by HW (not friend) (not friend) & &
documented. Prevent DR & spreaddocumented. Prevent DR & spread Non-cooperation is Non-cooperation is rarerare & illegal (PH law) & illegal (PH law) Coverage in Bangladesh 99%Coverage in Bangladesh 99%
5-point package:5-point package:– political commitment, fundpolitical commitment, fund– case detectioncase detection– standard Rx with supervision & supportstandard Rx with supervision & support– effective drug supplyeffective drug supply– monitoringmonitoring


81

ATD ATD
First line:First line: Rifampicin, INH, streptomycinRifampicin, INH, streptomycin 22ndnd line: line: Thiacetazone, PZA, ethambutolThiacetazone, PZA, ethambutol
Reserved:Reserved: ethionamide, PAS, amikacin, prothionamide, ethionamide, PAS, amikacin, prothionamide, cycloserine, ciprofloxacin, ofloxacin, capreomycincycloserine, ciprofloxacin, ofloxacin, capreomycin
They are safe & well tolerated; SE are uncommon in children; They are safe & well tolerated; SE are uncommon in children; no routine LFT, no routine B6no routine LFT, no routine B6
PZA: pyrazinamide. PAS: PZA: pyrazinamide. PAS: p-p-aminosalicylic acidaminosalicylic acid
83
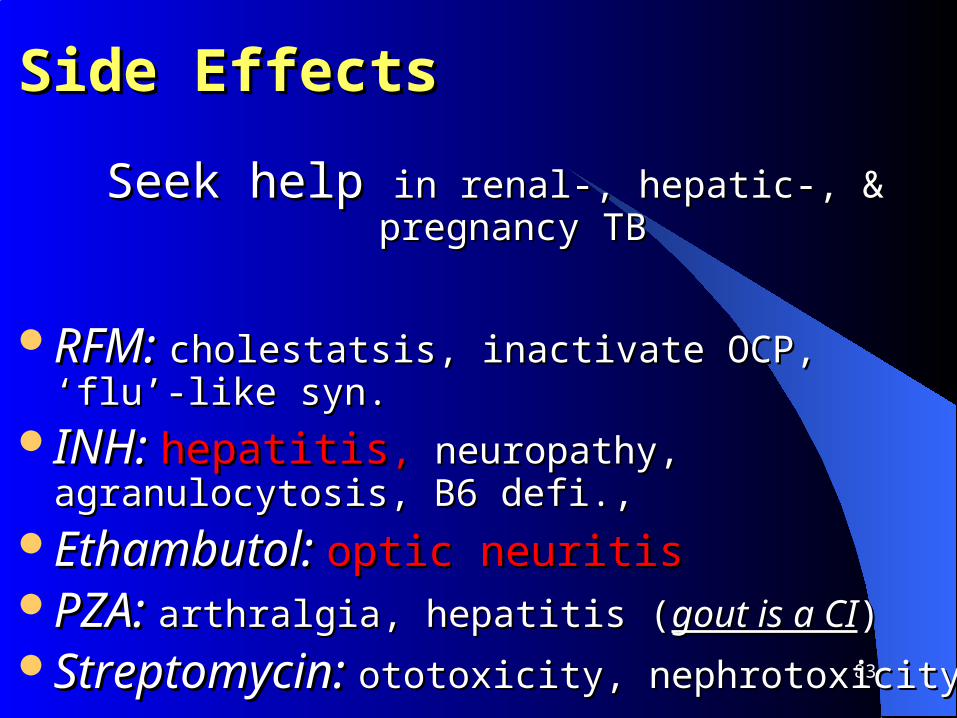
Side Effects Side Effects
Seek help Seek help in renal-, hepatic-, & pregnancy TBin renal-, hepatic-, & pregnancy TB
