Cerebral Venous Thrombosis Associated With...
6
1880 Cerebral Venous Thrombosis Associated With Pregnancy and Puerperium Review of 67 Cases Carlos Cantu, MD; Fernando Barinagarrementeria, MD Background and Purpose: Cerebral venous thrombosis is characterized by its clinical pleomorphism and pathogenetic variability. We studied 67 patients with cerebral venous thrombosis associated with pregnancy and puerperium and compared them with 46 other cases unrelated to obstetric causes to disclose differences in their clinical presentation, neuroradiological findings, clinical course, and prognosis. Methods: In this retrospective study, we analyzed the clinical, laboratory, and neuroimaging findings of 113 patients collected consecutively at our institute. The diagnosis of cerebral venous thrombosis was confirmed by angiography, magnetic resonance imaging, or neuropathological study. Results: Patients with cerebral venous thrombosis associated with pregnancy and puerperium were younger (average age, 26 versus 36 years), and in most, the onset of symptoms was acute (82% versus 54%; P=.003). The evolution of symptoms reached a plateau within 10 days in 70% of patients with thrombosis from obstetric causes, compared with only 45% in those from other causes (P=.01). Anemia was more frequent in the obstetric group (64% versus 26%; P=.00001). There were no differences regarding neurological and neuroradiological findings. Although the initial severity of illness was similar in both groups, the final outcome was considered good in 80%, of patients with obstetric causes, compared with 58% of patients with other causes (P=.01); mortality rates were 9% and 33%, respectively (P=.002). Conclusions: Cerebral venous thrombosis associated with pregnancy and puerperium has a more acute onset and a better prognosis than thrombosis due to other causes. These findings might be helpful in the diagnostic and therapeutic strategies for patients with cerebral venous thrombosis. (Stroke. 1993;24: 1880-1884.) KEY WoRDs * pregnancy * puerperium * thrombosis * women In 1828, Abercrombiel published the first clinico- pathological description of a case of puerperal cerebral venous thrombosis (CVT). Since then, the association of CVT with pregnancy and puerperium has been recognized, especially in developing coun- tries.2-4 Of 113 cases of aseptic CVT seen in the past 20 years at the National Institute of Neurology and Neu- rosurgery in Mexico City, 67 were diagnosed in the puerperal period, 5 during pregnancy, and in 1 patient after abortion. The aim of this paper is to analyze these 67 cases and compare them with the remaining 46 cases of CVT, which were not related to obstetric causes, to disclose some clinical, paraclinical, or prognostic fea- tures that may be distinctive for patients with CVT associated with pregnancy and puerperium. Subjects and Methods Patients with a diagnosis of aseptic CVT admitted to our hospital were included in this study when they satisfied any of the following criteria: Received March 24, 1993; final revision received July 18, 1993; accepted August 3, 1993. From the Stroke Clinic, National Institute of Neurology and Neurosurgery, Mexico City. Correspondence to Dr Carlos Cantu, Instituto Nacional de Neurologia y Neurocirugia, Insurgentes Sur 3877, Tlalpan, Mexico 14269 DF, Mexico. 1. Angiographic evidence of CVT5,6: total or partial lack of filling of at least one sinus on at least two projections. When the lack of filling involved only the anterior portion of the superior sagittal sinus or only one lateral sinus, additional signs of CVT were re- quired, such as evidence of delayed venous emptying or development of collateral circulation. 2. Evidence of CVT via neuropathological study: presence of thrombosis of venous sinuses or cerebral veins, with or without associated venous infarction. 3. Magnetic resonance imaging (MRI) evidence of CVT7: absence of voiding on TI weighted images with isointensity or hypointensity on T2 weighted images during the first few days and hyperintensity of the lumen of the sinus on T1 and T2 weighted images from about 1 week to 1 month after thrombosis. Patients were excluded when (1) clinical or radiolog- ical records were incomplete, (2) radiological studies were inconclusive, (3) there was cavernous sinus throm- bosis, or (4) CVT was associated with sepsis. Of 67 patients with CVT associated with pregnancy and pu- erperium (group 1), 50 were included on the basis of angiographic criteria, 10 by MRI criteria, and 7 by neuropathological criteria. Of the 46 cases with CVT unrelated to obstetric events (group 2), 26 were in- cluded on the basis of angiographic criteria, 11 by neuropathological criteria, and 9 by MRI criteria. The following characteristics were compared between the two groups: by guest on May 13, 2018 http://stroke.ahajournals.org/ Downloaded from
Transcript of Cerebral Venous Thrombosis Associated With...

