Childhood asthma
53
-
Upload
mukhtar-jamac -
Category
Health & Medicine
-
view
225 -
download
0
Transcript of Childhood asthma


CHILDHOOD ASTHMACHILDHOOD ASTHMA
FAISAL ABU-EKTEISH, MDFAISAL ABU-EKTEISH, MD
PROFESSOR OF PEDIATRICSPROFESSOR OF PEDIATRICS
CHILDHOOD ASTHMACHILDHOOD ASTHMA
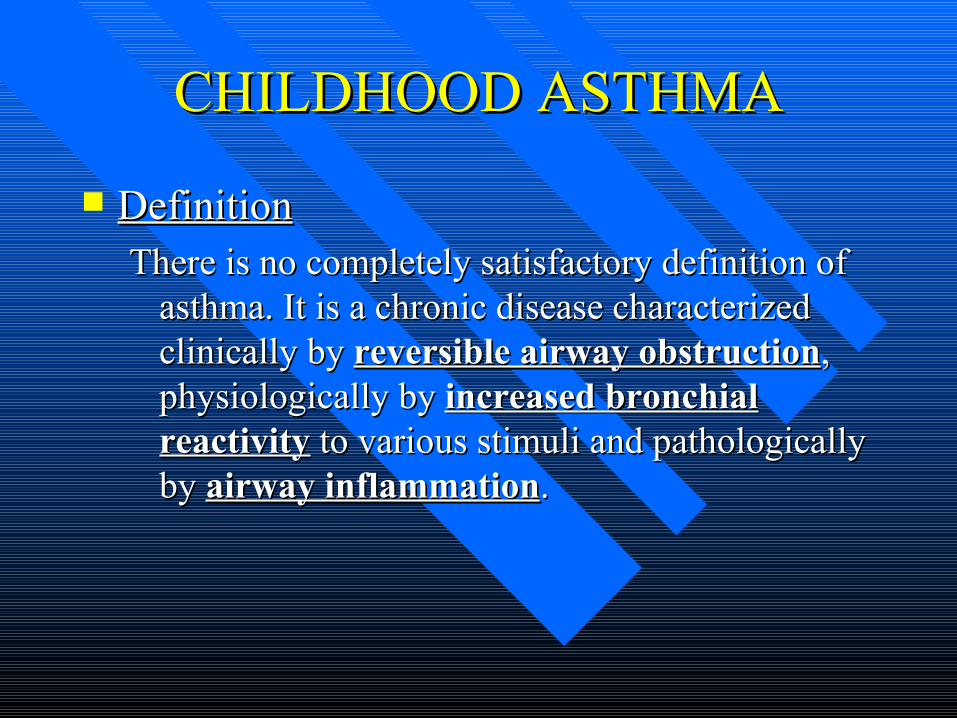
DefinitionDefinitionThere is no completely satisfactory definition of There is no completely satisfactory definition of
asthma. It is a chronic disease characterized asthma. It is a chronic disease characterized clinically by clinically by reversible airway obstructionreversible airway obstruction, , physiologically by physiologically by increased bronchial increased bronchial reactivityreactivity to various stimuli and pathologically to various stimuli and pathologically by by airway inflammationairway inflammation..

PrevalencePrevalence
It varies from country to another.It varies from country to another.
More common in Males.More common in Males.
Familial TendencyFamilial Tendency

Real lifeReal life facts about facts about asthma in childhood asthma in childhood

Asthma
176 deaths in US children
≤14 years in 1999Affects
~5 millionchildren <18 yearsin the US
Number 1 chronic illness
causing school absences ~3.5 million
physician or outpatient
hospital visitsfor US children
<15 years in 1999
>8.7 millionprescriptions in the USfor children <17 years
190,000 hospitalisationsfor US children <15 years in 1999
658,000 emergency department visits for asthma in US children
<15 years in 1999
AAAAI. Pediatric Asthma: Promoting Best Practice University of Rochester 1999; Mannino DM et al. MMWR Surveill Summ 2002;51:1–13;
American Lung Association. http://www.lungusa.org/asthma/ascpedfac99.html.

