
Valeology and sanology basics of providing safety of health and human life.
Upload
elmadana1988Category
view
37download
1
QUANTIFYINGSPORTS TRAINING
QUANTIFYINGSPORTS TRAINING AND DOPING
CHAPTER 12CHAPTER 12

Did You Know…?
A person’s rate of adaptation and response to training depends on that individual. He or she cannot be forced beyond his or her body’s capacity for development. Thus, training programs must take these individual differences into account.

Optimal Training Load
Progressive overload—progressive increase in training load as body adapts
Training volume—duration or frequency
Training intensity—force of muscle action and stress on the muscular and cardiovascular systems
Resistance training (high intensity and low volume)
Aerobic training (high volume and lower intensity)
Rest periods—without them, muscles become chronically depleted

CHANGES IN HEART RATE AND BLOOD LACTATE

Did You Know…?
Long daily workouts may not be the best training method for some sports. It appears that training volume could be reduced by as much as one half in some sports, without reducing the training benefits and with less risk of overloading.

Overtraining
Training beyond the point that would be optimal; can be related to intensity, duration, frequency, or any combination of these three
Staleness is a related concept
The key is to design a training program that will provide the optimal level of stress but will not overstress the athlete

Symptoms of Overtraining Syndrome
Decline in physical performance
Decreased appetite and body weight loss
Muscle tenderness
Head colds, allergic reactions, or both
Occasional nausea
Sleep disturbances
Elevated resting heart rate and blood pressure
Feeling of “heaviness” and loss of desire to train and compete
Emotional instability

Possible Causes of Overtraining
Periods of excessive training or emotional stress
Abnormal responses in the autonomic nervous system—sympathetic and parasympathetic
Disturbances in endocrine function
Depressed immune function

Sympathetic NS Overtraining
Increased resting heart rate and blood pressure
Loss of appetite and decreased body mass
Sleep disturbances and emotional instability
Elevated resting metabolic rate
Parasympathetic NS Overtraining
Early onset of fatigue
Decreased resting heart rate and blood pressure
Rapid heart rate recovery after exercise
Less common than sympathetic NS overtraining

TRAINING VOLUME AND RISK OF INFECTION

Predicting Overtraining
Increase in oxygen consumption for the same rate of work (though impractical for coach to measure)
Increased heart rate response to the same rate of work
Declines in performance

VO2 IN EARLY AND LATE SEASON.

HEART RATE RESPONSES TO TRAINING

Treatment of Overtraining
Reduce training intensity for several days
Rest completely for three to five days
Seek counseling
Prevent overtraining by alternating easy, moderate, and hard training
Eat sufficient carbohydrate to prevent glycogen depletion

Key Points
Excessive training refers to training with an unnecessarily high volume or intensity.
Excessive training does not lead to additional gains in performance and can lead to overtraining.
Training Demands
Increase the duration or frequency of training to increase training volume.
(continued)

Key Points
Training Demands
Training intensity can determine specific adaptations to training.
High-intensity, low-volume training increases muscle strength and speed.
High-volume, low-intensity training (50% to 90% VO2max) increases aerobic capacity.
.

Key Points
Overtraining leads to decreased performance capacity.
Symptoms of overtraining may occur briefly with regular training.
Overtraining
Overtraining may be caused by abnormal responses in the autonomic nervous and endocrine systems and suppressed immune function.
Heart rate response appears to be the most reliable warning of overtraining.
Overtraining syndrome is treated most effectively with rest and proper nutrition.

Did You Know…?
Tapering for competition involves a reduction in training intensity and volume. This rest allows your body to repair itself and restore its energy reserves to prepare you for your best performance.

Effects of Properly Tapering
Muscular strength increases
Energy reserves are restored
Performance increases (especially in swimmers)
No loss of VO2max occurs.

Detraining
Cessation of regular training; may be due to inactivity or immobilization
Loss of muscle size, strength, and power
Decrease in muscular and cardiorespiratory endurance
Loss of speed, agility, and flexibility

Loss of Muscle Strength
Muscle atrophy accounts for a loss in development of maximal muscle fiber tension.
Normal fiber recruitment is disrupted; some fibers are unable to be recruited.
Muscle requires minimal stimulation (training once every 10 to 14 days) to retain training gains.