RFM: RFM: cholestatsis, inactivate OCP, ‘flu’-like syn.cholestatsis, inactivate OCP, ‘flu’-like syn.INH: INH: hepatitishepatitis, , neuropathy, agranulocytosis, B6 defi., neuropathy, agranulocytosis, B6 defi., Ethambutol: Ethambutol: optic neuritisoptic neuritisPZA: PZA: arthralgia, hepatitis (arthralgia, hepatitis (gout is a CIgout is a CI))Streptomycin: Streptomycin: ototoxicity, nephrotoxicity ototoxicity, nephrotoxicity
84
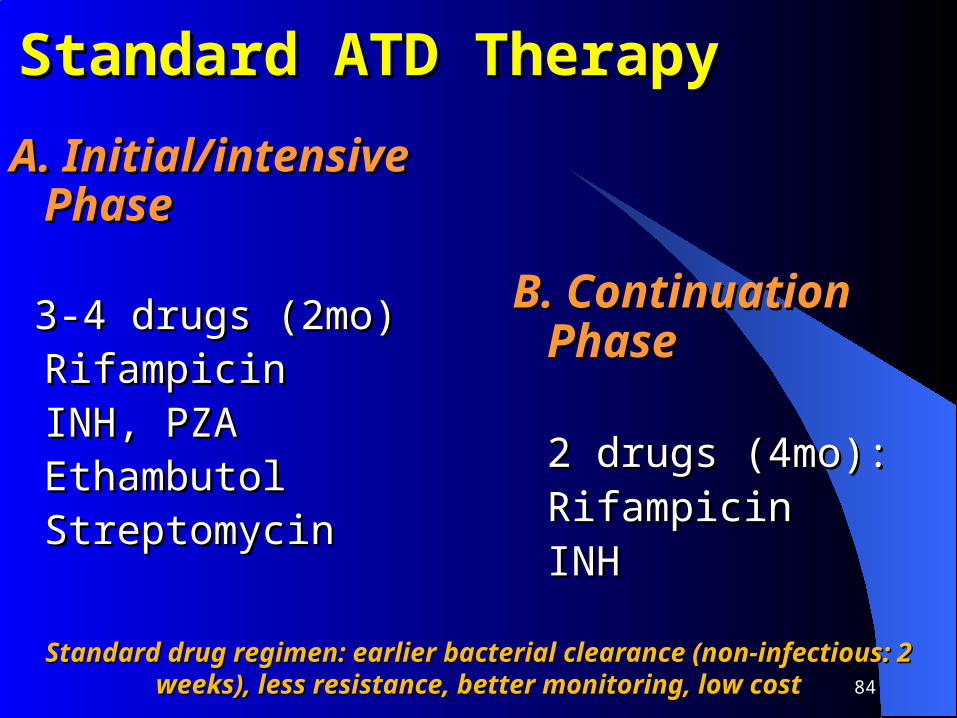
Standard ATD TherapyStandard ATD Therapy
A. Initial/intensive PhaseA. Initial/intensive Phase
3-4 drugs (2mo)3-4 drugs (2mo)RifampicinRifampicinINH, PZAINH, PZAEthambutol Ethambutol StreptomycinStreptomycin
B. Continuation PhaseB. Continuation Phase
2 drugs (4mo):2 drugs (4mo):RifampicinRifampicinINHINH
Standard drug regimen: earlier bacterial clearance (non-infectious: 2 Standard drug regimen: earlier bacterial clearance (non-infectious: 2 weeks), less resistance, better monitoring, low costweeks), less resistance, better monitoring, low cost
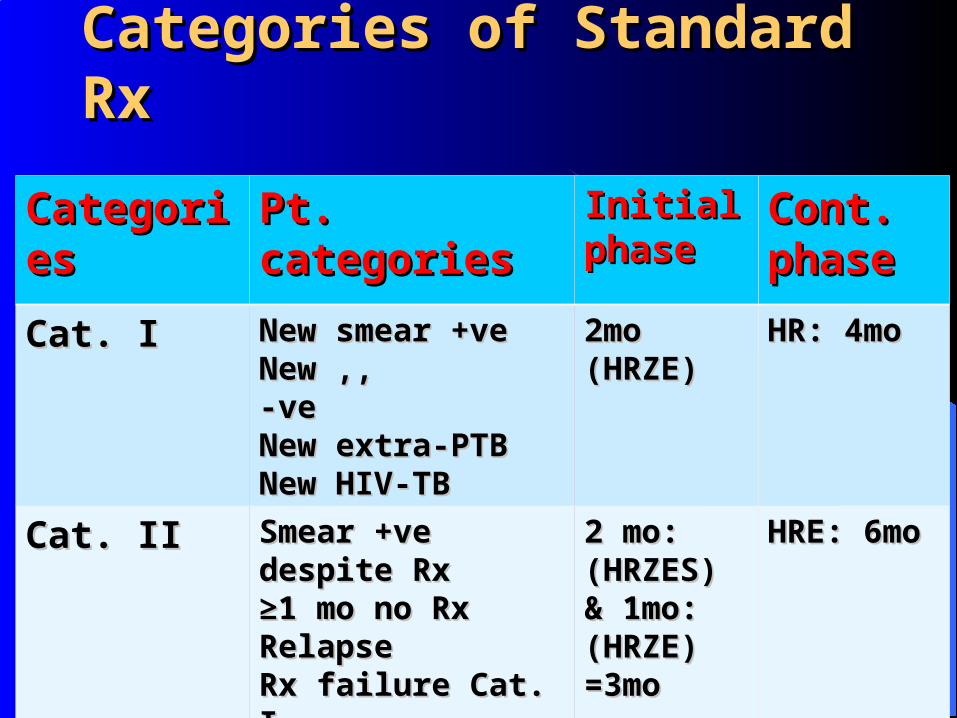
Categories of Standard RxCategories of Standard Rx
CategoriesCategories Pt. categoriesPt. categories Initial Initial phasephase
Cont. Cont. phasephase
Cat. ICat. I New smear +veNew smear +veNew ,, -veNew ,, -veNew extra-PTBNew extra-PTBNew HIV-TBNew HIV-TB
2mo (HRZE)2mo (HRZE) HR: 4moHR: 4mo
Cat. IICat. II Smear +ve despite Rx Smear +ve despite Rx ≥≥1 mo no Rx1 mo no RxRelapseRelapseRx failure Cat. IRx failure Cat. IRx after defaultRx after defaultOthersOthers
2 mo: 2 mo: (HRZES) & (HRZES) & 1mo: (HRZE)1mo: (HRZE)=3mo=3mo
