[Chapter 12] Amputations of the Hip and Pelvis
9
Alllputations of the Hip and Pelvis Chapter 12 Hip disarticulation and the various forms of hemipelvec- tomy most often are performed for the treatment of tumors. The dimensions of the amputation vary with oncological requirements, and nonstandard flaps often are necessary. Although satisfactory prostheses are available, few patients find them to be useful. Hip disarticulation occasionally is indicated after massive trauma, for arterial insufficiency, for infection (e.g., infected subtrochanteric nonunion, necrotizing fasciitis), or for certain congenital limb deficiencies. Most frequently, however, hip disarticulation is necessary for treatment of bone or soft-tissue sarcomas of the femur or thigh that cannot be resected adequately by limb-sparing methods. The inguinal or iliac lymph nodes are not routinely removed with hip disarticulation. The anatomical method of Boyd and the posterior flap method of Slocum are described here; however, modifications frequently are required based on location of pathology. Anatomical Hip Disarticulation TECHNIQUE 12-1 Boyd • Make an anterior racquet-shaped incision (Fig. 12-1A), beginning the incision at the anterior superior iliac spine and curving it distally and medially almost parallel with the Poupart ligament to a point on the medial aspect of the thigh 5 cm distal to the origin of the adductor muscles. Isolate and ligate the femoral artery and vein, and divide the femoral nerve; continue the incision around the posterior aspect of the thigh about 5 cm distal to the ischial tuberosity and along the lateral aspect of the thigh about 8 cm distal to the base of the greater trochanter. From this point, curve the incision proximally to join the beginning of the incision justinferior to the anterior superior iliac spine. • Detach the sartorius muscle from the anterior superior iliac spine and the rectus femoris from the anterior inferior iliac spine, and reflect them both distally • Divide the pectineus about 0.6 cmfrom the pubis. • Rotate the thigh externally to bring the lesser trochanter and the iliopsoas tendon into view; divide the latter at its insertion and reflect it proximally. • Detach theadductor and gracilis muscles from the pubis, and divide at its origin that part of the adductor mag nus that arises from the ischium • Develop the muscle plane between the pectineus and obturator extern us andshort external rotators of the hip to expose the branches of the obturator artery. Clamp, ligate, and divide thebranches at this point Later in the operation, the obturator externus muscle is divided at itsinsertion on the femur instead of at its origin on the pelvis because otherwise the obturator artery may be severed and might retract into the pelvis, leading to hemorrhage that could be difficult to control. • Rotate the thigh internally, and detach the gluteus medius and minimus muscles from their insertions on the greater trochanter, and retract them proximally. • Divide the fascia lata and the most distal fibers of the gluteus maximus muscledistal to theinsertion of the tensor fasciae latae musclein the line of the skinincision, and separate the tendon of thegluteus maximusfrom its insertion on thelinea aspera. Reflect this muscle mass proximally. • Identify, ligate, and divide the sciatic nerve. • Divide the short external rotators of the hip (i.e., the piriformis, gemelli, obturator intern us, obturator externus, and quadratus femoris) at their insertions on the femur, and sever the hamstring muscles from the ischial tuberosity.
-
Upload
savin-gabriela -
Category
Documents
-
view
60 -
download
7
description
Amputations of the Hip and Pelvis
Transcript of [Chapter 12] Amputations of the Hip and Pelvis
![Page 1: [Chapter 12] Amputations of the Hip and Pelvis](https://reader034.fdocuments.in/reader034/viewer/2022042502/54654bcdaf795979338b4d41/html5/thumbnails/1.jpg)
Alllputations of the Hipand Pelvis
Chapter 12
Hip disarticulation and the various forms of hemipelvec-tomy most often are performed for the treatment of tumors.The dimensions of the amputation vary with oncologicalrequirements, and nonstandard flaps often are necessary.Although satisfactory prostheses are available, few patientsfind them to be useful.
