
Cerebrovascular Accident Aka: Stroke Brain Attack.
64
Cerebrovascular Accident Aka: Stroke Brain Attack
-
Upload
camilla-wilcox -
Category
Documents
-
view
253 -
download
2
Transcript of Cerebrovascular Accident Aka: Stroke Brain Attack.
Cerebrovascular Accident
Aka: Stroke
Brain Attack
http://www.strokecenter.org/education/index.html

In this Session
• Brain structure and function• Cerebral circulation• Haemorrhagic stroke• TIA• Ischaemic stroke• Manifestations• Diagnosis and management• Long term disabilities

Review of Brain Structure & Function

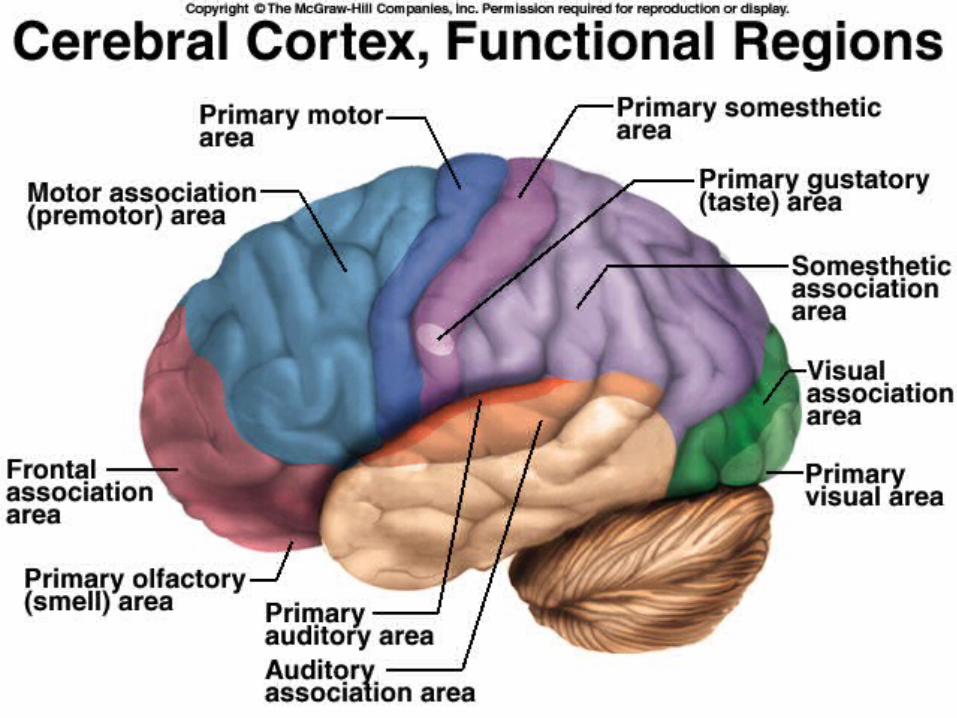
Cerebral Cortex
– Divided into Hemispheres
– Functions• Motor - Controlling voluntary movements
• Sensory - Registers and processing sensations
• Association - Higher mental functions
• Language - Comprehension and Production
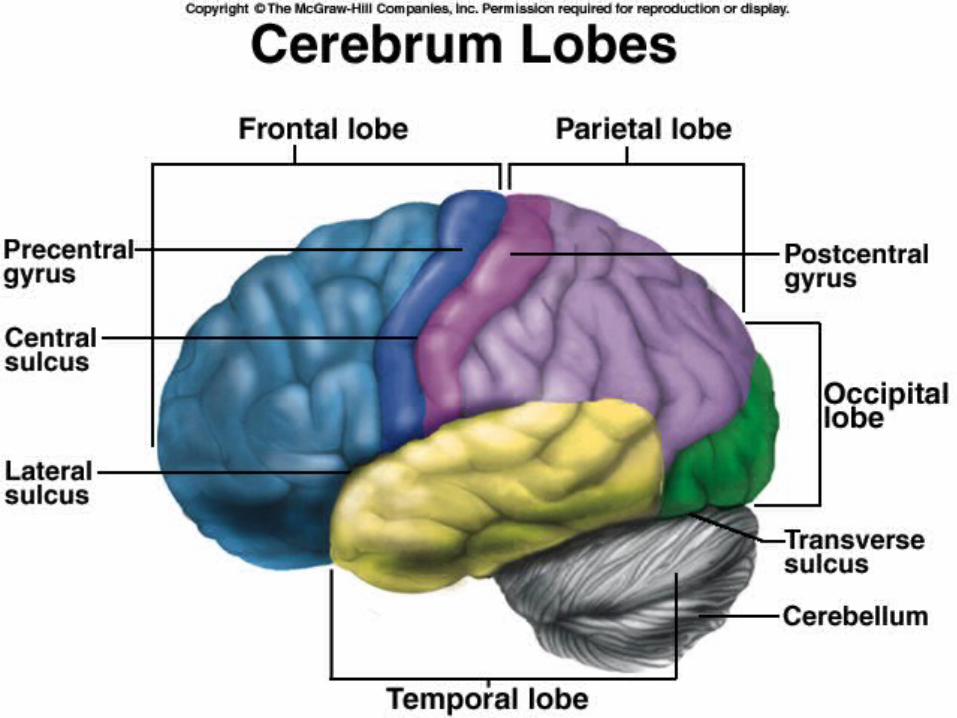