HRE: 6moHRE: 6mo
86
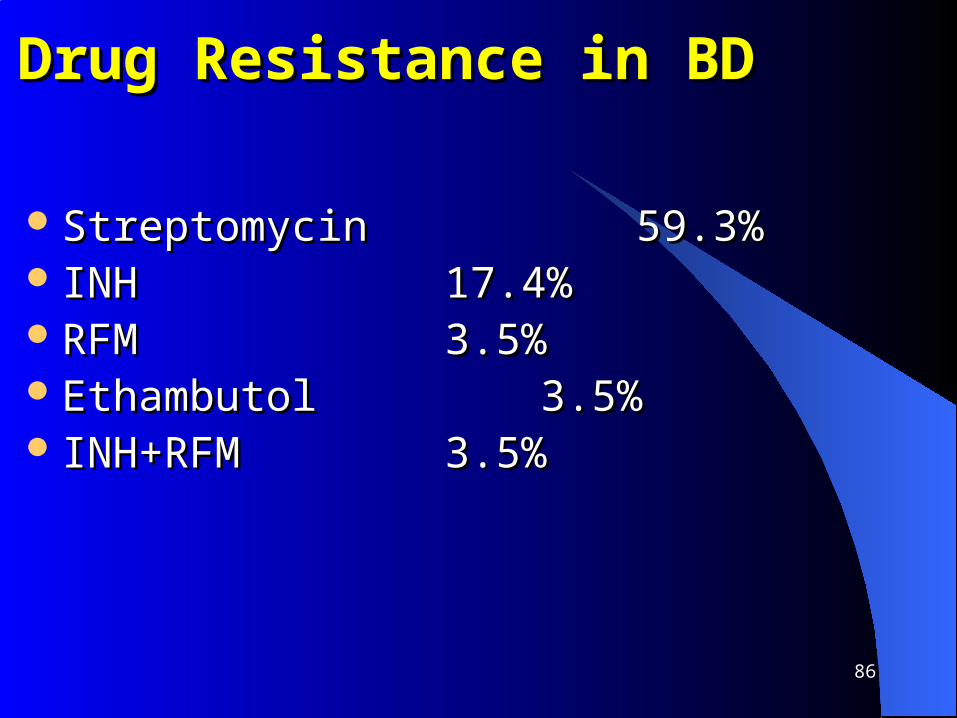
Drug Resistance in BDDrug Resistance in BD
StreptomycinStreptomycin 59.3%59.3% INHINH 17.4%17.4% RFMRFM 3.5%3.5% Ethambutol Ethambutol 3.5%3.5% INH+RFMINH+RFM 3.5%3.5%
87
Supportive RxSupportive Rx
Treatment of symptomsTreatment of symptoms Correction of malnutrition Correction of malnutrition Balanced foodBalanced food Adequate exerciseAdequate exercise RehabilitationRehabilitation
88
Treatment FailureTreatment Failure
Commonest: Commonest: noncompliancenoncompliance MDR/XDR-TBMDR/XDR-TB Inadequate number/dose/duration of drugsInadequate number/dose/duration of drugs Incorrect DxIncorrect Dx
89
Coricosteroids in TBCoricosteroids in TB
Indications: Indications: P. Effusion, TBM, pericarditis, HIV-TB, P. Effusion, TBM, pericarditis, HIV-TB, endobronchial TB, TB adrenal atrophy, MTB, endobronchial TB, TB adrenal atrophy, MTB, compressing TB lymphadenitiscompressing TB lymphadenitisPrednisolone is the DoCPrednisolone is the DoCDoes not shorten duration of RxDoes not shorten duration of Rx1-2 mg/kg/d. 6w in TBM1-2 mg/kg/d. 6w in TBM4-6w with tapering 4-6w with tapering
Advantages: Advantages: TBM:TBM: MM. MM. MTB:MTB: improves GC improves GC dramatically. dramatically. Pericardial E.:Pericardial E.: prevents constriction. prevents constriction. Pl. effusion:Pl. effusion: early relief. early relief. Endobronchial TB:Endobronchial TB: relieves distress relieves distress

