OF THE HIP & PELVIS - Master the Hip | Dr Alison Grimaldi
56
UNDERSTANDING TENDINOPATHIES OF THE HIP & PELVIS BOOK TWO: Greater Trochanteric Pain Gluteal Tendinopathy & Associated Pathologies
Transcript of OF THE HIP & PELVIS - Master the Hip | Dr Alison Grimaldi

UNDERSTANDINGTENDINOPATHIES
OF THE HIP & PELVIS
BOOK TWO: Greater Trochanteric PainGluteal Tendinopathy & Associated Pathologies

P A G E 2 O F 5 6 Copyright Alison Grimaldi 2018
IntroductionTendinopathies of the hip and pelvis represent a large burden on both the sporting and ageing populations. Growing evidence is shaping contemporary conservative management of tendinopathy.
This e-book series aims to provide readers with guidance towards a deeper understanding of tendinopathies of the hip and pelvis and more effective clinical management based on an emerging evidence base derived from scientific studies on structure and mechanobiological mechanisms, risk factors, impairments and the available information on effects of intervention.
Book 2 of this series builds on the understanding of mechanobiological mechanisms associated with tendinopathy and explores specific research findings for gluteal tendinopathy and the clinical implications for assessment and management of this common condition. A review of the local anatomy and patho-anatomy lays the groundwork for the proposed pathoaetiological model that underpins the assessment and management strategies presented. A firm evidence base from the available scientific literature is combined with over 25 years of clinical experience to provide clinically relevant and readily applicable information.
For more information
email [email protected] (07) 3342 4284web dralisongrimaldi.com
Is this e-book suitable for you?This book is suitable for anyone involved in management of tendinopathies of the hip and pelvis or prescription of exercise in at-risk groups – such as the athletic population or perimenopausal women. The content assumes readers have a basic knowledge of anatomy and muscle function in this region.

P A G E 3 O F 5 6Copyright Alison Grimaldi 2018
BOOKCONTENTS
Chapter 1 IMPACT AND PREVALENCE . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
Chapter 2 CLINICAL PRESENTATION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Chapter 3 REVIEW OF LOCAL ANATOMY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
Chapter 4 PATHOLOGY & TERMINOLOGY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
Chapter 5 PATHO-AETIOLOGY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
Chapter 6 IMPAIRMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
Chapter 7 DIAGNOSIS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
Chapter 8 MANAGEMENT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36
FINAL THOUGHTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50
REFERENCE LIST . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51

P A G E 4 O F 5 6 Copyright Alison Grimaldi 2018
CHAPTER ONEIMPACT & PREVALENCE
IMPACTPainDisabilityQuality of lifeSleepActivityEmployment
PREVALENCEGenderAgegroupHormonal statusAssociation with other conditions

P A G E 5 O F 5 6Copyright Alison Grimaldi 2018
Symptomatic gluteal tendinopathy has been rated the most common lower limb tendinopathy for which people seek help from a medical practitioner (Albers et al 2014).
The Impact of Gluteal Tendinopathy
Lateral hip pain associated with gluteal tendinopathy is a common condition in older females particularly, with the potential to impart a large societal burden on a gradually ageing population.
Symptomatic gluteal tendinopathy results in moderate to severe disability, with impacts on quality of life and functional ability equal to that of end stage hip osteoarthritis (Fearon et al 2014a). Pain in sidelying in individuals with this condition often has a substantial effect on quality and volume of sleep, with subsequent wider implications for general health. Pain and poor loadbearing capacity in single leg weightbearing impinges on many functional tasks in activities of daily living, work and sport. As a result, participation in sport, recreational exercise and employment may be reduced (Fearon et al 2014a).
Prevalence
This condition is most common in peri and post-menopausal females, present in 23.5% of women and 8.5% of men between the ages of 50 and 79 (Segal et al 2007). Although the prevalence is unknown in younger age groups, clinical presentations occur in younger runners and those participating in group activities involving step-up or lunging tasks. The incidence in runners and triathletes is expected to rise with increasing age of participants and increasing percentages of female athletes. The average age of a participant entering a road race in the USA is now 40, with more than 43% of triathletes aged over 40 and 38% female (Fields 2011, Lepers et al 2013, Wright 2012).
Gluteus medius and minimus tendinopathy may co-exist with hip joint pathology. Degenerative tears of the gluteus medius or minimus tendons have occur in 20% of patients with osteoarthritis (OA) of the hip (Howell et al 2001). Prevalence of earlier stages of tendinopathy in those with hip OA is therefore likely to be much higher. In clinical practice, coexistance of tendon and joint pathologies in the hip region is common.
Gluteus medius tendinopathy also occurs in 20-35% of patients with lower back pain. Due to the pseudoradicular referral pattern of gluteal tendinopathy, it is often misdiagnosed as lumbar pathology, leading to delays in diagnosis and treatment, some patients proceeding to unsuccessful lumbar surgery (Collee et al 1991, Tortolani et al 2002).
Considering the substantial impact of this condition and issues with delayed and inaccurate diagnosis, greater awareness of health practitioners regarding early and effective diagnostic testing and intervention is required.

P A G E 6 O F 5 6 Copyright Alison Grimaldi 2018
Figure 1: Prevalence of gluteal tendinopathy
Gluteal Tendinopathy
Prevalence
23.5% of females aged 50-79
8.5% of males
aged 50-79
Most common
lower limb tendinopathy
Increasing in runners & triathletes
Tendon tears in 20% with
hip OA
1° pain source in 20-35%
with LBP
>

P A G E 7 O F 5 6Copyright Alison Grimaldi 2018
CHAPTER TWOCLINICAL PRESENTATION
AREA & NATURE OF PAIN
PAINFUL POSTURES & ACTIVITIES
HISTORY OF SYMPTOM ONSET

P A G E 8 O F 5 6 Copyright Alison Grimaldi 2018
Area & Nature of PainThe most identifying feature of gluteal tendinopathy is pain and tenderness directly over the greater trochanter (Bird et al 2001, Grimaldi et al 2017, Lequesne 2006, Strauss et al 2010, Woodley et al 2008). Pain also commonly extends down the lateral thigh and even into the top of the lower leg, below the knee. There may also be a few centimetres radiation anterior or posterior to the greater trochanter. Consider other sources for pain further anterior, posterior or superior to the greater trochanter.
Other descriptions may include aching or burning down the lateral thigh. Burning pain is often thought to indicate a neurogenic source. Certainly a full assessment of the lumbar spine and relevant neural structures would be appropriate, but in clinical practice this description may be used by those with painful gluteal tendinopathy, in the absence of demonstrable neurogenic signs.
There may sometimes be report of sharp pain and even giving way during weightbearing tasks. It is important to clarify the exact area of pain, as sharp pain may also indicate intra-articular pathology or neuralgia. Sharp pain associated with gluteal tendinopathy should occur directly over the greater trochanter and may shoot down the lateral thigh a little, but not past the knee. This may occur for example as the hip drops into adduction during stair descent or a single leg squat and the iliotibial band (ITB) wraps firmly around the greater trochanter. A feeling of giving way in this circumstance is generally reflective of pain inhibition and rarely results in full collapse.
Sharp pain may be associated with a report of snapping or clicking. ‘ Lateral snapping hip’ occurs when the ITB snaps across the greater trochanter (Lee et al 2013). The physical slipping of the ITB is usually readily palpable.

P A G E 9 O F 5 6Copyright Alison Grimaldi 2018
Painful Postures & ActivitiesThe pain associated with gluteal tendinopathy is often worse at night, lying on either side, and may be aggravated by walking or running, particularly uphills and stairs and other single leg loading tasks such as standing on one leg to dress. Pain may develop during prolonged sitting, particularly in low seats or in the car and pain and stiffness for the first few steps after rising to stand is commonly reported.
History of Pain OnsetGluteal tendinopathy commonly becomes symptomatic when a weakened tendon is exposed to a sudden increase in loading such as taking up power walking, particularly walking up hills, moving to a new house that has lots of stairs, or going on holidays that involve lots of hill climbing or stair climbing. Presentation may occur after a slip or fall or a direct impact to the greater trochanter, where the tendon has been exposed to a large, sudden tensile or compressive load.
Often it may be difficult for the patient to identify a particular incident and the pain would appear to be of a more insidious onset, gradually becoming more symptomatic. This may be associated with a gradual deterioration of tendon health over time, so that eventually even everyday loads represent a situation of overload for the tendon, and subsequent onset of tendon pain.
General health questioning may reveal a change in hormonal status around menopause, a recent injury in an adjacent area resulting in a shift in load to the painful hip, mental health or immune stressors, a history of systemic disease, long term glucocorticoid use, statin use or a recent course of fluoroquinolone antibiotics. As discusssed in Book 1 of this series, any of these factors may increase risk of developing painful tendinopathy.

P A G E 1 0 O F 5 6 Copyright Alison Grimaldi 2018
CHAPTER THREEREVIEW OF LOCAL ANATOMY
THE ABDUCTOR SYNERGYITB TensionersTrochanteric Abductors
TROCHANTERIC ANATOMYFacetsTendon InsertionsBursae

P A G E 1 1 O F 5 6Copyright Alison Grimaldi 2018
The Hip Abductor SynergyThe muscles of the abductor synergy can be subdivided into two groups - the ITB tensioners (Figure 2 below) and the trochanteric abductors (Figure 3). The ITB tensioners exert their effect via the iliotibial band, contributing to abduction and helping balance the pelvis on the femur in single leg stance. This layer includes the tensor fascia lata (TFL) and the upper portion of the gluteus maximus (UGM), the portion of the gluteus maximus that sits above the centre of rotation of the head of the femur. The UGM inserts heavily into the ITB and has a primary abductor function rather than an extension function, like the lower portion of the gluteus maximus. TFL and UGM constitute the superficial layer of the abductor synergy. The vastus lateralis (VL), although it cannot be considered an abductor of the hip as it does not cross the hip joint , acts as a hydraulic amplifier for the iliotibial band by swelling beneath the band, and thereby increasing the tension in the band (Birnbaum et al 2004, Vleeming et al 1997). Pretensioning of the ITB allows greater effect from TFL and UGM contraction. The VL can therefore also be considered an ITB tensioner.
THE ITB TENSIONERS
TFL UGM VL
The most superficial layer of the abductor synergy, exerting it’s effect via tensioning of the ITB
Figure 2: The ITB Tensioners. UGM: Upper Gluteus Maximus; TFL: Tensor Fascia lata; ITB: Iliotibial Band; VL: Vastus Lateralis
TFL
ITB
VL
UGM

