Cervical carcinoma
29
SAMIA SHAHEEN 08-166 CERVICAL CARCINOMA
-
Upload
ayub-medical-college -
Category
Education
-
view
133 -
download
0
Transcript of Cervical carcinoma

SAMIA SHAHEEN
08-166
CERVICAL CARCINOMA

Cervical carcinoma
Definition
Malignant neoplasm
arising from the cells of
cervix uteri.

Epidemiology
Second most common cancer in women.
Third most common cause of death among women.
16 per 100,000 cases reported globally every year.
80% cases from developing countries.
Pakistan:19.5 cases per 1lac population (WHO 2008)
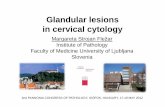
Anatomy of cervix
Lowest part of uterus
1 inch in length
Anatomical divisions

Histology
Stratified squamous
epithelium
Simple columnar
epithelium
SQUAMOCLOMNAR
JUNCTION
Nabothian cysts

Types
squamous cell carcinoma (about 80-85%)
adenocarcinoma (about 15%)
adenosquamous carcinoma
small cell carcinoma
neuroendocrine tumour
glassy cell carcinoma
villoglandular adenocarcinoma

Risk factors
Human Papillomavirus (HPV) Infection
Family History of Cervical Cancer
Age
Sexual and Reproductive History
Socioeconomic Status
Smoking
HIV Infection
In Utero DES Exposure
Long-term use of oral contraceptives

Human Papillomavirus
Small, circular, double
stranded DNA genome.
150-200 types of HPV
known
15 are classified as high-
risk types (16, 18, 31,
33, 35, 39, 45, 51, 52,
56, 58, 59, 68, 73, and
82)
Infects rapidly dividing
cells at squamocolumnar
junction
Oncogenes:E6 and E7

Symptoms
Asymptomatic
Postcoital bleed
Intermenstrual bleed
Postmenopausal bleed
Malodorous vaginal discharge
Urinary frequency, retention
Sciatic pain
Swelling of lower extremity(s)
Urinary/fecal incontinence
Bone fractures

Diagnosis
History and physical examination
Papanicolaou smear/liquid based cytology
HPV-DNA testing
Colposcopy: endocervical curettage
Per rectal examination
Biopsy

