
Catheter Wipeout Initiative: Updates Lisle Mukai, QI Coordinator August 2008.
47
Catheter Wipeout Initiative: Updates Lisle Mukai, QI Coordinator August 2008
-
Upload
milton-wilkins -
Category
Documents
-
view
218 -
download
0
Transcript of Catheter Wipeout Initiative: Updates Lisle Mukai, QI Coordinator August 2008.
Catheter Wipeout Initiative: Updates
Lisle Mukai, QI CoordinatorAugust 2008
2
DaVita Catheter Wipeout Initiative
The project addresses high catheter rates within the Riverside/San Bernardino area. The involved facilities are Surf-N-Sun Division facilities who are divided into 3 teams lead by their Regional Managers. The teams will be competing against each other for attaining the lowest catheter rates.
The facilities will utilize DaVita tracking tools and implement Fistula First Change Concepts to attain their goal.
3
Project GoalTo reduce the total catheter rate by 20% in
each of the intervention facilities over an 8 month period (May – December 2008).
Attained by implementing Change Concepts: #5: Full Range of Appropriate Surgical
Approaches to AVF Evaluation & Placement
#7: AVF Placement in Patients with Catheters Where Indicated
#9: Monitoring & Maintenance to Ensure Adequate Access Function.
4
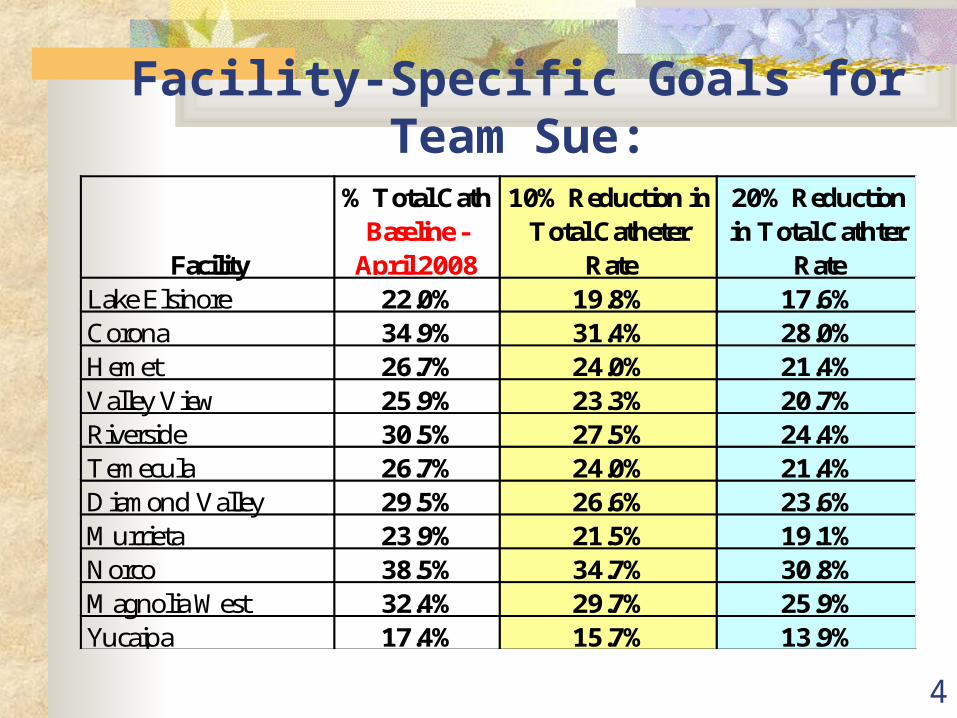
Facility-Specific Goals for Team Sue:
Facility
% Total Cath Baseline -
April 2008
10% Reduction in Total Catheter
Rate
20% Reduction in Total Cathter
RateLake Elsinore 22.0% 19.8% 17.6%Corona 34.9% 31.4% 28.0%Hemet 26.7% 24.0% 21.4%Valley View 25.9% 23.3% 20.7%Riverside 30.5% 27.5% 24.4%Temecula 26.7% 24.0% 21.4%Diamond Valley 29.5% 26.6% 23.6%Murrieta 23.9% 21.5% 19.1%Norco 38.5% 34.7% 30.8%Magnolia West 32.4% 29.7% 25.9%Yucaipa 17.4% 15.7% 13.9%
5
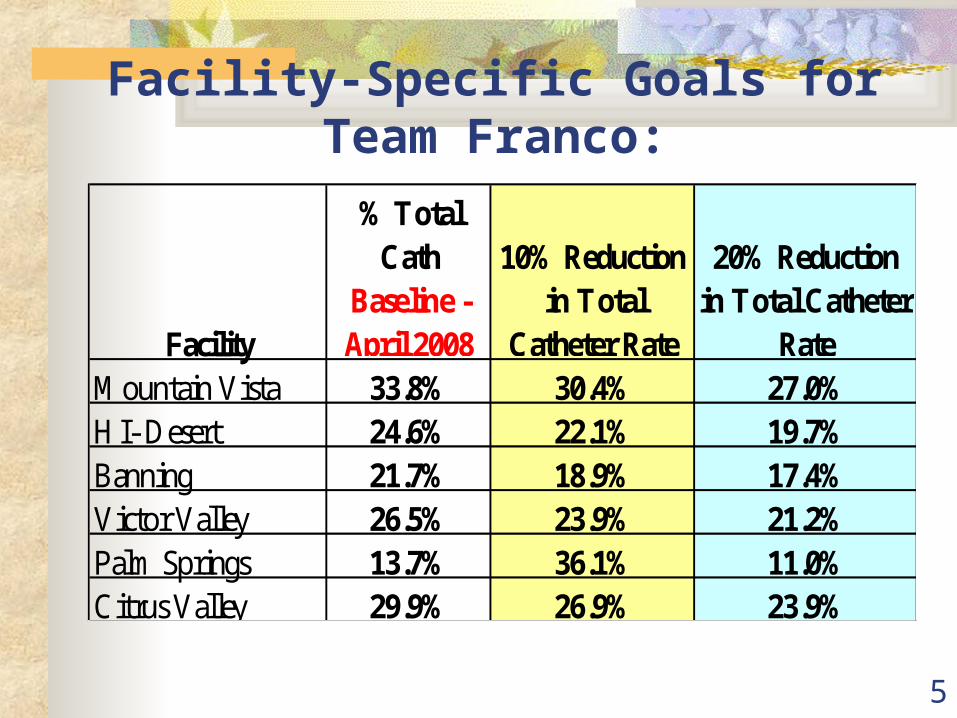
Facility
% Total Cath
Baseline - April 2008
10% Reduction in Total
Catheter Rate
20% Reduction in Total Catheter
RateMountain Vista 33.8% 30.4% 27.0%HI- Desert 24.6% 22.1% 19.7%Banning 21.7% 18.9% 17.4%Victor Valley 26.5% 23.9% 21.2%Palm Springs 13.7% 36.1% 11.0%Citrus Valley 29.9% 26.9% 23.9%
Facility-Specific Goals for Team Franco:

6
Facility-Specific Goals for Team Rosemarie:
Facility
% Total Cath
Baseline - April 2008
10% Reduction in Total Catheter
Rate
20% Reduction in Total Catheter
RateMontclair 28.9% 26.0% 22.4%Ontrario 42.9% 38.6% 34.3%Pomona 30.5% 27.5% 24.4%Chino 21.8% 19.6% 17.4%Upland Dialysis 20.7% 18.6% 16.6%Fontana 23.5% 21.2% 18.8%
7
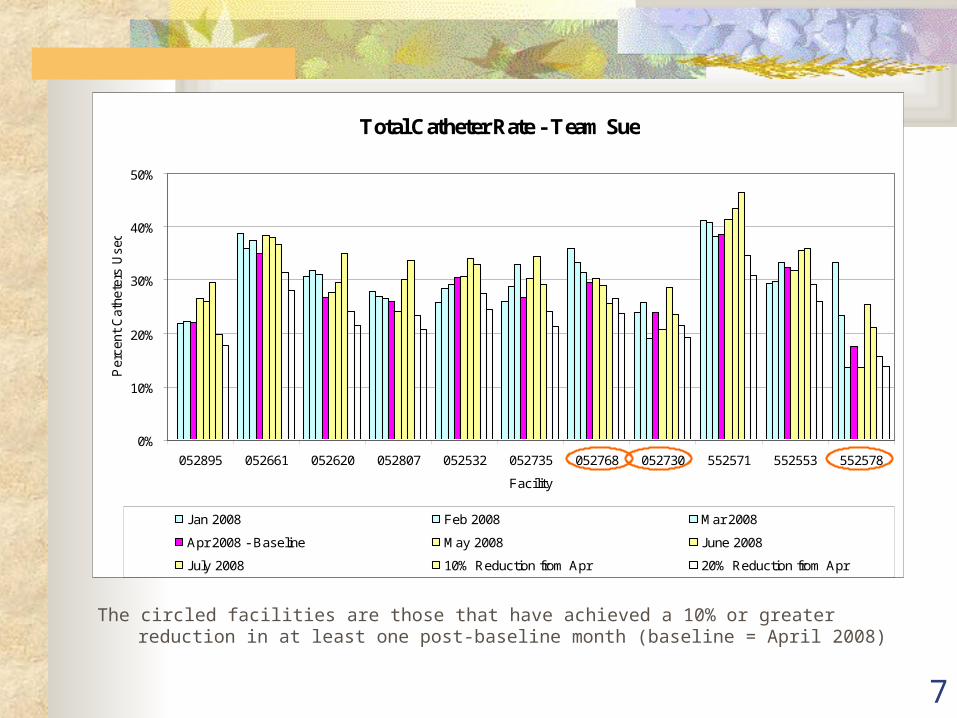