Cerebral Hemispheres: Lobes
– Frontal
– Temporal
– Parietal
– Occipital


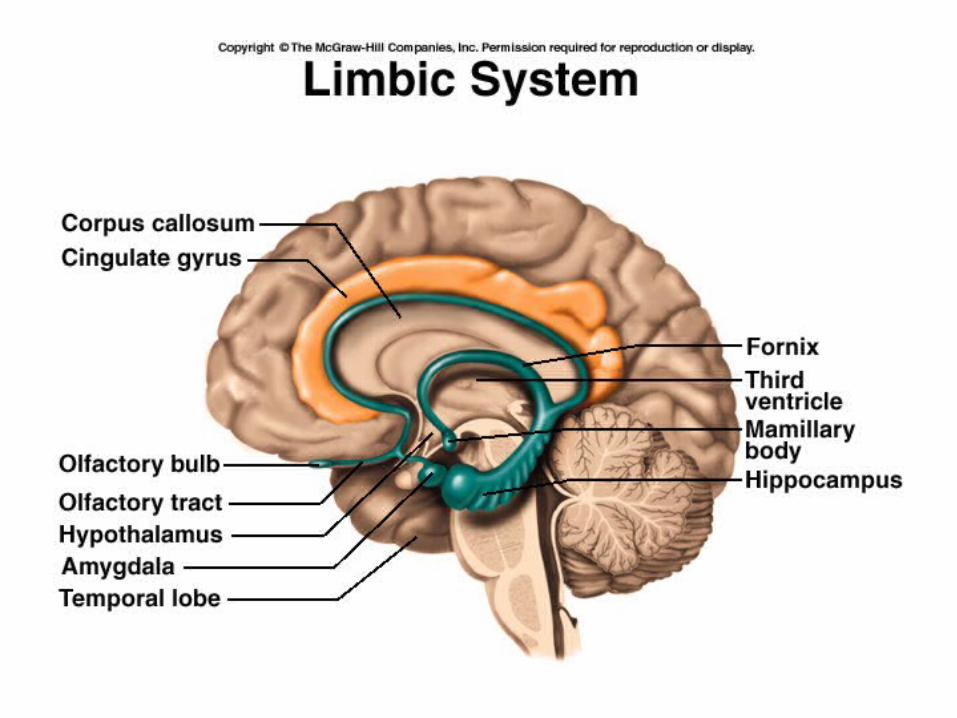
Other Brain Structures
– Brainstem – Medulla – Reticular formation


Other Brain Structures
– Thalamus

Other Brain Structures
– Cerebellum


Other Brain Structures
– Hypothalamus

Language
• Wernicke’s Area– Temporal lobe
– Recognition of spoken & written language
– Composition of spoken and written language

Language
• Broca’s Area– Frontal lobe
– Speech motor function


Coordination of Language in the Brain - How do we read aloud?

