
CDR JOHN P WEI, USN MC MD 4th Medical Battalion, 4th MLG BSRF-12 ABDOMINAL TRAUMA.
30
CDR JOHN P WEI, USN MC MD 4th Medical Battalion, 4th MLG BSRF-12 ABDOMINAL TRAUMA
-
Upload
isabella-eaton -
Category
Documents
-
view
218 -
download
4
Transcript of CDR JOHN P WEI, USN MC MD 4th Medical Battalion, 4th MLG BSRF-12 ABDOMINAL TRAUMA.
CDR JOHN P WEI, USN MC MD4th Medical Battalion, 4th MLGBSRF-12
ABDOMINAL TRAUMA
ABDOMINAL TRAUMA
ABDOMINAL TRAUMA
•Types of abdominal trauma•Anatomical regions of the
abdomen•Initial care and diagnosis•Evaluation of patient with blunt
and penetrating trauma•Specific organ trauma•Surgery for injuries
BLUNT ABDOMINAL TRAUMA
Common causes of injury
• motor vehicle accidents• fall from heights• explosive blast injuries• physical assault
BLUNT ABDOMINAL TRAUMA
• Solid organ injuries including liver, spleen, kidneys, pancreas
• Rupture of hollow viscus including small and large intestine, stomach, esophagus, and bladder
