Challenges in Capacity in SA for diagnosing DR-TB/media/Files... · Challenges in TB control •...
23
National Tuberculosis Reference Laboratory Challenges in Capacity in SA for diagnosing DR-TB March 2010 Gerrit Coetzee
-
Upload
truonghanh -
Category
Documents
-
view
213 -
download
0
Transcript of Challenges in Capacity in SA for diagnosing DR-TB/media/Files... · Challenges in TB control •...
National Tuberculosis Reference Laboratory
Challenges in Capacity in SA for diagnosing DR-TB
March 2010
Gerrit Coetzee
Rapid response to XDR-TBWHO Global Task Force on XDR-TB, October
2006• Accelerate access to rapid tests for rifampicin resistance• Adherence to WHO Drug Resistance Guidelines;
improve programme management; access to MDR-TB drugs including DOT; HIV+ cases adequately treated and started on ART
• Implementation of IC measures, especially among HIV+• Strengthen laboratory capacity to diagnose, manage and
survey DR; rapid survey to determine size of XDR-TB problem
• Initiate information sharing strategies that promote prevention, treatment and control of XDR-TB

Challenges in TB control• Health systems weaknesses one of the greatest challenges in TB control
• Laboratory services one of the weakest links
• Lack of diagnostic capacity a crucial barrier preventing an effective response to the challenges of HIV-associated TB and drug-resistant TB
• 500,000 new MDR-TB cases estimated annually
• 10% of MDR-TB cases XDR-TB and present in more than 50 countries
• SA: 4th highest total number MDR reported 2007
• 5% of MDR-TB cases projected to be treated in 2009 and 3% only under GLC standards
Why laboratory performance is unsatisfactory
• Inadequate human resources• Biosafety concerns• Lack of recognition of laboratory importance in TB
control • Weak communication between NTP and laboratory
services• Insufficient financial resources• Problems of laboratory availability and accessibility • Delay in technology transfer to resource-limited
settings