Vision


Cerebral Circulation



Arteries supplying the Brain
• Aortic Arch Common Carotid Artery (left & right) internal carotid artery (Left & Right) Circle of Willis
• Aortic Arch Subclavian Arteries Vertebral Arteries (Left & Right) Merge to form Basilar Artery Circle of Willis
• Circle of Willis left & right: Anterior, Middle & Posterior Cerebral Arteries


Definition of Stroke
• Acute focal neurological deficit as a result of vascular disorder
Epidemiology
• Third leading cause of death
• Over 70% strokes in people aged > 65 yr
• Ave. age males 68 yr, female 74 yr
• 1998 Age-standardised stroke mortality (per 100,000 pop) is 43 male, 42 female
• A leading cause of Disability

Risk Factors for Stroke
• Advanced age• Systolic hypertension• Diabetes mellitus• Hypercholesterolemia• Carotid artery stenosis• TIAs• CIGARETTE SMOKING• Lack of exercise• CV disease especially atrial fibrillation• Increased weight
Non-Modifiable Risk Factors
• Age– Risk doubles for each decade after 55 years of
age
• Gender– Men slightly higher than women
• Race
• Heredity
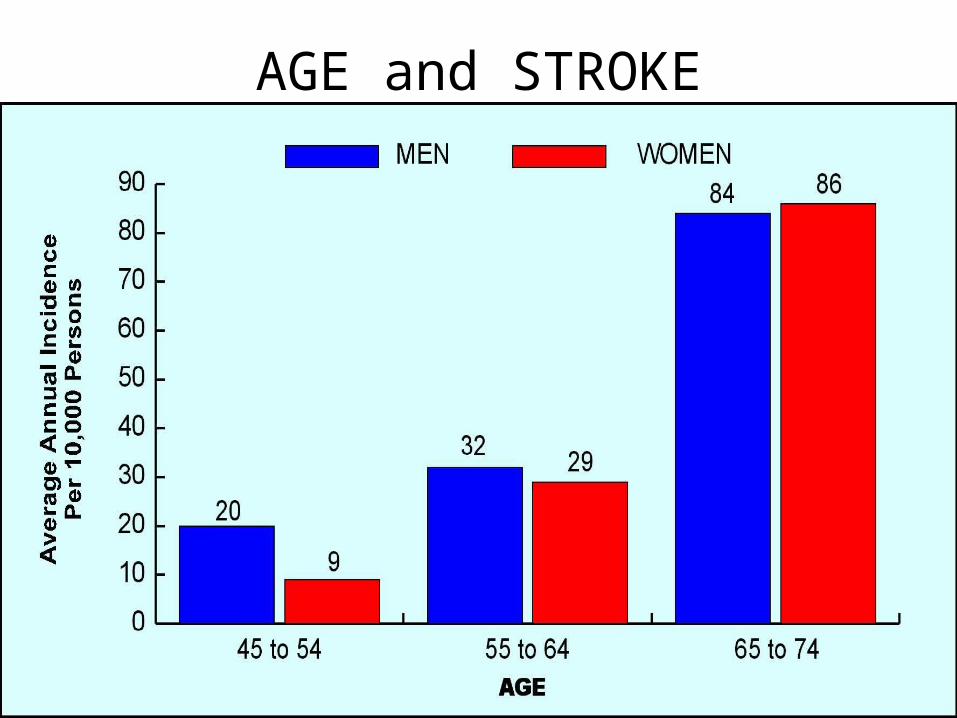
AGE and STROKE

Modifiable Risk Factors
Hypertension RR 4.0
Diabetes RR 1.8
Smoking RR 1.7
Coronary disease RR 2.2
TIA RR 3.9
Atrial fibrillation RR 2.6-4.5
Hyperlipidemia RR 1.8-2.6