• Vascular injuries• Bony fractures of pelvis and lumbar
spine
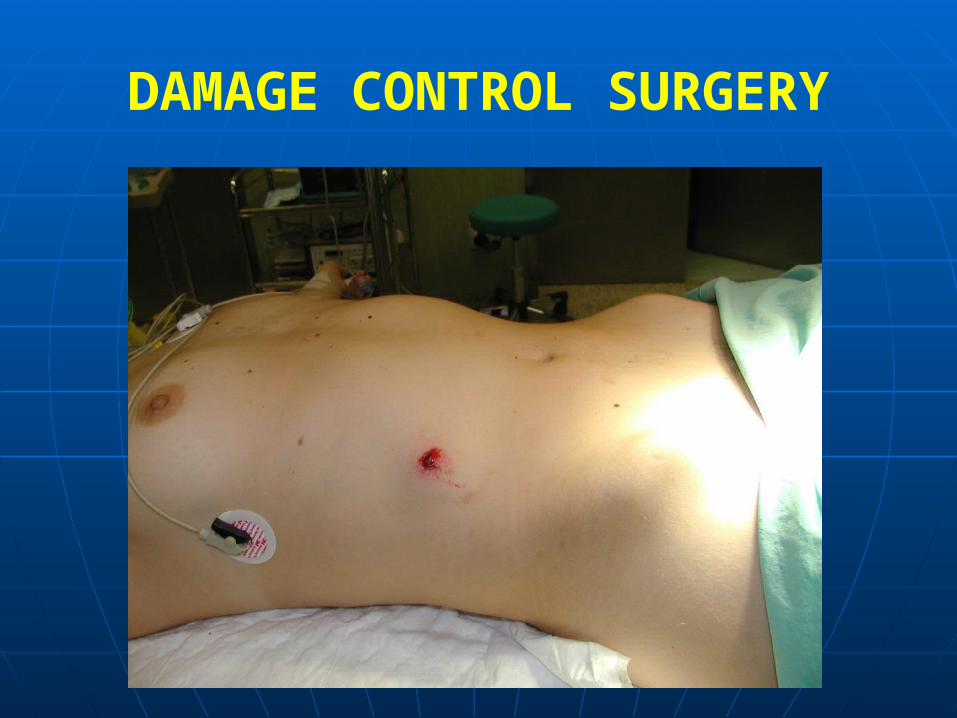
PENETRATING ABDOMINAL TRAUMA
• Mechanism of wounding and organ damage
• Stab wounds with knife or other instruments
• Gunshot wounds• Explosive injury with shrapnel or
secondary projectiles
PENETRATING ABDOMINAL TRAUMA
• Small and large intestine most commonly injured
• Lacerations of solid organs• Vascular injuries• Trajectory of penetrating instrument
and objects in its way
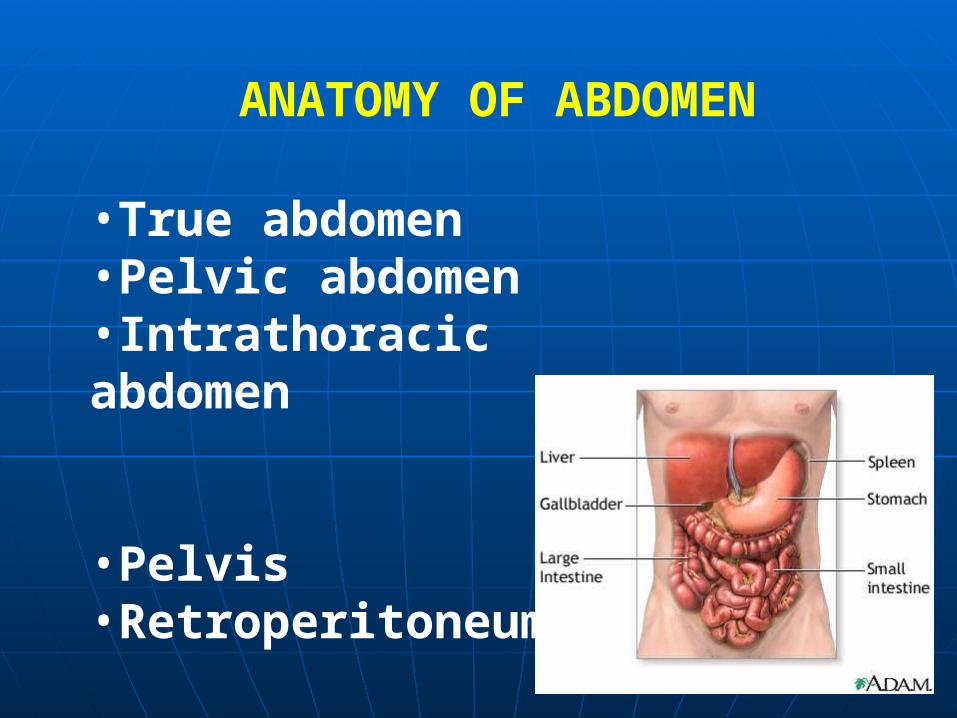
ANATOMY OF ABDOMEN
•True abdomen•Pelvic abdomen•Intrathoracic abdomen •Pelvis•Retroperitoneum
EVALUATION AND DIAGNOSISOF ABDOMINAL TRAUMA
EVALUATION AND DIAGNOSISOF ABDOMINAL TRAUMA
•Airway, Breathing, Circulation•History of injury and mechanism•Physical examination and vital signs•Radiologic studies•Laboratory testing
Resuscitation & management priorities of major abdominal trauma:
• Control airway and breathing
• Stabilize circulation with volume infusion or blood
• Hemorrhage control
• Nasogastric tube and urinary catheter if no pelvic fracture
Resuscitation & management priorities of major abdominal trauma:
• Control airway and breathing
• Stabilize circulation with volume infusion or blood
• Hemorrhage control
• Nasogastric tube and urinary catheter if no pelvic fracture
EVALUATION AND DIAGNOSIS OF ABDOMINAL TRAUMA
•HISTORY Blunt abdominal trauma
Penetrating abdominal trauma
•PHYSICAL EXAMINATION General physical examination Examination of the abdomen
•HISTORY Blunt abdominal trauma
Penetrating abdominal trauma
•PHYSICAL EXAMINATION General physical examination Examination of the abdomen
EVALUATION AND DIAGNOSISOF ABDOMINAL TRAUMA
Laboratory blood tests
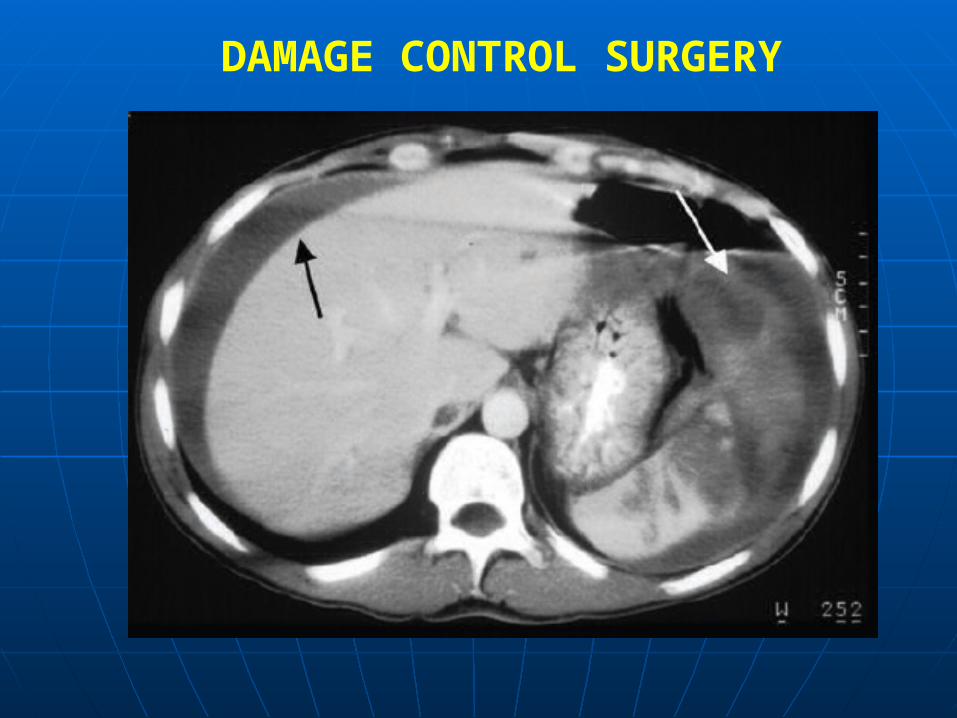
Urinalysis Radiological Studies (Plain abdominal X-ray, CXR) Peritoneal lavage (DPL) FAST U/S of abdomen CT scan of abdomen