Hip disarticulation occasionally is indicated after massivetrauma, for arterial insufficiency, for infection (e.g., infectedsubtrochanteric nonunion, necrotizing fasciitis), or forcertain congenital limb deficiencies. Most frequently,however, hip disarticulation is necessary for treatment ofbone or soft-tissue sarcomas of the femur or thigh thatcannot be resected adequately by limb-sparing methods.The inguinal or iliac lymph nodes are not routinelyremoved with hip disarticulation. The anatomical methodof Boyd and the posterior flap method of Slocum aredescribed here; however, modifications frequently arerequired based on location of pathology.
Anatomical Hip DisarticulationTECHNIQUE 12-1 Boyd
• Make an anterior racquet-shaped incision (Fig. 12-1A),beginning the incision at the anterior superior iliac spine andcurving it distally and medially almost parallel with the Poupartligament to a point on the medial aspect of the thigh 5 cm distal
to the origin of the adductor muscles. Isolate and ligate thefemoral artery and vein, and divide the femoral nerve; continuethe incision around the posterior aspect of the thigh about 5 cmdistal to the ischial tuberosity and along the lateral aspect of thethigh about 8 cm distal to the base of the greater trochanter.
From this point, curve the incision proximally to join the
beginning of the incision just inferior to the anterior superior iliacspine.
• Detach the sartorius muscle from the anterior superior iliacspine and the rectus femoris from the anterior inferior iliac spine,and reflect them both distally
• Divide the pectineus about 0.6 cm from the pubis.
• Rotate the thigh externally to bring the lesser trochanter andthe iliopsoas tendon into view; divide the latter at its insertionand reflect it proximally.
• Detach the adductor and gracilis muscles from the pubis, anddivide at its origin that part of the adductor mag nus that arisesfrom the ischium
• Develop the muscle plane between the pectineus andobturator extern us and short external rotators of the hip toexpose the branches of the obturator artery. Clamp, ligate, anddivide the branches at this point Later in the operation, theobturator externus muscle is divided at its insertion on the femurinstead of at its origin on the pelvis because otherwise theobturator artery may be severed and might retract into thepelvis, leading to hemorrhage that could be difficult to control.
• Rotate the thigh internally, and detach the gluteus medius andminimus muscles from their insertions on the greater trochanter,and retract them proximally.
• Divide the fascia lata and the most distal fibers of the gluteusmaximus muscle distal to the insertion of the tensor fasciae lataemuscle in the line of the skin incision, and separate the tendonof the gluteus maximus from its insertion on the linea aspera.Reflect this muscle mass proximally.
• Identify, ligate, and divide the sciatic nerve.
• Divide the short external rotators of the hip (i.e., the piriformis,gemelli, obturator intern us, obturator externus, and quadratusfemoris) at their insertions on the femur, and sever the hamstringmuscles from the ischial tuberosity.
![Page 2: [Chapter 12] Amputations of the Hip and Pelvis](https://reader034.fdocuments.in/reader034/viewer/2022042502/54654bcdaf795979338b4d41/html5/thumbnails/2.jpg)
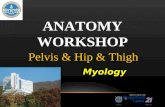
Gluteus mediusmuscle
Gluteus maximusmuscle
Vastus lateralismuscle
Rectus femorismuscle
Sartoriusmuscle
Adductor longus andbrevis muscles
Insertion of gluteusmaximus muscle
\\.••... ,-,,,
II
~ Vastus lateralismuscle
Shortexternalrotators
Gluteusmaximus
muscle
Obturatorexternusmuscle
Adductormuscles
Bicepsfemorismuscle
Semitendinosusmuscle
mWFl' Boyd disarticulation of hip. A, Femoral vessels and nerve have been ligated, andsartorius, rectus femoris, pectineus, and iliopsoas muscles have been detached. Inset, Line ofskin incision. B, Gluteal muscles have been separated from insertions, sciatic nerve and shortexternal rotators have been divided, and hamstring muscles have been detached from ischialtuberosity. Inset, Final closure of stump. (Redrawn from Boyd HB: Anatomic disarticulatioll of t/ze /zip,Surg Gynecol Obstet 84:346, 1947.)
![Page 3: [Chapter 12] Amputations of the Hip and Pelvis](https://reader034.fdocuments.in/reader034/viewer/2022042502/54654bcdaf795979338b4d41/html5/thumbnails/3.jpg)
Anatomic Hip DisarticulationTECHNIQUE 12-1 Boyd-cont'd
• Incise the hip joint capsule and the ligamentum teres tocomplete the disarticulation (Fig. 12-1B).