P A G E 1 2 O F 5 6 Copyright Alison Grimaldi 2018
Figure 3: The trochanter abductors.
The intermediate and deep muscle layers of the abductor synergy exerting their effect via direct attachment to the greater trochanter.
THE TROCHANTERIC ABDUCTORS
GLUTEUS MEDIUS GLUTEUS MINIMUS

P A G E 1 3 O F 5 6Copyright Alison Grimaldi 2018
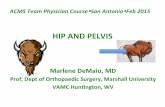
TROCHANTERIC ANATOMY
The gluteus medius and minimus muscles attach to the various facets of the greater trochanter. The greater trochanter has four facets: the anterior, lateral, posterior and the smaller superoposterior facet. The gluteus medius has two main bony attachments. The posterior muscle fibres insert onto the superoposterior facet via a stout tendon with a footprint of approximately 2cm2. The central and all of the anterior muscle fibres attach to the lateral facet with a fairly rectangular footprint of around 4cm2. The gluteus minimus has both a muscular insertion into the anterosuperior joint capsule and a tendinous insertion into the anterior facet of the greater trochanter. Its tendon is relatively longer than that of the gluteus medius. (Dwek et al 2005, Pfirrmann et al 2001, Robertson et al 2008)
Figure 4: Anatomy of the greater trochanter. Facets: ANT= Anterior; LAT = Lateral; Post = Posterior; SUP-POST= Superoposterior. Tendon Insertions: GMED:Gluteus Medius; GMIN: Gluteus Minimus. Bursae: SUB GMAX/TB: Sub-Gluteus Maximus/Trochanteric Bursa; SUB GMED: Sub-Gluteus Medius; SUB GMIN: Sub-Gluteus Minimus
ANTPOSTLAT
SUP-POST
GMED
SUBGMAX or TB
SUB GMED
SUBGMIN
Bald Spot
There are three main bursae at the lateral hip – the subgluteus minimus bursa that sits over the anterior facet, cushioning the gluteus minimus tendon as it crosses over to its insertion point. The subgluteus medius bursa covers the bald spot on the lateral facet and similarly helps protect the gluteus medius tendon from the underlying bone.The better known trochanteric bursa, now also referred to as the subgluteus maximus bursa is the largest and most superficial bursa. It covers the posterior facet, the distal lateral part of the gluteus medius tendon attachment, and the proximal part of the vastus lateralis insertion at the base of the greater trochanter. This bursa helps facilitate sliding of the iliotibial band and the more lateral fibres of the gluteus maximus over the posterior and lateral aspects of the greater trochanter and the inserting gluteus medius tendon. (Pfirrmann
et al 2001)
GMEDGMIN
TENDONINSERTIONS BURSAEFACETS

P A G E 1 4 O F 5 6 Copyright Alison Grimaldi 2018
CHAPTER FOURPATHOLOGY & TERMINOLOGY
TROCHANTERIC BURSITIS
TENDINITIS, TENDINOSIS, TENDINOPATHY OR ENTHESOPATHY?
ITB FASCIOPATHY
GREATER TROCHANTERIC PAIN SYNDROME

P A G E 1 5 O F 5 6Copyright Alison Grimaldi 2018
Trochanteric BursitisLateral hip pain has traditionally been referred to as trochanteric bursitis.Radiological studies have now shown however that bursal distension is an inconsistent feature of lateral hip pain, with various studies demonstrating bursal distension in only 8 - 20% of subjects with lateral hip pain (Bird et al 2001, Connell et al 2003, Long et al 2013). Bursal pathology is rare in isolation, usually co-presenting with tendon pathology. The incidence of bursal pathology appears to increase with severity of the tendon pathology. This is reflected in the report of bursal pathology in at least 50% of patients with more severe gluteal tendon pathology, undergoing surgical reconstruction of the gluteal tendons (Fearon et al 2010).
The use of the term ‘trochanteric bursitis’ as a diagnosis for lateral hip pain is not recommended for a number of reasons:
1. It suggests that trochanteric busitis is the primary pathology associated with lateral hip pain, which research has now demonstrated is incorrect.
2. Bursal distention can occur not only in the trochanteric bursa (sub-gluteus maximus bursa), but also the gluteus medius and minimus bursae).
3. Histological studies have so far been unable to demonstrate traditional cellular inflammation within the bursa, calling into question the suffix ‘itis’ ( Fearon et al 2014b, Silva et al 2008).
We cannot rule out at this stage that an acute inflammatory process may occur at an earlier point in the pathology, and certainly there is evidence of increased expression within the bursa of at least one inflammatory mediator, Substance P, in this population (Fearon et al 2014b). In the absence of histological evidence of cellular inflammation it may be prudent however to refer to bursal abnormality, where it is present, as bursal distension, enlargement or thickening. Use of the term ‘trochanteric bursitis’ has historicially engendered approaches that are primarily anti-inflammatory in nature (rest, ice, ultrasound) and targeted at the bursa (bursectomy, bursal corticosteroid injection).
Figure 5: Bursal thickening on ultrasound image. GT: Greater trochanter
GT
skin

P A G E 1 6 O F 5 6 Copyright Alison Grimaldi 2018
Tendinitis, Tendinosis Tendinopathy or Enthesopathy?While bursal distension does occur in those with lateral hip pain, numerous radiological and surgical studies have shown that bursal distension is almost always a secondary finding associated with a primary pathology of gluteus medius or minimus tendons (Bird et al 2001, Connell et al 2003, Dwek et al 2005, Kingzett-Taylor et al 1999, Kong et al 2007, Pfirrmann et al 2005, Woodley et al 2008).
So what is the correct term with respect to labelling the tendon disorder? The term tendinopathy is used where there is no histological evidence available to confirm either an inflammatory process which would be referred to as tendinitis, or a degenerative process, which would be referred to as tendinosis. The term tendinopathy is then most commonly selected, denoting a painful tendon condition. As gluteal tendinopathy occurs at the tendon insertion or enthesis, it can be referred to as an insertional tendinopathy or enthesopathy.
Tendinopathy may affect either or both of the gluteus medius and minimus tendons. As discussed in detail in Book 1 of this series, tenocytes within a pathological tendon increase production of large proteoglycans which are hydrophilic, binding water molecules. On MRI, the pathological tendons will appear hyperintense, or white (Figure 6 below). This does not necessarily indicate an inflammatory process but reflects the higher water content associated with the tendinopathic process.
Pathology in the gluteal tendons can progress to partial and full thickness tears and in severe cases, full rupture. Partial thickness tears tend to begin at the undersurface, closest to the bone, progressing eventually through the full thickness of the tendon. Tears are most common in the anterior portions of the tendons, extending posteriorly as the pathology progresses. (Thaunat et al 2016, Walsh et al 2011)
Bony spurring may also be evident within the gluteal tendons on imaging. This is consistent with shifts in cell type in the deep compressive zone of a tendon enthesis towards chondrocytes and osteocytes, in the presence of insertional tendinopathy (CCook & Purdam 2012).
Figure 6: Hyperintensity of gluteal tendons on MRI; Right (R) worse than left (L)

P A G E 1 7 O F 5 6Copyright Alison Grimaldi 2018
ITB Fasciopathy?
The iliotibial band itself as a source of nociception in those with lateral hip pain, is not commonly discussed in the literature. Clinically during ultrasound imaging, thickening of the iliotibial band certainly appears to be evident in some patients with gluteal tendinopathy (Figure 7 below). One large ultrasound study assessed thickening of the ITB in those with lateral hip pain and found it to be more common than bursal thickening - 29% versus 20% incidence (Long et al 2013). Another imaging paper also described findings of thickening and tearing of the ITB in a subset of patients with lateral hip pain, suggesting the ITB as an important pain source (Huang et al 2013).
The iliotibial band has a trilaminar structure, with two dense connective tissue layers, evident on ultrasound as white (hyperechoic) lines, sandwiching a darker (hypoechoic) loose connective tissue layer (Figure 7 above). Fascia is known to be highly innervated and the loose connective tissue layer is rich in nerve endings As within tendon tissue, fibroblasts within fascia are mechanosensitive and the source of the extracellular matrix components - collagen, elastin and proteogylcans. Similarly, these
Figure 7: Thickening of the Iliotibial band (ITB). Normal thickness between green arrowheads; thickening evident between pink arrowheads as ITB wraps over the greater trochanter. GMED:Gluteus Medius; GMIN: Gluteus Minimus; GT:Greater Trochanter; HOF:Head of Femur.
GMIN
GMED
GT
HOF
ITB
Distal Proximal
fibroblasts and resident mast cells can produce inflammatory mediators such as Substance P. (Klingler et al 2014, Szotek et al 2016).
The iliotibial band may respond to excess loads through structural change and become an additional source of pain, a ‘fasciopathy’ similar to plantar fasciopathy. This may provide some explanation for the pain in some with gluteal tendinopathy, that extends down the lateral thigh and into the upper leg, along the line of the ITB.

P A G E 1 8 O F 5 6 Copyright Alison Grimaldi 2018
GTPSThe umbrella term ‘Greater Trochanteric Pain Syndrome’ has also been used for pain in this region. This non-specific term however does little to provide the clinician with information regarding the structures involved, the nature of the condition or any guidance towards a possible management approach. Furthermore, from a patient perspective, the label ‘syndrome’ may reflect a lack of clarity in both diagnosis and treatment direction, possibly reducing a patient’s confidence and increasing their anxiety.
GTPS has also had variable definitions over the years, some including more distant referral sources such as the lumbar spine, pelvis and intra-articular hip pathologies. When using this term, the definition should be clearly outlined.
SummaryWhile recognising that nociception from this region is likely to be derived from multiple local soft tissue sources, gluteal tendinopathy is the primary and most consistent pathology (Figure 8). Treatment aimed at optimising load and health in this structure will provide similar benefits for adjacent soft tissues that have been influenced adversely by the same patho-aetiological factors.
P A G E 1 8 O F 6 2 Copyright Alison Grimaldi 2018

P A G E 1 9 O F 5 6Copyright Alison Grimaldi 2018
ITB THICKENING
GREATER TROCHANTERIC PAIN
BURSALTHICKENING
GLUTEAL TENDON PATHOLOGYTendinopathy/Enthesopathy
Calcification, Tears
Figure 8: Pathologies associated with greater trochanteric pain

P A G E 2 0 O F 5 6 Copyright Alison Grimaldi 2018
CHAPTER FIVEPATHO-AETIOLOGY
MECHANICAL FACTORSCompressionStress ShieldingProblem Postures & ActivitiesThe Impact of Bony Morphology

P A G E 2 1 O F 5 6Copyright Alison Grimaldi 2018
As explored in detail in Book 1 of this series, aetiology of tendinopathy is multifactorial with both mechanical and systemic health factors playing variable roles in different individuals and regions. Age, gender and hormonal status appear important factors in the development of symptomatic gluteal tendinopathy, considering the relatively higher prevalence in peri and post-menopasual women. With menopause, many women also experience weight gain, particularly in a gynoid distribution which has been linked with the development of tendinopathy in females (Gaida et al 2010) and evident in those with lateral hip pain (Fearon et al 2012).
Figure 9: Mechanbiological response to compressive load combinations in the soft tissues of the greater trochanter
Mechanical Factors
This chapter will focus on the proposed patho-mechanics underlying the development of gluteal tendinopathy and associated soft tissue pathology at the greater trochanter.
The pathological changes in the tendon, bursae and iliotibial band discussed in the previous chapter may all be a cell response to an adverse mechanical loading scenario. Stress shielding, compression and compression-tension combinations induce structural change that
will reduce tensile loading capacity and increase risk of pain and functional load intolerance (see Book 1 for detailed review).
Thickening of the gluteal tendons, ITB and bursae via increased fibroblast expression of larger proteoglycans and binding of more water molecules may be an adaptation to improve tolerance of compressive load combinations. Shifts towards chondrocytes and osteocytes may also reflect such an adaptation, both more tolerant of compressive loading than tenocytes. Such structural change however, leaves these tissues less able to transfer tensile loads (Figure 9 below).