TB CULTURES PER PROVINCE PER YEAR (excl KZN)PROVINCE 2004 2005 2006 2007 2008 2009 Grand TotalEC 35,132 47,866 69,229 96,496 140,559 154,600 543,882FS 18,240 22,434 29,288 37,072 36,629 31,569 175,232GP 79,481 124,193 155,780 172,968 223,785 225,889 982,096LP 4,128 5,315 8,407 13,504 16,884 19,550 67,788MP 13,246 13,813 15,616 21,047 34,880 46,237 144,839NW 14,312 17,864 24,036 36,134 44,388 41,842 178,576NC 20,016 25,062 31,949 35,133 41,362 44,250 197,772WS 115,300 135,106 158,584 177,710 211,902 230,228 1,028,830Total 299,855 391,653 492,889 590,064 750,389 794,165 3,319,015
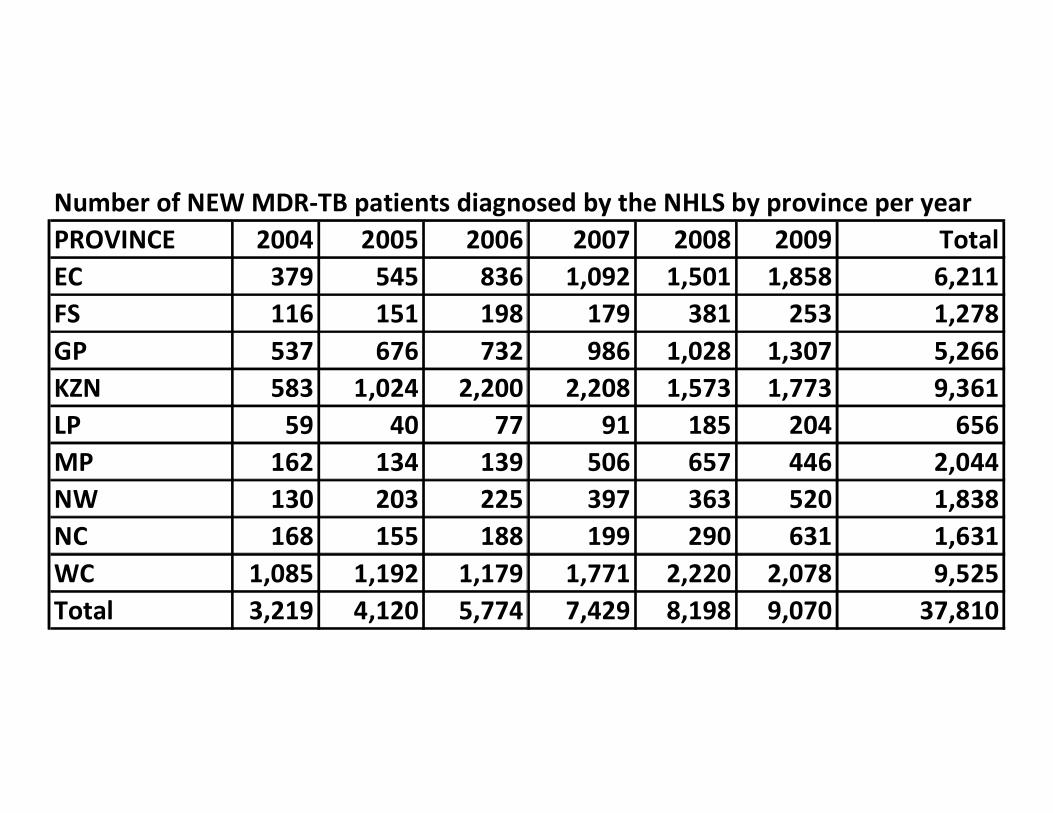
Number of NEW MDR-TB patients diagnosed by the NHLS by province per yearPROVINCE 2004 2005 2006 2007 2008 2009 TotalEC 379 545 836 1,092 1,501 1,858 6,211FS 116 151 198 179 381 253 1,278GP 537 676 732 986 1,028 1,307 5,266KZN 583 1,024 2,200 2,208 1,573 1,773 9,361LP 59 40 77 91 185 204 656MP 162 134 139 506 657 446 2,044NW 130 203 225 397 363 520 1,838NC 168 155 188 199 290 631 1,631WC 1,085 1,192 1,179 1,771 2,220 2,078 9,525Total 3,219 4,120 5,774 7,429 8,198 9,070 37,810

Number of NEW XDR-TB patients diagnosed by the NHLS by province per year
PROVINCE 2004 2005 2006 2007 2008 2009 Total
EC 3 18 61 108 175 123 488
FS 1 6 3 4 3 3 20
GP 5 14 19 38 30 65 171
KZN 59 227 336 241 181 254 1,298
LP 2 5 2 2 6 17
MP 12 14 18 44
NW 1 5 9 4 4 13 36
NC 4 10 3 7 19 40 83
WC 12 16 28 42 60 72 230
Total 85 298 464 458 488 594 2,387



4,411,529 bp ≈ 4000 genes
Genome of M. tuberculosis H37RvGenome of M. tuberculosis H37Rv

Line probe technologies endorsed by WHO in 2008 for the rapid detection of MDR-TB
rpoB
katG
CC AC TUB
rpoB
rpoB
rp
oB
rpoB
rp
oB
rpoB
rp
oB
rpoB
rp
oB
rpoB
rp
oB
rpoB
rp
oB W
T1W
T2W
T3W
T4W
T5W
T6W
T7W
T8M
UT1
MU
T2A
MU
T2B
MU
T3
katG
katG
katG
ka
tG W
TM
UT1
MU
T2
inhA
inhA
in
hA
inhA
in
hA
inhA
in
hA W
T1W
T2M
UT1
MU
T2M
UT3
AM
UT3
B
inhA
TUB
katG
WT
katG
MU
T
rpoB
MU
T
inhA
WT
inhA
MUT
++ + +- --+
+
--+ -+
+- +- - +++
--
+- - - +-
- +- +
RMP
++ +
+++
++++
sens
itive
resi
stan
t
INH
sens
itive
resi
stan
t#
1
2
3
4
5
+
Detects resistance to both rifampicin and isoniazid Licenced for use on AFB smear positive processed sputum specimens and positive cultures