• Bring the gluteal flap anteriorly, and suture the distal part ofthe gluteal muscles to the origin of the pectineus and adductormuscles.
• Place a drain in the inferior part of the incision, andapproximate the skin edges with interrupted nonabsorbablesutures.
Posterior FlapTECHNIQUE 12-2 Slocum
• Begin the incision at the level of the inguinal ligament, carry itdistally over the femoral artery for 10 cm, curve it along themedial aspect of the thigh, continue it laterally and proximallyover the greater trochanter, and swing it anteriorly to thestarting point. A posteromedial flap long enough to cover theend of the stump is formed.
• Isolate, ligate, and divide the femoral vessels, and section thefemoral nerve to fall well proximal to the inguinal ligament.
• Abduct the thigh widely, and divide the adductor muscles attheir pubic origins.
• Section the two branches of the obturator nerve so that theyretract away from pressure areas.
• Free the origins of the sartorius and rectus femoris from theanterior superior and anterior inferior iliac spines. Moderatelyadduct and internally rotate the thigh, and divide the tensorfasciae latae at the level of the proximal end of the greatertrochanter; at the same level, divide close to bone the musclesattached to the trochanter. Next, abduct the thigh markedly, anddivide the gluteus maximus at the distal end of the posterior skinflap.
• Identify, ligate, and divide the sciatic nerve.
• Divide the joint capsule, and complete the disarticulation.
• Swing the long posteromedial flap containing the gluteusmaximus anteriorly, and suture it to the anterior margins of theincision.
Hemipelvectomy most often is performed for tumors thatcannot be adequately resected by limb-sparing techniquesor hip disarticulation. Other indications for hemipelvec-tomy include life-threatening infection and arterial insuf-
ficiency. Chan et aL reported hemipelvectomy for decubitusulcers in patients with spinal cord injury. In contrast to hipdisarticulation, all types of hemipelvectomy remove theinguinal and iliac lymph nodes.
The standard hemipelvectomy employs a posterior or glutealflap and disarticulates the symphysis pubis and sacroiliacjoint. An extended hemipelvectomy involves the posteriorbony section passing through the sacrum. In a conservativehemipelvectomy, the bony section divides the ilium above theacetabulum, preserving the crest of the ilium. Internal hemi-pelvectomy is a limb-sparing resection, often achieving prox-imal and medial margins equal to the correspondingamputation. This procedure is discussed in Technique19-12.
All types of hemipelvectomy are extremely invasive andmutilating procedures. They require optimizing thepatient's nutritional status, preparing for blood replacement,and adequate monitoring during surgery. Many patientshave significant phantom pain in the early postoperativecourse. Flap necrosis and wound sloughs are common com-plications. Appropriate emotional and psychological supportis an important part of rehabilitation. Although good pros-theses are available for patients after hemipelvectomy, fewfind them usefuL Techniques for the standard anterior flapand conservative hemipelvectomy are described.
Standard HemipelvectomyTECHNIQUE 12-3
• Insert a Foley catheter. Place the patient in a lateral decubitusposition with the involved side up. Support the patient so thatthe table can be tilted to facilitate anterior and posteriordissection.
• Perform the anterior dissection first, making an incisionextending from 5 cm above the anterior superior iliac spine tothe pubic tubercle (Fig. 12-2A). Deepen the incision through thetensor fascia, external oblique aponeurosis, and internal obliqueand transversalis muscles.
• Retract the spermatic cord medially.
• Expose the iliac fossa by blunt dissection.
• Elevate the parietal peritoneum off the iliac vessels, and permitit to fall inferiorly with the viscera.
• Ligate the inferior epigastric vessels.
• Release the rectus muscle and sheath from the pubis.