Diagnosis
History and physical
examination
Risk factors, past
illness, treatments, signs
of health and disease,
lumps and swellings.
Pelvic examination
Bimanual pelvic
examination
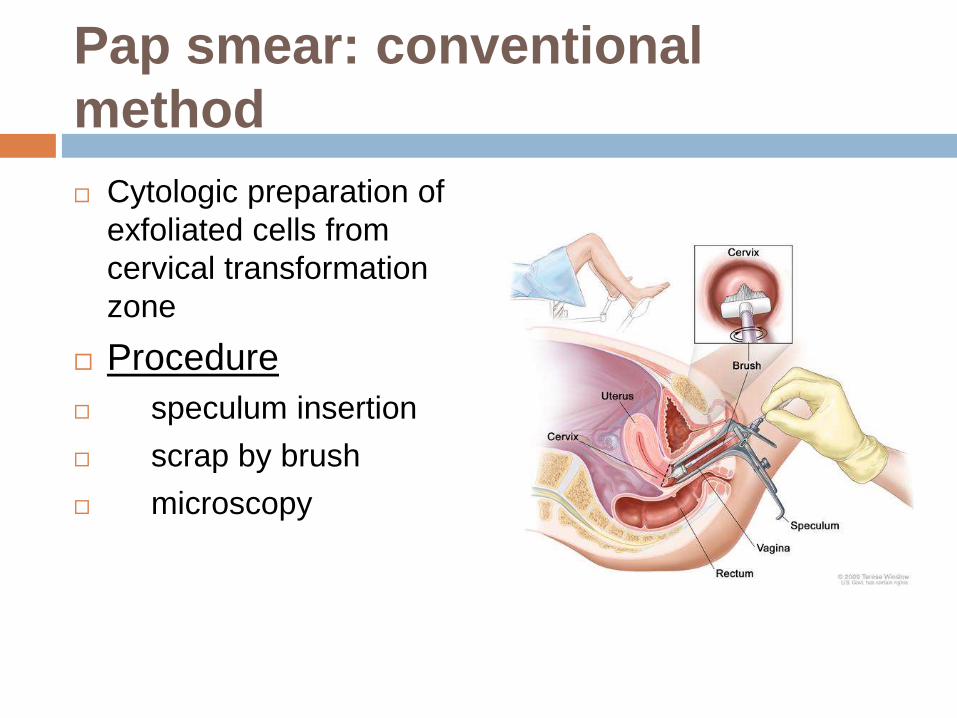
Pap smear: conventional
method
Cytologic preparation of
exfoliated cells from
cervical transformation
zone
Procedure
speculum insertion
scrap by brush
microscopy
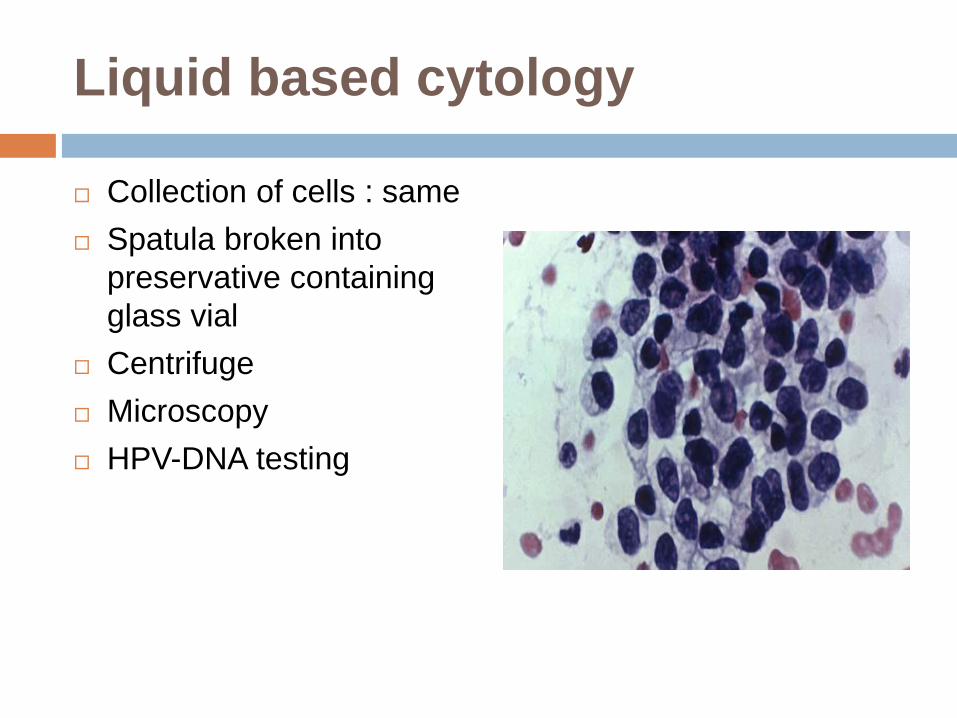
Liquid based cytology
Collection of cells : same
Spatula broken into
preservative containing
glass vial
Centrifuge
Microscopy
HPV-DNA testing
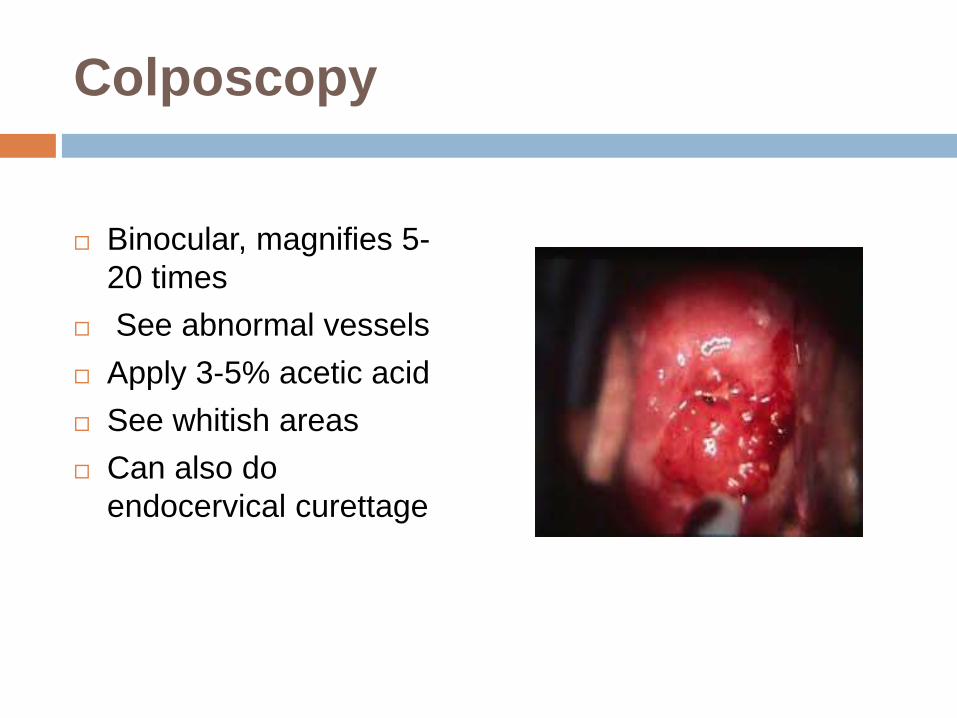
Colposcopy
Binocular, magnifies 5-
20 times
See abnormal vessels
Apply 3-5% acetic acid
See whitish areas
Can also do
endocervical curettage