P A G E 2 2 O F 5 6 Copyright Alison Grimaldi 2018
The gluteus medius and minimus tendons are at risk of compression between the bony greater trochanter into which they insert, and the thick, overlying iliotibial band. Postural habits such as hanging on one hip, or excess adduction in dynamic function will result in significant increases in tension in the iliotibial band, and therefore in compressive loading of the underlying tendons and bursae, and even of the iliotibial band itself against the bony trochanter.
Birnbaum and colleagues demonstrated that rapid increases in compressive loading occur beneath the ITB at the greater trochanter as the hip is moved into adduction. In neutral hip adduction, the ITB exerts only 4 Newtons (N) of compression. This has risen to 36N by 10° adduction and to 106N by 40° (Figure 10). Exposure of the trochanteric soft tissues to excessive compression associated with hip adduction may be a primary factor underpinning the structural changes characteristic of symptomatic gluteal tendinopathy (Birnbaum et al 2004).
4N 36N 106N0° 10° 40°
COMPRESSION EXERTED BY ITB INCREASES WITH ADDUCTION
X 9 X 26.5
Gluteus Medius
Gluteus Minimus
ITBGluteus Maximus
TFL
ITB
Birnbaum et al. 2004
Figure 10: Compressive loads exerted by the Iliotibial band (ITB) at the greater trochanter (Birnbaum et al 2004)

P A G E 2 3 O F 5 6Copyright Alison Grimaldi 2018
What common postures & activities involve adduction?
Postural habits such as standing hanging passively in hip adduction, resting on the iliotibial band and sitting with knees crossed, or knees together, will result in greater periods of time spent in relative hip adduction.
In functional tasks involving single leg loading such as walking, running, stairclimbing and many other sports and recreational activities, hip adduction is normal, but too much adduction too often, under high loads, over an extended period of time.... may induce adaptive structural change in the trochanteric soft tissues and predispose to intolerance of tensile loads.
How much is too much? There is no clear evidence for limit values and this would be difficult to ascertain as there are so many factors that may determine the relative response in the tissues. However, the evidence is clear, we know that hip adduction induces compressive load on the trochanteric soft tissues and that excessive compression or compressive load combinations are a potent catalyst for structural change within tendon tissues (and likely fascial and bursal tissues as well) - see Book 1 of this series for detailed review of this process.
Clinically, we need to ascertain if our patient with painful trochanteric soft tissues, is using adduction that is:
- of high degree > 10°- repetitive- sustained for long durations- performed under high load- any combination of the above.
Stress shielding of the gluteal tendons in adduction
Structural changes may also be induced in adduction by way of relative stress shielding - reduced tensile loading of the deep aspects of the gluteal tendons. At the shoulder, the deep fibres of the supraspinatus tendon that wrap closest around the underlying bone have been shown to be not only compressed but also relatively shielded from tensile load in lower ranges of shoulder abduction (Bey et al 2002). With increasing ranges of abduction, compression on these deep fibres reduce while tensile loading increases. It would seem reasonable that a similar premise would hold true for the deep fibres of the gluteal tendons.Hip adduction may then represent a situation of both high compressive load and stress shielding of the deeper fibres of the gluteal tendons from tensile load.
Degree of hip adduction may also influence the relative recruitment or load acceptance of different parts of the abductor synergy. Kumagai et al. demonstrated that the more superficial portion of gluteus medius was significantly more active when the abductor synergy was loaded in adduction, compared to an abducted or neutral hip position (Kumagai et al 1997). Loading in a position of hip adduction also pretensions the ITB, thereby providing a mechanical advantage for the ITB tensioners. Kummer determined that the ITB tensioners would control 30% of the bodyweight in single leg stance, while the trochanteric abductors would be responsible for the other 70% (Kummer 1993). In postures of increasing adduction, there may be a shift towards higher loads in the ITB tensioners and more superficial portions of the gluteus medius, consistent with a situation of higher compressive loads and reduced tensile loads for the deep gluteal tendon fibres.

P A G E 2 4 O F 5 6 Copyright Alison Grimaldi 2018
The impact of bony morphologyBirnbaum and colleagues also examined the influence of femoral neck angle on the force exerted by the ITB across the femur (Birnbaum et al 2010). In a biomechanical modelling study, reducing the femoral neck angle from a typical average physiological angle of 128° down to 115° (coxa vara), resulted in a significant increase in ITB load, rising approximately 50%.
In one clinical study, lower neck-shaft angles were reported in patients with painful, advanced gluteal tendon pathology (Fearon et al 2012). Another group demonstrated that those with lateral hip pain had a trochanteric width 28mm greater than their pelvic width compared to a difference of only 17mm in a painfree control group (Viradia et al 2011). Those with ‘wider hips’ relative to their pelvis may then be at risk of higher compressive loads at the greater trochanter as the ITB wraps around the more prominent trochanters. Fearon et al. (2012) however didn’t show an association with trochanteric width.
Moulton et al. (2015) were unable to demonstrate an association between femoral neck angle and the presence of gluteal tendinopathy on a retrospective magnetic resonance imaging (MRI) series. They did however find a correlation with increased acetabular anteversion (Moulton et al 2015). Increased acetabular anteversion may possibly encourage greater functional use of internal rotation/ adduction actions. The draw back of the study however, is that there is no clinical data on the subjects to indicate whether or not the patients with gluteal tendinopathy were suffering with lateral hip pain. The evidence suggests there are links between bony structure, forces imposed on the femoral soft tissues and presence of pathology. Further evidence is required to establish clear relationships with painful soft tissue pathologies of the greater trochanter.
As discussed previously, a single severe mechanical risk factor alone may be enough to induce structural change in the trochanteric soft tissues and ultimately pain and disability, but more often there is likely to be a combination of multiple milder risk factors. The challenge for the clinician is to be aware of the various potential contributors, assess for those features, adapt the strategy as necessary for the non-modifiable factors (such as bony morphology, age, sex, rheumatological disease etc) and focus on optimising the modifiable factors.

P A G E 2 5 O F 5 6Copyright Alison Grimaldi 2018
CHAPTER SIXIMPAIRMENTS
MUSCLE DEFICITSLength of the Abductor MechanismMuscle SizeMuscle StrengthMuscle Recruitment (EMG)
GAIT KINEMATICS & KINETICS The External Hip Adduction MomentKinematic Variables Impacting on Adduction Moments

P A G E 2 6 O F 5 6 Copyright Alison Grimaldi 2018
Muscle DeficitsLength of the Abductor MechanismConsidering the whole premise for the physical and surgical treatments for trochanteric bursitis was that the ITB was shortened and required lengthening, it is surprising that no evidence is provided to support such treatment approaches (Farr et al 2007).
The Ober’s and Modified Ober’s tests were both performed on patients with lateral hip pain in Woodley et al.’s comprehensive study (Woodley et al 2008). These tests were frequently positive in their subjects with lateral hip pain but did not provide a useful likelihood ratio. The tests were also deemed positive if either the range of motion was reduced and/or the pain was reproduced. Details about the most common mechanism for a positive test were not provided, so unfortunately it is not possible to make any assumptions from this paper on length of the abductor mechanism.
Fearon et al. found a painful, restricted Ober’s test to be indicative of greater trochanteric pain syndrome in those with non-specific hip pain (Fearon et al 2013) . However, a comparison of range of motion between those with lateral hip pain and asymptomatic controls was not performed. Certainly pain on passive hip adduction in the Ober’s test position has recently been found to be a useful indicator of the presence of painful gluteal tendinopathy (Grimaldi et al 2017), but clear evidence for a shortened abductor mechanism is lacking.
Clinically, patients presenting with painful gluteal tendinopathy are much more likely to have a lengthened abductor mechanism and test ‘long’ on an Ober’s test. This is the typical female patient who spends much of their day resting or functioning in excessive adduction. There is a subcategory of patients however, that presents with a restricted Ober’s test, generally male patients who sit and stand habitually in abduction or either males or females who use saddle chairs extensively. Regardless of the length, stretching is unlikely to be useful due to the provocative compressive forces applied across the greater trochanter (Figure 11).
Excesspostural adduction
Increased length of abductor mechanismLong but painful on modified Ober’s test
Excess functional adduction
MOST COMMON
Excesspostural abduction
Decreased length of abductor mechanismShort and painful on modified Ober’s test
Normal or reduced
functional adduction
LESS COMMON
Figure 11: Length of the abductor mechanism in patients with painful gluteal tendinopathy - two main presentations.
STRETCHING UNWARRANTED& PROVOCATIVE
STRETCHING PROVOCATIVE