• Identify the iliac vessels, retract the ureter medially, andligate and divide the common iliac artery and vein. Put lateraltraction on the iliac artery and vein, and ligate and divide theirbranches to the sacrum, rectum, and bladder, separating therectum and bladder from the pelvic side wall and exposing the
![Page 4: [Chapter 12] Amputations of the Hip and Pelvis](https://reader034.fdocuments.in/reader034/viewer/2022042502/54654bcdaf795979338b4d41/html5/thumbnails/4.jpg)
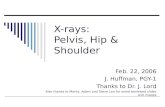
Common iliac artery
Internal iliac artery
Middlehemorrhoidal artery
~'~ ""'"
Symphysis pubis ~,
Inferiorgluteal artery
Internalpudendal
artery
External iliacartery
Inferior marginof gluteus maximusmuscle
Posterior inferioriliac spine
Sacroiliacjoint
Transection ofurogenital
diaphragm
Position ofright-angle clamp
WAf') Standard hemipelvectomy. A, Incision. Band C, Transection of iliac arteries anddivision of internal iliac vessels. D, Release of iliac crest and gluteus maximus. E, Division ofsymphysis pubis. P, Division of muscles from pelvis. (Redrawn from Sugarbaker PH, MalawerMM: Musculoskeletal surgery for cancer, Berlin, 19R2, Thieme.)
![Page 5: [Chapter 12] Amputations of the Hip and Pelvis](https://reader034.fdocuments.in/reader034/viewer/2022042502/54654bcdaf795979338b4d41/html5/thumbnails/5.jpg)
Standard HemipelvectomyTECHNIQUE 12·3-cont'd
sacral nerve roots (Fig. 12-28 and C) If necessary for exposure,divide the symphysis pubis and sacroiliac joint before thisdissection.
• Pack the anterior wound with warm, moist gauze packs.
• Make a posterior skin incision, extending from 5 cm above theanterior superior iliac spine, coursing over the anterior aspect ofthe greater trochanter, paralleling the gluteal crease posteriorly
around the thigh, and connecting with the inferior end of theanterior incision (see Fig. 12-2A).
• Raise the posterior flap by dissecting the gluteal fascia directlyoff the gluteus maximus. Include the fascia with the flap. Ifpossible, include the medial portion of the gluteus maximus withthe flap as recommended by Karakousis and Vezeridis. Superiorlyelevate the flap off the iliac crest.
• Divide the external oblique, sacrospinalis, latissimus dorsi, andquadratus lumborum from the crest of the ilium.
• Reflect the gluteus maximus from the sacrotuberous ligament,coccyx, and sacrum (Fig. 12-2D).
• Divide the iliopsoas muscle; genitofemoral, obturator, andfemoral nerves; and lumbosacral nerve trunk at the level of theiliac crest.
• Abduct the hip, placing tension on the soft tissues around thesymphysis pubis. Pass a long right-angle clamp around thesymphysis, and divide it with a scalpel (Fig. 12-2E).
• Divide the sacral nerve roots, preserving the nervi erigentes ifpossible. Reflect the iliacus muscle laterally, exposing the anterioraspect of the sacroiliac joint.
• Divide the joint anteriorly with a scalpel or osteotome, anddivide the iliolumbar ligament.
• Place considerable traction on the extremity, separating thepelvic side wall from the viscera. Proceeding from anterior toposterior, divide the following from the pelvic side wall:urogenital diaphragm, pubococcygeus, ischiococcygeus,iliococcygeus, piriformis, sacrotuberous ligament, andsacrospinous ligaments (Fig. 12-2F). All of these structures mustbe divided under tension. Move the extremity anteriorly, anddivide the posterior aspect of the sacroiliac joint to complete thedissection.
• Place suction drains in the wound, and suture thegluteal fascia to the fascia of the abdominal wall. Close
the skin.
AFTERTREATMENT The drains and Foley catheter shouldbe left in place for several days. Pressure should be kept offthe posterior flap for several days.
Anterior Flap Hemipelvectomy
Anterior flap hemipelvectomy is indicated for lesions of thebuttock or posterior proxim.al thigh that cannot be ade-quately treated by limb-sparing methods. The larger pos-terior defect is covered by a quadriceps myocutaneous flapmaintained by the superficial femoral artery.
