
Central granular cell odontogenic tumor: The first ... · Central granular cell odontogenic tumor:...
5
CASE REPORT Central granular cell odontogenic tumor: The first reported case in Oriental people and literature review Chien-Ta Chiang a , Kwang-Yu Hu b , Chien-Chen Tsai a, * a Department of Anatomical Pathology, Far Eastern Memorial Hospital, Taipei, Taiwan b Department of Oral Maxillofacial Surgery, Far Eastern Memorial Hospital, Taipei, Taiwan Received 27 January 2012; received in revised form 2 April 2012; accepted 25 April 2012 KEYWORDS central granular cell odontogenic tumor; granular cells; odontogenic tumors The central granular cell odontogenic tumor (CGCOT) is a rare odontogenic neoplasm, usually occurring in the mandible of middle-aged women. Previous studies have reported only 34 cases, all of whom were white or black individuals. The present study reports an additional case of CGCOT, occurring in the posterior mandible of a 69-year-old Taiwanese man. To the authors’ knowledge, this is the first reported case in Oriental people. The odontogenic epithe- lium exhibited strong positive immunoreactivity for pan-cytokeratin, and focal weak staining for bcl-2. The granular cells showed strong positivity for vimentin and a1-antichymotrypsin, and focal weak staining for carcinoembryonic antigen (CEA), neuron-specific enolase (NSE), and CD68. These features indicated a mesenchymal origin and possible histiocytic lineage for the granular cells. This study also presents a literature review and describes immunohisto- chemical features of the tumor. Copyright ª 2012, Elsevier Taiwan LLC & Formosan Medical Association. All rights reserved. Introduction Central granular cell odontogenic tumor (CGCOT) is a rare odontogenic benign neoplasm comprising varying amounts of large eosinophilic granular cells and an apparently inactive odontogenic epithelium. There have been 34 cases of CGCOT reported, using varied terminology. 1e21 The recent classification of odontogenic tumors of the World Health Organization does not include CGCOT; however, many authors regard this type of tumor as a distinct entity, recently naming it CGCOT. 13e18,20 CGCOT tends to surface in the mandible, occurring especially in women oplder than 50 years. Previously re- ported cases all regarded white or black people. The present study reports the first case of CGCOT occurring in an Oriental person. Conflicts of interest: The authors have no conflicts of interest relevant to this article. * Corresponding author. No. 21, Section 2, Nanya South Road, Banciao District, New Taipei City 220, Taiwan. E-mail address: [email protected] (C.-C. Tsai). 0929-6646/$ - see front matter Copyright ª 2012, Elsevier Taiwan LLC & Formosan Medical Association. All rights reserved. http://dx.doi.org/10.1016/j.jfma.2012.04.011 Available online at www.sciencedirect.com journal homepage: www.jfma-online.com Journal of the Formosan Medical Association (2014) 113, 321e325
Transcript of Central granular cell odontogenic tumor: The first ... · Central granular cell odontogenic tumor:...
Journal of the Formosan Medical Association (2014) 113, 321e325
Available online at www.sciencedirect.com
journal homepage: www.jfma-onl ine.com
CASE REPORT
Central granular cell odontogenic tumor:The first reported case in Oriental peopleand literature review
Chien-Ta Chiang a, Kwang-Yu Hu b, Chien-Chen Tsai a,*
aDepartment of Anatomical Pathology, Far Eastern Memorial Hospital, Taipei, TaiwanbDepartment of Oral Maxillofacial Surgery, Far Eastern Memorial Hospital, Taipei, Taiwan
Received 27 January 2012; received in revised form 2 April 2012; accepted 25 April 2012
KEYWORDScentral granular cellodontogenic tumor;
granular cells;odontogenic tumors
Conflicts of interest: The authorsrelevant to this article.* Corresponding author. No. 21, Se
Banciao District, New Taipei City 220,E-mail address: zerosedi@hotmail.