Laboratory blood tests
Urinalysis Radiological Studies (Plain abdominal X-ray, CXR) Peritoneal lavage (DPL) FAST U/S of abdomen CT scan of abdomen
EVALUATION AND DIAGNOSISOF ABDOMINAL TRAUMA
Peritonitis Hypotensive shock Evisceration of viscus Positive diagnostic (DPL) Determination of finding on FAST or CAT scan
Peritonitis Hypotensive shock Evisceration of viscus Positive diagnostic (DPL) Determination of finding on FAST or CAT scan
INDICATIONS FOR EMERGENT SURGERY
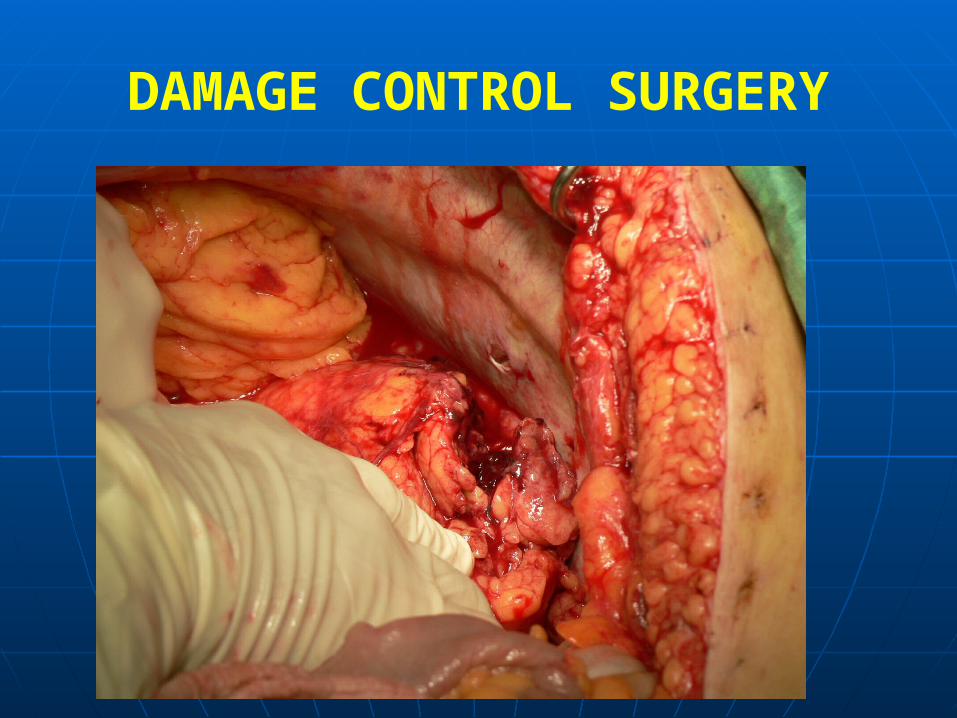
DAMAGE CONTROL SURGERY
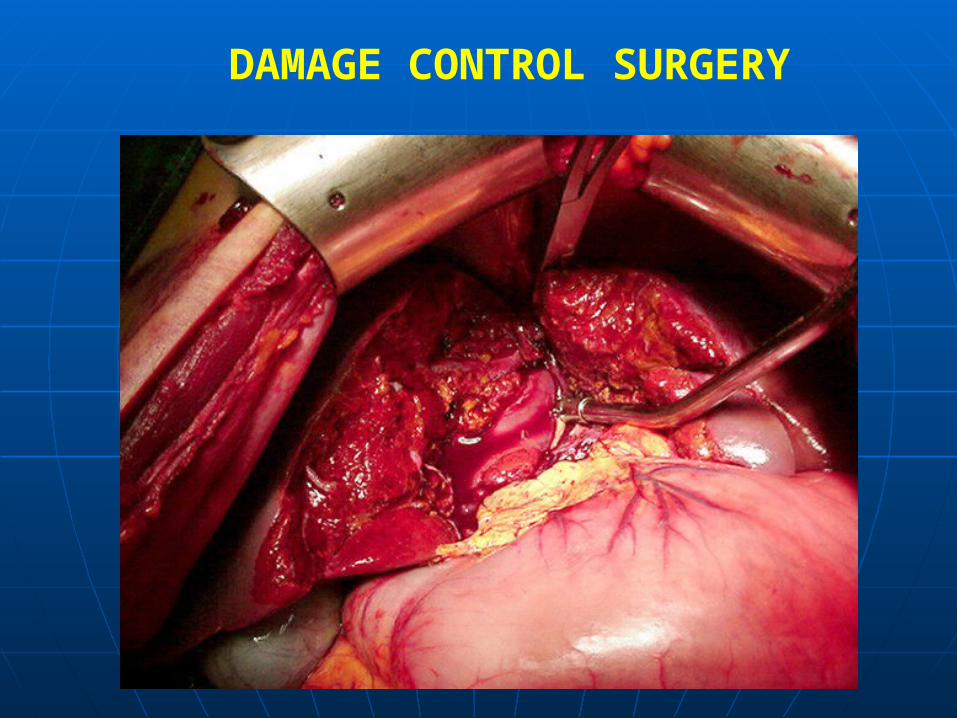
•Prep surgical field from neck to knees and from flank to flank•Longitudinal incision form xiphoid to pubis•Cell saver to reinfuse autologous blood if possible•Urgent exploration with packing of all four quadrants of abdomen•Serial controlled examination of each quadrant and organ•Pack liver injuries and splenic injuries•Control vascular injuries•Close off perforated gastrointestinal tract•Examine retroperitoneal structures