TECHNIQUE 12·4
• Insert a Foley catheter. Place the patient in the lateraldecubitus position with the operated side up, and secure thepatient to the table so that it can be tilted to facilitate theanterior and posterior dissections. Prepare the skin from toes torib cages, and drape the extremity free. Mark out the skinincision such that the length and width of the anterior flapadequately covers the posterior defect that is to be created(Fig 12-3A)
• Make an incision superiorly across the iliac crest to themidlateral point, around the buttock just lateral to the anus, andto the midmedial point of the thigh. Carry the incision down thethigh a distance adequate to cover the posterior defect, acrossthe front of the thigh to the midlateral point, and superiorly tojoin the superior incision.
• Perform the posterior dissection first. Preserve a skin margin of3 cm from the anus. Detach the gluteus maximus andsacrospinalis from the sacrum. Detach the external oblique,sacrospinalis, latissimus dorsi, and quadratus lumborum musclesfrom the iliac crest.
• Flex the hip, and place the tissues in the region of the glutealcrease under tension. Detach the remaining origins of the gluteusmaximus from the coccyx and sacrotuberous ligament (Fig. 12-38). 81untly dissect lateral to the rectum into the ischiorectalfossa.
• Move to the front of the patient, and deepen the anteriorincision at the junction of the middle and distal thirds of thethigh through the quadriceps to the femur. Continue thedissection laterally from this point in a cephalad direction to theanterior superior spine severing the vastus lateral is from thefemur and separating the tensor fascia femoris from its fasciasuch that it is included with the specimen (Fig. 12-3C) .
• Start the medial dissection at Hunter's canal, and ligate anddivide the superficial femoral vessels. Trace the vessels superiorlyto the inguinal ligament, dividing and ligating multiple smallbranches to the adductor muscles.
• Place upward traction on the myocutaneous flap, and detachthe vastus medialis and intermedius from the femur.
• Ligate and divide the profunda femoris vessels at their originfrom the common femoral artery and vein.
![Page 6: [Chapter 12] Amputations of the Hip and Pelvis](https://reader034.fdocuments.in/reader034/viewer/2022042502/54654bcdaf795979338b4d41/html5/thumbnails/6.jpg)
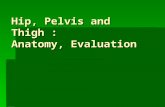
Gluteus maximus(ligamentous and
coccygeal attachments)
.FII Anterior flap hemipelvectomy. A, Anterior and posterior incision. B, Detachment ofgluteus maximus origins from coccyx and sacrotuberous ligament. C, Severing vastus lateralisfrom femur and separating tensor fascia femoris from fascia.
TECHNIQUE 12·4-cont'd
• Separate the myocutaneous flap from the pelvis by releasingthe abdominal muscles from the iliac crest, the sartorius from theanterior superior spine, the rectus femoris from the anteriorinferior spine, and the rectus abdominis from the pubis (Fig.12-3D)
• Retract the flap medially, and dissect along the femoral nerveinto the pelvis to expose the iliac vessels.
• Divide the symphysis pubis while protecting the bladder andurethra.
• Ligate and divide the internal iliac vessels at their origin fromthe common iliacs. While placing medial traction on the bladderand rectus, divide the visceral branches of the internal iliacvessels. Divide the psoas muscle as it joins the iliacus, and dividethe underlying obturator nerve, but protect the femoral nerve
going into the flap. Divide the lumbosacral nerve and the sacral
nerve roots (Fig. 12-3E).
• Put traction on the pelvic diaphragm by elevating theextremity, and divide the urogenital diaphragm, levator ani, and
piriformis near the pelvis.
• Divide the sacroiliac Joint and the iliolumbar ligament, andremove the specimen.
• Turn the quadriceps flap onto the posterior defect, andclose the wound over suction drains by suturing the quadricepsto the abdominal wall, sacrospinalis, sacrum, and pelvic
diaphragm.
AFTERTREATMENT The patient may ambulate whencomfort and stability permit. The drains and Foley cathetershould be left in place for several days. Skin slough is muchless common than with the classic posterior flap.