1880
Cerebral Venous Thrombosis Associated WithPregnancy and Puerperium
Review of 67 Cases
Carlos Cantu, MD; Fernando Barinagarrementeria, MD
Background and Purpose: Cerebral venous thrombosis is characterized by its clinical pleomorphism andpathogenetic variability. We studied 67 patients with cerebral venous thrombosis associated withpregnancy and puerperium and compared them with 46 other cases unrelated to obstetric causes todisclose differences in their clinical presentation, neuroradiological findings, clinical course, andprognosis.Methods: In this retrospective study, we analyzed the clinical, laboratory, and neuroimaging findings of
113 patients collected consecutively at our institute. The diagnosis of cerebral venous thrombosis wasconfirmed by angiography, magnetic resonance imaging, or neuropathological study.
Results: Patients with cerebral venous thrombosis associated with pregnancy and puerperium wereyounger (average age, 26 versus 36 years), and in most, the onset of symptoms was acute (82% versus 54%;P=.003). The evolution of symptoms reached a plateau within 10 days in 70% of patients with thrombosisfrom obstetric causes, compared with only 45% in those from other causes (P=.01). Anemia was morefrequent in the obstetric group (64% versus 26%; P=.00001). There were no differences regardingneurological and neuroradiological findings. Although the initial severity of illness was similar in bothgroups, the final outcome was considered good in 80%, of patients with obstetric causes, compared with58% of patients with other causes (P=.01); mortality rates were 9% and 33%, respectively (P=.002).
Conclusions: Cerebral venous thrombosis associated with pregnancy and puerperium has a more acuteonset and a better prognosis than thrombosis due to other causes. These findings might be helpful in thediagnostic and therapeutic strategies for patients with cerebral venous thrombosis. (Stroke. 1993;24:1880-1884.)KEY WoRDs * pregnancy * puerperium * thrombosis * women
In 1828, Abercrombiel published the first clinico-pathological description of a case of puerperalcerebral venous thrombosis (CVT). Since then,
the association of CVT with pregnancy and puerperiumhas been recognized, especially in developing coun-tries.2-4 Of 113 cases of aseptic CVT seen in the past 20years at the National Institute of Neurology and Neu-rosurgery in Mexico City, 67 were diagnosed in thepuerperal period, 5 during pregnancy, and in 1 patientafter abortion. The aim of this paper is to analyze these67 cases and compare them with the remaining 46 casesof CVT, which were not related to obstetric causes, todisclose some clinical, paraclinical, or prognostic fea-tures that may be distinctive for patients with CVTassociated with pregnancy and puerperium.
Subjects and MethodsPatients with a diagnosis of aseptic CVT admitted to
our hospital were included in this study when theysatisfied any of the following criteria:
Received March 24, 1993; final revision received July 18, 1993;accepted August 3, 1993.From the Stroke Clinic, National Institute of Neurology and
Neurosurgery, Mexico City.Correspondence to Dr Carlos Cantu, Instituto Nacional de
Neurologia y Neurocirugia, Insurgentes Sur 3877, Tlalpan, Mexico14269 DF, Mexico.
1. Angiographic evidence of CVT5,6: total or partiallack of filling of at least one sinus on at least twoprojections. When the lack of filling involved only theanterior portion of the superior sagittal sinus or onlyone lateral sinus, additional signs of CVT were re-quired, such as evidence of delayed venous emptying ordevelopment of collateral circulation.
2. Evidence of CVT via neuropathological study:presence of thrombosis of venous sinuses or cerebralveins, with or without associated venous infarction.