STRENGTH CHANGES WITH DETRAINING

Loss of Endurance
Decreased performance may be related to losses in cardiorespiratory endurance.
Oxidative enzyme activity in muscles decreases.
Glycolytic enzymes remain unchanged with up to 84 days of detraining.
Muscle glycogen content (and thus storage capacity) decreases.
Acid-base balance becomes disturbed.
Muscle capillary supply and fiber type may change.
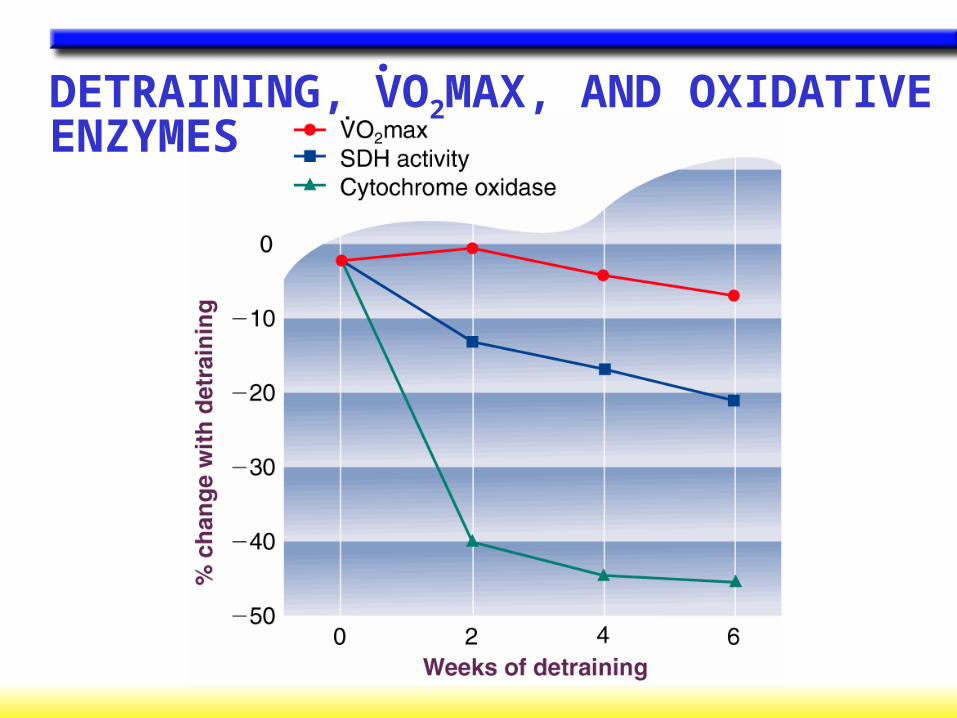
DETRAINING, VO2MAX, AND OXIDATIVE ENZYMES
.

DETRAINING AND MUSCLE GLYCOGEN

Loss of Cardiorespiratory Endurance
Losses are greatest in highly trained individuals.
Plasma volume decreases
Stroke volume decreases
Endurance performance decreases
VO2max decreases.

Did You Know…?
You can prevent rapid losses to your cardiorespiratory endurance with a minimum of three training sessions per week at an intensity of at least 70% VO2max.
.

CHANGES IN VO2MAX WITH BED REST.

Retraining
Recovery of conditioning after a period of activity.
Affected by fitness level and the length and extent of inactivity.
If a cast allows some range of movement, retraining time can be reduced.
Electrical stimulation of muscles can prevent muscle fiber atrophy.

Key Points
Detraining is the cessation of regular physical training
Retraining is resuming training after a period of inactivity.
Detraining and Retraining
The greater the training gains achieved, the greater the losses with detraining.
Detraining results in losses of muscle size, strength, power, and endurance; speed, agility, and flexibility; and cardiorespiratory endurance.
Detraining effects can be minimized by training three times a week at 70% VO2max..

Examples in Sports
Football—anabolic steroids
Cycling—blood doping or EPO; amphetamines
Weight category athletes—diuretics, amphetamines
Distance running—carbohydrate loading
Note: Scientific studies are limited by the accuracy of measurements and individual day-to-day variability. Events are won by hundredths of seconds or by centimeters.

Did You Know…?
The placebo effect refers to when your body’s expectations of a substance determine your body’s response to it. While the effect is psychological in origin, the body’s physical response to the substance is real.

THE PLACEBO EFFECT ON STRENGTH GAINS

Pharmacological Agents
Alcohol
Amphetamines
Beta blockers
Caffeine
Cocaine
Diuretics
Marijuana
Nicotine

Alcohol
Provides energy (7 kcal/g) but inhibits metabolism
Dulls pain sensation (increasing injury risk); reduces anxiety
Suppresses release of ADH which leads to dehydration
Appears to impair psychomotor function
Has no ergogenic effects on strength, power, speed, or endurance

ALCOHOL SUPPRESSES ADH RELEASE

Amphetamines
Increase mental alertness, blood pressure, heart rate, blood glucose and FFA levels, and muscle tension
Decrease sense of fatigue
Redistribute blood flow to skeletal muscles
May enhance speed, power, endurance, concentration, and fine motor coordination
May be addictive and can trigger cardiac arrhythmia or death

Beta Blockers
Prevent the binding of norepinephrine to its receptor, thus decreasing sympathetic nervous system effects
May improve accuracy (for shooting sports)
Decrease aerobic capacity but have no effect on strength, power, or muscular endurance
Prolonged use can cause bradycardia, heart blockage, hypotension, brochospasm, fatigue, and decreased motivation

Caffeine
Increases mental alertness, concentration, catecholamine release, and mobilization and use of FFA by the muscles
Decreases fatigue and lowers perception of effort
Improves endurance performance; may improve sprint and strength performance
Can cause nervousness, insomnia, tremors, diuresis, and lead to dehydration