0929-6646/$ - see front matter Copyrhttp://dx.doi.org/10.1016/j.jfma.201
The central granular cell odontogenic tumor (CGCOT) is a rare odontogenic neoplasm, usuallyoccurring in the mandible of middle-aged women. Previous studies have reported only 34cases, all of whom were white or black individuals. The present study reports an additionalcase of CGCOT, occurring in the posterior mandible of a 69-year-old Taiwanese man. To theauthors’ knowledge, this is the first reported case in Oriental people. The odontogenic epithe-lium exhibited strong positive immunoreactivity for pan-cytokeratin, and focal weak stainingfor bcl-2. The granular cells showed strong positivity for vimentin and a1-antichymotrypsin,and focal weak staining for carcinoembryonic antigen (CEA), neuron-specific enolase (NSE),and CD68. These features indicated a mesenchymal origin and possible histiocytic lineagefor the granular cells. This study also presents a literature review and describes immunohisto-chemical features of the tumor.Copyright ª 2012, Elsevier Taiwan LLC & Formosan Medical Association. All rights reserved.
Introduction
Central granular cell odontogenic tumor (CGCOT) is a rareodontogenic benign neoplasm comprising varying amountsof large eosinophilic granular cells and an apparently
have no conflicts of interest
ction 2, Nanya South Road,Taiwan.com (C.-C. Tsai).
ight ª 2012, Elsevier Taiwan LLC2.04.011
inactive odontogenic epithelium. There have been 34 casesof CGCOT reported, using varied terminology.1e21 Therecent classification of odontogenic tumors of the WorldHealth Organization does not include CGCOT; however,many authors regard this type of tumor as a distinct entity,recently naming it CGCOT.13e18,20
CGCOT tends to surface in the mandible, occurringespecially in women oplder than 50 years. Previously re-ported cases all regarded white or black people. Thepresent study reports the first case of CGCOT occurring inan Oriental person.
& Formosan Medical Association. All rights reserved.
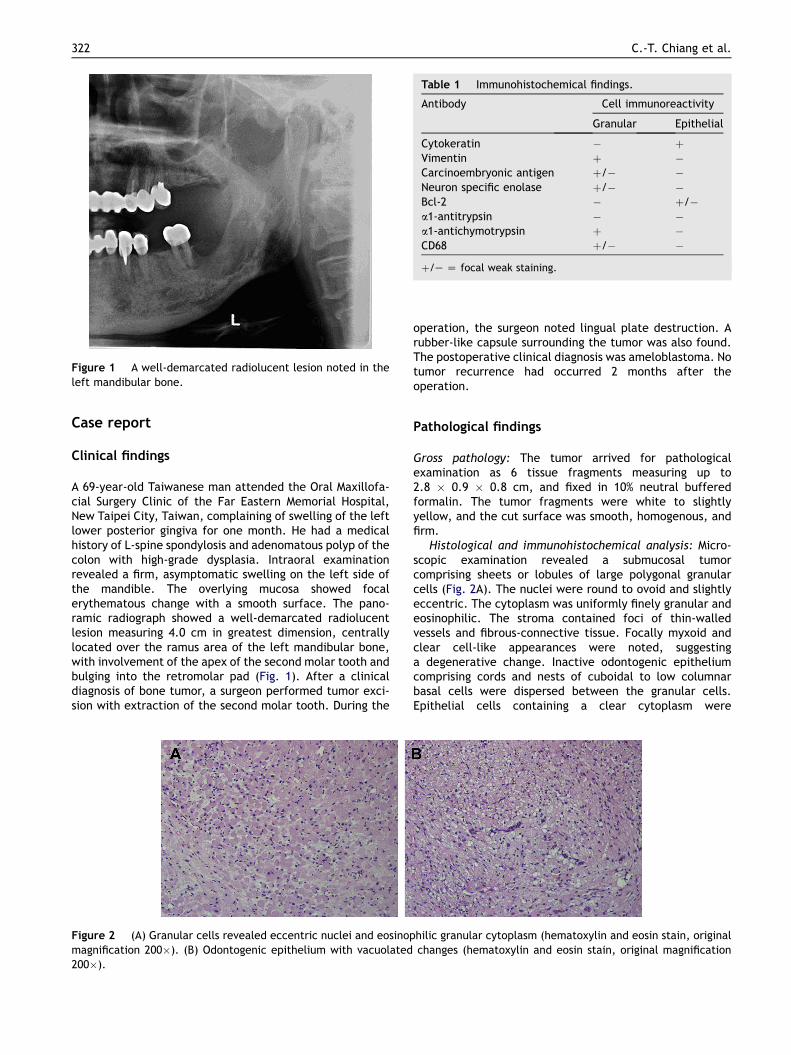
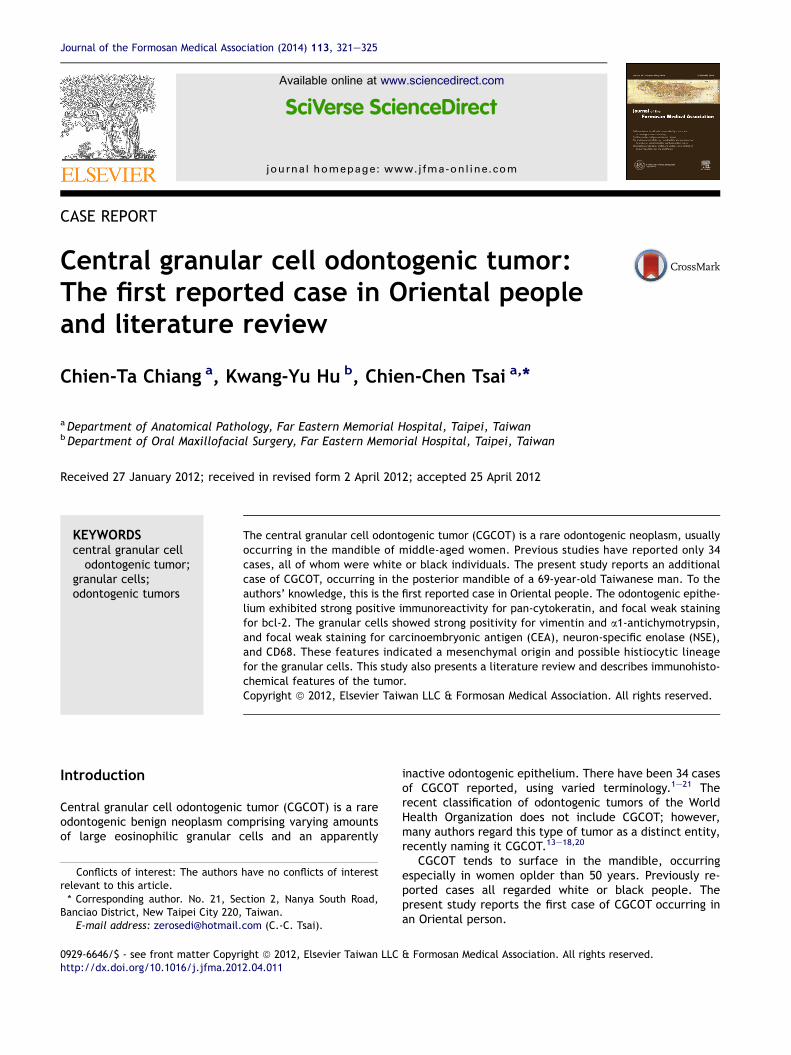
Figure 1 A well-demarcated radiolucent lesion noted in theleft mandibular bone.
Table 1 Immunohistochemical findings.
Antibody Cell immunoreactivity
Granular Epithelial
Cytokeratin � þVimentin þ �Carcinoembryonic antigen þ/� �Neuron specific enolase þ/� �Bcl-2 � þ/�a1-antitrypsin � �a1-antichymotrypsin þ �CD68 þ/� �þ/e Z focal weak staining.