P A G E 2 7 O F 5 6Copyright Alison Grimaldi 2018
Muscle SizeMRI studies have shown changes in abductor muscle size and quality in those with lateral hip pain. There is clear evidence of gluteus medius and minimus fatty atrophy in these patients (Pfirrmann et al 2005, Woodley et al 2008) (Figure 12 below), while similar changes in gluteus maximus and TFL are uncommon (Sutter et al 2013, Woodley et al 2008). In one small study, TFL was reported to be hypertrophied in those with gluteal tendon tears (Sutter et al 2013).
A B
C D E
Figure 12: MRI images demonstrating gluteal atrophy in patients with painful gluteal tendinopathy. A: Normal comparison frontal plane image. B: Marked atrophy of gluteus minimus and atrophy of deep, distal fibres of gluteus medius. C: Normal axial image for comparison. D: Diffuse atrophy of anterior gluteus minimus and medius. E: Block atrophy of central portion of gluteus minimus. Gluteus Minimus: pink asterisks and arrows; Gluteus Medius: green asterisks and arrows.
*
*
**
**
*
*

P A G E 2 8 O F 5 6 Copyright Alison Grimaldi 2018
Muscle StrengthAlthough abductor weakness was often noted in the literature with respect to gluteal tendinopathy or greater trochanteric pain syndrome, it was only recently that this was tested in a scientific study. Allison et al. demonstrated that participants with unilateral symptomatic gluteal tendinopathy were on average 32% weaker on the painful side and 23% weaker in hip abduction on the asymptomatic side than a painfree control group (Allison et al 2016a). Therefore, although the symptomatic abductors were 11% weaker than the asymptomatic side in the gluteal tendinopathy group, both hips were weaker than age and sex matched controls.
It is unclear whether changes in abductor size and strength precede or are a result of the pain and loading changes associated with gluteal tendinopathy. The effect may conceivably occur in either or both directions and vary between individuals. Also note that not all painful patients presenting for management of lateral hip pain will have atrophy and or strength deficits. For the clinician, the evidence suggests that abductor strength and muscle bulk should be assessed and that demonstrated impairments would be targets for rehabilitation.
Muscle RecruitmentRecently, fine wire electromyography studies have provided valuable information on abductor muscle recruitment during walking in those with painful gluteal tendinopathy. Ganderton et al. found that the anterior portion of gluteus minimus, usually most active in mid-late stance, also became very active in early stance phase in those with lateral hip pain (Ganderton et al 2017). Overall, increases in average activity levels were reported for all portions of gluteus minimus and medius and their recruitment pattern was less variable that the painfree control group.
Allison et al. recorded an extended burst of activity in the middle and posterior portions of gluteus minimus and medius in early to mid stance, where the limb is accepting weight and the hip reaches peak adduction (Allison et al 2018). They also reported greater contribution of TFL activity to this loading phase, suggesting that the ITB would be under greater tensile load and able to induce higher compressive loads on the underlying trochanteric soft tissues. Reduced recruitment variability was also evident.
Overall, the findings suggest that those with painful trochanteric soft tissue pathology activate their abductors at a higher level and for more extended bursts. Together with the reduced variability demonstrated by both studies, it means more motor units and the same motor units are recruited again and again and for longer periods. This results in increased co-contraction , a loss of precision and a loss of normal load sharing-load sparing strategies. The gluteal tendons and associated bursae may therefore be exposed to greater tensile and compressive loads.
Why are the muscles behaving this way? The associated lack of abductor strength may mean that more motor units are required to meet the demands of walking. Co-contraction strategies are also employed to splint a painful area. Both strengthening and motor control approaches are then likely to be required.

P A G E 2 9 O F 5 6Copyright Alison Grimaldi 2018
Kinematics & KineticsThe Hip Adduction MomentAllison et al. also collected kinematic and kinetic data in their gait studies (Allison et al 2016b). One of the most significant findings was that people with gluteal tendinopathy use gait strategies that result in much higher than normal external hip adduction moments during stance phase of gait. Moments were 9% higher in early stance, 33% higher in mid stance and 25% higher in late stance phase.
The external hip adduction moment is the external rotational force acting on the body to force the hip into adduction when standing on one leg (Figure 13 below). This is balanced by an internal abduction moment. The internal moment is supplied by both active and passive elements such as the abductor muscles, tendons, ITB and joint capsule but the main contributor is the musculotendinous force, so the external hip adduction moment can be used as a surrogate indicator of hip abductor loads.
The finding of high external hip adduction moments in Allison et al.’s (2016) study suggests that people with lateral hip pain walk in a way that may potentially overload the abductor mechanism.
What kinematic variables are driving these high loads?Many factors can impact on the external hip adduction moment, primarily factors that influence the magnitude and direction of the ground reaction force - bodyweight, pelvic width and gait parameters such as speed, stride length and width, cadence and vertical loading rate. Those with gluteal tendinopathy were on average heavier and had a greater pelvic width but the most significant driver of variability in the external hip adduction moment was contralateral pelvic drop.
Participants with lateral hip pain demonstrated significantly greater average contralateral pelvic drop in late stance and greater contralateral trunk lean in early stance (Allison et al 2016b). While significant, average differences between groups were only in the order of 1-2 degrees, which would be difficult for the clinician to perceive. These small differences however are due to the presence of two subgroups with opposite patterns of trunk and pelvic motion during walking.
One group used a large lateral pelvic drop and a contralateral trunk lean. They can be identified primarily by the large pelvic drop, an uncompensated Trendelenburg strategy.
Internal Abduction Moment
External Adduction Moment
Figure 13: Hip moments in single leg stance

P A G E 3 0 O F 5 6 Copyright Alison Grimaldi 2018
The second group can be recognised through a substantial ipsilateral trunk lean with a small lateral pelvic drop, similar to a compensated Trendelenburg gait pattern (Figure 14).
Patients with lateral hip pain exhibit various alterations in frontal plane control of the pelvis and trunk during walking. Evaluation of the specific strategy employed by the individual will direct gait retraining in the management of gluteal tendinopathy.
Figure 14: Two gait strategies used by people with symptomatic gluteal tendinopathy
With respect to spatiotemporal variables of gait , Allison et al. (2016) also found that study participants with painful gluteal tendinopathy, on average, walked more slowly and with smaller stride length (Allison et al 2016b). Remembering that the hip external adduction moment increases with velocity and stride length, these changes are likely to represent an antalgic adaptation. The patient presenting to the clinic, particularly early in the course of this problem, may not have adapted.
A common clinical presentation is the peri-menopausal woman who has started putting on weight or retired and decided to increase their activity level. They embark on large striding, heavy impact ‘power walking‘, only to develop pain over their lateral hip. In this scenario, gait retraining can be a powerful tool in the hands of a health professional - teaching the patient to walk with more appropriate stride length and impact force can have a dramatic impact on both pain and function.
DROPPERS
Large lateral pelvic drop
Contralateral trunk lean
Uncompensated Trendelenburg (non-adaptors)
LEANERS
Small lateral pelvic drop
Ipsilateral trunk lean
Compensated Trendelenburg
(adaptors)

P A G E 3 1 O F 5 6Copyright Alison Grimaldi 2018
CHAPTER SEVENDIAGNOSING GLUTEAL TENDINOPATHY
Attend a practical workshop to develop specific clinical skills to optimise your assessment of
gluteal tendinopathy Find a course or contact us for interest
Sign up for notifications regarding new courses or resources
www.dralisongrimaldi.com
DIAGNOSTIC TESTSFADER & FADER-RFABERADD-RSingle Leg StancePalpation
CLINICAL DIAGNOSIS OF GLUTEAL TENDINOPATHY Infographic

P A G E 3 2 O F 5 6 Copyright Alison Grimaldi 2018
Diagnostic Tests
In 2013, Reiman and colleagues reviewed the literature to determine the usefulness of clinical tests for the hip, including those for lateral hip pain (Reiman et al 2013). They reported that the literature available provided evidence of only weak diagnostic properties for these tests.
As a result, our research group at the University of Queensland, Australia, embarked on a project to assess the usefulness of a battery of clinical tests to diagnose MRI-confirmed gluteal tendinopathy in patients presenting with lateral hip pain (Grimaldi et al 2017). We chose tests that had shown promise in the literature despite inadequate methodology and/or had in our experience been useful in clinical practice. Sixty-five patients complaining of pain in the trochanteric region were put through our clinical test battery and then sent for MRI. Both clinical and radiological assessors were blind to each others results.
FADER & FADER-R TestsThe Flexion Adduction External Rotation (FADER) tests are modifications of Lequesne et al.’s (2008) resisted external de-rotationtest (Lequesne et al 2008). In the original test, the examiner passively flexes the hip to 90°, moves the hip into external rotation and then resists the patient actively internally rotating the hip back to a position of neutral rotation.
Based on the pathoaetiological premise that compression and particularly with added tensile loading represents a situation of adverse loading for the gluteal tendons, we aimed to maximise the compressive forces by adding maximal adduction to the test and sustaining the hip in the FADER position to perform an isometric internal rotation with the tendons maintained in a compressed position (Figure 15).
In clinical practice many patients will complain of reproduction of lateral hip pain simply by placing them passively into the FADER position. In our assessment then, we tested the passive-only component as the FADER test and the addition of the active tensile component, isometric hip internal rotation, as the FADER-Resisted (FADER-R) test. A positive test is the reproduction of the patient’s trochanteric pain. Sometimes a patient has difficulty distinguishing between a stretch and pain. Performing the test on the unaffected hip first can provide both the tester and the patient with a good comparison for subsequent testing of the painful side.
Figure 15: Positioning for the Flexion Adduction External Rotation (FADER) Test and the FADER-Resisted (FADER-R) Test

P A G E 3 3 O F 5 6Copyright Alison Grimaldi 2018
Figure 16: Positioning for the Flexion Abduction External Rotation (FABER) Test
Figure 17: Positioning for the Adduction (ADD) and Adduction-Resisted (ADD-R) Tests
FABER TestThe FABER test was found by Fearon et al. to be useful in differentiating between those with gluteal tendinopathy and those with hip OA (Fearon et al 2013). The test will be familar to clinicians, employed for various reasons but when used in the diagnosis of gluteal tendinopathy, the test must reproduce pain in the region of the greater trochanter when the hip is placed passively in hip flexion, abduction and external rotation (Figure 16 below). Compare range of motion and response between sides.
Range restriction in hip FABER can be indicative of intra-articular pathology (Fearon et al 2013). A full joint assessment is recommended for anyone presenting with lateral hip pain. Groin pain on articular tests and range restriction increases the likelihood of an intra-articular nociceptive source or component.
ADD & ADD-R TestsThe adduction tests seek to compress the gluteal tendons beneath the ITB, now in an extended hip position. The position is as for a modified Ober’s test, however when used as a diagnostic test, the only relevant feature is the reproduction of the patient’s trochanteric pain. Length of the abductor mechanism is not useful in diagnosis due to the presence of large variability in flexibility in this population, as discussed previously. Noting length however is useful for the clinician for subgrouping patients with respect to management approach.
From a sidelying position, the patients hip is first abducted and extended to neutral and then adducted to end of range, controlling femoral rotation to maintain the ITB over the greater trochanter. This test, as for the FADER, can be performed as a two part test: passive adduction only and then isometric active abduction in the compressed end-range position of hip adduction (Figure 17 below).

