Chapter 17 Obstetrics and Gynecological Emergencies.
34
Chapter 17 Obstetrics and Gynecological Emergencies
-
Upload
merry-johns -
Category
Documents
-
view
226 -
download
5
Transcript of Chapter 17 Obstetrics and Gynecological Emergencies.

Chapter 17
Obstetrics and Gynecological Emergencies

2
Chapter 17: Obstetrics and Gynecological Emergencies
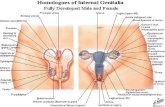
• Identify the following structures: uterus, vagina, fetus, placenta, umbilical cord, amniotic sac, perineum.
• Identify and explain the use of the contents of an obstetrics kit.
• Identify predelivery emergencies.
• State indicators of imminent delivery.
Objectives (1 of 3)

3
Chapter 17: Obstetrics and Gynecological Emergencies
• Differentiate the emergency medical care provided to a patient with predelivery emergencies from a normal delivery.
• Establish the relationship between body substance isolation and childbirth.
• State the steps to assist in the delivery.
Objectives (2 of 3)

4
Chapter 17: Obstetrics and Gynecological Emergencies
• Describe how and when to cut the umbilical cord.
• Discuss the emergency medical care of a patient with a gynecological emergency.
Objectives (3 of 3)

5
Chapter 17: Obstetrics and Gynecological Emergencies
Female Reproductive System

6
Chapter 17: Obstetrics and Gynecological Emergencies
Three Stages of Labor
• First stage
– Dilation of the cervix
• Second stage
– Expulsion of the infant
• Third stage
– Delivery of the placenta

7
Chapter 17: Obstetrics and Gynecological Emergencies
Predelivery Emergencies• Preeclampsia (hypertension)
– Headache, vision disturbance, edema, anxiety
• Eclampsia
– Convulsions resulting from hypertension
• Supine hypotensive syndrome
– Low blood pressure from lying supine

8
Chapter 17: Obstetrics and Gynecological Emergencies
Hemorrhage
• Vaginal bleeding that occurs before labor begins
• If present in early pregnancy, it may be a spontaneous abortion or ectopic pregnancy.

9
Chapter 17: Obstetrics and Gynecological Emergencies
Ectopic Pregnancy
• Pregnancy outside of the uterus
• Occurs once in every 200 pregnancies.
• Consider with a missed menstrual cycle and sudden, severe abdominal pain.
• History of PID, tubal ligation, or previous ectopic pregnancy

10
Chapter 17: Obstetrics and Gynecological Emergencies
Placenta Problems• Placenta abruptio
– Premature separation of the placenta
• Placenta previa– Development of
placenta over the cervix

11
Chapter 17: Obstetrics and Gynecological Emergencies
Trauma and Bleeding• Any vaginal bleeding with pregnancy is a serious
sign.
• Save all blood-soaked pads and any passed tissue.
• Do not insert pads into the vagina.
• Transport promptly with woman on her left side.
• Signs of shock can be delayed, but the fetus may be in trouble.

12
Chapter 17: Obstetrics and Gynecological Emergencies
When to Consider Field Delivery
• Delivery can be expected within a few minutes
• A natural disaster or other catastrophe makes it impossible to reach a hospital
• No transportation is available

13
Chapter 17: Obstetrics and Gynecological Emergencies
Crowning

14
Chapter 17: Obstetrics and Gynecological Emergencies
Preparing for Delivery
• Use proper BSI precautions.
• Be calm and reassuring while protecting the mother’s modesty.
• Contact medical control for a decision to deliver on scene or transport.
• Prepare OB kit.

15
Chapter 17: Obstetrics and Gynecological Emergencies
Positioning for Delivery

16
Chapter 17: Obstetrics and Gynecological Emergencies
Delivering the Infant (1 of 2)
• Support the head as it emerges, suction the mouth than nose.
• Check for nuchal cord, cut if necessary.
• Once the head emerges, the shoulders will be visible.

17
Chapter 17: Obstetrics and Gynecological Emergencies
Delivering the Infant (2 of 2)
• Support the head and upper body as the shoulders deliver.
• Handle the infant firmly but gently as the body delivers.
• Clamp the cord and cut it.

18
Chapter 17: Obstetrics and Gynecological Emergencies
Complications with Normal Vaginal Delivery
• Unruptured amniotic sac
– Puncture the sac and push it away from the baby.
• Umbilical cord around the neck (nuchal cord)
– Gently slip the cord over the infant’s head.
– Cut cord if necessary.