322 C.-T. Chiang et al.
Case report
Clinical findings
A 69-year-old Taiwanese man attended the Oral Maxillofa-cial Surgery Clinic of the Far Eastern Memorial Hospital,New Taipei City, Taiwan, complaining of swelling of the leftlower posterior gingiva for one month. He had a medicalhistory of L-spine spondylosis and adenomatous polyp of thecolon with high-grade dysplasia. Intraoral examinationrevealed a firm, asymptomatic swelling on the left side ofthe mandible. The overlying mucosa showed focalerythematous change with a smooth surface. The pano-ramic radiograph showed a well-demarcated radiolucentlesion measuring 4.0 cm in greatest dimension, centrallylocated over the ramus area of the left mandibular bone,with involvement of the apex of the second molar tooth andbulging into the retromolar pad (Fig. 1). After a clinicaldiagnosis of bone tumor, a surgeon performed tumor exci-sion with extraction of the second molar tooth. During the
Figure 2 (A) Granular cells revealed eccentric nuclei and eosinopmagnification 200�). (B) Odontogenic epithelium with vacuolated200�).
operation, the surgeon noted lingual plate destruction. Arubber-like capsule surrounding the tumor was also found.The postoperative clinical diagnosis was ameloblastoma. Notumor recurrence had occurred 2 months after theoperation.
Pathological findings
Gross pathology: The tumor arrived for pathologicalexamination as 6 tissue fragments measuring up to2.8 � 0.9 � 0.8 cm, and fixed in 10% neutral bufferedformalin. The tumor fragments were white to slightlyyellow, and the cut surface was smooth, homogenous, andfirm.
Histological and immunohistochemical analysis: Micro-scopic examination revealed a submucosal tumorcomprising sheets or lobules of large polygonal granularcells (Fig. 2A). The nuclei were round to ovoid and slightlyeccentric. The cytoplasm was uniformly finely granular andeosinophilic. The stroma contained foci of thin-walledvessels and fibrous-connective tissue. Focally myxoid andclear cell-like appearances were noted, suggestinga degenerative change. Inactive odontogenic epitheliumcomprising cords and nests of cuboidal to low columnarbasal cells were dispersed between the granular cells.Epithelial cells containing a clear cytoplasm were
hilic granular cytoplasm (hematoxylin and eosin stain, originalchanges (hematoxylin and eosin stain, original magnification
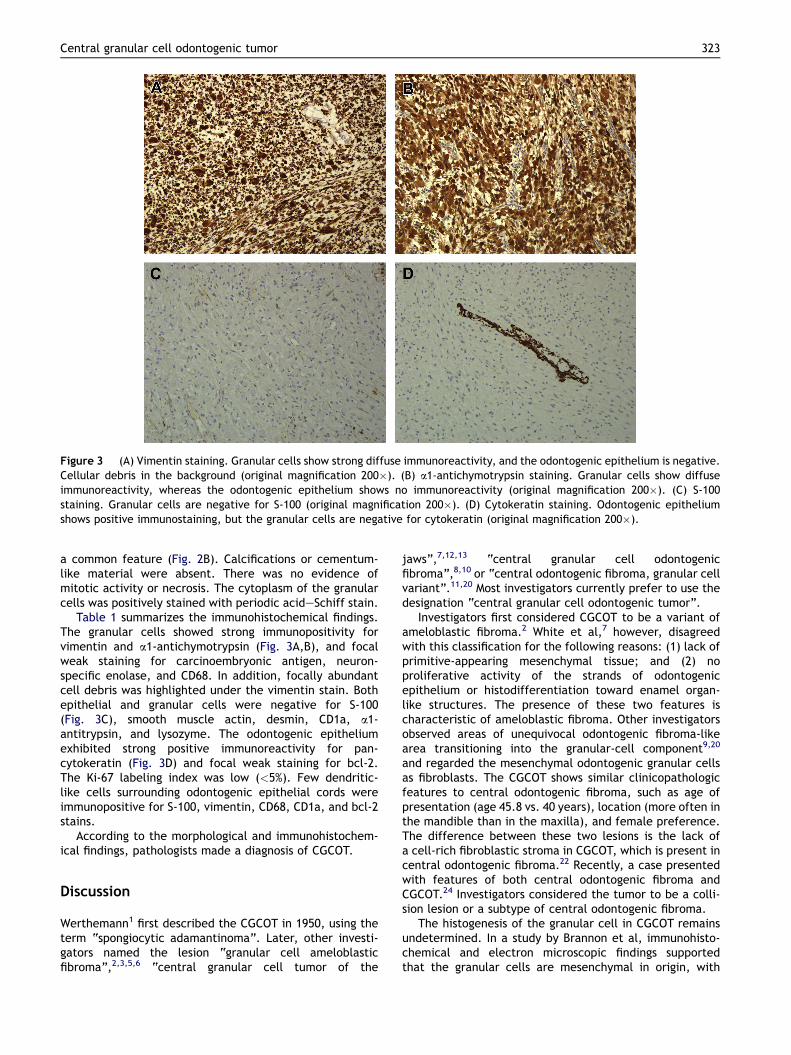
Figure 3 (A) Vimentin staining. Granular cells show strong diffuse immunoreactivity, and the odontogenic epithelium is negative.Cellular debris in the background (original magnification 200�). (B) a1-antichymotrypsin staining. Granular cells show diffuseimmunoreactivity, whereas the odontogenic epithelium shows no immunoreactivity (original magnification 200�). (C) S-100staining. Granular cells are negative for S-100 (original magnification 200�). (D) Cytokeratin staining. Odontogenic epitheliumshows positive immunostaining, but the granular cells are negative for cytokeratin (original magnification 200�).