Congenital TBCongenital TB
RareRare Primary complex usually lies in the liverPrimary complex usually lies in the liver Dx can be Dx can be difficultdifficult 50% die within 3-4 w50% die within 3-4 w CXR may shows MTB or primary TBCXR may shows MTB or primary TB May be born with primary skin TBMay be born with primary skin TB Mother may have no evidenceMother may have no evidence

PreventionPrevention Contact tracing & Rx are primary goals (13% un-identified)Contact tracing & Rx are primary goals (13% un-identified) BCG vaccinationBCG vaccination Raising living standard, nutrition & health Raising living standard, nutrition & health
educationeducation Cough etiquette & hand washingCough etiquette & hand washing
WHO responseWHO response to to control TB. control TB. Stop TB StrategyStop TB Strategy
Global leadershipGlobal leadership Policies, strategies, standards for Px, Rx, care & control. Policies, strategies, standards for Px, Rx, care & control.
Monitor theseMonitor these FinancingFinancing Provide technical supportProvide technical support Research & dissemination of knowledgeResearch & dissemination of knowledge Facilitate & engage in partnerships for TBFacilitate & engage in partnerships for TB
Stop TB (WHO)
Vision:Vision: A TB-FREE WORLDA TB-FREE WORLD Goal: Goal: to dramatically reduce TB by ‘15 (MDG6)to dramatically reduce TB by ‘15 (MDG6) Objectives:Objectives: universal access to HQ care for all universal access to HQ care for all
– Reduce suffering & SE burden of TBReduce suffering & SE burden of TB– Protect vulnerable popn. from TB, TB-HIV, MDR-TBProtect vulnerable popn. from TB, TB-HIV, MDR-TB
Targets: Targets: – by 2015: reduce cases & deaths by 50%by 2015: reduce cases & deaths by 50%– by 2050: eliminate TB as a PH problemby 2050: eliminate TB as a PH problem