3. Magnetic resonance imaging (MRI) evidence ofCVT7: absence of voiding on TI weighted images withisointensity or hypointensity on T2 weighted imagesduring the first few days and hyperintensity of thelumen of the sinus on T1 and T2 weighted images fromabout 1 week to 1 month after thrombosis.
Patients were excluded when (1) clinical or radiolog-ical records were incomplete, (2) radiological studieswere inconclusive, (3) there was cavernous sinus throm-bosis, or (4) CVT was associated with sepsis. Of 67patients with CVT associated with pregnancy and pu-erperium (group 1), 50 were included on the basis ofangiographic criteria, 10 by MRI criteria, and 7 byneuropathological criteria. Of the 46 cases with CVTunrelated to obstetric events (group 2), 26 were in-cluded on the basis of angiographic criteria, 11 byneuropathological criteria, and 9 by MRI criteria.The following characteristics were compared between
the two groups:
by guest on May 13, 2018
http://stroke.ahajournals.org/D
ownloaded from

Canti and Barinagarrementeria Cerebral Venous Thrombosis
TABLE 1. Clinical Profile and Evolution of Cerebral Venous Thrombosis
Group 1 (n=67) Group 2 (n=46)
n % n % P
Onset
Acute 55 82.1 25 54.3 .003
Insidious 12 17.9 21 45.7
Evolution
Progressive 48 71.6 24 52.2 .03
Nonprogressive 19 28.4 22 47.8
Time elapsed between onset andstabilization of symptoms
<10 days 47 70.1 21 45.7 .01
>10 days 20 29.9 25 54.3
Time elapsed between onset anddiagnosis<1 week 38 56.7 10 21.7 .0002
1-3 weeks 25 37.3 16 34.8
>3 weeks 4 6.0 20 43.5
1. Clinical: mode of onset, classified as "acute"(symptoms appeared suddenly or developed in less than48 hours) or "insidious" (gradual development of symp-toms over several days or weeks); presenting symptoms;clinical course, classified as "progressive" (developmentof additional symptoms and/or worsening of the pre-senting symptoms) or "nonprogressive" (presentingsymptoms remained stable or tended to subside withoutdevelopment of additional symptoms); neurologicalsigns and symptoms; time elapsed between the onsetand stabilization of symptoms; and time elapsed be-tween onset and diagnosis.
2. Hematologic: anemia (hemoglobin <12 g%), leu-kocytosis (white blood count >10 000/mm3), thrombo-cytosis (platelet count >450 000/mm3), erythrocyte sed-imentation rate (ESR) (normal 0 to 20 mm/h), andpolycythemia (hematocrit >60%).
3. Cerebrospinal fluid (CSF) data: opening pressure(normal pressure <200 mm water), total protein (nor-mal value 15 to 45 mg/dL), and cell count (normal value<5 cells/mm3).
4. Neuroimaging: evidence of CVT and associatedparenchymal lesions detected by computerized tomogra-phy (CT) and MRI. Abnormalities considered as directsigns of CVT on CT scan included the cord sign, thedense triangle, and the empty delta sign. Hemorrhagicinfarction was defined as patchy areas of high attenuationwith indistinct margins and a speckled or mottled appear-ance, whether separate or coalescent, within a venousinfarction. Intracerebral hemorrhage was defined as ahomogeneous region of high attenuation.
5. Sites of thrombosis within the cerebral venoussystem.
6. Clinical evaluation at the time of discharge fromhospital: classified as "good outcome" when patientsrecovered fully or had partial functional recovery withonly mild sequelae and "poor outcome" when sequelaewere serious or the patient died.
Treatment for both groups was mainly conservative.Only five patients with puerperal CVT received antico-agulation therapy, and their data were excluded fromthe final outcome evaluation tables because it is wellknown that anticoagulation in the early stages of CVTmodifies its natural history.8'9
Differences between groups were tested for statisticalsignificance using multivariate analysis with 2x 2 contin-gency tables, x2 test, and Fisher's exact test.
ResultsThe mean age of group 1 patients was 26 years (range,
16 to 44 years) and of group 2, 36 years (range, 15 to 77years). Thirteen male patients were included in group 2.