P A G E 3 4 O F 5 6 Copyright Alison Grimaldi 2018
Figure 18: The Single Leg Stance Test
PalpationThe final, but arguably most important part of the diagnostic testing process is palpation of the greater trochanter. With the patient lying on their side, knees stacked on top of each other, each facet of the greater trochanter can be palpated (Figure 19). A positive test is pain and tenderness over the greater trochanter.
AL SP
Figure 19: Palpation of the Greater Trochanter. A:Anterior facet, Gluteus minimus insertion; L:Lateral Facet, Gluteus medius insertion of anterior-mid fibres; SP:Supero-posterior facet, Gluteus medius insertion of posterior fibres.
Clinical Diagnosis of Gluteal TendinopathyFor the ‘LEAP’, lateral hip pain, randomised controlled trial (Mellor et al 2016), a clinical diagnosis of gluteal tendinopathy was determined to be tenderness on palpation of the greater trochanter plus at least one other positive test from the test battery. In clinical practice it is very useful to combine a highly sensitive test (good for ruling out a diagnosis) such as palpation, with highly specific tests (good for ruling in a diagnosis) such as the single leg stance, FADER-R and ADD-R tests.
Single Leg Stance TestThe single leg stance test was performed in the manner described by Lequesne (Lequesne et al 2008) whereby the patient may have light hand support (fingertip on the wall) while sustaining a single leg stance posture for up to 30 seconds (Figure 18). Single leg stance has been assessed in many different ways in previous literature for diagnosis of lateral hip pain. Neither ability to maintain pelvic position in the frontal plane (Woodley et al 2008) nor balance on one leg (Fearon et al 2013) is useful in diagnosing gluteal tendinopathy, as poor function on such tests is common to so many other conditions.
As for the other diagnostic tests, a positive for the Single Leg Stance test is the reproduction of pain over the greater trochanter (+/- lateral thigh pain) within 30 seconds of standing on one leg. If pain is reproduced within a few seconds, the test is recorded as positive and ceases at that point. If the patient has not reported pain at the lateral hip within the 30 seconds, the test is negative. In the clinic, it is useful to record the number of seconds until pain onset. Delay in pain onset can be an early indicator of improving load tolerance in reponse to the management program.

P A G E 3 5 O F 5 6Copyright Alison Grimaldi 2018
THE FINDINGS THE IMPLICATIONSTHE TESTS
Highest sensitivityBest negative LR
High positive LRs
Highest specificityBest positive LR
30% had GT on MRI but tested -ve clinically
If a patient is NOT tender on
palpation, they are unlikely to have GT
If +ve, FADER-R or ADD-R significantly
increase the likelihood of a
diagnosis of GT
BEST TESTS FOR DIAGNOSING GLUTEAL TENDINOPATHY (GT)
A patient who develops
trochanteric pain within 30s of SLS is highly likely to
have GT
MRI results should never be used in isolation in
the diagnosis of symptomatic GT
Grimaldi A, Mellor R, Nicolson P, Hodges P, Bennell K, Vicenzino B. Utility of clinical tests to diagnose MRI-confirmed gluteal tendinopathy in patients presenting with lateral hip pain. British Journal of Sports Medicine 2017;51(6):519-524.
FADER-R: Flexion,Adduction,External Rotation with resisted isometric internal rotation. ADD-R: Adduction with resisted isometric abduction.
PALPATION
FADER-R
ADD-R
SINGLE LEG STANCE
MRI
Most accurate test
High specificity
??

P A G E 3 6 O F 5 6 Copyright Alison Grimaldi 2018
CHAPTER EIGHTMANAGEMENT
LOAD MANAGEMENTStanding Posture AdviceSitting Posture AdviceSleep Posture AdviceStretching AdviceActivity Advice
EXERCISEMovement RetrainingGraduated Strengthening From the dralisongrimaldi.com blog: Does corticosteroid injection aid or hinder our rehabilitation process?
The Evidence for Physiotherapy Intervention - Results of the LEAP Lateral Hip Pain RCT

P A G E 3 7 O F 5 6Copyright Alison Grimaldi 2018
Traditional management for lateral hip pain has revolved around anti-inflammatory treatment and stretching into hip adduction. The rationale for such an approach is poor, with a possibility of worsening symptoms secondary to the provocative compressive loading inherent in stretching.
The more contemporary model of management proposed here is a two part approach, involving:
1. Load management, aiming to minimise exposure to provocative loads and graduate activity levels appropriately and
2. A graduated exercise programme aiming to improve load tolerance via a combination of graduated slow, heavy tensile loading and motor control retraining aiming to minimise functional adduction and associated soft tissue compression at the greater trochanter.
LOAD MANAGEMENT
The quickest way to start making a positive difference to pain, and presumably to tendon health, is to start reducing tendon compression and combinations of high compressive and tensile loading. Patients need to be educated regarding postures or activities in their daily life that cause potentially provocative tendon and bursal loading for those with lateral hip pain – any position where the hip is moved out to the side relative to the knee, such as standing hanging on one hip, or where the knee is brought across the body, such as sitting with legs crossed, or some buttock stretches.
The manner in which this information is presented is critical, as depending on how you transfer this information you may either instil hypervigilence or confidence. We are of course aiming for the latter, empowering the patient to take control of their symptoms and gradually return to appropriate activity.
When we talk about compression at the lateral hip, it is important to let the patient know that compression is completely normal in this region and the tendons and bursae are good at absorbing normal levels of compression. It’s just when exposed to higher than normal levels of compression, usually over long periods of time that the tissues start to adapt to that compression by ‘sucking in more water and pumping themselves up’, consequently making them less tolerant of their normal longitudinal loading that occurs when the muscle contracts during functional activities.
While we must educate patients about the positions of compression, they shouldn’t go home believing that moving into those positions intermittently will be damaging to their tissues. It is the accumulation of high load or high volume compression/compression-tension combinations that is likely to be provocative. The overall aim is to minimise sustained, repetitive or loaded hip adduction and direct compression over the greater trochanter.
Attend a practical workshop to develop specific clinical skills
to optimise your management of
gluteal tendinopathy www.dralisongrimaldi.com

P A G E 3 8 O F 5 6 Copyright Alison Grimaldi 2018
COPYRIGHT DR ALISON GRIMALDI 2018
COPYRIGHT DR ALISON GRIMALDI 2018 COPYRIGHT DR ALISON GRIMALDI 2018
COPYRIGHT DR ALISON GRIMALDI 2018
Standing Posture Advice
Avoid standing ‘hanging on one hip, or standing with legs crossed. Also avoid letting the pelvis translate forward (this winds up the anterior aspect of the ITB and may increase compression over the anterior aspects of the gluteus medius and minimus tendons).
Stand with feet hip width apart and grow gently tall, but avoid muscle ‘gripping’. Aim to use minimal muscle effort to achieve a relaxed upright posture. If fatigued, stand with the feet slightly wider, lean your back against the wall or sit on a high chair.

P A G E 3 9 O F 5 6Copyright Alison Grimaldi 2018
COPYRIGHT DR ALISON GRIMALDI 2018
COPYRIGHT DR ALISON GRIMALDI 2018 COPYRIGHT DR ALISON GRIMALDI 2018
COPYRIGHT DR ALISON GRIMALDI 2018
Sitting Posture Advice
Sitting with the legs crossed or knees together will significantly increase the tension in the iliotibial band. Sitting with the legs up to one side, or with one foot tucked up can also create some wind up of the band from the bottom end, so it is best to avoid these postures as well.
Sit with hips, knees and feet approximately aligned (except for those who are structurally tight in the abductor mechanism). Avoid low chairs and keep the hips slightly higher than the knees or the hips more open than 90° (eg recliner chair) if possible.
Using a wedge cushion in sitting can be helpful. Sitting in low chairs can cause problems during or after sitting, or car travel. This is most likely due to increased tension in the fascial connections of the ITB into the gluteal and thoracodorsal fascia as the hip flexes above 90degrees.

P A G E 4 0 O F 5 6 Copyright Alison Grimaldi 2018
COPYRIGHT DR ALISON GRIMALDI 2018
COPYRIGHT DR ALISON GRIMALDI 2018 COPYRIGHT DR ALISON GRIMALDI 2018
COPYRIGHT DR ALISON GRIMALDI 2018
Sleep Posture Advice
Minimise time spent sleeping directly on the affected side. When the affected side is uppermost, don’t let the leg hang down across the body. Avoid flexing the hip >90°.
If you are sleeping on your side, use pillows to bring the top hip, knee and ankle to a horizontal position, or roll your whole body halfway to facing the bed, placing a pillow under the top hip and abdomen.
Lying supine has no compressive load, as long as the ankles are not crossed. A pillow under the knees often improves comfort for the hips and lower back.

P A G E 4 1 O F 5 6Copyright Alison Grimaldi 2018
COPYRIGHT DR ALISON GRIMALDI 2018
COPYRIGHT DR ALISON GRIMALDI 2018 COPYRIGHT DR ALISON GRIMALDI 2018
COPYRIGHT DR ALISON GRIMALDI 2018
Stretching Advice
Avoid any stretches that bring the knee across the body (gluteal/piriformis/buttock stretches/strong lumbar rotation stretches) or that push the hip out to the side (ITB stretches).
Activity Advice
Avoid activities that provoke pain during or after the activity. Often ceasing the most provocative activities or provocative parts of an activity will allow continuation of modified activity.
Walking/running modifications- Avoid hills and stairclimbing - Reduce speed - Reduce stride length- Reduce impact force- Reduce volume
Avoid activities involving rapid stretch-shortening cycles, such as plyometric exercise - hopping, bounding, burpees.
If involved in floor based pilates, avoid clams and sidelying exercise due to compression and friction at the greater trochanter.
Avoid rapid increases in loadingMonitor response to activityNight-time pain is a good barometer of how the hip is tolerating daytime loads. If night-time pain increases, the activities of the day or last couple of days may have been too high and should be reviewed and modified as required.