The circled facilities are those that have achieved a 10% or greater reduction in at least one post-baseline month (baseline = April 2008)
Total Catheter Rate - Team Sue
0%
10%
20%
30%
40%
50%
052895 052661 052620 052807 052532 052735 052768 052730 552571 552553 552578
Facility
Per
cent
Cat
hete
rs U
sed
Jan 2008 Feb 2008 Mar 2008
Apr 2008 - Baseline May 2008 June 2008
July 2008 10% Reduction from Apr 20% Reduction from Apr

8
Total Catheter Rate - Team Franco
0%
10%
20%
30%
40%
052743 052776 552520 052561 052541 552541
Facility
Perc
ent C
athe
ters
Use
d
Jan 2008 Feb 2008 Mar 2008 Apr 2008 - Baseline May 2008
June 2008 July 2008 10% Reduction from Apr 20% Reduction from Apr
The circled facilities are those that have achieved a 10% or greater reduction in at least one post-baseline month (baseline = April 2008)
Banning Dialysis (#552520) has consistently maintained a 10% reduction within the 3 months.
9
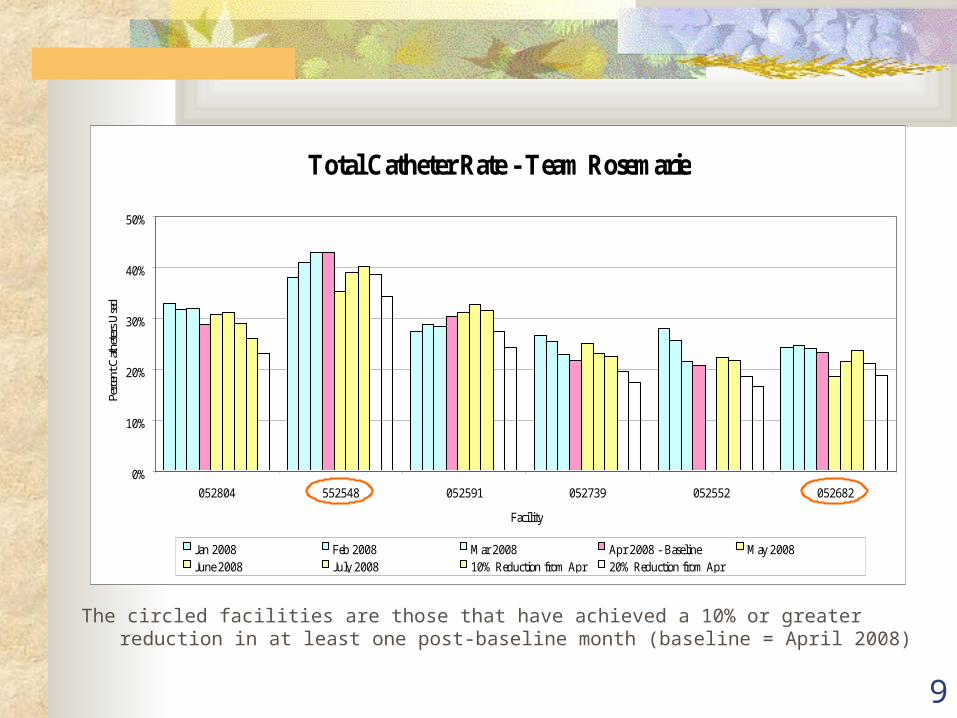
Total Catheter Rate - Team Rosemarie
0%
10%
20%
30%
40%
50%
052804 552548 052591 052739 052552 052682
Facility
Perc
ent C
athete
rs U
sed
Jan 2008 Feb 2008 Mar 2008 Apr 2008 - Baseline May 2008June 2008 July 2008 10% Reduction from Apr 20% Reduction from Apr