Regarding puerperal patients, 21 cases of CVT(34.4%) occurred during the first week after delivery (9within the first 48 hours) and 36 (59%) during weeks 2and 3 postpartum. Pregnant patients were affected inany trimester (1 in the first, 2 in the second, and 2 in thethird trimester). In group 1, there were 43 multiparas(64.1%), 36 women (53.7%) from low or rural socialstratum, and 21 women (31.3%) whose delivery wasconducted at home by midwives and who did not haveproper prenatal care. Three patients had a history ofvenous thrombosis outside the central nervous systemduring previous pregnancies (two instances of pelvicvenous thrombosis and 1 case of pulmonary embolism).
Patients from group 2 had the following predisposingfactors for CVT: use of oral contraceptives (7 patients),thrombocytosis in 4 patients, secondary polycythemia in3 cases, circulating lupus anticoagulant in 2, and proteinS deficiency in 2. In addition, an arteriovenous malfor-mation was present in 2 patients and metastatic carci-noma in 1. In the remaining 25 cases, no predisposingfactors were found.
Clinical, laboratory, and neuroradiological findingsare displayed in Tables 1 through 5. Results of the finalclinical evaluation are shown in Table 6. Several differ-ences were relevant: (1) Patients of group 1 had an
1881
by guest on May 13, 2018
http://stroke.ahajournals.org/D
ownloaded from
1882 Stroke Vol 24, No 12 December 1993
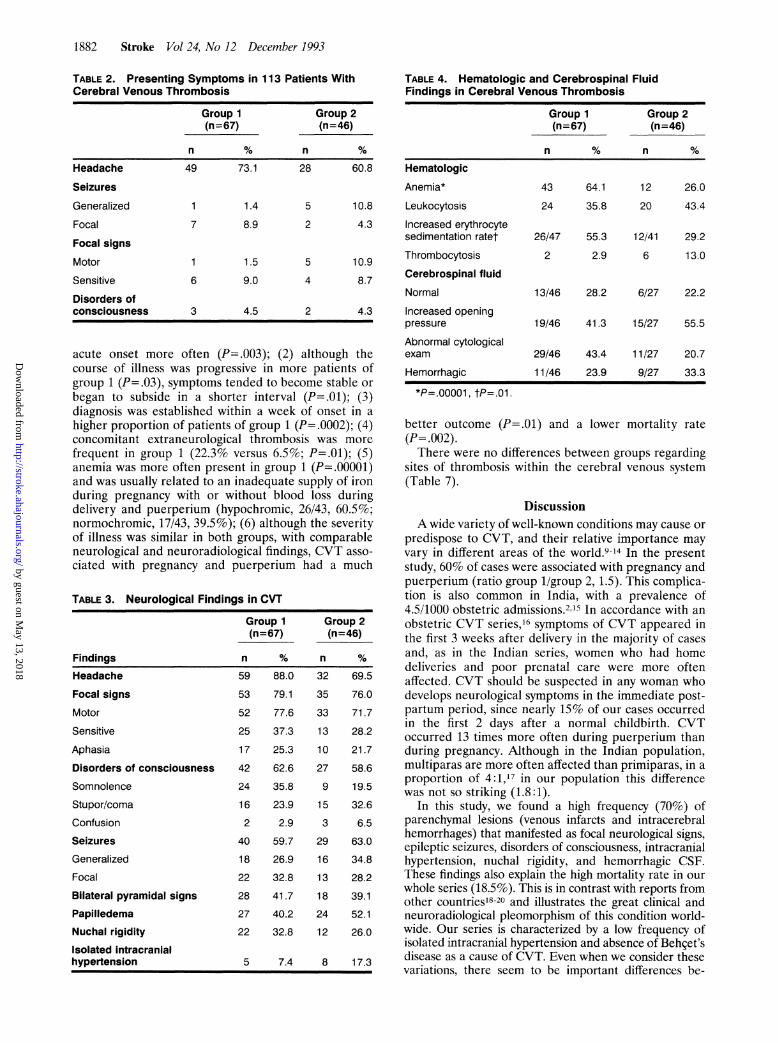
TABLE 2. Presenting Symptoms in 113 Patients WithCerebral Venous Thrombosis
Group 1 Group 2(n=67) (n=46)
n % n %
Headache 49 73.1 28 60.8
Seizures
Generalized 1 1.4 5 10.8
Focal 7 8.9 2 4.3
Focal signsMotor 1 1.5 5 10.9
Sensitive 6 9.0 4 8.7
Disorders ofconsciousness 3 4.5 2 4.3
acute onset more often (P=.003); (2) although thecourse of illness was progressive in more patients ofgroup 1 (P=.03), symptoms tended to become stable orbegan to subside in a shorter interval (P=.01); (3)diagnosis was established within a week of onset in ahigher proportion of patients of group 1 (P=.0002); (4)concomitant extraneurological thrombosis was morefrequent in group 1 (22.3% versus 6.5%; P=.01); (5)anemia was more often present in group 1 (P=.00001)and was usually related to an inadequate supply of ironduring pregnancy with or without blood loss duringdelivery and puerperium (hypochromic, 26/43, 60.5%;normochromic, 17/43, 39.5%); (6) although the severityof illness was similar in both groups, with comparableneurological and neuroradiological findings, CVT asso-ciated with pregnancy and puerperium had a much