Central granular cell odontogenic tumor 323
a common feature (Fig. 2B). Calcifications or cementum-like material were absent. There was no evidence ofmitotic activity or necrosis. The cytoplasm of the granularcells was positively stained with periodic acideSchiff stain.
Table 1 summarizes the immunohistochemical findings.The granular cells showed strong immunopositivity forvimentin and a1-antichymotrypsin (Fig. 3A,B), and focalweak staining for carcinoembryonic antigen, neuron-specific enolase, and CD68. In addition, focally abundantcell debris was highlighted under the vimentin stain. Bothepithelial and granular cells were negative for S-100(Fig. 3C), smooth muscle actin, desmin, CD1a, a1-antitrypsin, and lysozyme. The odontogenic epitheliumexhibited strong positive immunoreactivity for pan-cytokeratin (Fig. 3D) and focal weak staining for bcl-2.The Ki-67 labeling index was low (<5%). Few dendritic-like cells surrounding odontogenic epithelial cords wereimmunopositive for S-100, vimentin, CD68, CD1a, and bcl-2stains.
According to the morphological and immunohistochem-ical findings, pathologists made a diagnosis of CGCOT.
Discussion
Werthemann1 first described the CGCOT in 1950, using theterm “spongiocytic adamantinoma”. Later, other investi-gators named the lesion “granular cell ameloblasticfibroma”,2,3,5,6 “central granular cell tumor of the
jaws”,7,12,13 “central granular cell odontogenicfibroma”,8,10 or “central odontogenic fibroma, granular cellvariant”.11,20 Most investigators currently prefer to use thedesignation “central granular cell odontogenic tumor”.
Investigators first considered CGCOT to be a variant ofameloblastic fibroma.2 White et al,7 however, disagreedwith this classification for the following reasons: (1) lack ofprimitive-appearing mesenchymal tissue; and (2) noproliferative activity of the strands of odontogenicepithelium or histodifferentiation toward enamel organ-like structures. The presence of these two features ischaracteristic of ameloblastic fibroma. Other investigatorsobserved areas of unequivocal odontogenic fibroma-likearea transitioning into the granular-cell component9,20
and regarded the mesenchymal odontogenic granular cellsas fibroblasts. The CGCOT shows similar clinicopathologicfeatures to central odontogenic fibroma, such as age ofpresentation (age 45.8 vs. 40 years), location (more often inthe mandible than in the maxilla), and female preference.The difference between these two lesions is the lack ofa cell-rich fibroblastic stroma in CGCOT, which is present incentral odontogenic fibroma.22 Recently, a case presentedwith features of both central odontogenic fibroma andCGCOT.24 Investigators considered the tumor to be a colli-sion lesion or a subtype of central odontogenic fibroma.