Components of the Stop TB strategyComponents of the Stop TB strategy
1. DOT 1. DOT expansion: expansion: political will, detection & Dx, political will, detection & Dx, standard Rx & support, drug supply, standard Rx & support, drug supply, monitoring monitoring & evaluation& evaluation
2. TB-HIV, MDR-TB, 2. TB-HIV, MDR-TB, & the needs of poor popn.: & the needs of poor popn.: sscale-up collaborative TB/HIV activities, scale-cale-up collaborative TB/HIV activities, scale-up prevention & management of MDR-TB, up prevention & management of MDR-TB, address TB contacts, & needs of poor & address TB contacts, & needs of poor & vulnerable peoplevulnerable people
3. Strengthening primary HC: 3. Strengthening primary HC: improve policies, improve policies, develop HW, effective running; infx. control, develop HW, effective running; infx. control, lab networkslab networks
4. Engage all care providers: 4. Engage all care providers: involve all; promote involve all; promote International Standards for TB CareInternational Standards for TB Care
5. Empower people about TB5. Empower people about TB:: communication & communication & social mobilization; community participationsocial mobilization; community participation
6. Research: 6. Research: operational research; research to operational research; research to develop Dx, drugs, Vaxdevelop Dx, drugs, Vax

MDR-TBMDR-TB
do not respond to INH & rifampicin (2 most powerful)do not respond to INH & rifampicin (2 most powerful) The primary cause is inappropriate RxThe primary cause is inappropriate Rx 2013: globally 480k had MDR-TB: >50% in India, China, 2013: globally 480k had MDR-TB: >50% in India, China,
Russia. 9% MDR-TB are XDR-TBRussia. 9% MDR-TB are XDR-TB
Curable by 2Curable by 2ndnd-line drugs x2y: are limited, not plenty & v -line drugs x2y: are limited, not plenty & v expensive: ~severe SEexpensive: ~severe SE
XDR-TB: responds to fewer drugsXDR-TB: responds to fewer drugs
SummarySummary TB occurs everywhereTB occurs everywhere Mostly PTBMostly PTB It is curable & preventableIt is curable & preventable Spreads by droplets; only a few bacteria can infectSpreads by droplets; only a few bacteria can infect 1/31/3rdrd world popn. infected: world popn. infected: 10% lifetime risk of active TB10% lifetime risk of active TB Immunocompromised has a much higher riskImmunocompromised has a much higher risk One can infect 15 close contacts/yOne can infect 15 close contacts/y Untreated: 2/3Untreated: 2/3rdrd die die

99
Points to PonderPoints to Ponder
TB may mimic any S/S; oTB may mimic any S/S; oftenften under-diagnosed under-diagnosed Most primaries are asymptomaticMost primaries are asymptomatic More prevalent in AIDSMore prevalent in AIDS MDR-TB is almost a MDR-TB is almost a ‘death sentence’‘death sentence’ Treating open cases controls spreadTreating open cases controls spread
Contd. Contd.