Asthma EtiologyAsthma Etiology
Asthma is a complex traitAsthma is a complex trait– Heritable and environmental factors contribute to its Heritable and environmental factors contribute to its
pathogenesispathogenesis
Multiple interacting genesMultiple interacting genes– At least 20 distinct chromosomal regions with linkage At least 20 distinct chromosomal regions with linkage
to asthma and asthma related traits have been identifiedto asthma and asthma related traits have been identified

PathophysiologyPathophysiology Caused byCaused by
– Inflammation and edemaInflammation and edema– Bronchial smooth Bronchial smooth
muscle spasm and muscle spasm and hypertrophyhypertrophy
– Mucous plugging Mucous plugging
Jenkins, HA, et al. Chest 2003; 124: 32-41.
http://www.pathguy.com/histo/087.htm

CysLTs
AirwayEpithelium
Increasedmucus secretion
Decreased mucustransport
Cationic proteins(Epithelial cell damage)
Increased releaseof tachykinins
Sensory Cfibres
Smooth muscle
Contraction and proliferation
Inflammatory Cells(e.g., Mast Cells,
Eosinophils)
Bloodvessel
Oedema
Adapted from Hay DW. Chest 1997;111:35S–45S.
Eosinophilrecruitment

It is More Than Brochoconstriction.It is More Than Brochoconstriction.
MastMast cells, cells,
EosinophilsEosinophils tissue tissue destructiondestruction
Epithelium.Epithelium.
Sub epithelial Sub epithelial proliferation proliferation of of myofibroblastmyofibroblast..
So inadequate treatment So inadequate treatment lung damage. lung damage.

Triggering FactorsTriggering Factors
InfectionsInfections PollensPollens House dust mitesHouse dust mites Noxious agentsNoxious agents Exercise.Exercise. SmokingSmoking Crying, Laughing..etcCrying, Laughing..etc



Diagnosing AsthmaDiagnosing Asthma
Clinical diagnosis supported by the certain Clinical diagnosis supported by the certain historical, physical and laboratory findingshistorical, physical and laboratory findings– History of episodic symptoms of airflow History of episodic symptoms of airflow
obstructionobstruction– Physical: wheeze, hyperinflationPhysical: wheeze, hyperinflation– Laboratory: exhaled nitric oxide (eNO), Laboratory: exhaled nitric oxide (eNO),
spirometryspirometry
Exclude other possibilitiesExclude other possibilities

Diagnosing Asthma in Young Diagnosing Asthma in Young Children – Asthma Predictive IndexChildren – Asthma Predictive Index
>> 4 episodes/yr of 4 episodes/yr of wheezing lasting more wheezing lasting more than 1 day affecting than 1 day affecting sleep in a child with sleep in a child with one MAJOR or two one MAJOR or two MINOR criteriaMINOR criteria
Major criteriaMajor criteria– Parent with asthmaParent with asthma– Physician diagnosed Physician diagnosed
atopic dermatitisatopic dermatitis
Minor criteriaMinor criteria– Physician diagnosed Physician diagnosed
allergic rhinitisallergic rhinitis– Eosinophilia (Eosinophilia (>>4%)4%)– Wheezing apart from Wheezing apart from
coldscolds
Adapted from Castro-Rodriquez JA, et al. AJRCCM 2000; 162: 1403

DIAGNOSISDIAGNOSIS
History and physical examinationHistory and physical examination
Pulmonary function testsPulmonary function tests
Laboratory investigationsLaboratory investigations
Differential DiagnosisDifferential Diagnosis
BronchiolitisBronchiolitis Cystic FibrosisCystic Fibrosis Foreign body aspirationForeign body aspiration Gastroesophygeal refluxGastroesophygeal reflux Immotile cilia syndromeImmotile cilia syndrome Vascular ringVascular ring Psychogenic coughPsychogenic cough