![Page 7: [Chapter 12] Amputations of the Hip and Pelvis](https://reader034.fdocuments.in/reader034/viewer/2022042502/54654bcdaf795979338b4d41/html5/thumbnails/7.jpg)
yj!J,) Adductor magnus
muscle
Superficialfemoral
artery
D, Separation ofmyocutaneous flap. E, Transectionof internal iliac vessels andbranches. (Redrawn from SugarbakerPH, Malawer MM: Musculoskeletalsurgery for cancer, Berlin, 1982,Thieme.)
Profunda femoris artery
Superficial femoris artery
Conservative Hemipelvectomy TECHNIQUE 12-5
Conservative hemipelvectomy is indicated for tumorsaround the proximal thigh and hip that cannot be resectedadequately by limb-sparing techniques and do not requiresacroiliac disarticulation for satisfactory proximal margins.The operation is a supraacetabular amputation that dividesthe ilium through the greater sciatic notch.
• Insert a Foley catheter. Place the patient in a lateral decubitusposition with the operated side up, and secure the patient to thetable so that it can be tilted to either side.
• Start the incision 1 to 2 cm above the anterior superior iliacspine, and continue it posteriorly and laterally across the greatertrochanter to the gluteal crease. Follow the crease to the medial
![Page 8: [Chapter 12] Amputations of the Hip and Pelvis](https://reader034.fdocuments.in/reader034/viewer/2022042502/54654bcdaf795979338b4d41/html5/thumbnails/8.jpg)
mWEI' A, Racquet type of incision. B, Separation ofmuscles from ilium. C, Division of ilium by Gigli saw.(Redrawn from Sherman CD Jr, Duthie RB: Mod!fied hemipelvec-tollly, Cancer 13:51, 1960.)
TECHNIQUE 12-5-cont'd
thigh posteriorly. Begin a second incision from the first incision5 cm below its starting point, and continue it to just above andparallel to the inguinal ligament to the pubic tubercle. Carry theincision posteriorly across the medial thigh to join the firstincision (Fig. 12-4A).
• Perform the anterior dissection first. Divide the abdominal wallmuscles, exposing the peritoneum.
• Bluntly dissect the retroperitoneal space exposing the iliacvessels (Fig. 12-4B). Ligate and divide the external iliac vessels
just distal to the internal iliacs.
• Divide the symphysis pubis, protecting the bladder andurethra.
• Divide the ilium through the greater sciatic notch as follows:bluntly dissect the iliopsoas muscle from the medial wall of theilium by passing a finger from the anterior superior spine to thegreater sciatic notch. Similarly dissect the gluteal muscles fromthe lateral aspect of the ilium. Pass a Gigli saw through thegreater sciatic notch below the origin of the gluteus minimus,and divide the ilium (Fig. 12-4C)
• Now the extremity can be positioned to place the variousmuscle groups under tension so that they can be divided atappropriate levels along with the femoral, obturator, and sciaticnerves. Care should be taken to divide the urogenital and pelvicdiaphragms at their pelvic attachments, protecting the bladderand rectum.
AFTERTREATMENT The drains and Foley catheter are leftin place for several days. Pressure should be kept off theposterior flap for several days after surgery.
Bailey RW, Stevens DB: Radical exarticulation of the extremitiesfor the curative and palliative treatment of malignant neo-plasms,) Balle Joint SIII;g 43A:845, 1961.
Baliski CR, Schachar NS, McKinnon G, et al: Hemipelvectomy:a changing perspective for a rare procedure, Call) SlIrg 47:99,2004.
Boyd HB: Anatomic disarticulation of the hip, SlIrR GYllecolObstet 8-L346, 1947.
Brittain HA: Hindquarter amputation,) BOlle)oillt Surg 31B:10.+,1949.
Burgess EM, Romano RL, Zettl J H: The lIIaTlaRelnent of 101llerextremityalllplltations, TR 10-6, Washington, DC, 1969, VeteransAdministration.
Burgess EM, Traub JE, Wilson AB Jr: IlIImediate postsllrgical pros-thetics ill the lIIanagemellt of lower extremity amputees, TR 10-5,Washington, DC, 1967, Veterans Administration.
Chan JWH, Virgo KS, Johnson FE: Hemipelvectomy for severedecubitus ulcers in patients with previous spinal cord injury,Alii) SlIrg 185:69, 2003.