TABLE 3. Neurological Findings in CVT
Group 1 Group 2(n=67) (n=46)
Findings n % n %
Headache 59 88.0 32 69.5
Focal signs 53 79.1 35 76.0
Motor 52 77.6 33 71.7
Sensitive 25 37.3 13 28.2
Aphasia 17 25.3 10 21.7
Disorders of consciousness 42 62.6 27 58.6
Somnolence 24 35.8 9 19.5
Stupor/coma 16 23.9 15 32.6
Confusion 2 2.9 3 6.5
Seizures 40 59.7 29 63.0Generalized 18 26.9 16 34.8Focal 22 32.8 13 28.2Bilateral pyramidal signs 28 41.7 18 39.1Papilledema 27 40.2 24 52.1Nuchal rigidity 22 32.8 12 26.0Isolated intracranialhypertension 5 7.4 8 17.3
TABLE 4. Hematologic and Cerebrospinal FluidFindings in Cerebral Venous Thrombosis
Group 1 Group 2(n=67) (n=46)
n % n %Hematologic
Anemia* 43 64.1 12 26.0
Leukocytosis 24 35.8 20 43.4
Increased erythrocytesedimentation ratet 26/47 55.3 12/41 29.2
Thrombocytosis 2 2.9 6 13.0
Cerebrospinal fluid
Normal 13/46 28.2 6/27 22.2
Increased openingpressure 19/46 41.3 15/27 55.5
Abnormal cytologicalexam 29/46 43.4 11/27 20.7
Hemorrhagic 11/46 23.9 9/27 33.3
*P=.00001, tP=.01.
better outcome (P=.01) and(P=.002).
a lower mortality rate
There were no differences between groups regardingsites of thrombosis within the cerebral venous system(Table 7).
DiscussionA wide variety of well-known conditions may cause or
predispose to CVT, and their relative importance mayvary in different areas of the world.9-14 In the presentstudy. 60% of cases were associated with pregnancy andpuerperium (ratio group 1/group 2, 1.5). This complica-tion is also common in India, with a prevalence of4.5/1000 obstetric admissions.2.15 In accordance with anobstetric CVT series,16 symptoms of CVT appeared inthe first 3 weeks after delivery in the majority of casesand, as in the Indian series, women who had homedeliveries and poor prenatal care were more oftenaffected. CVT should be suspected in any woman whodevelops neurological symptoms in the immediate post-partum period, since nearly 15% of our cases occurredin the first 2 days after a normal childbirth. CVToccurred 13 times more often during puerperium thanduring pregnancy. Although in the Indian population,multiparas are more often affected than primiparas, in aproportion of 4: 1,17 in our population this differencewas not so striking (1.8:1).
