Obstetrics and Gynecological Emergencies Chapter 17.
59
Obstetrics and Gynecological Emergencies Chapter 17
-
Upload
curtis-stafford -
Category
Documents
-
view
224 -
download
2
Transcript of Obstetrics and Gynecological Emergencies Chapter 17.

Obstetrics and Gynecological
Emergencies Chapter 17

Topic Overview• Reproductive Anatomy• Normal Delivery• Care/Resuscitation of Newborn• Abnormal deliveries• Predelivery emergencies• Gynecologic emergencies


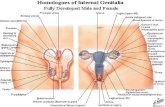
Anatomy

Childbirth
• Terms & Definitions– Crowning
• When the presenting part of the baby first bulges from the vaginal opening
– Cephalic presentation - Head first– Breech presentation
• Limb • Frank

LABOR
• First Stage• Begins with regular contractions, then thinning and
gradual dilation of the cervix and ends when the cervix if fully dilated
• Second Stage• Begins when the baby’s head enters the birth canal
until the baby is born
• Third Stage• Following the birth of the baby until the placenta is
delivered

Your Role
• Materials Needed– Need OB kit (if available)– Gloves– Towels and drapes– 4 x 4s– Bulb syringe– Umbilical tape or clamps– Scissors or scalpel for cutting the cord

Childbirth
– A baby blanket– Several sanitary napkins– Plastic bag– Standard BSI precautions

Childbirth Delivery Kit

Normal Delivery
• Transport Decision (911 Call)– Based on evaluation– Number of prior births– Distance to hospital or birthing center– Complications expected
• Delivery Precautions– Use of BSI– Keep mother out of bathroom– Do not hold mother’s knees together

Childbirth
• Evaluating the Mother– Patient name, age– Which pregnancy?– Gravida, Para and AB– How long in labor– Ask the patient if she feels the need to move
her bowels– Check for Crowning**– Time uterine contractions

Childbirth
– Vital signs if time allows– Remember if this first baby and crowing or
urge to push is not present then transport can be effect
– DO NOT LET MOTHER GO TO THE BATHROOM

Childbirth• Preparing for Delivery
– Control the scene– BSI– Position the patient– Remove clothing that can
obstruct view of delivery– Create a sterile field– Position OB kit or available
materials

Childbirth
The Delivery

Crowning of Infant’s Head

Delivery of Head - Prevent Explosive Delivery

Delivery of the Head

Delivery Procedures
• If amniotic sac has not broken, puncture sac and pull away from baby's face.
• Determine if umbilical cord is around baby’s neck. If so, clamp and cut cord.

• Suction mouth, then nose
• Aid in birth of upper shoulder

• Support the trunk
• Support the legs

Childbirth
• Delivery Procedures– Wipe blood, mucus from nose and mouth– Suction– Warmth is critical!– Wrap baby in warm towel, head lower than
trunk– Keep infant level with vagina until cord is cut

• Clamp or tie cord; then cut
• Evaluate baby

• Observe for delivery of placenta
• When placneta delivers, place in a plastic bag for transport to hospital

Childbirth– After Delivery Procedures
• Control vaginal bleeding after delivery – DO PLACE ANYTHING IN THE VAGINA– Place a sanitary napkin over the vaginal opening – Have mother lower her legs
• **Massage the fundus• **Nursing the baby can help the uterus contract and
return to normal
– Record time of delivery

Childbirth
• Vaginal Bleeding– A loss of 55 cc is well tolerated.– Treat for shock


Care of Newborn
• Position, dry, wipe, wrap
• Repeat clearing airway (suction)
• Cover the head

Normal AssessmentNormal AssessmentFindings NewbornFindings Newborn
AppearanceAppearancePulsePulseGrimaceGrimaceActivityActivityRespiratory Respiratory efforteffort
=====
APGAR
Color: No central cyanosis
Greater than 100/min.
Vigorous & crying
Good extremity motion
Normal, crying

Childbirth
Sign 0 1 2
Appearance(Skin Color)
Blue/Pale Body PinkExtremitiesBlue
Completelypink
Pulse Rate Absent Below 100 Above 100
Grimace NoResponse
Grimaces Cries
Activity Limp Someflexion ofextremities
Activemotion
Respiratory Absent Slow andirregular
Strong Cry
Total Score

ResuscitationResuscitationof the Newbornof the Newborn

Inverted Pyramid of Neonatal ResuscitationInverted Pyramid of Neonatal Resuscitation
Drying. Warming. Positioning.Suction. Tactile Stimulation.
Oxygen
Intubation
Medi-cations
Bag-Mask Ventilation
ChestCompressions

Breathing EffortBreathing Effort
If shallow, slow, or absent:If shallow, slow, or absent:• Provide artificial ventilations,Provide artificial ventilations, 40-60/minute.40-60/minute.• Reassess after 30 seconds.Reassess after 30 seconds.• Continue as necessary.Continue as necessary.