The circled facilities are those that have achieved a 10% or greater reduction in at least one post-baseline month (baseline = April 2008)

10
Team Goals:
% Total Cath Baseline -
April 2008
10% Reduction in Total Catheter
Rate20% Reduction in Total Catheter Rate
Team Franco 25.7% 23.1% 20.6%Team Rosemarie 27.7% 24.9% 22.2%
Team Sue 28.4% 25.6% 22.7%
Group Total: 27.6% 25.0% 22.2%
11
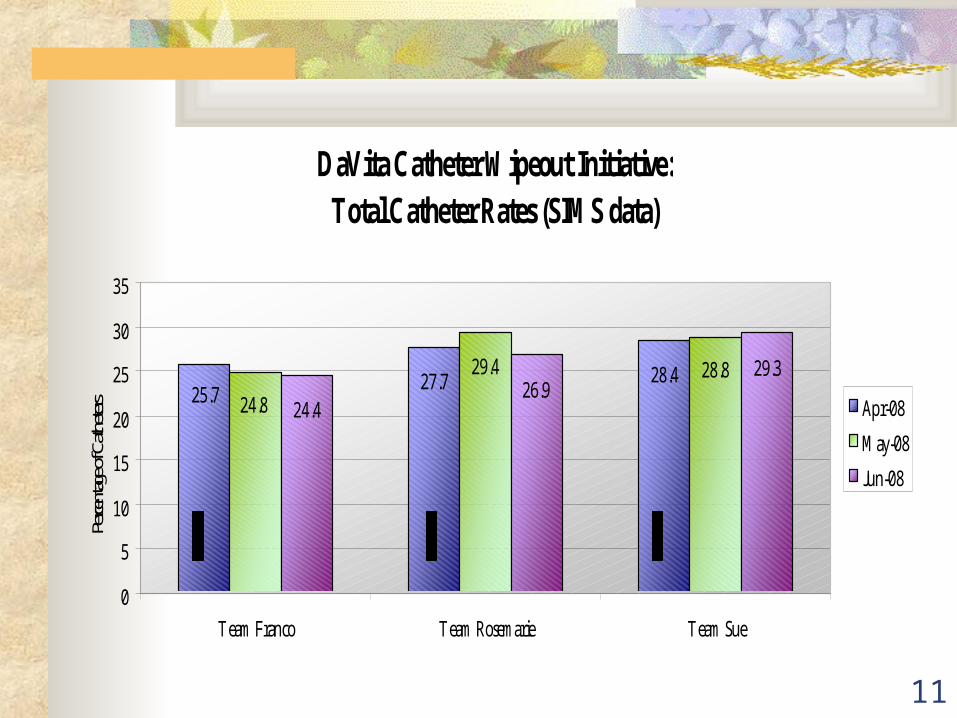
DaVita Catheter Wipeout Initiative: Total Catheter Rates (SIMS data)
28.427.725.7
28.829.4
24.8
29.326.9
24.4
0
5
10
15
20
25
30
35
Team Franco Team Rosemarie Team Sue
Perce
ntag
e of C
athete
rs Apr-08
May-08
Jun-08

12
DaVita Catheter Wipeout Initiative: Group Vascular Access Trends (SIMS data)
22.3
27.6
49.7
22
28
50
22.4
27.5
50.1
0
10
20
30
40
50
60
AVF Total Catheter AVG
Perce
ntag
e of A
VF Apr-08
May-08
Jun-08
Basel
ine
Basel
ine
Basel
ine
CMS AVF Goal: 66%Network 18 AVF Goal: 55.1%
CMS/Network 18 Catheter Goal: < 10%
CMS/Network 18 AVG Goal: < 24%

13
Change Concept # 5: Full Range of Appropriate Surgical
Approaches to AVF Evaluation & Placement
Fistula First Website: Surgical video series: “Creating AV
Fistulae in All Eligible Hemodialysis Patients”
Article: “Surgical salvage of the autogenous arteriovenous fistula (AVF).