DAMAGE CONTROL SURGERY
•Avoid hypotension, hypothermia, acidosis leading to coagulopathy
•Repair or ligate vascular injuries•Splenectomy if injured•Repair or resect intestines•Pack liver hemorrhage•Pack and leave open abdomen if necessary•Continue resuscitation and warming in ICU•Come back another day
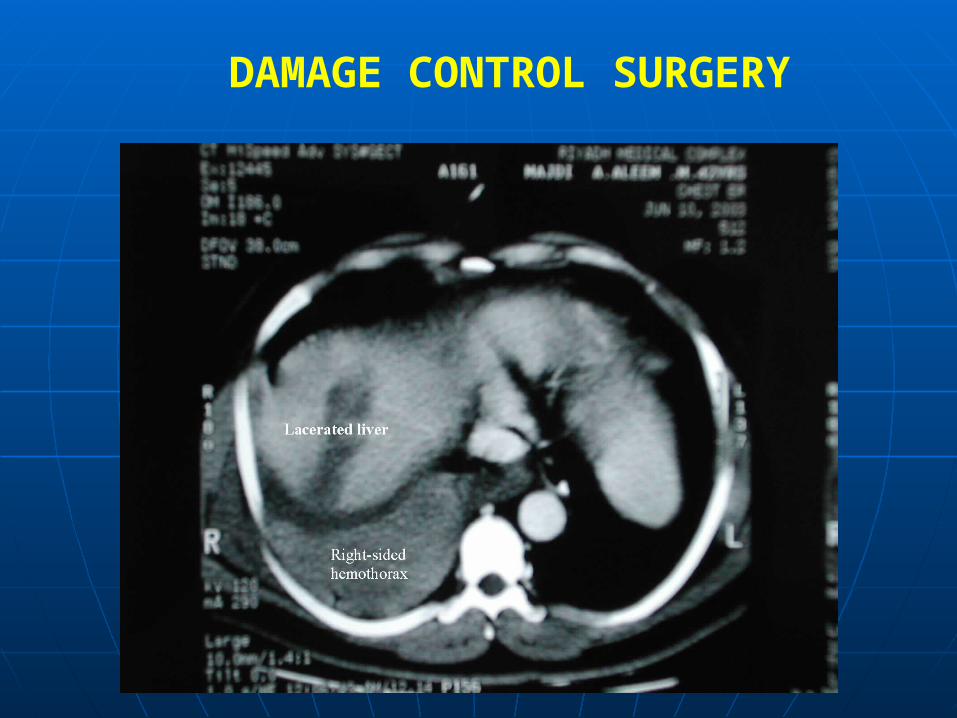
DAMAGE CONTROL SURGERY
DAMAGE CONTROL SURGERY
DAMAGE CONTROL SURGERY
DAMAGE CONTROL SURGERY
DAMAGE CONTROL SURGERY
DAMAGE CONTROL SURGERY
DAMAGE CONTROL SURGERY
Renal injuries on battlefield often complex injuries
If laceration and hematoma from blunt injury, may observe
If laceration from penetrating injury, may require nephrectomy to control bleeding
Need for drains after surgery
DAMAGE CONTROL SURGERY
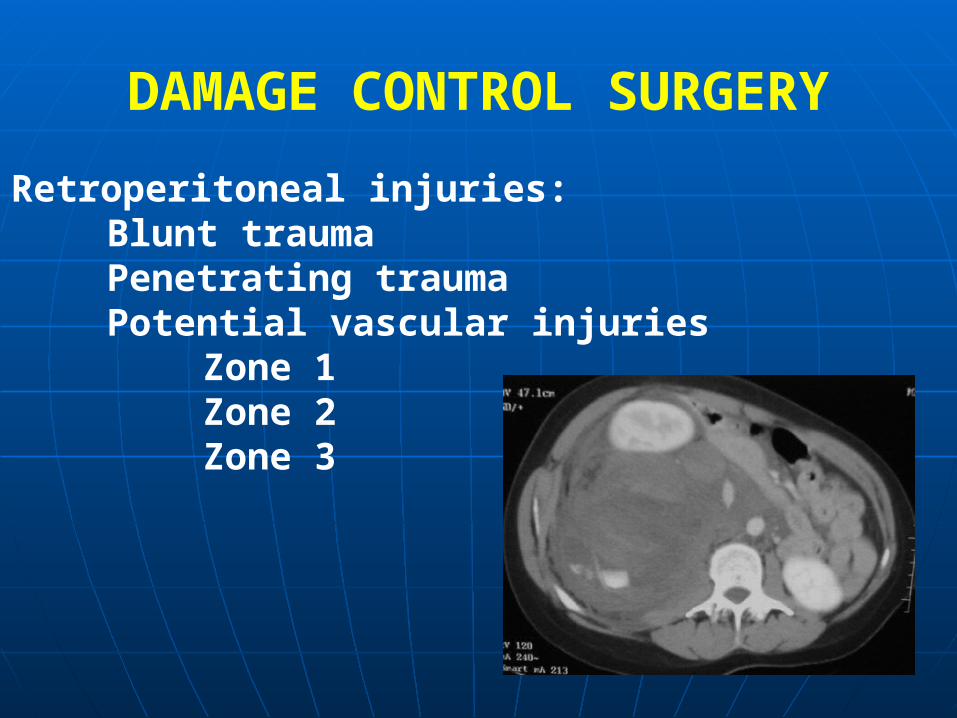
Retroperitoneal injuries:Blunt traumaPenetrating traumaPotential vascular injuries