Asthma ClassificationAsthma Classification
>30%<60%FrequentContinuousSevere Persistent
>30%>60-<80%>1x/weekDailyModerate Persistent
20-30%>80%>2x/month3-6x/weekMild Persistent
<20%>80%<2x/month<2x/weekMild Intermittent
PEF Variability
PEF or FEV1
Nights with symptoms
Days with symptoms
Adapted from Guidelines for the Diagnosis and Management of Asthma-Update on Selected Topics 2002. NIH Publication No. 02-5075.

Levels of Asthma Levels of Asthma ControlControl
3 or more features of partly controlled asthma present in any week
< 80% predicted or personal best (if
known) on any dayNormal
Lung function (PEF or FEV1)
One or more / year 1 in any weekNoneExacerbation
More than twice / week
None (2 or less / week)
Need for rescue / “reliever” treatment
AnyNoneNocturnal symptoms /
awakening
AnyNoneLimitations of
activities
More than twice / week
None (2 or less / week)
Daytime symptoms
Uncontrolled Partly controlled(Any present in any week)
Controlled(All of the following)
Characteristic

Goals of TreatmentGoals of Treatment
SLEEPSLEEP LEARNLEARN PLAYPLAY
Asthma EducationAsthma Education
Self management education associated with:Self management education associated with:– Improvements in airflowImprovements in airflow– Improvements in self-efficacy scalesImprovements in self-efficacy scales– Reductions in school absenceReductions in school absence– Reduction in days of restricted activityReduction in days of restricted activity– Reduction in emergency room visitsReduction in emergency room visits

Recognition and Assessment of Recognition and Assessment of severe acute asthmasevere acute asthma
HISTORY.HISTORY.
PHYSICAL EXAMINATION.PHYSICAL EXAMINATION.
INVESTIGATIONS.INVESTIGATIONS.

PHYSICAL EXAMINATIONPHYSICAL EXAMINATION
General appearance of the child.General appearance of the child. Vital signs.Vital signs. Signs of dehydration.Signs of dehydration. Signs of hypoxemia.Signs of hypoxemia. Pulsus paradoxus.Pulsus paradoxus. Wheezing.Wheezing. Signs and symptoms of complicating Signs and symptoms of complicating
features of asthma.features of asthma.

ABG ABG
Usually not necessary in children who have Usually not necessary in children who have responded partially to initial treatment and responded partially to initial treatment and continue to improve.continue to improve.
An ABG should be obtained on patientsAn ABG should be obtained on patients::
a. a. With moderate - severe respiratory With moderate - severe respiratory distress. distress.
b. b. Not responding to therapy.Not responding to therapy.
c. c. Serial ABG’s may be necessary to evaluate Serial ABG’s may be necessary to evaluate progress/ deterioration.progress/ deterioration.


OXYGENOXYGEN
Hypoxaemia is the usual finding in severe Hypoxaemia is the usual finding in severe asthma and is the main cause of morbidity asthma and is the main cause of morbidity and mortality.and mortality.
Oxygen should be given by mask: 8-10 Oxygen should be given by mask: 8-10 L/min to keep the saturation above 95%.L/min to keep the saturation above 95%.
Oxygen administration never suppresses the Oxygen administration never suppresses the respiratory drive in childhood asthma.respiratory drive in childhood asthma.
NEBULISED SALBUTAMOLNEBULISED SALBUTAMOL
Beta-2-sympathomimetics are the mainstay Beta-2-sympathomimetics are the mainstay of treatment.of treatment.
It can be given diluted or undiluted through It can be given diluted or undiluted through a jet nebulizer driven by 8-10 L/min.a jet nebulizer driven by 8-10 L/min.
The large volume and high gas flow The large volume and high gas flow through the nebulizer produce a small through the nebulizer produce a small aerosol particle size, maximizing deposition aerosol particle size, maximizing deposition of the drug in small airways.of the drug in small airways.