19
Chapter 17: Obstetrics and Gynecological Emergencies
Postdelivery Care
• Immediately wrap the infant in a towel with the head lower than the body.
• Suction the mouth and nose again.
• Clamp and cut the cord if not done already.
• Ensure the infant is pink and breathing well.

20
Chapter 17: Obstetrics and Gynecological Emergencies
Delivery of the Placenta
• Placenta is attached to the end of the umbilical cord.
• It should deliver within 30 minutes.• Once the placenta delivers, wrap it and
take it to the hospital so it can be examined.
• If the mother continues to bleed, transport promptly to the hospital.

21
Chapter 17: Obstetrics and Gynecological Emergencies
APGAR Scoring(0 to 10)
A Appearance
P Pulse
G Grimace
A Activity
R Respirations
• Scored at 1 and 5 minutes after birth

22
Chapter 17: Obstetrics and Gynecological Emergencies
Neonatal Resuscitation

23
Chapter 17: Obstetrics and Gynecological Emergencies
Giving Chest Compressions to an Infant (1 of 2)
• Find the proper position
– Just below the nipple line
– Middle third of the sternum
• Wrap your hands around the body, with your thumbs resting at that position.
• Press your thumbs gently against the sternum, compressing ½” to ¾” deep.

24
Chapter 17: Obstetrics and Gynecological Emergencies
Giving Chest Compressions to an Infant (2 of 2)
• Ventilate with a BVM device after every third compression.
• 90 compressions to 30 ventilations per minute
• Continue CPR while awaiting transport.

25
Chapter 17: Obstetrics and Gynecological Emergencies
Breech Delivery• Presenting part is the buttocks.
• Breech delivery is usually slow, giving you time to arrange for transport to the hospital.
• Support the infant as it comes out.
• Make a “V” with your gloved fingers then place them in the vagina to prevent it from compressing infant’s airway.

26
Chapter 17: Obstetrics and Gynecological Emergencies
Rare Presentations• Limb presentation
– This is a very rare occurrence.– This is a true emergency that requires
immediate transport.• Prolapsed cord
– Arrange for immediate transport.– Place fingers into the mother’s vagina and
push the cord away from the infant’s face.

27
Chapter 17: Obstetrics and Gynecological Emergencies
Excessive Bleeding
• Bleeding always occurs with delivery but should not exceed 500 mL.
• Massage the mother’s uterus to slow bleeding.
• Treat for shock.
• Place pad over vaginal opening.
• Arrange for immediate transport to hospital.

28
Chapter 17: Obstetrics and Gynecological Emergencies
Spontaneous Abortion (Miscarriage)
• Delivery of the fetus or placenta before the 20th week
• Infection and bleeding are the most important complications.
• Treat the mother for shock.• Arrange for immediate transport.• Bring tissue that has passed through the
vagina to the hospital.

29
Chapter 17: Obstetrics and Gynecological Emergencies
Twins
• Twins are usually smaller than single infants.
• Delivery procedures are the same as that for single infants.
• There may be one or two placentas to deliver.

30
Chapter 17: Obstetrics and Gynecological Emergencies
Premature Infants and Procedures
• Delivery before 8 months or weight less than 5 lb at birth.
– Keep the infant warm.
– Keep the mouth and nose clear of mucus.
– Give oxygen.
– Do not infect the infant.
– Notify EMS.

31
Chapter 17: Obstetrics and Gynecological Emergencies
Fetal Demise• An infant that has died in the uterus before
labor
• This is a very emotional situation for family and providers.
• The infant may be born with skin blisters, skin sloughing, and dark discoloration.
• Do not attempt to resuscitate an obviously dead infant.

32
Chapter 17: Obstetrics and Gynecological Emergencies
Delivery Without Sterile Supplies
• You should always have goggles and sterile gloves with you.
• Use clean sheets and towels.
• Do not cut or clamp umbilical cord.
• Keep placenta and infant at same level.

33
Chapter 17: Obstetrics and Gynecological Emergencies
Gynecologic Emergencies
• Soft-tissue injuries can be painful and bleed profusely.
• Treat as other soft-tissue injuries, and never insert dressing into the vagina.
• Have a second rescuer present, preferably female, when treating such emergencies.

34
Chapter 17: Obstetrics and Gynecological Emergencies
Stresses and Pregnancy• More women are now active well into the
third trimester of pregnancy.
• Environmental conditions can increase risks to mother and fetus.
– Altitude
– Diving
– Temperature and humidity