P A G E 4 2 O F 5 6 Copyright Alison Grimaldi 2018
EXERCISE
Together with load management advice, the exercise program should reduce pain and facilitate graduated return to painfree function. Impairments identified in the physical assessment are addressed - gluteal muscle atrophy and weakness, load intolerance of the musculotendinous complex and kinematic patterns that induce provocative combinations of compression and tensile load.
Isometric AbductionIsometric exercise potentially provides benefits via a number of mechanisms:
1. Analgesic response Isometric exercise has been shown to stimulate segmental and extrasegmental descending pain inhibitory pathways (Kosek & Ekholm 1995, Kosek & Lundberg 2003). Sustained low-intensity contractions (25% maximum voluntary isometric contraction) were most effective in a normal population for raising pain pressure thresholds (Hoeger Bement et al 2008). Isometric exercise has been shown to be more effective than isotonic exercise in inducing pain relief in patellar tendinopathy (Rio et al 2015).
2. Neuroplastic effect
(See Boudreau et al 2010 for review)Disturbance or imprecision of the homuncular representation of chronically painful bodyparts has been well documented and these changes are linked with pain and motor control disturbance. Exercise that requires focussed attention or skill is more effective than general exercise in inducing homuncular reorganisation (Boudreau et al 2010, Tsao et al 2010). Low load isometric activation of the transversus abdominis muscle in those with chronic low back pain was shown to change homuncular representation and muscle recruitment patterns during a functional movement task, with only two weeks of training (Tsao et al 2010). Furthermore, isometric exercise has been shown to reduce cortical inhibition
of the quadriceps in those with painful patellar tendinopathy (Rio et al 2015).
3.Local mechanotransductionAt a local level, applying load across a tendon is known to stimulate signalling within the tendon, often termed mechanotransduction (see Khan & Scott 2009 for review).
Isometrics for Gluteus Medius & Minimus
Isometrics can be performed in sidelying (affected hip uppermost), supine with a belt around the lower thighs for bilateral pain and in standing.
Key point:
Focus is on gluteus medius and minimus, so keep ITB tensioners relaxed.
Graduated Loading ProgramGraduated loading includes components of both movement patterning or motor control training and low velocity, high tensile load strengthening to optimise tendon structural health and load tolerance via re-adaptation to tensile loads and reduction of functional adduction and associated excessive compressive load combinations.

P A G E 4 3 O F 5 6Copyright Alison Grimaldi 2018
BRIDGING PROGRESSIONS
Maintain neutral spineEnsure good gluteal recruitmentMaintain pelvis level
Double Leg
Offset
Single Leg - Short Lever
Single Leg - Long Lever
Add external load
FUNCTIONAL LOADING PROGRESSIONS
Attention to frontal plane control **Ensure good gluteal recruitmentCheck technique if any pain at greater
trochanter
Double Leg
Offset
Single Leg Stance
Single Leg Squat
Step Up
Add
exte
rnal
cha
lleng
e e.
g. m
etro
nom
e pa
cing
, ext
ra lo
ad, p
ertu
rbat
ion
..

P A G E 4 4 O F 5 6 Copyright Alison Grimaldi 2018
FRONTAL PLANE LOADING
Attention to relative muscle recruitment*Trunk position alters recruitmentMonitor response to loading
Low load sidestep
Spring resisted bilateral abduction
(Upright skating)
Spring resisted bilateral abduction
(Skating in squat)
Progress resistance to hard - very hard level on Borg Scale. MUST achieve >40% MVC to
induce strength change
DYNAMIC PROGRESSIONS
Maintain attention to frontal plane controlIntroduce graduallyMonitor response to loading
Landing control
Direction change
Progress to tasks specific to the patients recreational,
sporting or occupational requirements

P A G E 4 5 O F 5 6Copyright Alison Grimaldi 2018
When physiotherapy treatment for tendinopathy fails, have you ever thought ‘Where did I go wrong’? Assuming you have applied contemporary evidence informed protocols that incorporate load management and appropriate exercise therapy (e.g. avoiding compressive loading combinations for insertional tendinopathies), there are a number of factors that may influence your success, including patient beliefs and compliance, systemic illness and psychosocial issues. Have you ever considered though that prior medical treatment may have had you fighting an uphill battle from the start?
If a patient with symptomatic tendinopathy presents initially to a medical physician, the first line of treatment is generally a corticosteroid injection (CSI), due to their known effects on early pain reduction. Hopefully the patient is then also sent off to the physiotherapist or this may be delayed until the problem is demonstrated to be recurrent. A second or third CSI may then be provided to help the patient through the impending rehabilitation process. The physician is practising within the current evidence base and is trying to do the best by patient and the therapist, because surely a patient whose pain has been lessened with CSI will be more easily rehabilitated.
Right?? Hmmm, maybe not…
Effects of exercise and CSI on tendon structure
Let’s consider the effects of both exercise and CSI on the intrinsic structure and function of a tendon. Khan and Scott (2009) describe in detail the process by which exercise, via mechanical shearing of tenocytes between collagen fibrils, initiates a biochemical cascade that forms new collagen and matrix proteins, a process referred to as ‘mechanotransduction’. Kongsgaard and colleagues demonstrated both clinical improvements and positive structural changes within patellar tendons in response to heavy, slow resistance exercise (Kongsgaard et al. 2010). While rehabilitative exercise appears to have a positive effect on tendon structure, the same cannot be said of the effect of CSI.
The conclusions of a systematic review of the effects of local glucocorticoid on tendon (CSI) were as follows: ‘Overall it is clear that the local administration of glucocorticoid has significant negative effects on tendon cells invitro, including reduced cell viability, cell proliferation and collagen synthesis. There is increased collagen disorganisation and necrosis as shown by invivo studies. The mechanical properties of tendon are also significantly reduced. This review supports the emerging clinical evidence that shows significant long-term harms to tendon tissue and cells associated with glucocorticoid injections.’ (Dean et al. 2014)
THOUGHTS ON CORTISONE INJECTIONS FROM THE DRALISONGRIMALDI.COM BLOG
Tendinopathy - Does corticosteroid injection aid or hinder our
rehabilitation process?Posted 2017

P A G E 4 6 O F 5 6 Copyright Alison Grimaldi 2018
Coombes, Bissett and Vicenzino (2015) have found through their high-quality trials on lateral elbow tendinopathy, that while CSI engenders short-term pain relief, longer term recovery is delayed and outcomes reduced compared to a wait-and-see approach or physical therapy management. Perhaps even more relevant for our discussion here is the fact that the application of this same physical therapy intervention to participants who were first given a single CSI, did not have the same positive benefit. The physical therapy intervention did not manage to overcome the delay in recovery and recurrence observed after CSI. ‘For these reasons’, these researchers ‘do not advocate corticosteroid injection as a first-line intervention for lateral elbow tendinopathy’.
For lateral hip pain, a treatment review highlighted that in those surgical studies that reported prior treatment, patients that failed conservative management and progressed to surgery had all received at least one CSI, mostly 2-5 and some more than 20 injections (Lustenberger et al. 2011). Were the injections provided because physiotherapy interventions failed or did physiotherapy intervention fail because patients were not referred for physiotherapy until after CSI, and the CSI hampered the ability of mechanical loading to induce positive change within the tendon and improvements in pain and load tolerance? Too simplistic? … yes, probably, pain and the effect of any intervention is complicated, as is the relationship between pain and tendon structure. While the presence of tendon pathology is commonly noted in painfree individuals, structural change within a tendon is a strong risk factor for pain and links between tendon mechanical properties and pain have been established ( (Kongsgaard et al. 2010, Lee et al. 2017)
From a clinical perspective, I have noted that of the hundreds of patients with gluteal tendinopathy treated within our clinic, there appears to be a pattern of diminishing returns from a load
management and exercise therapy approach, apparently correlating with the number of CSIs a patient has undergone prior to treatment – the more injections, the more difficulty in achieving early and optimal outcomes (in patients who have no other known systemic or psychological drivers). There may possibly be pre-conceived bias in my observations; much further research is required to establish the interaction between mechanical and pharmaceutical interventions. The type of medication – long or short acting glucocorticoid and method of injection – intra vs extratendinous and blind vs ultrasound guided may impact on these effects. For now, despite some early effects on pain, considering the known potential negative effects of CSI on tendon health and longer term rehabilitative outcomes for certain tendons, Coombes et al’s stance on avoiding CSI as a first line intervention may be wisely adopted as a general principle in the management of tendinopathy, particularly in the case of chronic, degenerative tendinopathy.
Our challenge as physiotherapists
Our challenge as physiotherapists is to provide optimal, evidence informed management that delivers early change in pain and function, reducing the need for that early CSI.
We must provide the medical profession with evidence that we can provide good early outcomes, without CSI. More high quality randomised controlled trials are required, but within your own multidisciplinary network you may be able to convince your referring physicians to give physiotherapy a try first with CSI as a backup, and see if you notice differences in your own outcomes. END BLOG
Effectiveness of physiotherapy intervention post CSI
P A G E 4 6 O F 5 6 Copyright Alison Grimaldi 2018

P A G E 4 7 O F 5 6Copyright Alison Grimaldi 2018
The outcomes of the LEAP (Lateral Hip Pain) randomised clinical trial have recently been published in the British Medical Journal (BMJ). The study contributes high quality evidence to demonstrate that an exercise and education approach should be considered the first-line treatment for painful gluteal tendinopathy.
The study was a multicentre trial, run through the University of Queensland and the University of Melbourne, with Professor Bill Vicenzino (UQ) as the Chief Investigator. Fourteen clinics across Brisbane and Melbourne were involved in the
delivery of the physiotherapy intervention. All treating physiotherapists attended a training workshop and received detailed information on the treatment approach, prescription, performance and progression of the exercise program. The education and exercise program tested was that outlined on pages 37-44. Further detailed information on the trial is available in the protocol paper (Mellor et al 2016) and the recent outcomes paper (Mellor et al 2018) - ensure you pick up the supplementary file from BMJ. Both papers are Open Access, so no payment is required to access these key papers.
THE EVIDENCE FOR PHYSIOTHERAPY INTERVENTION FOR GLUTEAL TENDINOPATHY
The LEAP Randomised Clinical Trial
Exercise & Education vs CSI vs Wait & See
Phone Screen n=1691
Physical Screen n=421
MRI/XRay n=248
Randomisation n=204
W&S n=69 CSI n=66 EDX n=69
Figure 20: Participant flow through trial. W&S: Wait and See; EDX: Education and exercise; CSI:Corticosteroid Injection.