Autologous AVF Algorithm (Developed by Dr. Spergel, MD, Clinical Chair for the FFBI)
Commonly Used Permanent Vascular Access Codes (CPT codes)
14
Change Concept # 5: Full Range of Appropriate Surgical Approaches to
AVF Evaluation & Placement (continued)
Make sure surgeons understand the logistics of cannulation so that they position the veins suitably and safely for cannulation “Cannulation of the Arteriovenous Fistula
(AVF)” DVD – Each facility should have received one DVD from your corporate office.
Encourage acute nursing staff to become more assertive in asking the Nephrologist to order vein mapping before discharging the patients from the hospital.

15
Change Concept # 5: Full Range of Appropriate Surgical Approaches to
AVF Evaluation & Placement (continued)
Dialysis Access Clubs Presentations and discussions regarding
creation, maintenance, and addressing complications of all types of vascular accesses are discussed.
This is a great forum for surgeons and interventional radiologists to share or ask questions with their peers about vascular access situations they encounter.
16
Change Concept # 5: Full Range of Appropriate Surgical Approaches to
AVF Evaluation & Placement (continued)
Currently there are two active Dialysis Access Clubs: San Diego and Orange County. These clubs were started by Vascular Access Surgeons who are truly engaged in the Fistula First program.
These meeting are usually held on a quarterly basis. Invitations are directly e-mailed to surgeons (the
sponsoring organization has a vascular surgeon database they use to e-mail these invitations), because there is no Access Club in the Inland Empire as of yet, encourage your surgeons to contact their colleagues within the Orange County & San Diego County area and find out when these meetings occur.
Hopefully this communication between colleagues will open opportunities for vascular access discussions and interest that will engage all surgeons.
17
Change Concept #7: AVF Placement in Patients with Catheters Where
Indicated Evaluation and mapping of catheter patients is crucial
to facilitate the placement of AV fistulae. While catheters are necessary in some circumstances (e.g., while an AV fistula matures), the increasing prevalence of catheters is a serious health risk to patients.
Per Dr. Nguyen: “Educate patients and their families. Patients don’t
want to hear about the operation when they do not feel sick and yet early surgery for fistula is key to success. "I spend a lot of time talking to patients and their families," Nguyen says. "I always invite the whole family to come to the first visit. Convince the family, and they will beat on the patient to do it."

18
Change Concept #7: AVF Placement in Patients with Catheters Where
Indicated (Continued) “It’s important to explain the procedure in very
simple terms” “Set expectations properly in case the first
operation doesn’t do the job, since we are dealing with sicker and older patients with higher risk of fistula failure to mature properly, we tell them that another surgery may be needed.”
Use diagrams when showing the patients where the catheter is located when educating them about their access.
19
Change Concept #7: AVF Placement in Patients with Catheters Where
Indicated (Continued) FFBI Payer Packets have been posted to
the Fistula First websitehttp://www.fistulafirst.org/pdfs/
FF_Intro_for_Payers.pdf
The payer packet is a set of documents that you can use to communicate with your insurance companies about promoting catheter reduction and AVF placement.
The documents includes: Introductory Letter for Payers Pay for Performance Summary Recommendations Fistula First Priority Recommendations PowerPoint slides
20
Change Concept #7: AVF Placement in Patients with Catheters Where
Indicated (Continued)
Introductory Letter for Payers
1 page document that explains who the Fistula First Breakthrough Initiative is
Why vascular access, specifically catheters, matters so much
What the organization (insurance company) can do about it.
21
Change Concept #7: AVF Placement in Patients with Catheters Where
Indicated (Continued)
Pay for Performance – Summary Recommendations
This is a payment position paper submitted by FFBI for consideration by CMS and other payers.
This is an educational item and not a final CMS decision for Pay for Performance.