In this study, we found a high frequency (70%) ofparenchymal lesions (venous infarcts and intracerebralhemorrhages) that manifested as focal neurological signs,epileptic seizures, disorders of consciousness, intracranialhypertension, nuchal rigidity, and hemorrhagic CSF.These findings also explain the high mortality rate in ourwhole series (18.5%). This is in contrast with reports fromother countries18-20 and illustrates the great clinical andneuroradiological pleomorphism of this condition world-wide. Our series is characterized by a low frequency ofisolated intracranial hypertension and absence of Behcet'sdisease as a cause of CVT. Even when we consider thesevariations, there seem to be important differences be-
by guest on May 13, 2018
http://stroke.ahajournals.org/D
ownloaded from

Cantu and Barinagarrementeria Cerebral Venous Thrombosis 1883
TABLE 5. Neuroradiological Findings
Computed Tomographic Scan Magnetic Resonance Imaging
Group 1 Group 2 Group 1 Group 2(n=59) (n=36) (n=19) (n=20)
Findings n % n % n % n %
Normal 5 8.4 4 11.1 0 0 0 0
Signs of cerebral venous thrombosis 19 32.2* 13 36.1* 17 89.4 19 95
Parenchymal lesions
Nonhemorrhagic venous infarct 16 27.1 7 19.4 3 15.7 2 10
Hemorrhagic venous infarct 21 35.5 12 33.3 10 52.6 11 55
Intracerebral hemorrhage 6 10.1 5 13.8 2 10.5 4 20
Unilateral lesion 25 42.3 15 41.6 8 42.1 12 60
Bilateral lesions 18 30.5 9 25 7 36.8 5 25
*Delta sign, dense triangle, or empty delta sign.
tween CVT associated with pregnancy and puerperiumand that with nonobstetric causes. The clinical picture ofthe former featured a disease with sudden or acute onset,with a progressive course that tends to become stable orbegin to subside in a short time (5 to 10 days). Innonobstetric cases, the onset was insidious in about halfthe patients; the course could be progressive or not andtended to be stable after 10 days in >50% of patients.These findings suggest that, in obstetric cases, the patho-physiological process leading to venous occlusion developsfaster but is usually self-limited and resolves itself in a
shorter time. Further evidence for this is the shorterperiod between onset of symptoms and diagnosis in ob-stetric patients; however, it should be born in mind thatpuerperium represents an important clue for suspectingCVT.Another important difference was the high frequency
of anemia in obstetric patients, probably reflecting a
poor diet during pregnancy and/or blood loss duringdelivery. The high prevalence of anemia has beenrecognized in most obstetric series of CVT23 and de-serves further study to clarify its role in the pathogen-esis of this entity.
Traditionally, the most frequently postulated mecha-nism involved in CVT in obstetric patients is a hyper-coagulable state2122 associated with dehydration andanemia. However, other factors may play an important
TABLE 6. Final Outcome in 108 Cases of CerebralVenous Thrombosis
Group 1 Group 2(n=62)* (n =46)
n % n % P
Good outcome .01
Total recovery 31 50.0 24 52.1
Mild sequelae 19 30.6 3 6.5
Poor outcome
Severe sequelae 6 9.7 4 8.7
Death 6 9.7 15 32.6 .002
*Five patients who had good outcome received anticoagula-tion and were excluded from statistical analysis.
role, such as protein S deficiency, which is commonduring pregnancy and puerperium.23 25 Deficiency ofprotein S has been reported in previous cases of CVT inobstetric patients.11,26.27 The higher prevalence of extra-neural thrombosis in CVT associated with pregnancyand puerperium may represent the systemic repercus-sion of a hypercoagulable state.Although the disease was of similar severity in both
groups, the outcome was more favorable in obstetricpatients. Possibly, CVT in obstetric subjects is a morebenign entity than the one affecting other types ofpatients because of a more limited and transient occlu-sion, with rapid sinovenous recanalization by spontane-ous thrombolysis or development of collaterals.
TABLE 7. Site of Venous Occlusion in 113 Patients WithCerebral Venous Thrombosis
Group 1 Group 2(n=67) (n=46)
n % n %
SSS 60 89.5 45 97.8
22 32.8* 11 23.9*
LS 23 34.3 20 43.4
1 1.4* 1 2.1*DVS 17 25.3 10 21.7
4 7.4* 0 ...