Zone 1Zone 2Zone 3
DAMAGE CONTROL SURGERY
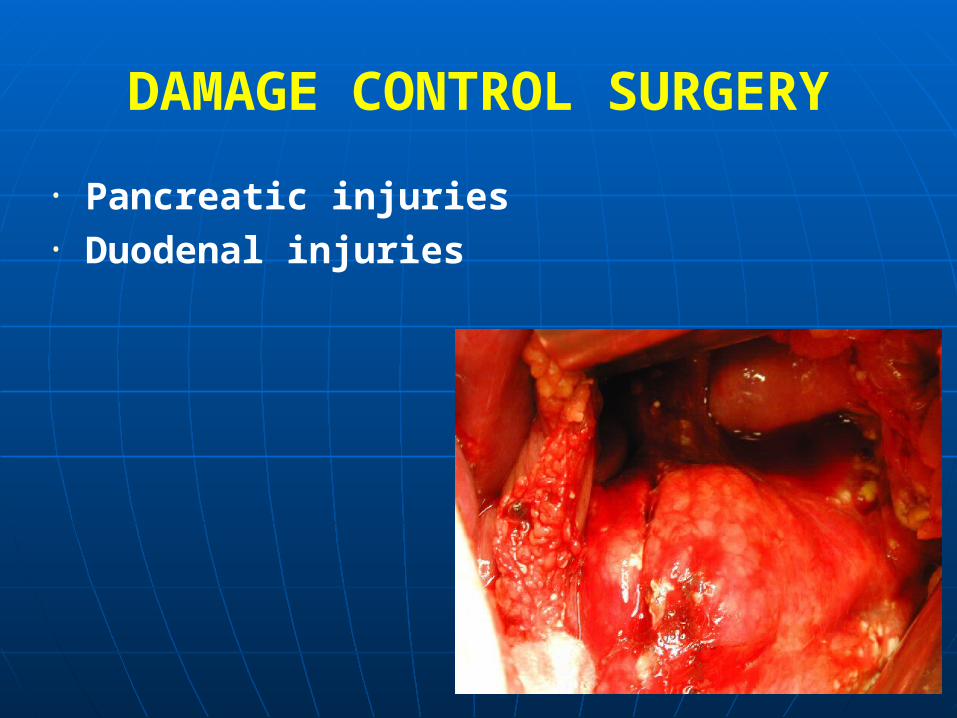
• Pancreatic injuries• Duodenal injuries
DAMAGE CONTROL SURGERY
• Pancreatic injuries vary from simple contusions and lacerations to complex injuries of head of pancreas
• Complicated by concomitant duodenal injuries
• Strategy to control hemorrhage• Drainage of injuries• Secondary procedures to divert GI tract
DAMAGE CONTROL SURGERY
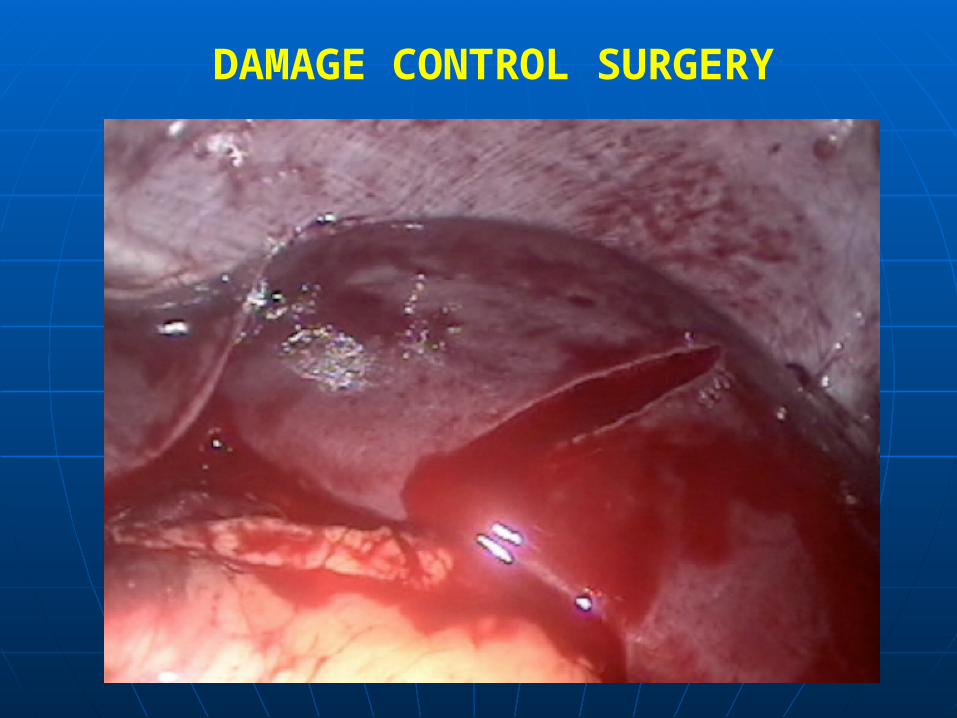
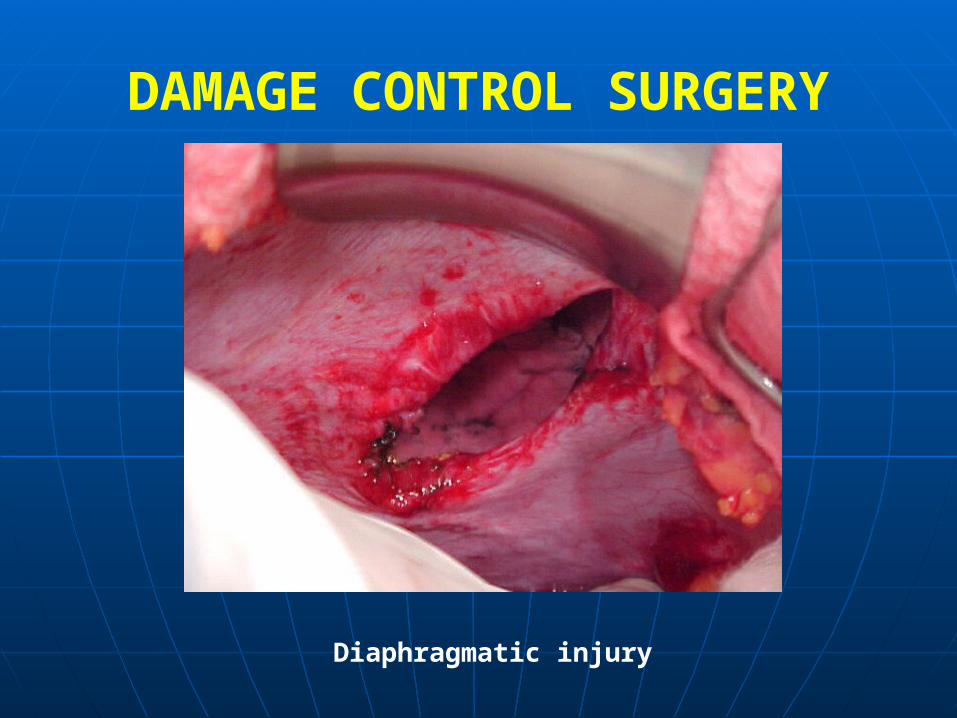
Diaphragmatic injury
DAMAGE CONTROL SURGERY
• Diaphagmatic injuries require surgical repair Diaphagmatic injuries require surgical repair to avoid herniation abdominal organs and to avoid herniation abdominal organs and compromise of pulmonary functioncompromise of pulmonary function
• Place chest tubes pleural cavity to control Place chest tubes pleural cavity to control pneumothoraxpneumothorax

DAMAGE CONTROL SURGERY
DAMAGE CONTROL SURGERY
• Surgical strategy depends on cause of intestine injury due to penetrating vs blunt vs explosive blast
• Degree of contamination• Small versus large bowel• Hemodynamic stability of patient• Suture repair• Stapled resection• No anastamosis if clinically unstable
SUMMARY
• Abdominal injury with potential for many Abdominal injury with potential for many organ systems at riskorgan systems at risk
• Blunt versus penetrating injuriesBlunt versus penetrating injuries• Surgery to repair damage and control Surgery to repair damage and control
hemorrhage from vascular structures and hemorrhage from vascular structures and organsorgans
• Damage control surgery to repair intestines Damage control surgery to repair intestines defined by battlefield conditionsdefined by battlefield conditions
• Stabilize and return for definitive repairStabilize and return for definitive repair


