22
Change Concept #7: AVF Placement in Patients with Catheters Where
Indicated (Continued)
FFBI Priority Recommendations
Recommendations by FFBI for developing and implementing an incentive program for practitioners.
References to specific Change Concept elements.
23
Change Concept #7: AVF Placement in Patients with Catheters Where
Indicated (Continued)
Slides
The PowerPoint slides illustrates costs for care: Medicare costs per person per year Per person per year access costs by type of access Hospitalization admissions for vascular access
complications per patient year Risk for infection comparison between catheters
and AV fistulas Variation on costs for inpatient hospital services per
Medicare enrollee Performance on Medicare Quality Indicators
24
Reducing Catheter Rate Strategies:
Surgical evaluation,vessel mapping (& placement) of permanent access during initial, acute hospitalization
Patient education Engagement of surgeons Early recognition & intervention for non-
maturing AVFs = Post-op exam @ 4 wks Protocol for catheter removal (FF website)
25
Proactive strategies to reduce catheter rate:
Surgical evaluation (& placement) of permanent access during initial hospitalization
Vessel mapping/optimal vessel selection to increase successful (usable) AVFs & Reduce non-maturing (FTM) AVFs (post-op exam @ 4 wks)
Monitoring & timely intervention for late failure/ aggressive salvage
26
Change Concept #9: Monitoring & Maintenance to Ensure Adequate
Access Function
AVF Maturation Process – Fistula maturation is defined as the process by
which a fistula becomes adequately dilated and thick-walled to make it suitable for cannulation.
Usually takes 8 – 12 weeks for a fistula to mature, but can take longer
Should be able to feel strong thrill at the arterial anastamosis
Listen for continuous low-pitched bruit Vessel diameter must be 4-6 mm, veins
should be firm to touch an no prominent collateral veins
27
Change Concept #9: Monitoring & Maintenance to Ensure Adequate
Access Function (Continued)
Most failing AVF’s can be identified on evaluation at 4 weeks
Many early AVF failures can be salvaged if identified before thrombosis occurs
If the AVF is patent but you are unable to cannulate the AVF or adequately dialyze the patient by 12 weeks, refer for exam/fistulogram to determine what intervention is needed
28
Change Concept #9: Monitoring & Maintenance to Ensure Adequate
Access Function (Continued)
Each treatment should include a physical assessment of the new
AVF:
Look at the access and compare the access extremity to the other extremity
Listen for bruit (USE A STETHESCOPE!) Feel for thrill
29
Change Concept #9: Monitoring & Maintenance to Ensure Adequate
Access Function (Continued)
Abnormal Changes in the Access Extremity:
Edema of the access extremity Cold to the touch with pain or numbness (possible Steal
Syndrome) Warm to the touch (possible infection) Bruising Loss of continuous briut/or change in the bruit Change in the quality of the “thrill” or complete loss of
thrill
ACTION: Refer for exam to determine intervention needed
30
AVF Dysfunction/Failure to Mature (FTM)
> 30% of new AVFs fail to mature (FTM) and may need some type of intervention before it can be used
You can markedly reduce early failure rate and interventions in AVFs by: Early referral & CKD program Improved patient & vessel
selection/standardized vessel mapping protocol Early recognition of FTM AVF by evaluation
(Monitoring & Surveillance) at 4 wks & timely intervention = high salvage rate
31
All patients should be taught how to:
Feel for thrill – Report absence to staff immediately! Listen for bruit - Report absence to staff immediately! Look and recognize signs & symptoms of infection -
Report signs/symptoms to staff immediately!
Exercise the fistula arm with some resistance to venous flow Squeezing a rubber ball with or without a lightly applied
tourniquet may increase flow, thereby enhancing vein maturation, and has been shown to significantly increase forearm vessel size, thereby potentially increasing flow through the AVF.
Avoid carrying heavy items and wearing occlusive clothing (occlusive bands/elastic over access areas)
Avoid sleeping on the access arm
32
Success Stories RMS Lifeline Outpatient Vascular Access
Center will remove catheters for Emergency Medi-Cal patients with a working AVF access free of charge!
Documentation of all access events can justify reason for request of AVF evaluation & placement for patients with Emergency Medi-Cal.