![Page 9: [Chapter 12] Amputations of the Hip and Pelvis](https://reader034.fdocuments.in/reader034/viewer/2022042502/54654bcdaf795979338b4d41/html5/thumbnails/9.jpg)
Chansky HA: Hip disarticulation and transpelvic amputation:surgical management. [n Smith DG, Michael JW, Bowker JH,eds: Atlas of alllplltatiollS alld lilllb deficielldes: sllI;!;ical, prosthetic,alld rehabiliralioll prillciples, 3rd ed, R.osemont, III, 2004,American Academy of Orthopaedic Surgeons.
Coley BL, Higinbotham NL, Romieu C: Hemipelvectomyfor tumors of bone: report of 14 cases, Alii ) SlIrg 82:27,1951.
Denes Z, Till A: Rehabilitation of patients after hip disarticula-tion, Arch Orthop Tralillta SlIrg 115:498, 1997.
Endean ED, Schwarcz TH, Barker DE, et al: Hip disarticulation:factors affecting outcome,) Vasc SlIrg 14:398, 199J.
Ghormley RK, Henderson MS, Lipscomb PR: [nterinnomino-abdominal amputation for chondrosarcoma and extensivechondroma: report of two cases, Mayo Clill Proc 19:193,1944.
Gordon-Taylor G, Monro RS: Technique and management of"hindquarter" amputation, Br) SlIrg 39:536, 1952.
Gordon-Taylor G, Wiles P, Patey DH, et al: The interinnomino-abdominal operation: observations on a series of fifty cases,)Balle )oillt Surg 3413:14, 1952.
Karakousis CP, Vezeridis MP: Variants of hemipelvectomy, Aliij SlIrg 145:273, 1983.
King D, Steelquist J: Transiliac amputation, ) Balle joillt SlIrg25:351, 19-13.
Lazzari JH, Rack FJ: Method of hemipelvectomy with abdominalexploration and temporary ligation of common iliac artery,AIIII Sill;!; 133:267, 1951.
Littlewood H: Amputations at the shoulder and at the hip, BM)1:381, 1922.
Luna-Perez P, Herrera L: Medial thigh myocutaneous flap forcovering extended hemipelvectomy, Eur) SlIrg Ollcol 21:623,1995.
Masterson EL, Davis AM, Wunder jS, et al: Hindquarter ampu-tation for pelvic tumors, Clill Orrhop Relar Res 350: 187,1998.
Pack GT: Major exarticulations for malignant neoplasms of theextremities: interscapulothoracic amputation, hip-joint disar-ticulation, and interilio-abdominal amputation: a report of endresults in 228 cases,) Balle joil1t SlIrg 38A:249, 1956.
Pack CT, Ehrlich HE: Exarticulation of the lower extremities formalignant tumors: hip joint disarticulation (with and withoutdeep iliac dissection) and sacroiliac disarticulation (hemipel-vectomy), AIIII SlIrg 123:965, 1946; 12-l:1, 19-16.
Phelan JT, Nadler SH: A technique of hemipelvectomy, SIII:r;CYllecol Obstet 119:311, 1964.
Pinzur MS, Angelats J, Bittar T: Salvage of failed amputationabout the hip in peripheral vascular disease by open woundcare and nutritional support, AII1) Orthop 8:561, 1998.
Ross DA, Lohman RF, Kroll SS, et al: Soft tissue reconstructionfollowing hemipelvectomy, AII1) S,I1:r; 176:25, 1998.
Sara T, Kour AK, De SD, et al: Wound cover in a hindquarteramputation with a free flap from the amputated limb, ClillOrthop Relat Res 304:248, 1994.
Slocum DB: Arias of all/p"tat"o"s, St Louis, 1949, Mosby.Sorondo JP, Ferre RL: Amputacion interilioabdominal, All
Orthop Tralllltatol 1:143, 1948.Troup J13, Bickel WH: Malignant disease of the extremiries
treated by exarticulation: analysis of two hundred and sixty-four consecutive cases with survival rates,) Balle joillt SlIrg-l2A:1041, 1960.