Cervical Stenosis and Myelopathy. Normal Anatomy.
18
Cervical Stenosis and Myelopathy
-
Upload
clyde-white -
Category
Documents
-
view
236 -
download
1
Transcript of Cervical Stenosis and Myelopathy. Normal Anatomy.

Cervical Stenosis and Myelopathy

Normal Anatomy

Pathophysiology• Spinal Stenosis
– Description rather than a diagnosis– narrowing of the vertebral canal, lateral recess or intervertebral
foramen – commonly caused by degenerative changes– May result in myelopathy
• Myelopathy– impaired function of the spinal cord caused by compression– generally progressive and develops slowly
• Myelopathy caused by spondylosis is called cervical spondylotic myelopathy (CSM)– most prevalent at the C5-C6 level– rarely seen in the upper cervical segments (C3-C4)

Cervical Spondylotic Myelopathy
• Result of degenerative changes – ligamentum flavum hypertrophy or buckling, – facet joint hypertrophy– disc protrusion– posterior spondylotic ridges
• overall reduction in canal diameter • cord compression


Mechanism Of Injury- Stenosis• Insidious
– Congenital/Inherited• Idiopathic (hereditary)• Achondroplastic
– Acquired Stenosis• Infection• Tumours• Foreign Bodies• Disc Protusion• Ligamentous Hypertrophy• Osteophyte formation• Facet joint Hypertophy• Spondylolisthesis
• Traumatic– Fractures– Upper Cervical Instability

Mechanism Of Injury- Myelopathy
• Insidious– Stenosis causes– Rheumatoid Arthritis
• Trauma– Fractures– Ligament Rupture (Upper Cervical Instability)

Subjective - StenosisStenosis• Presentation will depend on associated
pathology• Insidious onset• Progressive worsening of symptoms• Aggravating by positions that reduce space
(extension, rotation)

Subjective - MyelopathyMyelopathy• Upper and/or lower limb pain, weakness, sensation
changes• Clumsiness• Neuropathic pain• Gradually worsening symptoms• Bladder or bowel dysfunction• Difficulty walking for long distances• Reduced fine motor skills and co ordination• Falls• Insidious onset of pain• Neck pain may or may not be present

ObjectiveStenosis• Presentation will depend on associated pathology • Pain with movements that close space
Myelopathy• Upper and/or lower quarter sensation loss (bilateral or
quadrilateral)• Bilateral or quadrilateral weakness• Pathological reflexes• Poor co ordination and fine motor skills• Increased and Decrease Tone

Objective
Stenosis• Presentation will depend on associated pathology ie myelopathy
Myelopathy• Hyper reflexia in the upper or lower extremities• Hypertonia• Positive Hoffmans and/or Babinski sign• Sensory changes• Weakness• Decreased dexterity• Gait instability

Special Tests
• Hoffmans (upper limb Babinski)
• Babinski• Romberg

Further Investigation• MRI (angled sagittal)• CT with Myelogram
(dye injected to highlight the nerves)
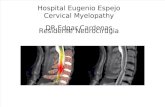
Sagittal T2-weighted magnetic resonance imaging of the cervical spine, which demonstrated moderately severe spinal stenosis at the C3–C4, C5–C6, and C6–C7 levels, with less severe spinal stenosis at the C4–C5 level

Axial T2 weighted MRI (A) and CT myelograph (B) at C4-C5 level showing an ossified mass on the right with bony protrusion into the canal

General Management
• Analgesia• Gabapentin• Activity modification

Conservative – Management - Myelopathy
Myelopathy• Immediate onwards referral • If diagnostics have already been completed and
conservative management suggested, monitor symptoms closely, if they worsen surgical intervention may be indicated.
• Myelopathy may develop rapidly and delays in surgical intervention may result in poor outcome.
• Heat/Ice• Traction

Conservative - Management - Stenosis
• Stenosis– Manage the underlying pathology
• Pain Relief– NSAID’s, Ice, Massage
• Restore Normal ROM– Tx, Cx and Shoulders– Soft tissue techniques and joint mobilisations
• Restore Normal Neurodynamics– Soft tissue techniques, joint mobilisations, nerve sliders
• Restore Normal Muscular Activation– Scapular stabilisers, deep cervical extensors, deep cervical flexors

Surgical - Management• Decompress the cervical spinal canal and achieve
an arthodesis of the treated levels. This can be achieved in the following ways:
Posterior approach• Laminectomy• LaminoplastyAnterior approach• Discectomy and interbody fusion• Corpectomy and fusion