100
Infection necessarily is not a diseaseInfection necessarily is not a disease Adult PTB is mostly open, child PTB is closedAdult PTB is mostly open, child PTB is closed Normal CXR, CBC do not exclude PTBNormal CXR, CBC do not exclude PTB TB is an important c/of PUOTB is an important c/of PUO BCG does not prevent TBBCG does not prevent TB
Points to Ponder …Points to Ponder …
101
ComplianceCompliance is essential: is essential:– prevents spreadprevents spread– less drug resistanceless drug resistance– full recoveryfull recovery
Monitoring: DOT, urine colorMonitoring: DOT, urine color Vision check in ethambutol useVision check in ethambutol use
Points to Ponder …Points to Ponder …
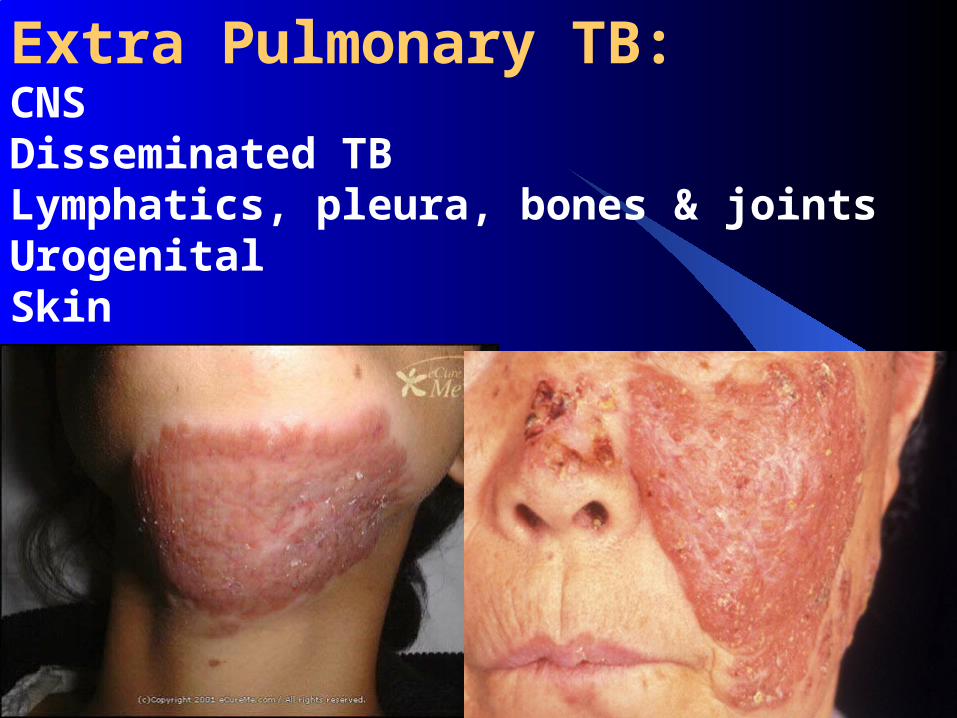
Extra Pulmonary TB:CNSDisseminated TBLymphatics, pleura, bones & jointsUrogenitalSkin

scrofulascrofula


Phlyctenular conjunctivitisPhlyctenular conjunctivitis



OSPEOSPE
Look at the CXR of a child whose mother has Look at the CXR of a child whose mother has persistent cough, irregular F, & wt losspersistent cough, irregular F, & wt loss
1.1. What abnormalities you find?What abnormalities you find?2.2. How do you confirm your Dx?How do you confirm your Dx?3.3. What are the complications of the primary infx.?What are the complications of the primary infx.?4.4. How do you treat?How do you treat?

109
Answer KeysAnswer Keys
Miliary mottling in both lung fieldsMiliary mottling in both lung fields MT, gastric/tracheal aspirate for CS, PCR, ALSMT, gastric/tracheal aspirate for CS, PCR, ALS Complications from primary focus …., enlarged LN Complications from primary focus …., enlarged LN
….. & from caseous material …..….. & from caseous material ….. 4 drug Rx for minimum 6mo4 drug Rx for minimum 6mo

MCQMCQ
BCG vax. prevents TBBCG vax. prevents TB Childhood TB is mostly contagiousChildhood TB is mostly contagious Normal CXR excludes PTBNormal CXR excludes PTB Normal CBC excludes TBNormal CBC excludes TB Commonest c/of pseudo-negative MT is faulty Commonest c/of pseudo-negative MT is faulty
techniquetechnique TB is an important c/of female infertilityTB is an important c/of female infertility

MCQMCQ
TB can mimic any sign or any symptomTB can mimic any sign or any symptom Most primary infx. healsMost primary infx. heals Use of steroid reduces Rx durationUse of steroid reduces Rx duration Non-compliance is the commonest c/of Rx failureNon-compliance is the commonest c/of Rx failure inadequate Rx is the main c/of MDR-TBinadequate Rx is the main c/of MDR-TB Most TB infx. leads to diseaseMost TB infx. leads to disease


Next Lec.Next Lec.
SALMONELLASALMONELLA

117THANK YOU


