Modifiable Risk Factors
For ischaemic stroke:
• Being overweight increases risk by 22%
• Being obese increases risk by 64%

Diet and Stroke• Fish: 3 servings a day associated with a 6% lower
risk of stroke• Fruits and vegetables: >5 servings a day
associated with a 26% lower risk of stroke• Meat: Each daily serving associated with a 24%
increased risk of stroke• Reduced-fat milk: associated with a lower risk of
stroke vs full-fat milk• Chocolate: High consumption associated with a
29% lower risk of stroke
Diet and Stroke• Coffee: 3 to 4 cups per day associated with a 17%
lower risk of stroke• Tea: ≥3 cups per day associated with a 21% lower
risk of stroke• Sugar-sweetened beverages: high intake
associated with increased obesity, diabetes, metabolic syndrome, and coronary heart disease
• Whole grains: high intake associated with a 21% lower incidence of cardiovascular events
• Rice: intake not associated with risk of stroke

Types of Stroke
• Haemorrhagic
• AND
• Ischaemic

Haemorrhagic Stroke
• 15% of strokes
• Release of blood into the extravascular space
• Caused by:– Hypertension– Aneurysms – Head Injury

Berry Aneurysm
• Cause unknown
• Usually around Circle of Willis


Haemorrhagic Stroke
• Rupture of blood vessel causes:– Haemorrhage– Oedema– Compression
• Death is common

Haemorrhage
• Intracerebral haemorrhage
• Subarachnoid haemorrhage

Transient Ischaemic Attack (TIA)
• Ministroke or Brain angina
• Fleeting attack of paralysis, numbness, tingling, aphasia, unilateral blindness or dizziness
• Zone of penumbra without central infarction
• Last less than 24 hours
TIA’s
• Warning
• First month after a TIA, carries a 4-8% risk of stroke
• First year, 12-13%; 24-29% over 5 years
• Note: Do not have associated pain (rare), so people may ignore them
• Person should seek immediate medical attention

Ischaemic Penumbra
• Prolonged hypoperfusion (<10 ml/100 gm/min) leads to Cell death
• Ischaemic penumbra is a zone of dysfunctional but not dead brain tissue surrounding an infarct
• Dysfunctional tissue may infarct • “Brain is Time”- need treatment within 3
hours

Ischaemic Stroke
• 85% of all strokes
• Ischaemic: lack of blood flow
• Caused by– Emboli– Thrombosis
• Types are Thrombotic Stroke, Cardiogenic Embolic Stroke, Lacunar Stroke

Thrombotic Stroke
• Most common
• Common sites are the origins of internal carotid, vertebral arteries and junctions of basilar and vertebral arteries
• Normally a single cerebral artery is affected
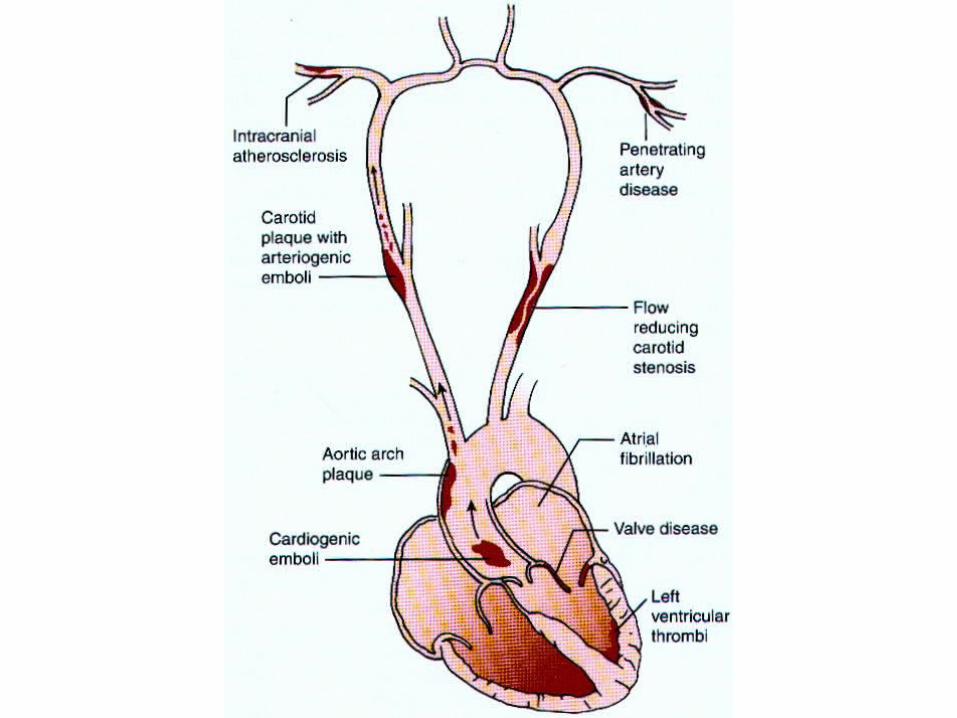