Biopsy
When abnormal cells are found on cytology
Simple biopsy
Small amount of tissue removed in doctor’s office
Cone biopsy
Cone of tissue removed, need to visit hospital

Grading: BATHESDA SYSTEM
LSIL
CIN I
HSIL
CIN II
CIN III
DOES NOT MEAN THE
STAGING

Staging
Inspection and palpation
Colposcopy
Hysteroscopy
X-Ray chest and skeleton
Abdominal ultrasound
Intravenous urography
MRI
PET scan
LEEP and conization
Results viewed together with the results of the original tumor biopsy to determine the cervical cancer stage.

FIGO Staging system
STAGE IA STAGE IB

FIGO system: cont
STAGE II

FIGO system: cont
STAGE IIIA STAGE IIIB

FIGO system: cont
STAGE IVA STAGE IVB

Treatment
Depends upon
Stage of tumor
Size
Age and general health
Desire to have children

Treatment
Stage I
IA1: LEEP or cone biopsy,trachelectomy
IA2: hystrectomy,remove lymph nodes as well
Stage IB1 and Stage IIA
Wertheim hysterectomy, radiation therapy
Stage IIB –IVA
Chemo radiotherapy followed by hysterectomy
Recurrence
Pelvic externation

Treatment during pregnancy
Depends on the time of diagnosis
1st trimester: external irradiation, abortion, internal
irradiation and chemotherapy
Last trimester:hysterotomy or caesarean section
followed by radical hysterectomy

Palliative treatment
At the advanced stage disease
Pain free and comfort
Expert nursing

Prognosis
Depends on volume and stage of the disease
5 year survival rate
Stage I: 80% -90%
Stage II: 60% -75%
Stage III: 30%-40%
Stage IV: 15%

Screening and prevention
Types of screening
Conventional cytology
Liquid-based monolayer cytology
Human papillomavirus testing
Testing in resource-poor areas
Visual inspection to detect pre-cancer or cancer
Prevention
HPV vaccination
Quit smoking
Limitation of sexual partners
Barrier methods of contraception
Regular Pap smears
Diet with anti oxidants: vita A, vit B12, vit C, vit E, beta
carotene.

THANK YOU






![A Phase II Clinical Trial of BMS–247550 (NSC 710428), an ... · 1.2.1 Cervical Carcinoma Cervical cancer is the second most common cancer among women worldwide [1]. The proportion](https://static.fdocuments.in/doc/165x107/5fa82680c104f33f0c59d8cf/a-phase-ii-clinical-trial-of-bmsa247550-nsc-710428-an-121-cervical-carcinoma.jpg)