South African LPA roll out
DNA•STRIP® Technology HAIN LIFESCIENCE

NHLS LPA Roll out
• LPA endorsed by WHO, will be part of National TB Control Programme
• Roll out over 2 years• ~20 additional regional sites• Now have LPA for 2nd line anti-TB drugs• Other systems eg gene Xpert also developing
LPA Roll out: Objectives• Provide rapid diagnosis of MDR-TB • Timeously effect appropriate treatment • Prevent further development of resistance to anti-
tuberculosis drugs• Prevent further transmission of tuberculosis• Cut down on the cost of diagnosing TB by screening
drug-susceptible TB out of conventional drug susceptibility testing (DST) using the LPA
• Decrease the cost of treating TB by reducing unnecessary transmission through early diagnosis, as well as preventing development of drug-resistant TB which is more expensive to treat

Project goals
• roll the assay out to additional 20 laboratories by December 2010
• implement the assay with as little disruption to the normal flow as possible
• standardize the performance, reading, interpretation and reporting of results across laboratories

Project Approach• Phase I: Secure laboratory space (renovate
existing labs or erect mobile labs)• Phase II: Order and install equipment• Phase III:Recruit staff (technicians/medical
scientists)• Phase IV: Train staff• Phase V: Implement the assay• Phase VI: Review success of initial roll out and
start the procedure for the next cycle

Laboratory name Status of laboratory renovations / mobile lab construction
Dr George Mukhari Completed 18August 2009
Edendale Completed 7 August 2009
PE Completed 5 August 2009
Mafikeng Completed 14 September 2009
Baragwanath PCR labs completed; DNA extraction room renovations to go on tender
Ngwelezane (M- PROJECTS) Completed – to sign off
Helen Joseph Awaiting Hospital approval
Paarl Awaiting Hospital approval
Worcester Ready for tender, on hold pending DOH
Welkom Contractor busy, estimated to finish by end of October
Madadeni (M-PROJECTS) Ground work quote finalized, Park Home Lab ready for delivery
Ermelo No. 1 (M-PROJECTS) Ground work quote finalized, Park Home Lab ready for delivery
Ermelo No. 2 (M-PROJECTS) Park Home Lab ready for delivery, to be adapted as a culture lab
Polokwane (PARK HOMES) Awaiting ground work quote, busy manufacturing Park Home Lab
East London Awaiting Hospital approval for Park home
Tshepong (PARK HOMES) Awaiting ground work quote, busy manufacturing Park Home Lab
George Awaiting Hospital approval
Letaba Awaiting Hospital approval. Business manager is following up
Nelspruit Space for mobile lab verbally allocated, though no formal letter. Concern is that space is about 200m from the lab & next to a crèche. Space to be renegotiated.
Rustenburg Two rooms at Rustenburg lab previously ear marked for viral loads, could be used as an alternative. Approval for placing a mobile lab will first be requested.
Kokstad Space for mobile lab identified. Awaiting hospital approval
LPA inter-laboratory comparison
• 10 DNA samples• Include fully susceptible, INH/Rifampicin
mono-resistance, MDR, MOTTS• Excellent performance• 4x pa.


Development of an Algorithm• Simplify current algorithms• Capacity of laboratories to inactivate sputum to
PCR friendly state• Cost to NTP should not increase• Laboratory capacity/physical structure for LPA
PCR• Available technical skills• At least provisionally confirm MDR
phenotypically• Technical problems eg amplicon contamination


THANK YOU