CCV 13 19.4 14 30.4
SSS+LS 16 23.8 15 32.6
SSS+CCV 9 13.4 8 17.3
SSS+DVS 6 8.9 5 10.8
SSS+LS+DVS 4 5.9 2 4.3
SSS+CCV+DVS 2 2.9 2 4.3
SSS+CCV+LS 1 1.4 1 2.1
SSS+CCV+LS+DVS 0 ... 1 2.1
CCV+LS 1 1.4 0 ...
SSS indicates superior sagittal sinus; LS, lateral sinus; DVS,deep venous system; and CCV, cortical cerebral veins.
*Isolated venous occlusion involvement.
by guest on May 13, 2018
http://stroke.ahajournals.org/D
ownloaded from

1884 Stroke Vol 24, No 12 December 1993
Prognosis and treatment are the most controversialissues of cerebral venous thrombosis. Prognosis is quitevariable. The outcome can range from total recovery todeath. Since the introduction of MRI, an increasingnumber of patients with a benign course of CVT havebeen diagnosed.28'29 Conversely, the benefit of anticoag-ulation now appears well established.89 It would be ofparamount importance to be able to identify the benigncases that will recover completely whatever the treat-ment and the severe cases that would justify the risk ofanticoagulation. Based on the experience acquired atour institution, we do not recommend anticoagulationin patients without the factors associated with a badprognosis.30
AcknowledgmentWe are grateful to Dr Carlos Marquez for his assistance.
References1. Abercrombie J. Pathological and practical researches on diseases
of the brain and spinal cord. Edinburgh: 1828:83-85. Cited by:Donaldson JO, ed. Neurology of Pregnancy. Philadelphia, Pa: WBSaunders; 1978.
2. Bansal BC, Gupta RR, Prakash C. Stroke during pregnancy andpuerperium in young females below the age of 40 as a result ofcerebral venous/venous sinus thrombosis. Jpn Heart J. 1980;21:171-183.
3. Srinivasan K. Cerebral venous and arterial thrombosis in pregnancyand puerperium, a study of 135 patients. Angiology. 1983;34:733-746.
4. Estaniol B, Rodriguez A, Conte G, Aleman JM, Loyo M, Pizzuto J.Intracranial venous thrombosis in young women. Stroke. 1979;10:680- 684.
5. Vines FS, Davis DO. Clinical-radiological correlation in cerebralvenous occlusive disease. Radiology. 1971;98:9-22.
6. Kalbag RM. Cerebral venous thrombosis. In: Kapp JP, SchmidekHH, eds. The Cerebral Venous System and Its Disorders. Orlando,Fla: Grune and Stratton; 1986:527-529.
7. Zimmerman RD, Ernst RJ. Neuroimaging of cerebral venousthrombosis. Neuroimaging Clin North Am. 1992;2:463-485.
8. Einhaupl HM, Villringer A, Meister W, Mehraein S, Garner C,Pellkofer M, Haberl RL, Pfister H-W, Schmiedek P. Heparintreatment in sinus venous thrombosis. Lancet. 1991;338:597-600.
9. Ameri A, Bousser M-G. Cerebral venous thrombosis. Neurol Clin.1992; 10:87-1 11.
10. Krayenbuhl H. Cerebral venous and sinus thrombosis. Clin Neu-rosurg. 1967;14:1-24.
11. Enevoldson TP, Ross-Russell RW. Cerebral venous thrombosis:new causes for an old syndrome? Q J Med. 1990:77:1255-1275.
12. Lefkowitz D. Cortical thrombophlebitis and sinovenous disease.In: Vinken PJ, Bruyn GW, Klawans HL, eds. Handbook of ClinicalNeurology, Vol 10: Vascular Diseases, Part II. New York/Amsterdam: Elsevier Science Publishing Co Inc. 1989:395-423.
13. Averback P. Primary cerebral venous thrombosis in young adults:the diverse manifestations of an underrecognized disease. AnnNeurol. 1978;3:81-86.