Cocaine
Blocks reuptake of norepinephrine and dopamine by neurons
Creates feelings of euphoria, alertness, and self-confidence
Masks fatigue and pain
Has no evidence of ergogenic properties; likely ergolytic
Extremely addictive; can cause psychological problems and compromise heart function

Diuretics
Increase urine production and excretion
Used for weight reduction and to mask other drugs during drug testing
Cause weight loss (water loss)
Can lead to dehydration, impaired thermoregulation, and electrolyte imbalances

Marijuana
Acts as a stimulant and depressant of CNS
Impairs performance requiring hand-eye and motor coordination, fast reaction times, tracking ability, and perceptual accuracy
Can lead to personality changes, memory impairment, hallucinations, and psychotic-like behavior
May pose same risks as cigarette smoking (if smoked)

Nicotine
Increases alertness and may calm nervousness
Increases heart rate, blood pressure, autonomic reactivity, vasoconstriction, ADH and catecholamine secretion, blood lipid levels, plasma glucose, glucagon, insulin, and cortisol
Lowers VO2max values (when smoked) and peripheral circulation
.
Is addictive and causes various cancers and cardiovascular diseases

Hormonal Agents
Anabolic steroids
Human growth hormone
Oral contraceptives

Anabolic Steroids
Are nearly identical to male sex hormones; synthetic form maximizes building effects
Increase muscle mass and strength
Can cause testicular atrophy, reduced sperm count, and prostate and breast enlargement in men
Can cause breast regression, masculinization, and menstrual disruption in women
Cause personality changes, liver damage, and cardiovascular disease

BODY CHANGES WITH ANABOLIC STEROIDS

Human Growth Hormone
Secreted naturally by pituitary; synthetic form used by some athletes
Difficult to detect synthetic from natural in drug testing
Proven to increase lipolysis and blood glucose levels; changes in muscle mass and strength are found in some studies, but not in the best controlled studies or studies with athletes
Can cause acromegaly, enlargement of internal organs, muscle and joint weakness, diabetes, hypertension, and heart disease
Oral Contraceptives
Control menstrual cycle
Little research on ergogenic properties
May alleviate symptoms of PMS and restore menstrual cycle
Can cause nausea, weight gain, fatigue, hypertension, liver tumors, blood clots, stroke, or heart attack.
Physiological Agents
Blood doping
Erythropoietin
Oxygen supplementation
Aspartic acid
Bicarbonate loading
Phosphate loading

Blood Doping
Artificial increase in total volume of red blood cells (via transfusion or EPO)
Improves endurance performance by increasing blood’s O2-carrying capacity
Can cause blood clotting, heart failure, and transfusion complications
Increases VO2max, time to exhaustion, and measurable performance
.

VO2MAX AND FATIGUE AFTER BLOOD DOPING
.

PERFORMANCE IMPROVEMENT AFTER BLOOD DOPING

Erythropoietin
Natural hormone produced by the kidneys to stimulate red blood cell production
Can be cloned and administered to increase red blood cell volume
Can cause blood clotting and heart failure due to increased blood viscosity
Increases VO2max and time to exhaustion.

Oxygen Supplementation
Breathed by athlete to increase oxygen content of blood
Can improve performance if administered during exercise, but not before or after
Too cumbersome to be practical
No serious risks known

OXYGEN SUPPLEMENTATION AND PERFORMANCE

Aspartic Acid
An amino acid involved in liver’s conversion of ammonia to urea
Thought to reduce ammonia buildup during exercise and thus offset fatigue
Insufficient and conflicting research of ergogenic properties
No serious risks known

Bicarbonate
Naturally part of body’s buffering system to maintain normal pH
Loading increases blood alkalinity so that more lactate can be cleared (delay fatigue)
Ingesting 300 mg per kg body weight can increase performance in all-out exercise bouts between 1 and 7 minutes
Can cause gastrointestinal cramping, bloating, and diarrhea

BICARBONATE AND BLOOD CONCENTRATIONS

Phosphate
Loading is thought to increase phosphate levels throughout body, which then
Increase potential for oxidative phosphorylation and PCr synthesis
Enhance oxygen release to the cells
Improve cardiovascular response to exercise and buffering and endurance capacities
Studies are divided on results of phosphate loading.
No risks are yet known.

Nutritional Agents
Amino acids
L-carnitine
Creatine
Chromium
Glycerol

Amino Acids
L-tryptophan and BCAA
Proposed to increase endurance performance by delaying fatigue
Studies are inconclusive on effects on performance

Creatine
Supplement to better maintain muscle ATP levels
Shown to increase strength and possibly fat-free body mass
Not shown to help endurance performance, sprint running, or sprint swimming performance

Chromium
Essential trace mineral in foods that helps metabolize carbohydrate, fat, and protein
Often deficient in diets and lost via exercise
Supplements thought to increase glycogen synthesis and amino acid incorporation in muscle and improve glucose tolerance
Studies show little or no benefit


