The histogenesis of the granular cell in CGCOT remainsundetermined. In a study by Brannon et al, immunohisto-chemical and electron microscopic findings supportedthat the granular cells are mesenchymal in origin, with

Table 2 Clinicopathologic details of reported cases ofcentral granular cell odontogenic tumor.
Total casenumber
35
Age Mean, 45.8 y (range, 16e77 y)Sex Female, 25; male, 9; unknown, 1Race White, 13; Black, 9; Oriental, 1;
unknown, 12Tumor site Mandible, 25; maxilla, 8;
unknown, 2Laterality ofthe tumors
Left, 16; right, 9; side unknown, 10
324 C.-T. Chiang et al.
a potential for histiocytic or fibroblastic differentiation.17
Some reports noted immunoreactivity for histiocyticmarkers, such as a-1-antitrypsin (AAT),10,13,17 a-1-antichymotrypsin (AACT),13,17 lysozyme,13,17 CD68,15,17
and HLA-DR.12 However, prior studies have also observedAACT, AAT, and CD68 immunoreactivity in granular cellameloblastomas and other nonmacrophage-derivedtumors.13,15 Granular cell OKT6 (CD1) positivity in one re-ported case12 suggested a Langerhans cell origin, but laterstudies (including the current case) demonstrated negativeimmunoreactivity for CD1a.17,19 At an ultrastructural level,many granular cells contained lysosome-like particles.Initially, investigators considered these particles identicalto those observed in the granular cell “myoblastoma”(granular cell tumor),7 but currently do not regard them asspecific for any particular cell line.15
To date, studies have reported 35 cases of CGCOT,including the current case (Table 2). The age range was 16to 77 years, with a mean of 45.8 years. The sex was knownin 34 cases; 25 (73.5%) cases were of women. The race wasknown in 23 cases: 13 (56%) white and nine (39%) blackpeople, and one (4%) Oriental person (the current case).
Table 3 Differential diagnosis of central granular cell odontoge
Differential diagnosis Clinical appearance H
Central granular cellodontogenic tumor
Female predominance,more common in mandiblethan maxilla
Go
Granular cell tumor Most common in tongue Pe
Granular cell ameloblastoma Most common in mandible Gt
Congenital epulis of thenewborn
Newborns, more commonin maxilla than mandible
Gve
Peripheral granular cellodontogenic fibroma
Arising in gingiva S
Central odontogenic fibroma,epithelium-richtype (WHO-type)
Female predominance,more common in mandiblethan maxilla
Ctie
The most common site was the premolar or molar region.The location of the tumor tended to be the mandible (25cases, 75%), or to a lesser extent, the maxilla (8 cases,24%). For cases in which the investigators knew the later-ality, there was a slight preference for tumor growth on theleft side (16 cases, 64%), as opposed to the right side (ninecases, 36%). However, this tendency occurred in themandible (left: 13, right: six) but not in the maxilla (left:three, right: three). In the current case, the tumor wasalmost entirely composed of granular cells and odonto-genic epithelium strands, and therefore, did not presentwith the typical solid sheet of spindle fibroblastic cellcharacteristic of central odontogenic fibroma. Of theimmunohistochemical markers for histiocyte, the granularcells showed positive immunoreactivity for a1-antichymotrypsin, focal equivocal staining for CD68 andlysozyme, but negative immunoreactivity for a1-anti-trypsin. The current case is the first reported case ofCGCOT occurring in Oriental people, although one previousstudy described a Japanese woman having peripheralGCOT.23 Peripheral GCOT is rarer than the central type,with only 4 cases reported since 1976.23,25 These tumorssurface on gingival tissue without a centrally located bonelesion, in contrast to CGCOT, which is always intraosseous.The morphologic appearance and immunohistochemicalresults were similar to those observed in CGCOT.17 In ourcase, although the tumor involved the regional soft tissue,it was still appropriate to classify it as a central rather thanperipheral type.