P A G E 4 8 O F 5 6 Copyright Alison Grimaldi 2018
EducationDetailed education was provided, regarding the condition and advice on load management as outlined on pages 38-41. A DVD was supplied that contained an education video and videos of all exercises in the program.
ExerciseA home exercise program and supervised exercise on an individual (1:1) basis was provided across 14 sessions in 8 weeks - 1 session/week in the first 2 weeks and then 2 sessions/week for the following 6 weeks.
EDX CSI W&S
INTERVENTIONS - What did each intervention involve?
Single InjectionA single corticosteroid injection was provided under ultrasound guidance into the trochanteric bursa, as is common practice for the management of lateral hip pain.
Those in the CSI group were also provided with a general advice brochure, without the specific detail of the load management advice provided to the EDX group.
Wait & SeeThose in the wait and see group were used as the control group, to assess as much as possible , the natural history of the condition when no active treatment is supplied.
This group was provided with the same general advice brochure as that provided to the CSI group, without the specific detail of the load management advice provided to the EDX group.

P A G E 4 9 O F 5 6Copyright Alison Grimaldi 2018
OUTCOMESTwo primary outcomes and timepoints for analysis were nominated prospectively at the time of trial registration. Patient rated outcome measures were collected at 4, 8, 12, 26 and 52 weeks, with primary analysis of the 8 and 52 week timepoints. The two primary outcome measures were the Global Rating of Change score (GROC) and Pain Severity in the last week, on an 11 point numeric rating scale.
Primary Outcome Measures
GLOBAL RATING OF CHANGE Very much better
Much better
Moderately better
Somewhat better
Slightly better
Same
Slightly worse
Somewhat worse
Moderately worse
Much worse
Very much worse
PAIN SEVERITY 10 Worst Pain Imaginable
9
8
7
6
5
4
3
2
1
0 No Pain
SUCCESS
NOSUCCESS
EDX W&SCSI
EDX and CSI provided more pain relief than W&S
EDX provided more pain relief than CSIApproximately
80% success in EDX group 20% more success than CSI50% more success than W&S
EDX W&SCSI
4.8 4.8 4.9
1.52.7
3.8
Between-group comparisons at 8 weeks
Figure 21: Primary Outcome Measures and 8 week outcomes for the LEAP, Lateral Hip Pain Randomised Cinical Trial. EDX: Education and exercise; CSI:Corticosteroid Injection; W&S: Wait and See.

P A G E 5 0 O F 5 6 Copyright Alison Grimaldi 2018
EDX W&SCSI
EDX and CSI groups lower pain levels than W&S
Approximately:
EDX 80% success EDX greater success than CSI (58%) EDX greater success than W&S (52%)CSI no significant benefit over W&S
EDX W&SCSI
4.8 4.8 4.9
2.1 2.33.2
% Success (GROC) Pain Severity (0-10 worst)
Between-group comparisons at 52 weeks
Secondary Outcome MeasuresMany secondary outcome measures were collected and although they cannot be used as strong indicators of effect, they are useful for understanding possible mechanisms. Although there was no significant difference in pain intensity between the EDX and CSI groups at 52 weeks, the secondary measures showed significantly reduced Pain Frequency (% of time pain was present over the previous week) for EDX participants at both 8 and 52 weeks. In comparison to both the CSI and W&S groups, the EDX group also reported greater improvements in Quality of Life (EQ-5D) at both 8 and 52 weeks. This suggests that the GROC is more reflective of the overall effect on Quality of Life than a unidimensional pain severity score. See the paper for a full report of all measures (Mellor et al 2018).
CONCLUSION
While there remain many unanswered questions, over the last decade much high quality research has provided important insights into impairments associated with gluteal tendinopathy and the most useful diagnostic tests and treatments. Further research is warranted to clarify what factors may moderate the effects of intervention and provide guidance as to what intervention or level of intervention may be effective for the individual standing before you in your clinic. For now, the evidence suggests that best practice involves assessing and addressing an individual’s impairments within a biopsychosocial framework and with a clear knowledge of local mechanisms.
P A G E 5 0 O F 5 6 Copyright Alison Grimaldi 2018
Figure 22: 52 week outcomes for the LEAP, Lateral Hip Pain Randomised Cinical Trial. EDX: Education and exercise; CSI:Corticosteroid Injection; W&S: Wait and See.

P A G E 5 1 O F 5 6Copyright Alison Grimaldi 2018
REFERENCE LISTAlbers S, Zwerver J, Van den Akker-Scheek I. Incidence and prevalence of lower extremity tendinopathy in the general population. British Journal of Sports Medicine. 2014;48(Suppl 2):A5.
Allison K, Salomoni SE, Bennell KL, Wrigley TV, Hug F, Vicenzino B, Grimaldi A, Hodges PW. Hip abductor muscle activity during walking in individuals with gluteal tendinopathy. Scandinavian Journal of Medicine & Science in Sports. 2018;28(2):686-695.
Allison K, Vicenzino B, Wrigley T, Grimaldi A, Hodges P, Bennell K. Hip abductor muscle weakness in individuals with gluteal tendinopathy. Medicine and Science in Sports and Exercise 2016a; 48(3):346–352.
Allison K, Wrigley T, Vicenzino B, Bennell K, Grimaldi A, Hodges P. Kinematics and kinetics during walking in individuals with gluteal tendinopathy. Clinical Biomechanics 2016b; 32:56–63.
Allison K, Bennell K, Grimaldi A, Vicenzino B, Wrigley T, Hodges P. Single leg stance control in individuals with symptomatic gluteal tendinopathy. Gait & Posture 2016c; 49:108–113.
Bey MJ, Song HK, Wehrli FW, et al. Intratendinous strain fields of the intact supraspinatus tendon: the effect of glenohumeral joint position and tendon region. J of Orthopaedic Research 2002;20(4):869–74.
Bird P, Oakley S, Shnier R, Kirkham B. Prospective evaluation of magnetic resonance imaging and physical examination findings in patients with greater trochanteric pain syndrome. Arthritis and Rheumatism 2001;44(9):2138-2145.
Birnbaum K, Siebert CH, Pandorf T, Schopphoff E, Prescher A, Niethard FU. Anatomical and biomechanical investigations of the iliotibial tract. Surgical and Radiological Anatomy 2004;26:433-446.
Birnbaum K, Prescher A, Niethard FU. Hip centralizing forces of the iliotibial tract within various femoral neck angles. Journal of Pediatric Orthopaedics Part B. 2010;19(2):140–9.
Boudreau S, Farina D, Falla D. The role of motor learning and neuroplasticity in designing rehabilitation approaches for musculoskeletal pain disorders. Manual Therapy 2010;15(5):410-4.
Collee G, Bijkmans BAC, Vandenbroucke JP, Rozing PM. A clinical epidemiological study in low back pain. Description of two clinical syndromes. British Journal of Rheumatology 1990;29:354-357.
Connell D, Bass C, Sykes C, Young D, Edwards E. Sonographic evaluation of gluteus medius and minimus tendinopathy. European Radiology 2003; 13:1339-1347.
Cook JL & Purdam C. Is compressive load a factor in the development of tendinopathy? British Journal of Sports Medicine 2012;46:163-168.

P A G E 5 2 O F 5 6 Copyright Alison Grimaldi 2018
Coombes BK, Bisset L, Vicenzino B. Management of Lateral Elbow Tendinopathy: One Size Does Not Fit All. Journal of Orthopaedic & Sports Physical Therapy 2015;45(11):938-949.
Dean BJS, Lostis E, Oakley T et al. The risks and benefits of glucocorticoid treatment for tendinopathy: A systematic review of the effects of local glucocorticoid on tendon. Seminars in Arthritis and Rheumatism 2014; 43:570–576.
Dwek J, Pfirrmann C, Stanley A, et al. MR imaging of the hip abductors: normal anatomy and commonly encountered pathology at the greater trochanter. Magnetic Resonance Imaging Clinics of North America 2005;13:691–704.
Farr D, Selesnick H, Janecki C, Cordas D. Arthroscopic bursectomy with concomitant iliotibial band release for the treatment of recalcitrant trochanteric bursitis. Arthroscopy: The Journal of Arthroscopic and Related Surgery 2007:23(8):905.e1-905.e5.
Fearon AM, Cook JL, Scarvell JM, et al. Greater trochanteric pain syndrome negatively affects work, physical activity and quality of life: a case control study. Journal of Arthroplasty 2014a;29(2):383–6.
Fearon AM, Scarvell JM, Cook JL, Smith PN. Does ultrasound correlate with surgical or histological findings in greater trochanteric pain syndrome? A pilot study. Clinical Orthopaedica and Related Research 2010;468:1838-44.
Fearon AM, Stephens S, Cook JL et al. The relationship of femoral neck shaft angle and adiposity to greater trochanteric pain syndrome in women. A case control morphology and anthropometric study. British Journal of Sports Medicine 2012;46(12):888-92.
Fearon AM, Scarvell JM, Neeman T, Cook JL, Cormick W, Smith PN. Greater trochanteric pain syndrome: defining the clinical syndrome. British Journal of Sports Medicine 2013;47:649-653.
Fearon A, Twin J, Dahlstrom J et al. Increased substance P expression in the trochanteric bursa of patients with greater trochanteric pain syndrome. Rheumatology International 2014b;34:1441–1448.
Fields KB. Running injuries—changing trends and demographics. Current Sports Medicine Reports. 2011;10(5):299–303.
Gaida JE, Alfredson H, Kiss ZS et al. Asymptomatic Achilles tendon pathology is associated with a central fat distribution in men and a peripheral fat distribution in women: a cross sectional study of 298 individuals. BMC Musculoskeletal Disorders 2010;11:41.
Ganderton C, Semciw A, Cook J, Pizzari T. Does menopausal hormone therapy, exercise or a combination of both, improve pain and function in post-menopausal women with greater trochanteric pain syndrome? A randomised controlled trial. BMC Women’s Health 2016; 16:32.
Ganderton C, Pizzari T, Harle T, Cook J, Semciw A. A comparison of gluteus medius, gluteus minimus and tensor facia latae muscle activation during gait in post-menopausal women with and without greater trochanteric pain syndrome. Journal of Electromyography and Kinesiology 2017;33:39-47.
Grimaldi A. Assessing lateral stability of the hip and pelvis. Manual Therapy 2011;16: 26-32.