CORTICOSTEROIDSCORTICOSTEROIDS
Reduce the severity of acute severe asthma.Reduce the severity of acute severe asthma. Reduce the inflammation in bronchial Reduce the inflammation in bronchial
mucosa.mucosa. Potentiate the relaxation of bronchial Potentiate the relaxation of bronchial
smooth muscle by Betasmooth muscle by Beta2 2 –agonists.–agonists.
Reduce mucous production.Reduce mucous production.
CORTICOSTEROIDSCORTICOSTEROIDS
The most important drug in treating asthma The most important drug in treating asthma
decreases recruitment and activation of decreases recruitment and activation of
inflammatory cells inflammatory cells up-regulates B2 receptors up-regulates B2 receptors decreases microvascular permeability decreases microvascular permeability decreases mucus production decreases mucus production

IPRATROPIUM BROMIDEIPRATROPIUM BROMIDE
It is an anticholinergic bronchodilator with It is an anticholinergic bronchodilator with no systemic atropine-like effects and no no systemic atropine-like effects and no inhibition of mucociliary clearance.inhibition of mucociliary clearance.
It has good synergy with betaIt has good synergy with beta2 2 agonist.agonist.
Ipratropium can be mixed with salbutamol Ipratropium can be mixed with salbutamol in the nebulizer.in the nebulizer.

AMINOPHYLLINEAMINOPHYLLINE
Aminophylline is a standard therapy for Aminophylline is a standard therapy for acute severe asthma, although the evidence acute severe asthma, although the evidence for its effectiveness is conflicting.for its effectiveness is conflicting.
It may have beneficial nonbronchodilator It may have beneficial nonbronchodilator effect; such as improvement in respiratory effect; such as improvement in respiratory muscle strength and also may have delayed muscle strength and also may have delayed anitinflammatory effect.anitinflammatory effect.
Plasma level must be monitored.Plasma level must be monitored.

IV SALBUTAMOLIV SALBUTAMOL
It appears as effective as inhaled route but it It appears as effective as inhaled route but it is not certain that I.V. infusions offers extra is not certain that I.V. infusions offers extra benefit in a child receiving maximal inhaled benefit in a child receiving maximal inhaled therapy.therapy.
It is used when the child’s tidal volume is It is used when the child’s tidal volume is so reduced that it limits aerosol drug so reduced that it limits aerosol drug delivery to the small airways.delivery to the small airways.

Magnesium SO4 Magnesium SO4
bronchodilatorbronchodilator - mech. unclear but may be due - mech. unclear but may be due to: to: – inhibition of Ca++-mediated smooth muscle inhibition of Ca++-mediated smooth muscle
contraction contraction – direct inhibition of smooth muscle contraction direct inhibition of smooth muscle contraction
given IV, onset minutes, duration about 2 hrs given IV, onset minutes, duration about 2 hrs side effectsside effects – –
– facial flushing/warmth, malaise facial flushing/warmth, malaise – hypotension/bradycardia only with rapid infusion hypotension/bradycardia only with rapid infusion
dosingdosing - 30-70 mg/kg IV over 20-30 min. - 30-70 mg/kg IV over 20-30 min. (max=2g) (max=2g)
bronchodilation proportional to serum levels bronchodilation proportional to serum levels

KETAMINEKETAMINE
relaxes smooth muscle directly, also increases relaxes smooth muscle directly, also increases chest wall compliance chest wall compliance
sympathomimetic properties sympathomimetic properties has been used in unintubated asthmatics to avoid has been used in unintubated asthmatics to avoid
intubation successfully intubation successfully side effects: side effects:
– arrhythmias arrhythmias – increased secretions increased secretions – laryngospasm laryngospasm
use benzodiazepines to decrease emergence use benzodiazepines to decrease emergence reactions reactions
dose:dose: 0.5-2.5mg/kg IV 0.5-2.5mg/kg IV