The differential diagnosis of granular cells in the oralcavity includes granular cell tumor, granular cell amelo-blastoma, and congenital epulis of the newborn (Table 3).10
Morphologically, granular cells of granular cell tumors showsimilarities to those of CGCOT. However, strong immuno-reactivity for the S-100 protein in granular cells of granularcell tumors can easily distinguish them from CGCOTcells, which are consistently negative for the S-100 protein.Granular cell ameloblastoma is a variant of
nic tumor.
istopathologic feature Immunoreactivity
ranular cell withdontogenic epithelium
Granular cell:Cytokeratin(�)S-100(�)Odontogenic epithelium:cytokeratin(þ)
lump granularosinophilic cell
S-100(þ)
ranular cell replacinghe stellate reticulum cells
Cytokeratin(þ)S-100(�)
ranular cell with prominentasculature, scatter odontogenicpithelium
Cytokeratin(�)S-100(�)
imilar as CGCOT Similar to CGCOT
ellular fibroblastic connectiveissue, islands or strands ofnactive-looking odontogenicpithelium
Cytokeratin(�)S-100(�)

Central granular cell odontogenic tumor 325
ameloblastoma, which shows changes within the epithelialislands, with granular cells replacing the stellatereticulum-like cells. These granular cells are immuno-positive for cytokeratin, but immunoreactivity for S-100protein remains inconclusive.9 Congenital epulis of thenewborn, also called congenital granular cell epulis, occursmainly in the alveolar ridges of newborns. The tumor cellsare immunopositive for vimentin and neuron specificenolase, but demonstrate no immunoreactivity for cyto-keratin or S-100 protein. The histological and immunohis-tochemical features of congenital epulis of newborns aresimilar to these of CGCOT, but the differing ages ofpatients may be helpful in distinguishing between thesetwo tumors.
The prognosis of CGCOT is good. All reported casesreceived treatment through excision and/or curettage.Brannon et al reported one case that recurred 13 yearsafter treatment.17 Another study reported a case of GCOTexhibiting clinicopathological features of malignancy.18
The malignant tumor cells exhibited nuclear pleomor-phism, prominent nucleoli, and mitotic figures, withextensive invasion of the oral and respiratory mucosa andthe adjacent soft tissues. Immunochemical findings weresimilar to those from other previously reported cases,except for the observation of a high Ki 67 index (21%) ingranular spindle cells. The patient experienced tumorrecurrence 16 months after radical surgery. This caseindicated the potential of CGCOT for malignancy; if clinicaland histopathological examinations identify aggressivebehavior, more aggressive treatment and longer clinicalfollow-up is necessary.
References
1. Werthemann A. Spongiocytic adamantinoma. Oncologia 1950;3:193e207.
2. Couch RD, Morris EE, Vellios F. Granular cell ameloblasticfibroma: report of 2 cases in adults, with observations on itssimilarity to congenital epulis. Am J Clin Pathol 1962;37:398e404.
3. Waldron CA, Thompson CW, Conner WA. Granular-cell amelo-blastic fibroma: report of two cases. Oral Surg Oral Med OralPathol 1963;16:1202e13.
4. Dalforno S, Donna A. Odontoma molle (fibroma ameloblastico)con stroma di cellule granulose. Cancro 1970;23:61e6.
5. Gorlin RJ, Goldman HM. Thoma’s oral pathology. 6th ed. StLouis: Mosby; 1970. p. 495.
6. Regezi JA, Kerr DA, Courtney RM. Odontogenic tumors: analysisof 706 cases. J Oral Surg 1978;36:771e8.
7. White DK, Chen SY, Hartman KS, Miller AS, Gomez LF. Centralgranular-cell tumor of the jaws (the so-call granular cellameloblastic fibroma). Oral Surg Oral Med Oral Pathol 1978;45:396e405.