Cardiogenic Emboli Stroke
• Caused by a moving blood clot
• Most common site is middle cerebral artery
• Most emboli originate in the left heart
• Atrial fibrillation and other heart disease predisposes to embolus formation
Lacunar Stroke
• Small infarcts in deeper, noncortical parts of brain or brain stem
• Cause can be embolism, hypertension, small haemorrhages
• Leave lacunae upon healing
• Produce “lacunar syndromes”
• MRI for diagnosis

Manifestations

Terminology
• Hemiplegia – Paralysis on one side of body• Hemiparesis – weakness on one side of
body• Hemianopia –vision loss in one side of
visual field• Aphasia –language disturbance (speech,
comprehension, writing)• Dysarthria – slurred speech

Terminology
• Diplopia – double vision
• Dysphagia – difficulty swallowing
• Agnosia – impairment of recognition of sensory stimuli
• Ataxia – imbalance
• Apraxia – inability to properly execute movements

Presentations of Acute Stroke
• Alteration in Consciousness• Stupor, delirium, coma, confusion,
memory loss, seizures• Headache; severe and/or neck or facial
pain (Not common)• Aphasia• Facial weakness or asymmetry

Presentations of Acute Stroke
• Weakness, paralysis, or sensory loss
• Ataxia (poor balance, clumsiness, or difficulty walking)
• Visual loss, monocular or binocular
• Intensive vertigo, double vision
Anterior Cerebral Artery Occlusion
• Paralysis of contralateral leg
• Paresis of contralateral arm
• Problems making decisions
• Speech disturbance (aphasia if left hemisphere stroke)
• Some sensory loss over toes, foot, leg

Middle Cerebral Artery Occlusion
• Contralateral hemiplegia (face & arm)
• Contralateral Sensory impairment
• Speech disturbance (aphasia), including difficulty in comprehending written words and writing
• Some visual field loss

Posterior Cerebral ArteryOcclusion
• Visual distubances (Hemianopsia, colour blindness)
• Memory deficits
• Loss of all sensory modalities (thalamus)

Basilar Artery Occlusion
• Complete obstruction of the basilar artery is usually rapidly fatal
• Rapid onset of unconsciousness and deepening coma.
• Supplies the Brain Stem
Vertebral Artery Occlusion
• Vertigo at onset
• Visual distubances (diplopia)
• Ataxia
• Dysphagia
• Dysphonia

Stroke Diagnosis
• Neurological Assessment
• Neuroimaging– Eg. CT, MRI (important for differentiating
ischaemic from haemorrhagic stroke)
• Vascular Imaging– Eg. Angiography
• Carotid Ultrasound

Management: Ischaemic Stroke
• Goal: protection of penumbra zone– Maximize cerebral blood flow and blood volume,
reduce viscosity– Maintain perfusion pressure
• Recanalization with thrombolytic therapy Eg. Tissue plasminogen activator (tPA), streptokinase, urokinase
• Anticoagulants to block occlusive processes (eg. Aspirin)

Long Term Disabilities
• Motor deficits
• Language and speech problems
• Dysarthria
• Aphasia
• Denial or hemiattention


