33
Fistula First AVF Goals
CMS Goal – 66% by June 30, 2009
Yearly Network 18 Goal – 55.1% by March 31, 2009
Yearly Network Stretch Goal – 56% by March 31, 2009
June 2008 AVF rates: NW 18 – 53.4 % US – 50.3%
34
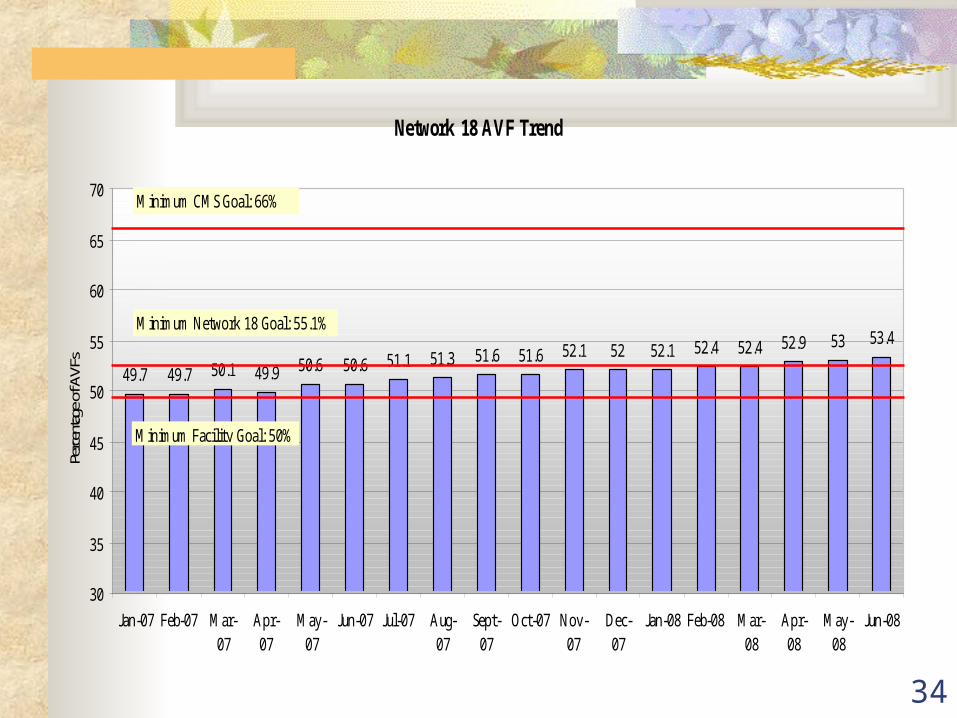
Network 18 AVF Trend
49.7 49.7 50.1 49.9 50.6 50.6 51.1 51.3 51.6 51.6 52.1 52 52.1 52.4 52.4 52.9 53 53.4
30
35
40
45
50
55
60
65
70
Jan-07 Feb-07 Mar-07
Apr-07
May-07
Jun-07 Jul-07 Aug-07
Sept-07
Oct-07 Nov-07
Dec-07
Jan-08 Feb-08 Mar-08
Apr-08
May-08
Jun-08
Perc
entag
e of A
VFs
Minimum CMS Goal: 66%
Minimum Network 18 Goal: 55.1%
Minimum Facility Goal: 50%
35
Fistula First Change Concepts
1. Routine CQI Review of vascular access
2. Timely referral to nephrologist
3. Early referral to surgeon for “AVF Only”
4. Surgeon Selection5. Full range of
appropriate surgical approaches
6. Secondary AVFs in AVG patients
7. AVF evaluation/placement in catheter pts where indicated
8. Cannulation training9. Monitoring and
maintenance10. Continuing Education11. Outcomes feedback
36
Change Concept #6: Secondary AVF Placement in Patients with AV Grafts
Convincing a patient, Nephrologist, and Vascular Access Surgeon to evaluate and place a secondary AVF can be difficult, especially when a problem has not been experienced. Education is key. It is well known that when an AV graft clots or problems occur, they will more likely happen again.
The Fistula First Breakthrough Initiative and Network 18 would like to emphasize the importance of monitoring and surveillance for stenosis. By monitoring and tracking problems with an AV graft the Nephrologist
can easily refer the patient for a secondary AVF evaluation and placement before failure of the AV graft.