8. Vincent SD, Hammond HL, Ellis GL, Juhlin JP. Central granularcell odontogenic fibroma. Oral Surg Oral Med Oral Pathol 1987;63:715e21.
9. Ruhl GH, Akuamoa-Boateng E. Granular cells in odontogenicand non-odontogenic tumours. Virchows Arch A Pathol AnatHistopathol 1989;415:403e9.
10. Mirchandani R, Sciubba JJ, Mir R. Granular cell lesions of thejaws and oral cavity: a clinicopathologic, immunohistochem-ical, and ultrastructural study. J Oral Maxillofac Surg 1989;47:1248e55.
11. Shiro BC, Jacoway JR, Mirmiran SA, McGuirt Jr WF, Siegal GP.Central odontogenic fibroma, granular cell variant: a casereport with S-100 immunohistochemistry and a review ofthe ;literature. Oral Surg Oral Med Oral Pathol 1989;67:725e30.
12. Chen SY. Central granular cell tumor of the jaw: an electronmicroscopic and immunohistochemical study. Oral Surg OralMed Oral Pathol 1991;72:75e81.
13. Yih WY, Thompson C, Meshul CK, Bartley MH. Central odonto-genic granular cell tumor of the jaw: report of case andimmunohistochemical and electron microscopic study. J OralMaxillofac Surg 1995;53:453e9.
14. Gesek Jr DJ, Adrian JC, Reid EN. Central granular cell odon-togenic tumor: a case report including light microscopy,immunohistochemistry, and literature review. J Oral Max-illofac Surg 1995;53:945e9.
15. De Sousa SO, de Araujo NS, Melhado RM, de Araujo VC. Centralodontogenic granular cell tumor: immunohistochemical studyof two cases. J Oral Maxillofac Surg 1998;56:787e91.
16. Ardekian L, Manor R, Gaspar R, Laufer D. Central granular cellodontogenic tumor: case report and review of literature. JOral Maxillofac Surg 1998;56:1343e5.
17. Brannon RB, Goode RK, Eversole LR, Carr RF. The centralgranular cell odontogenic tumor: report of 5 new cases. OralSurg Oral Med Oral Pathol Oral Radiol Endod 2002;94:614e21.
18. Piattelli A, Rubini C, Goteri G, Fioroni M, Maiorano E. Centralgranular cell odontogenic tumour: report of the first malignantcase and review of the literature. Oral Oncol 2003;39:78e82.
19. Meer S, Altini M, Coleman H, Daya N. Central granular cellodontogenic tumor: immunohistochemistry and ultrastructure.Am J Otol 2004;25:73e8.
20. Reichart PA, Philipsen HP, Moegelin A, Thalmann U. Centralodontogenic fibroma, granular cell variant. Oral Surg Oral MedOral Pathol 2006;42:5e9.
21. Gomes CC, Naves MD, Pereira MV, Silva LM, Mesquita RA,Gomez RS. Granular cell odontogenic tumour: case report andreview of literature. Oral Surg Oral Med Oral Pathol 2006;42:277e80.
22. Gardner DG. Central odontogenic fibroma current concepts.J Oral Pathol Med 1996;25:556e61.
23. Takeda Y. Granular cell ameloblastic fibroma, ultrastructureand histogenesis. Int J Oral Maxillofac Surg 1986;15:190e5.
24. Lotay HS, Kalmar J, DeLeeuw K. Central odontogenic fibromawith features of central granular cell odontogenic tumor. OralSurg Oral Med Oral Pathol Oral Radiol Endod 2010;109:e63e6.
25. Daley TD, Wysocki GP. Peripheral odontogenic fibroma. OralSurg Oral Med Oral Pathol 1994;78:329e36.


