Mechanical VentilationMechanical Ventilation
10-33% of all PICU admissions for status 10-33% of all PICU admissions for status asthmaticus require MVasthmaticus require MV
mortality rates for those requiring MVmortality rates for those requiring MV
in children = up to 5% in children = up to 5% MV usually for hours to few days MV usually for hours to few days

IV FLUIDIV FLUID
Most patients are dehydrated due to:Most patients are dehydrated due to: ↑↑ metabolismmetabolism ↑↑ insensible lossinsensible loss ↓↓ intakeintake VomitingVomiting Dehydration Dehydration ↑↑ viscosity of secretions and viscosity of secretions and
worsen already poor cardiac output.worsen already poor cardiac output.
Correct Metabolic AcidosisCorrect Metabolic Acidosis
↑↑ lactic acid production by respiratory lactic acid production by respiratory muscles.muscles.
↓↓ utilazation of lactate by underperfused utilazation of lactate by underperfused liver and skeletal muscles.liver and skeletal muscles.
B-agonist(IV) direct effect on muscle tissue.B-agonist(IV) direct effect on muscle tissue. Keep pH > 7.2.Keep pH > 7.2.
AntibioticsAntibiotics
No role for routine use.No role for routine use. Indications:Indications:
– Sputum/tracheal aspirate predominantly PMNsSputum/tracheal aspirate predominantly PMNs– Evidence of pneumoniaEvidence of pneumonia

SedativeSedative
ketamine is ideal ketamine is ideal benzodiazepams benzodiazepams propofol propofol avoid opiates may cause histamine release, avoid opiates may cause histamine release,
worsen symptoms worsen symptoms

Risk factors for persistent Risk factors for persistent wheezing and predisposing to wheezing and predisposing to
asthma asthma
Frequent wheezing in the first year of life.Frequent wheezing in the first year of life. Eczema.Eczema. Maternal history of asthma. Maternal history of asthma. Elevated IgE levels.Elevated IgE levels. Maternal smoking.Maternal smoking.

Non Conventional InterventionsNon Conventional Interventions
Manual chest compressionManual chest compression Inhalation anestheticsInhalation anesthetics Nitric oxideNitric oxide BronchoscopyBronchoscopy HelioxHeliox ECMOECMO CPAP/non-invasive positive pressure ventilationCPAP/non-invasive positive pressure ventilation

Prevention of subsequent attacks Prevention of subsequent attacks of asthmaof asthma
Avoidance of triggering factors.Avoidance of triggering factors. Environmental control.Environmental control. Prompt recognition and treatment of exacerbation Prompt recognition and treatment of exacerbation
factors.factors. Patient and parents education.Patient and parents education. Monitor PEFR at home.Monitor PEFR at home. Development plan for management at home.Development plan for management at home. Development good communication and good Development good communication and good
relationship between the physician and he patient.relationship between the physician and he patient.

Controller Medications
Inhaled glucocorticosteroids Leukotriene modifiers Long-acting inhaled β2-agonists
Theophylline Cromones Long-acting oral β2-agonists
Anti-IgE Systemic glucocorticosteroids


PROPHYLACTIC THERAPYPROPHYLACTIC THERAPY
Inhaled CorticosteroidsInhaled Corticosteroids Long acting SalbutamolLong acting Salbutamol Leukotriens AntagonistLeukotriens Antagonist Sodium cromoglygateSodium cromoglygate NodocromilNodocromil





Natural History of AsthmaNatural History of Asthma
•27 percent never reported wheezing •21 percent reported wheezing at only one assessment •10 percent had intermittent wheezing •14 percent had wheezing that persisted throughout the study •15 percent had remission during adolescence and no further wheezing •12 percent had remission with subsequent relapse