14. Banerjee AK, Varma M, Vasista RK, Chopra JS. Cerebrovasculardisease in North-West India: a study of necropsy material. J VelurolNeurosurg Psychiatry. 1989;52:512-515.
15. Srinivasan K. Puerperal cerebral venous and arterial thrombosis.Semin Neurol 1988;8:222-225.
16. Dibakdsib JO. Cerebrovascular disease. In: Donaldson JO, ed.Neurology of Pregnancy. Philadelphia. Pa: WB Saunders: 1978:135-144.
17. Chopra JS, Banerjee AK. Primary intracranial sinovenousocclusions in youth and pregnancy. In: Vinken PJ, Bruyn GW,Klawans HL, eds. Handbook of Clinical Neurology, Vol 10: VascularDiseases, Part II. New York/Amsterdam: Elsevier Science Pub-lishing Co Inc; 1989:425-452.
18. Bousser M-G, Chiras J, Bories J, Castaigne P. Cerebral venousthrombosis: a review of 38 cases. Stroke. 1985;16:199-221.
19. Thron A, Wessel K, Linden D, Schroth G, Dichgans J. Superiorsagittal sinus thrombosis: neuroradiological evaluation and clinicalfindings. J Neurol. 1986;233:283 -288.
20. Wechsler B, Vidhaihet M, Piette JC, Bousser MG, Dell Isola B,Bletry 0, Godeau P. Cerebral venous thrombosis in Behget'sdisease: clinical study and long-term follow-up of 25 cases. NVeu-rology. 1992;42:614-618.
21. Strauss HS, Diamond LK. Elevation of factor VIII duringpregnancy in normal persons and in a patient with von Wille-brand's disease. N Engl J Med. 1963;269:1251-1252.
22. Inglis TCM, Stuart J, George AJ, Davies AJ. Haemostatic andrheological changes in normal pregnancy and pre-eclampsia. Br JHaematol. 1982;50:461-465.
23. Comp PC, Thurnau GR, Welsh J. Esmon CT. Functional andimmunologic protein S levels are decreased during pregnancy.Blood. 1986;68:881- 885.
24. Boerger LM, Morris PC, Thurnau GR, Esmon CT, Comp PC. Oralcontraceptives and gender affect protein S status. Blood. 1987;69:692-694.
25. Mackinnon S, Walker ID, Davidson JF, Walker JJ. Plasma fibri-nolysis during and after normal childbirth. Br J Haematol. 1987;65:339-342.
26. Cros D, Comp PC, Beltran G, Gum G. Superior sagittal sinusthrombosis in a patient with protein S deficiency. Stroke. 1990:21:633- 636.
27. Moreb J, Kitchens CS. Acquired functional protein S deficiency,cerebral venous thrombosis and coumarin skin necrosis in asso-ciation with antiphospholipid syndrome: report of two cases. Am JMed. 1989;87:207-210.
28. Hulcelle PJ, Dooms GC, Mathurin P, Cornelis G. MRI assessmentof unsuspected dural sinus thrombosis. Neuroradiology. 1989:31:217-221.
29. Sze G. Simmons B, Krol G, Walker R, Zimmerman RD, DeckMDF. Dural sinus thrombosis: verification with spin echo tech-niques. AJNR Am J Neuroradiol. 1988;9:679-686.
30. Barinagarrementeria F, Cantu C, Arredondo H. Aseptic cerebralvenous thrombosis: proposed prognostic scale. J Stroke CerebrovascDis. 1992;2:34-39.
by guest on May 13, 2018
http://stroke.ahajournals.org/D
ownloaded from

C Cantú and F Barinagarrementeriacases.
Cerebral venous thrombosis associated with pregnancy and puerperium. Review of 67
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 1993 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/01.STR.24.12.1880
1993;24:1880-1884Stroke.
http://stroke.ahajournals.org/content/24/12/1880World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer process is available in the
Request Permissions in the middle column of the Web page under Services. Further information about thisOnce the online version of the published article for which permission is being requested is located, click
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Strokein Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on May 13, 2018
http://stroke.ahajournals.org/D
ownloaded from