Heart RateHeart Rate
If less than If less than 100100/minute:/minute:• Provide artificial ventilations,Provide artificial ventilations, 40-60/minute. 40-60/minute.• Reassess after 30 seconds.Reassess after 30 seconds.• If no improvement, continueIf no improvement, continue ventilations. ventilations.
(Continued)(Continued)

Heart RateHeart Rate
If less than If less than 60-8060-80/minute and/minute and not responding to ventilation: not responding to ventilation:
• Start chest compressions.Start chest compressions.
(Continued)(Continued)

Heart RateHeart Rate
If at any time the heart rate is lessIf at any time the heart rate is lessthan than 6060, begin ventilations and , begin ventilations and compressions immediately.compressions immediately.

ColorColor
If central (trunk) cyanosis isIf central (trunk) cyanosis ispresent with adequate breathingpresent with adequate breathingand heart rate, administer and heart rate, administer blow-by oxygen. blow-by oxygen.

Childbirth
Complications / Abnormal Deliveries

Complications
• Supine Hypotensive Syndrome– The weight of the baby, placenta and
amniotic fluid can compress the vena cava– Care
• Place mother on lateral left side

Complications
• Breach Birth
– Baby’s buttocks or lower extremities presenting• Greater risk of trauma, prolapsed cord
– Care• Never pull on the babies legs• High flow oxygen• Place mother in head-down position with hips
elevated

Complications
– If body delivers support the body and prevent an explosive delivery of the head
– If necessary to create an airway, place two fingers of gloved hand into vagina making a “V” with your fingers to create an airway. Hope position until EMS arrives or baby delivers

Complications
• Prolapsed Umbilical Cord– Mother in head down and buttocks up
(kneeling with buttocks up) – High flow oxygen– Check cord for a pulse– Wrap the cord in a towel to keep warm– Insert gloved fingers in the vaginal and
pressure gently on the babies head or buttocks to take pressure off the cord



Complications• Limb Presentation
– High flow oxygen– Do Not pull on the baby

Complications
• Multiple Births– Delivery procedures the same for each birth
• Prepare for multiple resuscitations
– Clamp the cord of the first baby – 2nd baby may be born before or after the
placenta– Care for first infant– Maintain body temperature of the infants

Complications
• Premature Birth– Keep baby WARM– Keep airway clear– Provide ventilation (BVM) and
chest compressions as needed– Watch the umbilical cord for
bleeding– Oxygen using blow by method– Avoid contamination, Do Not
breath into the face of the baby

Complications
• Pre-birth bleeding– If you have any pre-birth bleeding place a
pad at the opening of the vagina– Save any tissue which is passed
• Meconium– Green or brown amniotic fluid indicates
presence of fecal matter– Suggests fetal distress during labor

Complications
• Pre-Eclampsia– High blood pressure and swelling of the
extremities– The pregnant female needs to be
monitored closely
• Eclampsia– Seizures during pregnancy– Seizures are a dire emergency– Mother should be transported by EMS– Administer high-flow oxygen

Complications
• Fetal tissue goes to hospital
– Provide emotional support for mother

Complications
• Miscarriage (Spontaneous Abortion)– Complete patient assessment– treatment based on assessment– 911 (Save all tissue expelled)– Vital Signs– Treat for shock– Place a napkin over the vaginal opening– Replace all blood soaked pads and keep– Emotional support for the patient

Obstetrics and Gynecological Emergencies
Trauma In Pregnancy- Patient Assessment– Pulse will be 10-15 beats higher– A pregnant female has 30-35% more blood
so signs of shock will be delayed– Ask patient about any blows to the back,
pelvis or abdomen– Ask if the patient is bleeding or has any
discharge (water has broken)

Obstetrics and Gynecological Emergencies
Treatment for Pregnant Trauma Patient– High flow oxygen– Be ready to suction due due to nausea and
possible vomiting– Activate EMS– Provide emotional support

Gynecological Emergencies

Gynecological Emergencies
Vaginal Bleeding
Can be potentially life-threatening– Follow BSI precautions– Assure airway– Assess and treat for shock– Provide oxygen– Activate EMS if bleeding is severe

Gynecological Emergencies
Trauma to the External Genitalia– Scene size up and look at the mechanism of
injury– During initial assessment look for signs of
shock– Treat like any soft-tissue injury
• Control bleeding with direct pressure
• Never pack vagina
– If signs of shock high flow O2

Gynecological Emergencies
Sexual Assault– Treat scene as a crime scene– Complete patient assessment and care
• Take care not to destroy evidence on the scene• Activate EMS
– Provide comfort for the patient– Non-judgemental attitude– Psychological care required

Gynecological Emergencies
Sexual Assault– Preserve potential evidence– Discourage patient from bathing, voiding

Review Questions
• Describe the anatomy of the reproductive system
• List the items you will need in a childbirth kit
• What factors will determine whether 911 should transport or deliver at scene

Review Questions
• Describe the normal delivery process• Describe the APGAR scoring system• Describe the following, and the care for
each:– Limb presentation– Prolapsed cord– Breech presentation– Meconium