Converting to an AVF will help improve patient care by decreasing missed treatment time for frequent interventions/revisions thus improving the patient’s quality of life and increasing the performance of the access.
37
Change Concept #6: Secondary AVF Placement in Patients with AV Grafts
(Continued)
Nephrologist should evaluate every AVG patient for an AVF.
Conducting the “Sleeves Up” exam monthly will help identify if a patient with an AVG may be a candidate for an AVF conversion. (Protocol was distributed at the Kick-off meeting in April)
Vessel mapping if suitable veins are not identified on physical exam.
A secondary AVF plan should be documented in the chart and discussed with the patient, family, staff, nephrologists, & surgeons in anticipation of AVF construction on the earliest evidence of AVG failure.

38
Sleeves Up Exam

39
Timing of AVG conversion to a secondary AVF
1st AVG failure triggers evaluation for conversion to a secondary AVF A plan of care should be developed in
anticipation of AVG failure
At the sign of a second impeding AVG failure, the patient should be sent for an AV fistula conversion.
Any delay in conversion beyond this point is likely to result in loss of the window of opportunity for this AVF option.

40
FFBI Strategies to increase Secondary AV Fistulae:
Re-evaluation of all patients for AVF K/DOQI guideline 29: Every patient
should be evaluated for a secondary fistula after each episode of graft failure
Physical exam, vessel mapping and/or fistulogram
Develop plan of care for anticipation of AVG failure Conversion of existing AVG to AVF, utilizing
outflow vein of graft for AVF where feasible
41
Patients without medical insurance
Med-Cal only patients
Restricted Medi-Cal
HMO (ex. RMC, PMD) that requires authorization
No good surgeons
Not all surgeons accept Med-Cal and those who accept require long waiting time
System Roadblocks Identified by Facilities
Afraid of needles Comfortable with
catheter Exhausted sites Language
barriers Forgetting follow-
ups and missing appointments
Lack of education
Patient Roadblocks Identified by Facilities:
Lack of knowledge and effort from the PCP offices
Communication between dialysis unit and surgeon’s office
Problems with the newly placed AVF (does not mature or clots)
More Roadblocks:
42
Educate patients Vessel mapping for
everyone Establish “Sleeves-up”
Monday and Tuesday (At least monthly)
Utilize Outpatient Vascular Access Center
Establish relationship with surgeon’s office
Establish relationship with HMO contacts
Early follow-up on newly placed AVFs (As early as 4 weeks)
Address every single catheter
Documentation is the key!
Visit www.fistulafirst.org website for resources & tools
Utilize FFBI tools and tools that are available through DaVita
Recognize issues and address them early
Empower your staff by delegating roles
Share successes and approach vascular access as one community
Call your Network for help
Possible Solutions:
43
DaVita Vascular Access Tracking Tools
Patient Report Facility Report Catheter Tracking tool Vascular Access Event Log
44
Ongoing Issues No surgeons in the area Patients with no medical insurance No access placed prior to starting dialysis (CKD)
or long-term dialysis patients
Language barriers Patient’s noncompliance
These are some issues we may not be able to solve alone but we can try and find ways together to solve them or at least work around them. If you find successful ways to deal with some of these issues….
PLEASE SHARE THEM WITH EVERYONE!
45
Action Plan Use the FFBI Payer Packet to communicate with your insurance
carries about the benefits of having an AVF placed for ESRD patients. (If all your facilities have the same insurance companies, all facilities communicate this concern and urgency.)
Find ways to engage your surgeons (i.e. Share your facility specific data that you receive from the Network, inform them about the vascular access clubs, etc.).
If your facilities all use the same surgeon(s), all facilities should communicate the same message/urgency regarding AVF placement.
Share the Cannulation DVD with the surgeons so that they understand the logistics of cannulation and can position the veins suitably and safely for cannulation.
Educate both the patient and the FAMILY about vascular access – specifically AVFs.
Share best practices with everyone!

46
Conclusion:
• We are all partners
• We are on the right track
• Utilize available recourses and steal shamelessly (Best practices)
• Visit the FFBI website for more resources
• Call your Network for help
• Share successes
• It CAN be done!

47
Lisle Mukai, RN,
Quality Improvement Coordinator
ESRD Network 18
Phone: 323-962-2020
Fax: 323-962-2891


