P A G E 5 3 O F 5 6Copyright Alison Grimaldi 2018
Grimaldi A, Fearon A. Gluteal Tendinopathy: Integrating Pathomechanics and Clinical Features in Its Management. Journal of Orthopaedics and Sports Physical Therapy 2015;45(11):910-922.
Grimaldi A, Mellor R, Hodges P, Bennell K, Wajswelner H, Vicenzino B. Gluteal Tendinopathy: A Review of Mechanisms, Assessment and Management. Sports Medicine 2015;45:1107-1119.
Grimaldi A, Mellor R, Nicolson P, Hodges P, Bennell K, Vicenzino B. Utility of clinical tests to diagnose MRI-confirmed gluteal tendinopathy in patients presenting with lateral hip pain. British Journal of Sports Medicine 2017;51(6):519-524.
Hoeger Bement MK, Dicapo J, Rasiarmos R, Hunter SK. Dose response of isometric contrac-tions on pain perception in healthy adults. Medicine & Science in Sports and Exercise 2008;40:1880-1889.
Howell GED, Biggs RE, Bourne RB. Prevalence of abductor mechanism tears of the hips in patients with osteoarthritis. The Journal of Arthroplasty 2001; 16:121-123.
Huang B, Campos J, Peschka P et al. Injury of the gluteal aponeurotic fascia and proximal iliotibial band: Anatomy, pathologic conditions, and MR imaging. Radiographics 2013;33(5):1437-52.
Khan KM & Scott A. Mechanotherapy: how physical therapists’ prescription of exercise promotes tissue repair. British Journal of Sports Medicine 2009; 43:247-252.
Kingzett-Taylor A, Tirman P, Feller J, McGann W, Prieto V, Wischer T, Cameron J, Cvitanic O, Genant H. Tendinosis and tears of gluteus medius and minimus muscles as a cause of hip pain: MR imaging findings. American Journal of Roentgenology 1999; 173:1123-1126.
Klingler W, Velders M, Hoppe K, Pedro M, Schleip R. Clinical relevance of fascial tissue and dysfunctions. Current Pain and Headache Reports 2014;18(8):439.
Kong A, van der Vliet A, Zadow S. MRI and US of gluteal tendinopathy in greater trochanteric pain syndrome. European Radiology 2007;17:1772-1783.
Kongsgaard M, Qvortrup K, Larsen J et al. Fibril morphology and tendon mechanical properties in patellar tendinopathy - effects of heavy slow resistance training. The American Journal of Sports Medicine 2010; 38 (4): 749-56.
Kosek E, Ekholm J. Modulation of pressure pain thresholds during and following isometric contraction. Pain 1995;61:481-486.
Kosek E, Lundberg L. Segmental and plurisegmental modulation of pressure pain thresholds during static muscle contractions in healthy individuals. European Journal of Pain. 2003;7:251-258.
Kumagai M, Shiba N, Higuchi F, Nishimura H, Inoue A. Functional evaluation of hip abductor muscles with use of magnetic resonance imaging. Journal of Orthopaedic Research 1997;15:888-893.

P A G E 5 4 O F 5 6 Copyright Alison Grimaldi 2018
Kummer, B. Is the Pauwels theory of hip biomechanics still valid? A critical analysis, based on modern methods. Annals of Anatomy 1993;175:203-210.
Lee K, Rosas H, Phancao J. Snapping Hip: Imaging and Treatment. Seminars in Musculoskeletal Radiology 2013;17:286–294.
Lee WC, Zhang ZJ, Masci L et al. Alterations in mechanical properties of the patellar tendon is associated with pain in athletes with patellar tendinopathy. European Journal of Applied Physiology 2017;117:1039–1045.
Lepers R, Knechtle B, Stapley PJ. Trends in triathlon performance: effects of sex and age. Sports Medicine. 2013;43(9):851–63.
Lequesne M. From ‘‘periarthritis’’ to hip ‘‘rotator cuff’’ tears: trochanteric tendinobursitis. Joint Bone Spine 2006;73(4):344–8.
Lequesne M, Mathieu P, Vuillemin-Bodaghi V, et al. Gluteal tendinopathy in refractory greater trochanter pain syndrome: diagnostic value of two clinical tests. Arthritis & Rheumatology 2008;59:241–6.
Long S, Surrey D, Nazarian L. Sonography of greater trochanteric pain syndrome and the rarity of primary bursitis. American Journal of Roentgenology 2013;201(5):1083-6.
Lustenberger DP, Ng VY, Best TM, et al. Efficacy of treatment of trochanteric bursitis: a systematic review. Clinical Journal of Sports Medicine 2011;21(5):447–53.
Mellor R, Bennel K, Grimaldi A, Nicolson P, Kasza J, Hodges P, Wajswelner H, Vicenzino B. Education plus exercise versus corticosteroid injection use versus a wait and see approach on global outcome and pain from gluteal tendinopathy: prospective, single blinded, randomised clinical trial. British Medical Journal 2018; 361: k1662 (Published 02 May 2018).
Mellor R, Grimaldi A, Wajswelner H, Hodges P, Abbott JH, Bennell K, Vicenzino B. Exercise and load modification versus corticosteroid injection versus ‘wait and see’ for persistent gluteus medius/minimus tendinopathy (the LEAP trial): a protocol for a randomised clinical trial. BMC Musculoskelet Disord. 2016; 17: 196.
Moulton KM, Aly AR, Rajasekaran S, Shepel M, Obaid H. Acetabular anteversion is associated with gluteal tendinopathy at MRI. Skeletal Radiol. 2015 Jan;44(1):47-54.
Pfirrmann C, Chung C, Theumann N, Trudell D, Resnick D. Greater trochanter of the hip: attachment of the abductor mechanism and a complex of three bursae—MR imaging and MR bursography in cadavers and MR imaging in asymptomatic volunteers. Radiology 2001;221(2):469-77.
Pfirrmann C, Notzli H, Dora C, Hodler J, Zanetti M. Abductor tendons and muscles assessed at MR imaging after total hip arthroplasty in asymptomatic and symptomatic patients. Radiology 2005; 235:969-976.
Reiman MP, Goode AP, Hegedus EJ, et al. Diagnostic accuracy of clinical tests of the hip: a systematic review with meta-analysis. British Journal of Sports Medicine 2013;47:893–902.

P A G E 5 5 O F 5 6Copyright Alison Grimaldi 2018
Rio E, Kidgell D, Purdam C, et al. Isometric exercise induces analgesia and reduces inhibition in patellar tendinopathy. Br J Sports Med. 2015; 0:1–8; doi:10.1136/bjsports-2014-094386.
Robertson WJ, Gardner MJ, Barker JU, Boraiah S, Lorich DG, Kelly BT. Anatomy and dimensions of the gluteus medius insertion. Arthroscopy: The Journal of Arthroscopic and Related Surgery 2008; 24(2):130-136.
Scott A, Zwerver J, Grewal N et al. Lipids, adiposity and tendinopathy: Is there a mechanistic link? Critical review. British Journal of Sports Medicine 2015;49:984–988.
Segal NA, Felson DT, Torner JC, Zhu Y, Curtis JR, Niu J, Nevitt MC. Greater trochanteric pain syndrome: Epidemiology and associated factors. Archives of Physical Medicine and Rehabilitation 2007;88:988-992.
Silva F, Adams T, Feinstein J, Arroyo RA. Trochanteric bursitis: refuting the myth of inflammation. Journal of Clinical Rheumatology 2008;14:82-86.
Strauss EJ, Nho SJ, Kelly BT. Greater trochanteric pain syndrome. Sports Med Arthrosc. 2010;18(2):113–9.
Szotek S, Dawidowicz J, Eyden B. Morphological features of fascia lata in relation to fascia diseases. Ultrastructural Pathology 2016;40(6):297–310.
Sutter R, Kalberer F, Binkert CA, Graf N, Pfirrmann CWA, Gutzeit A. Abductor tendon tears are associated with hypertrophy of the tensor fasciae latae muscle. Skeletal Radiology 2013;42(5):627-33. Thaunat M, Noel E, Nove´-Josserand L et al. Endoscopic Management of Gluteus Medius Tendon Tears. Sports Medicine and Arthroscopy Review 2016;24:11–18.
Tortolani PJ, Carbone JJ, Quartararo LG. Greater trochanteric pain syndrome in patients referred to orthopaedic spine specialists. The Spine Journal 2002;2:251-254.
Tsao H, Galea M, Hodges P. Driving plasticity in the motor cortex in recurrent low back pain. European Journal of Pain 2010;14(8):832-9.
Viradia NK, Berger AA, Dahners LE. Relationship between width of greater trochanters and width of iliac wings in trochanteric bursitis. American Journal of Orthopedics (Belle Mead NJ) 2011;40(9):E159–62.
Vleeming A, Mooney V, Snijders C, Doorman T, Stoeckart R. 1997. Movement, stability and low back pain. The essential role of the pelvis. New York: Churchill Livingstone.
Walsh M, Walton J, Walsh N. Surgical repair of the gluteal tendons: A report of 72 cases. The Journal of Arthroplasty 2011;26(8):1514-1519.
Woodley SJ, Nicholson HD, Livingstone V, et al. Lateral hip pain: findings from magnetic resonance imaging and clinical examination. Journal of Orthopaedic and Sports Physical Therapy 2008;38(6):313–28.
Wright VJ. Masterful care of the aging triathlete. Sports Medicine and Arthroscopy. 2012;20(4):231–6.

With over 25 years of clinical experience, Alison is Principal Physiotherapist at Physiotec Physiotherapy in Brisbane, Australia and an Adjunct Research Fellow in the School of Health & Rehabilitation Sciences, University of Queensland. Alison has a special interest in movement, muscle dysfunction and optimising musculoskeletal loads and is a committed lifelong learner.
Alison completed a Bachelor of Physiotherapy at the University of Queensland in 1990, a Masters of Sports Physiotherapy in 1997, and her Doctorate in Philosophy in the Field of Physiotherapy (PhD) in 2008. Her PhD studies were concerned with improving our understanding of hip muscle function and the relationship with hip joint pathology and weightbearing stimulus. Alison continues to be passionate about extending our understanding of why we develop problems around the hip and pelvis, and what we can do to most effectively prevent and manage these problems. She has ongoing involvement in research studies investigating lateral hip pain, proximal hamstring tendinopathy, groin pain and function of the deep hip flexors and rotators.
It is one of Alison’s core beliefs that research should be relevant to clinical practice and helping the patients we treat every day, and that physiotherapists in the community should have access to this valuable information to allow them to transfer this knowledge into clinical practice as quickly as possible. To this end, Alison continues to publish, present and provide practical workshops for other health professionals. Alison has published many peer-reviewed papers in scientific journals, has contributed detailed information freely accessible via podcasts by PhysioEdge (itunes) and the British Journal of Sports Medicine (SoundCloud), and has recently contributed to 3 leading physiotherapy and sports medicine text books. She has presented her research and clinical teachings in Australia, New Zealand, England, Ireland, Scotland, Wales, Singapore, HongKong, the Netherlands, France, Belgium, the Unites States of America, Canada and the United Arab Emirates.
dralisongrimaldi.com